Rhinitis, Other Upper Airway andOcular Disorders 25-32 A9-A11
Rhinitis, Other Upper Airway, Ocular Disorders,Aerobiology, Allergens and Allergen Extracts 33-40 A11-A14
Adverse Food, Drug and Insect Reactions,Anaphylaxis, Basic Science Allergyand Immunology 41-48 A14-A16
Clinical Immunology, Immunodeficiency,Other and Basic Science 49-56 A16-A19
Pharmacology, Pharmacotherapeutics,Asthma, Other Lower Airway Diseases 57-64 A19-A21
VOLUME 102, JANUARY, 2009 A1
ABSTRACTS: CONCURRENT SESSIONS
A2 ANNALS OF ALLERGY, ASTHMA & IMMUNOLOGY
ABSTRACTS: CONCURRENT SESSIONS
VOLUME 102, JANUARY, 2009 A3
1SPIROMETRY IN CHILDREN WITH PERSISTENT ASTHMAAND GASTROESOPHAGEAL REFLUX: BEFORE AND TWOYEARSAFTERANTI-REFLUXTREATMENT.A.K. Kobernick*1, V. Khoshoo2, R. Haydel1, 1. New Orleans, LA;2. Marrero, LA.
Introduction: Gastroesophageal reflux disease (GERD) has been implicatedin provoking asthma.The outcome of anti-GERD treatment on pulmonary func-tions in these children is not clear. Our objective was to assess pulmonary func-tions using spirometry in non-atopic children with moderate-persistent asthmaand GERD before and 2 years after anti-GERD treatment. Methods: Follow-ing IRB approval and informed consent, 62 non-atopic children (6-11 yrs) withmoderate-persistent asthma and no other risk factors underwent extendedesophageal pH monitoring. Forty-four children with abnormal studies sug-gesting GERD received either medical (n=32, Group A) or surgical (n=12,Group B) anti-GERD treatment. The remaining 18 patients continued theirasthma treatment and served as controls (Group C). Pulmonary functions wereassessed using spirometry before and after 2 years of treatment. Results: Despitereduced asthmamedications but with continued anti-GERD treatment, the num-ber of asthma exacerbations per patient per year in GroupA (0.61) and in GroupB (0.78) were comparable (p>0.05) but significantly lower (p<0.05) than inGroup C (2.9) who received only asthma medications. Greater than 20%improvement in FEV1 over the initial value (2 years earlier) was observed in15 of 32 (47%) children in group A, 7 of 12 (58%) children in group B, and 5of 18 (28%) children in control group C (Table 1). The proportion of childrenshowing this improvement was comparable in GroupsA and B but significantlymore than in Group C (p<0.05). After 2 years of treatment, greater than 20%improvement in FEF 25-75% was observed in 6 of 32 (22%) children in groupA, 3 of 12 (25%) children in group B, and 2 of 18 (11%) children in controlgroup C (Table 1). The FEF 25-75% for groups A and B were comparable butsignificantly higher than for Group C (p<0.05). Conclusions: After 2 years ofanti-GERD treatment in non-atopic asthmatic children with GERD there is asignificant improvement in pulmonary functions (p<0.05).
Patients with a more than twenty percent improvement in lung functions
Figures in parentheses denote percentages. Group A: medical anti-refluxtreatment. Group B: surgical anti-reflux treatment. Group C: control. Allpatients receieved asthma treatment
2LIVINGNEARFREEWAYSASSOCIATEDWITHPOORASTHMACONTROL.P.N. Huynh*1, C. Luu2, A. Ratnayake3, T. Morphew3, K. Kwong3, 1. SanMarino, CA; 2. NewYork, NY; 3. Los Angeles, CA.
Background: Living near heavy traffic has been linked to increasedasthma severity. However, it is unknown whether exposure to heavy trafficis associated with the ability to achieve and maintain asthma control. Objec-tives: This study examines whether exposure to heavy traffic is associatedwith the ability to achieve and maintain asthma control in inner city childrenenrolled in a pediatric asthma management program. Methods: 756 chil-dren with asthma were followed and engaged for 1 year in an asthma dis-ease management program. At each scheduled visit, physicians trackedpatients’ initial asthma severity (on first visit) and asthma disease activity(on subsequent visits) and managed their asthma based on 1997 NAEPPguidelines. The patients’ residential distance from the nearest freeway wascalculated based on residential address at study entry. Distance to the near-est freeway was used as a surrogate for high exposure from traffic relatedair pollutants. Patients were divided into two groups: the near group livedless than 2 miles from a freeway and the far group lived more than 2 milesfrom a freeway. Well controlled asthma was defined as maintenance of con-trol in more than 80% of follow-up clinic visits. Uncontrolled asthma wasdefined as maintenance of control 50% to 79.9% of follow-up clinic visits.
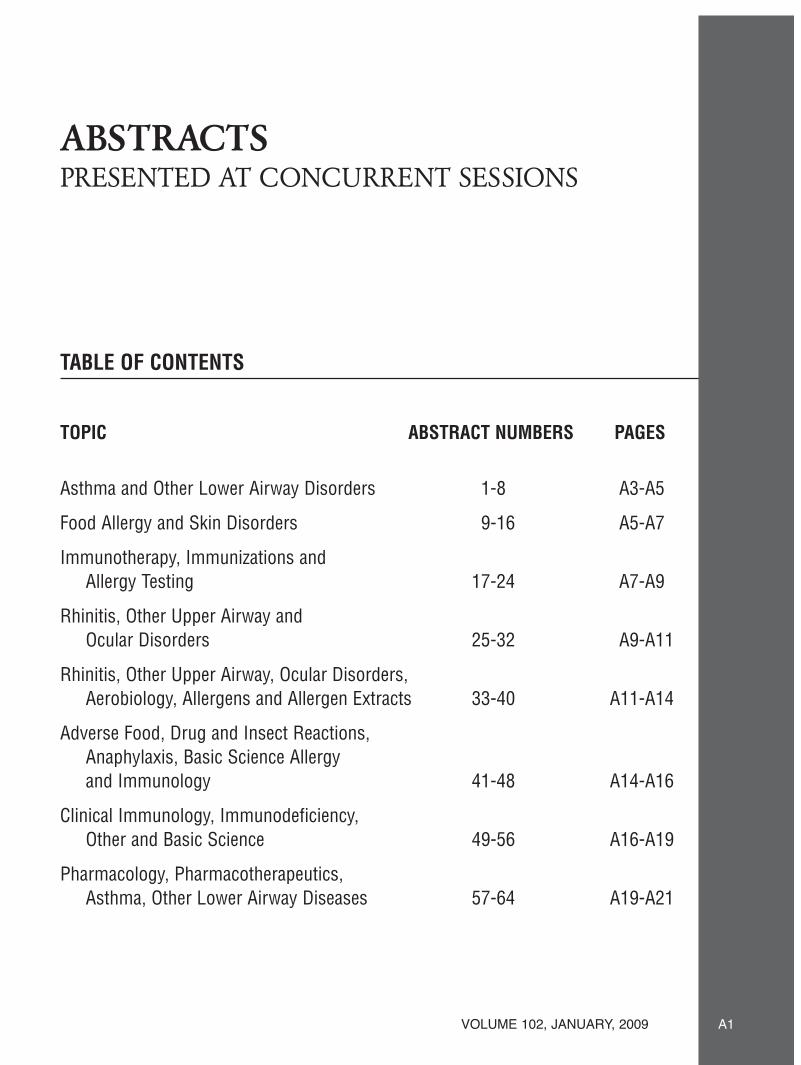
Poorly controlled asthma was defined as maintenance of control at less than50% of follow-up visits. Results : Patients who lived less than 2 miles fromthe nearest freeway (near group) had asthma that was more difficult to con-trol (p=0.02). The patients in this group were more than 3 times as likely tohave poorly controlled asthma (p=0.003) than those who lived farther awayfrom the nearest freeway (far group). Baseline severity also interacted inthe relationship between distance from freeway and asthma control. Patientswith mild asthma who lived close to a freeway (near group) were more thantwice as likely to have asthma that was not well controlled (OR 2.2). Con-clusion: In children with asthma, living near freeways is associated with poorasthma control. Proximity to freeways is more important to long term con-trol in patients with mild baseline asthma than in patients with severe base-line asthma.
J. Blair1, F. Koppenhagen*2, D. Kennedy1, 1.Waterford, Ireland; 2. Miami,FL.
All albuterol HFA MDIs are at risk of clogging, particularly if not used inaccordance with their patient instruction leaflets (PIL). Regular cleaning ofactuators minimizes the risk for clogging. Unfortunately, many patients do notwash their inhalers regularly. This study was done to evaluate the risk for clog-ging if albuterol inhalers are not cleaned through the life of the device. For eachof the three albuterol HFA MDIs, two shots were fired (32 test and 8 controlactuators) every 4 hours over a maximum 36 day period until shot 200 wasreached or until the actuator clogged. Inhalers were determined to be cloggedbased on visual and audible examination of each emitted dose. Once an actu-ator was deemed clogged, the rear of the stem block orifice was examined toestablish the presence or absence of drug deposits. These data were verifiedby multi-stage Cascade Impactor (CI) measurements. Control actuators werewashed every 56 shots and dried in accordance with the product PILs. The rateof clogging for the three albuterol HFAMDIs are presented inTable 1. Proven-til demonstrated the worst risk of clogging compared to either ProAir or Ven-tolin, when the products were not washed.All three products did not clog whenused according to their PILs. Patients need to be advised to wash their albuterolinhalers according to each product’s PIL in order to ensure the product per-forms appropriately.This is especially important for patients prescribed Proven-til HFA MDIs due to its high propensity to clog if not washed regularly.
Comparison of Albuterol HFAMDIs
*The first clogged actuator was observed at shots 133-134
ABSTRACTS: CONCURRENT SESSIONS
A4 ANNALS OF ALLERGY, ASTHMA & IMMUNOLOGY
4STATUS OF ASTHMA CONTROL IN PRIMARY CARE IN THEUS: RESULTS FROM THE ASTHMA CONTROL CHARACTER-ISTICSAND PREVALENCE SURVEY STUDY (ACCESS).R.H. Stanford*, A.W. Gilsenan, W. Lincourt, C. Lankevich, H. Ortega,Research Triangle Park, NC.
Background: The 2007 NHLBI Asthma Guidelines stress the importanceof monitoring asthma control by both physicians and patients. Prevalence ofasthma control in patients being seen for a non-respiratory related reason byprimary care providers (PCP) is currently not known and may be underesti-mated. Objective: To evaluate the level of not well controlled asthma (NWCA)within PCP practices in the US in asthma patients seeking care for non-respi-ratory conditions. Methods: Cross-sectional epidemiological survey adminis-tered to patients with a self-reported diagnosis of asthma. Participants ≥18 yearsof age were recruited from 35 primary care practices geographically distrib-uted across the US. Prior to seeing the PCP, participants completed a brief, self-administered questionnaire that included the Asthma Control Test™ (ACT),questions about demographics, health behaviors (e.g., smoking status), med-ical history, asthma exacerbation history and reason for seeing their PCP. Par-ticipants were enrolled from February 1 to May 2, 2008. NWCA was deter-mined by anACT score of <20 and NWCA prevalence rates were weighted toreflect the US asthma population. Results:A total of 2417 subjects were screenedand 2238 (93%) completed the survey. Of those providing a primary reasonfor visit (n=2,150), 861 (40%) were seen for a respiratory related reason and1289 (60%) for a non-respiratory related reason. The weighted prevalence ofNWCA in the non-respiratory related group was 47.9% (95% CI, 45.7 – 50.1).Among the non-respiratory cohort, NWCA was reported more frequently inAfrican-Americans (AA) than in Caucasians (C) or Hispanics (H), 54.6%,45.63%, 48.3% respectively. In additions, asthma exacerbations (use of oralcorticosteroid, asthma-related emergency department or urgent care or inpa-tient visits) in the previous 12 months were higher in NWCA compared withcontrolled asthma patients (34.2% vs 25%) Conclusion: The prevalence ofNWCA in asthma patients seen in PCP for non-respiratory related reasons isnearly 48% with AA’s having a higher prevalence compared to C’s and H’s. Inaddition, approximately 1 in 4 patients with well controlled asthma experiencedan asthma exacerbation in the prior year. (ADA111118)
5ACORRELATIVE STUDYOFELEVATEDSERUMLEPTINCON-CENTRATIONSANDASTHMASEVERITY INADULTPATIENTS:A POSIBLE LEPTIN RESISTENCE?U.N. García-Ramírez*, C. Velazquez- Avalos, G. Saldoval-Sanchez,J. Miyagui-Namikawa, J. Ramirez-Heredia, N. Segura-Mendez, MexicoCity, Mexico.
