52
Therapeutic Effects of Low Frequency Currents on Tissues Lecture IV Dr. Amal Hassan Mohammed Ibrahim [email protected]
| Date post: | 21-Jul-2016 |
| Category: |
Documents |
| Upload: | huxley2378 |
| View: | 15 times |
| Download: | 3 times |
Therapeutic Effects of Low Frequency Currents on
Tissues Lecture IV
Dr. Amal Hassan Mohammed Ibrahim
OBJECTIVES
Review on the difference between high, medium, and low
frequency currents and their therapeutic/clinical implications
OBJECTIVES • Enumerate the characteristics of
the three types of low/medium frequency currents
• Formulate guidelines in the selection and/or prescription of the most appropriate (low/medium frequency current) electrical modality
OBJECTIVES
• Know the main therapeutic effects of low and medium frequency currents used by physiotherapists
A review on the differences…
High Frequency Currents
Medium Frequency Currents
Low Frequency Currents
HIGH FREQUENCY CURRENTS
• Frequency is >6000 H
• Short wavelengths (<10 mm)
• Effects occur only at superficial structures
• General effect = HEATING
• Sample modalities:
US, MWD, SWD, IRR, UVR, LASER
MEDIUM and LOW FREQUENCY CURRENTS
• Frequency ranges from 1 to 6000 Hz
• Longer wavelengths (>10 mm)
• Effects occur at deeper structures
• General effects:
MFC: blocks pain
LFC: nerve stimulation
MEDIUM and LOW FREQUENCY CURRENTS
• Sample modalities:
• Electrical stimulators, Diadynamics, Biofeedback, Iontophoresis, TENS, IF, Faradic and HVPGS
Therapeutic Effects of Low Frequency Currents on
Tissues
• When therapeutic low frequency electric pulses passed through tissues there are some effects on the excitable tissues (nerves and muscles) and on the non excitable tissues (cellular level).
The Effects of Low Frequency Currents on The Excitable Tissues
•1- Modifying pain perception in the central nervous
system.
What is Pain?
• Pain is an unpleasant subjective feeling can be ranged from mild irritation to severe intolerable pain that can be beyond endurance.
• The sensory receptors (nociceptors) are responsible for painful stimuli which are free nerve endings found in almost all types of body tissues.
Why feel pain?
• Gives conscious awareness of tissue damage
• Protection:
– Remove body from danger
– Promote healing by preventing further damage
– Avoid noxious stimuli
• Elicits behavioral and emotional responses
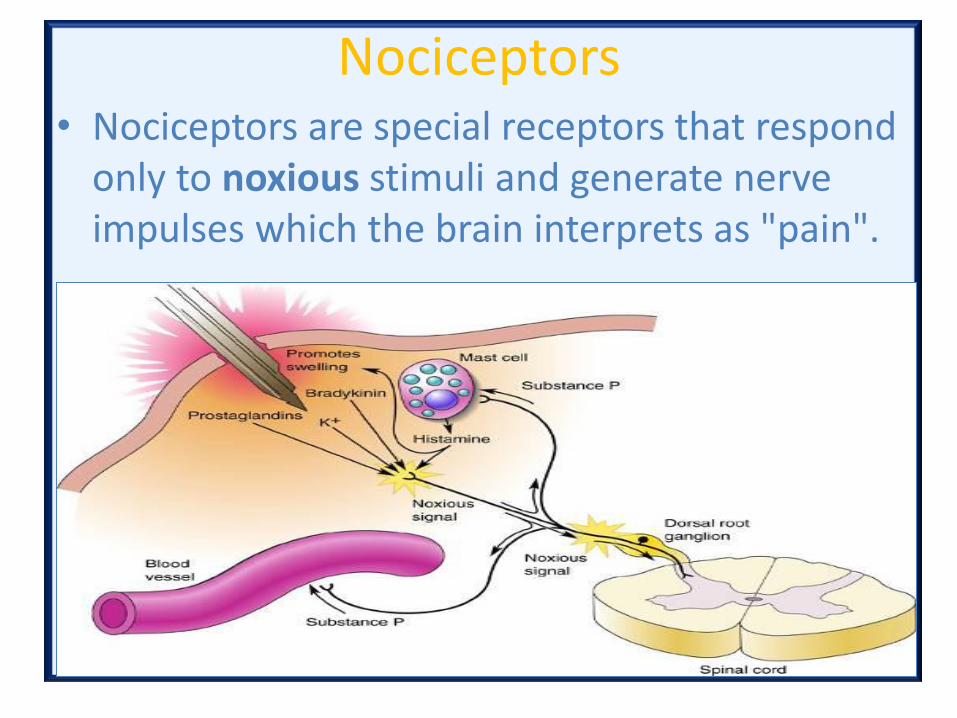
Nociceptors • Nociceptors are special receptors that respond
only to noxious stimuli and generate nerve impulses which the brain interprets as "pain".
1- Modifying pain perception in the central nervous system.
• The nociceptors are of two afferent types:
• Small diameter myelinated nerve fiber, A delta (Aδ ) which is responsible for sharp, pricking, acute, and fast pain.
• Small diameter non-myelinated nerve fiber (C fiber) which is responsible for dull, throbbing, burning, chronic, and slow pain.
