157
A Total Approach to Treating the Neck & Scapula Assessment, Manual & Exercise Techniques Sue Dupont, MS, MBA, PT, ATC Cross Country Education, Inc.
| Date post: | 19-Mar-2018 |
| Category: |
Documents |
| Upload: | duongkhanh |
| View: | 220 times |
| Download: | 4 times |
A Total Approach to Treating the Neck &
Scapula Assessment, Manual & Exercise
Techniques
Sue Dupont, MS, MBA, PT, ATCCross Country Education, Inc.

Good Morning!

3
Sue Dupont, MS, MBA, PT, ATC
Cross Country EducationLeading the Way in Professional Development. www.CrossCountryEducation.com
To comply with professional boards & associations standards:
• I declare that I or my family do not have any financial relationship in any amount, occurring in the last 12 months with a commercial interest whose products or services are discussed in my presentation.
•Requirements for successful completion is attendance for the full day seminar.• If not attending full day, amended CE will be granted accordingly based on your boards or associations requirements along with a completed course evaluation form.•Cross Country Education and all current accreditation statuses does not imply endorsement of any commercial products displayed in conjunction with this activity.
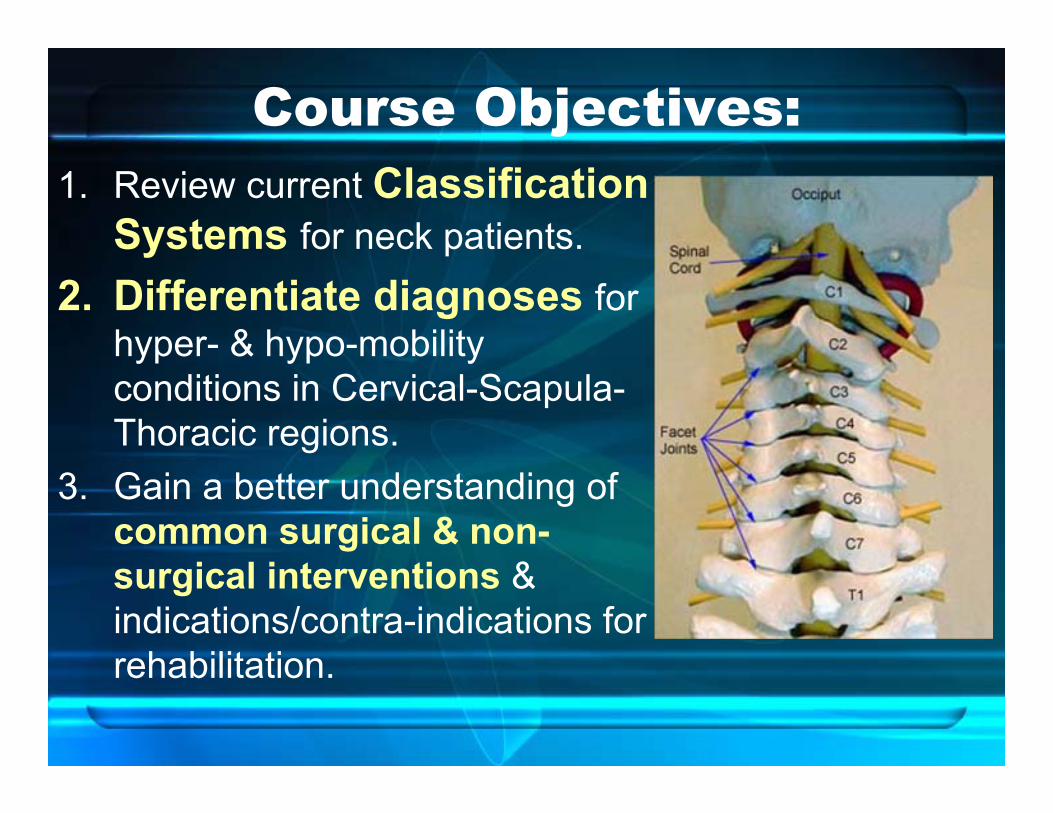
Course Objectives:1. Review current Classification
Systems for neck patients.2. Differentiate diagnoses for
hyper- & hypo-mobility conditions in Cervical-Scapula-Thoracic regions.
3. Gain a better understanding of common surgical & non-surgical interventions & indications/contra-indications for rehabilitation.

4. Review the clinical application of modalities & demonstrate manual therapy techniques to improve function & relieve pain.
5. Identify specific stabilization & mobilization exercise progressions, & apply PNF and Pilates principles to retrain movement.

WHO study on Neck Pain
• 2000 to 2010• 9 countries• 19 clinical & scientific disciplinesPurpose:
–To inform and empower the public–Prevent disabling neck pain
S. Haldeman, et al., 2009– J Manip & Physiol Ther.

Why Do We Need to Understand the Neck & Scapula Better?
Injuries are Costly:• Total annual medical cost to U.S. society for neck
injury is estimated to be $3.9 billion.Injuries are Disabling:• 4 to 42% of people who sustain neck injuries in
MVA exhibit symptoms that persist for years and can be disabling.
(Winkelstein et al. 2000)
Injuries are Prevalent:• Neck pain affects1/3 of adult population• Over 50% of patients with neck pain are referred
for therapy. (Cleland et al., 2007)
Lack of Diagnostic Evidence:• X-ray findings of neck often do not correlate with
symptoms. • Neck muscle functioning is usually accepted as
satisfactory if gross movements are normal.
Lack of Favorable Outcomes:• “The efficacy of active exercises and passive
physiotherapy has been partly disappointing.”(Olson et al. 2000, Ylinen et al. 1994)
“Act as if what you do makes a difference. It does.”
-William James
Differential Diagnosis
Classifications Systems for Neck Patients
• Goal: to improve outcomes for neck patients

Neck Classification System
• Moffett & McLean (Rheum. 2006)
3 group classifications: Serious pathology, Neuro. involved, Non-specific– Non-specific is most common– Red/yellow/green flags for treatment– Emphasis on pt education & self-
management– Focus on return to normal activities

WHO: 4-Grade System
• Grade I: No major structural pathology; min. impact on ADLs
• Grade II: No major structural pathology; major impact on ADLs
• Grade III: No major structural pathology; positive neurological signs/symptoms
• Grade IV: Major structural pathology; requires prompt testing and treatment
Fritz & Brennan (Phys Ther 2007)
5 Classifications based on treatment1. Mobility— younger, more acute symptoms;
manual tx plus strengthen deep neck flexors2. Centralization— signs of nerve
compression; longer duration, peripheralization with ROM; treat with traction and retraction
3. Exercise & Conditioning— chronic pain, older pts; strengthen neck flexors & upper quadrant
5 Classifications (cont)
4. Pain Control– acute, traumatic onset; high pain & disability levels; tx with mobilization, ROM; avoid immobilization
5. Cervicogenic Headache– h/a originates from C-spine structure; tx with strengthen deep neck flexors & upper quad, mobilize C-spine
Matched vs Unmatched Interventions
• Most common: 1. Centralization, 2. Exercise
• Of matched interventions, 72.5%patients with appropriate “minimal detectable change” (MDC) on NDI–Unmatched interventions only had a
53.8% MDC on NDI(n=274)
Matched vs Unmatched Interventions
• Pain group —highest % pts with matched
• Mobility group —most change in pain & disability after matched intervention given

Matched vs. Unmatched (cont)Exercise & H/A groups:• Had least % matched
interventions with criteria!!!
• May indicate tendency not to emphasize strength with older, chronic neck patients even though indicated.
Clinical Prediction Rule
Cleland, et al. Phys Therapy 2007:• 6 criteria for neck patients who may
benefit from thoracic spine mobilization:1. Duration < 30 days2. No symptoms distal to shoulder3. Cervical Extension does not increase sx’s4. FABQPA score <12 (fear-avoidance beliefs)5. Diminished T-spine kyphosis (T3-T5)6. Cervical Extension AROM < 30 deg.

Biomechanical Link in C-T junction
• If pt had 4 of 6 criteria = 93% prob. Success
• If 5 or 6 of 6 criteria = 100% prob. success
(95% conf interval)
Clinical Application of Results• ↓ thoracic kyphosis & ↓
cervical extension may be associated with biomechanical link b/w Thoracic & Cervical spines.
• Correlation b/w mobility in C-T junction & Thoracic spine with Neck & Shoulder pain.

Causes of Neck Pain & Disability• Trauma (Acute or
Repetitive) • Aging• Posture
Resulting disability may be due to:1. Biomechanical & Structural Changes2. Motor Control Changes
Biomechanical & Structural Changes
• Breakdown in the Kinetic Link– Movement forces need to be decelerated– If constraint system is weak, or mechanically-
deficient, get ↓ performance & anatomic instability develops (McMullen et al. 2000)
• Traumatic or repetitive strain injury – causes damage & loss of integrity to joint
structures (Olson et al. 2000)

Biomechanical & Structural Changes• Untreated joint laxity & torsional
deformities– Normal variations in joint laxity & torsional
deformities in children, if left untreated, may persist in adulthood
– Produce symptoms due to premature DJD (Salter 1984)
• Diseases and degenerative conditions – break down integrity of joint structures
(Olson et al. 2000)
Motor Control Changes• Changes in Central Nervous System
Processing – Affect movement, reaction & information
processing• Changes in the musculoskeletal system
– Loss of strength, different timing & activation patterns, loss of proprioception & balance
(Light 1990; Woollacott & Shumway-Cook 1990; Schenkman et al. 1996)
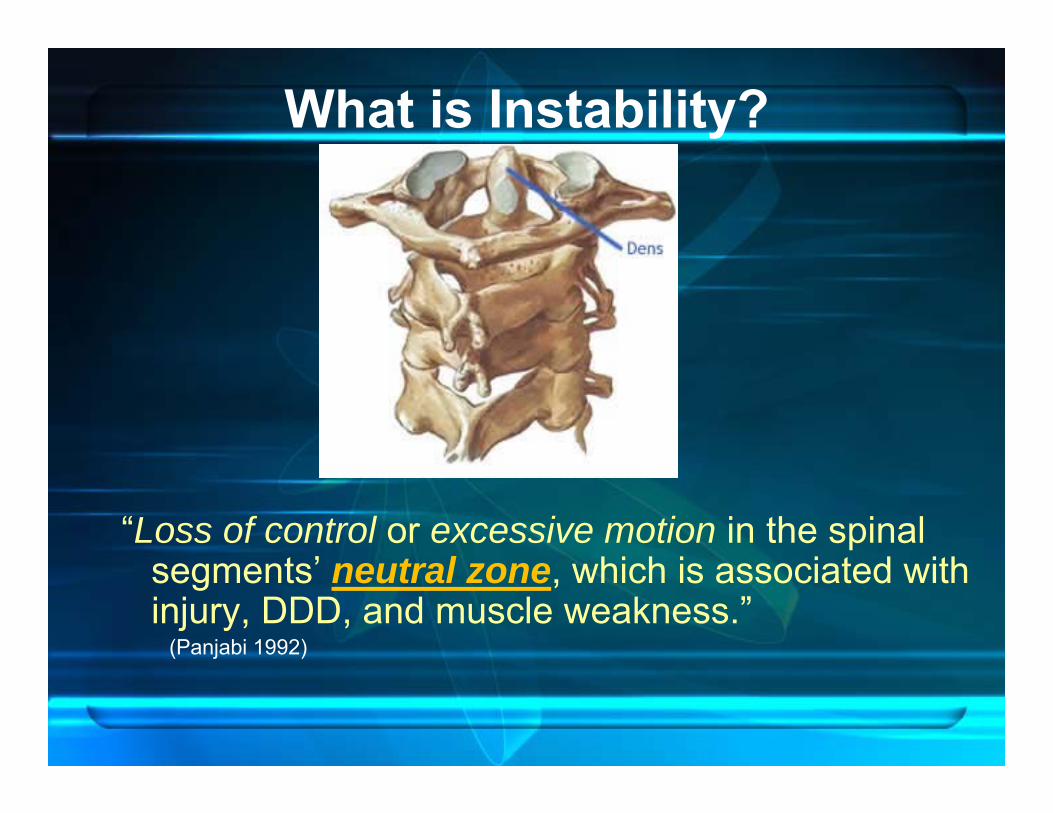
What is Instability?
“Loss of control or excessive motion in the spinal segments’ neutral zone, which is associated with injury, DDD, and muscle weakness.”
(Panjabi 1992)

Common Diagnoses We Treat• Hyper-Mobility Conditions:
– Whiplash – Degenerative Disc Disease– Spondylosis (early stage)– Herniated Disc– Facet Joint Syndrome– Scoliosis
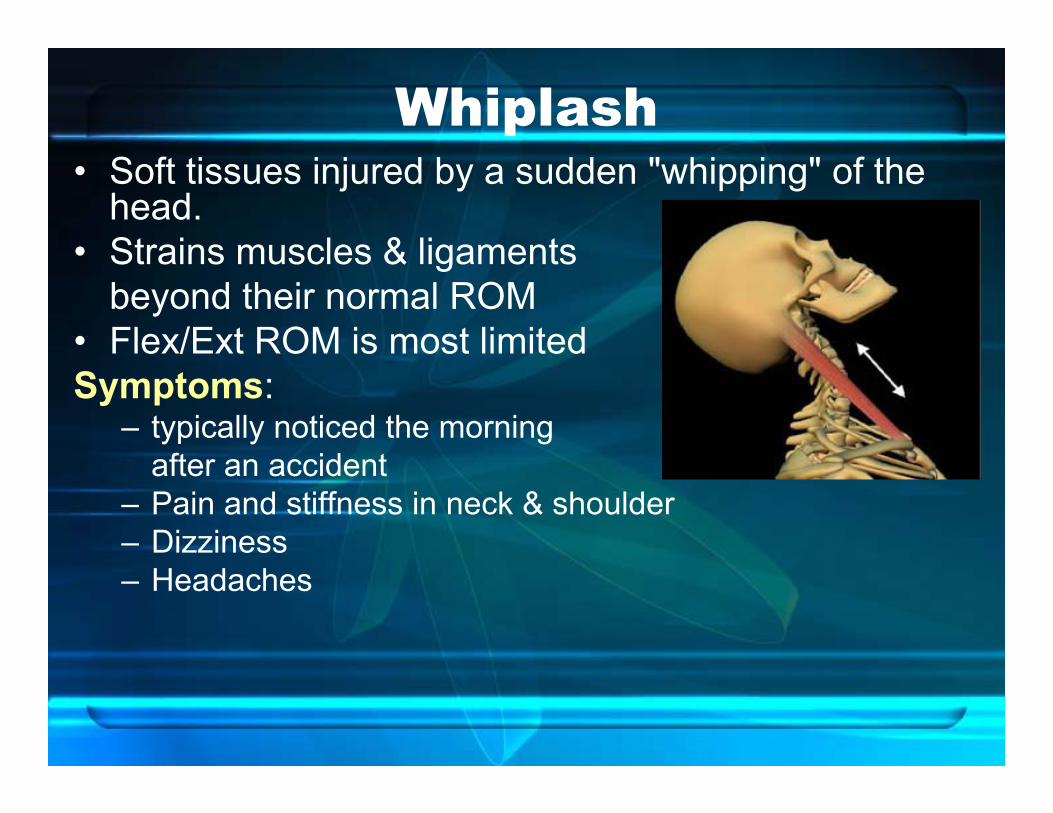
Whiplash• Soft tissues injured by a sudden "whipping" of the
head.• Strains muscles & ligaments
beyond their normal ROM• Flex/Ext ROM is most limitedSymptoms:
– typically noticed the morning after an accident
– Pain and stiffness in neck & shoulder– Dizziness– Headaches

Spondylosis & DDD
• Abnormal wear on cartilage, disc & cervical vertebrae with degeneration & mineral deposits in vertebral discs.