INTRODUCTION: Leptin is a hormone protein produced by adipose tis-sue that has two important functions: 1) inhibition of hypothalamic control ofappetite, and; 2) pro-inflammatory activity. Since leptin resistance appears tobe common in the extremely obese, but rarely seen in normal weight subjects,it may play an important role in the pathogenesis obesity-related breathingdisorders and asthma. Epidemiologic data indicate that obesity increases theprevalence and incidence of asthma and reduces asthma control with an increasein disease severity. The aim of the present study was to determine leptin serumconcentrations in subjects with different body mass indices (BMIs) and to cor-relate these with severity of asthma. METHODS: This is a cross-sectional andobservational study, in which serum leptin was measured in subjects who weregrouped according to their BMI and stratified according to levels of diseaseseverity. Statistical analysis of data used the SPSS 15 Anova program (Bon-ferroni) assuming equal variances with a level of significance at a p <0.05RESULTS:A total of 49 subjects (with a ratio of women/men 3:1) were dividedinto 3 groups: Group 1, included 17 asthmatic eutrophic (n = 17) subjects;Group 2 included 15 asthmatic overweight subjects; and Group 3 included 17asthmatic obese subjects. The mean concentrations of leptin were 6.7 ng / dl,9.3 ng / dl and 19.4 ng /dl for Group 1, 2 and 3, respectively, with statisticallysignificant differences between groups 1 and 3, and groups 2 and 3, (p <0.05).The correlation of mean serum concentrations of leptin with disease activityshowed leptin serum values of 8.9 ng /dL, for patients with intermittent asthma,14.5 ng/dl for mild persistent asthma and 18.9 ng/dl in subjects with moderatepersistent asthma, (p <0.05). There were no differences of serum leptin con-centrations between groups when compared by severity. CONCLUSIONS:Although the precise mechanism of action of leptin as a proinflamatory agentand with its relationship with asthma and obesity is unclear, our findings sug-gest a correlation between high serum leptin concentrations in patients with
obesity and increased asthma severity in adults. This may be related to leptinresistance in the obese patients known to have high BMI values, which werehigher in women than in men.
6PREDICTORS FOR EARLY VS LATE HOSPITAL READMIS-SIONSAMONG INNER CITYASTHMATICS.S. Kaipa, A. Das, R. Neugebauer, N. Krishnan,Y.K. Persaud*, Bronx, NY.
Background: Asthma is the most common chronic pediatric illness in theUnited States, affecting approximately 25% of children in an urban population.It is the second most common cause of hospitalization and frequently leads topatients being readmitted a short time after discharge. Objective: In an areawith one of the highest prevalence of asthma nationwide, we attempted to deter-mine predictors of early hospital readmissions. Design/Methods:After receiv-ing IRB approval a chart review was done for asthmatics that were readmittedto our hospital from 9/06 to 3/08. Index admissions were investigated for asthmaseverity, treatment prescribed, and discharge instructions. An early admissionwas one that occurred less than 3 months from an index admission. Statisticalanalyses were performed using SPSS Version 10.1 for Windows. Results: 23of 55 patients (42%) had an early readmission. The age range of the patientswere 2months to 16 years, with the average age of the patients being 59monthsduring their index admission; 50% wereAfricanAmerican and 50% were His-panics. The primary insurance was Medicaid (60%). The majority of earlyadmissions occurred among females (16.7%). A statistically significant pro-portion of children younger than 4 years and those who were born premature(p=.05) had an early readmission(p=.02). Also, patients with allergic rhinitistended to be readmitted earlier. When asthma severity was classified patientstended to have later readmissions (61%) compared to not having asthma sever-ity assessed (41%). We did not see a statistical difference between early/latereadmissions and severity of asthma, previous emergency room vis-its/admissions, and past ICU admissions. Conclusions: Pediatric asthma read-missions can be predicted based on risk factors during the index admissionssuch as prematurity and younger age. Based on this study, hospitalists shouldbe aware of these factors when an asthmatic is admitted.Although the NAEPPrecommends evaluation of day time/nighttime symptoms, we found that themajority(85%) of charts did not report them. Furthermore only a small per-centage of readmissions (15.4%) had a consultation by an allergist and weregiven asthma action plan. We suggest that readmissions can be delayed andpossibly prevented by adherence to National Asthma Guidelines and identify-ing predictors during the index admission.
Rationale: Oxidative stress is heightened in severe asthma and during exac-erbations, which is also associated with steroid resistance. We hypothesizedthat ROS will inhibit GR function in cells. This inhibition could be mediatedthrough mitogen-activated protein kinases, which are known to be activatedby ROS. Methods: Lung fibroblasts were transfected with a GR-Green Fluo-rescent Protein (GFP) construct, and then exposed to a range of concentrationsof H2O2 or superoxide anion (generated by Xanthine/Xanthine Oxidase -X/XO), for 30 min, and 24 hrs. Following ROS exposure, dex (100nM) wasused to induce GR translocation to the nucleus. Cells were fixed, and GR dis-tribution was quantified by the GFP fluorescence signal in nuclear and cyto-plasmic regions using semi-automatedsoftware.A subgroup of cells exposed to H2O2were also pretreated with either1,10-phenanthroline to inhibit production of hydroxyl radicals, phenyl-N-tert-butylnitrone (PBN), an ROS scavenger, or different kinase inhibitors todemonstrate reversibility of any effect seen. The effect of ROS on GR tran-scription was also measured using a luciferase reporter gene assay. Results:Dex producedGR-GFP nuclear translocation in control cells. H2O2 exposure produced sig-nificant reductions in GR translocation in a dose-dependent manner. PBNblocked the inhibiting effects of H2O2 on GR translocation. Phenanthrolinelimited the reduction of translocation seen with H2O2 treatment. X/XO treat-ment produced significant reductions in nuclear translocation of GR at 24hrsonly. The inhibition of GR translocation by ROS was not seen when cells arepretreated with ERK and p38MAPK inhibitors. Western Blot analyses revealthat phospho-ERK and phospho-p38MAPK are both increased at 10 min ofROS exposure, with a subsequent decrease in phosphorylation over time. The
ABSTRACTS: CONCURRENT SESSIONS
VOLUME 102, JANUARY, 2009 A5
transcriptional assay showed that there was no significant impairment in GRtranscriptional activity when cells are treated with H2O2. Conclusion: ROSimpair GR translocation into the nucleus in a dose-dependent fashion. Thisimpairment seems to be mediated by MAPK’s, specifically ERK andp38MAPK. GR transcription is not completely impaired with exposure toH2O2. Oxidative inhibition of GR function may play an important role in thesteroid resistance of asthma exacerbations and the severe asthma phenotype.
8ATOPIC AND CLINICAL CHARACTERISTICS OF CHILDRENWITH FREQUENT MODERATE TO SEVEREVIRAL RESPIRA-TORY ILLNESSESDURINGTHEFIRSTTHREEYEARSOFLIFE.C. Virnig*, T. Pappas, K. Roberg, E. Anderson, D. DaSilva, L. Salazar,C. Tisler, M. Evans, R. Gangnon, J. Gern, R. Lemanske, Madison, WI.
Introduction: The hygiene hypothesis theorizes that increased exposure toinfections early in life confers protection against the development of allergicdiseases.To test this hypothesis, we prospectively analyzed the influence of fre-quent viral respiratory illnesses on various clinical and atopic characteristics.Methods: Patient characteristics were obtained on 277 children enrolled in theCOAST (Childhood Origins of ASThma) study. At years 1, 3 and 6, the pres-ence of eczema and wheezing was assessed, and plasma was obtained for aneosinophil count, total IgE, and allergen-specific IgE. Asthma was diagnosedat 6 years of age. Approval was obtained from the Human Subjects Commit-tee, and written informed consent was obtained from the parents of all subjects.Results: 25 children experienced frequent (≥ 12) moderate to severe illnesses(MSI) in the first 3 years of life while 22 children had no MSIs. Those chil-dren with frequent MSIs were more likely to have attended daycare in the firstyear of life (64% vs. 27%, p = 0.01) and to have been breastfed (52% vs. 18%,p = 0.02) when compared to children with no MSIs. Additionally, the childrenwith frequent infections were more likely to wheeze at 1 and 3 years of age (p< 0.0001 at both time points) and to be diagnosed with asthma at 6 years ofage (59% vs. 9%, p = 0.002). None of the other patient characteristics evalu-ated, which included birth weight, gender, presence of older siblings, exposureto smoke during the first year of life, presence of a cat in the home at birth,presence of a dog in the home at birth, history of maternal asthma, history ofpaternal asthma, presence of atopic dermatitis, total IgE level, allergen-spe-cific IgE to foods and aeroallergens, and blood eosinophil level, were signifi-cantly different between those children with frequent viral respiratory infec-tions in the first 3 years of life and those with no MSIs. Conclusions: In theCOAST birth cohort, children with frequent MSIs during the first 3 years oflife were more likely to have attended daycare and to have been breastfed. Fre-quent illnesses did not protect against the development of atopic diseases astheorized by the hygiene hypotheses, but rather increased the risk of develop-ing wheezing and asthma.
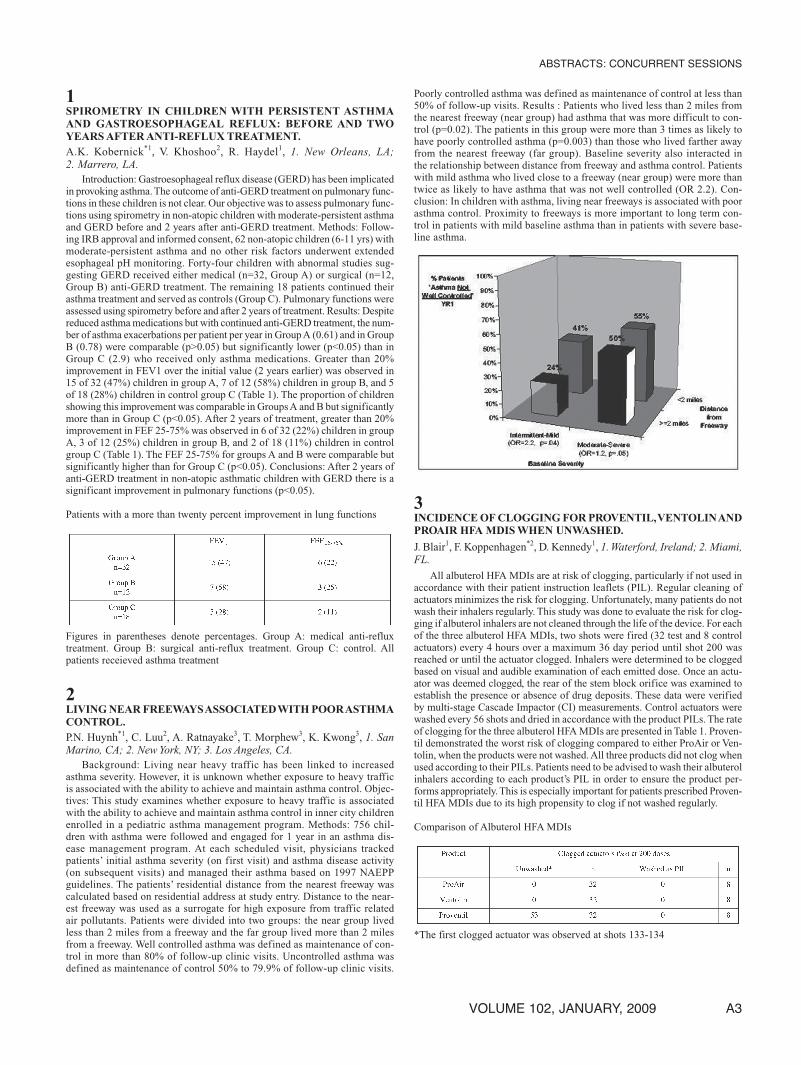
9DIFFERENCES BETWEEN HEAT-TREATED, RAW AND COM-MERCIAL PEANUT EXTRACTS BY SKIN TESTING ANDIMMUNOBLOTTING.U. Kaza*1, A. Casillas2, B. Wilson2, J. Nesbit3, H. Cheng3, S. Maleki3,S. Bahna2, 1. Bloomfield Hills, MI; 2. Shreveport, LA; 3. New Orleans, LA.
Background: Peanut allergenicity has been reported to be influenced byheat treatment, yet the commonly available extracts for skin prick testing (SPT)are derived from raw peanut. Objective: To assess the effect of heat treatmenton the SPT reactivity and serum specific IgE binding to peanut. Methods:Threecommercial extracts and 3 laboratory-prepared extracts, including raw, roastedand boiled peanut, were used for SPT in 22 patients with suspected peanutallergy and in 5 non-allergic subjects. In addition to total IgE, specific IgE bind-ing patterns were assessed by immunoblotting against the same 6 extracts.Results: Twelve of the 22 patients had a positive peanut challenge or a stronghistory of peanut allergy. SPT with the prepared and commercial reagentsshowed that the boiled extract had the highest specificity (67% vs 30 to 50%for the other extracts). All 3 prepared extracts showed the same sensitivity(75%).Three patients with a strong history of anaphylaxis had strong IgE bind-ing to the 3 prepared extracts, yet had variable reactions to one or more of thecommercial extracts. IgE binding to Ara h 2 was found in nearly all patients,regardless of their clinical reactivity. Conclusions: Since none of the individ-ual extracts tested showed high diagnostic reliability, peanut SPT sensitivitycan be enhanced by using a mixture of extracts.