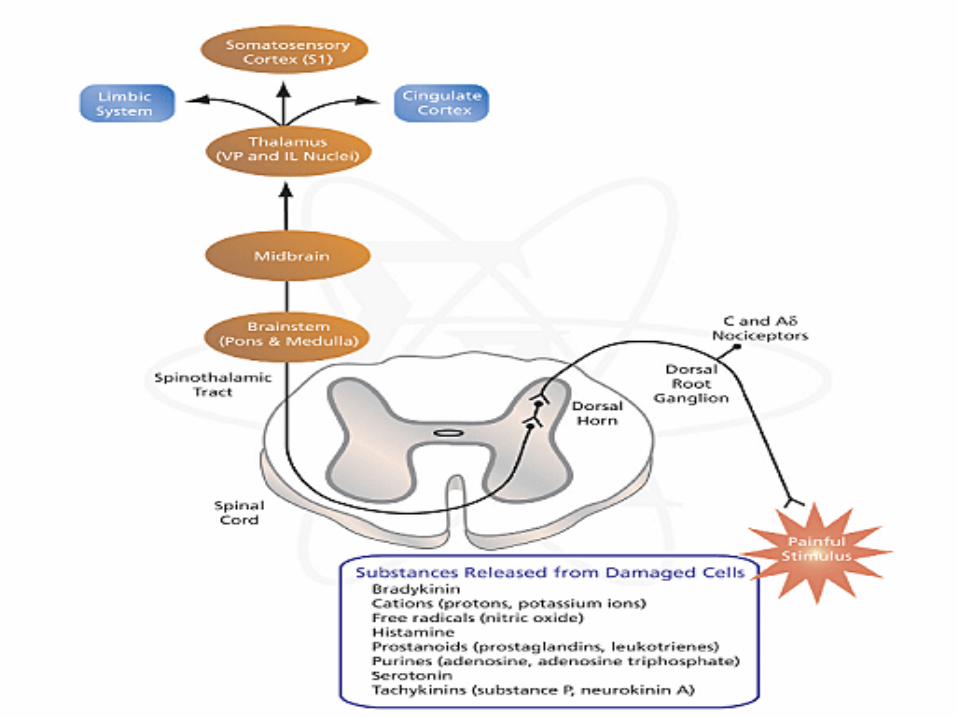
1- Modifying pain perception in the central nervous system
• Both of nociceptors are responding to a variety of stimuli (mechanical, thermal, and chemical) that can damage tissues.
• The activated nociceptors and damaged tissues release some chemical mediators like substance P, histamine, bradykinin, serotonin and prostaglandins.
Central Pathway of Pain
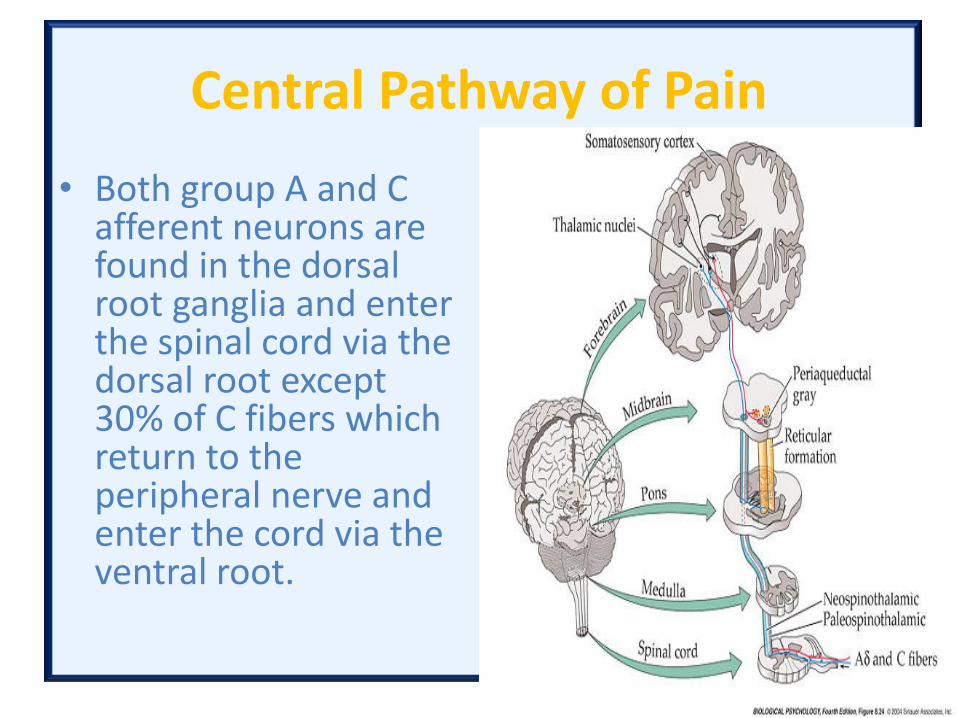
• Both group A and C afferent neurons are found in the dorsal root ganglia and enter the spinal cord via the dorsal root except 30% of C fibers which return to the peripheral nerve and enter the cord via the ventral root.
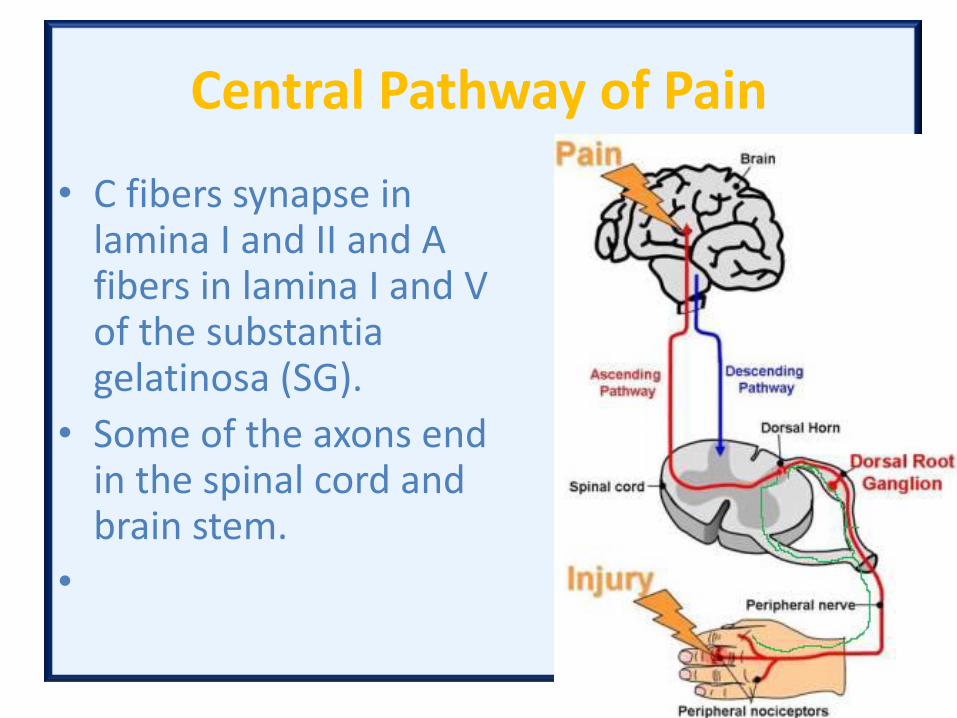
Central Pathway of Pain
• C fibers synapse in lamina I and II and A fibers in lamina I and V of the substantia gelatinosa (SG).
