A SURVEY OF COMPETENCY BASED RECRUITMENT AND SELECTION PRACTICES ADOPTED BY REGISTERED HOSPITALS IN NAIROBI DORIS MWANGI A RESEARCH PROPOSAL SUBMITTED IN PARTIAL FULFILMENT OF THE REQUIREMENTS FOR THE AWARD OF THE DEGREE OF MASTERS OF BUSINESS ADMINISTRATION (MBA), SCHOOL OF BUSINESS, UNIVERSITY OF NAIROBI NOVEMBER 2013
Transcript
A SURVEY OF COMPETENCY BASED RECRUITMENT AND
SELECTION PRACTICES ADOPTED BY REGISTERED
HOSPITALS IN NAIROBI
DORIS MWANGI
A RESEARCH PROPOSAL SUBMITTED IN PARTIAL FULFILMENT OF THE
REQUIREMENTS FOR THE AWARD OF THE DEGREE OF MASTERS OF
BUSINESS ADMINISTRATION (MBA), SCHOOL OF BUSINESS, UNIVERSITY
OF NAIROBI
NOVEMBER 2013
ii
DECLARATION
This research project is my original work and has not been presented for a degree award to
any other university.
Signed: ………………….. Date: ……………………
DORIS MWANGI
This research project has been submitted for examination with my approval as University
Supervisor
Signed: ………………….. Date: ……………………
PROF K’OBONYO
iii
DEDICATION
I would like to dedicate this research project paper to my father, who has instilled in me the
love of knowledge and continuous learning, all the way from kindergarten stage up until
my current level. I will always treasure his support and belief in my capabilities.
iv
ACKNOWLEDGEMENT
I would like to acknowledge the University of Nairobi as a whole for giving me the
opportunity to pursue my higher education at an advanced level. In particular, the
mentorship of my supervisor greatly assisted me in my professional skill set. Thank you
all.
v
TABLE OF CONTENTS
Declaration ....................................................................................................................... ii
Dedication ....................................................................................................................... iii
Acknowledgement ........................................................................................................... iv
List of Tables ................................................................................................................. viii
List of Figures .................................................................................................................. ix
List of Abbreviations and Acronyms ..................................................................................x
Abstract ........................................................................................................................... xi
Appendix II: List of Hospitals .......................................................................................... 60
Appendix III: List of Sampled Hospitals .......................................................................... 62
viii
LIST OF TABLES
Table 4.1: Distribution of respondents by gender ............................................................. 33
Table 4.2: The extent to which various factors are considered in recruiting new staff ....... 35
Table 4.3: Mean and standard deviation for the measures interpersonal relations.............. 36
Table 4.4: Mean score and standard deviation for measure of self-awareness/ confidence 37
Table 4.5: Mean and standard deviaitions for the measure of analytical thinking .............. 38
Table 4.6: Mean scores and standard deviations for measures of adaptability/flexibility ... 39
Table 4.7: Mean scores and standard deviations for measures of observation skills .......... 40
Table 4.8: Mean scores and standard deviations for measures of sense of mission ............ 40
Table 4.9: Mean scores and standard deviations for measures of communication skills .... 41
Table 4.10: Mean scores and standard deviations for measures of motivation ................... 42
Table 4.11: Mean scores and standard deviations for measures of planning and organizing work ................................................................................................................................ 43
Table 4.12: Mean scores and standard deviations for measures of teamwork .................... 44
ix
LIST OF FIGURES
Figure 4.1: Distribution of respondents by age bracket ..................................................... 34
x
LIST OF ABBREVIATIONS AND ACRONYMS
CBHRM: Competency based human resource management
CIPD: Chartered Institute of Personnel and Development
HRH: Human Resource for Health
HRM: Human Resource Management
WHO: World Health Organisation
xi
ABSTRACT
The current Human Resource for Health (HRH) challenges include inadequate and inequitable distribution of health workers; high turnover; weak Human Resource Development, planning, management and Human Resource for Health information systems and the performance management framework at all level. Most organizations have little insight into the recruiter skills that have the greatest impact on quality of hire and time to productivity. As a result, recruiter training is often unfocused and misaligned with the drivers of new hire quality. The research objective was to determine the competency based recruitment and selection practices by registered hospitals in Kenya. This study was descriptive in nature. This design is preferred because it permits comparative analysis. The researcher targeted all the sixty (60) registerd hospitals in Nairobi where a sample size of forty hospitals was selected.Primary data was collected. This was used to address competency based recruitment and selection practices. Data collected from respondents was both quantitative and qualitative in nature. Quantitative data will be analyzed using the descriptive statistics such as mean scores and standard deviations. The findings were then presented using tables, pie charts, and bar graphs for easier interpretation. On the other hand, qualitative data was analyzed using content analysis. The qualitative information was used to interpret or better understand quantitative findings. It can be concluded that the results from the findings of the questionaire demonstrated that competency based recruitment procedures were paramount in selecting new hires. The respondents recognized that competency based recruitment procedures can work hand in hand with traditional recruitment and selection procedures. The competency based approach to recruitment and selection was considered important in the recruitment and selection stage of Human Resource Management processes.Based on the findings, it is recommended that, the need to develop and implement a communication strategy to support the Human Resource Departments. It is also important to build awareness is an important starting point. HR staff and hospital management should attend workshops, classes, or conferences on competency modelling or invite external consultants.
1
CHAPTER ONE
INTRODUCTION
1.1 Background of the study
Smit and Cronje (1982) claim that it is people who give life to an organisation and that
they can be regarded as an organisation’s most important resources. Covey (1997) agrees,
stating that people attain the highest value in an organisation, because they are the
programmers-who produce everything else at the personal, interpersonal, managerial and
organisational levels. Grier (1999) explains that the economic turbulence, globalisation,
technology, changing demographics, and differences in workforce values have created
almost unprecedented environmental uncertainty. In these conditions human resources is
one of the few factors over which organisations have a measure of control, thus reinforcing
human resources as a distinctive factor for competitive advantage. This automatically
implies that other factors are conditional for entry into competition. Johnson and Scholes
(2002) state that the possession of resources, including people, does not guarantee strategic
success. However, the way these resources are deployed, managed, controlled and, in the
case of people, motivated to create competence in those activities and business processes
needed to achieve competitive advantage, differentiate the mediocre from the market
leaders.
According to Mullins (2010), if the HRM function is to remain effective, there must be
consistently good levels of teamwork, plus ongoing co-operation and consultation between
line managers and the HR manager.’’ This is most definitely the case in recruitment and
2
selection as specialist HR managers (or even external consultants) can be an important
repository of up-to-date knowledge and skills. In a dynamic environment, health managers
need to combine leadership, en entrepreneurial and administrative skills to meet the
challenges that the changing socio-political, economic and technological landscape
presents, as well as the expectations of patients, health professionals, politicians and the
public. Without good management we will be unable to improve efficiency, effectiveness
and responsiveness in the delivery of health services or upscale to achieve health goals
(Travis et al.2004).
Hospitals are important vehicles for the delivery of health care, and managers of these
institutions are to a large extent responsible for operationalizing the visions and objectives
that policy-makers have for the health and wellbeing of a nation (Lehman et.al.
2002).Determining and assessing competencies is a vital precursor to improving
professional development and the alignment of individual development with the need of an
organization or profession (Calhoun et.al. 2004). The competency-based approach to
professional development is well accepted in higher education (Westera 2001), and in
human resource management literature where it is regarded as a critical part of the overall
management development process, as it allows one to identify the gaps between current
skills and the skills required (Brown 2002,Jinabhai 2005) . Appropriate programmes based
on the personal needs and experiences of health managers can then be put in place to train
managers to provide leadership and to ensure a sustainable improvement in the work
context of health workers, and hence on the quality of care and health of the communities
their organizations serve (Gough and Price 2004).
3
1.1.1 The Concept of Competency
The definitions of competency are varied and include the ability of a person to perform a
job (Woodruffe, 1993); skills that are developed in a pattern (Bradley & Huseman, 2003);
a behavior or series of actions that can be demonstrated, observed, and assessed (Manley &
Garbett, 2000). The concept of competence or competency dominated the management
strategy literature of the 1990s, which emphasized core competence as a key organizational
resource that could be exploited to gain competitive advantage (Campbell and Sommers
Luchs,1997; Mitrani et al., 1992; Nadler and Tushman, 1999). Hamel and Prahalad defined
core competence as ‘’the collective learning in the organisation, especially how to co-
ordinate diverse production skills and integrate multiple streams of technologies’’
(Prahalad and Hamel, 1990).
From the perspective of a resource-based theory of the firm, sustained competitive
advantage is seen as deriving from a firm’s internal resources .If these can add value, are
unique or rare, are difficult for competitors to imitate and are non-substitutable (Cappelli
and Crocker-Hefter, 1996; Ellestro1992; Foss and Knudsen, 1996). The virtue of the core
competence approach is that it ‘recognises the complex interaction of people, skills and
technologies that drives firm performance and addresses the importance of learning and
path dependency in its evolution’ (Scarborough, 1998). Snyder and Ebeling (1992) refer to
competence in a functional sense, but use ‘competencies’ in the plural. Some authors
consistently use ‘competency’ when referring to occupational competence (Boam and
Sparrow, 1992; Mitrani et al.,1992; Smith, 1993) or treat the two as synonymous (Brown,
1993, 1994). Hartle argues that competency as a characteristic of an individual that has
4
been shown to drive superior job performance (1995) includes both visible competencies
of knowledge and skills and underlying elements of competencies like traits and motives.
Elkin (1990) associates competence with micro-level job performance and competencies
with higher management attributes and, in defining managerial competencies for the
future, Cockerill (1989) combines output competences, like presentation skills, with inputs
like self-confidence. The difficulty of using competence as an overarching term as well as
a specific one is demonstrated by the apparently tautological definition provided by
Dooley et al(2004).Competency-based behavioural anchors are defined as performance
capabilities needed to demonstrate knowledge, skill and ability (competency) acquisition.