10COMPARISON OF FOOD TEST REACTIVITY IN ADULT ANDPEDIATRIC PATIENTSWITH EOSINOPHILIC ESOPHAGITIS.G. Ghaffari*, T. Craig, S. Chegini, Hershey, PA.
Background: Eosinophilic esophagitis (EE) is considered an allergic phe-nomenon and could be associated with hypersensitivity reactions to foods. Themajority of studies related to EE and food allergy have been performed in pedi-atric age groups.The purpose of this study is to identify the differences betweenreactions to foods in adult and pediatric patients with EE in our patient popu-lation. Methods: We included 24 patients with biopsy proven diagnosis of EEin this study. Skin prick testing (SPT) and/or serum specific IgE for immediatetype hypersensitivity and food patch testing (FPT) for delayed reactions wereperformed in all patients. Fourteen patients were adults (10 males, 4 females),between 21 to 68 years with median age of 29 years. Ten patients were in pedi-atric age group (7 males, 3 females), between 2 and 17 years with median ageof 8 years. Chi Test made comparison of food test reactivity between adult andpediatric patients. Results: Personal as well as family history of atopy, were pres-ent in 18 patients with equal distribution between adults and pediatric patients.Themost common presenting symptoms in adult age groupwere dysphagia andreflux symptoms. In pediatric patients, symptoms suggestive of reflux, vomit-ing and poor weight gain were the most common presenting symptoms. IgEtest was positive in 16 patients (10 adult, 6 pediatric), with average of positiveIgE tests being four. Regarding FPT, 12 patients (4 adults and 8 pediatric) hadpositive tests, with average of positive FPT being 2. IgE test reactivity, were sim-ilar in both age groups, whereas FPT reactivity were more likely in pediatricpatients (P<0.01). Conclusion: In population under study with EE, pediatricpatients weremore likely to have positive FPT compared to adults. IgE test reac-tivity was similar between the two groups. Other triggers for induction ofeosinophilic infiltration in the esophagus, such as aeroallergens, should be con-sidered in patients in whom food tests fail to identify foods
11FOODALLERGYANDECZEMA IN PEDIATRICLIVERTRANS-PLANT PATIENTS.M. Braskett*, R.S. Venick, S.V. McDiarmid, J.H. Vargas, D.G. Farmer,E.R. McCabe, R.W. Busuttil, S.A. McGhee, Los Angeles, CA.
Rationale: Increasing reports suggest that up to 10% of pediatric liver trans-plant (LTx) patients treated with tacrolimus demonstrate hypersensitivity tofoods. In general, adult LTx patients and pediatric recipients of other solid organtransplants treated with tacrolimus do not share this phenotype. Additionally,the clinical observation of eczema in many of these patients is unexpected. Weaim to identify risk factors for the development of food hypersensitivity andeczema in pediatric LTx patients.Methods:This retrospective case control studyincluded 130 pediatric LTx patients who received an initial graft during 1997-2007. Immune suppression was limited to steroids and tacrolimus. Cases wereidentified by physician diagnosed eczema or food hypersensitivity. Primary out-come variables were age at transplant and underlying diagnoses. Secondary out-comes included peak absolute eosinophil count and duration of steroid therapy.P values were calculated using Chi-Square analysis for categorical data and theMann- Whitney test for median data. Results: We identified 30 patients witheczema, 20 with food hypersensitivity and 8 with both conditions. 88 controlslacked these diagnoses.Younger age at transplant was the only variable that dif-fered between cases and controls (median age: cases 11 months, controls 16months, p=0.01). Most of the literature consists of cases of food allergy in bil-iary atresia patients, however, we did not detect an increased prevalence of thisdiagnosis in the case population (p = 0.14). Median values for peak eosinophilcount and duration of steroid therapy did not differ between groups.We did notdetect statistically significant differences in demographic variables. Conclu-sions: Clinically significant food allergy and/or eczema are common findingsin pediatric liver transplant patients treated with tacrolimus. One third of ourstudy populationwas diagnosedwith either condition (42/130, 32%). Our resultssuggest that post-Tx food allergy and eczema are not solely a feature of theunderlying diagnosis. Younger patients appear to be at increased risk. The eti-ology is unknown and likely includes genetic susceptibility and altered barrierfunction and flora. Moreover, as tacrolimus modulates NFAT to decrease IL-2,we speculate that post-Tx food hypersensitivity and eczema may result fromregulatory T cell impairment in the setting of altered antigen exposure.
ABSTRACTS: CONCURRENT SESSIONS
A6 ANNALS OF ALLERGY, ASTHMA & IMMUNOLOGY
12CAN THE OCCURRENCE OF AN ADULT-ONSET RED MEATALLERGY BE EXPLAINED BY IGEANTIBODIESTOA CARBO-HYDRATE?S.P. Commins*, S.M. Satinover, J.M. Roper, T. Platts-Mills, Charlottesville,VA.
Although the occurrence of adult-onset mammalian meat immediate HSRis rare, recent clinical experience suggests that there has been an increase inadult patients who report an allergic reaction 3-6 hrs after eating red meat. Theunusually long delay between eating meat and developing symptoms promptedan investigation of whether an IgE antibody (ab) to the carbohydrate galactose-α-1,3-galactose (α-gal), which is expressed on non-primate mammalian pro-teins, was present in sera from adult patients who develop an allergy to beef,pork or lamb. Method: With IRB approval, detailed histories were taken frompatients presenting with allergy to beef, pork or lamb. Prick tests (SPT), intra-dermal tests (ID), serum IgE ab analysis, & absorption experiments were per-formed. Results: 15 patients with IgE ab toα-gal were identified.These patientsdescribed a similar history of anaphylaxis or urticaria 3-6 hrs after the inges-tion of meat and reported fewer or no episodes when following an avoidancediet. SPT to mammalian meat produced wheals usually <4mm, whereas ID orfresh food SPT provided larger, more consistent wheal responses. In keepingwith the distribution ofα-gal, serum assays for IgE ab to beef, pork, lamb, cow’smilk, cat & dog were positive. Skin testing to chicken, turkey & fish producedno response, and this was supported by the lack of serum IgE ab to these aller-gens.Analysis of serum IgE ab results showed a significant correlation betweenIgE ab to α-gal and IgE anti-beef (r=0.81). Surprisingly, the titers of IgE ab tocat and dog epithelia were closely correlated (r=0.98), however, IgE ab to catwas not explained by sensitivity to Fel d 1 (r=0.35). The results from absorp-tion experiments show that α-gal bound to sepharose beads reduced specificIgE ab binding to α-gal, beef, pork, cat & dog (p<0.01) but did not affect thelevels of IgE ab to chicken, turkey & fish. Taken together, these results indicatethat the pattern of sensitivity was explained by IgE ab binding to α-gal epitopespresent on a wide range of mammalian proteins. Conclusion:We report a novel,severe food allergy related to IgE ab to the carbohydrate moiety, α-gal. Thesepatients report no oral allergy syndrome-type symptoms; experience systemicsymptoms starting 3-6 hrs after eating meat; have a consistent pattern of SPTand ID testing; & have similar serum IgE ab profiles.
13THE CONTRIBUTION OF CHEMICAL AND STRUCTURALALTERATIONSOFARAH3TOTHEALLERGENICPROPERTIES.S. Dyer*1, S. Bahna2, J. Nesbit1, H. Cheng1, B. Wilson2, U. Kaza2,S.J. Maleki1, 1. New Orleans, LA; 2. Shreveport, LA.
Rational: The IgE binding and structural characteristics of Ara h 3 fromraw and roasted peanuts were assessed towards understanding the enhancedskin prick test (SPT) reactivity and IgE binding to roasted peanuts. Methods:Ara h 3, partially denatured with 1 hour of heating at 65°C in the presence ofa reducing agent andAra h 3 purified from raw (R) and light roast (LR) peanutwas subjected to circular dichroism (CD) spectroscopy and IgE binding analy-sis with sera of peanut allergic and non-allergic patients using immunoblotanalysis and compared to SPT for those patients. Results:While the serum IgEof majority of the patients was shown to bind the LRAra h 3 at a much higherlevel than the RAra h3, roasting only slightly altered the secondary structure.CD revealed that R Ara h 3, partially denatured with heat and reducing agent,showed a decreased percentage of alpha helices and a corresponding reductionin IgE binding. Conclusions: Reduction in alpha helices in the Ara h 3 struc-ture caused a significant reduction in the IgE binding by patient sera. On theother hand, roasting caused a significant increase in the IgE binding to Ara h3, while no changes were seen in the structural elements between R Ara h 3and LR Ara h 3. This data indicates that 1) either chemically induced alter-ation of the IgE binding epitopes or oligomeric state are responsible forenhanced IgE binding to LR Ara h 3 and that 2) the alpha-helical structuresare the most important contributors to the recognition of Ara h 3 by the IgE ofpeanut allergic individuals.
14NATURALHISTORYOFCOW’SMILKALLERGY INCHILDRENWITHATOPIC DERMATITIS.H. Lee*, J.H. Kim, K.M. Ahn, S.I. Lee, Seoul, South Korea.
Background: Cow’s milk is one of the most common foods to cause allergyin children with atopic dermatitis (AD). It is well known that most children out-grow their allergy to cow’s milk during the time of early childhood and that therate of tolerance is higher than other food allergies. Objectives: The aim of thisstudy was to describe the natural course of cow’s milk allergy in children withatopic dermatitis over time, and to identify factors predictive of outcome. Andwe tried to determine the cutoff values of cow’s milk specific IgE antibody toserve as predictors of developing tolerance in cow’s milk allergy. Methods: Wereviewedmedical records of 83 childrenwhowere diagnosedwithAD and cow’smilk allergy before 12 months of age to evaluate clinical characteristics andprognostic factors. Results: During follow-up period (4-72 month; mean 32months), Sixty-three (75.9%) children developed tolerance to cow’s milk, andthe median age for tolerance was 48 months. Outgrowing was related to thelogarithm of peak total IgE (P < 0.001), the logarithm of peak cow’s milk spe-cific IgE (P < 0.001) before 12 months of age and severity of AD by SASSADscore (P = 0.033).There was no correlation between tolerance and sex, the onsetage ofAD, duration of breast milk feeding, family history of allergic disorders.The cutoff point for the cow’s milk specific IgE level at initial evaluation foroutgrowing the allergy at 36months of agewas 4.37KUA/L (Sensitivity 62.2%,Specificity 73.9%). Conclusions: Half of the children younger than 12 monthsof age with AD and cow’s milk allergy would develop tolerance at 48 monthsof age. The most important prognostic factor was the peak cow’s milk specificIgE antibody level.
