A HOT REVIEW OF BASIC BIOMECHANICS....................................................................................................................................................................................................................................... 2 MATRIX MOLECULES ........................................................................................................................................................................................................................................................................ 2 STRUCTURE AND FUNCTION OF BONE ................................................................................................................................................................................................................................................... 3 BONE DEGRADATION ........................................................................................................................................................................................................................................................................ 4 STRUCTURE AND FUNCTION OF CARTILAGE, LIGAMENTS, TENDONS, DIARTHRODIAL JOINTS ...................................................................................................................................................... 5 JOINT DISEASE................................................................................................................................................................................................................................................................................. 6 LIGAMENTS AND TENDONS ................................................................................................................................................................................................................................................................. 6 CONTROL OF CONNECTIVE TISSUE (BONE) METABOLISM .............................................................................................................................................................................................................. 6 BONE METABOLISM ......................................................................................................................................................................................................................................................................... 7 PATHOPHYSIOLOGY ........................................................................................................................................................................................................................................................................ 8 GOUT............................................................................................................................................................................................................................................................................................ 8 ANKYLOSING SPONDYLITIS.................................................................................................................................................................................................................................................................. 9 LYME DISEASE ............................................................................................................................................................................................................................................................................... 10 TEMPORAL ARTERITIS (GIANT CELL ARTERITIS)...................................................................................................................................................................................................................................... 11 JUVENILE IDIOPATHIC ARTERITIS (JIA) ................................................................................................................................................................................................................................................. 12 SYSTEMIC LUPUS ERYTHEMATOUS (SLE) ............................................................................................................................................................................................................................................. 13 MARFAN SYNDROME ...................................................................................................................................................................................................................................................................... 15 REACTIVE ARTHRITIS ....................................................................................................................................................................................................................................................................... 15 SJOGREN SYNDROME .................................................................................................................................................................................................................................................................... 16 SALIVARY GLAND AND SALIVA REVIEW ................................................................................................................................................................................................................................................ 16 SJOGRENS SYNDROME..................................................................................................................................................................................................................................................................... 16 OSTEOMALACIA, IMPLANTS, BONE GRAFTING AND MRONJ ........................................................................................................................................................................................................ 18 OSTEOMALACIA ............................................................................................................................................................................................................................................................................. 18 BONE GRAFTING AND IMPLANTS........................................................................................................................................................................................................................................................ 19 IMPLANTS .................................................................................................................................................................................................................................................................................... 19 MEDICATION-RELATED OSTEONECROSIS OF THE JAW (MRONJ) ............................................................................................................................................................................................................... 20 MUSCULOSKELETAL PHARMACOLOGY ......................................................................................................................................................................................................................................... 21 MUSCLE RELAXANTS ....................................................................................................................................................................................................................................................................... 21 RHEUMATOLOGY AND OSTEOPOROSIS DRUGS....................................................................................................................................................................................................................................... 25 PBL 1 – ANNA WRIGHT .................................................................................................................................................................................................................................................................. 29 PHYSIOLOGIC CHANGES DURING PREGNANCY........................................................................................................................................................................................................................................ 29 MORNING SICKNESS VS. ORAL HEATH ................................................................................................................................................................................................................................................ 30 FETAL RISK WITH DRUGS.................................................................................................................................................................................................................................................................. 30 DENTAL CONSIDERATIONS................................................................................................................................................................................................................................................................ 31 PBL 2 – SIGMA CHI-GUY ................................................................................................................................................................................................................................................................ 32 BRUXISM ..................................................................................................................................................................................................................................................................................... 32 TEMPOROMANDIBULAR DYSFUNCTION................................................................................................................................................................................................................................................ 32 TRISMUS ...................................................................................................................................................................................................................................................................................... 34 PBL 3 - BETTINA ............................................................................................................................................................................................................................................................................. 34 SMART BMI ................................................................................................................................................................................................................................................................................. 34 BONES......................................................................................................................................................................................................................................................................................... 35 ELDERLY INJURIES........................................................................................................................................................................................................................................................................... 35 MANDIBLE FRACTURE ..................................................................................................................................................................................................................................................................... 36 STAGES OF FRACTURE HEALING ......................................................................................................................................................................................................................................................... 37 AFTER-CARE TREATMENT OF FRACTURES .............................................................................................................................................................................................................................................. 38 BONE REMODELLING ...................................................................................................................................................................................................................................................................... 38 PBL 4 – JACKIE FALLS ..................................................................................................................................................................................................................................................................... 39 OSTEOPOROSIS.............................................................................................................................................................................................................................................................................. 39 POLYMYALGIA RHEUMATICA ............................................................................................................................................................................................................................................................. 41 MRONJ (MEDICATION RELATED OSTEONECROSIS OF THE JAW) ............................................................................................................................................................................................................... 41 PBL 5 – MRS. STEPHANIE CURRY ................................................................................................................................................................................................................................................... 42 RADIOGRAPHS OF TMJ ................................................................................................................................................................................................................................................................... 42 ARTHRITIS .................................................................................................................................................................................................................................................................................... 42 GENETIC PREDISPOSITION............................................................................................................................................................................................................................................................. 44 VARIATIONS IN THE GENOME ............................................................................................................................................................................................................................................................ 45 DENTAL TRAITS WITH GENETIC BASIS.................................................................................................................................................................................................................................................. 46 PHARMAGOGENOMICS .................................................................................................................................................................................................................................................................... 46 EPIGENETICS ................................................................................................................................................................................................................................................................................. 46
Transcript
A HOT REVIEW OF BASIC BIOMECHANICS....................................................................................................................................................................................................................................... 2
STRUCTURE AND FUNCTION OF BONE ................................................................................................................................................................................................................................................... 3
BONE DEGRADATION ........................................................................................................................................................................................................................................................................ 4
STRUCTURE AND FUNCTION OF CARTILAGE, LIGAMENTS, TENDONS, DIARTHRODIAL JOINTS ...................................................................................................................................................... 5
LIGAMENTS AND TENDONS ................................................................................................................................................................................................................................................................. 6
CONTROL OF CONNECTIVE TISSUE (BONE) METABOLISM .............................................................................................................................................................................................................. 6
BONE METABOLISM ......................................................................................................................................................................................................................................................................... 7
OSTEOMALACIA, IMPLANTS, BONE GRAFTING AND MRONJ ........................................................................................................................................................................................................ 18
BONE GRAFTING AND IMPLANTS ........................................................................................................................................................................................................................................................ 19
MEDICATION-RELATED OSTEONECROSIS OF THE JAW (MRONJ) ............................................................................................................................................................................................................... 20
RHEUMATOLOGY AND OSTEOPOROSIS DRUGS....................................................................................................................................................................................................................................... 25
PBL 1 – ANNA WRIGHT .................................................................................................................................................................................................................................................................. 29
PHYSIOLOGIC CHANGES DURING PREGNANCY ........................................................................................................................................................................................................................................ 29
MORNING SICKNESS VS. ORAL HEATH ................................................................................................................................................................................................................................................ 30
FETAL RISK WITH DRUGS.................................................................................................................................................................................................................................................................. 30
STAGES OF FRACTURE HEALING ......................................................................................................................................................................................................................................................... 37
AFTER-CARE TREATMENT OF FRACTURES .............................................................................................................................................................................................................................................. 38
BONE REMODELLING ...................................................................................................................................................................................................................................................................... 38
MRONJ (MEDICATION RELATED OSTEONECROSIS OF THE JAW) ............................................................................................................................................................................................................... 41
RADIOGRAPHS OF TMJ ................................................................................................................................................................................................................................................................... 42
VARIATIONS IN THE GENOME ............................................................................................................................................................................................................................................................ 45
DENTAL TRAITS WITH GENETIC BASIS .................................................................................................................................................................................................................................................. 46
Adhesion Kinase - Talin - Plectin - Alpha - Actinin
Involved in cell migration and adhesion in proteoglycan rich matrices - Low affinity (allows cells to move) - Important in development, nervous system, inflammation
and wound healing
Molecule Function Analogy
Collagens - Tendon - Ligament - Type I Collagen - Bone (Type 1 Collagen mineralized
with calcium phosphate)
Provide Tensile Strength
Elastics - Elastin - Blood Vessels (not a molecule but
whatever)
Provide Elasticity/stretch
Proteoglycans - Cartilage (type II collagen mesh w/
aggrecan/proteoglycans)
Resistance to compressive forces
Structure and Function of Bone Cell Function
Osteoblasts Deposit bone matric
Osteocytes Mechanical sensors (deem whether or not to degrade or build bone)
Osteoclasts Degrade bone
Step 1: Collagen - All fibrillar collagens are 1/3 glycine -> Smallest and simplest amino acid, the only one that will fit within the center of a triple helix
- High content of proline -> Puts a kink in chain to create the helical shape
- Hydroxyproline and hydroxylysine -> presumably also contribute to the shape?
- Long sequences of (Gly-X-Y)n -> Frequently (Gly-Pro-Hydroxypro)n
- Red = Glycine. It’s a constant, regardless of the polypeptide on the outside.
- Every 3rd residue is always glycine. Many genetic disorders in collagen involve a glycine mutation,
making the proteins fold incorrectly
- Pretty self-explanatory depiction of collagen formation…seen it 100 times
- If folding fucks up (step 5) then the proteins are exported to cytosol and recycled -> if everything
works fine, then it wont get secreted.
- Different genes code for alpha chains in different tissues -> How we get different types of
cartilage.
Step 2: Mineralization - Collagen laid down and is mineralized by osteoblasts
a. Proteoglycanases degrade proteoglycan to create a gap in between collagen rods
b. Phosphoproteins with 3 phosphates fill in the gap created
c. Osteoblasts secrete alkaline phosphatase -> Cleaves phosphates from the
phosphoproteins = ↑ free phosphate
d. Ca++ binds the phosphate and crystalizes = CaPO4 -> Matures into hydroxyapatite
- Osteoblast matrix vesicles (cellular processes) are covered in membrane bound alkaline phosphatase to start the mineralization reaction
Bone Degradation - Controlled by Osteoclasts, occurs at the ruffled border of these cells
a. ATP dependent proton pump creates a low pH -> Dissolves the mineralized bone
o pH creates protection from inhibitors that would stop the demineralization
o 10% of serum proteins are designed and dedicated to neutralizing the low pH
in the ruffled border to control the process
b. High content of lysosomal proteinases to degrade collagen once the acid has
demineralized
During bone remodeling a Degradation/Formation effort is balanced together:
- Regulated by the mechanical censorship of osteocytes -> influence osteoblasts which influence osteoclast proliferation and activity
- At the leading edge are the osteoclasts, moving forward and eating through old bone
- Behind the osteoclasts blood vessels form which contain stem cells needed to follow the bone cell lineage -> Forms pre-osteoblast and
osteoblasts
- Pre-osteoblasts mature into osteoblasts behind the osteoclasts and synthesize sheets of type 1 collagen that will be the starting point of
lamellae ring formation around the osteon.
- Osteocytes sense mechanical stimulation to regulate the remodelling
- Osteoblasts then mineralize the lamellae
Endochondral Bone Formation Intramembranous Bone Formation
- Cartilage model is made first - Perichondrial cells develop into osteoblasts which mineralize the cartilage template - Extension predominantly occurs at growth plate
- No cartilage model - Compact and spongy bone develops directly from sheets of
mesenchymal (undifferentiated) connective tissue. - Flat bones of the face, most of the cranial bones, and the
clavicles (collarbones) are formed via intramembranous ossification
Mandible
- Both Endochondral and Intramembranous Formation Endochondral
- Entire body of the mandible (Except Anterior portion) - Ramus of the Mandible up to mandibular Foramen
Intramembranous
- Anterior portion of the mandible (symphysis) - Coronoid process - Condylar Process
Trabecular bone stores calcium -> can be readily released under the control of parathyroid hormone
- Inside of the mandible surrounded by a layer of compact bone
Structure and Function of cartilage, ligaments, tendons, diarthrodial joints Proteoglycan = glycoprotein containing glycosaminoglycans
Aggrecan
- Aggregating proteoglycan of cartilage -> Forms large aggregates with hyaluronan (a polysaccharide)
o Hyaluronic acid is extruded through a pore (strange) and can by mm long! Very important
molecule for cartilage
- Core is covalently linked to >100 chondroitin sulphate chains (VERY –‘ve charge)
o Chondroitin sulfate imparts the –‘ve charge. Up to 3 –‘ve charges per molecule!
o Marketed as Tx for oseoarthritis, but there is no evidence of it working directly
o –‘ve charge attracts +’ve ions = creates osmotic pressure = water surrounds molecule =
provides cushing effect
- Entrapped in a matrix of Type II collagen, within the “bag” hydrated glycosaminoglycan-rich matrix
provides resistance to compression
- Blue = hyaline cartilage -> Providing
the impact resistance for the joint.