Mangham (1986) noted that competence may relate to personal models, outcome models
or education and training models, as well as to the standards approach in which
benchmarking criteria are used. Mansfield (2004) similarly contrasts three different usages
of competence: outcomes (vocational standards describing what people need to be able to
do in employment); tasks that people do (describing what currently happens); and personal
traits or characteristics (describing what people are like). Weinert (2001) lists nine
different ways in which competence has been defined or interpreted: general cognitive
Since competences are centred on the individual, they are viewed as independent of the
social and task-specific context in which performance occurs, yet skill level is a
characteristic not only of a person but also of a context. People do not have competences
5
independent of context (Fischer et al, 1993). Constructivist and interpretative approaches
derived from phenomenology view competence as a function of the context in which it is
applied, where worker and work form one entity through lived experience of work
(Sandberg, 2000). Competence is constituted by the meaning that the work has for the
worker in their experience (Stoof et al., 2002; Velde, 1999). Dreyfus and Dreyfus (1986),
who used an interpretative approach to investigate competence among pilots and others,
found that attributes used in accomplishing work are bound to the work context regardless
of the level of competence attained and that in the work situation individuals acquire
situational or context-dependent knowledge and skills. Other interpretative studies, with
nurses (Benner, 1984) and police officers (Fielding, 1988a, 1988b), have equally
demonstrated that attributes acquire context-dependency through individuals’ experience
of work.
1.1.2 Recruitment and Selection
Labour market shortages and recruitment difficulties have led to a more competitive
recruitment market in the last decade. Lievens, van Dam and Anderson (2002) asserted that
the war for talent meant that the emphasis in organisations moved from the selection to the
attraction of employees. Recruitment “includes those practices and activities carried out by
the organisation with the primary purpose of identifying and attracting potential
employees” (Breaugh & Starke, 2000) and has long been regarded as an important part of
human resource management as it performs the essential function of drawing an important
resource - human capital- into the organisation (Barber, 1998). The strategic significance
of recruitment is often reported in the literature (Boxall and Purcell, 2003), the emphasis
6
being upon the need to attract and retain high quality people in order to gain a competitive
advantage, as is consistent with the resource-based view (Barney1991; Barney and Wright,
1998; Wright and McMahon, 1992).
Recruitment and selection play a pivotal role in service delivery. If utilised efficiently it
can be cost effective in more than one way. From a managers point of view the objective is
to get the maximum return on investment from human capital. Investments, such as
salaries, cost of recruitment, training, fringe benefits, are expected to be returned in the
form of profits or some sort of increase in the bottom-line. Hammersak (2002) explained
that star performers usually return three to seven times their salary’s worth in productivity.
If the right person is appointed, training cost will be minimised, breaks in delivery
decreased, and production or service increased, putting the organisation in a position of
achieving its key performance objectives of: dependability, cost, speed and quality (Slack,
Chamber and Johnson, 2001). The wrong appointment implies extended training, thus no
service or production, or incorrect service or production, over a longer period, and higher
cost to the organisation.
1.1.3 Competency Based Recruitment and Selection
Sparrow (1995) has observed that the competency literature includes a huge range of
claimed benefits specific to HR processes in organisations. Included are improved
recruitment and selection practices through a focus on required competencies.
Hiring competent people is of paramount importance and this is dependent on effective
recruitment and selection procedures which aim to select the right individuals and reject
7
the wrong ones .(Hacker 1997) Costs incurred can include low productivity, potential loss
of clients ,training costs ,advertising costs, recruitment fees and redundancy packages
.(Smith and Granes 2002)
One of the earliest ,management writers FW Taylor(1911) bemoaned the way in which
individuals were selected based on’ who you knew’ or who was first in the queue. Taylor
introduced the idea that people should be selected for their particular skills and abilities
which should be tested prior to the selection decision. Traditional recruitment and selection
has been viewed as a process by which the organization tries to accurately match the
individual to the job and can be compared to a jigsaw puzzle. (Stephen Bach 1990) The
introduction of a competency based recruitment process can help to improve workplace
performance by allowing managers to assess candidates more objectively (Farnham 2000)
1.1.4 Kenya HealthCare System
The health sector comprises the public system, with major players including the MOH and
parastatal organisations, and the private sector, which includes private, for-profit, NGO,
and FBO facilities. Health services are provided through a network of over 4,700 health
facilities countrywide, with the public sector system accounting for about 51 percent of
these facilities.
Kenya’s health care delivery system, which is charged with meeting health policy
objectives, is organised around the Ministry of Health (MoH). The Ministry of Health
headed by the Minister is charged with the responsibility of setting policies, coordinating
the activities of Non-Governmental Organisations (NGOs), and managing, monitoring and
8
evaluating policy implementation (Owino 1997). Kenya’s Ministry of Health is the largest
provider of health care (curative, preventive and promotive) and undertakes environmental
protection and pollution surveillance (Odada and Odhiambo 1989). In general, the Ministry
of Health is involved in six-health related programmes, namely promotional and
preventive health care, family planning and population control, environmental protection
and programme supervision, special programmes (such as disease control projects), and
research. (Odada and Odhiambo 1989)
The public health system consists of the following levels of health facilities: national
referral hospitals, provincial general hospitals, district hospitals, health centres, and
dispensaries. National referral hospitals are at the apex of the health care system, providing
sophisticated diagnostic, therapeutic, and rehabilitative services. The two national referral
hospitals are Kenyatta National Hospital in Nairobi and Moi Referral and Teaching
Hospital in Eldoret. The equivalent private referral hospitals are Nairobi Hospital and Aga
Khan Hospital in Nairobi.
Provincial hospitals act as referral hospitals to their district hospitals. They also provide
very specialized care. The provincial level acts as an intermediary between the national
central level and the districts. They oversee the implementation of health policy at the
district level, maintain quality standards, and coordinate and control all district health
activities. Similar private hospitals at the provincial level include Aga Khan Hospitals in
Kisumu and Mombasa. District hospitals concentrate on the delivery of health care
services and generate their own expenditure plans and budget requirements based on
9
guidelines from headquarters through the provinces. (Dr. Richard Muga, Dr. Paul Kizito,
Mr. Michael Mbayah, Dr. Terry Gakuruh, 2005).
The network of health centres provides many of the ambulatory health services. Health
centres generally offer preventive and curative services, mostly adapted to local needs.
Dispensaries are meant to be the system’s first line of contact with patients, but in some
areas, health centres or even hospitals are effectively the first points of contact.
Dispensaries provide wider coverage for preventive health measures, which is a primary
goal of the health policy.
The government health service is supplemented by privately owned and operated hospitals
and clinics and faith-based organisations’ hospitals and clinics, which together provide
between 30 and 40 percent of the hospital beds in Kenya. (Dr. Richard Muga, Dr. Paul
Kizito, Mr. Michael Mbayah, Dr. Terry Gakuruh,2005) This study, however, will be
concentrated on registered hospitals in Nairobi with the view of finding(s) on the
competency based procedures they utilize for recruitment.
1.1.5 Hospitals in Nairobi County
Hospitals in Nairobi are classified under various levels with the highest health institution
being the referral hospital, followed by the general hospital then followed by the health
centre then finally the dispensary in descending order. Clinics are normally the smallest
health facilities in Kenya and can be mobile or fixed premise in nature. Nairobi county
hospitals spread 1 referral hospital, 60 hospitals, 61 health centres and 395 sub health
centres and dispensaries. Most of the hospitals in Nairobi have recognized modern
10
diagnostic and treatment center throughout East Africa. The hospitals have a state-of-the-
art emergency center which provides medical care that is in keeping with international
standards. Apart from the emergency center, the hospitals also have facilities such as a
highly sophisticated and comprehensive diagnostic laboratory, a physical medicine center,
ambulatory surgery and medical advisory services. A typical one is the Nairobi Hospital
which runs clinics throughout different days and times of the week to meet the various
medical needs of the patients. These clinics are Family Health Clinic, Child Welfare
Clinic, Antenatal Clinic, Senior Citizens clinic, Chemotherapy Center, Diabetes Clinic,
Travel and Immunization Clinic, Breast Health Clinic and Chest Clinic. The address for
this hospital is Argwings Kodhek Road.
1.2 Research Problem
The current Human Resource for Health (HRH) challenges include inadequate and
inequitable distribution of health workers; high turnover; weak Human Resource
Development, planning, management and Human Resource for Health information systems
and the performance management framework at all level (AHWO,2009). Most
organizations have little insight into the recruiter skills that have the greatest impact on
quality of hire and time to productivity. As a result, recruiter training is often unfocused
and misaligned with the drivers of new hire quality (Recruiting Roundtable, 2008
Corporate Executive Board). Progress in achieving goals in Human Resource Recruitment
strategies relies on increasing resources and most importantly on managers who are able to
lead and manage teams at all levels of the health system to transform HR Strategies, plans
11
and recommendations into a comprehensive, harmonized approach that is effectively
implemented and sustained (Amref, 2009).
The health sector is labour-intensive and dependant on its workforce for the precise
application of the knowledge and technical skills in the provision of health care services.
Human Resources (HR) in the sector is both a strategic capital and a critical resource for
the performance of the health system. The overall goal is for employment of optimal levels
of human resources and the development of capacity in line with the health needs of the
population (AHWO, 2009). Over the years, organizations and industry have utilized
diverse approaches to select employees. With a dire need for transformation so as to match
environmental dynamics, the trend to use competency-based approaches for assessment,
and development of workers has experienced a significant emergence. Organizations have
turned their focus from skills acquisition and assessment to the competency modeling
process for determining the needs of business and employers. Competency based human
resource management (CBHRM) utilizes the concept of competency analysis to inform and
improve the processes of recruitment and selection as well as performance management
(Armstrong, 2005). Today’s knowledge based operating environment is subject to
accelerating changes, which require efficient and effective recruiting methods to satisfy the
demand of organizations in addition to getting the right employees into the right jobs
(Lindgren et al, 2004). In response to these demands, it’s imperative to have a model that
integrates competencies of persons into the recruitment process.
Currently there are several competency models available in the market which can be used
for enhancing effectiveness of the HR function. These models have been developed by
12
functional experts, academicians and consultants basically to educate people and help them
develop these competencies. For example Ulrich Dave has come out with a Human
resource competency model. The need for more research into the construction of
personality in addition to determinants and consequences of behavior is doubtlessly a
perpetual concern of scholars. The predictive utility of employee assessment is enhanced
when job type and personality constructs are matched, either based on the findings of
previous research, rational analysis, or a thorough personality oriented job analysis
(Raymark, Schmit, & Guion, 1997). Each year, about two hundred doctors and six hundred
nurses exit the service due to poor remuneration and working environment amongst others.