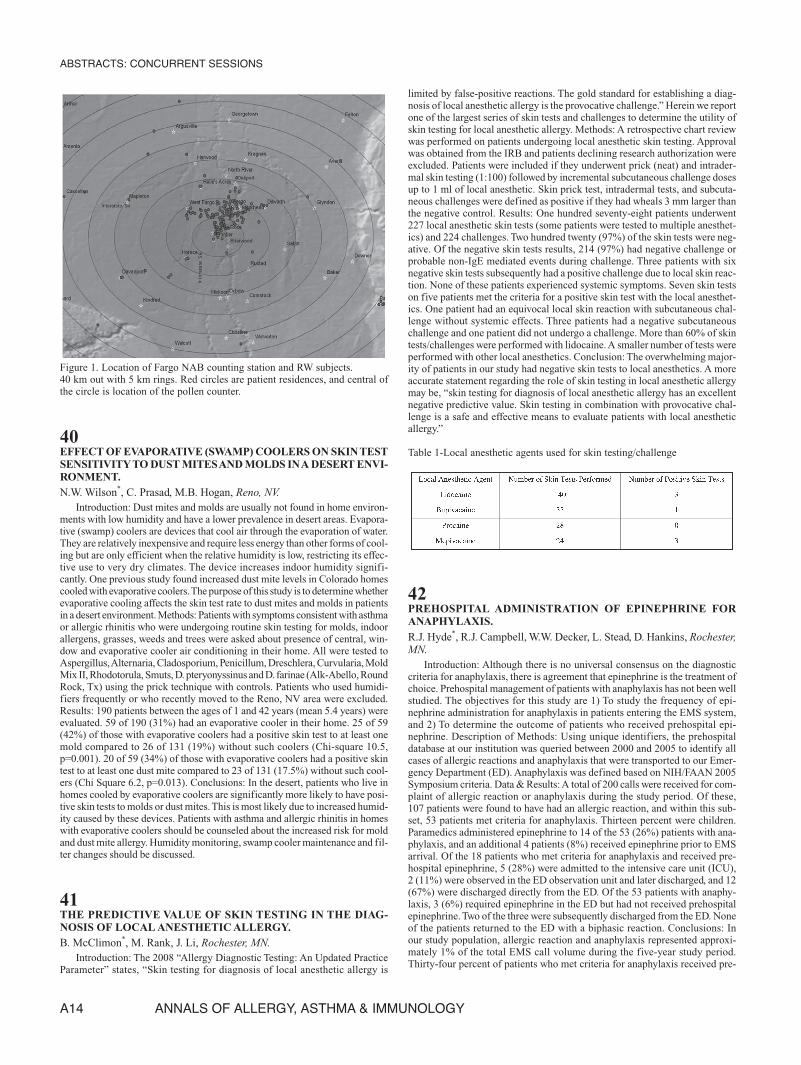
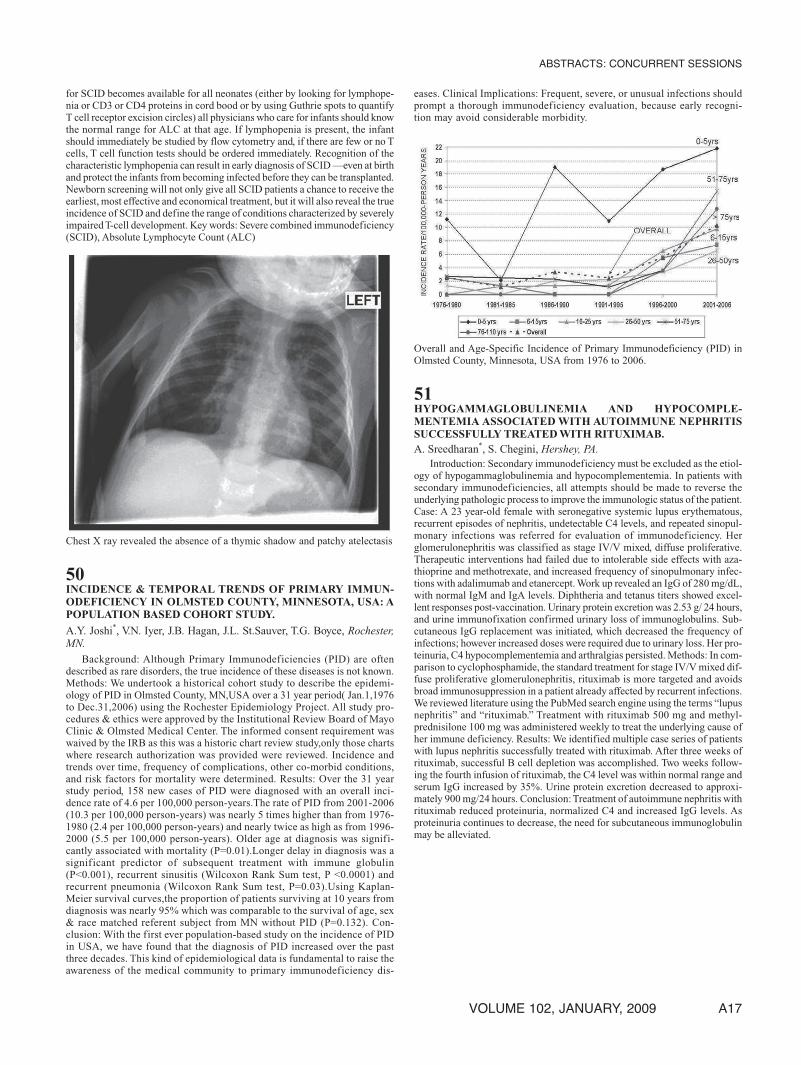
15IDENTIFICATIONOFTCELLEPITOPESFORARAH2ANDARAH 8 INA PEANUTALLERGIC INDIVIDUALWITH HLA CLASSII TETRAMERS.
K.A. Hetherington*, D.M. Robinson, E.A. James, J. DeLong,W.W. Kwok,Seattle, WA.
Introduction: The prevalence of peanut allergy in the US is estimated to be1% and is increasing. Peanut allergic individuals have increased risk of ana-phylaxis and sudden death. Our goal is to identify class II restricted T cell epi-topes for major peanut allergens using novel MHC class II tetramer technol-ogy to develop effective and safe peptide immunotherapy as well as improveddiagnostic tests. We have begun studies to characterize the major T cell epi-topes for the peanut allergens Ara h 2 and Ara h 8 in peanut allergic individu-als. Methods: We used MHC class II tetramers and Tetramer Guided EpitopeMapping (TGEM) to identify the antigenic peptides for the peanut allergen pro-teins Ara h 2 and Ara h 8. PBMCs were obtained from peanut allergic andnon-allergic individuals with written informed consent under an IRB approvedstudy. Peanut allergic individuals were identified by clinical history, skin pricktest, and/or ImmunoCap. In initial studies, T cells were isolated from 1 peanutallergic individual and 1 non-allergic control. TheT cells were stimulated withpools of 15 amino acid peptides representing the entire sequence for eachpurified peanut protein and stained with tetramer reagents after in vitro ampli-fication. Results: In the peanut allergic patient with the DR1501 haplotype, twoDR 1501 restricted antigenic peptides were found for Ara h 2: Arah h 2 (91-106) andAra h 2 (127-141). One additional DR 1501 restricted antigenic pep-tide was found for Ara h 8: Ara h 8 (142-156). Peptide prediction based on thesubject’s HLA type revealed the most likely minimal epitope within Ara h 2(127-141) to be LRNLPQQCG.Theminimal epitope forAra h 2 (91-106) couldnot be determined based on current data. Additionally, the most likely mini-mal epitope forAra h 8 (142-156) is FRAIEGYVL.These responses were absentfor a non-allergic individual with HLA-DRB1*1501. Conclusions: In this casestudy, T cell epitopes for Ara h 2 and Ara h 8 were identified for one peanutallergic individual with HLA-DRB1*1501. These findings suggest that MHCclass II tetramers provide a powerful approach for identification of HLArestricted epitopes in peanut allergic subjects. Funding sources: NIAID con-tract HHSN272200700046C and The Elizabeth Campbell Fund
ABSTRACTS: CONCURRENT SESSIONS
VOLUME 102, JANUARY, 2009 A7
16PREDICTORS OF CLINICIAN-DIAGNOSED ATOPIC DER-MATITIS AT AGES ONE AND TWO: THE CINCINNATI CHILD-HOODALLERGYANDAIR POLLUTION STUDY (CCAAPS).
Introduction:Atopic dermatitis is an early manifestation of allergic disease.The purpose of this study is to identify environmental and host characteristicsas predictors of physician-diagnosed atopic dermatitis in one and two year oldinfants. Methods: A prospective birth cohort of 680 infants born to one atopicparent was identified from birth records. University of Cincinnati IRB approvalwas obtained andwritten informed consent obtained from parents of all researchsubjects. Evaluations at ages one and two years included questionnaires, phys-ical examination, and skin prick testing (SPT) to milk, egg and 15 aeroaller-gens. Clinician-diagnosed atopic dermatitis was defined as having either signsand symptoms “definitive” or “probable” for atopic dermatitis, or the pres-ence of “mild”, “moderate” or “severe” erythema, papulation and infiltration.Multivariate logistic regressions with the outcome of clinician-diagnosed atopicdermatitis were performed. Odds ratios for significant effects from the modelwere estimated. Results: Mean age at time of the annual visits was 13.7 and24.8 months. Clinician-diagnosed atopic dermatitis was present in 14.5% and15.4% at years one and two, respectively. In the multivariate model, clinician-diagnosed atopic dermatitis at age two was associated with a significant tenfold risk if the child had been diagnosed with atopic dermatitis at age one (oddsratio [OR]=10.9; 95% confidence interval [CI]= 5.0-23.4; p<0.0001). Also,positive SPT to any aeroallergen or food at year one (OR= 3.7; 95% CI 1.8-7.8; p=0.003), and positive SPT to mold at year two (OR= 3.6; 95% CI 1.4-9.4; p=0.009), was also associated with atopic dermatitis after adjusting forrace and gender. Conclusions: Infants born to atopic parents who have atopicdermatitis at age one are at high risk at age two. Further early sensitization tonot only foods but also aeroallergens in infancy increases the child’s risk forhaving clinician-diagnosed atopic dermatitis at year two.
17EFFECT OF PRETREATMENTWITH OMALIZUMAB ON THETOLERABILITY OF SPECIFIC IMMUNOTHERAPY INPATIENTSWITHPERSISTENTSYMPTOMATICASTHMA INAD-EQUATELY CONTROLLED WITH INHALED CORTICOS-TEROIDS.M.Massanari1, H. Nelson*2,T. Casale3,W. Busse4, F. Kianifard1, G. Geba5,R. Zeldin1, 1. East Hanover, NJ; 2. Denver, CO; 3. Omaha, NE; 4. Madi-son, WI; 5. Sparta, NJ.
Introduction: Immunotherapy (IT) is a valuable treatment option for patientswith allergic rhinitis and asthma. However, the potential for systemic allergicreactions (SARs) to IT has limited its use, particularly in patients with asthma.Recent data demonstrated pretreatment with omalizumab (OMA) reduced therate of anaphylaxis following ragweed-specific rush IT in patients with aller-gic rhinitis. Here we evaluated OMA’s effect on the tolerability of IT in patientswith persistent, symptomatic asthma inadequately controlled with inhaledcorticosteroids (ICS).Methods:This multi-center, double-blind, parallel-group,26-week study randomized 275 patients, 18-55 years of age, with at least mod-erate persistent symptomatic asthma (FEV1 >75% predicted), total serum IgE>30 and <700 IU/ml, and skin test sensitivity to at least one of three perennialaeroallergens (cat, dog and house dust mite). Patients were randomized to 16weeks of OMA or placebo (PBO). Specific IT to the relevant aeroallergens wasbegun after 12 weeks of OMA/PBO. IT was titrated to a target dose (15ug Feld1/Can f1, 5ug/3.5ug Der f1/p1) using 18 injections at 8 visits over a 4 weekperiod followed by an 8 week period of maintenance therapy. The proportionof patients who experienced a SAR following IT was evaluated using Cochran-Mantel-Haenszel test, adjusting for OMA/PBO dosing regimen (2/4 weeks),perennial allergen sensitivity (single or multiple), and cat sensitivity (yes/no).IRB approval was obtained and all patients provided written informed con-sent. Results: 248 patients (126 OMA, 122 PBO) received at least one IT doseand were included in the efficacy population. Groups had similar baselineIgE, FEV1, ICS dose and allergen sensitivity. A smaller proportion of patientsreceiving OMA experienced SARs during IT (17/126 vs 32/122 PBO; absolutetreatment difference = 0.1274, p = 0.017; 95% CI: 0.0291, 0.2256) and hadfewer respiratory related SARs (7 vs 24, respectively). More OMA patientswere able to reach target maintenance IT dose (87.3% vs 72.1%, respectively,p=0.004). Conclusion: Use of omalizumab in patients with symptomatic asthma
was associated with fewer systemic allergic reactions to specific immunother-apy and enabled more patients to achieve target IT maintenance dose.
18SUBCUTANEOUS IMMUNOTHERAPYREDUCES FUTURE SEN-SITIZATION INALLERGIC CHILDREN UNDER SIXYEARS OFAGE.Z.D. Jacobs*, T.A. DeWees, M.L. Vandewalker, Columbia, MO.