• Some of the axons end in the spinal cord and brain stem.
•
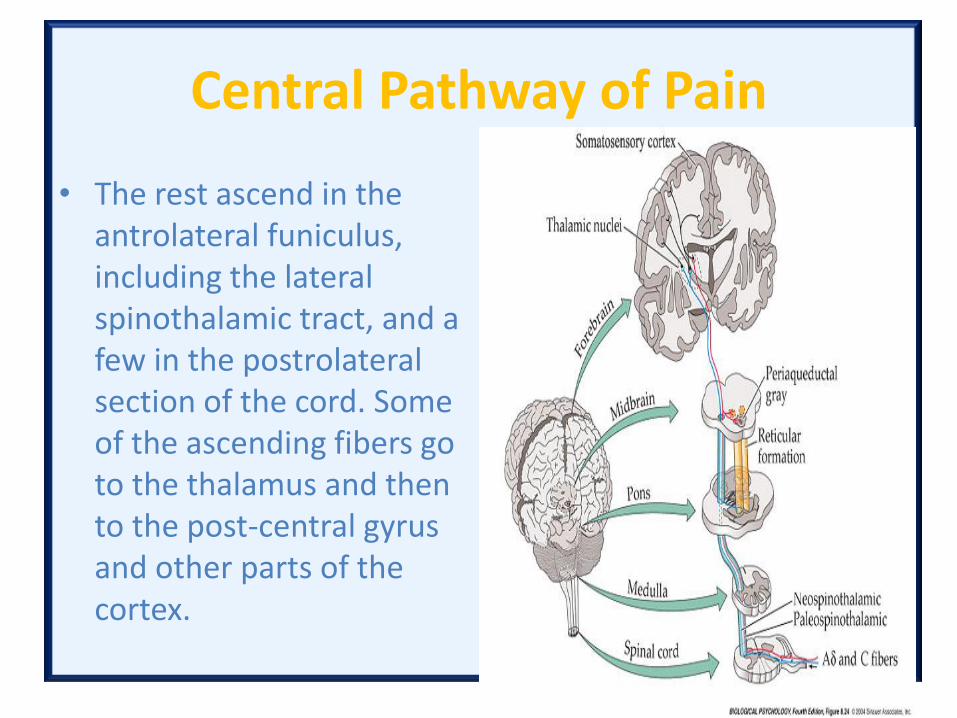
Central Pathway of Pain
• The rest ascend in the antrolateral funiculus, including the lateral spinothalamic tract, and a few in the postrolateral section of the cord. Some of the ascending fibers go to the thalamus and then to the post-central gyrus and other parts of the cortex.

Central Pathway of Pain
• Many go to the reticular formation, while others go to the hypothalamus and the periaqueductal grey matter. The synaptic transmitter of the primary afferent pain fibers is substance P
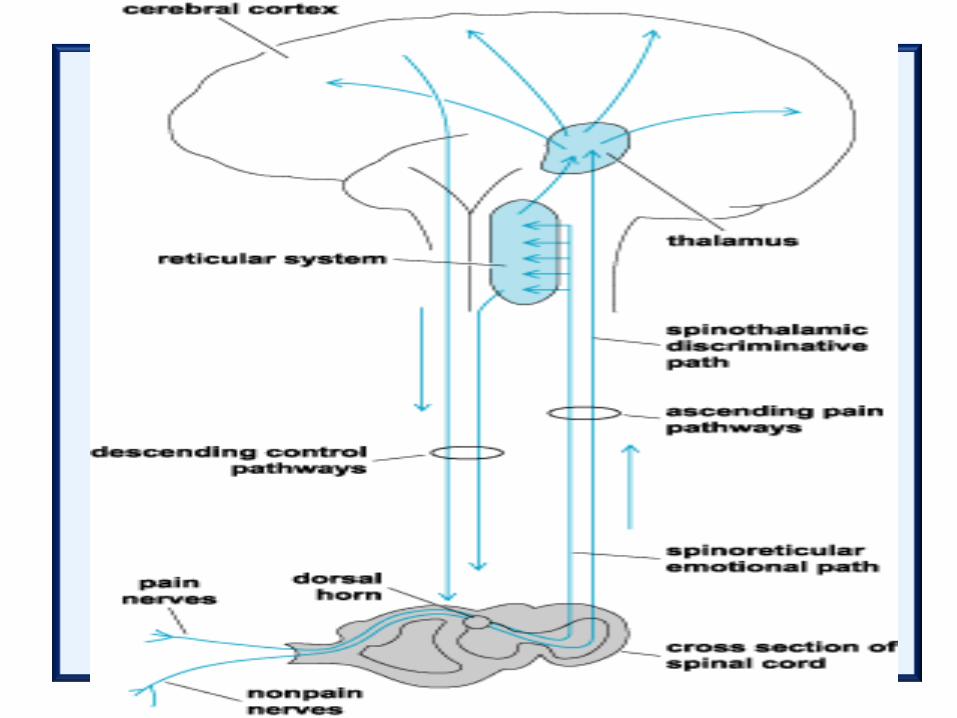
Control of pain by electrical stimulation
• The modulation of pain transmission by altering afferent input to the spinal cord is known as the gate-control theory, which was established by Melzack and Wall in 1965.