Resignations constitute the highest percentile of attrition. Improving the disciplinary
control is still a challenge due to the poor leadership and management standards especially
given that supervisors are themselves guilty of flaunting ethical standards and engaging in
unprofessional conduct. Absenteeism is quite rampant and occasioned by dual practice
among doctors, part-time employment of health workers on locum basis in private facilities
and unauthorised private practice (African Health Workforce Observatory, 2009)
Accumulated research in academic and applied settings supports the assertion that
personality can be reliably measured and is a valid predictor of job performance for most
tasks. This research has demonstrated that despite the great value they portend,
competency based assessment are yet to be meaningfully exploited within Kenyan
recruitment settings. Therefore given this trend it would be important to conduct a study to
determine the competency based procedures by registered hospitals in Nairobi. This is
critical because each organization requires a tailored & standardized competency
framework and previous studies such as BMC Health Services (Australia) and Amref
13
(2009 have indicated the need for more research on the use of competencies especially in
the recruitment and selection process. However, it is clear that there is also considerable
variation in the understanding and application of the competency approach in health
promotion and related fields. Despite these, past studies have inadequately addressed
competency based recruitment and selection practices. Beside this, no any research on
recruitment and selection is known to have been done in Nairobi. This study therefore
sought to fill the existing gap by investigating the competency based recruitment and
selection practices for hospitals in Nairobi County.
1.3 Research Objective
The research objective was to determine the competency based recruitment and selection
practices by registered hospitals in Kenya.
1.4 Value of the Study
This research study will have various beneficiaries. The information provided can prepare
organizations to face long term strategies and specifically Human Resource recruitment
problems that span entire organizations and command attention of senior managers.
Human Resource professionals mastering competencies can also use the findings of this
study in shaping organizations to deliver productivity gain, increased retention and
improved organizational needs. Human Resource leaders using competencies are able to
track critical organizational challenges relevant to recruitment. Architects of Human
Resource Solutions can use the findings of this paper to transform organizations into
admired centres of excellence. Furthermore, continuing Human Resource students can
utilize this research paper for further insight and research on competencies and
14
recruitment. Overall, competencies have been shown to provide a useful base for health
promotion training, academic preparation, and continuing professional develop.
The study will also be useful to the relevant government authority which rely on it in
development of policy framework for recruitment and selection of personnel in hospital
who are competent for the field they are mandated.
15
CHAPTER TWO
LITERATURE REVIEW
2.1 Meaning and Importance of Competencies
Competency refers to skills or knowledge that leads to superior performance. These are
formed through an individual/organization’s knowledge, skills and abilities and provide a
framework for distinguishing between poor performances through to exceptional
performance. Competencies can apply at organizational, individual, team, and occupational
and functional levels. Competencies are individual abilities or characteristics that are key
to effectiveness in work. Competencies are the characteristics of a manager that lead to the
demonstration of skills and abilities, which result in effective performance within an
organizational area. Competencies have been increasingly used in education and the labor
market since the 1970s, when psychologists suggested the importance of testing for
competency rather than intelligence. As a relatively new concept it has engaged the interest
of academics and practitioners, particularly of those working in professions that have been
affected by technological, organizational or cultural changes. It is accepted that a
competencies approach can be helpful to describe sets of tasks, performances, skills and
abilities in real-life work situations (Meresman et al.2004).
Amatetti and Carnes (2009) articulated a framework where they defined competencies as a
set of related knowledge, skills, attitudes/attributes that are necessary to successfully
perform job duties and responsibilities. Knowledge, in this context, refers to what someone
16
knows (facts, research and principles) and it may be acquired and applied in a variety of
settings, for example, through education and training or in the workplace. Skills are
described as what someone does and the specific proficiencies and techniques that enable
individuals to deliver effective services. Attitudes and attributes are defined as a person’s
perspective and personal qualities which include empathy and support, and attributes are
personal characteristics such as respect and recognition. These definitions highlight that
competencies refer not only to knowledge, but also to skills and attitudes. Core
competency development is widely used in workforce initiatives to identify the essential
elements for effective performance. Characteristics of core competencies are that they
provide a set of unifying principles, are pervasive in all strategies and that they are rare
and/or difficult to imitate (Prahalad and Hamel, 1990). Efforts to expand capacity to meet
the needs of the population are reported as requiring a workforce with sufficient
competencies to address the challenges faced (Ameretti and Cairnes, 2009). Competencies
which are specific to health promotion, therefore, need to be based on the core concepts,
principles and actions of health promotion as articulated in the World Health Organisation
(WHO) declarations.
Core competencies need to be regularly reviewed and updated in response to changes in
contemporary practice, new health needs and policy contexts. In addition, competencies
may also be used as the basis for the development of standards and quality assurance
mechanism, such as the certification of individual practitioners and accreditation of
academic professional preparation programmes (Taub et al., 2009).
17
2.2 Competency Framework
Competency frameworks are a method of describing the underpinning values that shape
and define the culture of an organization. They also provide clear focus to support the
development of staff in order to deliver the best possible services. There are a number of
competencies in each framework. Underneath each is a general description of the
competency, followed by a list of attitudes/behaviours that would indicate competence in
the relevant area. The process of competency development is a lifelong series of doing and
reflecting. As competencies apply to careers as well as jobs, lifelong competency
development is linked with personal development as a management concept. And it
requires a special environment, where the rules are necessary in order to introduce novices,
but people at a more advanced level of competency will systematically break the rules if
the situations require it. This environment is synonymously described using terms such as
learning organization, knowledge creation, self-organizing and empowerment. Within a
specific organization or professional community, professional competency, is frequently
valued. They are usually the same competencies that must be demonstrated in a job
interview. But today there is another way of looking at it: that there are general areas of
occupational competency required to retain a post, or earn a promotion. For all
organizations and communities there is a set of primary tasks that competent people have
to contribute to all the time (Amatetti and Carnes, 2009).
A universal framework for examining health problems and for suggesting courses of action
needed for their solution was proposed and as these ideas were comprehensive they had a
unifying effect, bringing together into one common front: health professionals, health
18
services, the scientific community, educational system, governments (municipal,
provincial, federal), business sector, trade unions, voluntary organisations and the
Canadian people. The Lalonde report was very influential internationally and it has been
claimed, laid the foundations for the development of the Ottawa Charter, which was
published by the WHO in 1986. Health promotion is viewed as not only the responsibility
of the health sector, but goes beyond healthy lifestyles to well-being. Health promotion,
therefore, represents a comprehensive social and political process, which not only
embraces actions directed at strengthening the skills and capabilities of individuals, but
also action directed towards changing social, environmental and economic conditions so as
to alleviate their impact on public and individual health (WHO, 1986).
Five key action areas are identified for improving the health of populations (WHO, 1986;
Kicksusch, 2003). These actions include building a healthy public policy, creating
supportive environments by embracing the socio-ecological approach to health where the
societies in which people live and work must be able to support healthy choices in order
for people to achieve health, strengthening community action by empowering and enabling
communities to improve their health by becoming involved in setting priorities, making
decisions, planning strategies and implementing them to achieve better health ,developing
personal skills and enhancing life skills and finally by reorienting the health services
through a shared responsibility by individuals, community groups, health professionals,
health service institutions and governments.
19
2.3 Recruitment and Selection Practices
Recruitment and selection practices form a core part of the central activities underlying
human resource management: namely, the acquisition, development and reward of
workers. It frequently forms an important part of the work of human resource managers –
or designated specialists within work organizations. However, and importantly,
recruitment and selection practices are often for good reason taken by non-specialists, by
the line managers. There is, therefore, an important sense in which it is the responsibility
of all managers, and where human resource departments exist, it may be that HR managers
play more of a supporting advisory role to those people who will supervise or in other
ways work with the new employee.
As Mullins (2010) notes: ‘If the HRM function is to remain effective, there must be
consistently good levels of teamwork, plus ongoing co-operation and consultation between
line managers and the HR manager.’ This is most definitely the case in recruitment and
selection as specialist HR managers (or even external consultants) can be an important
repository of up-to-date knowledge and skills, for example on the important legal
dimensions of this area. Recruitment and selection is often presented as a planned rational
activity, comprising certain sequentially-linked phases within a process of employee
resourcing, which itself may be located within a wider HR management strategy (Bratton
and Gold 2007).
According to Mullins (2010), some of the common benchmark competency-based
practices in Recruitment and Selection include:
20
Notices of job requirements - A template is developed to define how competencies will be
reflected in .notices regarding the requirements of jobs to be filled. As the competency
profiles are completed, sample notices are developed for the varied types of jobs/ roles. .
Interview and Reference Checking Guides - Template interview and reference checking
guides are developed for varied types of jobs/ roles, including instructions and rating
guides. These are made available to hiring managers and HR Advisors.
Template Interview and Reference Checking Guides - Template interview and reference
checking guides are developed for roles/career streams and levels within Occupational
Groups including instructions and rating guides. These are made available to hiring
managers and HR Advisors.
Competency-based Track Record / Portfolio Reviews - Track record / portfolio reviews
allow employees / applicants to document their past experiences and accomplishments that
relate to the competency requirements for positions within the organization. Once
completed, trained evaluators score the extent to which the required competencies are
demonstrated in the written examples using standardized scoring criteria. Typically, the
candidate / employee also provides references who can attest to the validity of the
examples provided. Results can be used as part of the staffing process and / or for other
purposes (e.g., competency gap analysis for Learning and Development; Succession
Management; HR Planning).
Other Competency-based Assessment Methodologies - A variety of other competency-
based assessment methodologies can be incorporated into the selection process, including
21
In-basket assessments, role plays or simulations of workplace situations that the employee
will encounter, multi-source input (as appropriate), etc. When designing and implementing
any methodology, it is important that it be defensible (i.e., reliable, fair, valid and
unbiased).
Training on Competency-based Selection - Managers must have the knowledge and skills
to be able to apply the various competency-based assessment methodologies noted above
to arrive at valid selection decisions. Likewise, employees must be able to participate
effectively to provide an accurate picture of the competencies they possess. Finally, both
managers and HR professionals must be able to establish selection processes that are both
efficient and effective (i.e., reliable, fair, valid and unbiased). All of this requires targeted
training / orientation programs to ensure that all stakeholders have the necessary skills.
2.4 Competencies and changing perspectives on HRM
Baruch (1998) highlights the short-comings of traditional ‘hard’ approaches to HRM
where the emphasis is on making the best use of resources (including human resources)
and aligning Human Resource strategies with business plans. Baruch argues that this
approach to Human Resource Management uses and involves people as passive actors. By
contrast, the soft approach emphasises that people are one of the key factors involved in
whether or not an organisation can deliver, and that HRM must unleash the potential that
every individual can make to the organisation. Thus the soft approach emphasises people
as a valued asset, as proactive actors who can be trusted and who should be developed. It
emphasises participation and empowerment and expects that in return for truly
22
demonstrated leadership and commitment to people, people will demonstrate true
commitment and loyalty to the organisation. While the hard and soft approaches are not
mutually exclusive, Baruch suggests that it is the soft approach that has the potential to
provide the leverage to move organisations forward, to change-enable them and to provide
competitive advantage. In this light Horton (2000) suggests that competency-based
management represents a cultural change towards greater employee self-direction and
responsibility in the search for excellence rather than standard performance.