Collagen is actually highly organized and non-random
- Attached to the subchondral bone with woven vertical fibers (Tide mark = attachment site)
- At the “artificial split line” the vertical collagen fibers transition to a horizontal orientation
o Can peel off the layer above artificial split line -> Lamina Splendens (Its so splendid)
TMJ
- Considered a synovial joint
- Articulating surfaces are considered fibrocartilage, have more collagen than a
typical diarthrodial joint
Joint Disease Osteoarthritis – Involves spicules in the joint and bony enlargement
- Age related wear and tear mostly -> Inability of cartilage to accurately repair damage
- Hyaline cartilage is replaced with fibrocartilage -> Picks up CaPO4 and mineralizes = find bony bits within a joint (calcification)
Inflammatory Arthritis
- Joint inflammation leading to cartilage degradation and skeletal remodelling
Ligaments and Tendons - Type I collagen -> very high tensile strength
- Depending on the ligament or tendon might contain elastic fibers or cartilage-like regions.
- Collagen fibers contain small proteoglycans considered as “spacers” during assembly (This is the starting point for bone formation as well)
Control of Connective Tissue (Bone) Metabolism Wolff’s Law -> If you don’t use it you lose it!
- Bones grow and remodel throughout life to adapt to mechanical environment. Bone is able to sense stress and respond to mechanical
loads.
Review of terms
Axial Skeleton Head, Neck, Trunk (Spine and Ribcage)
Appendicular Skeleton Bone of limbs (includes Pelvis and Clavicle)
Skeleton Cartilage AND Bone, surrounded by perichondrium and periosteum
Intramembranous Ossification Mesenchymal bone DIRECTLY formed during embryonic and prenatal periods - Cranial Bones - Growth at sutures (& Periosteal surface) -> Osteoid synthesized and mineralized directly w/o
cartilage model - Flat Bones
Endochondral Ossification Cartilage models formed during the fetal period -> Bone replaces cartilage after birth - Long Bones
Osteoid Type I collagen-rich matrix that will later mineralize to form bone - Analogous to Pre-Dentin
Bone Function Mechanical support Movement Storage (Calcium) Synthesis of blood cells (RBC, WBC etc)
Bone Metabolism = Balance between bone synthesis and bone degradation
- Involves regulation of activity and generation of osteoblasts and osteoclasts
- Osteoblasts produce and express RANKL to Osteoclast precursors
- RANKL binding to RANK on the precursor = initiates gene transcription for
- Osteoprotegerin (OPG) is also created by Osteoblasts in presence of growth factors and
cytokines
- OPG intercepts RANKL and prevents it from binding to RANK -> ↓ Osteoclast activation,
↑ bone formation
Regulation of Bone Metabolism
** Osteoclasts controlled mostly by signals from osteoblasts**
Parathyroid Hormone regulation of Ca++
↑ PTH = ↑ RANKL production, ↓ OPG production by osteoblasts = ↑ RANKL binding and ↓ OPG regulation of osteoclasts
o ↑ Osteoclasts = ↑ dissolution of bone = ↑ Ca++ release into blood
Catabolic Signals (Degrades Bone)
M-CSF and TNF11 - Activate and Proliferate osteoclasts - Synergistic with RANKL, but it is not inhibited by OPG
Excessive catabolism -> Osteoporosis
Anabolic Signals (Builds bone)
Osteoprotegerin (OPG) - Blocks RANKL and osteoclast activation -> protects bone
TGF β - Stimulates new matrix synthesis and OPG synthesis - Released from bone matrix during remodelling as a feedback mechanism to stimulate re-synthesis after
2. ↑ production from purine metabolism - ↑ cellular turnover during chemo = ↑ purine production (chemo induced gout) - Alcohol ↑ purine catabolism in liver, and urate synthesis
3. ↓ excretion from kidneys - Loop or Thiazide Diuretics ↑ water excretion which ↑ relative concentration of urate in blood - Low dose Aspirin inhibits renal secretion of uric acid (patients with cardiac concerns) - Alcohol ↓ urate secretion in renal tubules - ↓ GFR = ↓ uric acid excretion
Alcohol: - Beer has strongest association > Spirits have moderate association >Wine has no association -> Gout = Wine Drunk Wednesdays
4 Stages of Gout 1. Asymptomatic Hyperuricemia - Common, not clinically significant - >6.8mg/dL starts to precipitate out
2. Acute Gout - Rapid Inflammation (Erythema, edema, heat, pain) starting at night or early morning -> peaks within 24-48 hours) - Spontaneous resolution in 3-14 days - Frequently monoarticular, affecting big toe (first metatarsophalangeal joint) -> Uncommon in Axial joint - In severe attacks skin desquamation may occur over affected joint with pyrexia, chills, malaise Tx: - NSAIDs, Corticosteroids (symptomatic relief) 3. Asymptomatic Inter Critical Period - Sometimes lasts forever Tx:
- Allopurinol (↓ uric acid formation by inhibiting xanthine oxidase) - Probenecid (↑ uric acid excretion in urine)
4. Chronic Tophaceous Gout (TOEphaceous) -> crippling disease - Tophy present in big toe - about 12 years after initial attack - Joints permanently stiff and swollen from chronic inflammation - Bony erosions evident on radiographs (osteoclastic activity) Tophy = deposite of crystaline uric acid
Epidemiology - More prevalent in Males (3.6:1 Male:Female) -> most common inflammatory arthritis in males - Mean Age: 40-60 (later for women) - 35% ↑ risk if 1st degree relative has gout - 50% ↑ in incidence in 2010 vs 1990
**Gout attack can occur before these are diagnosed. The association with gout helps the Dx**
Dental Implications Joint pain impairs oral hygiene -> Helps to tape tennis ball to toothbrush so it’s easier to grab Chair position is important -> Muchos pillows Short Appointments (No electrive treatment during acute attacks) Can Affect TMJ Drug Interactions:
- NSAIDS -> Prolonged bleeding - Corticosteroids -> Immunosuppression (↑ infection risk) - Allopurinol -> Dysguesia, oral paresthesia, altered drug metabolism in liver, oral erythema multiforme, erosion from vomit
Exam Q on this:
Ankylosing Spondylitis = Chronic, Progressive, Painful inflammatory arthritis causing arthritic pain in sacroiliac joints and spine
- Associated with HLA-B27 genetic marker
- No cure!
Back Pain:
- Insidious onset with dull quality radiating to the glutes -> worse in the AM, gets better as you
move
Axial arthritis progresses from sacroiliac joints up the spine until the whole thing is involved
3 results of limited spinal mobility:
1. Flattening of lumbar lordosis
2. Exaggerated thoracic kyphosis
3. Hyperextension of cervical spine
Pathogenesis Occurs at attachment between tendon, ligament, capsule and bone in 3 processes: 1. Inflammation
- Tumor Necrosis Factor (TNF) plays big role 2. Bone Erosion
- Occurs at corners of vertebral bodies early in disease 3. Spur formation
- Syndesmophytes (spurs) appear as tissue is replaced by ossified fibrocartilage -> eventually fuse making spine look like 1 piece (Bamboo spine)
Pathophysiology Mostly unclear - Multiple genes/gene variants are involed - HLA-B27 -> codes MHC molecule presenting Ag to CD8 T cells (Cytotoxic T-cell)
- 90% of patients with AS have this varient, but only 5% of people with the variant have AS Hypothesis:
- Misfolded, dysfunctional, or autoimune against HLA B-27 = Inflammation Trigger:
- Bacteria travel from GI -> Bloodstream -> SI Joints -> Inflammation -> Chronic inflammation -> Pain & Ossification -> Erosion of vertebrae + syndesmophyte formation -> fused vertebrae -> ↓ flexibility and difficulty breathing
Epidemiology 4-8x more common in men - Average starts at 23 years old
Risk Factors: Family Hx
- Ankylosing Spondylitis - IBD (inflammation starts in GI and spreads to spine) - Frequent GI infections
HLA-B27 (encondes MHC I) -> regulates immune system
Clinical Presentation
Pain and Stiffness - Acute pain in SI joint, lumbar vertebrae, costal cartilage, hip joint, and shoulder joint
Fused Vertebrae and ribs - Results in stiffness and difficulty breathing (ribcase can fuse together as well)
Osteopenia/Osteoporosis - ↓ bone density from chronic inflammation -> ↑ risk of compression fractures
- Secondary Osteoporosis - May affect TMJ and Mandible -> ↑ risk of TMJ, trismus and clicking
- Assess cervical bone erosion and ankylosis prior to surgery - Rule out spinal fracture before to avoid lawsuit
- Tipping the head too far back can cause spinal cord compression - Difficulty intubating during general anaesthesia - Kyphosis can make it difficult to get to the dentist = ↓ oral hygiene - Associations with secondary sjogrens (↑ caries and fungal infections) - Need lots of pillows and short appointments for patient comfort - Difficult breathing with rubber dam due to limited chest expansion
- Bacteria live in saliva of deer ticks -> tick falls off infected deer into grass -> jump onto us when we walk through tall grass - Nymph ticks responsible for most infections because they are hard to spot on skin
Pathophysiology (Largely unknown)
Large mammals + rodents = reservoirs for Borrelia burgdorferi -> Tick feeds on blood of reservoir and takes up microbe -> Tick bites human, if stays on for 24-48 hours can transmit bacteria -> Tick saliva disturbs our immune system at bite -> bacteria can multiply in dermis safely -> 3-32 days later invades surrounding skin (erythema migrans bullseye rash) -> Bacteria enters lymphatics (inflammatory adenopathy) and blood (heart, nervous system, skin, joints) = neurologic, cardiac and joint issues
Erythema Migrans Pathagnomic of Lyme disease (found in 75% of patients) -> absence of rash however does not rule out lyme disease
- Bullseye rash, can be up to 30cm in diameter, no pain or itch - Goes away after 1 month (but still have disease)
3 Phases 1. Early Localized (3-32 days post bite) - Erythema migrans appear
2. Early Disseminated - Bacteria spreads to blood and lymphatics - Flu like symptoms, Arthralgia/joint pain (most common presentation of lyme disease) - Cardiac Issues -> Arrhythmia, Myopericarditis - Neurologic Issues -> cranial nerve palsy, meningitis, neurologic pain (1-2 months after initial bite)
3. Late Stage (months – years post bite) - Lyme Arthritis -> inflamed, swollen, painful joints (including TMJ) - Late neurological symptoms -> Encephalopathy, Neurocognitive dysfunction, peripheral neuropathy (↓
sensation, movement, gland function)
Autoimmune disorders linked with HLA-B27
- Ankylosing spondylitis
- Reactive Arthritis
- Rheumatoid Arthritis
- Psoriasis
- Enthesitis Related JIA
- SLE
- MS
- Type 1 DM
- Narcolepsy
- Celiac Disease
DMARDS – Disease-modifying Antirheumatic Drugs:
- Powerful anti-inflammatories
- Used to prevent joint damage (↓ cartilage and bone destruction)
Treatment Antibiotics - Early Lyme -> Doxycycline, Amoxicillin orally 1-2weeks - Early Disseminated -> Cefotaxime IV - Late Lyme -> 2-4 weeks of antibiotics
Dental Implications TMJ Inflammation Dental Neuralgia (Facial palsy resembling Bell’s Palsy) -> Be aware of before delivering LA or might be sued
- Twitching muscles might make Tx challenging
Temporal Arteritis (Giant Cell Arteritis) **Medical Emergency! -> 50% of cases end up going blind**
Subtype of Giant Cell Arteritis -> chronic systemic vasculitis of large/medium arteries - Can lead to ischemia, blindness, stroke, MI - Most common systemic vasculitis >50yrs old - Amaurosis Fugax (transient blindness) = warning sign of permanent vision loss (involvement of ophthalmic artery or posterior ciliary
artery
Pathophysiology T-cell dependent and antigen driven (inflammatory condition) -> TNF and IL-6 have a major role Environmental : –> Seasonal with cyclic patterns with geographic variation Genetic -> TNF, ↑ IL-6 (proinflammatory), IFδ, ↓ IL-10 (anti-Inflammatory), Vascular endothelial growth factor
1. Exposure to exogenous antigen 2. T-cells recruited to vessel wall -> release cytokines to act upon macrophages 3. Matrix Metalloproteinases (MMP) degrade collagen in the vessel walls allowing access to macrophages at the basement
membrane 4. In the Adventitia (outer layer), macrophages release cytokine IL-6 to ↑ inflammatory response. 5. In the Media (middle layer), macrophages produce free radicals and MMP’s to degrade the arterial wall and break down
elastic lamina (Inner most layer) 6. Migrating fibroblasts add more ECM to the intima which thickens the vessel walls -> narrows the lumen = ischemia and ↑ prevalence of cranial pain, blindness, TIA and stokes.