Control of pain by electrical stimulation
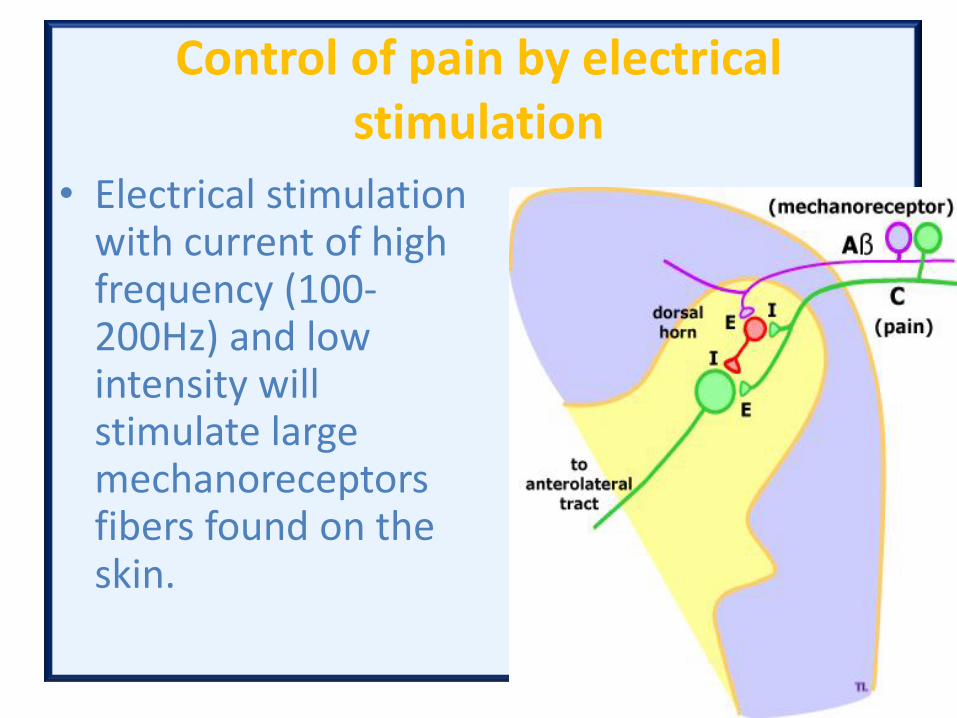
• Electrical stimulation with current of high frequency (100-200Hz) and low intensity will stimulate large mechanoreceptors fibers found on the skin.
Control of pain by electrical stimulation
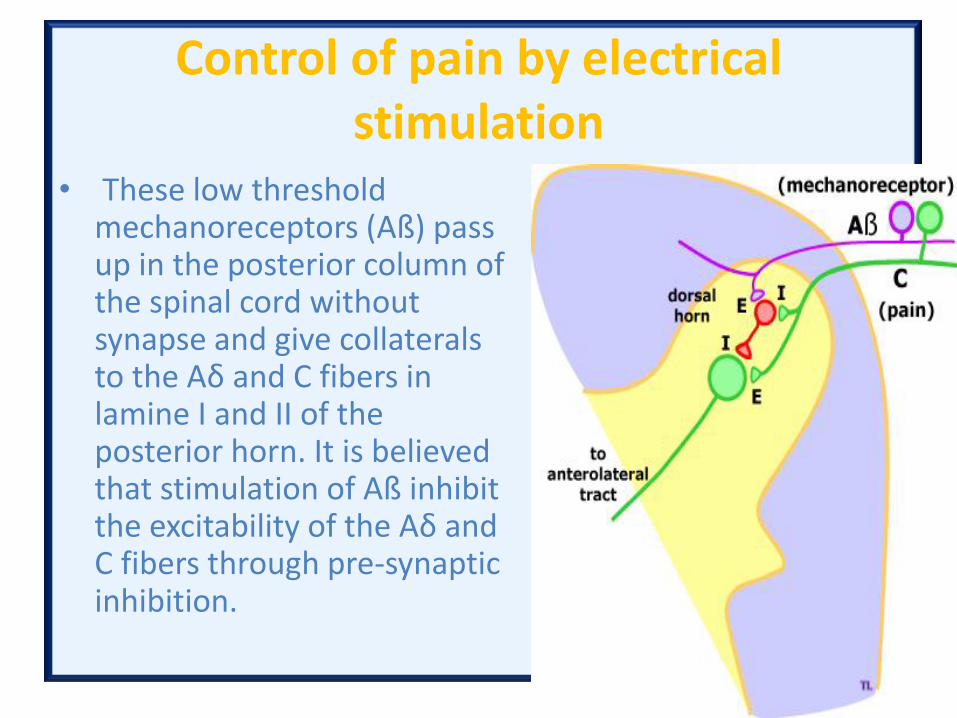
• These low threshold mechanoreceptors (Aß) pass up in the posterior column of the spinal cord without synapse and give collaterals to the Aδ and C fibers in lamine I and II of the posterior horn. It is believed that stimulation of Aß inhibit the excitability of the Aδ and C fibers through pre-synaptic inhibition.
Control of pain by electrical stimulation
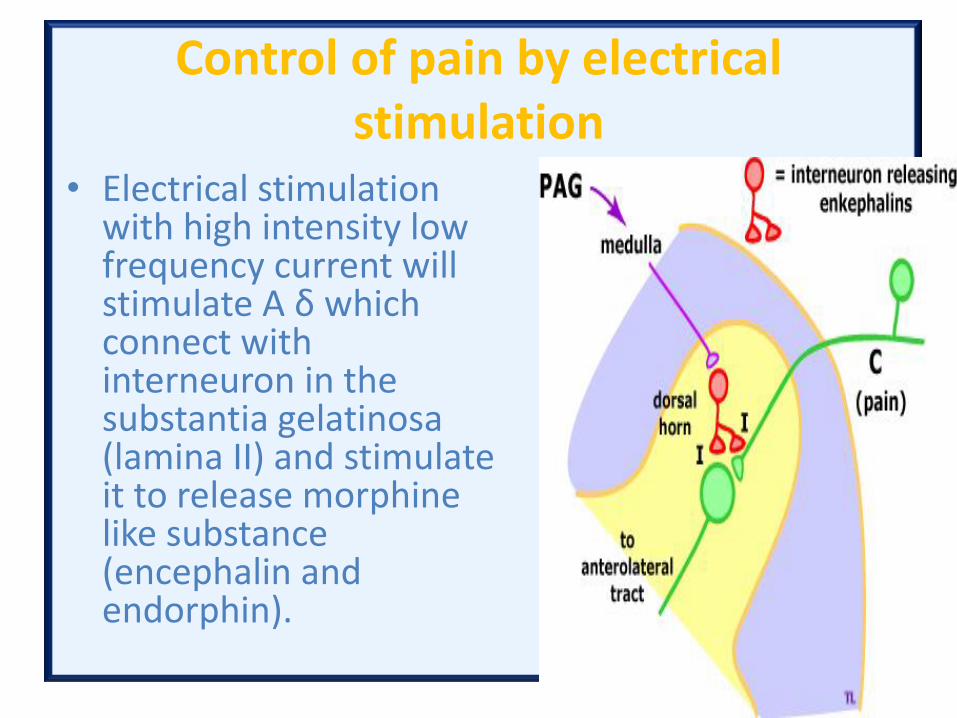
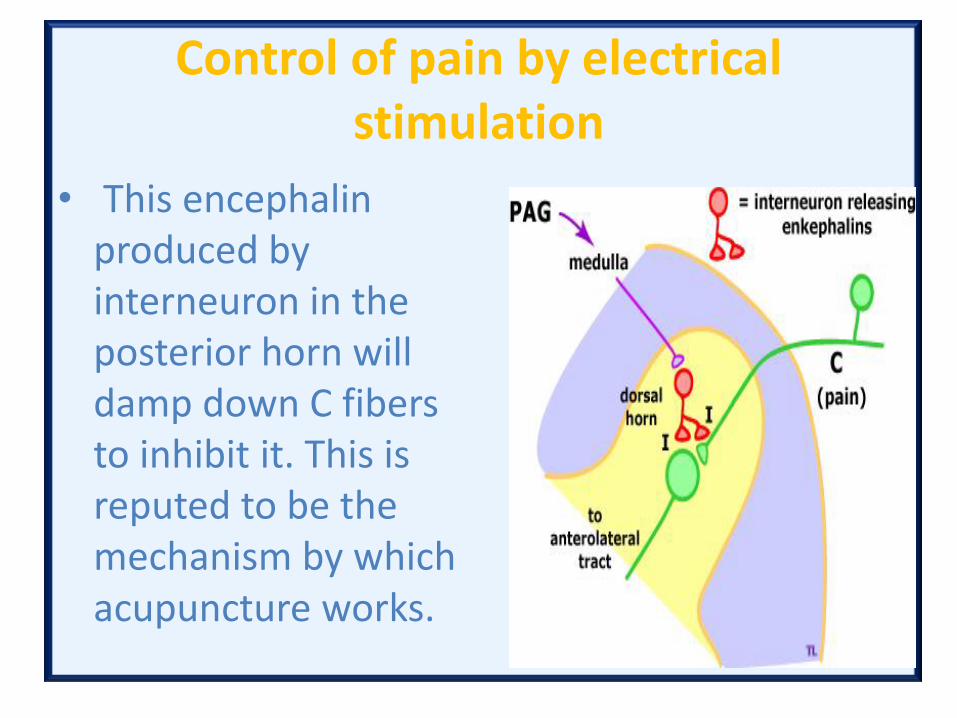