Hartle (1995) suggests that it is not just the organisation but also the individual who stands
to benefit from the competency-based approach. The organisation benefits from better
planning, better communications, improved managerial capabilities an empowered
workforce, focused development planning, better value for money, and improved
performance at all levels. Similarly the benefits for individuals can include clarity about
what they are required to do, better dialogue with managers and colleagues, better quality
management, feedback and support, more freedom to decide on the what and how of
performance, a structured framework for developing performance and potential, better
recognition for doing good work and an opportunity to meet expected performance in a
structured and consistent way.
Within competency-based HRM, Hondeghem and Vandermeulen (2000) suggest that there
are three possible roles for the HR function. The first is the customer service model, where
HR managers serve line managers as customers. The second is the organisational
development or consultancy model, where the HR officer functions as an internal
consultant to the line manager on a range of organisational issues. The third model is the
23
strategic HRM model, where HR managers act as full members of the strategic
management team, linking HR policy to agency mission, goals and policy.
2.5 An integrated approach to HRM – the role of competencies
The development of an effective competencies framework can provide opportunities for
individual and organisational growth and, in the longer term, can enhance the success of an
organisation. More specifically, when used effectively competency-based approaches can
act as a powerful development and motivational tool for staff.
Research carried out in the UK in 1994 ( Garavan et al, 1995) highlights a range of
motives for the introduction of competencies. Interestingly, while the most common reason
for the introduction of competencies was to improve performance, the numbers who did so
for recruitment and training and development purposes are also significant. In a study
carried out by the Hay Group ( HR Focus, 1996) of competency practices in 217
companies, it was found that ninety per cent of companies used competency-based
appraisal for employee development purposes, while eightyeight per cent used them to
make selection or hiring decisions. This study also showed that almost twenty five percent
of the companies surveyed had competency based pay systems in place. Research cited by
Pickett (1998) also highlights employee development and recruitment and selection needs
as common motives for the introduction of competencies. The potential role of
competencies in achieving an integrated approach has been highlighted by Klein (1996)-
Competencies align and integrate all HR systems if the behavioural standards of excellent
24
performers become the foundation for recruitment, selection, pay, performance
management, promotions and development.
Armstrong (1997) stresses that competencies lie at the heart of Human resource
Management since they are directly linked to a fundamental aim of strategic Human
Resource Management – to obtain and develop highly competent people who will readily
achieve their objectives and thus maximise their contribution to the attainment of the goals
of the enterprise. He suggests that a competence framework can provide an invaluable
basis for integrating key Human resource Management activities and achieving a coherent
approach to the management of employees.
Similarly, Mirabile (1997) argues that while competency models provide potentially
valuable information, they will be useless if they are not promoted using a coherent and
systematic implementation strategy, supported by appropriate structures and processes
including HR systems. For example, if identified competencies are not linked to the
performance management system, or if different criteria are used to select or promote
people, confused signals will be sent out to employees as to what really matters in terms of
behaviour and performance.
2.6 Methodologies for developing competencies
A literature review is the most commonly used starting point (McCracken et al., 2000;
Health Scotland, 2003; Shilton et al., 2003, 2005; Moloughney, 2006 and Melville et al.,
2006). A literature review will inform the researcher not only on the approaches used in
relation to developing the competencies but can also give important information on the
25
health promotion workforce and setting. This is important as countries with similar
systems can benefit from flaws highlighted or gaps identified in previous studies. In
addition, a literature review will add to the theory base and enhance the understanding and
knowledge of the field of competency development. Finally the information gathered from
the literature review can provide a focus and starting point and guide in the development
phase of similar projects.
An alternative is to carry out an information gathering exercise. The purpose of this is to
focus on what actually happens in practice. This activity can be carried using a number of
methods but involves some sort of consultation.This can also include observing or
interviewing or an exemplary practitioner to identify the actions, content and context
involved in their exemplary practice (Centre for Health Policy, 2008).Other initiatives
undertook surveys of a representative sample of practicing professionals to determine what
they actually do in practice as they did in Scotland and the US (Health Scotland, 2003,
Gilmore et al., 2005).
Mapping exercises have also been used (Meresman, 2004; Health Scotland, 2003) where
mapping the domains and competencies can help identify what is considered to be core in
other settings. Functional analysis is also used in developing competencies (Skills for
Health, 2001, 2004). Functional analysis can be used to try and explain a recurrent activity
or behaviour pattern in individuals or groups. It can seek to understand how a socio
cultural institution works in terms or its roles or tasks (Hempel, 2001). This process
involves identifying the core functions of a group or organisation. Then these functions are
used to form a map and then key tasks are identified. However, functional analysis has
26
been criticised as being overly reductionist because there is too much focus on task, and on
how tasks should be undertaken, to allow what has been described as the artistry of health
promotion (Mendoza, et al., 1994).
Consensus building using the Delphi technique is commonly used (Howatt et al., 2000;
Shilton et al., 2003, 2005; Hyndman, 2009). The Delphi method, is an attempt to obtain
expert opinion and information in a systematic manner where participants are polled
individually usually with a self-administered questionnaire (Fink et al., 1984). This is a
multi-stage process where each stage builds on the results of the previous stage The survey
is conducted over a few rounds and after each one, the results are elicited, analysed and
then reported back to the group. It is an iterative process with the aim of using expert
opinion to reach consensus. A Delphi is considered complete when there is a convergence
of opinion or when a point of diminishing returns is reached (Fink et al., 1984). The Delphi
technique, although frequently used, has been criticised as it is suggested that it reduces
competencies to a meaningless middle ground and that the political aspects of health
promotion can be lost in the move towards the centre (Mendoza, 1994).
All consultations whether they are Delphi, think tanks or focus groups, will use multiple
rounds of consultation to ensure the widest scope of feedback possible. The feedback from
the consultation process is then analysed and this is used to prepare a final draft of the
competencies which can then be disseminated and ratified. However, as Moloughney
(2006) states, competency set development is an iterative process and it may be necessary
to cycle through some of these steps a few times. Even when a final draft set is produced, it
is really only a working draft that will need to be periodically reviewed and revised as
27
experience with the competencies accumulates and the field itself evolves. It is generally
agreed in the literature that competencies are more likely to be seen as appropriate and
valid if they are developed from the bottom up with the close involvement of the
professionals who have to demonstrate competence on a daily basis in their work (Birt and
Foldspang, 2009). However, it can also be argued that, by basing competencies on practice
as described and defined by practitioners, what is reflected is not necessarily best or
evidence-based practice but rather what is commonly done (Battel-Kirk et al., 2009).
There are also limitations in using current practice (or what might be termed ‘past’ practice
given that the development of competencies is a slow process) as the basis for
competencies, particularly if they are to be used in future planning.( Prastacos et al 2005)
for example, indicates that, in the business environment, competencies are often backward-
looking and recommend the use of a forward-looking development model which takes
cognisance of the context and the current trends within which the organisation operates. A
strategic approach that looks to the future as well as current practice when developing
health promotion competencies (Shilton et al.2001) and the importance of grounding
competencies in current policy has also been highlighted (Health Scotland, 2003). For this
reason the development of agreed upon lists of competencies has to be the result of a
repeated and continuing process, characterised by interaction between the main
stakeholders across the academic, practice and policy areas. It is not a purely academic
exercise, neither for that matter a purely practical or political endeavour, accordingly it is
necessary to develop a strongly communicative culture, with consensus building processes
in focus (Birt and Foldspang, 2009).
28
2.6 Criticisms on Competency Frameworks
The Chartered Institute of Personnel and Development in the UK (CIPD) includes the
following as the common criticisms of competency frameworks; they capture the past and
are therefore out of date, they cannot keep up to date with the fast changing world, they
were introduced to improve performance and they have not done so, they are unwieldy and
not user friendly- they create clones; everyone is expected to behave in the same way. The
publication while acknowledging the validity of these criticisms, also notes that they have
been levelled with justification mainly at frameworks produced using poor practice and
highlights the need for care and understanding when developing and implementing
competency frameworks.
A major criticism of the competency approach, particularly in relation to professional
practice, which has already been noted in relation to health promotion (Shilton, 2001) is
that it may be overly prescriptive and can, therefore, limit intuition, creativity and
innovation. For example, Talbot (2004) suggests that the competencies approach has a
tendency to limit the reflection, intuition, experience and higher order competence
necessary for expert, holistic or well developed practice. Talbot (2004) also argues that a
reductionist tendency, which focuses on tasks and outcomes inherent in the approach,
ignores the complex processes needed for professional practice.
Lester notes that this approach has been extensively criticised for weaknesses in its ability
to represent occupations which are characterised by a high degree of uncertainty,
unpredictability and discretion, and its tendency to atomise work roles rather than represent
29
them holistically (Lester, 1994). The competency approach has also been criticised as
being overly universalistic (Bolden and Gosling 2004; Mendoza et al.1994). There is
discussion in the literature of the fact that there can be an assumption that competencies
and standards are equally relevant to all practitioners in all settings and situations, an
assumption that is, it is suggested, obviously incorrect. This again has resonance for health
promotion, which is practiced at different levels, by people from different backgrounds and
in a wide variety of settings. The concept of equifinality (Berttalanffy, 1968), which argues
that there can be many different and valid origins for a given outcome, can be related to the
context of practice, meaning that many different behaviours on the part of the practitioner
may lead to competent outcomes.
This broader interpretation of competencies should inform both the development and the
implementation of competencies. The challenge of establishing competency frameworks,
therefore, includes addressing the complexity of practice in a manner which is meaningful
and clear while also leaving room for the many varied paths possible in successful practice.
There is a need, therefore, to consider how core competencies will be expressed to be
meaningful, useable, relevant and succinct. ‘”What is needed is a set of commonalities
underlying the actions, with the recognition that specific actions will and should vary
depending on the context of practice” (Miller et al., 2010). It is important when
considering the potentially negative aspects of the competency approach and the
difficulties in the development, implementation and revision process to view this in
balance with the many listed positive aspects of competencies which include ( Shilton et
al., 2001) usefulness as a shared/agreed language for defining boundaries of profession and
the tasks, skills and knowledge required for adequate practice, helpfulness in developing
30
programmes and projects, curriculum development and in recruitment and selection
,contribution to defining/defending discipline.
31
CHAPTER THREE
RESEARCH METHODOLOGY
3.1 Introduction
This chapter discusses the research methodology for the study including the research
design, target population and sample design. In addition, data collection instruments and
procedures as well as the data analysis are elaborated in this chapter.