Clinical Presentation - New-onset unilateral headache -> noticed which brushing hair, head on pillow or wearing hat -> If not treated has serious implications - Pain in muscles of mastication on chewing - Intermittent claudication of jaw and tongue - Visual Disturbance - ↑ erythrocyte sedimentation rate (inflammation = sticky RBC, sediment together) - ↑ C-reactive protein
Treatment Early initiation of high-dose corticosteroid therapy for 2-4 weeks until reversible signs are gone - Adding DMARDS (Methotrexate) to corticosteroids ↓ relapse rate
Pt’s treated for 1-2 years
Juvenile Idiopathic Arteritis (JIA) = Chronic arthritides involving 1+ joint for at least 6 weeks in patient < 16 years old
- Influenced by Genetic and environmental factors
*Systemic JIA = autoinflammatory condition, all other
types are autoimmune**
Epidemiology - Ages 6 months – 16 years (no primary age). Issues for 6 weeks+ - Boys and girls equally affected - More common if European ancestry
Laboratory Tests No Dx tests - Do CBC -> check Rheumatoid Factor (RF), Cyclic Citrullinated Peptide Ab (CCP), Antinuclear Ab (ANA),
Erythrocyte sedimentation Rate (ESR), and C-reactive protein (CRP) Eliminate other causes of arthritis
Treatment - No cure, but with aggressive Tx and early Dx remission is possible Non-Pharma: Physical and occupational therapy + collaboration among healthcare team = best results Pharma: DMARDS (methotrexate, leflunomide, sulfasalazine) Biologics -> cytokine inhibitors are 1st line therapy
Systemic Corticosteroids -> should be limited to allow regular growth of kid Injected Corticosteroids -> Selected joints to relieve inflammation NSAIDs
Dental Implications TMJ - 25-43% of JIA’s have TMJ issues - Pain on palpation - Trismus - Mandible deviation when opening - Ankylosis of joint - Facial asymmetry
Other issues: - Prolonged morning stiffness -> book late morning appointments - Avoid neck hyperextension in case C1-C2 subluxation and spinal compression
Autoinflammatory Autoimmune
Problems in innate immune system Characterized by neutrophils, macrophages, and NK cells releasing cytokines
Problems in adaptive immune system B & T cells lose ability to differentiate self from non-self
7 Types of JIA -> Focus on the main differences between them, not the little details
Systemic JIA (Still’s Disease if in
adults)
Autoinflammatory disease (the rest are autoimmune), arthritis in 1+ joints preceded by daily high-grade fever associated with at least one of:
Inflammatory synovitis -> leads to pannus formation w/ cartilage and bone erosions
- Abnormal thickening of synovial tissue (membrane of granulation tissue w/ mesenchyme + bone marrow derived cells)
- Synovium migrates along articular cartilage, eroding it as it goes - Stimulates release of IL-1, IL-6, and TNF, prostaglandins, Substance P by macrophages = destruction +
erosion of cartilage and bone Abnormal cytokine levels (↑ TNF, ↑ IL-6)
Oligoarticular JIA -Most common form
Arthritis in <4 joints in 1st 6 months of disease 2 subtypes:
1. Persistent -> <4 joints throughout disease 2. Extended -> <4 joints for 6 months then > 4 joints after 6 months
↑ risk of uveitis (eye inflammation) vs other subtypes - Positive test for antinuclear antibody (ANA) = risk of uveitis and blindness
Polyarticular JIA (Rheumatoid Factor –‘ve)
Arthritis in >5 joints AND negative for RF - Found typically in weight bearing joints and TMJ
Polyarticular JIA (Rheumatoid Factor +’ve)
Arthritis in >5 joints AND positive for RF - Anti-cyclic citrullinated (CCP) antibodies may also be present - Most similar to adult rheumatoid arthritis = ↑ risk of progression
More severe than RF –‘ve
Psoriatic JIA Psoriasis AND Arthritis, OR arthritis and 2+ of: - Dactylitis (inflammation of fingers/toes) - Nail pitting - Onycholysis (separation of fingernail from nail bed) - Psoriasis in a 1st degree relative (Erythematous plaques covered by silvery scales)
Enthesitis-Related JIA Arthritis or enthesitis AND 2+: - Sacroiliac tenderness - Acute anterior uveitis - HLA-B27 +’ve - 1st degree relative with HLA-B27 related disease - Male and >6 yrs
Tenderness (enthesitis) where bone beets a tendon, ligament or CT -> typically hips, knees, feet
Undifferentiated Arthritis
Fulfills criteria of 2+ of the other 6 categories, or none of them
Systemic Lupus Erythematous (SLE) 2 Types of Lupus -> Systemic and Discoid
Systemic more serious and affects more organs:
- Skin (Discoid only affects skin)
- Joints
- CNS
- Kidneys (causes highest mortality)
- Lung
- Heart
- GI
- Hematologic System
= Multisystem, autoimmune disorder of the connective tissue Characterised by:
- Antinuclear antibodies (autoantibodies targeting nuclear ag) - Remissions and flares - Variable presentation, disease course and prognosis
Pathophysiology Not completely understood (classic) Thought to be genetically determined immune issue triggered by environmental factors:
Strongest genetic risk = deficiency in Complement protein (C1q deficiency)
Auto-immune antibodies form pro-inflammatory immune complexes that deposit onto tissues - Complexes clog up kidneys = kidney failure = death - Immune cells and Complement recruited to complexes and damage tissues
Main immune pathways affected 1. ↓ clearance of nucleic acid-containing debris and immune complexes (ANA antibodies) 2. ↑ innate immune activation 3. Abnormal T and B cell activation
Clinical Presentation Renal - Main cause of mortality (60% of people afflicted renally) - Range from asymptomatic proteinuria -> glomerulonephritis -> renal failure - Renal status is prognostic indicator
Musculoskeletal - 1st symptom of SLE is arthralgia in 50% of patients with SLE - Non-erosive arthritis of hands, wrists, and knees, TMJ involved in 67% cases - Corticosteroid therapy can cause avascular bony necrosis
Gastrointestinal - Abdominal pain, nausea and vomiting
Skin - Butterfly rash across face/bridge of nose (worse when in sunlight), upper truck and/or exposed skin - Raynaud Syndrome -> vasospasm causing ↓ blood flow to extremities
Risk Factors - ↑ in Women vs men (especially 15-45 child bearing years) - ↓ Complement proteins = biggest genetic risk factor -> Family Hx has a role - Current smoking (not Hx of smoking though)
Medications - Oral contraceptives and Hormone replacement therapy
Oral Manifestations Oral Lesions -> ulcerations or mucosal inflammation - Transient, waxes and wanes - Resemble lichen planus, leukoplakia, candidiasis, Erythroplakia - Ulcerated lesions are hard to distinguish from common aphthous ulcer - Discoid Lupus lesion has white striae
Xerostomia (from meds and secondary sjogrens) Dysgeusia Glossodynia TMJ issues
Dental Implications Medications can cause immunosuppression and eventually adrenal insufficiency Antimalarials can cause lichenoid like reactions or oral hyperpigmentation If have renal failure
- May be on blood thinners, have an AV fistula, or may be taking cyclosporine (gingival hyperplasia)
Marfan Syndrome = connective tissue disease
- Autosomal Dominant mutation of FBN1 gene (encodes fibrillin = structural weakness of CT) - Fibrillin-1 = glycoprotein in microfibrils essential for elastic fiber formation in CT potential issues with heart and aortic aneurysm/dissection
- Fibrillin -1 also involved in TGF-β signalling and is found in ciliary zones, aorta, and ligaments (Skeleton, Eyes, CV system affected)
Presentation Tall, thin stature -> long limbs (arm span exceeds height, legs longer than torso) Disproportionally long fingers Inward or outward displacement of sternum Joint hypermobility Diaphragmatic and inguinal hernias Kyphoscoliosis (anterior and lateral curved spine) Facial/Oral features
- Long thin face (dolichocephaly) - Downward sloping palpebral features - Malar hypoplasia - Strabismus - Retrognathia - High, narrow palate (crowding, posterior cross-bite, malocclusion, TMD)
Quick Test:
- Thumb overlaps pinky finger when held around wrist - Can see thumb nail when closed in a fist
Treatment Early diagnosis can save lives -> Notice oral facial features! Restrict high intensity activity (or risk aortic dissection or aneurysm)
Dental Implications ↑ TMD -> painful mastication, headache, clicking, trismus May need orthodontic treatment for crowded jaw, posterior crossbite and disproportionate arches
- Kids should see ortho at 7 years old
Reactive Arthritis Aseptic arthritis triggered by infectious agent outside the joint -> Asymmetric polyarthritis, mostly in lower extremities
- Begins 1-5 weeks after genitourinary or GI infection Unknown if autoimmune or a response to infection
Presentation Axial inflammation and damage Peripheral arthritis Enthesopathy Extra-articular issues:
- IBD - Psoriasis - Uveitis -> can progress to blindness - Urethritis - Cervicitis - Dysentery
Etiology 20-40 years old - More men than women following UTI, but equally Men:Women following GI
Pathophysiology Triggered by GI or UTI infection spreading to joints - Strong association with HLA-B27
Self-limited and spontaneously resolves w/o Tx after 3-12 months Defined by a triad of: Arthritis, Nongonococcal urethritis or cervicitis, and conjunctivitis
2. Infection disseminates to synovial joints 3. Viable bacteria or bacterial antigens in the joints 4. Host Immune reaction -> Can lead to bacterial elimination, bacterial persistence (tolerated) or autoimmune synovitis (leading to arthritis) 5. Aberrant immune response or persistent microbial infection leads to prolonged inflammation
Treatment NSAIDs for acute phase -> indomethacin (25-50 PO tid) Corticosteroids if inflammation severe DMARDS -> pt’s where NSAIDs are insufficient -> methotrexate infliximab NO Antibiotics, ↑ risk of GI adverse effects -> the bacteria arnt in the joints, so won’t help the arthritis
Sjogren Syndrome
Salivary Gland and Saliva Review Salivary glands are organized like grapes with a functional acinar unit at the bottom, can be 1 type of acinus or a mix of
both types
Acinar units can be of 2 types:
1. Serous -> flowable and liquidy
2. Mucinous -> Thicker and viscous
Saliva
Function Lubricate Aid in Swallowing Digestion Antimicrobial Buffering against acid Tooth remineralization Mediation of taste
Volume 600-1500mL/day - 5% during sleep (0.1mL/min) - 80-90% response to stimuli (4-5mL/min) -> Parotid and Submandibular produce same amount when stim. - Resting (0.3mL/min) -> Submandibular produces most at rest
Control Parasympathetic Stimulation -> High levels of watery Serous flow Sympathetic Stimulation -> Low flow of mucinous protein rich flow Masticatory Salivary Reflex -> Mechanical receptors in periodontal ligament and in masticatory muscle fibers Gustatory Salivary Reflex -> Taste bud activated chemoreceptors, use CN VII, IX and X to bring signal to Medulla Oblongata
Aging Salivary function DOES NOT naturally ↓ with age - ↑ number of drugs taken with ↑ age though can contribute to ↓ salivary flow (usually will find this if on 5+ drugs)
Sjogrens Syndrome Epidemiology Slowly progressive autoimmune disease with wide range of organ specific and systemic manifestations
9:1 Female:Male ratio -> WAY more in females (as it is with most autoimmune issues) Onset: 40-50yrs old ↑ Malignancy Risk
Etiology Primary: No other connective Tissue Disorder Secondary: Secondary to accompanying autoimmune disorder
Pathophysiology Affects Lacrimal Glands and mucosal exocrine glands of respiratory and GI tracts - Salivary glands = main targets -> they are a local source of autoantigens and signal for lymphocyte organization
1. Salivary gland epithelial cells secrete cytokines to activate T-cells 2. CD4 T cells and dendritic cells infiltrate -> Produce Type 1 IFN 3. ↑ in B cells occurs during course of the disease, and correlates to onset
of systemic manifestations 4. Immune complexes form and stimulate further inflammation (loops) 5. Over time 20% of patients developt germinal centers within the
lymphocytic foci located around the parotid gland (germinal centers associated with B-cell Lymphoma development)
Major Salivary Glands
Parotid -> mostly Serous (helps swallowing and lubricating food) Submandibular -> Most important! Mixed Mucinous and Serous Saliva
- Important for taste, protection, lubrication, remineralizing teeth Sublingual -> Mostly mucinous, no major roles
Minor Salivary Glands
More radioresistant than major glands -> ↑ change of surviving during radiotherapy
**Periodontitis NOT associated w/ hyposalivation, because it’s not directly associated with bacteria. It’s an immune reaction Musculoskeletal
- Intermittent polyarticular arthropathy of small joints - 53% get arthralgia - 23% get myalgia
Dermatological - Dry Skin - Some with mild Reynaud Syndrome - Vasculitis - Palpable purpura
Pulmonary, GI, Renal involvement usually rare Neurologic
- Sensory neuropathy - CNS rarely involved
Hematologic
- 44x ↑ risk of lymphoma -> Especially around parotid gland, and B-cells (low grade and mostly curable
Clinical Predictors of lymphoma - Persistent parotid enlargement - Splenomegaly - Lymphadenopathy - Palpable Purpura - Leg Ulcers
Diagnosis Ocular Tests - Schirmer Test -> Stick some filters under eyelids, if after 5 mins <5mm of wetting = Sjrogens - Rose Bengal Scoring -> Rose Bengal solution stains eyes for something - Slit Lamp exam -> detects destroyed conjunctiva
Salivary Tests - Sialometry -> is <1.5mL in 15 mins = Sjorgrens - Minor salivary gland biopsy -> 1.2-2cm incision middle of the lower lip. Looking for foci of 50
- Auto-antibodies precede clinical disease, but prophylactic Tx doesn’t prevent development. Its inevitable
Consensus DX Dry Eyes -> Symptoms, and Test confirmed Dry Mouth -> Symptoms and test confirmed Minor salivary gland biopsy Autoantibodies -> SS-A and SS-B
- Parasympathetic agent (muscarinic agonist) - Can cause GI upset, sweating, bradycardia, ↑ pulmonary secretions, ↑ smooth muscle tone, Blurred vision - Tabs not covered under insurance…but eye drops are. Can Px the drops and get them to mix with water!