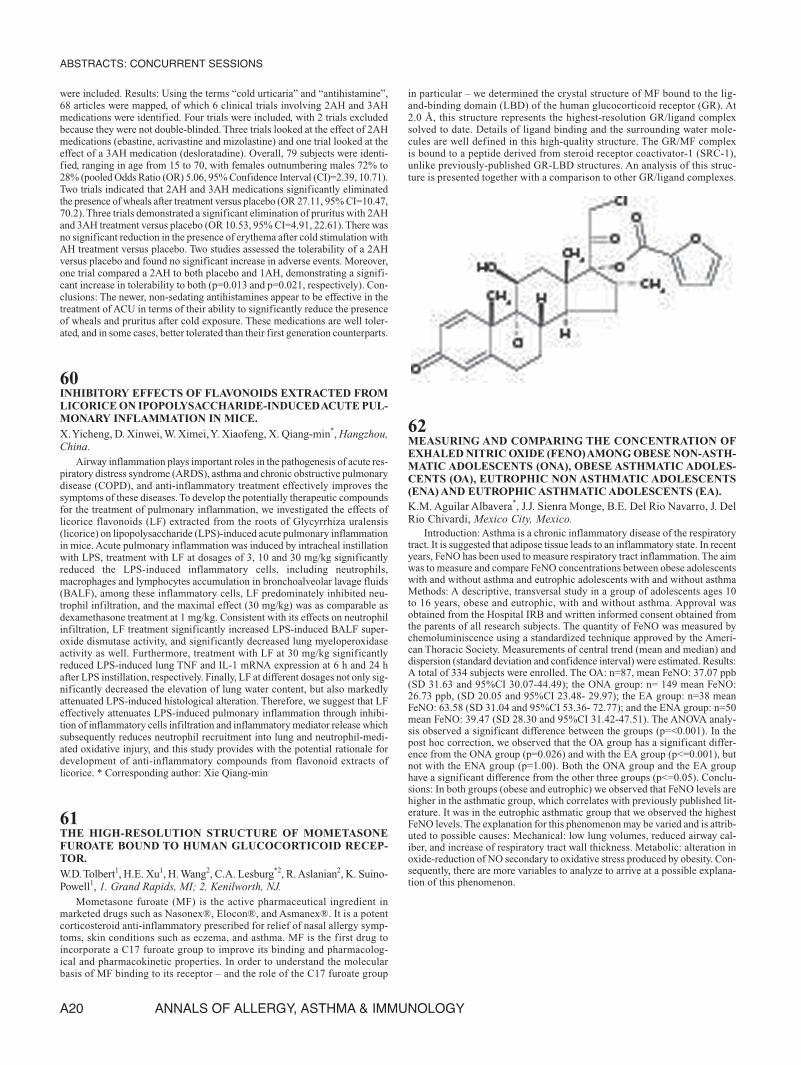
INTRODUCTION: Controversy exists over the use of allergen-specificsubcutaneous immunotherapy (SCIT) among children under six. Studies showSCIT is safe and effective in this age group and may prevent the developmentof asthma in sensitized patients, leading some to recommend usage at earlierages.Thus we investigated the response to SCIT of skin prick test (SPT) changein children under six compared to similar age patients not on IT. METHODS:Patients:A retrospective chart review of oneMidwest allergy clinic from 1992-2007 identified 59 patients on SCIT aged 18 months to 5 years for analysis.All children had clinical presentations consistent with allergic rhinitis (AR),suboptimal benefit from previous therapy, and at least one positive SPT. Sincethere were insufficient age-matched patients not on SCIT in the clinic popu-lation for controls, we used published data from 97 asthmatic children underage 6 not on IT followed with repeat SPT to pollen, dust mite, and animal dan-der to assess their tendency for new sensitization.As a retrospective chart review,our study was exempt from institutional review board approval. Skin testing:SPTs were performed on the forearm or back before and about two years afterinitiation of SCITwith pollen, dust mite, and animal extracts. Positive responsefor analysis was defined as a mean wheal diameter of at least 3 mm > negativecontrol with bifurcated needle or Multitest. Treatment: SCIT was initiated andupdosed with standardized allergen extracts (Greer, ALK-Abello, Hollister-Stier) over 15-20 weeks. Maintenance injections containing major allergen inaccordance with published parameters were given every 2-4 weeks. Statisticalmethods: One-way analyses of variance were done on the SCIT and controlgroups using total positive SPTs at first and repeat testing as the variable.RESULTS: In patients receiving SCIT, the mean number of sensitivities perchild was 2.0 which decreased 10% to 1.8 ( p=0.42). In contrast, the controlgroup had a highly significant increase of 62% (p < 0.0001) in sensitivitiesfrom 1.0 to 1.62. CONCLUSIONS: This retrospective data analysis showsthat allergic preschool children receiving allergen-specific SCIT develop fewernew sensitivities compared to age-matched controls not on IT. SCIT should beconsidered in pediatric patients with AR as young as 18 months to reducefuture sensitization.
ABSTRACTS: CONCURRENT SESSIONS
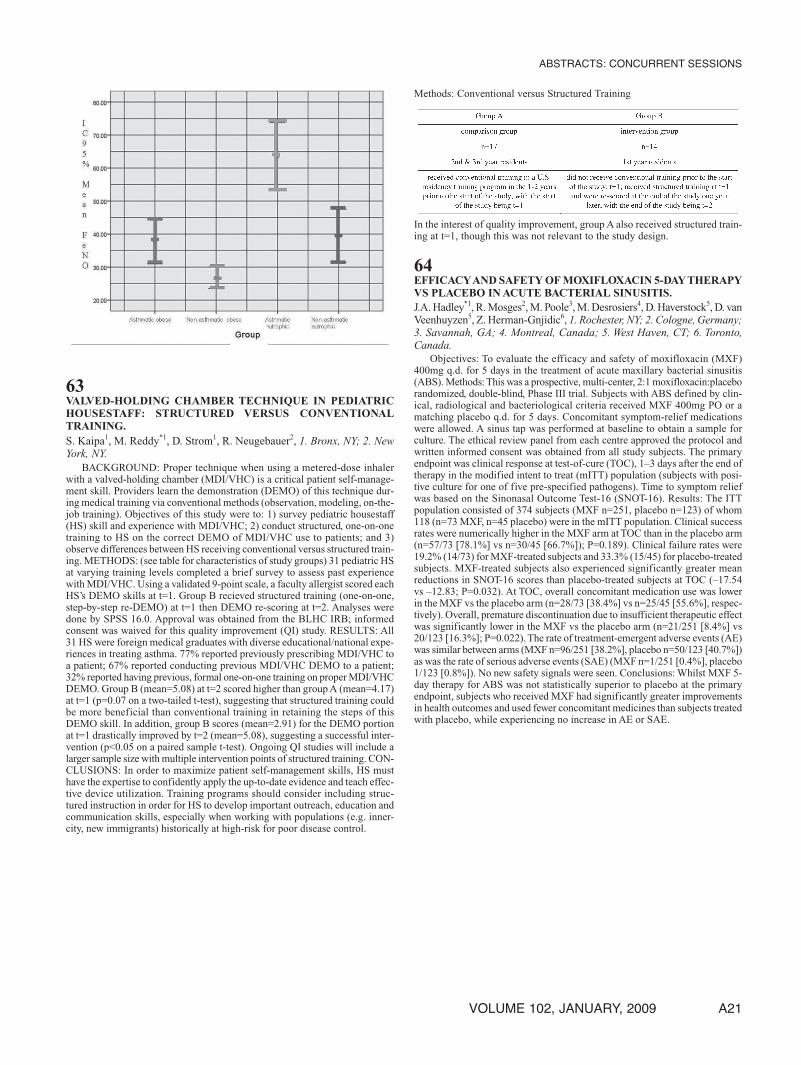
A8 ANNALS OF ALLERGY, ASTHMA & IMMUNOLOGY
19CYT003-QBG10, A NOVEL ALLERGEN-INDEPENDENTIMMUNOTHERAPY, SHOWNTO BE SAFEAND EFFICACIOUSIN PLACEBO-CONTROLLED PHASE II STUDY.A. Blaziene*1, P. Leisyte2, B. Sitkauskiene2, L. Kits3, M. Savisaar3,V. Lozovskis4, M. Bukovskis4, P. Maurer5, J. Willers5, P. Mueller5, 1. Vil-nius, Lithuania; 2. Kaunas, Lithuania; 3. Tartu, Estonia; 4. Riga, Latvia;5. Schlieren, Switzerland.
Introduction: Specific immunotherapy (SIT) is currently the only disease-modifying treatment for allergic rhinoconjunctivitis and allergic asthma. Con-ventional SIT, however, is time-consuming, requires up to 80 allergen injec-tions and exposure to the allergen causes frequent adverse events. Thesedisadvantages have limited the widespread use of SIT and only few allergy suf-ferers make use of this therapy. CYT003-QbG10 is a novel allergen-independentimmunotherapeutic developed for the treatment of a broad range of allergicdiseases. The product candidate consists of a virus-like particle (VLP) loadedwith the immunostimulatory CpG oligonucleotide G10. The immunothera-peutic aims to alter the immunological milieu and allergic effector cell responsesto ameliorate disease symptoms. Methods: CYT003-QbG10 has been testedin a randomized, double-blind, placebo-controlled phase II study that evaluatedthe safety, tolerability and efficacy of the immunotherapeutic. The studyincluded 80 patients suffering from mild-to-moderate perennial allergicrhinoconjunctivitis due to house dust mites and/or cat allergens. All patientsreceived 6 weekly injections of either CYT003-QbG10 (n=40) or placebo(n=40). Efficacy is monitored by assessment of the total rhinoconjunctivitissymptoms in daily life and bymeasurement of the allergen tolerance in the con-junctival provocation test (CPT) before and at different time points after treat-ment. Results: First results obtained 8 weeks after start of treatment demon-strated that treatment with CYT003-QbG10 was safe, well tolerated andefficacious. CYT003-QbG10 achieved a significant reduction of the rhinocon-junctivitis symptoms in daily life compared to placebo (p=0.008). The meantotal rhinoconjunctivitis score had fallen in the CYT003-QbG10 treatmentgroup from 9.3 points pre-treatment to 3.6 points post-treatment (-61%), andin the placebo group from 9.2 points pre-treatment to 6.3 points post-treat-ment (-32%).Also the allergen tolerance as measured in the CPTwas improvedafter CYT003-QbG10 treatment compared to placebo (borderline significant,p=0.06). Conclusions: CYT003-QbG10 was safe, well tolerated and effica-cious. This opens a new avenue for a disease-modifying and allergen-inde-pendent therapy able to address multiple allergies.
20EFFICACYOFSINGLEGRASSALLERGEN IMMUNOTHERAPYIN MULTISENSITIZED PATIENTS.W. Emminger*1, R. Dahl2, J. Maloney3, H. Nolte3, 1. Vienna, Austria; 2.Aarhus, Denmark; 3. Kenilworth, NJ.
Single grass allergen immunotherapy tablet (AIT) treatment can reducesymptoms in patients (pts) with allergic rhinitis. However, the efficacy of AITtherapy in pts with multiple sensitivities compared with monosensitized pts hasnot been systematically investigated.We report an analysis performed to assesswhether pts with multiple sensitivities may benefit from grass AIT treatment.A post-hoc analysis of data from 568 adults who participated in yr 1 of a 3-yrplacebo (PBO)-controlled trial measuring the efficacy of grass AIT treatment(75,000 SQ-T/2,800 BAU, Phleum pratense, ALK-Abelló) was performed.Treatment commenced 16 weeks prior to expected start of the grass pollen sea-son. Differences in symptom severity and rescue medication use by mono-and multisensitized pts were quantified. Comparisons were made of effects ofgrass AIT in pts sensitive to: a) grass only; b) grass + 1 other allergen; and c)grass + ≥2 other allergens. Allergen sensitivity was determined using a skin-prick test (15 allergens). Rhinoconjunctivitis symptoms (runny nose, blockednose, sneezing, itchy nose, gritty feeling/red/itchy eyes and watery eyes) wererated daily on a 0–3 scale (0=no, 1=slight, 2=moderate, 3=severe symptoms).Treatment effects were compared using Daily Symptom Scores (DSS) and DailyMedication Scores (DMS). Results were analyzed based on a 3-way ANOVAmodel, with treatment and sensitization type as the fixed effect, study site asa random effect, and DSS/DMS as the response variable. 161 pts were identi-fied as sensitive to grass only, 170 pts as sensitive to grass + 1 other allergen,and 237 pts as sensitive to grass + ≥2 other allergens. Compared with PBO,treatment with grass AIT was found to reduce DSS by approximately 30%regardless of whether pts were mono-or multisensitized. Average reductionsranged from 25.57% (sensitivity to grass only) to 34.64% (sensitivity to grass+ ≥2 other allergens). Similar findings were observed when medication usewas assessed. GrassAIT reduced DMS by approximately 35% relative to PBO,
with average reduction ranging from 32.43% (sensitivity to grass only) to39.98% (sensitivity to grass+ ≥2 allergens). No significant differences in ther-apeutic effects across pts groups were observed (p<0.0001). There was no dif-ference in the efficacy of the grass allergy immunotherapy tablet in subjectsmonosensitized or multisensitized to inhalant allergens.
21EFFECT OF SINGLEALLERGEN IMMUNOTHERAPYTABLETONTHETIMETO FIRST RHINOCONJUNCTIVITIS SYMPTOMAND TIME TO FIRST USE OF RESCUE MEDICATION INPATIENTSWITHALLERGIC RHINITIS.
W. Emminger*1, R. Dahl2, J. Maloney3, H. Nolte3, 1. Vienna, Austria; 2.Aarhus, Denmark; 3. Kenilworth, NJ.
Allergy immunotherapy tablet (AIT) treatment has been shown to reducesymptoms and the need for rescue medications in patients (pts) with allergicrhinitis.We investigated whether treatment with grassAIT can prolong the timebefore pts experience symptoms. This is a post-hoc analysis of data from 634pts who participated in the 1st year of a 3-year placebo (PBO)-controlled trialexamining the efficacy of grassAIT (75,000 SQ-T/2,800 BAU, Phleum pratense,ALK-Abelló). Treatment commenced 16 weeks prior to the expected start ofthe grass pollen season. Time to 1st-symptom analysis was performed using aKaplan–Meier methodology. Response variables were time to 1st-use of step1–3 rescue medication and time to total symptom score (TSS) calculated fromthe 1st day of the pollen season. Stepwise rescue medication (step 1 [deslo-ratadine]; step 2 [nasal budesonide spray]; step 3 [prednisone]) was intro-duced depending on persistence and severity of symptoms. TSS comprisedsymptoms (runny nose, blocked nose, sneezing, itchy nose, gritty feel-ing/red/itchy eyes and watery eyes) were daily graded 0–3 (0=no, 1=slight,2=moderate, and 3=severe symptoms, respectively). Study protocol and con-sent forms were approved by the institutional review board for each study cen-ter. Time to first use of step 1 medication or TSS ≥4 and time to first use ofstep 2 medication were significantly greater in pts who received grass AIT vsPBO. Pts treated with grass AIT reported a median time to first use of step 1medication or TSS ≥4 of 7 days vs 4 days for PBO (p=0.015). The % pts whorequired step 2 medication was 34.9% and 52.2% in the grass AIT and PBOgroups, respectively (p<0.0001). Time to first use of step 2 medication was 25days in the grass AIT group vs 11 days in the PBO group (25th percentile).Analysis of time to TSS of ≥4 to TSS of ≥8 showed a significantly greatermedian time for grassAIT compared with PBO (p<0.05). Median time to TSSof ≥8 was 22 days in the grass AIT group and 13 days in the PBO group. Thiscorresponds to a median delay of 9 days for pts who received grass AIT vs ptson PBO (p<0.0001). Treatment with a grass allergy immunotherapy tablet sig-nificantly prolonged the time to first rhinoconjunctivitis symptoms and theneed for rescue medication in patients with allergic rhinitis.