3.1 Research Design
This study was descriptive in nature. This design is preferred because it permits
comparative analysis.
3.2 Target Population
The researcher targeted all registerd hospitals in Nairobi. According to Kenya Medical
Association directory (2012), there are 60 registered hospitals in Nairobi. The list of
hospitals is attached as Appendix II.
3.3 Sampling Design
A sample size of forty hospitals was selected .This number is well above the generally
accepted minimum of thirty. It is also large enough to give room for possible non response.
Simple random technique was used to select the sample. The selected sample is attached as
Appendix III.
32
3.4 Data Collection
Primary data was collected. This was used to address competency based recruitment and
selection practices. The questionnaire was divided into two parts A and B. Part A
addressed the respondent firms’ profiles while part B will capture data on competency
based recruitment. The questionnaire was administered to the officer in charge of the
human resource function at each hospital.
3.5 Data Analysis
Data collected from respondents was both quantitative and qualitative in nature.
Quantitative data will be analyzed using the descriptive statistics such as mean scores and
standard deviations. The findings were then presented using tables, pie charts, and bar
graphs for easier interpretation. On the other hand, qualitative data was analyzed using
content analysis. The qualitative information was used to interpret or better understand
quantitative findings.
33
CHAPTER FOUR
FINDINGS, ANALYSIS AND INTERPRETATION
4.1 Introduction
This chapter presents data analysis, findings, interpretation and presentation. Data was
analyzed using descriptive tools where frequencies, percentages were used to interpret the
findings. The purpose of this study was to determine competency based recruitment and
selection practices by registered hospitals in Nairobi County.
4.2 Demographic Data
Table 4.1: Distribution of respondents by gender
Frequency Percent
Male 22 57.9
Female 16 42.1
Total 38 100.1
As shown in Table 4.2, majority of the respondents (57.9 percent) were male while 42.1
percent were female. This implies that majority of the officers in charge of the Human
Resource Function were male.
34
Figure 4.1: Distribution of respondents by age bracket
Findings presented in Figure 4.1 show that a vast majority of the respondents (68.4
percent) were below 30 years, 26.3 percent were between 30-40 years while the remaining
2.6 percent and 2.6 percent were between 41-50 and over 50 years respectively. This
suggests that majority of the Human Resource Officers in registered hospitals in Nairobi
County are below the age of 30 years. This is good for hospital because this category of
people are young, energetic and flexible enough to cope with a fast paced working
environment that is typical of institutions of this nature..
35
4.3 Factors considered in recruiting new staff
Table 4.2: The extent to which various factors are considered in recruiting new staff
Factor Mean Standard deviation
A staff with strategic thought 3.7 0.7
Good understanding of Organisation 3.3 0.8
Innovative Person 3.9 0.8
Effective and fluent communication 4.3 1.1
Good customer focus and public relations 4.3 0.9
Leadership abilities 3.7 0.9
Ability for teamwork 4.1 0.8
Ability for time management 4.4 0.6
Regarding the extent to which various factors are considered in recruiting new employees,
the respondents said that good customer relations is an important factor to consider with a
mean of 4.3 out of 5 (see table 4.2). Effective and fluent communication together with
good customer focus and public relations are also considered as important with a mean of
4.3 each. Ability for teamwork is also not overlooked when recruiting new staff. It had a
mean of 4.1. The ability to be innovative attained a mean of 3.9.
Other factors considered include leadership abilities and having strategic thought. These
two factors are equally considered with a mean of 3.7. The findings implied that the most
important factor to be considered when undertaking competence based recruitment and
selection was the ability to manage time well. Proper time management is an important
36
factor to be considered in hospitals because it enables one meet set objectives within
stipulated time.
As Gough and price (2004) note, appropriate programmes based on the personal needs and
experiences of health managers can then be put in place to train managers to provide
leadership and to ensure a sustainable improvement in the work context of health workers,
and hence on the quality of care and health of the communities their organizations serve
(Gough and Price 2004).
4.4 Interpersonal relations
Table 4.3: Mean and standard deviation for the measures interpersonal relations
Mean
Standard
deviation
Demonstrates trust, sensitivity and mutual respect 4.2 0.7
Recognizes the contrubutions diversity brings to job
performance and creativity 3.9 0.7
Demonstrates altruistic empathy 4.1 0.9
As shown in Table 4.3, majority of the respondents felt that a new recruit who
demonstrated trust, sensitivity and mutual respect was great. It had mean of 4.2 out of 5
while the competency aspect related to diversity in job performance had a mean of 4.1,
which is relatively high. The use of altruistic empathy scored a mean of 4.1. That
registered hospitals in Nairobi have embraced this aspect of interpersonal relations.
Frequent disagreements and lack for respect to one another by workers, especially those
within the same department bring about inefficiency which in turn threatens the very
37
survival of the organization. Hamel and Prahalad (1990) defined core competence as the
collective learning in the organisation, especially how to co-ordinate diverse production
skills and integrate multiple streams of technologies.
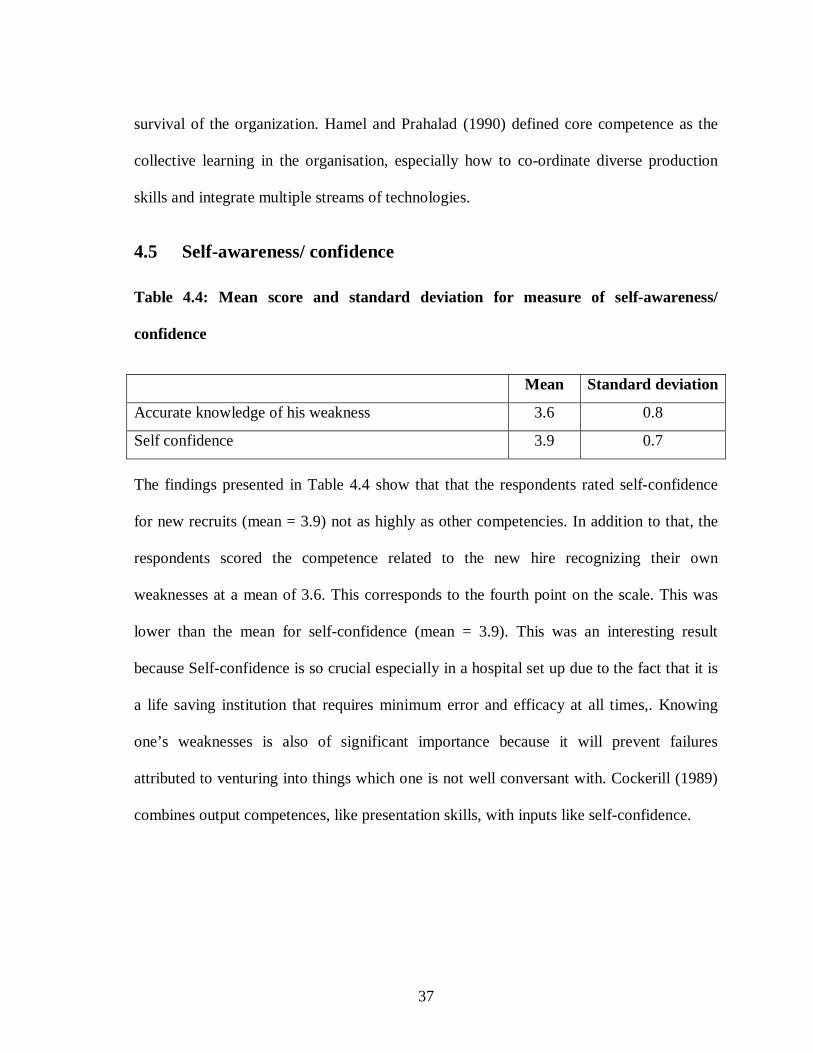
4.5 Self-awareness/ confidence
Table 4.4: Mean score and standard deviation for measure of self-awareness/
confidence
Mean Standard deviation
Accurate knowledge of his weakness 3.6 0.8
Self confidence 3.9 0.7
The findings presented in Table 4.4 show that that the respondents rated self-confidence
for new recruits (mean = 3.9) not as highly as other competencies. In addition to that, the
respondents scored the competence related to the new hire recognizing their own
weaknesses at a mean of 3.6. This corresponds to the fourth point on the scale. This was
lower than the mean for self-confidence (mean = 3.9). This was an interesting result
because Self-confidence is so crucial especially in a hospital set up due to the fact that it is
a life saving institution that requires minimum error and efficacy at all times,. Knowing
one’s weaknesses is also of significant importance because it will prevent failures
attributed to venturing into things which one is not well conversant with. Cockerill (1989)
combines output competences, like presentation skills, with inputs like self-confidence.
38
4.6 Analytical thinking
Table 4.5: Mean and standard deviaitions for the measure of analytical thinking
Mean Standard deviation
Information gathering skills 3.7 0.6
Use of range of resources 3.4 0.6
Looking beyond routinely explanations of organizational
performance 3.7 0.8
Good in decisionmaking 4.4 0.9
The researcher was also concerned with whether the respondents applied analytical
thinking in their work. The results are presented in Table 4.5, majority of the respondents
felt like the competence aspect related to good decision making was of most importance to
them in the recruitment and selection process and scored a high mean of 4.4. The
respondents also felt that when undertaking the recruiting and selection of staff the
competences related to the ability to collect and gather information in relation to the
respective departments was a consideration. This had a mean of 3.7. However this was
relatively lower than the competence related to decision making (mean = 4.4). In addition
to that, the respondents gave a fair amount of consideration to a new hire who had the
ability to think outside the box and use multiple sources when undertaking their work
roles. This aspect of analytical thinking had given a mean of 3.7. The above tabulation
shows that the most highly valued aspect of analytical thinking considered by the Human
Resource Officers from registered hospitals in Nairobi County when undertaking their
recruitment and selection of staff was a candidate who had the skills and ability to make
39
sound decisions in their work duties. The ability to make good and independent decisions
is important especially in a hospital environment.
4.7 Adaptability/flexibility
Table 4.6: Mean scores and standard deviations for measures of
adaptability/flexibility
Mean Standard deviation
Ability to adapt to styles and shift gears 3.8 0.8
Shows evidence of coping skills 3.9 0.8
Comfortable with new ideas and open to new information 4.1 1.0
Findings on adaptability and flexibility showed that many respondents were keen on
recruiting individuals who demonstrated the ability to bring new ideas and readily accept
changes that occur within organizations. As indicated in Table 4.7, innovative individuals
were considered as valuable assets to their institutions and they gave a high mean of 4.1.
The respondents also indicated that an individual who demonstorates that they are able to
cope with their work load,work times and their peers in general was something they were
on the look out for in the recruitment and selection process and gave. This measure
received a score of 3.9..