- Cevimeline (30mg, tid) - Specific paraympathetic agent (muscarinic agonist that doesn’t act on heart or lungs)
Dry Eyes - Artificial Tears - Pilocarpine (↑ production of tears) - Punctal plugs (↓ removal of tears)
Bone Pain Muscle Weakness Waddling Gait ↓ bone mass detectable on x-ray and bone densitometry Pseudo-fracture -> Clinical Hallmark
Pathogenesis Early Stage: - ↓ Ca++ absorption causes secondary hyperparathyroidism -> prevents hypocalcaemia but ↑ renal phosphate excretion = hypophosphataemia
Late Stage: - Hypocalcaemia + Hypophosphataemia
Osteomalacia vs Osteoporosis Osteomalacia Osteoporosis
↓ ratio of mineral to matrix (too much matrix relative to bone), but normal bone mass
- Affects Quality of the bone Clinical Features:
- Soft bones, bow legs
↓ bone mass and normal mineral to matrix ratio “normal bone, but not enough of it”
- Affects the Quantity of bone Clinical Features:
- Fractures from minimal trauma
Bone Grafting and Implants
Implants Osseointegration = formation of direct interface btwn implant and bone without intervening soft tissue
Screw threads on implants are more to ↑ surface area for better osseointegration
Material: Titanium - High biocompatibility - Good Resistance to Corrosion - No toxicity to macrophages or fibroblasts - No inflammatory response - Oxide layer of titanium allows it to repair itself by reoxidizing when damaged
-> That’s some Wolverine shit… (except Adamantium)
Implant Properties
Mechanical - Wear related to strength and surface roughness - Must be strong -> ion implantation minimizes wear
Topographical - Degree of roughness is related to surface and orientation of surface irregularities - Chemical composition of implant interface on surface affects initial cell attachment
Definition Graft material acts as scaffold for new bone growth
Stimulation of osteoprogenitors to differentiate into osteoblasts and make new bone Bone Morphogenic Proteins = most studied osteoinducer Can have a material be both conductive and indictive
↑ osteoinduction without having osteoinductive properties itself
Vital osteoblasts from bone graft contribute to new bone growth
Medication-Related Osteonecrosis of the Jaw (MRONJ) Definition Adverse drug reaction consisting of progressive bone destruction (of jaw) in patients under current or previous
treatment with antiresorptive and antiangiogenic meds - Very challenging to treat
Diagnosis if ALL are present:
1. Current or previous Tx with antiresorptive or antiangiogenic agents 2. Exposed bone, or bone probable through intra/extraoral sinus/fistula for > 8weeks
- Sinus = internal to external surface communication - Fistula = 2 outside surfaces communicating
3. No Hx of radiation therapy to jaws or obvious metastasis to the jaw (Osteoradionecrosis of jaw is different)
Avascular Necrosis
= Death of bone tissue due to lack of blood supply (aka osteonecrosis) -> leads to tiny breaks in bone until it eventually collapses
- Blow flow can be interrupted from bone fracture or dislocation
Phossy Jaw -> Historical, not really a thing anymore
= Chronic exposure of phosphorus vapour = phosphorous deposition in the jaw -
> Bone dies, painful toothache and gum swelling
- Jaws rot away and glow green in the dark (not sure if the glow in the
dark jaws is Matthews fucking with us…but just in case)
Management: Excision of affected jaw, otherwise death
MRONJ Staging Treatment
At Risk - No apparent necrotic bone
No tx Patient Education
Stage 0 - No clinical evidence of necrotic bone, but non-
specific clinical findings exist, radiographic changes & symptoms
Systemic management: Pain meds and antibiotics
Stage 1 - Exposed necrotic bone or fistulae that probes
to bone - Asymptomatic and no infection
Antibacterial rinses (Chlorhexidine) Quarterly clinical follow ups Patient education Review indications for continued bisphosphonate use
Stage 2 - Exposed necrotic bone or fistulae that probes
to bone - Infection evidenced by pain and erythema in
region of exposed bone - W or W/O purulent drainage
Symptomatic Tx with antibiotics + Mouth rinses Pain Control Debridement to relieve soft tissue irritation Infection control
Stage 3 - Exposed necrotic bone or fistulae that probes
to bone - Infection evidenced by pain and erythema in
region of exposed bone and one of the following:
- Necrotic bone beyond alveolar bone resulting in pathologic fracture
- Extra-oral fistula - Oral nasal communication - Osteolysis extending to inferior border of
mandible or sinus floor
Mouth Rinses and antibiotic therapy Pain control Surgical debridement/resection for long term palliation of infection and pain
Musculoskeletal Pharmacology
Muscle Relaxants
1. Choline + Acetyl CoA = Acetylcholine
2. Action Potential stimulates Ach containing vesicles to release
contents into synapse.
3. 2 Ach molecules bind muscarinic receptor to cause conformational
change
-> Allows Na+ to flow in and depolarize muscle cell
4. Depolarization of the muscle cell propagates AP and stimulates
contraction pathway
Neuromuscular Blocker - Produce paralysis by being structurally similar to acetylcholine
2 Types:
1. Depolarizing Blockers
2. Non-depolarizing Blockers
Depolarizing Blocker
Drug Succinylcholine (only clinically useful one)
MOA Agonist at nicotinic acetylcholine receptors -> Open channel, enzymes have issues breaking it down -> Prolonged Depol. Phase I Block (depolarizing):
- Succinylcholine binds to nic. Receptor to open ion channel -> Na enters cell -> transient muscle contraction (twitching)
- Not metabolized well @ synapse -> prolonged depolarization -> unresponsive to nerve impulses = flaccid paralysis - Cholinesterase inhibitors prolongs depol. even longer
Phase II Block (Desensitizing): - After prolonged succinylcholine exposure, depol ↓ and membrane can repolarize - Subsequent depol is hard to achieve -> has become desensitized (possibly refractory period)
Clinical Uses Surgery (relaxes muscles to make suturing easier) Tetanus Electroconvulsive therapy -> drug prevents spasm Laryngospam
Adverse Effects
Arrythmias Hyperkalemia Transient ↑ in intra-abdominal and intraocular pressure Post-op myalgia Malignant Hyperthermia
Special Considerations
Has NO anaesthetic or analgesic effects - Make SURE anesthetic is working before using -> Won’t be able to see pain reflex twitching if anesthetic isn’t
working
Malignant Hyperthermia
Potential side effect when undergoing general anesthesia, can occur from Succinylcholine. - From genetic disorder of skeletal muscle
Many mutations associated: - RyR1 (Skeletal muscle ryanodine receptor) -> calcium release channel in Sarcoplasmic Reticulum - Mutated a1 subunit of skeletal muscle L-type voltage-dependent Ca channel
↑ free cytosolic calcium concentration w/I skeletal muscle cells = Severe muscle contraction and ↑ Body temp
Treatment Dantrolene -> ↓ Ca release from sarcoplasmic reticulum -> via RyR1 receptor Control body temperature Restore electrolyte and acid-base balance
Dental Use ↓ Facial pain from muscle spasms associated with TMD Treatment of Trismus Muscle relaxation in General anesthesia
Adverse Effects Don’t give to elderly - Acts within the CNS -> can cause ataxia (↓ muscle coordination) = falling -> Thrombus -> Stroke -> Death
Non-depolarizing Blockers
Drug (-curonium)
Pancuronium Rocuronium Vecuronium d-tubocurarine
MOA Reversible competitive inhibitor of Nicotinic acetylcholine receptor - Experiences co-operative binding: ↑ concentration = more bind = more blocking - 2 Ach binding sites on the Ach Receptor
Effects Prevents depolarization by Ach - Causes flaccid paralysis
Clinical Application
Prolonged muscle relaxation for surgical procedures Relaxation of respiratory muscles to facilitate intubation and mechanical ventilation
Spasmolytics Spasticity = disordered sensorimotor control from upper motor neuron lesion
- Presents as intermittent or sustained involuntary activation of muscles - Causes stiffness or tightness of the muscles and can interfere with normal movement, speech and gait
Pathophysiology Stretch reflex arc involved - Upper motor neuron lesion causes damage to the descending pathway in
spinal cord (inhibitory/Excitatory interneuron) - Hyperexcitability of the α-motor neurons in the spinal cord
= ↑ in tonic stretch reflexes and flexor muscle spasm + Muscle weakness
Pharmacological Treatment Goal
↓ spinal “polysynapse” arc
Dental Uses Relieve Anxiety Treat post-procedure trismus Treat muscle spasms of head and neck
Spinal Cord Reflex Arc GABA Receptors in Spinal Cord
Regulates speed and extent of muscle stretch Sensory muscle spindle fiber fires and sends signal through Ia Sensory neurons
- Signal transferred through gamma and alpha motor neurons
- Gamma transmits back to muscle spindle to moderate sensitivity to stretching
- Alpha transmits to striated muscle fiber to contract
This is what happens when the doc bangs your tendon with the little hammer and you kick up
1. Signal (pain) sensed with sensory receptor 2. Signal sent through afferent neuron to
integration center in spinal chord 3. Afferent synapses on Interneuron which
transmits signal through Efferent motor neuron to muscle (bicep for example) to cause contraction (pulling hand up off burner)
4. Interneuron also synapses on inhibitory neuron which sends signal through motor efferent to other muscles to cause relaxation (allowing recoil, tricep for example)
5. Interneuron also synapses on efferents sent to the brain so you can remember to not burn your hand off ** Inhibitory Interneurons release GABA to regulate the muscle contraction from the Efferent
Some good instruction
https://www.youtube.com/watch?v=6noV8AHcM6E
GABAergic Agents -> Acts on Efferent Neuron
Benzodiazepine (Diazepam, Midazolam, Lorazepam)
MOA GABAA Agonist
(Ligand gated Cl channel) - Binds to allosteric site on GABAA ↑ ability of GABA ligand to bind and cause change in shape - Cl- flows in causing hyperpolarization with its –‘ve charge - ↓ response to action potential
Effect Potentiates neural inhibition mediated by GABA -> still need GABA to bind and cause effect though
Baclofen
MOA GABAB Agonist (G-protein coupled linked to K channels)
- Binds GABAB causes signal to open up K+ channels
- K+ flows out of the cell causing hyperpolarization - ↓ response to action potential
Results in Hyperpolarization by: 1. Closure of pre-synaptic Ca channels 2. ↑ post synaptic K conductance 3. ↓ dendritic Ca++ influx **Causes a ↓ in excitatory transmitter release**
Effect Suppression of la sensory afferents, spinal interneurons, motor neurons
Common Uses Alleviating spasticity of MS and spinal cord injury Treatment for trigeminal neuralgia
Drug Interactions ↑ Effect of Baclofen - Benzodiazepines - Antihypertensives - Opioid analgesics
↓ Effects of Baclofen - Lithium
Considerations May ↑ seizures in epileptic patients -> slowly taper off drug Use cautiously in renal impaired patients Can cause drowsiness, ataxia, and confusion -> caution with elderly Sudden withdrawal associated with hallucination and tachycardia
Tizanidine -> Acts on Afferent Neuron
MOA Adrenergic α2 agonist (mechanism unknown)