• Electrical stimulation with high intensity low frequency current will stimulate A δ which connect with interneuron in the substantia gelatinosa (lamina II) and stimulate it to release morphine like substance (encephalin and endorphin).
Control of pain by electrical stimulation
• This encephalin produced by interneuron in the posterior horn will damp down C fibers to inhibit it. This is reputed to be the mechanism by which acupuncture works.
Control of pain by electrical stimulation
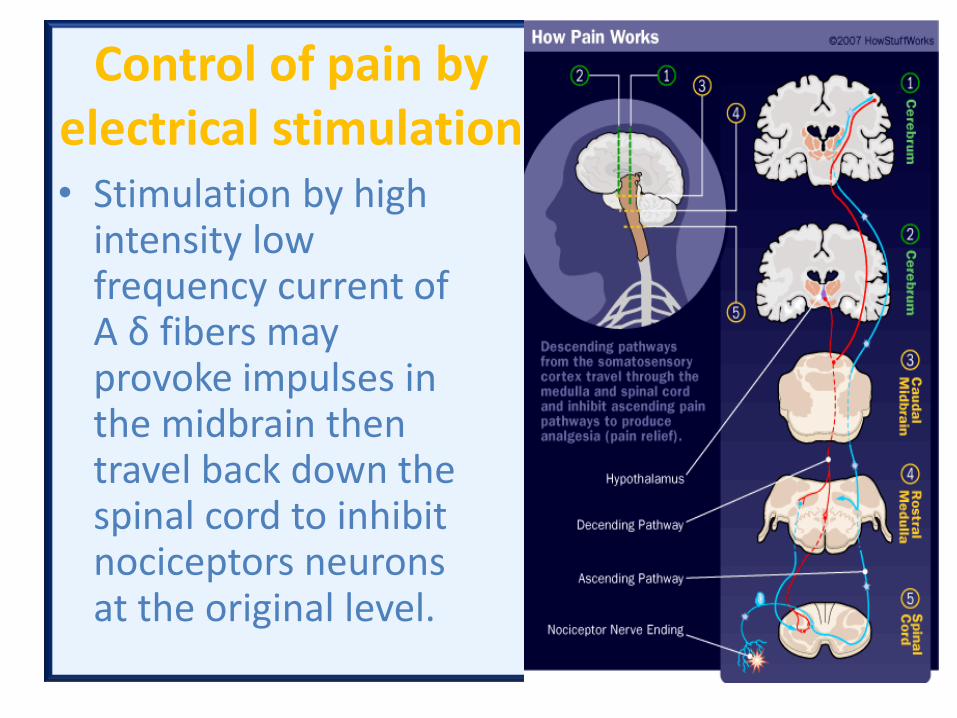
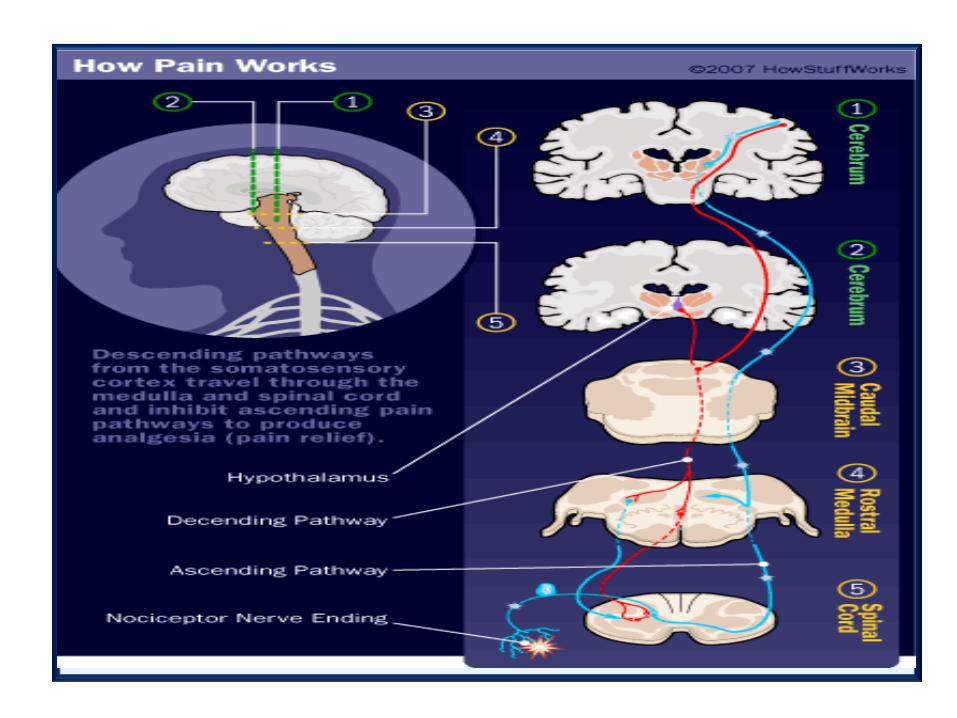
• Stimulation by high intensity low frequency current of A δ fibers may provoke impulses in the midbrain then travel back down the spinal cord to inhibit nociceptors neurons at the original level.