40
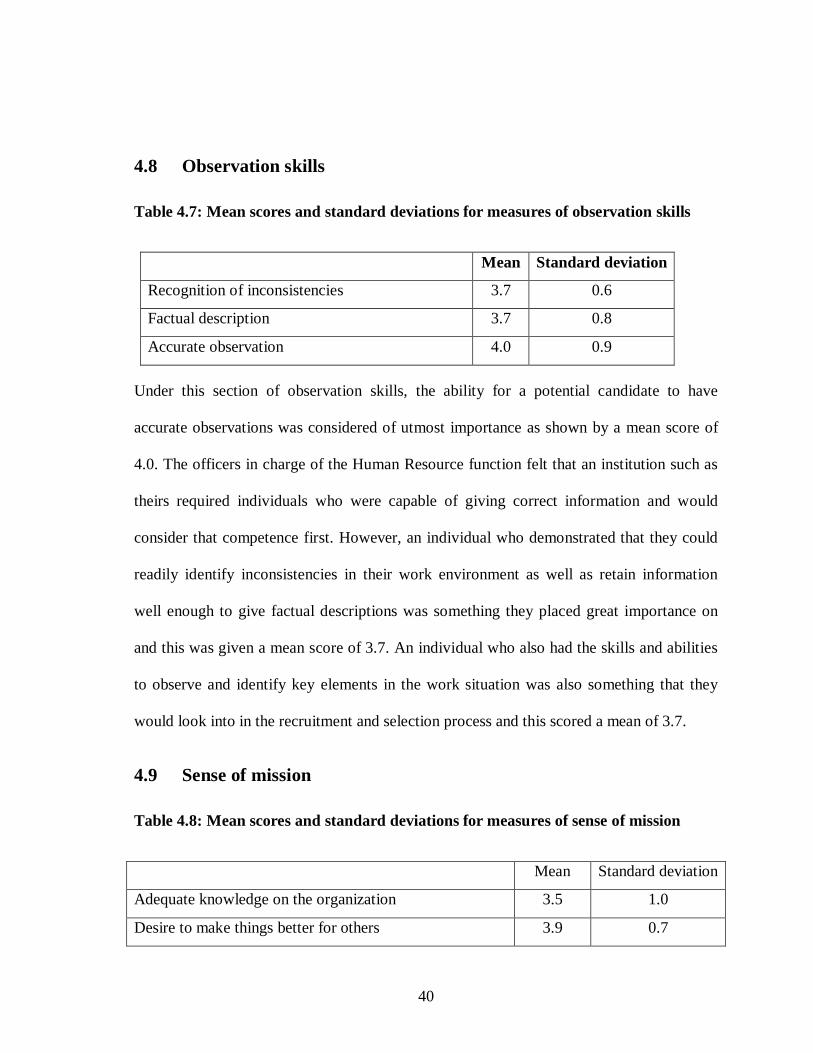
4.8 Observation skills
Table 4.7: Mean scores and standard deviations for measures of observation skills
Mean Standard deviation
Recognition of inconsistencies 3.7 0.6
Factual description 3.7 0.8
Accurate observation 4.0 0.9
Under this section of observation skills, the ability for a potential candidate to have
accurate observations was considered of utmost importance as shown by a mean score of
4.0. The officers in charge of the Human Resource function felt that an institution such as
theirs required individuals who were capable of giving correct information and would
consider that competence first. However, an individual who demonstrated that they could
readily identify inconsistencies in their work environment as well as retain information
well enough to give factual descriptions was something they placed great importance on
and this was given a mean score of 3.7. An individual who also had the skills and abilities
to observe and identify key elements in the work situation was also something that they
would look into in the recruitment and selection process and this scored a mean of 3.7.
4.9 Sense of mission
Table 4.8: Mean scores and standard deviations for measures of sense of mission
Mean Standard deviation
Adequate knowledge on the organization 3.5 1.0
Desire to make things better for others 3.9 0.7
41
The results from the findings in Table 4.1 show that the Human Resource Officers were
flexible when it came to a potential hire that may not have adequate knowledge of the
organization because they could learn more about the organization once they were
recruited. Because of this they gave a mean score of 3.5. However they felt that a potential
new hire who not only wanted to improve their own performance but also wanted to
improve performance of their workmates and thus improving the performance of the
institution as a whole, was one they would consider greatly in the recruitment and selection
process. This was given a mean score of 3.9.
4.10 Communication skills
Table 4.9: Mean scores and standard deviations for measures of communication skills
Mean Standard deviation
Speaks clearly and expresses self well 4.1 0.9
Demonstrates attentive listening 4.0 0.9
Conveys information 3.9 1.0
Communication is one of the aspects that is critical in many organizations especially the
service industry. As depicted in Table 4.9, the respondents felt that an individual who
demonstrates the ability to speak well and clearly was of utmost importance to them and
gave a high mean score of 4.1. However, all aspects of communication were also
considered important when looking for a new recruit and consequently high mean scores
were given to individuals who were good listeners and who were able to convey
information efficiently and effectively. The mean scores given were 4.0 and 3.9
respectively. This goes to show that the respondents felt that a potential new hire who had
42
good communication skills would be greatly considered and have an edge over other
potential candidates.
4.11 Motivation
Table 4.10: Mean scores and standard deviations for measures of motivation
Mean Standard deviation
Commitment to organizational goals 4.2 0.8
Strive to achieve/improve 4.2 0.7
Sets high standards of performance 4.1 0.7
Disaplay high level of effort and commitment
towards performing the work 4.1 0.8
Optimism/ persistence in pursuing goals 4.2 0.8
It is clear from the results in Table 4.9 that the respondents in the various hospitals felt that
whenever they were undertaking the recruitment and selection exercise, they would be
looking for an individual who was highly motivated. They scored all aspects of motivation
generously. An individual who was committed to their institutions, who was result driven
and constantly wanted to improve was someone who they were keen to recruit and they
gave a mean score of 4.2. In addition, the respondents also felt that an individual who set
high standards of performance in their work roles and displayed commitment in their work
duties- be it working overtime or doing the job right the first time would be considered a
good fit for their institutions and gave a high score of 4.1. Commitment, persistence and
desire to achieve are very important inputs to any organization. If the organization gets to a
level where everyone is committed and moves ahead with persistence this will make
achievement of set goals and objectives easier. Hartle argues that competency is a
43
characteristic of an individual that has been shown to drive superior job performance
(1995) includes both visible competencies of knowledge and skills and underlying
elements of competencies like traits and motives.
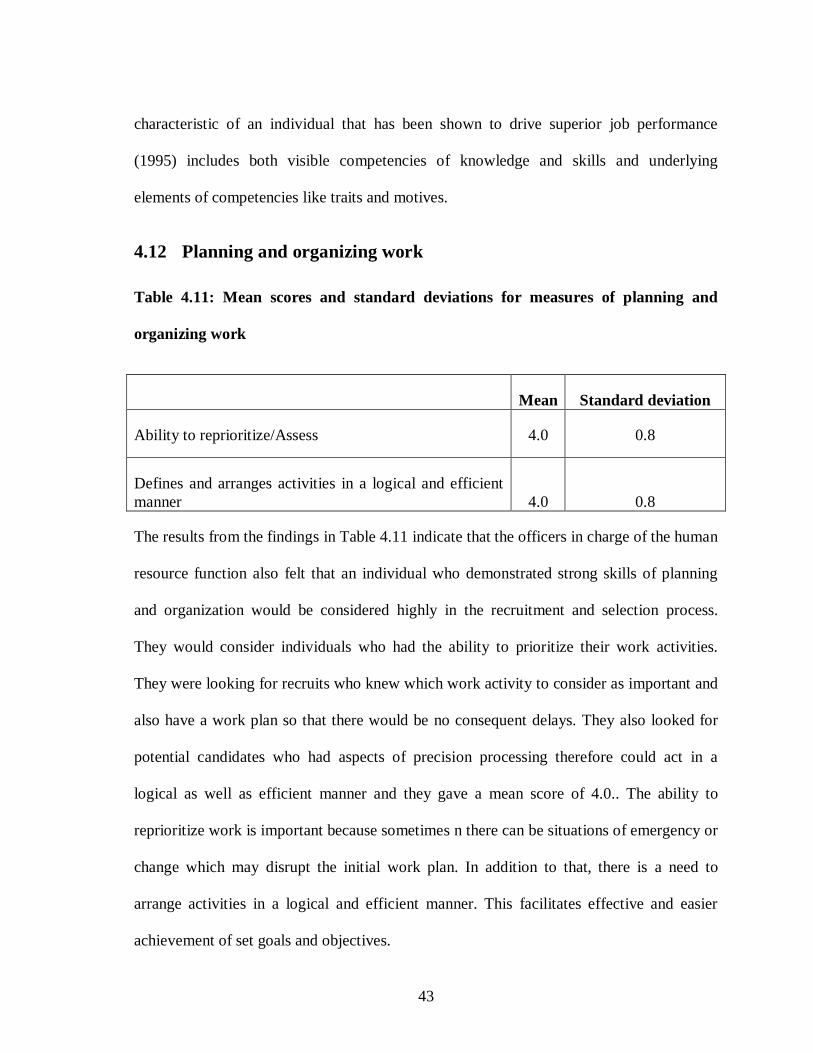
4.12 Planning and organizing work
Table 4.11: Mean scores and standard deviations for measures of planning and
organizing work
Mean Standard deviation
Ability to reprioritize/Assess 4.0 0.8
Defines and arranges activities in a logical and efficient manner 4.0 0.8
The results from the findings in Table 4.11 indicate that the officers in charge of the human
resource function also felt that an individual who demonstrated strong skills of planning
and organization would be considered highly in the recruitment and selection process.
They would consider individuals who had the ability to prioritize their work activities.
They were looking for recruits who knew which work activity to consider as important and
also have a work plan so that there would be no consequent delays. They also looked for
potential candidates who had aspects of precision processing therefore could act in a
logical as well as efficient manner and they gave a mean score of 4.0.. The ability to
reprioritize work is important because sometimes n there can be situations of emergency or
change which may disrupt the initial work plan. In addition to that, there is a need to
arrange activities in a logical and efficient manner. This facilitates effective and easier
achievement of set goals and objectives.