Effects Reinforces pre- and post-synaptic inhibition within spinal cord to ↓ spasticity - Inhibits nociceptive transmission in spinal dorsal horn (↓ release of Ach and Norepinephrine)
-> Pain reflex (recoil after putting your hand on hot thing)
Uses Treatment of myofascial pain in head and neck
Dental consideration Additive effects when used with other CNS depressants Oral contraceptives -> ↓ tizanidine clearance by 50% (↑ duration of effects) ↑ levels of antihypertensive drugs DON’T USE with other Adrenergic α2 agonist
Other Centrally Acting Anti-Spasmolytics
Dantrolene
MOA Acts on skeletal muscle by ↓ Ca released from the SR (blocks RyR1 ryanodine receptor) - Doesn’t act in the CNS (unlike the others mentioned above)
Clinical uses Treats malignant hyperthermia Treats spasm from cerebral palsy, spinal cord injury and MS
Cyclobenzaprine (Flexeril)
MOA Unknown (thought to act in the brainstem) - Structurally related to tricyclic antidepressants -> produces anti-muscarinic effects
Dental Use Treats muscle spasm associated with TMJ pain
Adverse Effects Drowsiness and malaise, Tachycardia/dysrhythmia ↑ effects of alcohol, barbituates and CNS depressants
Contraindications DO NOT TAKE with - Monoamine oxidase inhibitors, - Hyperthyroidism - CHF - Recent MI - Dysrhythmias
Musculoskeletal Toxins Botulinum Toxin - Botox
The heck is it? Neurotoxin from Clostridium botulinum
MOA Cleaves fusion proteins in nerve endings - Prevents Ach release by interfering with vesicle fusion - No Ach = no contraction
Effects Flaccid paralysis
Clinical use Treatment of spams from cerebral palsy, MS, overactive bladder, migraine
- Cytotoxic folate antagonist (cancer tx) with immunosuppressant action. Inhibits Dihydrofolate Reductase in the production of folate during DNA repair or replication
- Associated with bone marrow suppression Sulfazaline
- Unknown MOA, thought to scavenge Toxic oxygen metabolites from neutrophils
- Bacterial in colon aid in activation through metabolism - Used in IBD and RA
Penicillamine - Hydrolysed penicillin - MOA unknown, thought to ↓ immune response and IL-1 production - Prevents maturation of collagen
-> disrupts cytoskeletal function by inhibiting β-tubulin polymerization into microtubules = prevents activation and migration of neutrophils Side Effects: GI hemorrhage, kidney damage, bone marrow depression, peripheral neuropathy
Prophylaxis Management Allopurinol
- Competitive inhibitor of xanthine oxidase (enzyme involved in production of uric acid) Side Effects: - GI disturbance, Stevens-Johnson syndrome
Febuxostat - Similar to Allopurinol
Probenecid and Sulfinpryazone - Uricosuric agents -> ↑ renal excretion of uric acid by inhibiting its reabsorption - Must drink ↑ water - Less effective and more toxic than allopurinol (only for patients who can’t handle allo)
Pegloticase and Rasburicase - Recombinant urate-oxidase enzyme -> converts uric acid to allantoin = non-reactive metabolite - Allantoin excreted more readily
Treatment Non-Pharma - Genetic counseling - Surgery - Physical aids - Family support - Dietary advice
Pharma For spasity
- Baclofen For Cramps
- Phenytoin Idiopathic Inflammatory
- Glucocorticoid - DMARDs - Biologics
Osteoporosis Bone disorder characterized by:
- ↓ density
- Impaired bone architecture
- Compromised bone strength predisposing to fragility fractures
Pathophysiology = Bone resorption > Bone formation
- Starts at 35 years old
- Estrogen deficiency during menopause ↑ osteoclast activity -> accelerates OP 10 fold
- Age related OP comes from ↓ Ca, ↓ Vit. D. -> ↓ Osteoblast
Tx:
Non-Pharma Pharma
- ↑ Ca and Vitamin D - Limit alcohol to 1 drink/ day women, and 2/day men - Limit Caffeine - Stop Smoking - ↑ weight bearing aerobic and strengthening activities
Medication Related ONJ (Osteonecrosis of the Jaw from Bisphosphonates/meds)
Drugs of Concern IV or Oral bisphosphonates Denosumab (biologic) – RANKL inhibitor
Pathophysiology Inhibits Osteoclastic remodeling of bone (healing bone from surgery or damage) -> ↓ clearance of damage and infection - Mandible affected the most -> ↓ blood in cortical bone so it’s harder to heal
Risk Factors - Many variables makes it hard to
predict
Concomitant use with corticosteroids, or chemo Dental extraction, trauma or infection Being female Clotting disorders Arthritis Alcohol abuse Smoking Malnutrition Bony exostosis Periodontal disease
May have MRONJ if ALL are present:
1. Current or previous tx w/ antiresorptive or antiangiogenic agents 2. Exposed bone, or probable bone through intra or extra oral fistulae for 8+ weeks 3. No Hx of radiation therapy to jaws or obvious metastatic disease in jaw
Avoiding MRONJ Avoid elective Tx that will require bone healing Provide routine clinical dental exams Perform invasive procedures PRIOR to bisphosphonate therapy begins Perform dental prophylaxis, caries control and stabilize restorative care Oral hygiene education is very important NO ANTIBIOTIC PROPHYLAXIS NEEDED
Management Consult with oral surgeon Minimal bony debridement -> reduce sharp edges to ↓ trauma on tissues Removable appliance to protect exposed bone
AAOMA Recommendations
Exposure to oral Bisphosphonates Recommendation
< 4 years, No clinical risk factors No alteration or delay in surgery needed
< 4 years, taken with corticosteroids or antiangiogenic meds Consider drug holiday for 2 months prior to surgery -> Physician has to make the call, consult
> 4 years, w/ or w/o other meds Consider drug holiday for 2 months prior to surgery -> Physician has to make the call, consult
- Anti-resorptive drugs should not be restarted until osseous healing occurred
Staging Treatment
At Risk - No apparent necrotic bone
No tx Patient Education
Stage 0 - No clinical evidence of necrotic bone, but non-specific clinical
findings exist, radiographic changes & symptoms
Systemic management: Pain meds and antibiotics
Stage 1 - Exposed necrotic bone or fistulae that probes to bone - Asymptomatic and no infection
Antibacterial rinses (Chlorhexidine) Quarterly clinical follow ups Patient education Review indications for continued bisphosphonate use
Stage 2 - Exposed necrotic bone or fistulae that probes to bone - Infection evidenced by pain and erythema in region of exposed
bone - W or W/O purulent drainage
Symptomatic Tx with antibiotics + Mouth rinses Pain Control Debridement to relieve soft tissue irritation Infection control
Stage 3 - Exposed necrotic bone or fistulae that probes to bone - Infection evidenced by pain and erythema in region of exposed
bone and one of the following: - Necrotic bone beyond alveolar bone resulting in pathologic
fracture - Extra-oral fistula - Oral nasal communication - Osteolysis extending to inferior border of mandible or sinus
floor
Mouth Rinses and antibiotic therapy Pain control Surgical debridement/resection for long term palliation of infection and pain
PBL 1 – Anna Wright
Physiologic Changes during Pregnancy System Change In Short
Cardiovascular - ↑ Blood volume to meet both maternal and fetal demands - Enlarged cardiac chambers & myocardial hypertrophy
- ↑ HR and Stroke Volume = ↑ Cardiac output (by up to 50%) - ↓ BP in 2nd and 3rd trimester
Dental Implication: - Hypotension may occur when patient is supine -> fetus compresses inferior vena cava and aorta
-> Left Lateral Decubitus position - ↑ Distribution Volume = ↑ dose of hydrophilic drugs to reach therapeutic concentrations - ↓ serum albumin = Other drugs may have to ↓ dosage b/c ↑ free drug concentrations
Eclampsia: - Only occurs during pregnancy and causes seizures late in pregnancy - Follows pre-eclampsia ↑ BP (can ↓ oxygenated blood to fetus)
↑ CO ↑ SV ↑HR ↓ BP
Respiratory - Diaphragm moves 3-4cm upwards (make space for fetus) - ↑ O2 consumption by 15%-20% - Progesterone stimulates ventilation by ↑ sensitivity to CO2 in respiratory center
- ↑ tidal volume to eliminate CO2 = ↑ minute volume - Nasal breathing may become difficult = mouth breathing = ↑ xerostomia
Renal - ↑ renal blood flow and glomerular filtration rate by 50-60% - ↑ creatinine clearance up to 50% - ↑ RAAS system = ↑ aldosterone
↑ Renal Blood flow ↑ GFR ↑ Creatinine clearance
Oral Lesions Associated with Pregnancy
Description Image
Aphthous Stomatitis (canker sore)
- Mostly during 3rd trimester -> exacerbation after delivery - Occurrence during menstruation suggests hormonal cause - Worsens when smoking is stopped (worth it doeeee)
Pyogenic granuloma - Red nodular overgrowth of granulation tissue - Typically, on gingivae, lips, tongue, buccal mucosa, palate,
vestibule - Most common is interdental papilla -> can cause diastema - Bleeds A LOT when cut out
Plaque -induced gingivitis
- ↑ by pregnancy and puberty
Morning Sickness Vs. Oral Heath - ↑ Vomiting, gagging, overheating
o Encourage to drink electrolyte rich fluids
o Provide fluoride treatment (varnish)
- Edema of the nose, oral cavity and larynx during pregnancy
o May lead to congestion resulting in mouth breathing -> Xerostomia
Fetal Risk with Drugs Drug Category
Description
A No risk at all in any trimester
B No risk to the fetus in any trimester
C Potential risk to fetus, but benefit of drug may outweigh risk
D Positive evidence of fetal risk, but benefit of drug may outweigh risk
X Definite evidence of fetal abnormalities, drug DOESN’T outweigh risk
N Unclassified drug
Dental Considerations Procedure Recommendation
Radiographs THEY ARE FINE (with usual precautious: lead shield, thyroid guard etc) - We don’t take radiographs low enough to be cause for concern - Most concerned in 1st trimester, but again our dose and location don’t pose risk - ALARA principle is the gospel!
Local Anesthetic ALSO FINE (unless other contraindications with the patient exist of course)
IV Sedation Benzodiazepines - Px for: Anxiety, insomnia, seizures, muscle spasms, alcohol withdrawal etc - Category D drug -> Avoid during pregnancy
- Implicated in cleft lip and palate
Nitrous Oxide - Used for conscious sedation - ↓ Folate production -> Vital for DNA production in fetus - AVOID during 1st trimester (Safe in 2nd and 3rd trimester though)
General Anaesthesia - Can cross placental circulation - AVOID near time of delivery -> impairs infant’s breathing
Analgesics for the Pregnant
Drug FDA Class Recommendations
Aspirin C Short Duration use Avoid in 1st and 3rd trimester and if breastfeeding
Acetaminophen (Tylenol)
B Choice analgesic!
Ibuprofen B/D Short Duration use (no longer than 48-72hrs) Avoid in 1st and 3rd trimester Ok with breastfeeding Category D in 3rd trimester
Naproxen B Short Duration use (no longer than 48-72hrs) Avoid in 1st and 3rd trimester Ok with breastfeeding
Codeine C Ok with breastfeeding In high maternal doses can cause infant drowsiness and depression
Morphine B/D Category D with prolonged use In high maternal doses can cause infant drowsiness and depression
Meperidine B/D Ok with breastfeeding Category D with prolonged use
Percocet C Opioids may cause physical dependence in neonates Respiratory depression may occur in newborn if opioids used prior to delivery
PBL 2 – Sigma Chi-Guy
Bruxism = involuntary habitual grinding of teeth.