22PERSISTENT EFFICACY OF LONG-TERM TREATMENT FORALLERGIC RHINITIS WITH A GRASS ALLERGYIMMUNOTHERAPYTABLET:FINDINGSFROMA3-YEARCLIN-ICALTRIAL.
M. Calderon*1, R. Dahl2, J. Maloney3, S.R. Durham1, 1. London, UnitedKingdom; 2. Aarhus, Denmark; 3. Kenilworth, NJ.
Sublingual allergen immunotherapy improves symptoms and reduces theneed for rescue medication in patients (pts) with allergic rhinitis. However, theefficacy of grass allergy immunotherapy tablets (AIT) following several yearsof use has not been established.We report findings from a 3-year trial designedto investigate the long-term efficacy and safety characteristics of a grass AIT(75,000 SQ-T/2,800 BAU,Phleum pratense,ALK-Abelló). Grass allergic adultpts were enrolled in a multicenter clinical trial and received either grass AITtreatment or placebo (PBO) continually for 3 years (3 grass pollen seasons).Study protocol and informed consent forms were approved by each center’sinstitutional review board. Grass AIT efficacy was measured using dailyrhinoconjunctivitis symptom and medication scores. Health-related quality oflife (HRQoL) was assessed using the Juniper’s Rhinoconjunctivitis Quality ofLife Questionnaire (RQLQ). Compared with PBO (n=127), pts on grass AIT(n=160) demonstrated significant improvements in symptom and medicationscores, which were sustained throughout the 3 grass pollen seasons. Pts on grassAIT experienced statistically significant improvements in median symptomscores that were 37%, 42%, and 37% (p≤0.0001 over 3 years) greater than thoseon PBO during the 1st, 2nd, and 3rd treatment seasons, respectively. Improve-
ABSTRACTS: CONCURRENT SESSIONS
VOLUME 102, JANUARY, 2009 A9
ments in median medication scores relative to PBO in the 1st, 2nd, and 3rd sea-sons were 45%, 74%, and 60% (p≤0.0027 over 3 years) greater in pts on grassAIT. Similarly, differences in total RQLQ scores between PBO and grass AITtreatments in the 1st, 2nd, and 3rd seasons were 7.83 (p<0.0001), 5.72(p<0.0001) and 5.48 (p<0.0001) favoring those on grass AIT. The majority(>80%) of treatment-related adverse events were mild and resolved quickly.No serious treatment-related adverse events were reported. Findings from this3-year clinical trial demonstrate that long-term treatment for allergic rhinitiswith a grass allergy immunotherapy tablet was well tolerated and was associ-ated with a sustained reduction of symptoms and rescue medications use aswell as in improvements in HRQoL.
23TENYEARS OF DOG IMMUNOTHERAPY: PRESCRIBING PAT-TERNSAMONGMILITARYALLERGISTS.
J. Turbyville*, M. Nelson,Washington DC.
Introduction: Studies on the efficacy of dog immunotherapy have shownmixed results, and a recent survey of allergists revealed that most felt that pollenimmunotherapy was more efficacious than animal dander immunotherapy.The2007 immunotherapy practice parameter suggests 15 mcg of the major dogallergen, Can f 1, in maintenance immunotherapy as a probable effective dose.We sought to determine the number of patients who were prescribed dogimmunotherapy and to compare the dose prescribed to the most recent sug-gested dose. Methods: The US Army Centralized Allergen Extract Lab(USACAEL) processes nearly all the allergen immunotherapy prescriptions inthe US military. For the past 10 years, USACAEL has stocked a 1:10 wt/volconventional dog extract (Greer Laboratories, Lenoir, NC) both for diagnostictesting and for immunotherapy prescriptions. Nonstandardized dog extractshave been shown to contain about 5 mcg/mL of the major dog allergen, Can f1.We reviewed the USACAEL database to determine how many patients wereprescribed immunotherapy to dog over the past 10 years, and what dose theywere receiving. Results: From 1997-2007 there were 79,986 immunotherapyprescriptions filled through USACAEL, and 9,115, or 11.4% contained dog.The most common amount of dog stock extract added to make a 10 mL main-tenance vial was 1 mL (57%). Over 95% of prescriptions used between 0.2and 3 mL. In terms of major allergen content, a dose of 1 mL of 1:10 wt/volconventional dog extract equates to 0.25 mcg of major allergen, significantlyless than the probable effective maintenance dose of 15 mcg of Can f 1 perinjection. Conclusions: All prescriptions contained significantly less than therecommended probable effective dose of 15 mcg of Can f 1. To achieve thisdose with conventional dog extract, an unfeasible 3 mL per injection of undi-luted, stock extract would be required.These results reflect prescribing patternsprior to release of the 2007 allergen immunotherapy practice parameter, andmight help explain why dog immunotherapy has been perceived as less effi-cacious than pollen immunotherapy by most allergists.
24CAN F1 PROTEIN MEASUREMENT AND THE CONCEPT OFTHE HYPOALLERGENIC DOG.H.J. Bowbeer, J. St. Clair, E.M. Ron, B.A. Petrak-Ron*, Boulder, CO.
Introduction:All dogs produceCan f1 protein, which is allergenic in humans.Studies analyzing scrapings from dog coats have foundwidely varying amountsof Can f1 protein, and have not yielded evidence suggesting that any particu-lar dog breed is hypoallergenic. Our lab has endeavored to consistently meas-ure Can f1 protein in canine saliva to see if the concentration of Can f1 variesfrom one dog to another. Methods: Saliva samples were obtained in a consis-tent fashion using a salivary stimulant.Can f1 protein concentration was deter-mined using a standard Elisa assay. Results: Forty dogs were studied. Salivawas obtained from all dogs in quantities sufficient for the measurement ofCan f1 concentration. Samples were processed according to a standard proto-col and then compared. The concentration of Can f1 ranged from 0.04 μg/mlto 40.0 μg/ml. Five dogs (12.5%) had a high concentration of protein (>10.0μg/ml); 20 dogs (50%) had a medium concentration (3.0-10.0 μg/ml); 13 dogs(32.5%) had a low concentration (0.20 μg/ml- 3.0 μg/ml); and 2 dogs (5%)had a very low concentration (<0.20 μg). Concentrations varied widely betweendogs of the same breed. Conclusion: The use of a standard Elisa assay in themeasurement ofCan f1 protein in dog saliva represents a promising newmethodby which to study Can f1 production; it further allows us to classify dogs ashigh, medium, low and very low producers of Can f1 protein. Future studieswill further our understanding of humans’ allergic reactions to pets, and willenable us to explore the concept of a hypoallergenic dog.
25CLINICAL STUDIES OF THE COMBINATION OF MON-TELUKASTANDLORATADINE INPATIENTSWITHSEASONALALLERGIC RHINITIS.S. Lu*1,M.P.Malice2, K. Newcomb1,T.F. Reiss1, 1. Rahway, NJ; 2.Antares,Belgium.
Introduction: Montelukast (10 mg) monotherapy has been reported toimprove nasal congestion, eye symptoms, and rhinoconjunctivitis quality of lifein patients with seasonal allergic rhinitis (SAR). Monotherapy with the anti-histamine loratadine improved rhinitis endpoints.Two studies are described thatevaluated montelukast and loratadine as monotherapy and in combination fortreatment of daytime nasal and eye symptoms, nighttime symptoms, andrhinoconjunctivitis quality of life in patients with SAR. Methods: Patients (N= 632 in Study 1 & 530 in Study 2) ≥15 years of age with ≥2 years of docu-mented clinical history of SAR (both studies) and ≥1 year of documented his-tory of asthma (Study 2) were randomly allocated to treatments for 2 weeks:(Studies 1 & 2) placebo, montelukast 10 mg + loratadine 10 mg, montelukast10mg, or loratadine 10mg once daily at bedtime, or (Study 1 only) beclometha-sone nasal inhaler 50 μg/actuation, 2 sprays in each nostril in the morning andat bedtime. The primary endpoint in both studies was the average of daytimenasal and nighttime symptoms scores. The protocol was approved by the insti-tutional review boards of all participating centers, and all patients providedwrit-ten informed consent. Results: In Study 1, montelukast + loratadine signifi-cantly improved the primary endpoint compared with placebo (p≤0.050).Improvementwith nasal beclomethasonewas significantly better thanwithmon-telukast + loratadine for most endpoints (p≤0.050). The primary endpoint wasnot significantly improvedwithmontelukast + loratadine comparedwith lorata-dine alone but was significantly better compared with montelukast. In Study 2,montelukast + loratadine demonstrated borderline significant improvement overloratadine for the primary endpoint (p=0.072). The difference between mon-telukast + loratadine and montelukast (p=0.545) or placebo (p=0.152) was notsignificant for the primary endpoint. In both studies, all active treatments werewell tolerated, with safety and tolerability profiles similar to that of placebo.Conclusion: In this study, efficacy of montelukast + loratadine was similar toloratadine and comparable or superior tomontelukast alone formost symptomsof SAR. Nasal beclomethasone had a significantly greater effect than mon-telukast + loratadine on most daily symptoms of SAR.
26REGIONAL PREVALENCE OF ALLERGIC RHINITIS SYMP-TOMS: FINDINGS FROM THE PEDIATRIC ALLERGIES INAMERICA SURVEY.M.S. Blaiss*1, M.J. Derebery2, E.O. Meltzer3, R.M. Naclerio4,M. Wingertzahn5, 1. Memphis, TN; 2. Los Angeles, CO; 3. San Diego,CA; 4. Chicago, IL; 5. Florham Park, NJ.
Introduction: Allergic rhinitis (AR) is a common chronic condition associ-ated with a range of bothersome symptoms. Regional differences in AR preva-lence and frequency of 12 common symptoms in US children were examined.Methods: Data were obtained from Pediatric Allergies in America, a nationaltelephone survey of the parents of 500 children (aged 4-17 years) with cur-rently diagnosed nasal allergies among 35,757 US households. Allergic Rhini-tis prevalence was based on all households surveyed. Parents of children diag-nosed with AR were asked which of 12 common AR symptoms their childrenexperienced every day in their worst month in the past year. Regional data wereobtained based on area codes dialed, with regions defined according to USCensus data criteria (Northeast, Midwest, South, and West). Results: Nation-ally, the prevalence of children withARwas 13% (Northeast, 12%; South, 16%;Midwest 12%;West, 11%). Data on symptoms by region were collected for 500parents of children with AR. In the overall sample, parents reported sneezing(mean, 25%; range, 20%-28%), nasal congestion (mean, 25%; range, 20%-29%),and rhinorrhea (mean, 18%; range, 16%-22%) as being the most frequentlyoccurring AR symptoms in their children (multiple answers permitted). Inter-estingly, the occurrence of ocular symptoms associated with AR such as red,itching, and watering eyes – collectively called allergic rhinoconjunctivitis –appeared to be more common among children withAR in the Northeast than inother regions. Children in theMidwest reported experiencing headache and facialpain nearly twice as often as children in other regions. Conclusions: Findingsfrom the PediatricAllergies inAmerica survey suggest that there may be impor-tant differences in symptomology for children with AR depending on the USregion in which they live. Possible contributing factors include exposure to dif-ferent allergens common to different geographic regions and pollution in areaswith higher population density. Data from the PediatricAllergies inAmerica sur-
ABSTRACTS: CONCURRENT SESSIONS
A10 ANNALS OF ALLERGY, ASTHMA & IMMUNOLOGY
vey suggest that further study into the effect of treatment on the symptomsmost common to a particular geographic region may improve the quality ofcare for these children.
Pediatric Allergic Rhinitis Symptoms Reported Every Day by US CensusRegion
Respondents reported for worst month for allergy symptoms in the past year.
27ALLERGIC RHINITIS AND COMMON SECONDARY SYMP-TOMS: FINDINGS FROM THE PEDIATRIC ALLERGIES INAMERICA SURVEY.R.M. Naclerio*1, M.J. Derebery2, E.O. Meltzer3, M.S. Blaiss4,M. Wingertzahn5, 1. Chicago, IL; 2. Los Angeles, CA; 3. San Diego, CA;4. Memphis, TN; 5. Florham Park, NJ.