44
4.13 Teamwork
Table 4.12: Mean scores and standard deviations for measures of teamwork
Mean Standard deviation
Contributes to organizational goals 4.3 0.6
Fosters collaboration among team members as part of teamwork 3.9 0.8
The researcher also wanted to find out whether teamwork contributed to organizational
goals. The findings in Table 4.12 confirmed that the virtue of teamwork did contribute to
organizational goals. This had a mean score of 4.3 with respects to individuals who were
willing to contribute their current skills and abilities for the improvement of the institutions
goals and objectives. At the same time, collaboration among team members as part of
teamwork was expressed as imperative for a fully employment of competency based
recruitment and selection with mean of 3.9. The respondents further reiterated that when
conducting the recruitment and selection process they would be looking for a potential
recruit who apart from utilizing their skills to contribute to organizational goals, would be
able to work well with their peers through good relations and collaboration. The
respondents gave a mean score of 4.3. This high score indicates that the Human Resource
personnel in hospitals in Nairobi county value individuals who display these kind of
competencies in order for the institutions to run smoothly. Mullins (2010) notes that the
HRM function is to remain effective; there must be consistently good levels of teamwork,
plus ongoing co-operation and consultation between line managers and the HR manager.
45
CHAPTER FIVE
SUMMARY, DISCUSSION, CONCLUSIONS AND
RECOMMENDATIONS
5.1 Introduction
This chapter presents the summary of findings, conclusions and recommendations. The
chapter also give suggestions for further studies
5.2 Summary of findings
This study used descriptive survey to investigate competency based recruitment practices
by registered hospitals in Nairobi.. The target respondents were selected registered
hospitals in Nairobi County. Majority of the respondents (57.89 percent) were male while
42.12 percent were female.
Findings on the age of respondents showed that a vast majority of the respondents (68.4
percent) were below 30 years, 26.3 percent were between 30-40 years while the rest2.6 and
2.6 percent were between 41-50 and over 50 years respectively
Regarding the extent to which various factors are considered in recruiting new members,
the respondents said that good customer relations is an important factor to consider with a
mean of 4.4. Effective and fluent communication together with good customer focus and
public relations are also importantly considered with a mean of 4.3 each. Ability for
teamwork is not also overlooked when recruiting new members. It is considered with a
mean of 4.3. A person who is innovative is also taken into consideration with a mean of
46
3.9. Other factors considered include leadership abilities and having a strategic thought.
These two factors are equally considered with a mean of 3.7.The findings also indicated
that having a good understanding of the organization was also a consideration when
recruiting new members.
Concerning interpersonal relations, majority of the respondents demonstrated trust,
sensitivity and mutual respect with a mean of 4.2 while others recognized the contributions
diversity brings to job performance and creativity with a mean of 4.1, At the same time,
some respondents demonstrated altruistic empathy. On whether the respondents have self-
awareness and confidence, it was evident from the findings that many respondents
considered self-confidence as an important factor in the recruitment and selection process
and gave a mean of 3.9. In addition to that, they were looking for an individual who had
accurate knowledge of their weaknesses but was not deemed as important as some of the
other competencies and thus gave a mean score of 3.6 With regard to whether the
respondents were looking for an individual who applied analytical thinking in their work,
the aspect of a potential hire who had good decision making skills scored the highest with
a mean score of 4.4.However individuals who displayed characteristics of having the
ability to gather information systematically and have vision were also given relatively
good mean scores of 3.7.
Findings on competency aspects of tadaptability and flexibility showed that many
respondents were comfortable with potential candidates who were willing to bring in new
ideas and who were open to new information or changes that come up in the work
situation. For example introduction of Information technology systems that could improve
47
the work situation in order to achieve organizational goals. The mean score was a
favourable 4.1..In addition the respondents emphasizedthe importance of looking for an
individual who had good coping skills.This was considered in the recruitment and selection
process and the mean score awarded for this was a4.0. Concerning competencies related to
observation skills, majority of the respondents said that they put great consideration for a
potential new hire who had a strong command of accuracy and this was given a high score
of 4.0.In addition a potential hire was also required to exhibit skills relation to identifying
inconsistencies as well as being able to be factual at all times. They gave a mean score for
3.7 for the two.
The researcher also wanted to know whether there was a sense of mission among the
respondents. From the findings, majority of the respondents indicated that in their
recruitment and selection process they were looking for individuals who possessed the
desire to make things better for others with whom they were working with and not just
their own individual progress in the organization. This was a necessity because in order for
the organization to improve and meet its said objectives growth was required at the
individual level as well as the organizational level.. The respondent also indicated that they
were looking for individuals with good communication skills. The service industry heavily
relies on its human resource to keep the organization running.
Hence having employees with good communication skills was of paramount importance to
them.Emphasis was placed on recruiting individuals who had the ability to express
themselves well, were good listeners and could convey information to the recipients
efficiently and effectively. The mean scores had highs of 4.1. The respondents were also
48
looking for individuals who were highly motivated and this also included self motivation.
A hospital, being a 24 hour institution has long working hours midnight shifts as well as
patients coming with different levels of sickness from minor to major hence they would
always look for a potential candidate who would be able to motivate themselves under
such working conditions. The respondents gave a mean score of 4.2 for all the
characteristics that entail motivation. These include commitment to the hospital, result
driven, and perseverance among other characteristics. There was also great emphasis in the
recruitment and selection process for looking for an individual who had good planning and
organizing skills. They were looking for individuals who knew how to use tools of
management for the betterment of the organization to speed up their work duties in an
effective manner. They also wanted individuals who were able to prioritize their specific
workloads to maximize on efficiency and who did this in a logical and systematic manner.
They gave a mean score of 4.0.
The researcher also wanted to find whether teamwork contributed to organizational goals
and respondents confirmed that teamwork contributed to organizational goals because
hospitals operate in a time sensitive environment and all employees need to work well
together because all departments heavily rely on each other to ensure that patients have the
best care and attention and have a smooth transition from point of entry with the nurse,
then the doctor and payment section. This had a mean score of 4.3
49
5.3 Conclusions
This study was carried out with the objective of determining the competency based
recruitment and selection practices adopted by registered hospitals in Nairobi. It can be
concluded that the results from the findings of the questionaire demonstrated that
competency based recruitment procedures were paramount in selecting new hires. The
respondents recognized that competency based recruitment procedures can work hand in
hand with traditional recruitment and selection procedures. The competency based
approach to recruitment and selection was considered important in the recruitment and
selection stage of Human Resource Management processes.
The research also found that adopting a competency based recruitment and selection
system is a results oriented process. It makes it easier to concentrate on the results expected
of a successful or exemplary performer (Guinn, 1998). In addition the competency based
recruitment and selection technique gave the recruitment staff the opportunity to focus less
attention on approximations of competence such as educational level or years of
experience that have little connection to verifiable results. Also competency-based
recruitment plays an important role in attracting individuals who possess characteristics
that might be difficult, if not impossible, to acquire by training or development efforts. A
competency based approach encourages managers and other decision makers to clarify the
verifiable, measurable results they expect from successful performers before a selection
decision is made.
Competency-based selection, according to the respondents provides some insight into
whether or not a new hire will be a good fit with the institutions culture. A competency-
50
based recruitment and selection process provides applicants with opportunities to outline,
explain, and demonstrate their qualifications in competency-based terms. Potential
candidates will not be confronted during the selection process with questions that have
little or no bearing on their ability to produce desired work results
From the findings, it was noted that competencies predict effective performance, result in
valid selection criteria, recognize the transferability of employees' skills and are flexible to
meet the changing needs of future requirements. Furthermore, the competency model
covers all aspects of what it takes to be successful in a job by examining not only
knowledge and skills required but the personal attributes required as well.
5.4 Recommendation
The recruitment and selection process is one of the most important and costly investments
an organization can make. Risks can be high and the cost of a bad hire can have
tremendous impact in time, money and company culture.
In addition to the above discussed and detailed conclusions, the following
recommendations should be taken into consideration by hospitals in their competency
based recruitment and selection
Need to develop and implement a communication strategy to support the Human
Resource Departments
51
Building awareness is an important starting point. HR staff and hospital
management should attend workshops, classes, or conferences on competency
modelling or invite external consultants.
The management of the hospitals need to provide time and money to carry out the
individualized competency identification and assessment for those targeted to
receive training.
The management of the hospitals should provide strong, long-term support for the
projects and act as role models for the process. Required resources need to be
available over the long term. Managers will face increased workloads as a
competency-based approach requires them to provide new hires with additional
and more effective feedback as well as accept responsibilities for addressing
performance obstacles.
The Human Resource Department must continuously evaluate the competency
based recruitment and selection process and make revisions as necessary
5.5 Suggestions for further studies
While this study was able to provide additional insight into the use of competencies and its
relationship to an effective recruitment and selection process in hospitals, it also revealed
areas that would benefit from further research. These are:
Future research could thus focus on the other functions such as compensation and benefits.
By doing so, a better and fuller understanding of the effects of core competencies on an
organization’s performance may be achieved.
52
Secondly, this study recognized the importance of measuring the performance of the
hospitals’ employees according to their core competencies, hence, there is a need for
further study on the benefits of the competency based performance management systems.
53
REFERENCES
Boyatzis,R.E. (1982),The Competent manager: A model for Effective Performance. New
York: Wiley
Dreyfus, H.L. & S.E. Dreyfus (1986), Mind over Machine: The Power of Human Intuition
and Experience in the Era of the Computer. Oxford: Basil Blackwell.
Dubois, D.D. (1993), Competency-Based Performance Improvement: A Strategy for
Organizational Change. Amherst: HRD Press.
Creese, A., (1997), ‘User Fees – They Don’t Reduce Costs, and They Increase Inequity’,
British Medical Journal, 315, 202-203.
Hamel, G. & C.K. Prahalad (1994), Competing for the future. Boston: Harvard Business
School.
McClelland, D.C. (1973), Testing for Competence rather than for ‘Intelligence’. American
Psychologist, 26, pp. 211 –242.
Odada, J. E. O. and Ayako A. B., eds., (1989), Report of the Proceedings of the Workshop
on ‘The Impact of Structural Adjustment Policies on the Well-being of the Vulnerable
Groups in Kenya’, November 3-5, (1988).
Odada, J. E. O. and Odhiambo, L. O., (1989), Report of the Proceedings of the Workshop
on ‘Cost-sharing in Kenya’, 29 March-2 April 1989.
Okwemba, A., (2004), ‘KNH Raises Fees Amid Graft
Owino, P. S. W., (1997), ‘Public Health Sector Efficiency in Kenya: Estimation and Policy
Implications’, IPAR Discussion Papers.
54
Owino, P. S. W., (1998), ‘Public Health Care Pricing Practices: The Question of Fee
Adjustment’, IPAR Discussion Papers.
Prahalad, C.K. & G. Hamel (1990),The Core Competence of the Corporation. Harvard
Business Review, May-June, 79-91.