2 circadian manifestations:
Sleep Bruxism Awake Bruxism
- More common than awake - 5-8% in adults, 10-20% in children, 3% in elderly - In children develops during “teething” when first teeth erupt
Risk Factors:
- Smoking - Caffeine - Illicit Drugs (cocaine or other stimulants) - Anxiety
Clinical Features based on self-report, partner report, clinical observation
- Possibly from emotions: Anxiety, Stress, Anger, Frustration
- Coping strategy or habit during deep concentration
Underlying Issues
Issue Description
Stress Sometimes not even consciously done or recognized. Making them aware can often help during awake bruxism (STAY WOKE)
Anxiety 70% of cases associated with stress or anxiety (affects people during sleep)
Sleep Disorders Obstructive Sleep Apnea = ↑ risk of grinding
Drug Induced Linked to Selective Serotonin Reuptake Inhibitor (SSRI) use -> Anti-anxiety/depression
Lifestyle Drinking and smoking ↑ risk Recreational drug use (ecstasy and cocaine, crystal meth. especially) Caffeine (6+ cups a day)
Drugs Succinylcholine (strange…this is a muscle relaxant) Phenothiazines Tricyclic anti-depressants known to cause trismus
Radiotherapy Fibrosis of muscles of mastication when within field of radiation
Medial Ptyerygoid Haematoma
- Caused by damage to medial pterygoid muscle (bent needle tip in this case)
- More common in older patients. 2-5 days after mandibular block given
- LA injection directly into MP muscle can cause myotoxic reaction leading to necrosis
- Hematoma in the muscle can lead to fibrosis -> trismus
- Management: Hot packs (20mins every hour), stretching with wooden spatulas, analgesics as required
Osteomyelitis
= infection of the bone
Radiographic findings Initially soft tissue changes: - Muscle swelling and blurring of soft tissue planes
1st changes in bone indicate infectious process present for 2-3 weeks + - Extends 1cm and compromises 30-50% to produce noticeable changes in radiographs - Early changes not obvious until 5-7 days in kids or 10=-14 days in adults
** If patient doesn’t feel right, need to see them right away or could have a lawsuit**
PBL 3 - Bettina
Smart BMI Differs from the traditional BMI in 3 ways:
1. Takes Age and Sex into account in addition to the weight and height
2. Purely comparative (no physical units) on a scale /70
3. Can relate to your health whereas BMI cannot
SBMI Assessment Risk Level
0/70 – 9/70 Extreme Anorexia Red
10/70 – 19/70 Anorexia to underweight Orange
20/70 – 29/70 Moderate to slight underweight Yellow
30/70 – 39/70 Normal Weight Green
40/70 – 49/70 Slight to Moderate Overweight Yellow
50/70 – 59/70 Overweight to obese Orange
60/70 – 70/70 Extreme Overweight Red
Bones Functions Facial Skeleton
- House and protect brain, organs of smell, sight, and taste - Provide framework for muscles of mastication, facial expression, breathing, and speech to function on
In General: - Haematopoiesis -> Red bone marrow (Axial Skeleton, Pectoral Girdle, Pelvic Girdle, Proximal of humerus and
femur bones) - Lipid and Mineral storage - Shape and framework for the body - Resist compressive forces
Characterizations
Appearance Bone Type
Gross Appearance Flat - Skull, Pelvis, Scapula
Long - Axial Skeleton
Macroscopic Appearance
Compact/Cortical - Mature bone, Flat bones, Shaft of long bones - Dense and solid, surrounds marrow space - Entire mandible is bicortical
Spongy/Trabecular
- Early bone, interior of extremities/epiphysis of long bone - Honeycombed network of trabecular plates and rods within the marrow component
Development/ Formation Intramembranous - Direct formation of mesenchyme - Flat Bones
Endochondral - From a cartilage model - Long Bones
Regions Diaphysis - Shaft
Metaphysis - Transition of shaft leading to growth plate zone
Lamellar - Collagen arranged in concentric layer (like rings of a tree)
Disposition of lamellae Circumferential - Periosteal and industrial surfaces
Osteonic - Concentric lamellae forming osteons (new bone)
Interstitial - Residual fragments between newly forming osteons (older bone)
Types of Osteons Primary - 1st formed Haversion systems consisting of poorly organized lamellae
Definitive - Higher ordered osteons after the remodelling of primary osteons
Elderly Injuries Falling Hypertension Drugs are common causes of falling
- Vasodilators, diuretics, certain CCB’s exacerbate postural blood pressure changes -> orthostatic hypotention = light headedness and falling
β-blockers, ACE inhibitors, Angiotensin-receptor antagonists are safer to prevent falling
Bruising/Contusion Occurs when there is a subcutaneous or submucosal haemorrhage without breaking the skin - From trauma or body damage rupturing blood vessels under skin
Elderly prone to bruising (↓ force required to cause one) - ↓ elasticity of the vasculature making vessels more fragile
Saggy/wrinkly skin -yummm
Moisture retention of skin ↓ making it dry, scaly and wrinkled Skin loses elasticity also = sagging
Mandible Fracture Types
Simple Closed linear fractures (condyle, coronoid, ramus, edentulous body of the mandible) - Single break, no bone exposure
Compound
Fractures of the tooth bearing portions of the mandible, protruding into the mouth via periodontal membrane - Rare, but can also expose through the skin - May cause a step in the arch
Comminuted
Often a compound fracture, but with multiple pieces of broken bone, not 1 single break
Pathological A break resulting from a weakened mandible (ONJ, Bone Cysts etc)
Condyle is most frequently broken > Angle / Body > Parasymphysis > Ramus > Coronoid Process
Favorable Fractures Occur in a direction where the pull of the muscle of mastication do not displace the 2 ½’s of the break. - Horizontal: In relation to the upward pull of the masseter - Vertical: In relation to the medial pull of the mylohyoid, digastric etc.
Unfavorable Fractures Occurs in a direction thast the pull of the muscles of mastication separates the 2 halves of the break - Horizontal: In relation to the upward pull of the masseter - Vertical: In relation to the medial pull of the mylohyoid, digastric etc.
A: Horizontally Unfavorable B: Horizontally Favorable C: Vertically Unfavorable D: Vertically Favorable **The “vertical and horizontal” classifications seem counter intuitive. The name doesn’t refer to the direction of favourability as much as it refers to the plane at which the fracture is viewed** - A and B are viewed from the side (horiz.) - C and D are usually viewed from above (Vert)
Management of the fracture
Reduction Placing the fractured fragments in the correct alignment - Closed Reduction: No surgical intervention. The tissues remained closed - Open Reduction: Surgical access used to expose the bone. Tissues were opened
Essential to place in relation to the mandible to recreate the normal occlusal relationship Approximated reduction puts the fragments close to each other, but not directly in contact to allow “indirect fracture healing”
- Both endochondral and intramembranous bone healing occurs, enhanced by micro-motion and weight bearing
Fixation Holding/fixing the bony fragments in position once reduction is complete Maxillomandibular Fixation:
- Wiring the Max. and Man. together - Good to keep occlusal relationship - Very uncomfortable for the patient - Liquids only - Must educate the patient on how to cut the wires or elastics off in case of vomiting!
Rigid Internal Fixation: - Screws and PLastes - If the direction of the break allows, the 2 pieces can be screwed together - An overlying plate can be screwed on to hold pieces together -> Used in comminuted fractures with many fragments.
Secondary Bone Healing -> Micro movement present, bones not screwed or fixed solidly in place, large gap between segments
Immediately after break
Haematoma formed (cells of peripheral and intramedullary blood, bone marrow cells) - Initiates inflammatory response -> Clot forms between and around the fracture pieces and within the medulla
= Template for callus formation
Within 48 Hours Chemotactic molecules attract more inflammatory cells Blood clot provides fibrin mesh to seal fracture site & provide framework for inflammatory cells fibroblasts and new capillaries Platelets + Inflammatory cells -> release PDGF, TGF-β̛, FGF etc = Activates osteoprogenitor cells and stimulate osteoblasts and osteoclasts
Early Fibroplastic Stage
Occurs if fractured ends are >1mm apart - Large amounts of collagen have to be laid down to bridge the gap first
Osteoprogenitors differentiate and proliferate into osteoblasts, clasts and chondroblasts, capillary budding begins
End of Week 1 Matrix production in adjacent tissues and fractured ends of bone start remodeling Fibroblasts and chondroblasts produce ECM of fibrous tissue and cartilage where woven bone can be deposited by osteoblasts -> Soft Tissue Callus
- Provides anchorage between ends of bone (but isn’t rigid for weight bearing)
End of Week 2 Soft Tissue Callus turns into bony callus - Woven bone is first to be laid down - Mesh of woven bone replaced by lamellar bone organized parallel to the axis of bone
Osteoprogenitor cells deposit subperiosteal trabeculae of woven bone (perpendicular to cortical axis) within the medullary cavity
Late Fibroplastic Stage
Osteoclasts resorb necrotic bone - Areas of ↑ O2 tension: Osteoblasts deposit bone - Areas of ↓ O2 tension: Chondroblasts lay down cartilage
Capillary and Callus growth continues
End of Week 3 Bony callus reaches largest girth -> helps stabilize fracture - Will be able to feel for 3-4 months until the fragments are firmly united by new bone
New cartilage along fracture line undergoes endochondral ossification to form bone w/ trabeculae in medulla and beneath periosteum
Final Stages Bony union is achieved when fracture site is completely bridge with woven bone (the first bone to go down) - w/ functional stresses (Wolff’s law) callus is remodelled to form mature lamellar bone
Fully healed Initial stages of bony healing lasts about 6 weeks
Primary Bone Healing -> Absolute Rigidity of 2 pieces is achieved by screwing or plating the 2 pieces together is tight approximation
- <200nm -> Lamellar bone is directly formed in gap
- >200nm – Woven bone fills gap and is replaced with lamellar bone
A good video!
https://www.youtube.com/watch?v=MNkI6Of2PRs
After-care treatment of fractures Emergency Release of Wires Teach patient how to release the MMF in case starts choking or vomiting
- Can give wire cutters or use elastics instead of wires
Radiographs Postop radiographs taken within first days post-surgery and prior to removing MMF
Follow-up Check stability of occlusion and infection 1 week after surgery - Periodically check oral hygiene and signs of infection
Physiotherapy Mandible will be hypomobile after MMF with atrophic and tight muscle - Opening and excursive exercises should be Rx - If has trismus can use a Therabite device (super expensive), or
just stack popsicle sticks between teeth to force mouth open
Speech Patient should speak as freely as possible to ↑ range of jaw motion and provide the micro-motion necessary to ↑ healing of the jaw
Oral Hygiene Rx Chlorhexidine rinse used 3x/day Use a waterpik and sulcabrush to clean between teeth and toothbrush for buccal surface
Bone Remodelling Complex process controlled by hormones (Leptin and serotonin) from the CNS and by mechanically induced micro-damage
- Depends on Basic Multicellular Unit of Bone (Osteoblast, Osteoclast, Osteocyte) -> BMU
Wnt family of molecules/genes regulates differentiation of pluripotent mesenchymal stem cells into the osteoblastic lineage and ↑ osteoblastic
bone formation
Factors Influencing Remodeling
Type of fracture Displaced, or comminuted fractures have delayed union because must bridge a larger gap during healing. - Any soft tissue trapped between bone ends can prevent union completely
↑ Mobility at fracture site Too much mobility interferes with vascularization of the fracture haematoma -> ↑ strain and disturbing bridging callus
Age Kids bones remodel and unite faster than older patients
Nutrition and Drugs ↓ nutrition, long term corticosteroids and NSAIDs can impair inflammatory response and delay fracture healing
Infection ↓ healing due to prolonged inflammatory phase
Smoking This is generally always bad…just don’t do it…you don’t look cool...and no one wants to kiss you
Response to loading occurs via mechano-transduction where mechanical forces are converted to biochemical signals (Integrins do the sensing of
the ECM)
- Trabecular bone first resorbed by osteoclasts -> creates a shallow pit called “Howship’s Lacuna”
- Osteoblasts then deposit compact bone within the lacuna
Stages
Phase Description
Resorptive Phase
Osteoclasts from bone marrow monocytes resorb discrete area of bone matrix
Reversal Phase Osteoprogenitor cells proliferate and differentiate into osteoblasts
- Migrate to the resorption lacuna to stop osteoclast activity
Formative Phase
Osteoblasts deposit new bone -> initially unmineralized and called “ostia weight”
- Eventually mineralizes and surrounds osteoblast into an osteoid
Resting Phase Once embedded in osteoid osteoblasts mature into osteocytes - Osteoblasts lying on the surface lay dormant until
activated
PBL 4 – Jackie Falls
Osteoporosis Overview Primary Secondary
Females predominantly - ↓ estrogen after menopause - Faster bone loss in general
Caused by chronic medical conditions - Endocrine disorders (hyperthyroidism) - Intestinal Disorders (↓ Vit. D and Ca++ absorption) - COPD - Hypogonadism - Multiple Myeloma
Risk Factors Modifiable Non-Modifiable
↓ Estrogen/Testosterone ↓ Ca++ & Vitamin D Inactive Lifestyle Excessive Alcohol Cigarette Smoking Hyperparathyroidism Hyperthyroidism Malnutrition (Malabsorption or Diet) Steroids or Cushing’s Syndrome Proton Pump Inhibitors (↓ Ca++ absorption)
↑ Age Low BMI Ethnicity (White>Asian>Black) Family Hx Rheumatoid Arthritis
Secondary Causes
Misc. -> Most common causes - Alcoholism - Smoking - Organ transplant - COPD - End-stage renal disease - Immobilisation
Screening DEXA scan - Dual Energy X-ray Absorptiometry -> 2 photons released from X-ray tube to give precise measurements at important sites - Measures bone mineral density and is the best predictor of fracture risk - Woman 65+ should get this scan done and men 70+
T-score - Post menopausal women - Determine if has OP Normal T-score: > -1.0 Osteopenia: -1.0 - -2.5 Osteoporosis: <-2.5 Z-Score
- Premenopausal Women - Determines BMD relative to healthy young controls FRAX – Fracture Risk Assessment X
- Assesses Age, Gender, BMI, Fracture Hx, Current Smoking, Glucocorticoid use, and Rheumatoid Arthritis Hx
Prevention Adequate Nutrition (Ca and Vitamin D specifically) Weight Bearing exercise Stopping Smoking Discourage Alcohol Abuse ↓ Falling risks Hip Protectors
= Any fall from standing height or less that causes a fracture (when it shouldn’t normally)
- Commonly Hip, Spine, Wrist
Factors Leading to Fracture
Vertebral Fractures Compression fractures can vary from Mild Wedge fractures to complete compression - Varying degrees of pain, can be almost asymptomatic is a slow insidious onset
Dorsal Kyphosis (Dowager’s Hump)
- Occurs with exaggerated lordosis -> Outward curve of stomach. Makes old ladies think they are getting fat.