Stages of Disc Herniation• Annulus may be weakened by sudden or
repetitive trauma• Nucleus is forced through a weakened
part of annulus• Result:
Bulging or herniated disc with or without radiculopathy

Cervical Disc Herniation• C5-C6 represents 90% of
cervical disc lesions
Provocation:Symptoms worse with: - activity - awakening in morning - neck extension - coughing, sneezing, or
straining

Symptoms of Cervical HNPObjective Findings:• Decreased ROM• Neck hyperextension
elicits pain • Localized C-Spine
tenderness • Trigger Point
tenderness over inter-scapular area
• Spurling Test positive
Referred pain:1. Into shoulder— along
Radial Nerve• Does not often
radiate below elbow • In contrast with
Paresthesias (distal radiation)
2. Into medial scapula – Inter-scapular
pain not of shoulder origin
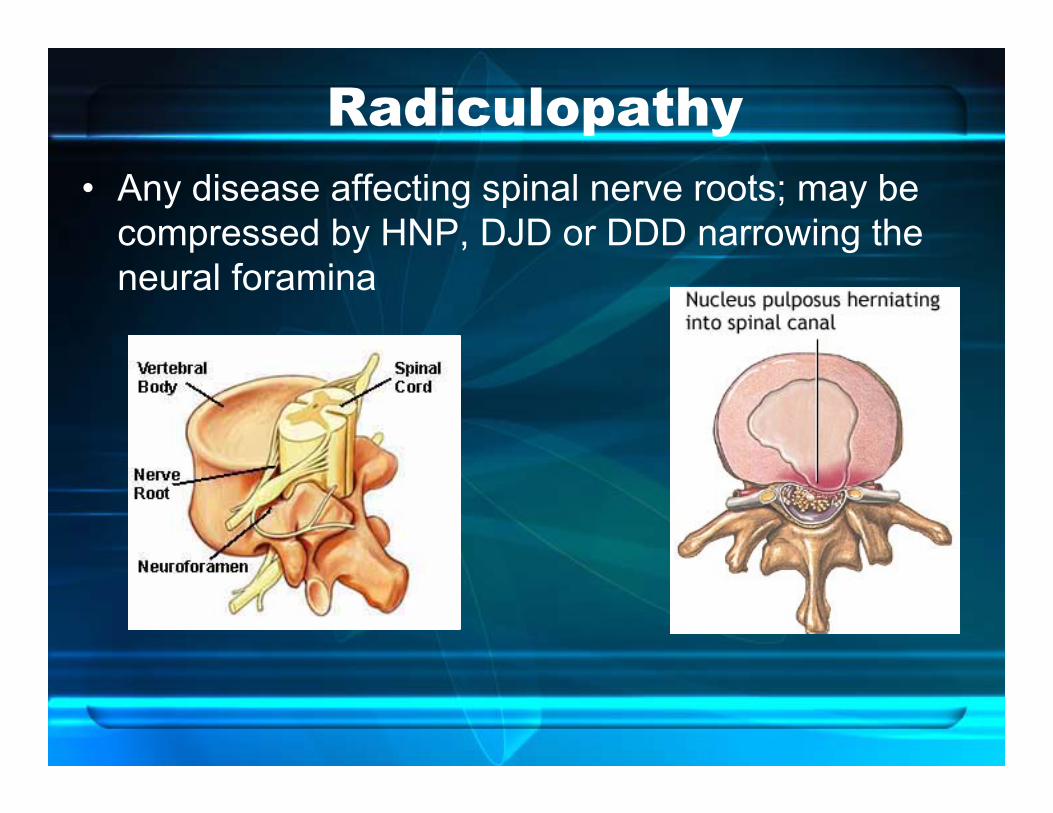
Radiculopathy• Any disease affecting spinal nerve roots; may be
compressed by HNP, DJD or DDD narrowing the neural foramina

RadiculopathySymptoms:
• Neck Pain—may radiate to the arms or shoulder • Abnormal sensations in shoulders & arms • Weakness of the arms• Neck stiffness that progressively worsens • Headaches— particularly in the back of the head
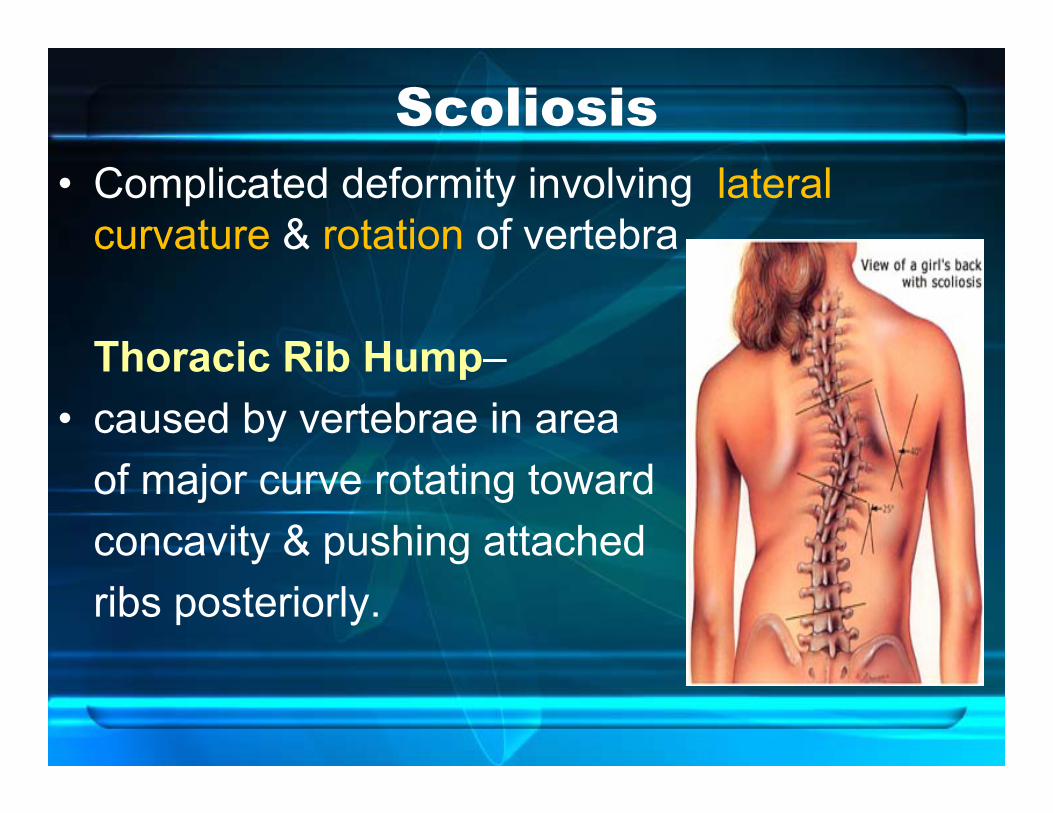
Scoliosis• Complicated deformity involving lateral
curvature & rotation of vertebra
Thoracic Rib Hump–• caused by vertebrae in area
of major curve rotating toward concavity & pushing attached ribs posteriorly.
3 Main Causes of Scoliosis
1. Congenital defect2. Neuromuscular—muscular weakness or
paralysis due to diseases 3. Idiopathic
• Osteoporosis & micro-fractures, along with muscle weakness contribute to progression of spinal deformity in elderly (Salter 1994)
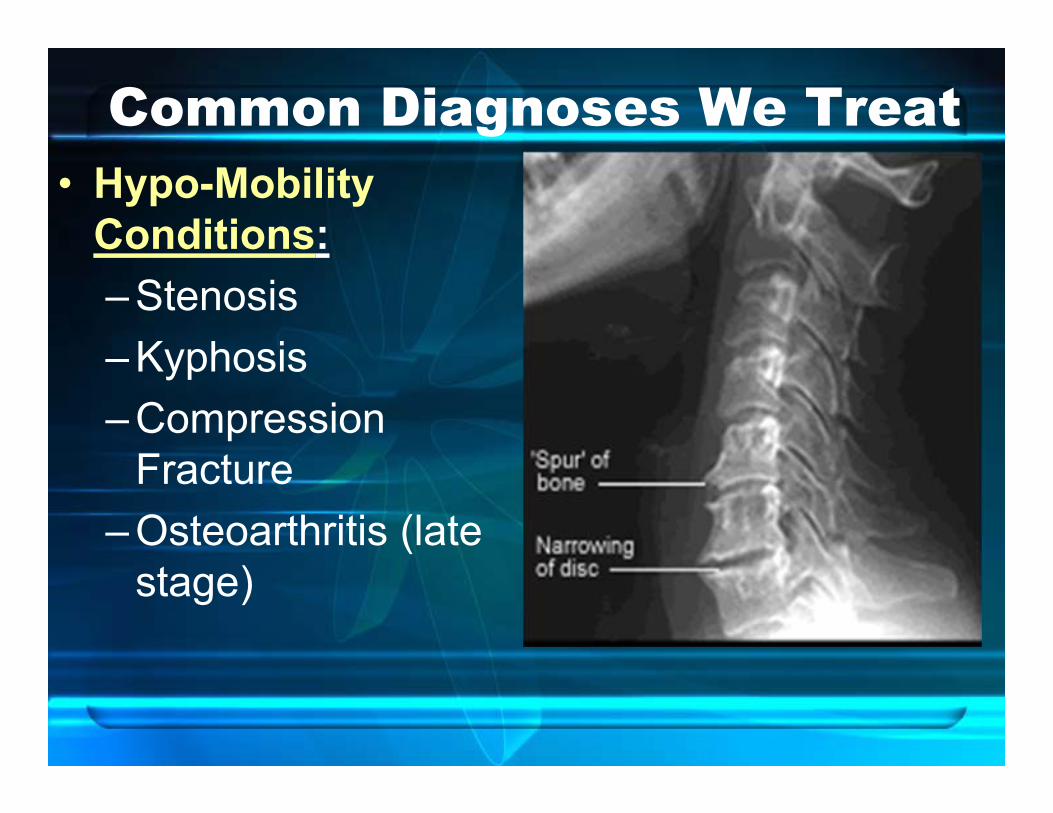
Common Diagnoses We Treat• Hypo-Mobility
Conditions:– Stenosis– Kyphosis– Compression
Fracture– Osteoarthritis (late
stage)
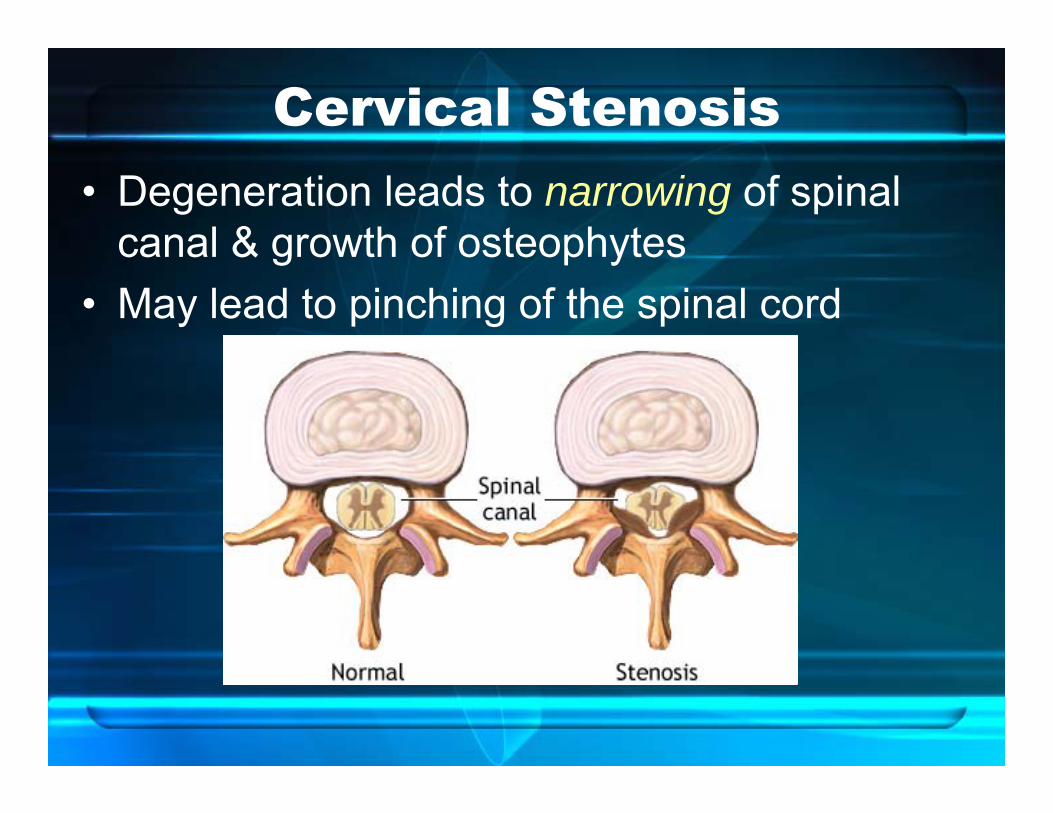
Cervical Stenosis• Degeneration leads to narrowing of spinal
canal & growth of osteophytes• May lead to pinching of the spinal cord

Spinal Cord CompressionCauses myelopathy:• Neck & shoulder
stiffness and pain • Arm or Leg tingling
and/or numbness• Trouble walking• Changes in reflexes• Loss of bladder or
bowel control.

Nerve Root Compression• Caused by changing
consistency of discs & ligaments—begins at age 30 !!
• Discs become dry and lose elasticity
• Ligaments & muscles become stiff
• Risk may be reduced early on by exercise & practicing good posture.

Osteophyte & Nerve Root Compression
◄

Kyphosis* Curve more than 50
degrees is abnormal. • Postural kyphosis:
most common type; often attributed to "slouching." Discs appear normal.
• Scheuermann's kyphosis: Discs are wedge-shaped, painful.

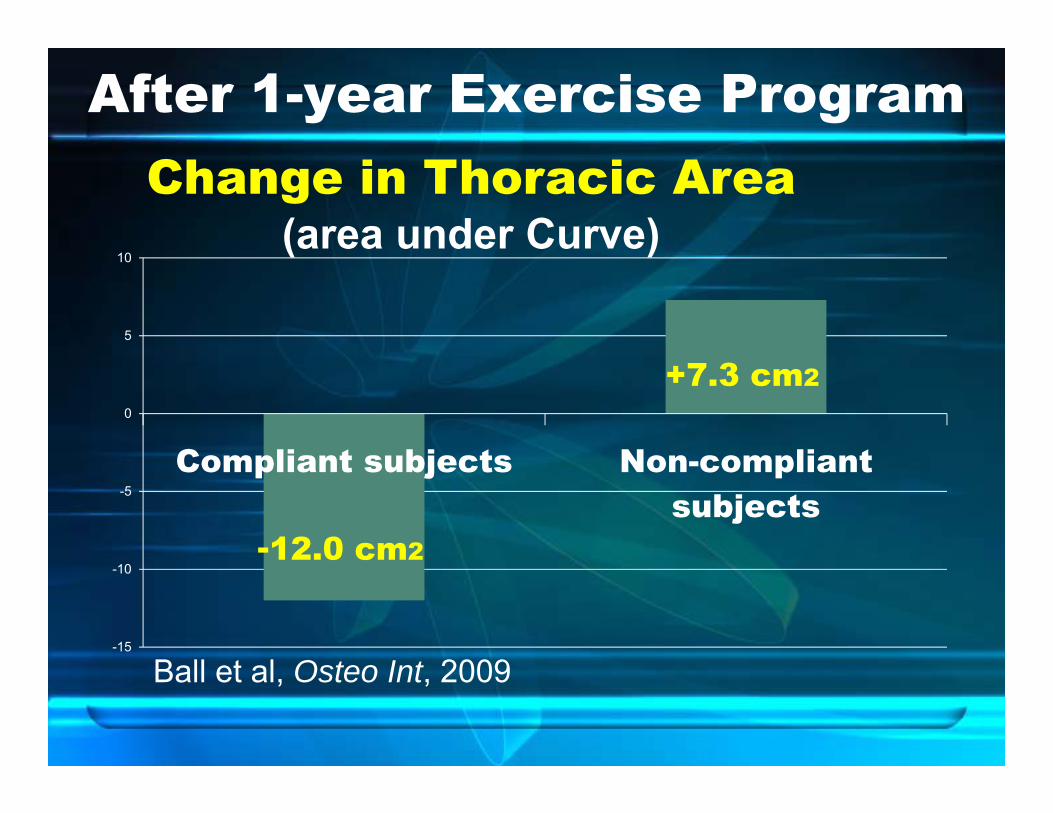
Kyphosis—Current Evidence:• Angle increases with age, esp.
b/w 50-60 y.o.• Most at Risk:
– Less physically fit– Poor posture– Heredity, habits & stress
• Prevent and improve with extension exercises!!!
• Use of spinal bracing may reduce angle in severe cases.
ref: Ball et al, Osteo Int, 2009.
-15
-10
-5
0
5
10
Compliant subjects Non-compliantsubjects
Change in Thoracic Area (area under Curve)
Ball et al, Osteo Int, 2009
-12.0 cm2
+7.3 cm2
After 1-year Exercise Program