Control of pain by electrical stimulation
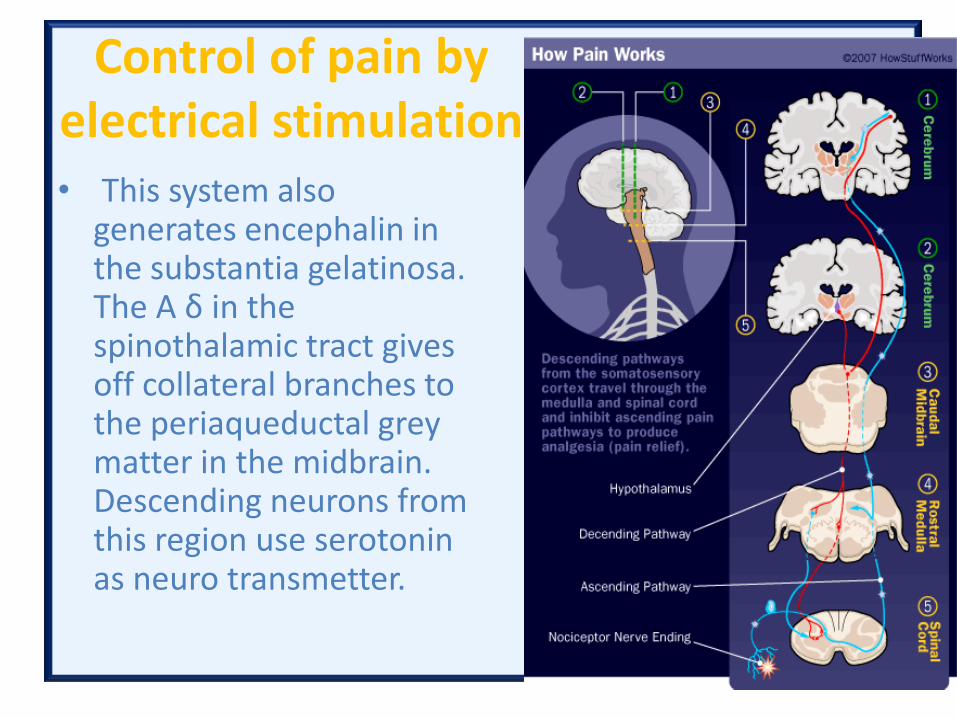
• This system also generates encephalin in the substantia gelatinosa. The A δ in the spinothalamic tract gives off collateral branches to the periaqueductal grey matter in the midbrain. Descending neurons from this region use serotonin as neuro transmetter.
2- Electrical stimulation of innervated muscles
• Before discussing the difference between voluntary contraction and contraction by using electrical stimulation we must know some scientific facts:
• - There are two types of muscle fibers have these characteristics
2- Electrical stimulation of innervated muscles
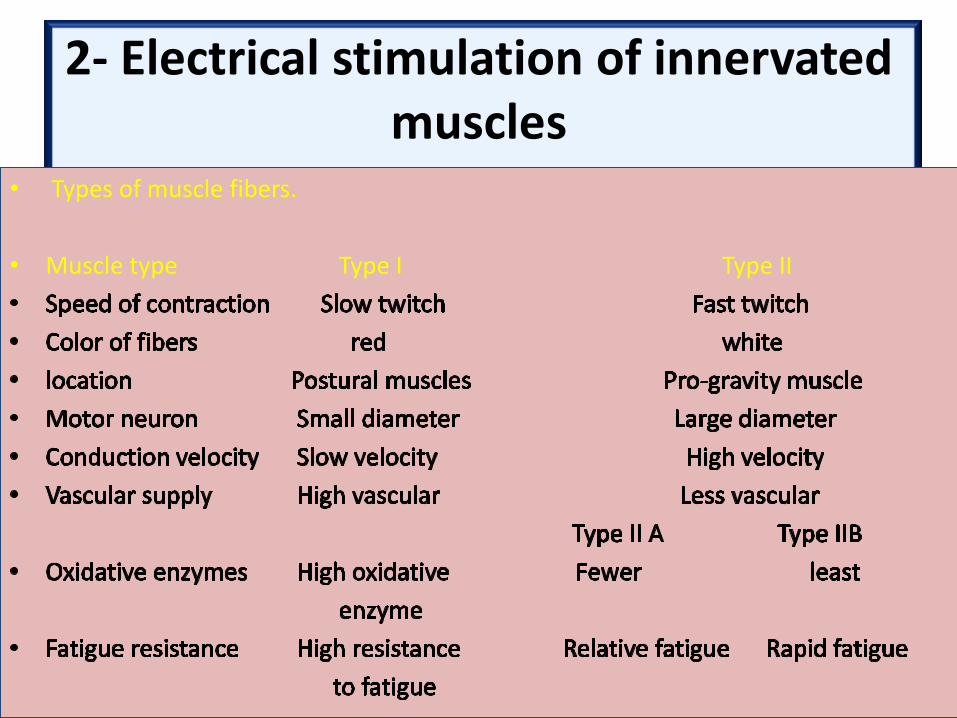
• Types of muscle fibers.
• Muscle type Type I Type II
2- Electrical stimulation of innervated muscles
• The structure of living muscle is variable. There is a balance between synthesis and breakdown of muscle proteins (about 10% of muscle fibers). These process occurring at higher rate in type I slow twitch than in type II fast twitch.
• More anabolic than catabolic will lead to muscle hypertrophy.