- Can be result of multiple compression fractures
Calcium Homeostasis
↓ Ca++ (Hypocalcaemia) ↑ Ca++ (Hypercalcaemia)
Voltage gated ion channels open spontaneously - Nerve and muscle cells become hyperactive - Involuntary muscle spasms potentially leading to hypocalcaemic
tetany
Ion channels have a hard time opening - ↓ nervous system functioning - Ca combines with PO4 = deposits of Ca(PO4) in vessels and kidneys
Influenced by dietary intake, Ca++ absorption in small intestine and excretion of Ca++ in urine - Bones are reservoir of Ca++ used to maintain homeostasis
Endocrine Regulation
Parathyroid hormone (PTH) Secretion stimulated by hypocalcaemia to ↑ Ca++ - Stimulates bone resorption - ↓ urinary loss = ↑ Ca++ reabsorption in kidneys - Stimulates synthesis of Vitamin D -> ↑ Ca++ absorption from small intestine
Vitamin D [1,25(OH)2D ]
↑ Ca++ absorption from the small intestine
Thyroid Hormone Act directly on osteoblasts -> important for skeletal growth in children - Hypothyroidism = ↓ bone growth, short stature - Hyperthyroidism = ↑ bone loss (osteoclastic), suppression of PTH, ↓ Vitamin D metabolism, ↓ Ca++
absorption
Polymyalgia Rheumatica - Inflammatory Rheumatic (non-articular) condition characterised by aching and morning stiffness in the shoulders, hip girdle, and neck
o Closely related to Giant Cell Arteritis (GCA)
o No muscle weakness
MRONJ (Medication Related Osteonecrosis of the Jaw) Risk Factors Concomitant use of estrogen
Prolonged use of bisphosphonates Age >65 Smoking Alcohol Use Poor Oral Hygiene Chemotherapeutic drugs
IV vs Oral bisphosphonates
IV - 6 doses (monthly) ↑ risk of MRONJ -> 6 months before effects
Oral - 156 continuous weekly doses (3 years) ↑ risk of MRONJ -> 3 years before effects - ↓ lipid solubility = ↓ absorption in small intestine, need to take with milk to ↑ absorption - Accumulate in bone slowly -> Doesn’t show clinically exposed bone until 3 years after drug
** Important for dentist to evaluate all teeth before start of treatment and complete all work before the risk of MRONJ ↑ (6 months if IV, 3 years if Oral)**
Clinical Presentation - Exposed bone (varying amounts from pinpoint to extensive) -> necrotic bone beneath - Alveolar bone extending into inferior border of mandible Rami and zygoma or maxillary sinus walls
-> high bone turnover & Greater reliance on osteoclast-mediated remodeling - Pressure and tension forces ↑ in alveolar bone by occlusion or dentures - Deep Bone Pain -> painful when infected with microbes - Tooth Mobility unexplained by dental or other pathologies
Radiographic Signs Widened periodontal ligament space (not Dx of MRONJ) Sclerosis of Lamina Dura (not Dx of MRONJ) Ill-defined diffuse radiolucency/opacity
Prevention Before IV Bisphosphonates - Have 6 months to prepare oral cavity - Eliminate pathology ASAP so you don’t need to do invasive procedures while on Bisphosphonates - Remove teeth that are non-restorable, abscessed, periodontally compromised, or with failing root canals - Perio care to ↓ inflammation, save treatable teeth, educate patient - Restore restorable teeth
During IV Bisphosphonates
- Avoid invasive surgical procedures affecting the bone - Restorative procedures not affecting bone are ok (crowns, bridges, Removable partial and full dentures) - Non-restorative teeth give root canals instead of extraction - Splint mobile teeth
-> D-Pyd Test - Deoxypyridinium cross links organic matrix in Type I collagen of the bone -> ↑ amounts in urine indicate rapid bone loss/turnover
-> Can predict the possibility of developing MRONJ if patient has been on it for 3 years Concomitant use with:
- Prednisone and Methotrexate ↑ risk of MRONJ and its severity - Ranitidine and other H2 blockers ↑ risk of MRONJ
Treatment of MRONJ Self-maintenance will ↓ possibility of developing multiple more sites Follow up every 4 months Bone resection may be needed for severe cases Antibiotics:
-> If allergic to penicillin: Levofloxacin 500mg 1x/day; Doxycycline 100mg 1x/day; or Zithromycin 250mg 1x/day - Metronidazole 500mg TID for 10 days adds control for gram –‘ve anaerobes
PBL 5 – Mrs. Stephanie Curry
Radiographs of TMJ - Hard to evaluate TMJ with conventional radiographs -> Many structures in front of it superimposed makes clear image not possible
o Need advanced imaging to see mild bony changes
Cone Beam Computed Tomography (CBCT) -> High-res multiplanar images allowing 3D examination of the TMJ without superimposition or
distortion
- Allows us to evaluate bone morphology, Joint Space, Dynamic Function
Magnetic Resonance Imaging (MRI) also a good diagnostic tool for the TMJ
CBCT Cephalometric Radiograph
Seeing: -Erosions of the condylar head -Sclerosis -Osteophyte formation -↓ joint space
Really hard to see anything here because of all the superimposition infront of the TMJ, but we can see a pretty major anterior open bite - This is caused by significant erosions to the Condylar head making its relationship in the TMJ different
Arthritis Primary Arthritis
- Joint pain is main feature of disease Secondary Arthritis
Chronic inflammation leads to ↓ cartilage, erosion and weakness of the bone -> joint deformity, destruction and ↓ function - Swan Neck deformity, Z-thumb, Ulnar Deviation of the fingers
Etiology Not known for sure - Complex interplay of environmental and genetic factors -> Combo of: Infection, Autoimmunity, Genetics
Rheumatoid Factor
Autoantibody produced by B-cells - IgG targeted against Fc portion of IgG’s -> Form complexes and activate complement system = ↑ inflammation and
persistent synovitis Found in:
- Rheumatoid Arthritis - Systemic Lupus Erythematous (SLE) - Sjogren’s Syndrome - Hepatitis B - Chronic Liver disease and hepatitis
Pathogenesis Initial triggering event causes proliferation of synovial macrophages and fibroblasts (Fibroblast- Like Synvocytes) - Lymphocytes infiltrate perivascular regions and angiogenesis ↑ vascular access to area - Blood vessels affected in joint become occluded with clots and inflammatory cells
Inflamed synovial tissue grows irregularly and forms pannus which invades and destroys cartilage and bone
- Pannus = thickened synovial tissue -> stimulates release of IL-1, IL-6, TNF, PDGF, Prostaglandins, Substance P by macrophages = cartilage destruction and bone erosion
RA of the TMJ Affects 50% of RA patients -> correlated to severity and duration of disease 1. Intra-articular Osteopenia w/ soft tissue swelling 2. Erosions and joint space loss
Affected bilaterally often quite late in disease progression - Pain - Swelling - ↓ Movement (opening and lateral) - Crepitus - Morning stiffness (lasting >30mins)
Symptoms are usually transient but if severe enough can lead to: - Bilateral destruction of condyle - Anterior Open bite - Malocclusion - Micrognathia in JIA patients
Treatment Complex and non-curative -> just trying to maintain function and keep disease from progressing 1st Line:
- NSAIDs and cortisone -> fast acting to ↓ pain and inflammation 2nd Line:
- DMARDs (Methotrexate and hydroxychloroquine) -> promote remission and prevent progression - Biologics (Infliximab, Adalimumab etc)
Methotrexate
- Antimetabolite targeted against dihydrofolate reductase -> Prevents folate synthesis = prevents DNA replication and repair in replicating cells
- Indicated in cancer (Lymphoma, Breast cancer, Leukaemia, Head and Neck cancer) - HIGHLY toxic when combined with NSAIDs, Corticosteroids and Penicillin’s
Drug Side Effects
NSAIDS -> Prolonged Bleeding DMARDS
- Methotrexate -> Ulcerative stomatitis, gingivitis, glossitis, mucositis - Anti-malarial -> Lichenoid reactions, Oral hyperpigmentation - Use with NSAIDS can cause bone marrow suppression and aplastic anemia
TNF Blockers (infliximab)
- Immunosuppression - Consult with physician re: drug holiday or elective surgery
Genetic Predisposition Genome = ALL the genetic material in the cells (Gene coding exons and non-coding introns)
Pregenomic = Crude mapping of trains to certain chromosomal regions
- Based on phenotypic associations -> Blue eyes and blonde hair are closely associated so it is likely they are close on a chromosome
Genomic = Precision mapping of DNA sequence variations
Mutations
Hereditary Passed down to offspring through germ line mutations in egg or sperm Can be de novo mutation occurring for the first time and still be considered hereditary, just needs to be a germ line mutation.
Non-Hereditary
Occurs in cells outside of the germ line Cancer
Mutation Types
Silent Single base change in a codon, but the amino acid encoded is the same -> no effect to the protein
Missense Single Base change to encode a different amino acid
Non-sense Early Stop codon
Frameshift Many different codons completely changes the protein
** Non-sense and Frameshift mutations are most likely to cause disease**
Micro-mutations
Deletion Base is deleted, changing the reading frame
Insertion Base added, changing the reading frame
Substitution 1 base replaces another, possibly changes the amino acid
Macro-mutations
Deletion Whole sections of the chromosome are deleted/removed
Duplication Whole sections of the chromosome are duplicated
Inversion Section of the chromosome is flipped upside down
Substitution Section of 1 chromosome moved to another chromosome
Translocation 2 sections from 2 chromosomes are switched
- Can act at many levels to alter protein synthesis and function
o Regulatory areas (non-coding)
o Cause splicing errors in the exons
o Affect RNA stability
o Alter protein expression and stability
Inheritance patterns Autosomal Dominant: 50% chance of inheriting trait
- With 2 generations having the trait, can find the causative mutation within the 3 billion base pairs!