Spinal Fractures• Acute• Indirect• Compression fracture
– break in vertebral body due to loss of bony mass

Facet Joint SyndromeAcute: Due to sudden excessive movement
– May pinch facet capsule– Painful extension to one side
Chronic: due to long-term DJD
How Do We Stabilize?
Review of Anatomy

Stability of Cervical Column
• Stability in sagittal plane depends on constant equilibrium between:– Extension (post. & lat. neck muscles)– Flexion (ant. & lat. neck muscles)
• Simultaneous contraction maintains cervical column stiffness in neutral zone, which equals STABILITY
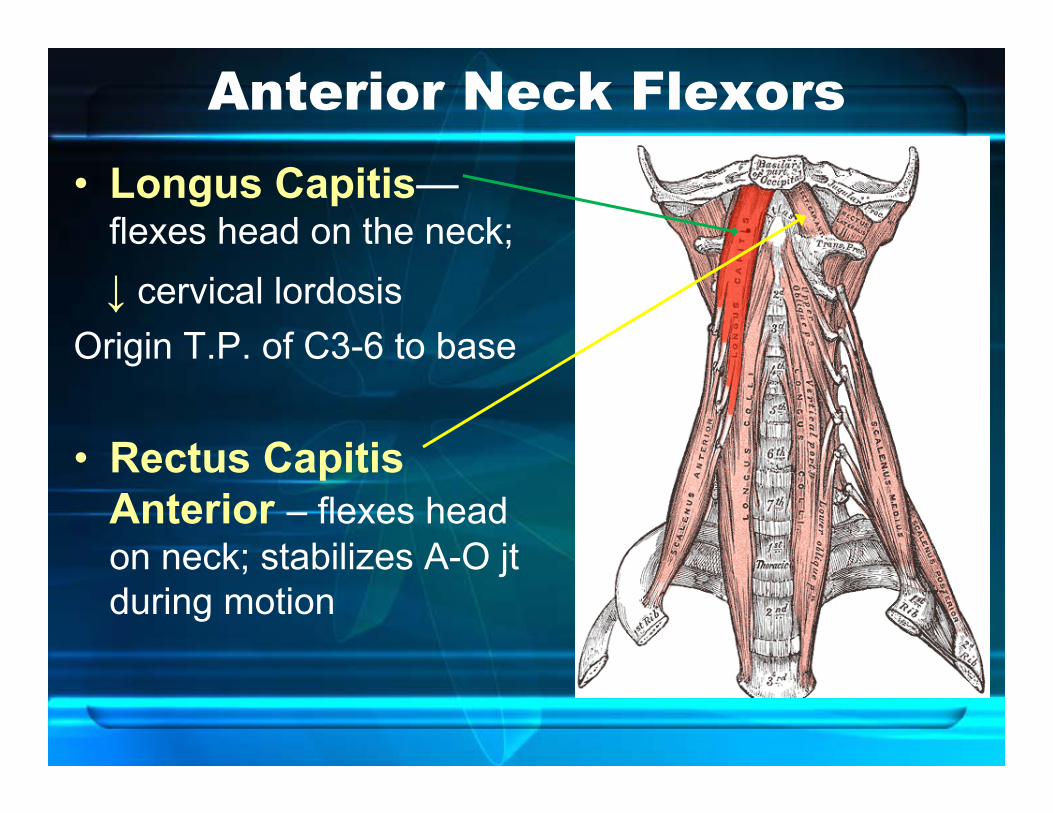
Anterior Neck Flexors• Longus Capitis—
flexes head on the neck; ↓ cervical lordosis
Origin T.P. of C3-6 to base
• Rectus Capitis Anterior – flexes head on neck; stabilizes A-O jt during motion
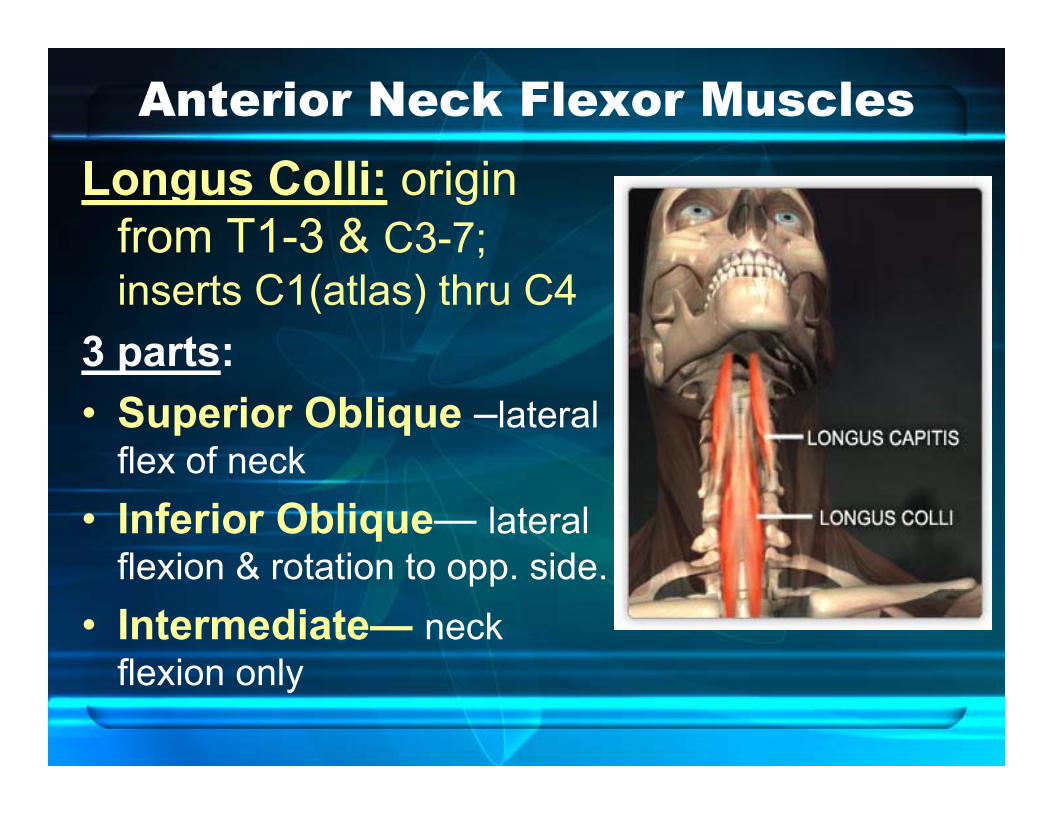
Anterior Neck Flexor MusclesLongus Colli: origin
from T1-3 & C3-7; inserts C1(atlas) thru C4
3 parts: • Superior Oblique –lateral
flex of neck• Inferior Oblique— lateral
flexion & rotation to opp. side. • Intermediate— neck
flexion only

Anterior Flexor Muscles• Scalene Muscles–
flexes neck, ↑ cervical lordosis (unless counter-acted by longus capitis & hyoid muscles)

Lateral Neck Muscles
Why are SCM & Scalenes a Problem???
• SCM and Ant. Scalene are superficial muscles– typically substituted for weak deep neck flexors
during chin tuck exercise• BUT:
– SCM has an Extensor Moment– Ant. Scalene is NOT attached to cranium
• Can’t flex the head on the neck!!
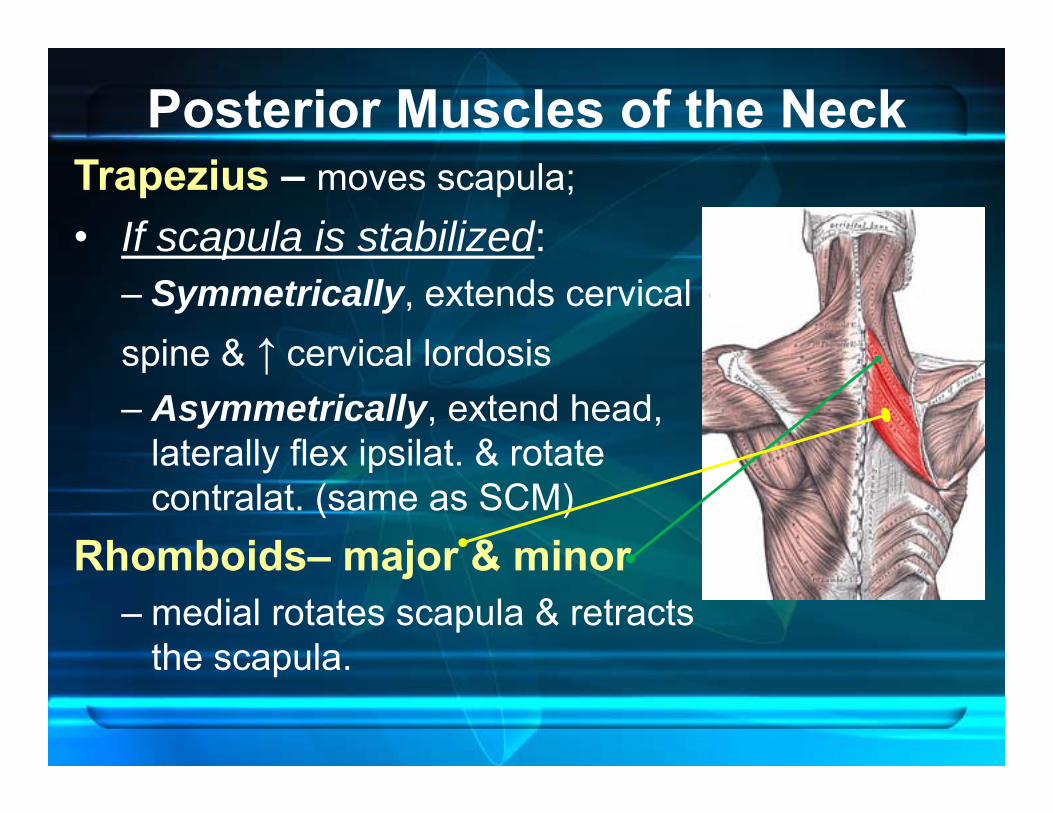
Posterior Muscles of the NeckTrapezius – moves scapula; • If scapula is stabilized:
– Symmetrically, extends cervical spine & ↑ cervical lordosis– Asymmetrically, extend head,
laterally flex ipsilat. & rotate contralat. (same as SCM)
Rhomboids– major & minor– medial rotates scapula & retracts
the scapula.
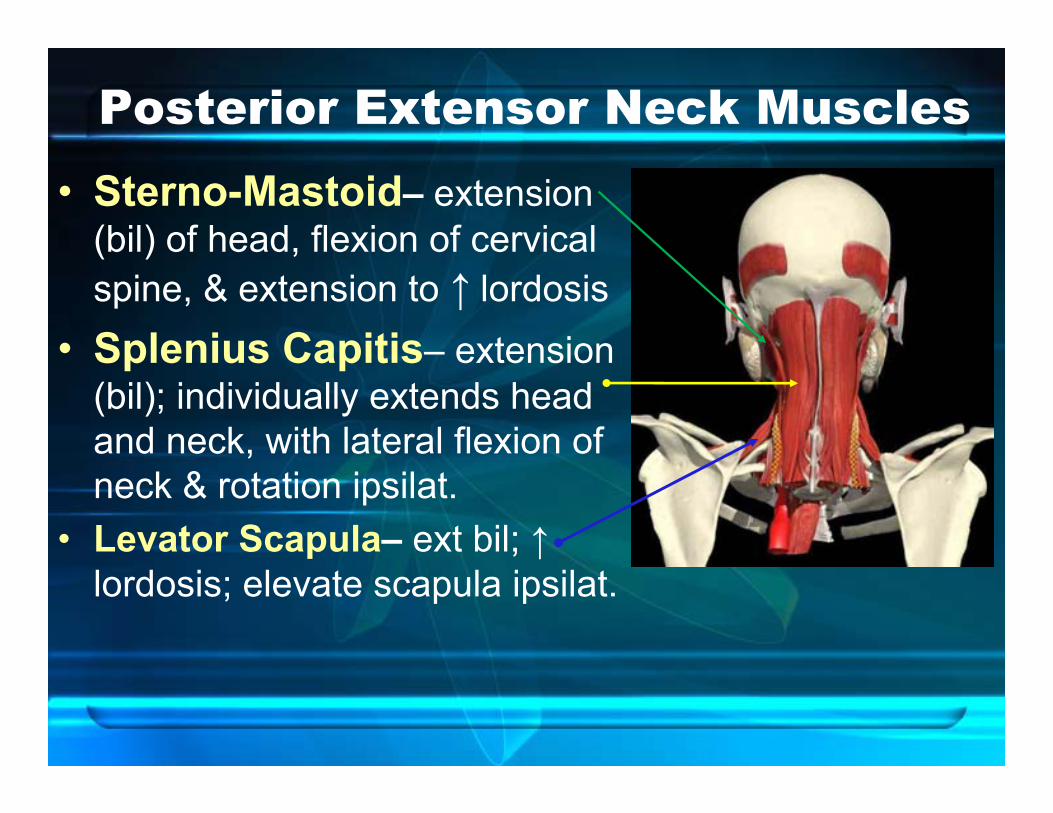
Posterior Extensor Neck Muscles• Sterno-Mastoid– extension
(bil) of head, flexion of cervical spine, & extension to ↑ lordosis
• Splenius Capitis– extension (bil); individually extends head and neck, with lateral flexion of neck & rotation ipsilat.
• Levator Scapula– ext bil; ↑lordosis; elevate scapula ipsilat.
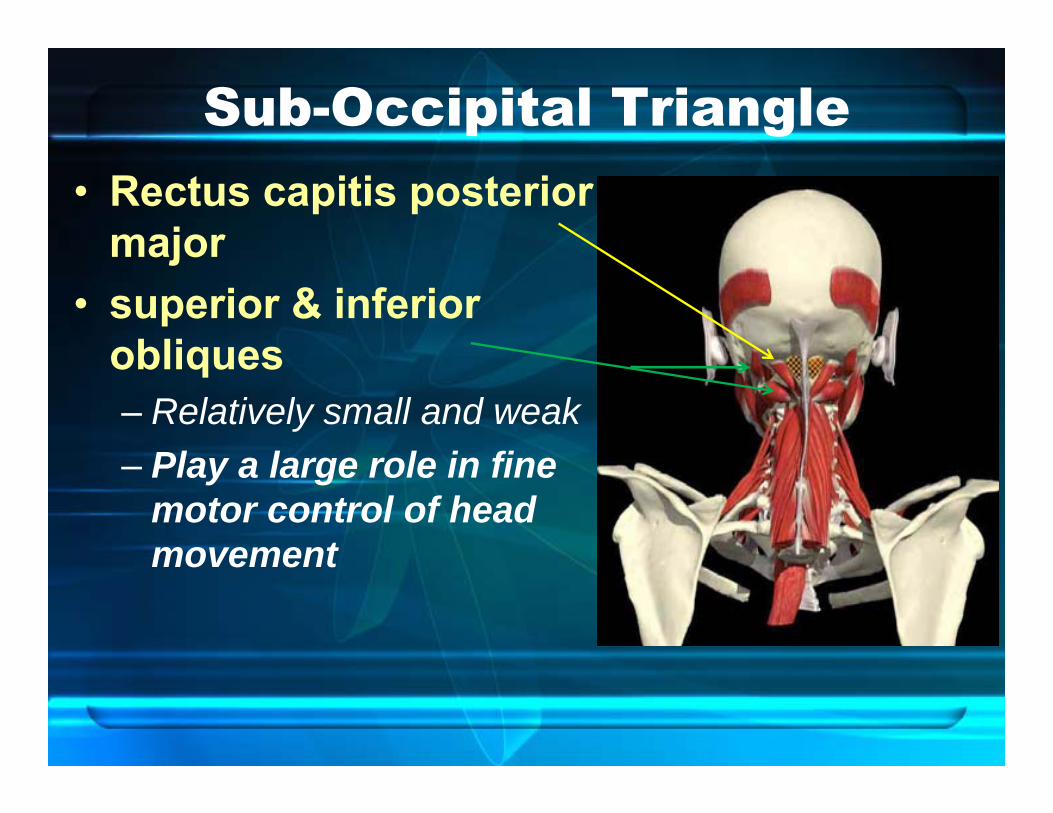
Sub-Occipital Triangle• Rectus capitis posterior
major• superior & inferior
obliques– Relatively small and weak – Play a large role in fine
motor control of head movement
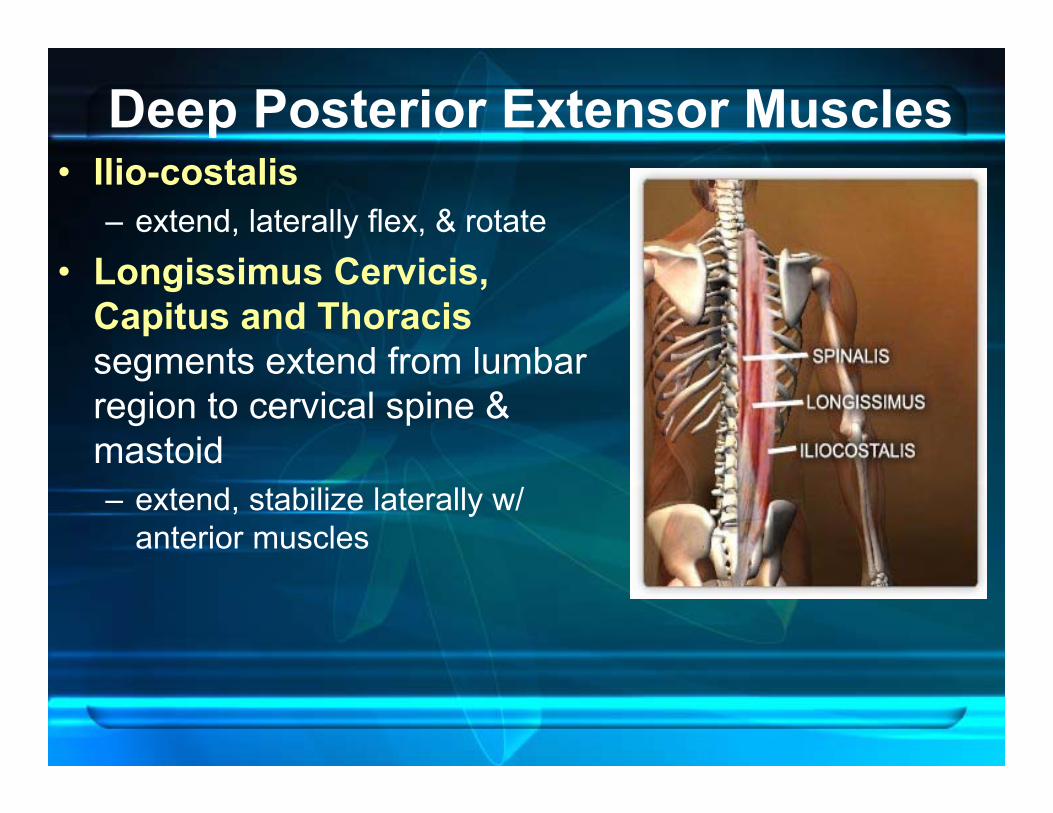
Deep Posterior Extensor Muscles• Ilio-costalis
– extend, laterally flex, & rotate • Longissimus Cervicis,
Capitus and Thoracis segments extend from lumbar region to cervical spine & mastoid– extend, stabilize laterally w/
anterior muscles
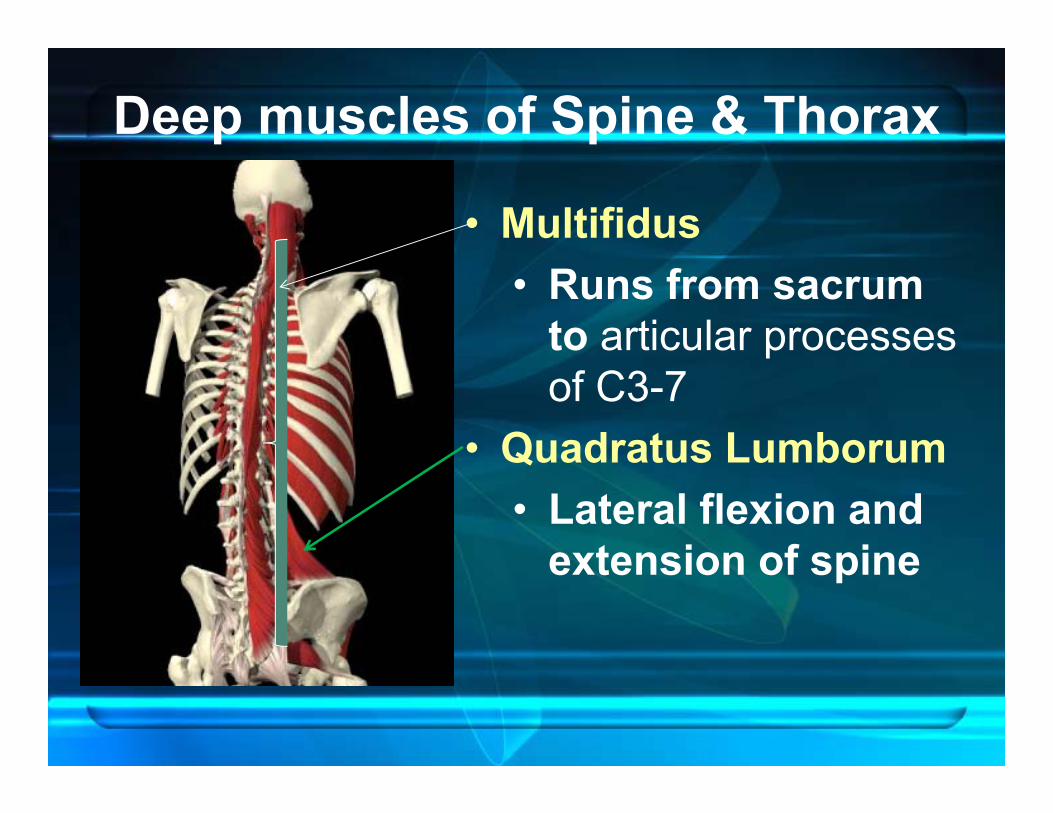
Deep muscles of Spine & Thorax
• Multifidus• Runs from sacrum
to articular processes of C3-7
• Quadratus Lumborum• Lateral flexion and
extension of spine
Common Symptoms in Patients:
• Inflammation/tenderness• Pain in neck & arm• Loss of pain-free motion• Difficulty sleeping• Headache