• More catabolic than anabolic lead to muscle atrophy.
2- Electrical stimulation of innervated muscles
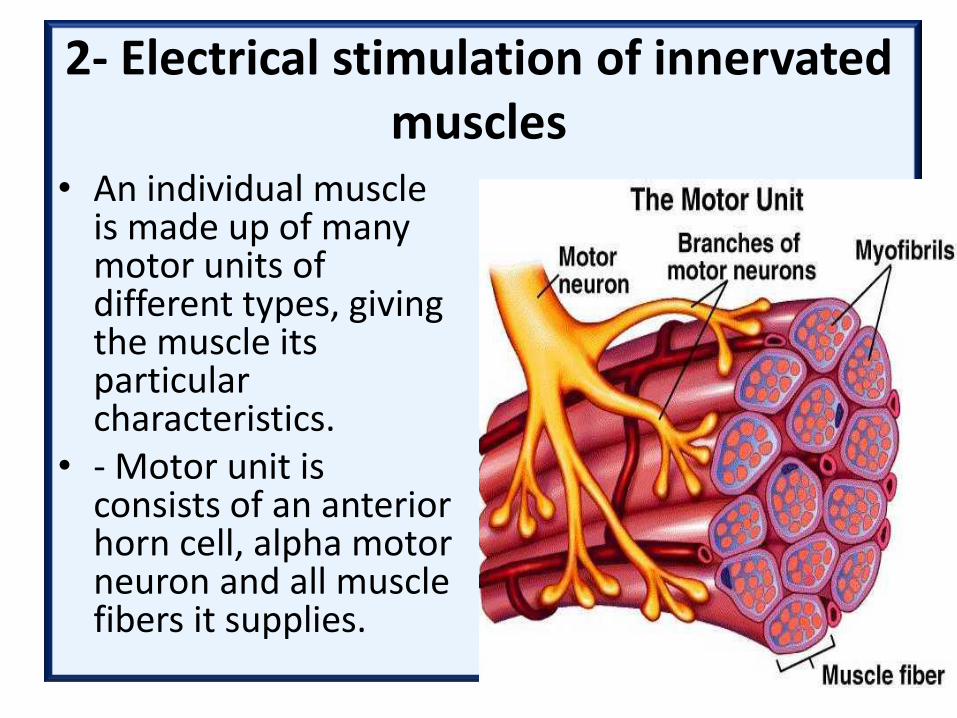
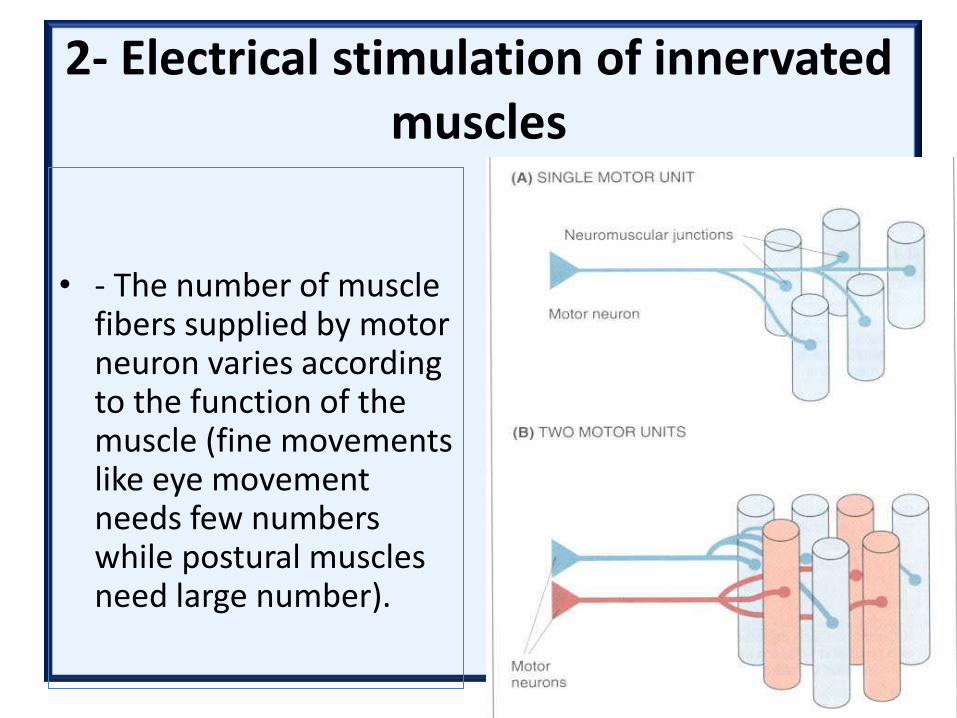
• An individual muscle is made up of many motor units of different types, giving the muscle its particular characteristics.
• - Motor unit is consists of an anterior horn cell, alpha motor neuron and all muscle fibers it supplies.
2- Electrical stimulation of innervated muscles
• - The number of muscle fibers supplied by motor neuron varies according to the function of the muscle (fine movements like eye movement needs few numbers while postural muscles need large number).
2- Electrical stimulation of innervated muscles
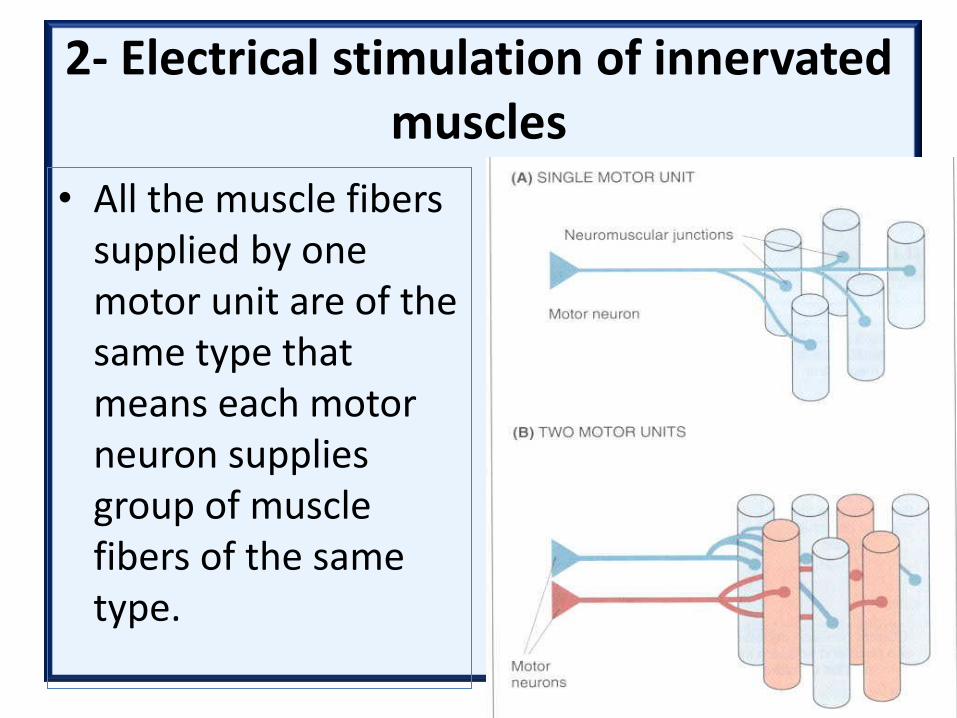
• All the muscle fibers supplied by one motor unit are of the same type that means each motor neuron supplies group of muscle fibers of the same type.