Rodriguez, D., Patel, R., Bright, A., Gregory, D. and Gowing, M. K. (2002) ,Developing
competency model to promote integrated human resource practices, Human Resource
Management, 41, pp. 309 –324.
Roos, J. & G. von Krogh (1992), Figuring out your Competence Configuration. European
Management Journal, 10, 4, 422-427.
Rothwell, W.J. (1996),ASTD Models for Human Performance Improvement: Roles,
Competencies and Outputs. Alexandria: American Society for Training and Development.
Sandberg, J. (1994) ,Human Competence at Work: An Interpretive Approach (Go¨ teburg:
Bas).
Sandberg, J. (2000), Competence – the basis for a smart workforce, in: R. Gerber and C.
Lankshear (Eds) Training for a Smart Workforce, pp. 47 – 72 (London: Routledge).
Senge, P.M. (1990), The Fifth Discipline: The Art & Practice of The Learning
Organization. New York: Doubleday.
Scarborough, H. (1998), Pathological dependency? Core competencies from an
organizational perspective, British Journal of Management, 9,pp.219-232.
Smith, B. (1993), Building managers from the inside out: competency based action
learning, Journal of Management Development, 12(1), pp. 43 – 48.
Mullins, S. H. (2010) ,Human Resource Management. Oxford: Oxford University Press.
Chapter 5 takes a themed approach to the topic of employee selection.
55
Bratton, P. and Gold, D. (2007),Work Organisations: A critical approach, 4th ed.
Basingstoke: Palgrave Macmillan. In Chapter 19 entitled ‘Masks for Tasks’, the authors
take a critical perspective on the topics of how we assess others’ attributes and how such
perceptions are used in employee selection.
Smithers, A. (1993,) All Our Futures: Britain’s Education Revolution (London: Channel
Four).
Snyder, A. and Ebeling, H. W. (1992), Targeting a company’s real core competencies,
Journal of Business Strategy, 13(6), pp. 26 – 32.
Spencer, L. and Spencer, S. (1993), Competence at Work: A Model for Superior
Performance (New York: Wiley). Amref Competency report, 2009
World Bank, (1997), The State in a Changing World - World Development Report, Oxford,
Oxford University Press.
56
APPENDICES
Appendix I: Questionnaire
This questionnaire is designed to gather information on Competence Based Recruitment and Selection. The information you give will be treated with utmost confidentiality and will be solely used for academic purposes intended in this research. Please tick where appropriate next to the response you deem necessary or fill in the required information. Please respond to all the items.
PART A: PROFILE OF THE FIRM/RESPONDENT
1) Indicate your gender?
a) Male [ ] b) Female [ ]
2) Indicate your designation/position in the institution? _____________________________
3) Indicate your age bracket a) Below 30 years [ ]
b) 30-40 years [ ]
c) 41-50 years [ ]
d) Over 50 years [ ]
PART B: COMPETENCY BASED RECRUITMENT
4) When recruiting new members of staff, to what extent do you consider the following aspects?
Aspect Not at all
Little extent
Moderate extent
Large extent
Very large extent
a) Good understanding of your organization
b) A person with strategic thought
c) Innovative person d) Able to communicate
fluently and effectively e) Good customer focus and
able to relate well with the
57
public f) leadership abilities g) Ability to teamwork h) Ability to manage time
well i) Any other (specify)
On a scale of 1 to 5 where 1 represents the least extent while 5 gives the greatest
extent, indicate the level to which you consider the following factors when you are
recruiting.
1 2 3 4 5
5) Interpersonal Relations: Awareness of others’ feelings, needs, perceptions and concerns
a) Relates well to others
b) Demonstrates trust, sensitivity and mutual respect
c) Recognizes the contributions diversity brings to job performance and creativity
d) Demonstrates altruistic empathy – caring for others
b) Self-confidence: strong sense of self worth and capabilities (self efficacy)
7) Analytic Thinking: Using data to understand patterns and develop concepts
a) Information gathering skills
b) Use of range of sources
c) Looking beyond routinely explanations of organizational performance
58
d) Good in decision making
8) Adaptability: Flexibility in handling change
a) Handles day-to-day challenges confidently
b) Is willing to adjust to multiple demands, shift priorities, ambiguity and rapid change depending on organizational demands
c) Shows resilience in the face of constraints, frustrations or adversity
d) Ability to adapt styles and shift gears
e) Shows evidence of coping skills
f) Innovation: comfortable with new ideas; open to new information.
9) Observation Skills: Ability to describe events factually
a) Ability to observe and identify key elements
b) Recognition of inconsistencies
c) Factual descriptions
d) Accurate observations
10) Sense of mission: Commitment to the achievement of the organizational objectives
a) Evidence of adequate knowledge on the organization
b) Desire to make things better for others
11) Communication Skills: Open clear communication
a) Speaks clearly and expresses self well
b) Demonstrates attentive listening
c) Conveys information clearly and effectively through
59
written documents
12) Motivation: Emotional tendencies that guide or facilitate reaching organizational goals
a) Commitment: aligning with the goals of the organizational
b) Achievement: strives to improve, drives for results and success
c) Sets high standards of performance
d) Displays a high level of effort and commitment to perseverance performing the work
e) Optimism: persistence in pursuing goals
13) Planning and organizing work: Ordering activities to achieve goals
a) Ability to assess/reprioritize
b) Use of time management tools
c) Defines and arranges activities in a logical and efficient manner
14) Teamwork: Creating group synergy in pursuing collective goals
a) Contributes to organizational goals
b) Fosters collaboration among team members and among teams
15) Any other comments ________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
THANK YOU FOR YOUR COOPERATION
60
Appendix II: List of Hospitals
Name Location 1) Aga Khan Hospital Parklands 2) Alpha Maternity & Nursing Home Eastleigh 3) Avenue Hospital Parklands 4) Central Park Hospital Kibera 5) Chiromo Lane Med Centre Westlands 6) City Nursing Home Mufungano Street 7) City Park Hospital Park Road 8) Comprehensive Medical Services Thetha Road off Lenana Road 9) Coptic Church Nursing Home Ngong Road 10) Dorkcare Nursing home Munyu Road 11) Eastleigh Community Clinic 5th street, Eastleigh 12) Emmaus Innercare Nursing Home Umoja Inner core 13) Genisis Nursing & Maternity Hospital 14) Getrude Garden Childrens Hospital Muthaiga 15) Guru Nanak ramgarhia Sikh Hospital Murang’a Road 16) Huruma Nursing Home Huruma estate 17) Ideal Nursing Home Juja Road 18) Inder Nursing Home Pangani 19) Jamaa Home & maternity Hospital Rabai Road, Uhuru Estate 20) Kabiro Health care Trust Kawangware 46 21) Kasarani Maternity & Nursing Home Kasarani 22) Kayole Hospital Ltd Kayole 23) Kilimanjaro Nursing Home Eastleigh Section 1 24) Komarok Nursing Home Komarock 25) Lions Sightfirst Eye Hospital Loresho 26) M. P Shah Hospital Parklands 27) Mara Maternity & Nursing Home Kayole Estate 28) Madina Nursing Home 9 th street Eastleigh 29) Kenyatta Hospital Private Wing KNH 30) Karen Hospital Karen 31) Family Health Care Off Langata Road 32) Maria Immaculate Mission Hospital Gitanga Road 33) Mariakani Cottage Hospital South B 34) Masaba Hospital Adams Arcade 35) The Mater Hospital South B 36) Melchizedek Hospital Naivasha Road 37) Metropolitan Hospital Rabai Road 38) Mother & Child Hospital Eastleigh Sec vii 39) Nairobi Equator Hospital Nairobi West
61
40) The Nairobi Hospice Next to KNH 41) The Nairobi Hospital Argwings Kodhek Road 42) Nairobi Women’s Hospital Nairobi west 43) Nairobi West Hospital Hurlingham 44) Ngara Nursing Home Ngara 45) Lianas Hospital Kangemi 46) The Olive Tree Hospital South C 47) Kijabe Mission Hospital Kijabe 48) Kikuyu Mission Hospital Kikuyu 49) Park Road Nursing Home Park Road 50) Parklands ambulatory Surgical Centre Parklnads 51) Prime Care Hospital Tena estate 52) Redient Health Nursing home Pangani 53) Right Medical Centre Lavington 54) St. James Hospital Mombasa Road 55) St. James Medical Centre Ltd Komarock Road 56) St. Marys’ Mission Hospital Otiende 57) Samar Clinic & Maternity Home Kahawa Sukari 58) South B Nursing Home South B 59) Umoja Nursing Home Umoja Phase 1 60) Westlands Cottage Hospital East Church Road
62
Appendix III: List of Sampled Hospitals
Name Location 1) Aga Khan Hospital Parklands 2) Alpha Maternity & Nursing Home Eastleigh 3) Central Park Hospital Kibera 4) Chiromo Lane Med Centre Westlands 5) City Park Hospital Park Road 6) Comprehensive Medical Services Thetha Road off Lenana Road 7) Dorkcare Nursing home Munyu Road 8) Eastleigh Community Clinic 5th street, Eastleigh 9) Genisis Nursing & Maternity Hospital 10) Getrude Garden Childrens Hospital Muthaiga 11) Huruma Nursing Home Huruma estate 12) Ideal Nursing Home Juja Road 13) Jamaa Home & maternity Hospital Rabai Road, Uhuru Estate 14) Kabiro Health care Trust Kawangware 46 15) Kayole Hospital Ltd Kayole 16) Kilimanjaro Nursing Home Eastleigh Section 1 17) Lions Sightfirst Eye Hospital Loresho 18) M. P Shah Hospital Parklands 19) Madina Nursing Home 9 th street Eastleigh 20) Kenyatta Hospital Private Wing KNH 21) Family Health Care Off Langata Road 22) Maria Immaculate Mission Hospital Gitanga Road 23) Masaba Hospital Adams Arcade 24) The Mater Hospital South B 25) Metropolitan Hospital Rabai Road 26) Mother & Child Hospital Eastleigh Sec vii 27) The Nairobi Hospice Next to KNH 28) The Nairobi Hospital Argwings Kodhek Road 29) Nairobi West Hospital Hurlingham 30) Ngara Nursing Home Ngara 31) The Olive Tree Hospital South C 32) Kijabe Mission Hospital Kijabe 33) Park Road Nursing Home Park Road 34) Parklands ambulatory Surgical Centre Parklnads 35) Redient Health Nursing home Pangani 36) Right Medical Centre Lavington 37) St. James Medical Centre Ltd Komarock Road 38) Samar Clinic & Maternity Home Kahawa Sukari 39) South B Nursing Home South B