What is causing the pain?
• Facet Joints?• Intervertebral Disc?• Ligaments?• Muscles?
“Neither palpation tenderness, nor cervical ROM have been strong predictors of pain & disability in subjects with neck pain.”
Olson et al. 2000
Cervical Motion Segment (CMS)• Models created to test role of ligaments, facet
joints & discs:1. If CMS has: [all anterior elements + 1 post.
element], or [all posterior elements + 1 ant. element], then CMS remains stable in sagittal plane under load.
2. Flexion stability is preserved with severing of posterior ligaments & capsular ligaments.

CMS Models– Facet Joint
3. Bilateral resection of >50% of facet jointcompromises shear strength of CMS.
4. Under torsion, rotational displacement >20% after a 50% resection of facet capsule.
Ref : Teo & Ng 2001
Effect of Sagittal Forces on CMS• Discs less significant• Ligaments & facets play larger role for
stabilization• Without Ligaments:
– More flexible in flexion vs. extension – Under extension, facets play greater role
Effect of Sagittal Forces on CMS
• Removal of both ligaments & facets— in extension, get
instability!

Role of Disc, Facets & Ligaments• Ligaments
– resist cervical flexion• Disc nucleus
– controls compressive loads– provides initial stiffness under
flexion/ extension loads• Facet joints
– more important in resisting compression at higher loads, & resisting extension.
(Teo & Ng 2001)

Importance of Facet Joints• Cervical coupled motions = result of intact
vertebral ring & combination of 2 facet joints
• Intact Vertebral Ring & Facets are necessary for lateral bending & rotational stability (Teo & Ng 2001)

Directional Coupled movements in Cervical Spine
• Right lateral bending coupled w/ Rightrotation in C2- C7
Cook, et al. Journal of Manipul. & Physiol. Therapeutics, Sept. 2006

Interfacet AnglesControl how strictly lateral flex & rotation are
coupled in cervical spine:• At C1-C2, facet surfaces are nearly flat • At mid C-spine:• Unusual combo of disc-
facet & inter-facet angles (~ 45º) may allow excessive motion
(Thoracic angle 60º, Lumbar 90º)
(Milne 1991)

Effects of C5-6 DDD• Causes decreased segmental flexibility, esp. in
flexion• Causes changes in disc pressure & facet load:
– Higher in lateral bending & axial rotation– Posterior facets more affected than discs
**RESULT:DDD may increase risk of overloading posterior
facet joints & contribute to DJD in facet joints(Hussain, M., et al., Spine Journal, Dec. 2010.)

Does Fusion Affect Stability in CMS?• There is a nonlinear rise of deformation forces
in ligaments & discs at other levels– Segments immediately adjacent to fused lower
CMS are next most likely to show degeneration– Will cause fairly uniform increase in motion across
all remaining segments– Rotation axes may shift after fusion
• may alter load transfer especially about the fusion.
– Higher loads may be concentrated at smaller regions. (Fuller et al. 1998)

Effects of Aging
“How old would you be if you didn’t know how old you are?”
-Satchel Paige

Effects of Aging on Tissues• ↓ in muscle mass &
strength• ↓ in joint motion• ↓ in H2O content of inter-
vertebral discs• ↓ bone density
(osteoporosis)• Softening of articular
cartilage
Evidence suggests that exercise helps maintain joint motion, increase strength, & decrease rate of bone loss, thus reducing risk of falls in the elderly.
(Schenkman 1996; Petersen 2004)

Effects of Aging on Information Processing
Response & movement time slows due to:
1. Decline in sensory receptor function– due more to CNS processing than
Peripheral 2. Altered movement response
selection3. Difficulty programming new
movements

Aging & Response Programming
“Even though general response speed declines with age, functional performance speed is a reasonable goal with the elderly.”
• Practice improves movement and response time in the elderly.– Therapy can train response using gradual increased task
complexity
(Light 1990)
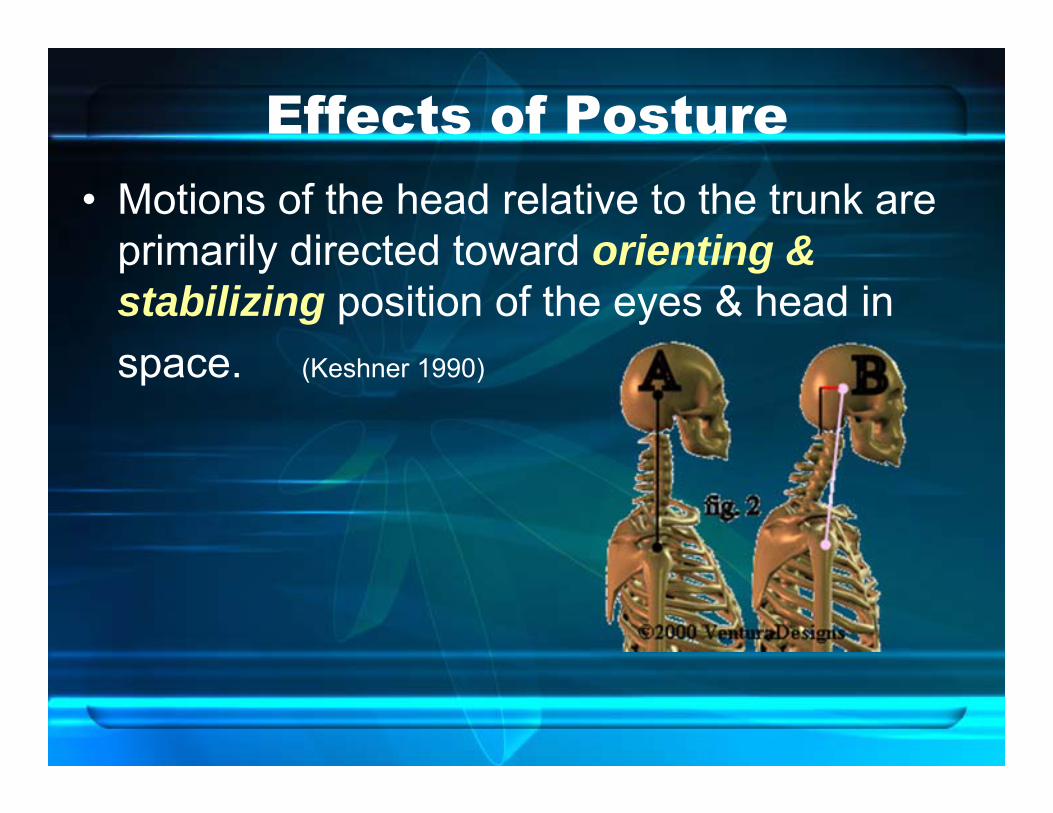
Effects of Posture• Motions of the head relative to the trunk are
primarily directed toward orienting & stabilizing position of the eyes & head in space. (Keshner 1990)

Upper Crossed Syndrome
• Pattern of weakened & shortenedmuscles in upper body due to postural changes
• Produces overstress at Cervical-Cranial junction, C4-5 & T4 segments, and the shoulder joint
• Leads to premature joint degeneration
(Model developed by Janda)
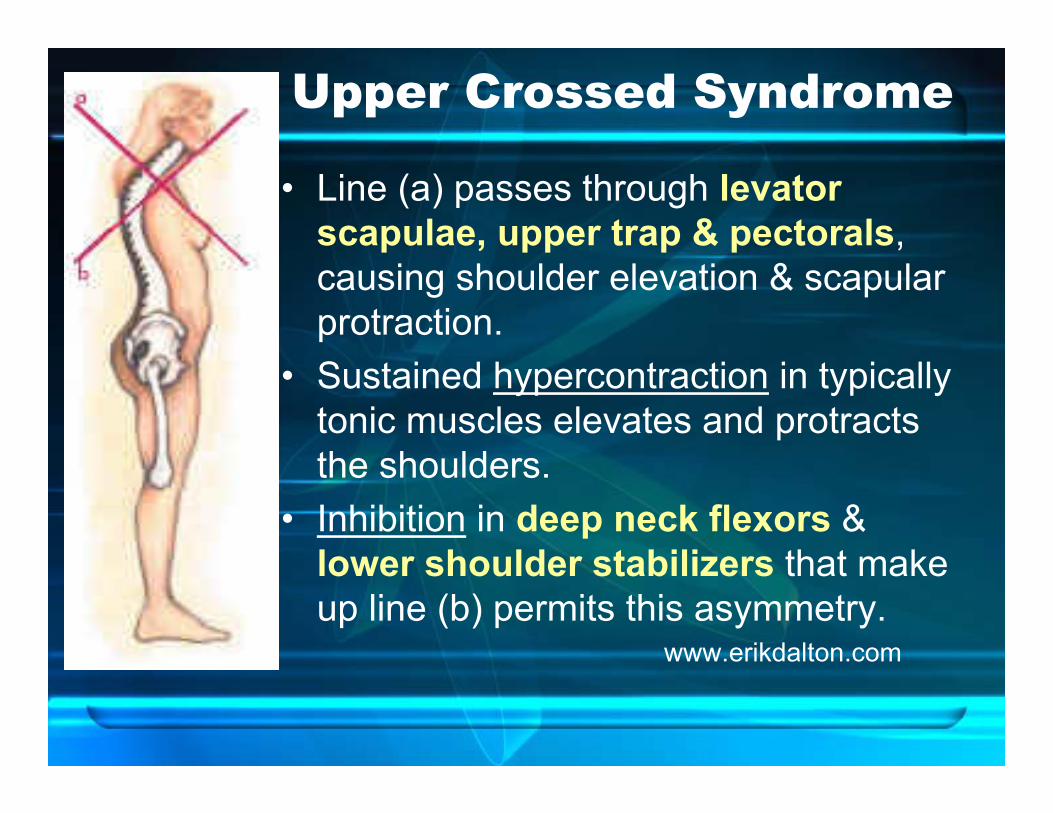
Upper Crossed Syndrome
• Line (a) passes through levator scapulae, upper trap & pectorals, causing shoulder elevation & scapular protraction.
• Sustained hypercontraction in typically tonic muscles elevates and protracts the shoulders.
• Inhibition in deep neck flexors & lower shoulder stabilizers that make up line (b) permits this asymmetry.
www.erikdalton.com
Morning Break
LAB 1-A: Palpation & Posture Assessment