Introduction:Allergic rhinitis (AR) is a common chronicmalady that impairsthe quality of life of children in the United States. In addition to nasal conges-tion, one of the primary symptoms associatedwithAR, common secondary asso-ciated symptoms of AR include facial pain/pressure, ear pain/pressure, sinusproblems, and headache. Methods: The prevalence of facial pain/pressure, earpain/pressure, sinus problems, headache, and potentially related surgery in chil-dren treated for AR was obtained in Pediatric Allergies in America, a 2007national survey of the parents of 500 children with currently diagnosed nasalallergies and 504 children without nasal allergies (aged 4 to 17 years) among35,757US households. Results:The occurrence of facial pain/pressure (29% vs3%), ear pain/pressure (24% vs 5%), and headaches (55% vs 18%) was morefrequent in children with AR compared with those without AR, respectively.These figures represent nearly a 10-fold increase in facial pain/pressure, anapproximately 5-fold increase in ear pain/pressure, and an approximately 3fold increase in headaches in children with diagnosedAR compared with chil-dren without AR. Parents report that sinus problems (43% vs 4%) also occurmore frequently in children diagnosed with AR compared with children with-out AR, a 10-fold increase. More than half of parents and older children (aged10 to 17 years) reported facial pain/pressure (53% vs 54%), ear pain/pressure(56% vs 44%), and headache (59% vs 63%) as being at least moderately both-ersome, respectively. Fourteen percent of children with AR have had tympa-nostomy tubes placed in their ears compared with 9% of children without aller-gies. Additionally, 18% of children with AR have had tonsillectomy and/oradenoidectomy compared with 11% of children without allergies. These find-ings demonstrate a nearly 2-fold increased incidence of surgery in patients withAR. Conclusions: Findings from the PediatricAllergies inAmerica survey sug-gest that childrenwith symptomaticARmay be at increased risk for facial symp-toms, sinus problems, headache, and possibly ear and upper-airway infectionsrequiring surgery than children without AR. Further study of the effect of ARtreatment on these conditions in children may be warranted.
28ARE MIGRAINE HEADACHES MORE FREQUENTLY ASSOCI-ATEDWITH SPECIFIC CHRONIC RHINITIS SUBTYPES?J.A. Bernstein*, D. Brandt, F. Taylor, J. Ellison, B. Gebbhardt, V. Martin,Cincinnati, OH.
Rationale: Headaches are a common occurrence in patients with allergicrhinitis (AR). Previously, an irritant index scale (IIS) was developed to helpclassify patients with different chronic rhinitis (CR) subtypes and headaches.We found that physician diagnoses of CR subtypes based on current consen-sus definitions differed in 23.6% (103/436) of patients when the IIS was usedas a classification criteria. Objective: To determine the prevalence of migraineand/or tension-type headaches in CR subtypes and the frequency and/or dis-ability of headache in these populations. Methods: Consecutive patients pre-senting to a large allergy practice between ages 17-65 years were enrolled.Patients were excluded if they were specifically referred to determine if aller-gies were causing their headaches All patients underwent a verbal structureddiagnostic interview for headache by a research coordinator blinded to the physi-cian’s CR subtype diagnosis in addition to completing the IIS, MIDAS, HIT-6,PHQ-9, GAD-7 and Berlin Sleep Apnea questionnaires. Subsequently, chartreviews were performed to identify the physician’s diagnosis and results ofallergy skin prick or Immunocap testing. Patient diagnoses were re-classifiedusing the ISS questionnaire results. Statistical analysis was performed usingthe Fishers exact test, Kruskal-Wallis test and Dunn’s Multiple ComparisonTest. Results: 436 patients with CR subtype diagnoses were enrolled; 66%werefemale. CR diagnoses using the IIS with a cut-off of ≥ 24 revealed 226/436(52%) were allergic rhinitis (AR), 115/436 (26%) non-AR (NAR) and 95/436(22%) mixed rhinitis (MR); 90% of all subjects were Caucasian, 6% AfricanAmerican, 2%Asian and 2%Hispanic. Tension type headaches were more fre-quent in AR vs. MR and NAR patients (p<.05) whereas migraine headacheswere more frequent in MR and NAR patients (p<.05). Interestingly, the fre-quency and disability of all headaches were greater in theMR subtype (p<.05).Conclusions: The diagnosis of migraine headache was significantly higher inCR patients with a NAR component. The increased frequency and disability ofheadaches inMR subjects suggests that an important interaction between aller-gic and non-allergic triggers exists in the development of migraine and/or ten-sion type headaches that requires further investigation.
29PREVALENCE OF CONDITIONS ASSOCIATEDWITH ALLER-GIC RHINITIS IN CHILDRENANDADULTS.E.O. Meltzer*1, M.S. Blaiss2, M.J. Derebery3, R.M. Naclerio4,M.Wingertzahn5, 1. San Diego, CA; 2. Memphis, TN; 3. LosAngeles, CA;4. Chicago, IL; 5. Florham Park, NJ.
Introduction: Allergic rhinitis (AR), asthma, and sinusitis are commonchronic conditions that adversely affect quality of life and performance in USchildren and adults. The prevalence of sinus problems, asthma, and other asso-ciated conditions was compared in children and adults with AR. Methods: Theprevalence of conditions associated with AR in children was drawn from Pedi-atric Allergies in America, a national telephone survey of parents of 500 chil-dren withAR (between 4 and 17 years old) obtained from surveying 35,757 UShouseholds. In adults (aged ≥18 years), prevalence was obtained fromAllergiesinAmerica, a national survey of 2,500 adults (31,470 US households) withAR.Results: When children and adults with AR were asked which conditions theyexperienced in the week before the surveys, sinus problems (43% vs 50%),cold/flu symptoms (20% vs 18%), earaches (10% vs 16%), andmigraines (10%vs 15%)were reported, respectively. In addition, asthma diagnoses (39%vs 32%)and asthma symptoms in the past 12 months (28% vs 21%) were common inboth children and adults, respectively. Headaches also occurred frequently; bothchildren (55%) and adults (65%) with AR reported having headaches at least afew days per month during their worst month for allergy symptoms in the pastyear. Moreover, children with AR have a 10-fold increased incidence of sinusproblems and a 3- to 4-fold increased incidence of asthma compared with chil-drenwithoutAR. In addition, heartburn or gastroesophageal reflux disease, skinrashes, and fever occurred in ≥5% of children with AR in the week precedingthe survey (a >3-fold increase over children without AR). Conclusions: TheAllergies inAmerica surveys show that sinus problems, asthma, and other con-ditions are relatively common in both pediatric and adult patients withAR. Thereporting between the 2 groups was similar with respect to concomitant condi-tions.Approximately two thirds experienced headaches, nearly half experiencedsinus problems, and more than one third had a diagnosis of asthma. Further-more, children with AR had substantially more reported sinus problems andasthma comparedwith childrenwithoutAR.These findings suggest that the link
ABSTRACTS: CONCURRENT SESSIONS
VOLUME 102, JANUARY, 2009 A11
between AR and sinus problems, asthma, and other associated conditions war-rants further examination and that an expanded understanding ofAR treatmenteffect on these comorbidities is needed.
30FLUTICASONE FUROATE NASAL SPRAY PROVIDES BETTERRELIEF FROM THE NIGHTTIME SYMPTOMS OF SEASONALALLERGIC RHINITIS (SAR) THAN ORAL FEXOFENADINE.N.J.Amar*1, H.B. Kaiser2,M.L.Vandewalker3,W.T.Toler4, B.A. Prillaman4,E.E. Philpot4, 1. Waco, TX; 2. Minneapolis, MN; 3. Columbia, MO; 4.Research Triangle Park, NC.
INTRODUCTION: Nighttime nasal symptoms often impact the sleep ofseasonal allergy sufferers. Two treatments for SAR, fluticasone furoate nasalspray (FFNS) 110mcg, an enhanced-affinity intranasal corticosteroid, and oralfexofenadine (FEX) 180mg, a non-sedating antihistamine, were compared usinga validated nighttime symptom questionnaire (Nighttime Symptoms Score,NSS), nasal patency as measured by peak nasal inspiratory flow (PNIF), andsubject-rated nasal and ocular symptoms. METHODS: Study centers obtainedIRB/Ethics Committee approval and written informed consent from all sub-jects. 680 subjects with ragweed allergy were randomized to receive FFNS110mcg (N=224), fexofenadine 180mg (N=227), or placebo (N=229) oncedaily for two weeks in this double-blind, double-dummy, multi-center study(FFU109047). The primary endpoint was the mean change from baseline(MCFB) over the treatment period in the NSS which assesses difficulty goingto sleep and nighttime awakenings, both due to nasal symptoms, and morningcongestion on awakening. Supportive secondary endpoints included MCFB inPNIF (L/min), 12-hour nighttime reflective total nasal (congestion, itching,sneezing, and rhinorrhea) and ocular (watering/tearing, itching/burning, red-ness) symptom scores, and morning instantaneous nasal and ocular symptomscores. RESULTS:A significant difference was seen between FFNS and FEX(-0.9, p<0.001) in theMCFB of the NSS.Morning PNIF increased significantlyin the FFNS group compared with those receiving FEX (10.6, p<0.001). Sig-nificant differences were also seen between FFNS and FEX in the 12-hournighttime reflective (-1.3, p<0.001) and instantaneous (-1.5, p<0.001) totalnasal scores, as well as the 12-hour nighttime reflective (-0.6, p=0.002) andinstantaneous (-0.6, p=0.002) total ocular symptom scores. Differences in theseendpoints between FFNS and placebo were significant (p<0.034) but no sig-nificant differences were seen between FEX and placebo (p�0.176). CON-CLUSIONS: Compared with FEX and placebo, FFNS significantly improvedthe nighttime nasal symptoms of seasonal allergy sufferers as determined bythe NSS, with a corresponding increase in morning PNIF. FFNS also showedstatistically significant improvement over both FEX and placebo with respectto all subject-rated nasal and ocular symptom assessments.
31PHARMACOKINETICS,PHARMACODYNAMICS, SAFETY,ANDTOLERABILITY OF CICLESONIDE HYDROFLUOROALKANENASALAEROSOL.P.H. Ratner*1, R. Nave2, M.Wingertzahn3, 1. SanAntonio,TX; 2. Konstanz,Germany; 3. Florham Park, NJ.
Introduction: Aqueous corticosteroid nasal sprays are effective for thetreatment of allergic rhinitis; however, aerosol-based nasal formulations maybe preferred by some patients. This dose ranging study evaluated the phar-macokinetics, pharmacodynamics, safety, and tolerability of a hydrofluo-roalkane (HFA) nasal aerosol formulation of ciclesonide in adult patients withperennial allergic rhinitis (PAR) and healthy volunteers without PAR. Meth-ods: Adult patients with a ≥ 2-year history of PAR (n = 18) and healthy vol-unteers (n = 18) were randomized in a double-blind, placebo-controlled, 3-period crossover manner to 300 μg or 150 μg ciclesonide HFA nasal aerosolor placebo once daily (1 spray/nostril) for 2 weeks (each period), with a 2-week washout between each treatment period. The concentration of desisobu-tyryl-ciclesonide (des-CIC), the pharmacologically active metabolite ofciclesonide (measured by LC-MS/MS with a lower limit of quantification of10 pg/mL), was evaluated by maximum serum concentration (Cmax) and areaunder the serum concentration time curve (AUC). Serum cortisol (AUC0-24h) was also evaluated. The safety and tolerability of ciclesonide was eval-uated by monitoring adverse events. Approval was obtained from Coast IRB(Lake Forest, California); all study participants provided written informedconsent. Results: Levels of des-CIC were detectable in most participants for12 hours postadministration and were similar on days 1 and 14 in both healthy
volunteers and patients with PAR. Mean Cmax for des-CIC on day 14 was36 pg/mL and 26 pg/mL for the ciclesonide 300-μg and 150-μg doses, respec-tively. Mean AUC0,last was 213 pg*h/mL and 112 pg*h/mL for ciclesonide300 μg and 150 μg, respectively. Twenty-four-hour mean serum cortisol AUCwas similar for ciclesonide 300 μg (178 μg*h/dL), ciclesonide 150 μg (169μg*h/dL), and placebo (174 μg*h/dL). Incidence of adverse events was lowand similar for all groups. Conclusions: Systemic exposure of des-CIC waslow and similar in both healthy volunteers and patients with PAR, with noevidence of accumulation over the 14-day treatment period in either dosegroup. Ciclesonide HFA is well tolerated and does not appear to have a sig-nificant effect on HPA-axis function as serum cortisol levels after ciclesonidetreatment were comparable to placebo.