2- Electrical stimulation of innervated muscles
• - During voluntary contraction of muscle there is smooth contraction due to asynchronous firing of motor neuron.
• - Force of contraction is graded by an increase in the number of motor unit recruited (spatial summation) and increase in frequency of nerve impulse (temporal summation).
2- Electrical stimulation of innervated muscles
• Electrical stimulation to produce muscle contraction is differing from voluntary contraction in these points:
• - Synchronous firing of all motor neurons stimulated.
• - Large diameter motor neurons (type II) are stimulated first.
• - The frequency of firing is fixed unlike voluntary contraction.
• - Sensory nerves are inevitably stimulated.
2- Electrical stimulation of innervated muscles
• Electrical stimulation of muscle through motor nerve will lead to rapid muscle fatigue due to fixed stimulated number of motor units and stimulation of type II fast muscle fibers first.
• - The degree and duration of muscle fatigue is directly related to the extent of the electrical stimulation.
Uses of electrical stimulation for innervated muscle
• Strength muscles as shown by Hon Sun Lai et al. (1988) that electrical stimulation of muscles for 3 weeks gain more muscle strength in group treated with high intensity current than other group treated with low intensity current. The force of isometric contraction showed greater gain than that of concentric contraction. Eccentric contraction showed no significant gain.
Uses of electrical stimulation for innervated muscle
• Reduce of muscle atrophy by maintenance of protein synthesis in muscle rather than preventing protein breakdown in cases of inhibited muscle contraction due to pain (as to stimulate quadriceps muscle after knee injury or surgery) or during splinting to maintain muscle power.
Uses of electrical stimulation for innervated muscle
• Stimulation of muscles very difficult to be under voluntary control like pelvic floor muscles and lumbricals in postural flatfoot.
·• Stimulation of muscle or motor nerve has been transplanted to new action.
·• Later stage of recovery of peripheral nerve lesion.
• For hysterical paralysis.
Uses of electrical stimulation for innervated muscle
• In cerebral palsy to enhance muscle contraction.
·• Increase ranges of motion by stretch shorten and contracture muscles as in cases of hemiplegia and scoliosis.
• Electrical stimulation of innervated muscle will lead to increase metabolism and blood flow (increase oxygen uptake, carbon dioxide, lactic acid, and local temperature).
• Increasing muscle contraction by electrical stimulation will lead to increase venous return and lymphatic flow which help in reducing odema.
Uses of electrical stimulation for innervated muscle
• Increasing muscle contraction by electrical stimulation will lead to increase venous return and lymphatic flow which help in reducing oedema.
• Electrical stimulation to reduce spasticity by stimulating agonist muscle or antagonist or alternating approach to stimulate agonist and antagonist.
• ·• The most current used for stimulation of innervated muscle is faradic current or similar electrical pulses applied to cause muscle contraction.
Uses of electrical stimulation for innervated muscle
Use of electrical stimulation for long term to change the contractile properties of the muscle fiber (convert fast twitch muscle fibers to slow twitch muscle fiber in animals by using of low frequency current). The changes started in the muscle membrane and capillary circulation and completed with exchange of fast to slow type myosin.
Uses of electrical stimulation for innervated muscle
These effect have also demonstrated in humans by Scott et al., 1985, by using low frequency current (10 Hz) to stimulate popliteal nerve, for one hour three times daily for 6 weeks at a sufficient intensity to give visible contraction of the tibialis anterior. This lead to significant increase in resistance to fatigue suggesting a change in the properties of type II muscle fibers.
Uses of electrical stimulation for innervated muscle
• Eutrophic electrotherapy is the record of frequencies of the motor unit action potential by electromyogram and used to determine the frequency of the muscle to improve the functional ability. Eutrophic electrotherapy used in Bell’s palsy and applied to quadriceps muscles of elderly subjects with disuse atrophy.

3- Electrical stimulation of denervated muscle
• When muscle is denervated many structural and functional changes occur like loss of voluntary and reflex activity, atrophy, degeneration and fibrosis. In addition to these changes fibrillation and spontaneous contraction occur.
3- Electrical stimulation of denervated muscle
• There are many differences between electrical stimulation of innervated and electrical stimulation of denervated muscles including:
• - Denervated muscle contract due to direct stimulation of the muscle fibers because there is no nerve supply.
• - Muscle tissue is less excitable than nerve so that more electric charge is needed.
3- Electrical stimulation of denervated muscle
• Current with sufficient pulse duration (more than 30 ms) and appropriate intensity in a square wave form is suitable for stimulation of denervated muscle.
• - Pulses with short duration need more intensity to provoke muscle contraction (strength duration curve).
3- Electrical stimulation of denervated muscle
• The rate of contraction and relaxation of denervated muscle is slower than innervated muscle. The contraction of denervated muscle by using electrical stimulation is called ‘worm-like’ contraction.
3- Electrical stimulation of denervated muscle
• Muscle fibers have less ability to accommodate than nerve (nerve accommodation is due to slow rising pulses which provide slow ionic changes), so that slow changes can stimulate muscle fibers by means of slow rising triangular pulses.
• - Electrical stimulation for denervated muscle maintain it healthy as possible as we can (used as artificial exercises until reinnervation occur).
Questions????????

