Aspects of Good Posture• Minimum of muscle force• Balance between agonist & antagonist
muscle groups• Sufficient “relative flexibility”• Adequate coordination of movement• Well-developed postural reflexes
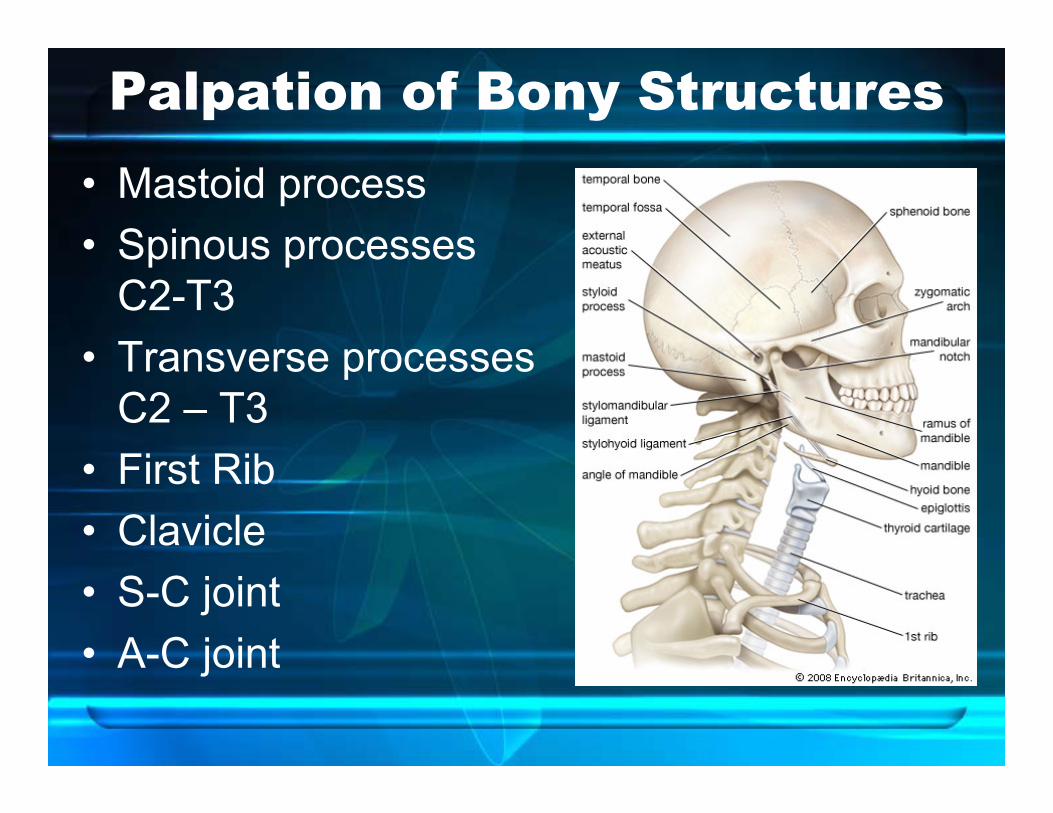
Palpation of Bony Structures• Mastoid process• Spinous processes
C2-T3• Transverse processes
C2 – T3• First Rib• Clavicle• S-C joint• A-C joint
Gross Muscle Testing• Chin Tuck/Flexion (C1-2)• Push Head Up (C1-2)• Sidebend (C3)• Upper Traps (C4)• Deltoid (C5)• Biceps (C5-6)• Wrist Extension (C6)• Triceps (C7)• Extensor Pollicis Longus (C8)• Lumbricals (T1)

Special Tests
• Axial Compression & Distraction test
• Spurling’s Test

Jull’s TestOld test: Head lift• Maximum load on muscles to lift head• Superficial muscles provide 83%of Cervical flexion:
– Ant. Scalenes– SCM
• Deep neck flexors provide only 17%!!

New Test: CCFT• Use Pressure biofeedback at 20 mm Hg• 5 stages w/ progressive +2 mm pressure
increases Level 1 thru 5 • [ 22 –24 – 26 - 28 - 30 mm Hg ]• Hold 10 sec. x 10 reps• Progress to next level if 3 successful trials.

Scoring CCFT• Activation Score = which level achieved?
– 2 to 10 mm Hg (Level 1 thru 5)• Performance Index =
Activation Score x # trials held 10 sec.
Example: If performed 6 trials at Level 2 (24 mm Hg) without substitution pattern,
Perform Index = 4 x 6 = 24
Ref: G. Jull, et al., Sept 2008, J Manip & Physio Ther.
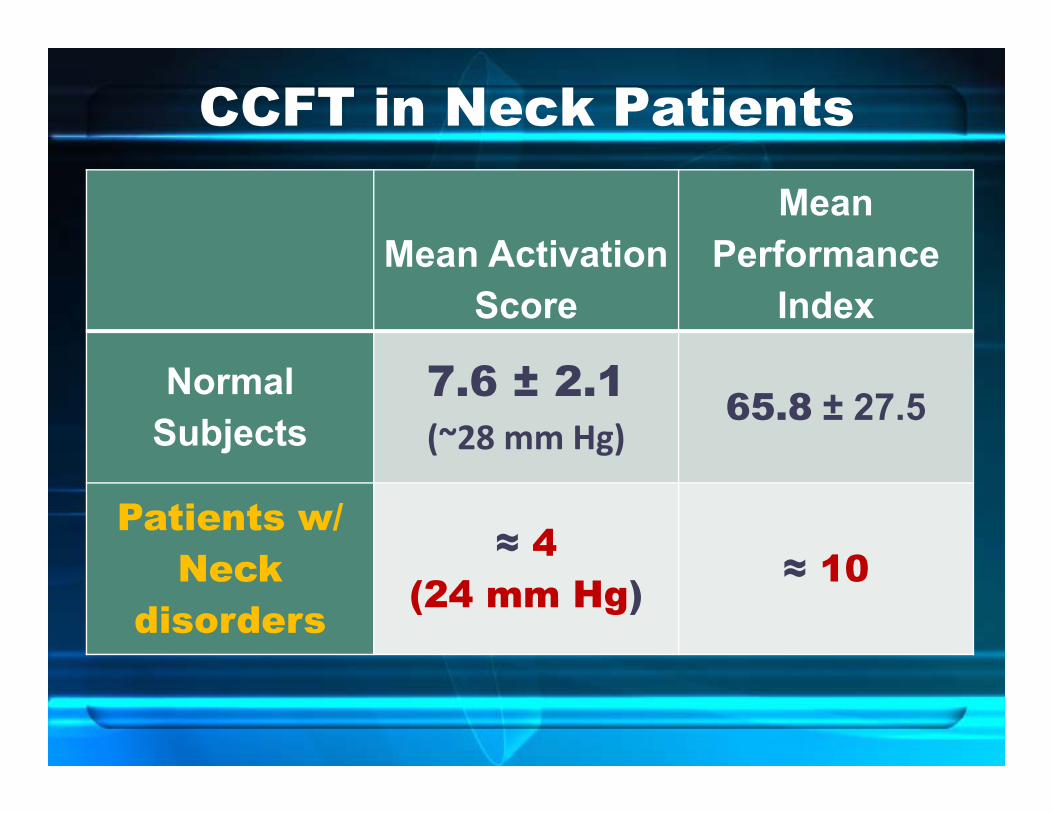
CCFT in Neck Patients
Mean Activation Score
Mean Performance
Index
Normal Subjects
7.6 ± 2.1(~28 mm Hg)
65.8 ± 27.5
Patients w/ Neck
disorders
≈ 4(24 mm Hg) ≈ 10
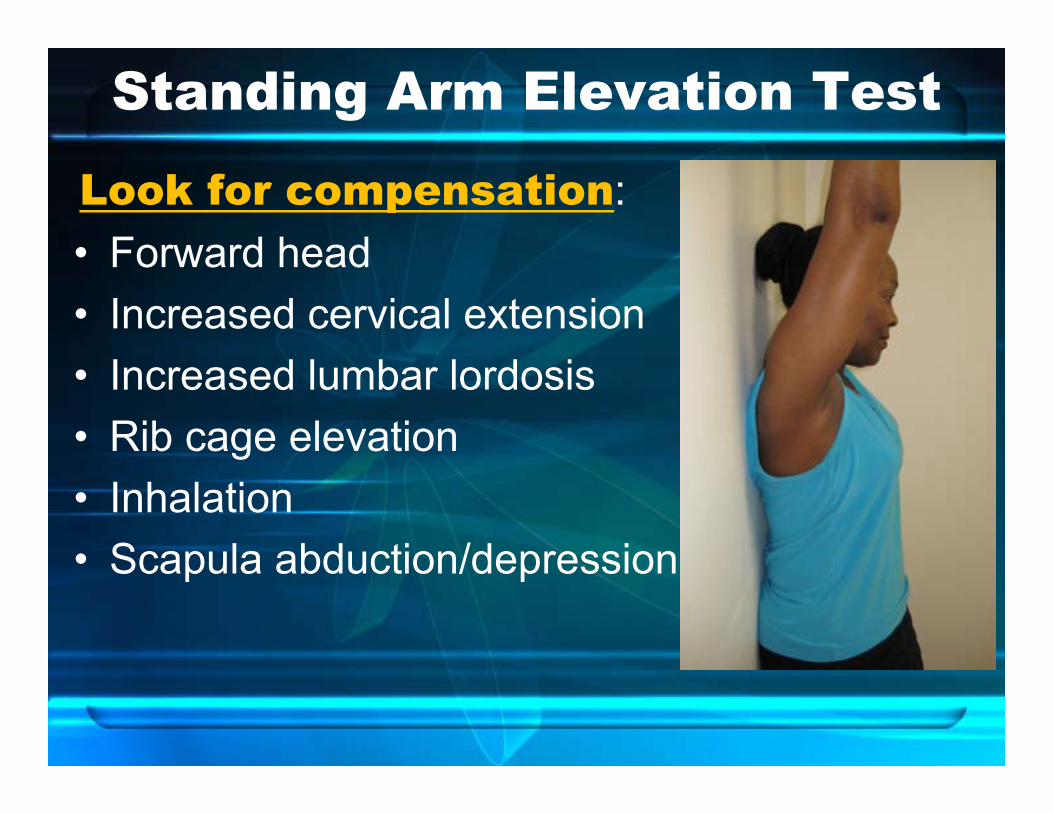
Standing Arm Elevation Test
Look for compensation:• Forward head• Increased cervical extension • Increased lumbar lordosis• Rib cage elevation• Inhalation• Scapula abduction/depression
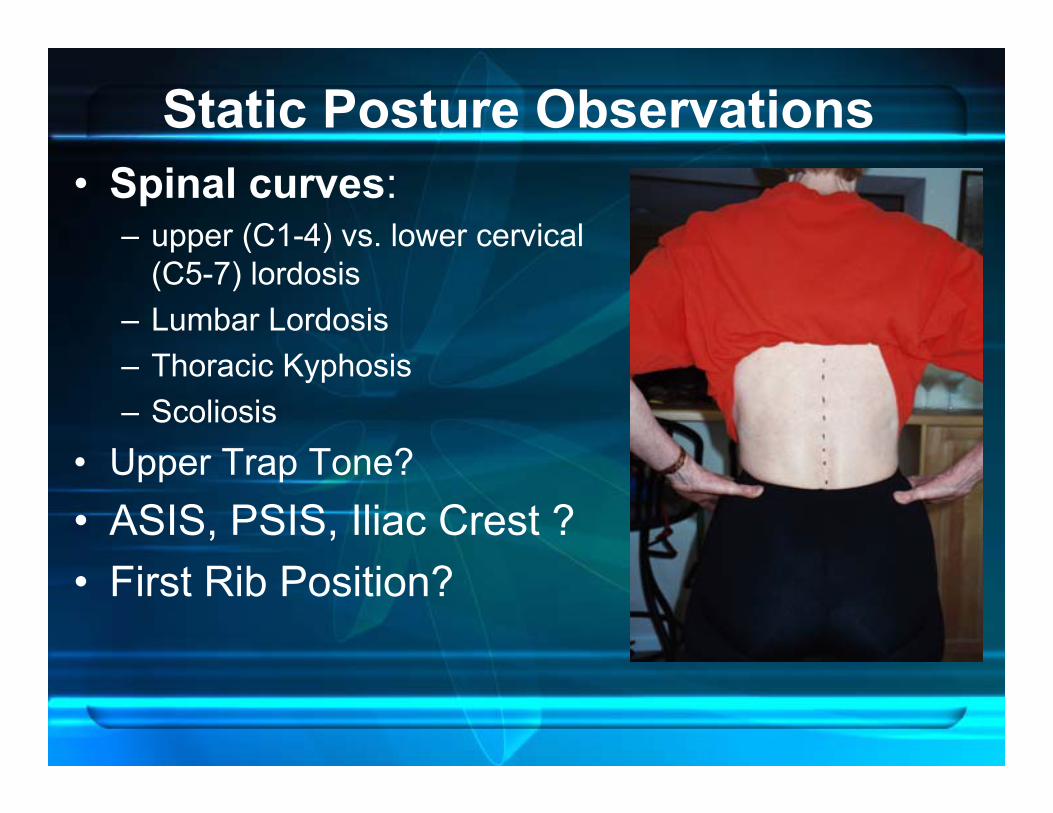
Static Posture Observations• Spinal curves:
– upper (C1-4) vs. lower cervical (C5-7) lordosis
– Lumbar Lordosis– Thoracic Kyphosis– Scoliosis
• Upper Trap Tone?• ASIS, PSIS, Iliac Crest ?• First Rib Position?
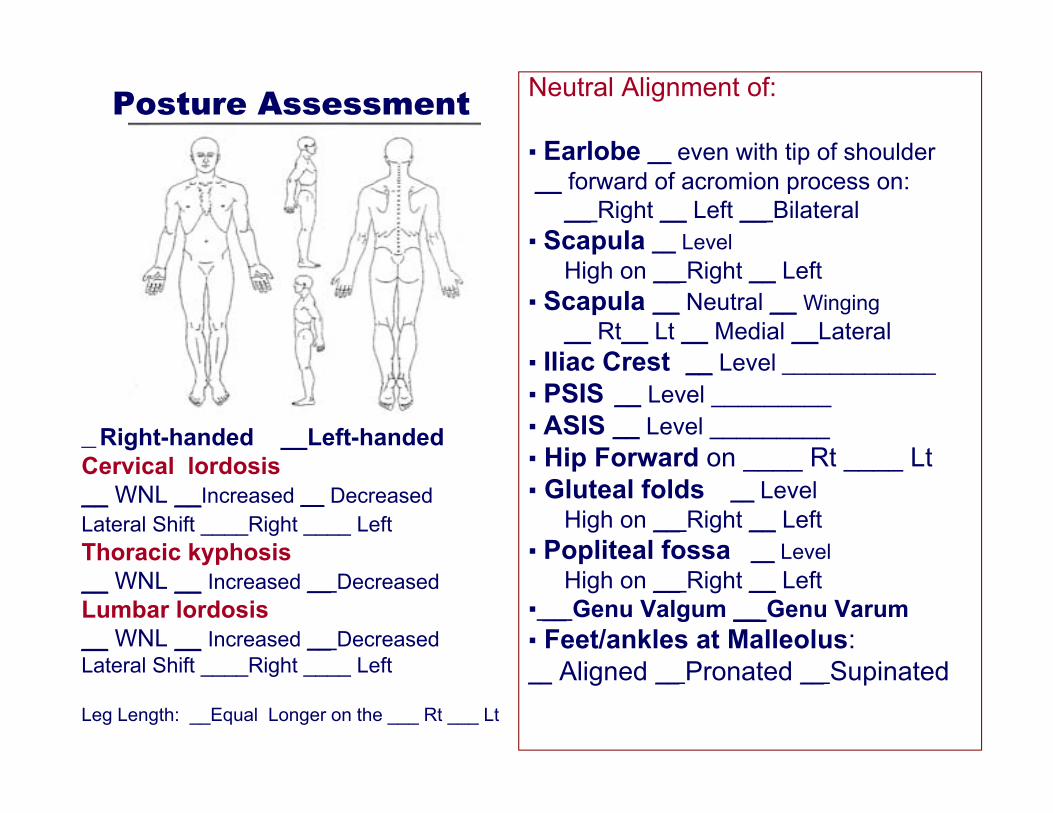
Posture Assessment
__ Right-handed __Left-handedCervical lordosis__ WNL __Increased __ DecreasedLateral Shift ____Right ____ LeftThoracic kyphosis__ WNL __ Increased __ DecreasedLumbar lordosis__ WNL __ Increased __ DecreasedLateral Shift ____Right ____ Left
Leg Length: __Equal Longer on the ___ Rt ___ Lt
Neutral Alignment of:
▪ Earlobe __ even with tip of shoulder__ forward of acromion process on:
__ Right __ Left __ Bilateral▪ Scapula __ Level
High on __ Right __ Left▪ Scapula __ Neutral __ Winging
__ Rt__ Lt __ Medial __Lateral▪ Iliac Crest __ Level _____________▪ PSIS __ Level _________▪ ASIS __ Level _________▪ Hip Forward on ____ Rt ____ Lt ▪ Gluteal folds __ Level
High on __ Right __ Left▪ Popliteal fossa __ Level
High on __ Right __ Left▪ __ Genu Valgum __ Genu Varum▪ Feet/ankles at Malleolus: __ Aligned __ Pronated __ Supinated

Right concavity@
Right Concavity @ T 5-6
Left concavity @ L3-4
Right concavity@
T 5-6
Right concavity@
Notation for Scoliosis or Lateral Curvature
Shoulders higher on Left
Hips higher on Right

Scapular static position• Level? Test for Winging:• Medial--wall pushup• Is Medial border more
prominent?• Lateral--
arm abduction to 90º • Is Upper Trap flat?• Is Lateral border more
prominent?