Amelogenesis Imperfecta
Inheritance Patterns of the AMELX gene
All 3! Autosomal Dominant
- Can be found in every generation
Autosomal Recessive - If there is consanguinity can lose the normal copy of the gene and have
2 mutated versions (That’s why you don’t sleep with your cousins!) X-Linked
- Males will express mutated genes on X chromosomes (only have 1) if they inherit a bad one from the mom
- Females can present also if X-inactivation occurs on the normal chromosome
Genes that can cause AI Fam83H Enamelin Ameloblastin Amelogenin Mmp-20
Dentinogenesis Imperfecta
Presentation Translucent, amber discoloration of the teeth Rough surface prone to wear Enamel is sheered off leaving exposed dentin
Inheritance Pattern Autosomal Dominant
Oligodontia
Whats going on >6 teeth missing (not including 8’s) - Usually a single gene mutation that causes agenesis of multiple teeth
Variations in the Genome Ways that we can get normal variation:
Independent Assortment Randomly sorts which copies of the gene go into the individual sperm or eggs during Meiosis
Cross Over Mixing of the mother and father’s DNA during Meiosis - Homologous chromosomes can swap sections of genes to create new variants
Random fertilization 1 sperm fertilizes 1 egg -> completely random which egg and which sperm will fertilize
Single Nucleotide Polymorphisms (SNP)
Variation at a single position in a DNA sequence among individuals - May not directly cause a disorder but are associated with certain diseases
-> Can asses genetic predisposition to certain disease development! To be called a SNP -> >1% of the population have the variant
- No disease-causing variants are this common Challenging to know if SNP contributes to a disease
- Can be in a gene desert with nothing around, but may affect a long range enhancer! Can’t say for sure in SNP is disease causing or pathogenic
- Can change protein function, BUT not considered a mutation if it is commonly found in population = variant
Dental Traits with Genetic Basis Strong Basis
- Few genes affecting the trait
Toot Agenesis Many genes needed for tooth initiation, a few are associated with agenesis - WNT10A - AXIN2 - EDA
Posterior Agenesis - PAX9 - MSX1 - AXIN2
Aggressive Periodontal Disease
…I guess there is nothing much to say here?
Cleft Palate Only Whole-Exome Sequencing (WES) used to identify 2/26 candidate genes with association - GRHL3 - CREBBP
Weak Genetic Links - Dozens of genes involved
Cleft lip w/ or w/o cleft palate
- Need HUGE data to find genes with significant contribution to clefting - Deep phenotyping needed to find more affected family members acting as carriers
Facial Appearance Genome-Wide Association study found multiple loci influencing normal human facial morphology! - MAFB - PAX9 - MIPOL1 - ALX3 - HDAC8 - PAX1
One step closer to true designer babies
Malocclusion Especially class III - ADAMTS1
Pain Sensitivity
Drug Sensitivity
Pharmagogenomics = how genes affect a person’s response to drugs
- Used to develop safe and effective meds with doses tailored to persons genetic profile. Can also be used to predict if a person will have a
good or bad response to a drug
Pharmacogenetics = inherited differences in drug metabolism
**Once again we can use SNP’s do determine certain variants associated with good or bad responses to a drug
Cytochrome Enzymes Strong players in drug metabolism - Affected by genetic variation to affect its function with certain drugs
CYP2D6 variants lead to ↑ levels of morphine for a particular dose of codiene: ↑ risk of opioid induce respiratory depression
- Rapid Metabolizer phenotype: overactive system caused by gene duplication - Poor metabolizer phenotype: Enzyme inhibition or defect in one of the 2 alleles
Redheads MC1R gene variants = ↑ dental anxiety and fear of dental pain - Found specifically in females, Males are unaffected by this variant
MC1R ↓ expression with pheomelanin (molecule that causes redheads to be readheads)
Epigenetics = Environmental changing of the genome (methylation, histone packing via acetylation)


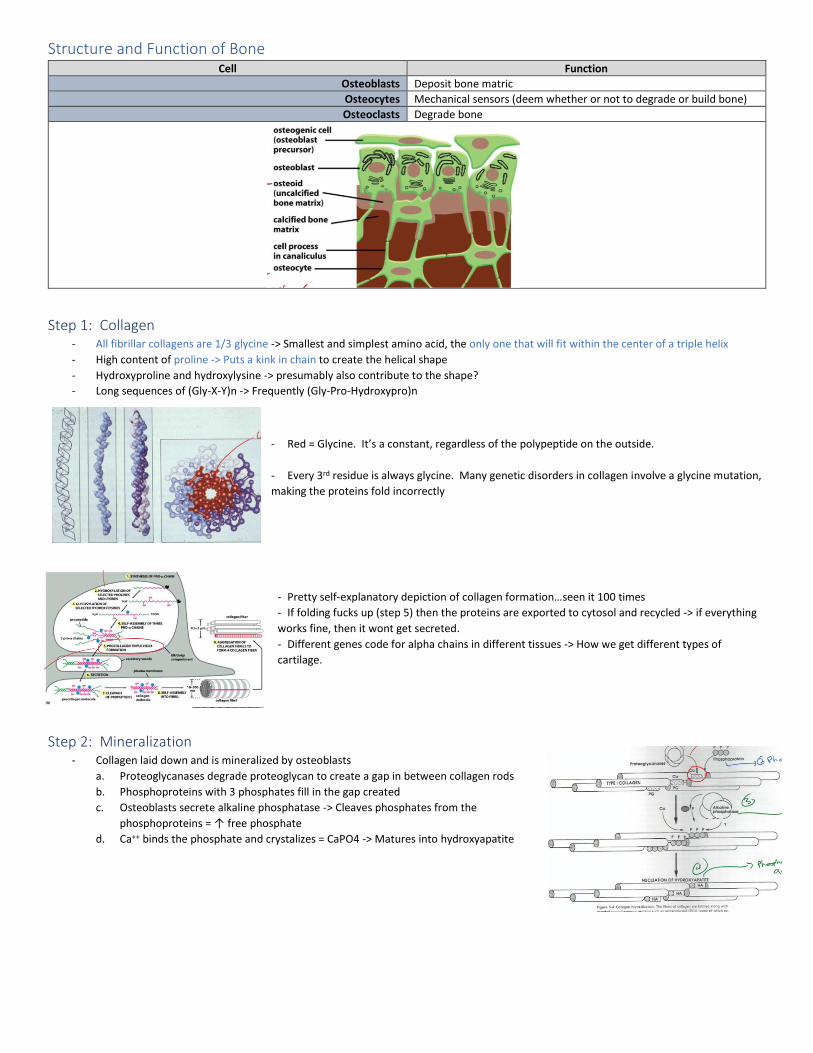












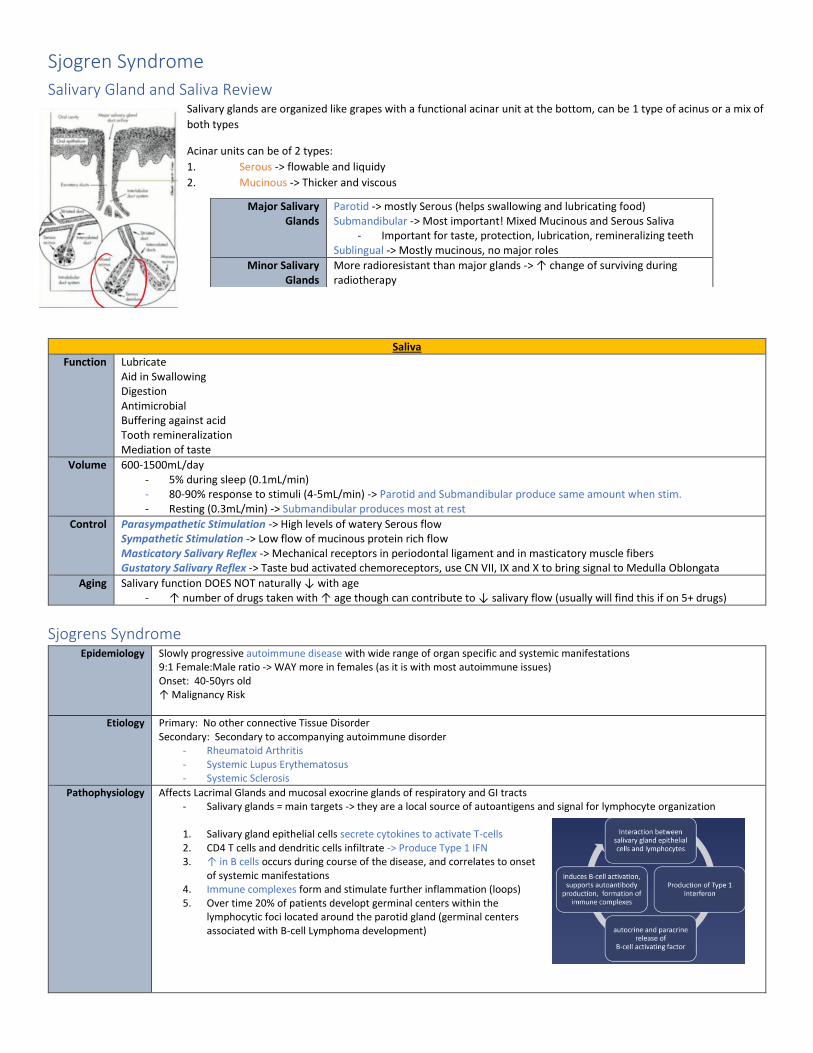










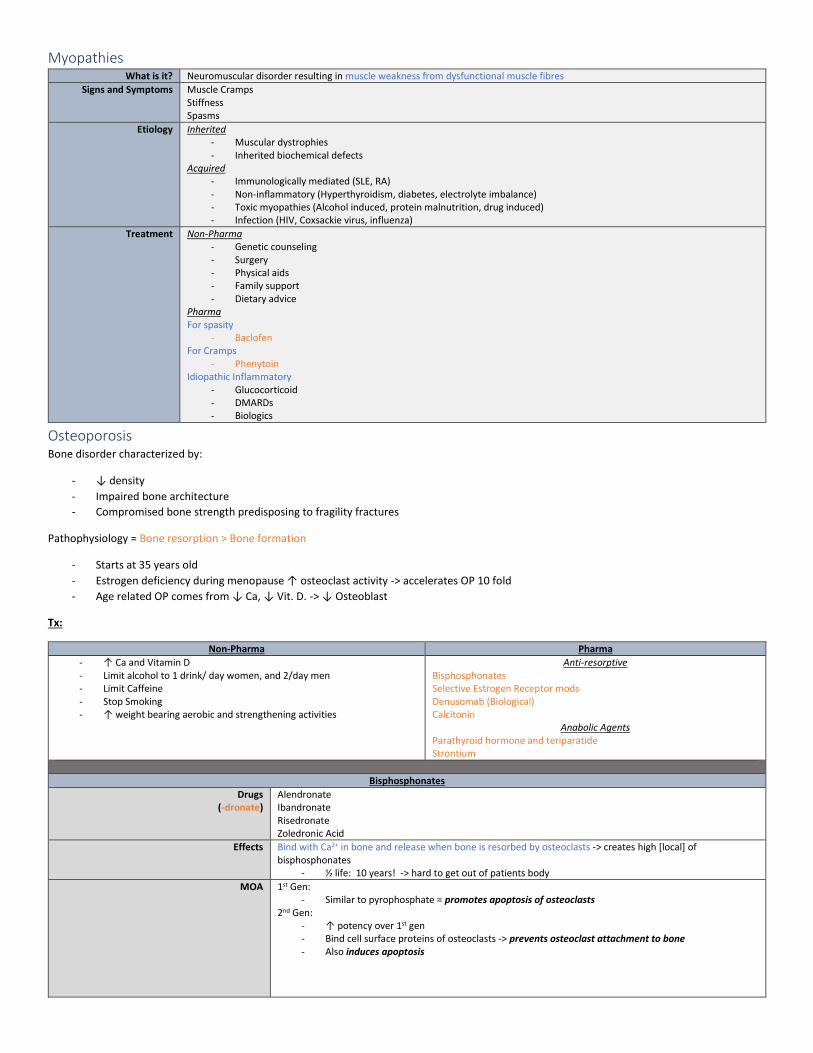






















![Intermediate Matrix - SRAR.com Intermediate_CRISNet.pdfIntermediate Matrix Tech Support SRAR-SFV 818 947 2202 SRAR-SCV 661 295 7117 techsupport@srar.com [7] HOT SHEETS Hot Sheets give](https://static.documents.pub/doc/80x56/60c6050d4fcd5763f97c125f/intermediate-matrix-srarcom-intermediate-intermediate-matrix-tech-support-srar-sfv.jpg)