Scapular Balancing Index6-part test— degree of Scapular
Control:1. Lateral Scapular Slide Test2. Neuromuscular Evaluation
(PNF)3. Strength & Endurance (10
reps)4. Cervical Posture5. Thoracic Posture6. Thoracic Segmental MobilityTOTAL SCORE: Part 1-6= 0 - 20 points Brownstein & Bronner, 1997)

Common Surgical & Conservative Treatmentsin the Cervical-Thoracic
Spine

Posterior Cervical Laminectomy
Objective: remove lamina (& spinous process) to decompress spinal cord
• make trough in bilat. lamina before facet joint.
• Lamina with the spinous process can then be removed as one piece
Problem: Cervical stenosis places pressure posteriorly on the spinal cord

Cervical Discectomy• Relieves pressure on nerve
root by removal of disc anteriorly
• Each disc & vertebra are identified using X-ray; then,proper disc is removed
• Usually combined with anterior spinal fusion
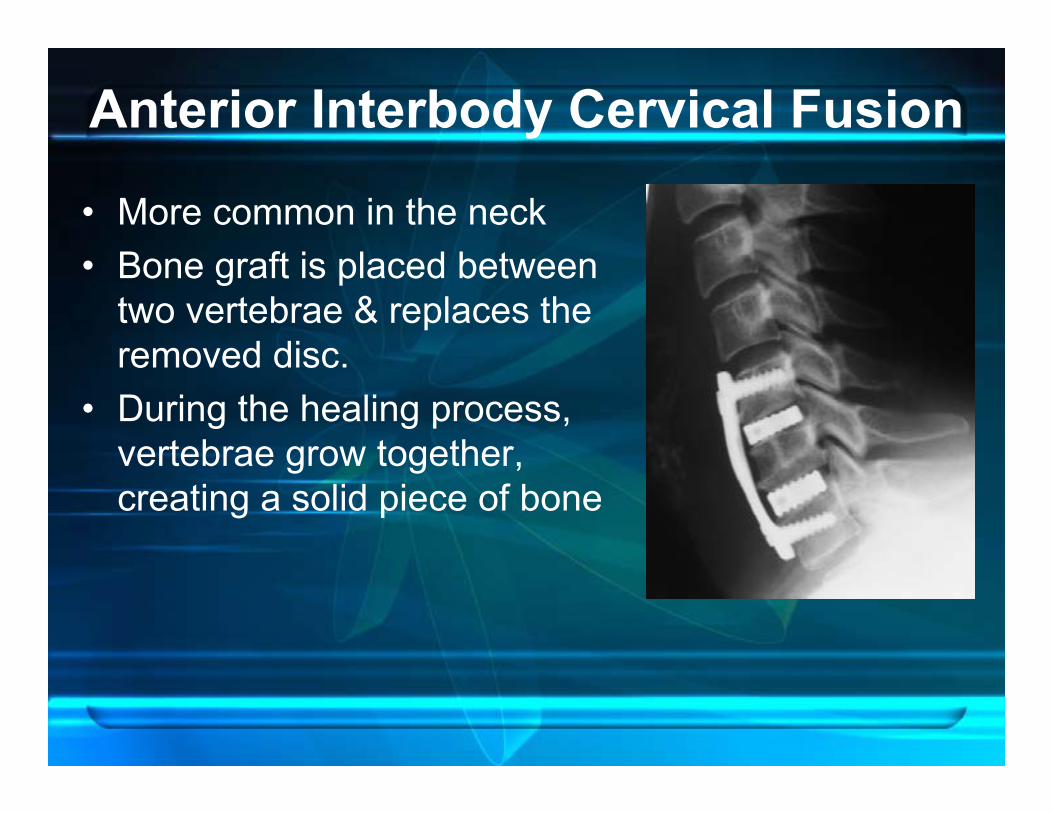
Anterior Interbody Cervical Fusion
• More common in the neck • Bone graft is placed between
two vertebrae & replaces the removed disc.
• During the healing process, vertebrae grow together, creating a solid piece of bone

Posterior Cervical Fusion• Bone graft is placed on posterior
aspect of the vertebrae.
• Recommended for several reasons: – To stop motion between two
or more spinal segments – To straighten C/S & stop progression of spinal
deformity – To stabilize C/S after a fracture or dislocation
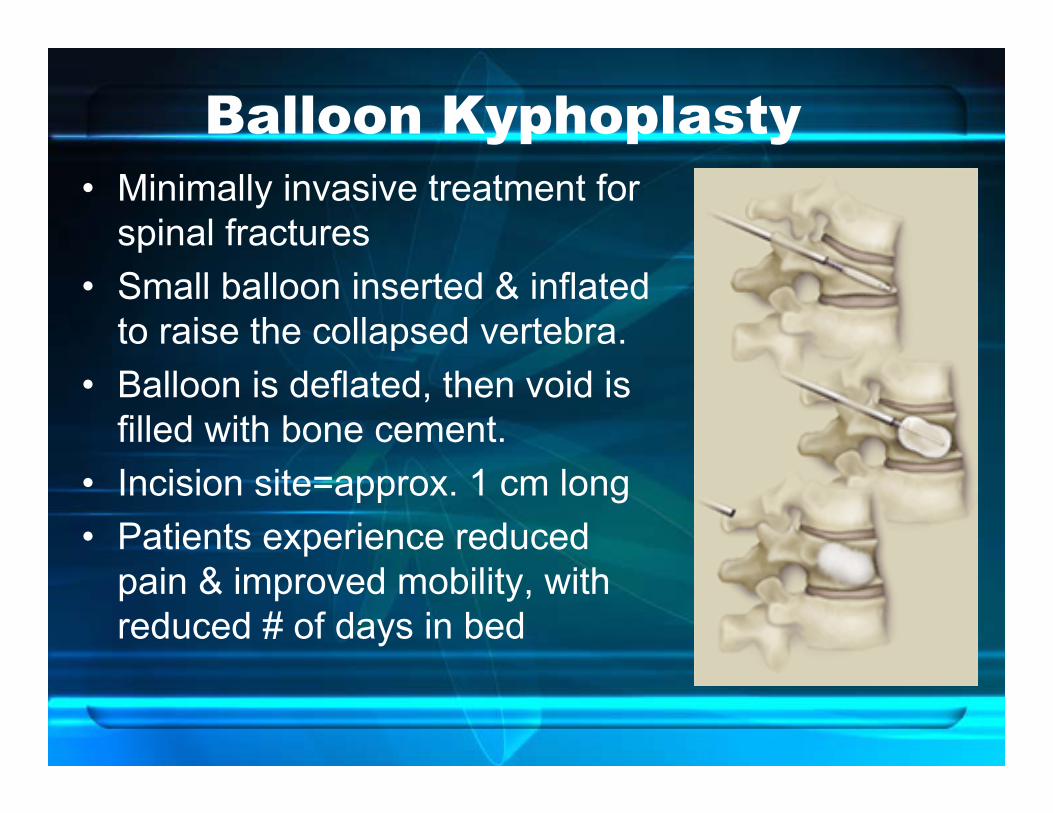
Balloon Kyphoplasty• Minimally invasive treatment for
spinal fractures • Small balloon inserted & inflated
to raise the collapsed vertebra.• Balloon is deflated, then void is
filled with bone cement.• Incision site=approx. 1 cm long• Patients experience reduced
pain & improved mobility, with reduced # of days in bed
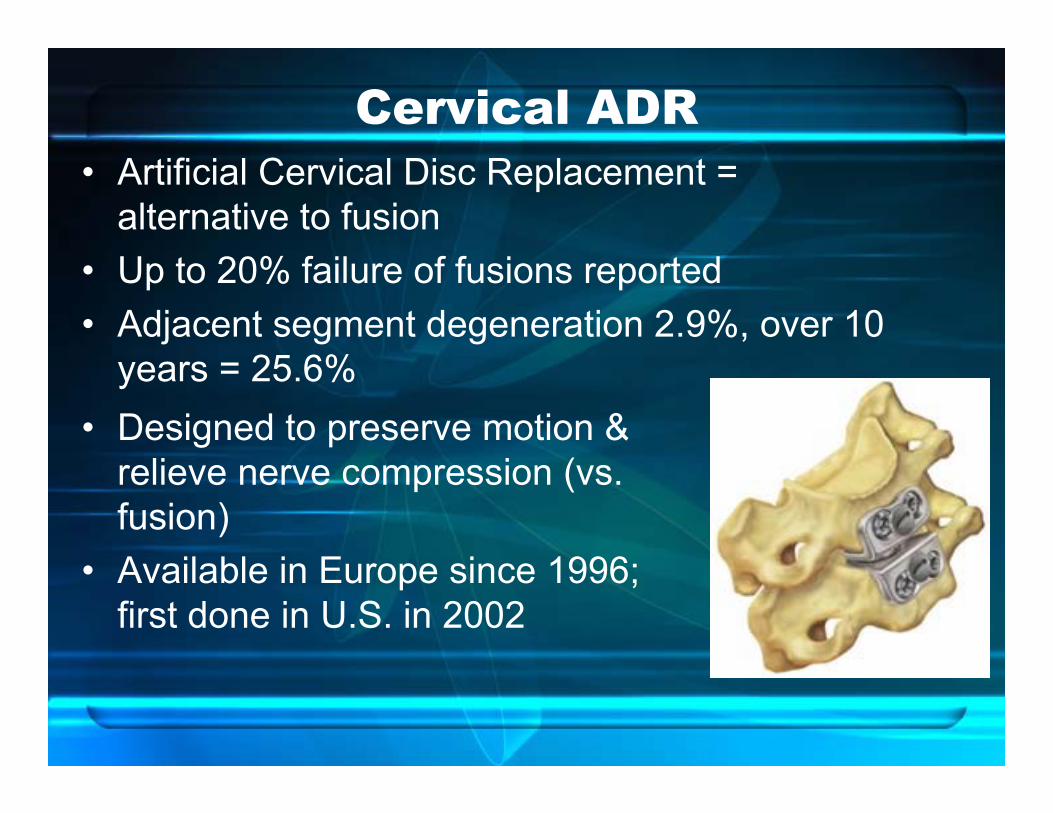
Cervical ADR• Artificial Cervical Disc Replacement =
alternative to fusion• Up to 20% failure of fusions reported• Adjacent segment degeneration 2.9%, over 10
years = 25.6%• Designed to preserve motion &
relieve nerve compression (vs. fusion)
• Available in Europe since 1996; first done in U.S. in 2002

Spinal Injections, etc.
• Facet Joint Injections– Inject steroid into the facet
joints or blocks of nerves that go to facets to relieve pain.
• Epidural Steroid Injection– given within the spinal canal
in series to decrease inflammation of nerves and other soft tissues
Trigger Point Injections
• Myofascial trigger points — hyper-irritable points in muscles & fascia with taut muscles
• Diagnosed by palpation— produce a local twitch response & a referred pain pattern distal to site of muscle irritability.
• A saline injection is usually paired with local anesthetic.

Botox Injections• Small doses of toxin are injected into affected
muscles. • Toxin binds to nerve endings, blocking the release
of acetylcholine, which would otherwise signal muscle to contract.
• Leaves the other muscles unaffected.• Pain-relief usually last for 4-6 months. • Injections "block extra contraction but leave
enough strength for normal use."Barbara Karp, M.D., deputy clinical director of NIH’s National Institute of Neurological Disorders & Stroke.

Acupuncture• Channels of energy (meridians) run in regular
patterns through the body & become blocked. • Needles are inserted, & heat
or electrical stimulation is applied at very precise acupuncture points.
• Stimulates the nervous system to release chemicals which influence the body’s own internal regulating system.

Neurological Effect of Acupuncture• Real-time functional brain MRI
images showed:– Superficial needling stimulated the
cortex, as would touch or pain– Deep needling deactivated the limbic
system in brain • Results indicate a mechanism for
pain relief via acupuncture.
www.bris.ac.uk/news/2006/889.html

Pain ReliefClinical Treatments

Common Modalities We Use• Moist heat• Cold therapy• Massage• Manual Therapy • Traction• TENS- Electrical Stimulation• Ultrasound• Cold Laser Therapy• Iontophoresis & Phonophoresis
Factors in Choosing a Modality• Structure causing the pain• Depth of treatment required• Bony tissue vs. soft tissue in
surrounding area • Patient tolerance to treatment &
positioning • Availability of modality• Cost-effectiveness of treatment• Time management issues

Iontophoresis• Uses small direct current (~ 0.5 mA/cm2) to
deliver medication through body tissues• Delivers to depth of 1-3 cm• Great for treating facet syndrome
Medications used to treat pain & inflammation:– Ketoprofen 10% (-)– Dexamethasone sodium phosphate 0.4% (-)– Diclofenac sodium 1% (-)

Manual Traction• Research shows no significant change in
upper trap tone after mechanical traction• Per Saunders: Use cervical manual traction
when trying to mobilize soft tissue or treat facet joint impingement.
• Advantage of manual traction: clinician can incorporate range of motion
When to Use Mechanical Traction
• Manual cervical traction is NOT effective for more severe HNP & nerve compressions – not possible to sustain force long enough to
obtain adequate separation of vertebral bodies– X-ray studies show visible separations of
cervical segments with mechanical traction forces of 25-50 lbs
1 Hour LUNCH BREAK

Lab 2: Treatment TechniquesModalities & Hands-On
Treatment
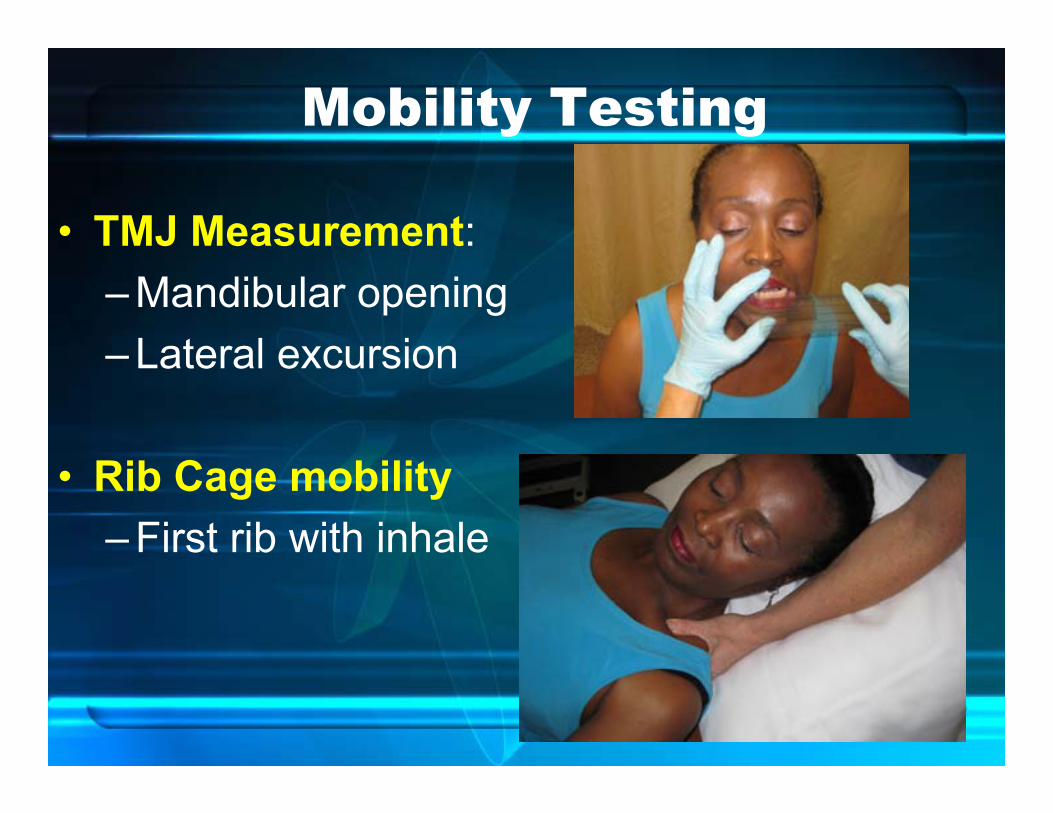
Mobility Testing
• TMJ Measurement:– Mandibular opening– Lateral excursion
• Rib Cage mobility– First rib with inhale

C-T Junction Mobilization• With cervical rotation & arm elevation
– “Arm Pit Sniff” MET

Passive Release Techniques
• Levator Scapula & Upper Trap
• Subscapularis & Serratus Anterior
• Rhomboids• Pectoralis
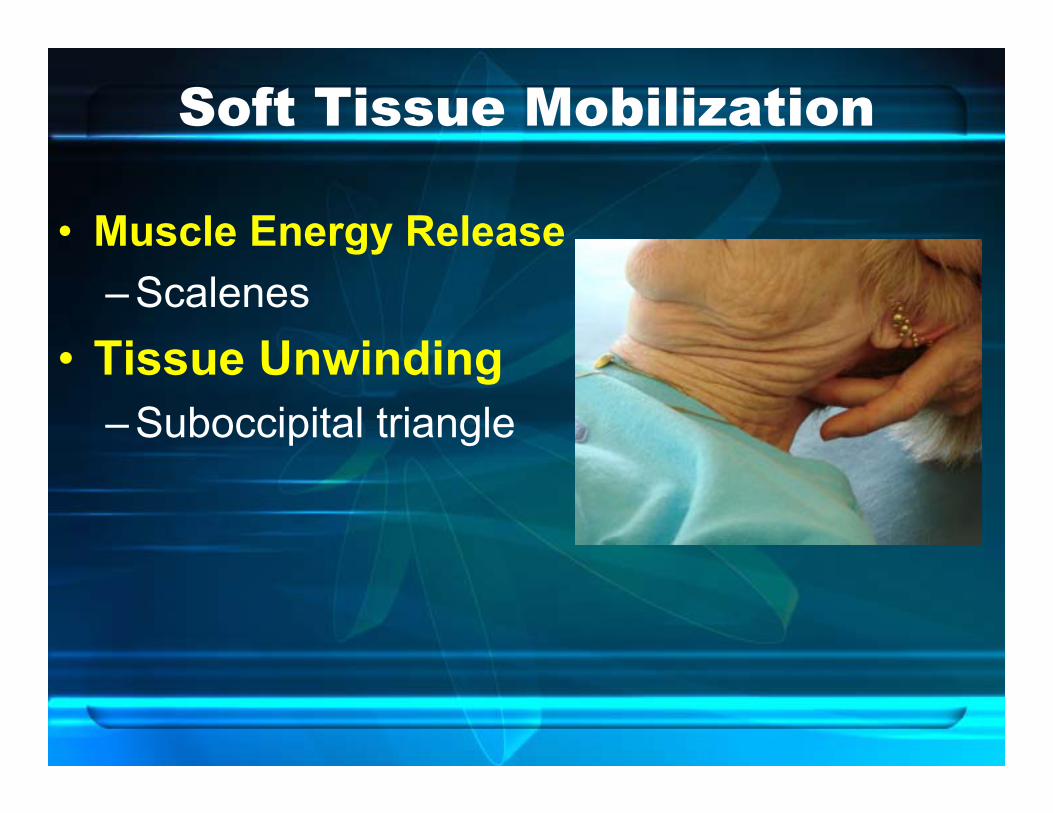
Soft Tissue Mobilization
• Muscle Energy Release– Scalenes
• Tissue Unwinding– Suboccipital triangle

Joint Play & NM Re-Ed
• Palpate transverse processes
• Translate right/left at each segment with facets OPEN
• Check for asymmetry

Mobilization with MovementTreatment:1. Submax. Isometric Hold
– with translation maintained2. AAROM:
– assist SB (≤10º), back to center
3. Resist ROM: – AAROM to SB ≤10º– resist back to center while
monitoring segment

Neuromuscular Re-Education
Clinical Applications & Treatments
• With decreased proprioception after injury or inactivity:– ↓ tonic (SMU) muscle recruitment – hyperactivity in global phasic (FMU) muscles– » INSTABILITY!
• Need to retrain SMU to improve stability• Recognize substitution patterns & retrain
early and often
Neuromuscular Re-Education

Common Substitution Patterns in Cervical & Scapular Regions
• Increased upper trap tone & scapular elevation/ant. tilt/ abduction
• Poor control of scapular depression, retraction, & adduction
• Hyperactivity in extensor muscles• Weakness in deep neck flexors

from Jeffrey R. Cram, Ph.D.Sierra Health Institute, Nevada City, CA

BiofeedbackFacilitation of:• deep neck flexors, scapular depressors,
shoulder external rotators, transverse abdominus, obliques & gluteal muscles
Inhibition of:• neck, thoracic and lumbar extensors• Upper trapezius

Specialized Taping
Fig. 2-- Facilitate Shoulder External Rotation & Scapular Depression ►
◄Fig. 1-- Inhibit UT elevation & facilitate Scapular depression

Kinesio Taping• Inhibit UT tone • Inhibit Para-spinal Extensor tone• Support damaged/strained muscle
tissue

Shoulder Kinesiotaping

Biofeedback for Re-education
• Pressure Biofeedbackteaches patients how to activate stabilizers with right amount of force
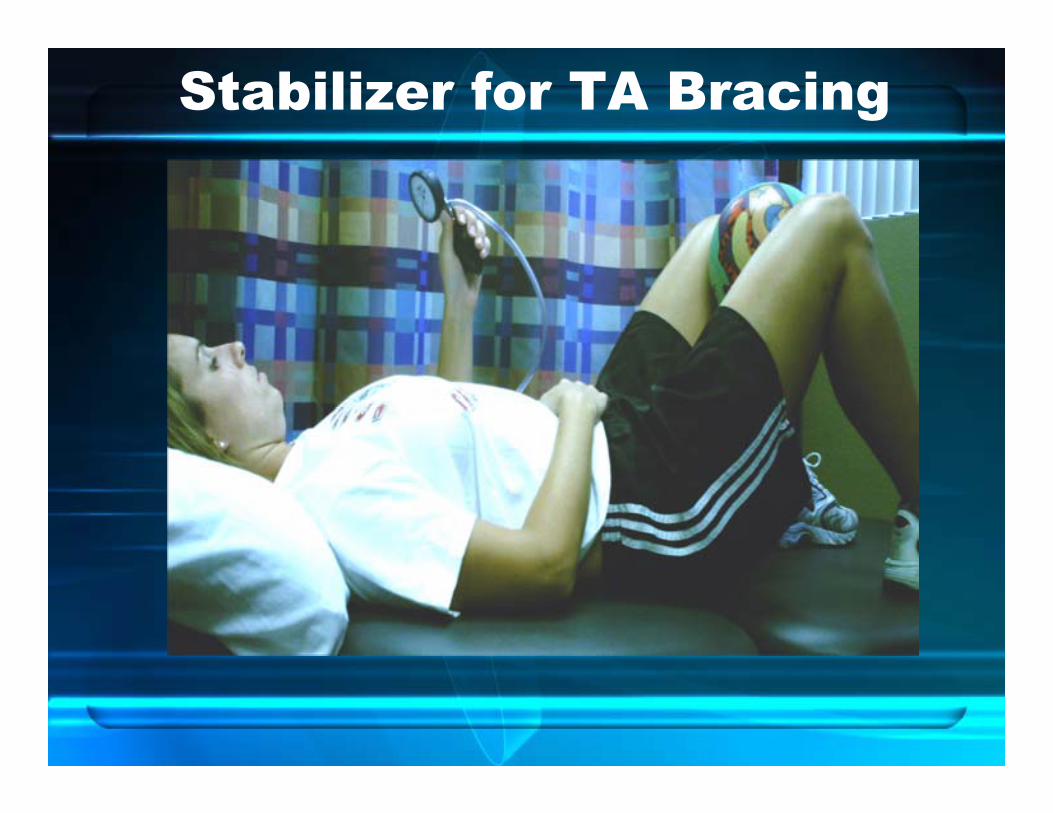
Stabilizer for TA Bracing

Deep Neck Flexors
• Fold Stabilizer in three sections and fasten with studs.• Place Stabilizer under neck and inflate to 20 mmHg. • Gently nod head as though saying "yes" without lifting
head. Increase the pressure 2mmHg and hold steady. • Relax and repeat, increasing at each target pressure to 30
mmHg. • Hold for 10-15 seconds, repeat 10 times on the highest
pressure target that can be held steady.

Other uses for Stabilizer• Scapular stabilization
with arm elevation:– Inflate to ~30 mm Hg– Maintain with AROM
• Scapular stabilization with 90/90 External Rotation:

15 Minute Afternoon
Break

Critical Links b/w Neck &Scapula
Pilates Principles–3 Postural Control Zones:
1. Head & neck 2. Shoulder girdle3. Pelvic girdle
• What stabilizers connect these zones?– Longus colli, Scalenus, SCM, Longissimus,
Spinalis & Multifidus help control rib cage.

Weak Links in the Stability Chain• Deep neck flexors• Co-contractions for lat flex & rotation in mid-
C/S during sagittal plane motion• Scapular & thorax/rib cage mobility during
arm elevation• Transverse Abdominus & Multifidus• Obliques• Gluteal muscles

Progression of Stabilization Exercises• Train Inner ROM for
Stability• Start with sub-maximal
Isometric holding– “Blockhead”
Exercise– Increase hold time, then
reps

Progression of Stabilization Exercises• Increase body weight to more
functional positions(standing/sitting)
• Include Rotation & Deceleration/Eccentriccontrol in all 3 planes
• Increase external loads (light dumbbells, medicine ball, tubing)

• Set your patient up for success—don’t progress too quickly
• Combine equipment to increase challenge
Progression of Stabilization Exercises

Lab 3: Stabilization Exercises
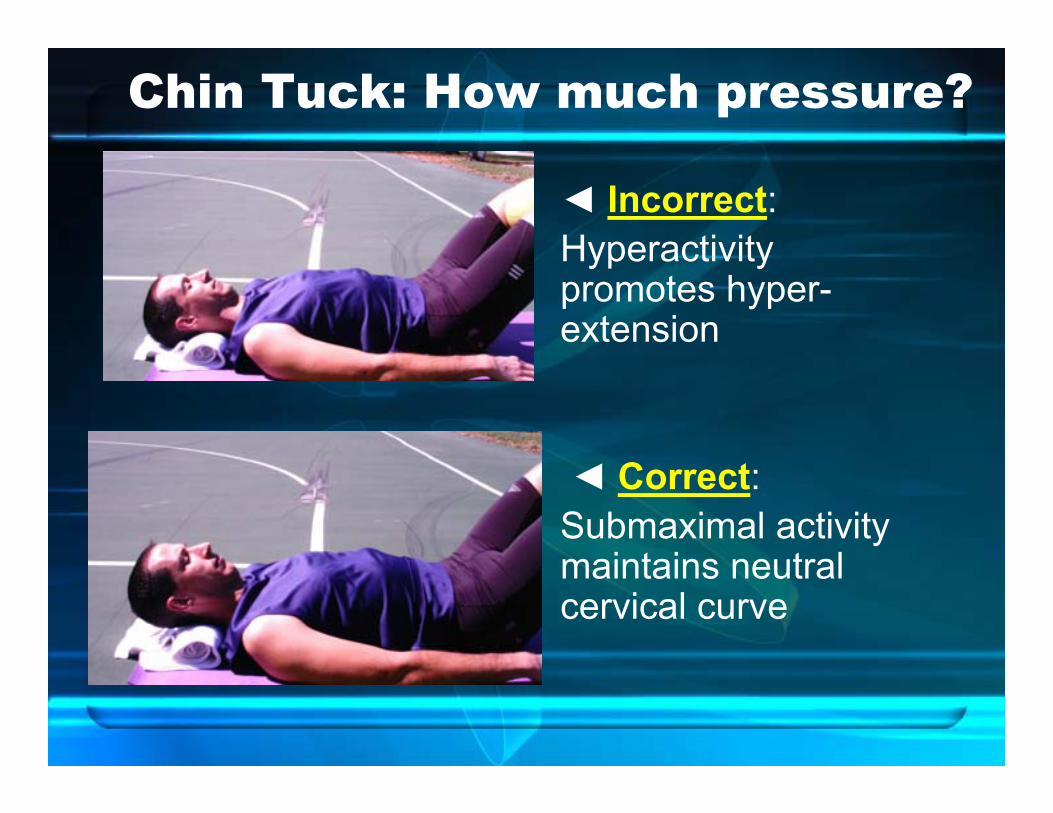
Chin Tuck: How much pressure?
◄ Incorrect:Hyperactivity promotes hyper-extension
◄ Correct:Submaximal activity maintains neutral cervical curve

Proper Chin Tuck Position◄ Incorrect: Chin “Jutting”
Correct ►Neutral Chin Tuck
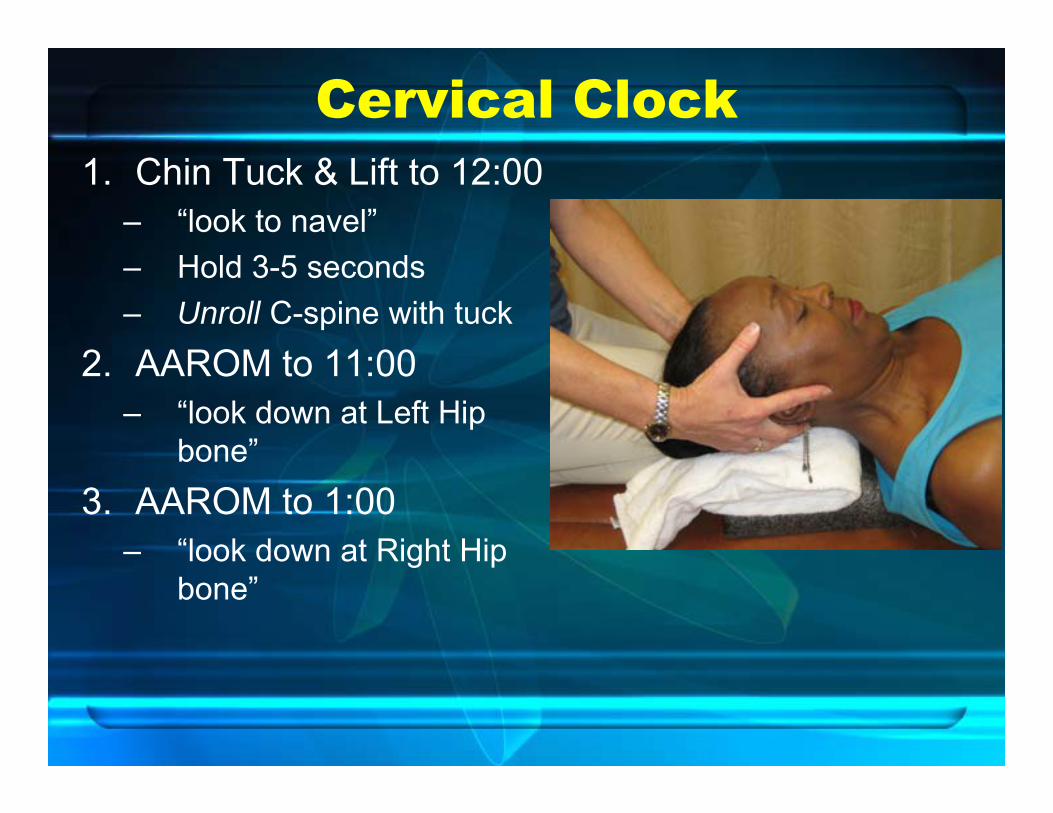
Cervical Clock1. Chin Tuck & Lift to 12:00
– “look to navel”– Hold 3-5 seconds– Unroll C-spine with tuck
2. AAROM to 11:00 – “look down at Left Hip
bone”3. AAROM to 1:00
– “look down at Right Hip bone”
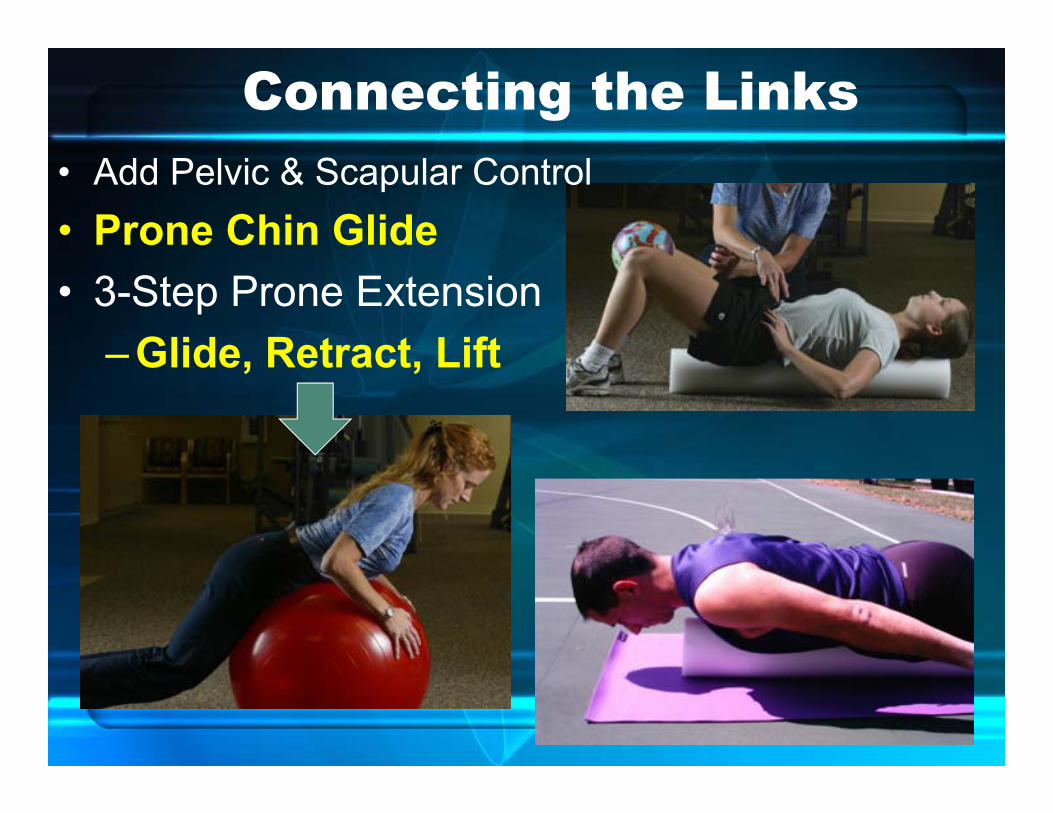
Connecting the Links• Add Pelvic & Scapular Control• Prone Chin Glide• 3-Step Prone Extension
– Glide, Retract, Lift

Posture Retraining & Scapular Mobilization
Snow Angels►
◄Chicken Wings
Butterflies ►
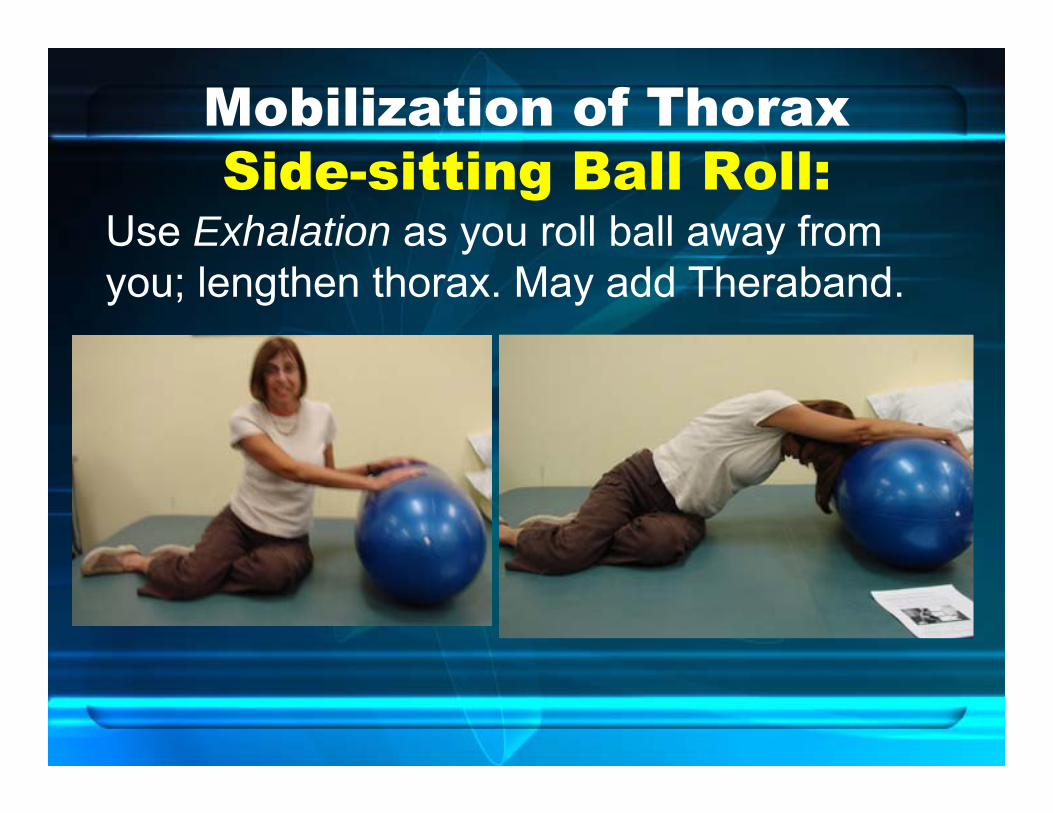
Mobilization of ThoraxSide-sitting Ball Roll:
Use Exhalation as you roll ball away from you; lengthen thorax. May add Theraband.

Kolar’s Wall Slide Position• Facing Wall, hands
under forehead, elbows outward
• Lean into wall, gaining thoracic extension
• Maintain neutral cervical spine with chin tucked down slightly

Yoga: Breathing Tall Stand Gull Modified Pose:• Stand with heels and toes
together, with fingers interlaced under chin, elbows inward as shown.
• Begin breathing in while raising elbows out to side.
• Exhale and bring elbows together in front.

Breathing Tall Standing Gull
Full pose:• Exhale and
pull elbows in• Extend head
back while exhaling.
Functional Integration Training
“FIT” Training– Adding the “core”

Scapulothoracic Control• Supine Punch Ups• Isometric Horizontal ABD• Alternate Arms-(“Monkey”)• Alternate Arms-”Clam”

Scapulothoracic Control• Modified Dead Bug • Quadruped
– Alt. arms– Alt. legs

Gliding Disc ExercisesClosed-Chain
Quadruped
“Swimming” over foam roll
# 1 # 2
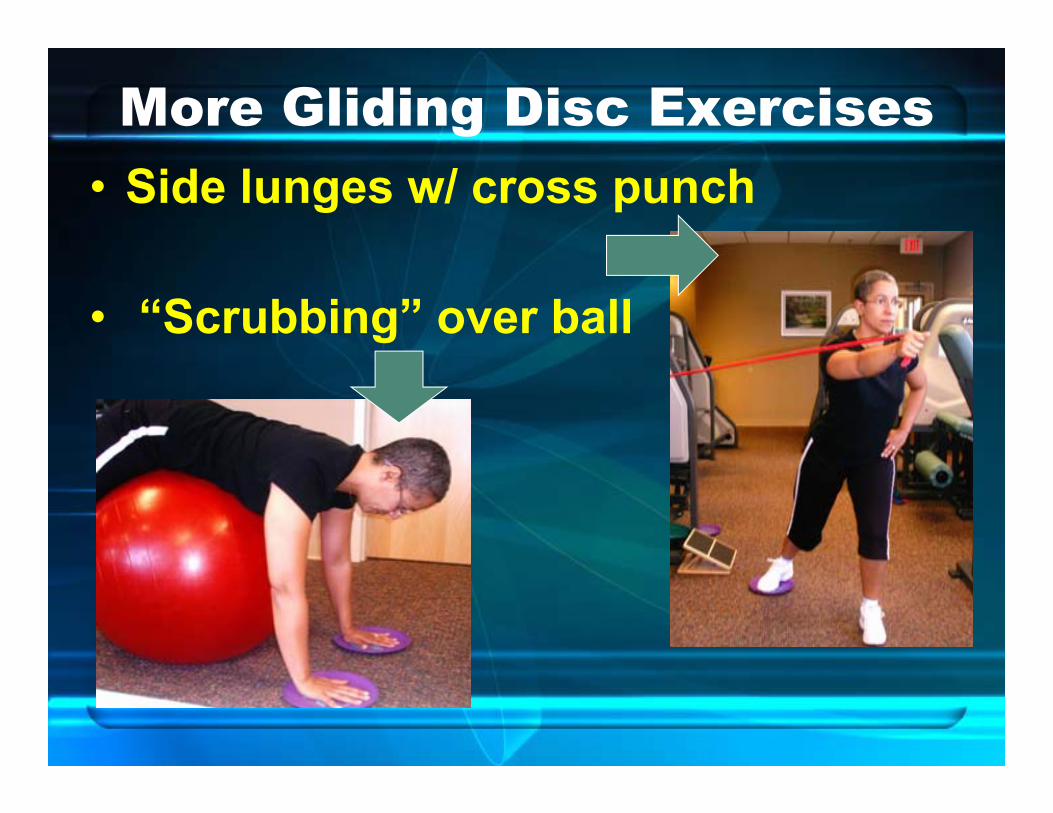
More Gliding Disc Exercises• Side lunges w/ cross punch
• “Scrubbing” over ball

Sidelying Thoracic & Oblique Control
• Sidelying Plank• Sidelying Leg Series
– Rotational control of trunk
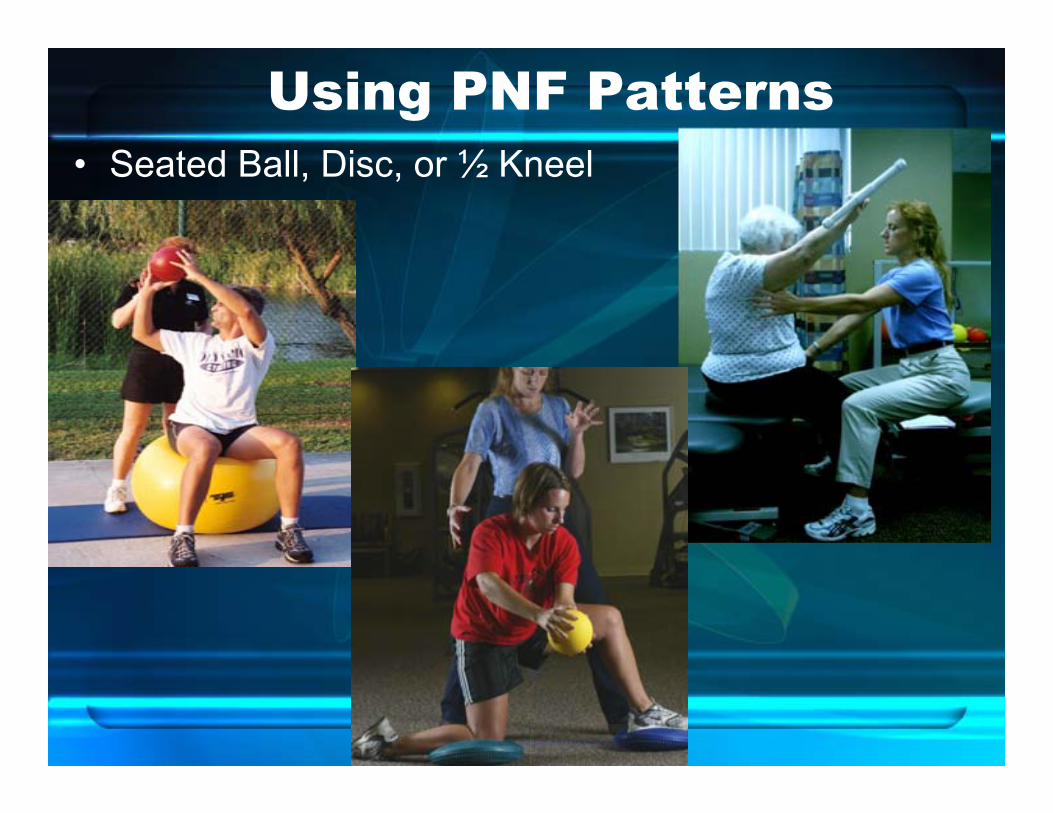
Using PNF Patterns• Seated Ball, Disc, or ½ Kneel

Standing Dynamic Stabilization
• Using Wobble Board: – Standing Rhythmic Stab– Mini Squat & Wt Shifting
--Side lunges
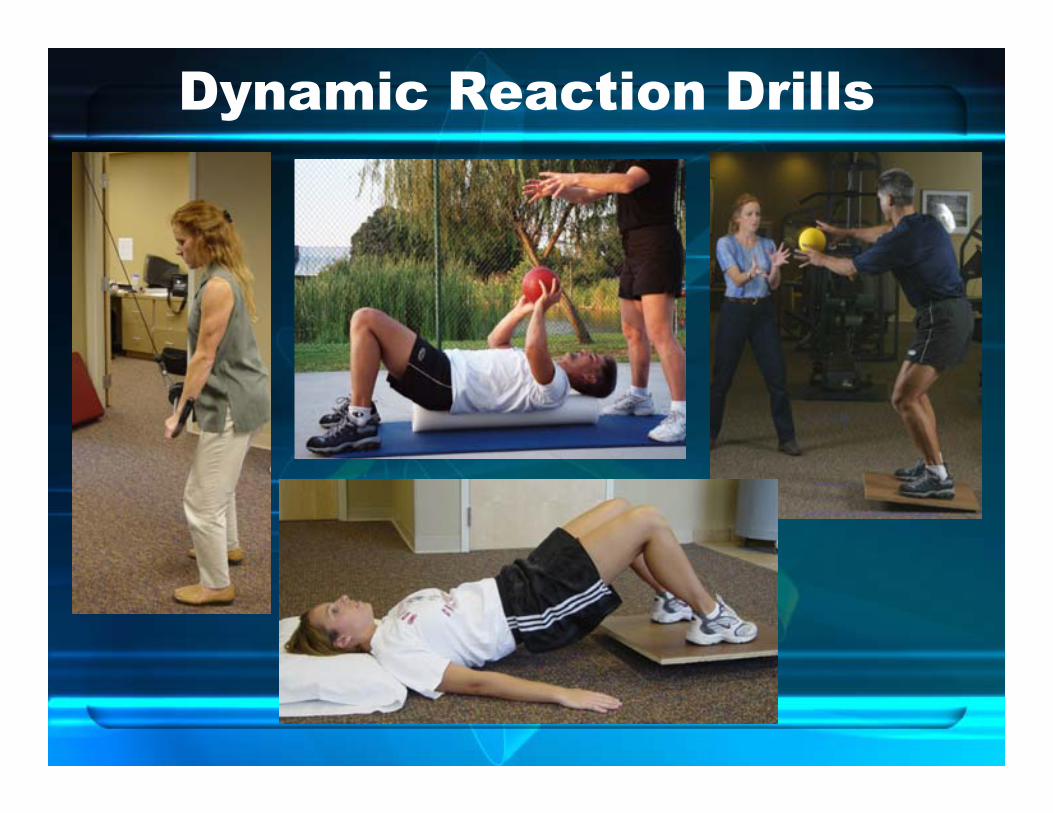
Dynamic Reaction Drills


