Introduction:Atrophic rhinosinusitis is a clinical syndrome associated withprogressive loss of normal ciliated nasal epithelium, resulting in intractable nasalsymptoms. Diagnostic criteria are currently not available for multicenter trialsto be performed for this condition.We sought to determine if commonly observedclinical features would be adequate for use as diagnostic criteria for atrophicrhinosinusitis. These include greater than six months of nasal obstruction, epis-taxis, anosmia, nasal purulence, nasal crusting, coexistent inflammatory respi-ratory disease (i.e. sarcoidosis orWegener’s granulomatosis), or a history of twoor more sinus surgeries. Methods: We identified 22 patients in our universityclinic for whom there was a consensus on the diagnosis of atrophic rhinosinusitisamong a team of faculty allergist-immunologists and otolaryngologists.We per-formed retrospective chart reviews and compared these patients to 22 randomlyselected patients with chronic rhinosinusitis. Results: Over 80 percent of studypatients had a history of two or more sinus surgeries, chronic nasal obstruction,and nasal purulence. More than half of the study group had nasal crusting.Chronic nasal obstruction did not discriminate among the two populations as itwas present in 77% of the control group (P≥0.7). Less than half of the controlpopulation reported any of the other six proposed criteria for diagnosis of atrophicrhinosinusitis.When chronic rhinitis was present, there was a 25 fold increasedprevalence of atrophic rhinosinusitis (95% confidence interval [CI], 2.9-221.7)with nasal purulence; a 12 fold increased prevalence (95% CI, 1.3-106.8) withepistaxis; and a 15 fold increased prevalence (95% CI, 3.5-66.7) with two ormore sinus surgeries as compared to the control group. Sensitivity and speci-ficity analysis demonstrated that two ormore of the six criteria resulted in a 0.95sensitivity and 0.77 specificity for the diagnosis. Conclusion: Six of the sevenproposed diagnostic criteria for atrophic rhinosinusitis distinguish these patientsfrom chronic rhinosinusitis when present for greater than six months.
Proposed Diagnostic Criteria for Atrophic Rhinosinusitus
33SLEEP-DISORDEREDBREATHINGANDSTRUCTURALALTER-ATIONSOFNOSEANDNASOPHARYNX INANOBESEADOLES-CENTS GROUPWITHASTHMAAND RHINITIS VERSUS CON-TROLS.R. Lara*, B.E. Del Rio, C. De la Torre,Mexico City, Mexico.
Introduction:Asthma and obesity are important health public problems.Theaim of this study is to determine the prevalence of sleep-disordered breathing(SDB) and structural alterations of nose and nasopharynx in an obese adoles-cents group with asthma and rhinitis and compare with controls groups. Meth-ods: Approval was obtained from the Hospital IRB and written informed con-sent was obtained from all the parents of the research subjects.We studied a totalgroup of 89 patients with ages between 11 to 16 years; 40 obese adolescents,43% (n=17) suffer intermittent asthma and intermittentmild rhinitis, 57% (n=23)non asthmatic obese adolescents, and 25 normal weight asthmatic with rhinitisadolescents. We included a control group of 25 healthy adolescents. All ado-lescents underwent a set of physical examinations, nocturnal polysomnographyand nasal endoscopy. Diagnostic criteria for SDB: Apnea/hypopnea index
ABSTRACTS: CONCURRENT SESSIONS
A12 ANNALS OF ALLERGY, ASTHMA & IMMUNOLOGY
(AHI)≥1 was used as diagnostic criteria for SleepApnea/Hypopnea Syndrome(SAHS). Septum deviation (if it obstructed the nostril or was connected withturbinate), turbinate hypertrophy(increase in the volume ≥50%), adenoids hyper-trophy(adenoids/coan index ≥50%). Results: We classified the prevalence ofSDB by groups: In the first group we had obese adolescents with asthma andrhinitis with the following results: 70.6% had SAHS. In the second group ofobese non asthmatic adolescent 73.9% had SAHS.The group of normal weightasthmatic adolescent had 52% of SAHS. Finally the group of healthy adoles-cents had 12.5% of SAHS with significant statistic difference compared withthe others groups. p<.05. We found the higher frequency of septum deviationin the group of obese adolescent with 56%, compared with the healthy adoles-cents group with the 16% (p<.05). In relation to turbinate hypertrophy bothgroup of obese adolescent and the group of normal weight asthmatic with rhini-tis had a frequency near to 70% compared with only 20% in the healthy ado-lescents group (p<.05) Conclusions: Obese and asthmatic adolescents havemorerisk of SDB compared to healthy adolescents. It was found that the frequency,either in SDB and structural alterations of nose in the studied population wasabove of the range reported in literature, which suggest that these pathologiesare underdiagnosed in the pediatric population.
34DOESALLERGY IMMUNOTHERAPY CONFERHEALTHCARECOSTBENEFITS FORCHILDRENWITHALLERGICRHINITIS?A LARGE-SCALE, RETROSPECTIVE, CLAIMS-BASED STUDY.C. Hankin*1, L. Cox2, D. Lang3, G. Gross4, 1. Moss Beach, CA; 2. FortLauderdale, FL; 3. Cleveland, OH; 4. Dallas, TX.
Background: Although the disease modifying effects of allergyimmunotherapy (IT) on childhood allergic rhinitis (AR) are well documented,potential cost benefits remain largely unknown. Methods: We examined 9-year (1997-2006), retrospective, Florida Medicaid paid claims to identify newlyAR-diagnosed children (<18 years) who received IT and had 18 months of fol-low-up data (IT Group). These were matched, over the same period, to newlyAR-diagnosed children who received no IT (No-IT Group) by age atAR diag-nosis, presence of asthma, atopic dermatitis, and conjunctivitis, sex, and race.Wilcoxon signed-rank tests were performed to compare median resource use.Cost data were log-transformed to correct for skewness; paired t-tests wereperformed to examine statistical significance of transformed costs. Results:Among 3,240,046 Medicaid-enrolled children over 9 years, 196,687 (6%)received an AR diagnosis. Of these, 3,931 (2%) initiated IT following theirAR diagnosis. A subset (N=2,288) had 18 months of follow-up data; this ITGroup was matched to No-IT controls (N=71,790). The mean number of ITadministrations over the 18-month follow-up was 23 (SD 19 administrations,median 18, minimum 2, and maximum 122). The average cost per IT admin-istration was $44.00 (SD $35.30). Mean 18-month IT cost was $944 (SD$1,006). During the 18-month follow-up, the IT Group had significantly fewermedian number of inpatient stays (1.0 vs 1.4, p=0.02) and outpatient visitsexclusive of IT (14.0 vs 28.6, p<0.0001) than the No-IT Group; there were no
significant differences in median number of outpatient visits inclusive of IT(42.2 vs 38.3) or median number of pharmacy claims (21.0 vs 22.8). Therewas a trend toward lower 18-month mean costs for inpatient services amongthose who received IT ($12,933 vs $13,347, p=0.052). Mean outpatient costsexcluding IT ($3,628 vs $6,504) or including IT ($4,502 vs $6,450), pharmacycosts ($2,737 vs $3,261), and total healthcare costs ($8,344 vs $11,934) weresignificantly lower among the IT versus the No-IT Group (all p< 0.0001).Con-clusions: Results suggest that, among children with AR, IT may confer a sig-nificant healthcare cost-offset benefit that is realized within 18 months of ITinitiation. This benefit appears to exceed the 18-month outlay for IT.
35TRIALS IN AN ENVIRONMENTAL EXPOSURE CHAMBER(EEC) CAN BE PERFORMED IN- OR OUT- OF THE NATURALPOLLEN SEASON: A RANDOMIZED, DOUBLE-BLIND,PLACEBO-CONTROLLED, TWO-WAY CROSSOVER STUDY INPATIENTSWITH SAR INDICATES NO DIFFERENCE IN EFFI-CACY OUTCOMES IN- OR OUT- OFTHE POLLEN SEASON.P. Patel*, M. Bates, J. Liu, P. D’Angelo,A. Salapatek,Mississauga, Canada.
Introduction: Allergic rhinitis (AR) has been studied using the “fieldmodel” where many patients are exposed to variable aeroallergen concentra-tions in the environment during limited pollen seasons. AR can also be stud-ied using the EEC model, where fewer patients are exposed to controlledpollen levels simultaneously at any time of year. This study examined if effi-cacy results vary between EEC studies conducted in- or out- of the ragweedseason. Methods: The protocol was approved by a national IRB and informedconsent obtained from all participants. Part 1 of the study took place duringthe ragweed season and Part 2, after the end of the season. Visits took placein an EEC. Each period consisted of two priming visits followed by a treat-ment visit [Cetirizine HCl 1x10 mg plus Pseudoephedrine HCl 2x60 mg (CPE)or Placebo]. Patients recorded nasal symptom scores using a 4 point scale.The primary endpoint was baseline adjusted Area Under the Curve (AUC)for TNSS. Changes from baseline were compared between treatment groupsusing ANCOVA. Results: A significant treatment effect (p<0.0001) wasobserved for CPE over Placebo during the ragweed season. There was adecrease in adjusted TNSSAUC of 11.5±9.66 for CPE compared to 4.94±7.50for Placebo. AUCs for each nasal symptom in TNSS showed larger decreasesfor CPE versus Placebo (all p values <0.0001). This was supported by the in-season mean TNSS scores and the mean scores for each nasal symptom. Sim-ilar results were obtained after the ragweed season with a decrease in adjustedTNSS AUC of 12.5 ± 9.92 for CPE compared to 5.55 ± 9.19 for Placebo(p<0.0001). This was also supported by the individual symptom score AUCs,the mean TNSS scores, and the mean scores for each nasal symptom. Thetreatment effect comparison between in and out of season data based on TNSSAUC was not significant (p=0.9681). Similar results were observed betweenseasons for the adjusted AUCs of all nasal symptoms (all p values > 0.5).Conclusions: The EEC is an ideal clinical model for the study of AR result-ing in reproducible and significant treatment effects using a minimal num-ber of patients, at any time of the year, in- or out- of natural pollen seasons.
36PREVALENCE OF ORAL BREATHINGANDASSOCIATED FAC-TORS IN PATIENTSWITH RESPIRATORYALLERGY.M.Treviño-Salinas, D. Muñoz-Mendoza*, A. Arias-Cruz, S.N. Gonzalez-Díaz, P.G. Rodriguez-Ortiz, A.A. Rojas-Lozano, D.A. Herrera-Castro,Monterrey, Mexico.
Introduction: Allergic rhinitis and asthma have been associated with cran-iofacial abnormalities due to there high association with oral breathing. Mate-rial and Methods: We conducted an observational and prospective study;patients with allergic rhinitis and asthma, between 6 and 15 years, whichwere seen for the fist time at our center during one full year, were included.Parents/caretakers signed a written consent form. A complete history andphysical examination were done, in order to document craniofacial abnor-malities. Patient’s parents answered a questionnaire inquiring about the snor-ing, day-time sleepiness and academic performance of their child. Results:One hounded and seven patients were included, 42 males (39.3%) and 65females (60.7%) with a mean age of 8.8 years. Allergic rhinitis was themost prevalent diagnosis in 80.4% (86 cases) of the patients, followed byasthma and allergic rhinitis in 19.6% (21 cases). Snoring episodes were clas-sified as mild 10.3%, moderate in 16.8%, and habitual snorers in 9.3%, theremaining 63.6% did not snore. On physical examination allergic shiners,
ABSTRACTS: CONCURRENT SESSIONS
VOLUME 102, JANUARY, 2009 A13
dry lips, thin upper lip, deep palate, and inadequate lip closure (55.1%, 51.4%,24.3%, 17.8%, and 16.8% respectively) were the most common findings.Twenty-nine percent of the patients gather more than 2 characteristics thuswere classified as oral breathers. Eighty-three percent of oral-breather patientshad >3 snore episodes/week compared to the 2% with nasal-breathing(p<0.001). Day-time sleepiness was documented based on the easiness forthe patient to fall asleep while traveling on car (23.4%), at school (2.8%),doing homework (4.7%), or while watching TV (6.5%), the rest of the patientsdid not present any of this symptoms. In 7.5% patients had excessive day-time sleepiness, defined as ≥2 of the previous characteristics. Ninety-twopercent of the children with sub-standard academic performance were thosewith oral breathing. Good conduct grades were most frequent in nasal-breathers than in oral-breathers (80% vs 20%, p<0.001). The prevalence oforal-breathing in patients with respiratory allergies was 29%. Conclusion:Oral-breathing is more prevalent in patients with respiratory allergies, thereincreased tendency to snore at night causes them to have day time sleepinesswhich impacts both on the academic performance and quality of life of thechildren.
37NASAL CONGESTION RELIEF IN SEASONAL ALLERGICRHINITIS (AR)WITHMOMETASONEFUROATENASALSPRAY(MFNS) MEASUREDWITH ACOUSTIC RHINOMETRY (ACR)AND SUBJECTIVE SYMPTOM SCORING CORRELATESWITHOVERALL QUALITY OF LIFE (QOL).
A. Salapatek*1, P. Patel1, G. Gopalan2, S.T. Varghese2, 1. Mississauga,Canada; 2. Kenilworth, NJ.
Background: Individuals with AR report nasal congestion as the mostbothersome symptom affecting their daily lives. Performed in an environ-mental exposure chamber (EEC) in which ragweed exposure was controlled,this study assessed effects of MFNS on nasal congestion using subjectivesymptom scoring and objective measurement of nasal patency with AcR.Correlation between nasal congestion relief and overall QOL was exam-ined. Methods: In a double-blind, placebo-controlled, IRB-approved study,310 ragweed-sensitive subjects, who gave informed consent, were exposedto controlled levels of ragweed pollen for 2 h, given MFNS 200 mcg orplacebo, and studied for 6 h postdose (Day 1). A subset of subjects (n=155)received MFNS 200 mcg or placebo QD in AM for next 6 days, returningto EEC on Day 8 (4 h of pollen exposure). Subjects rated nasal congestion(NSS-C; scale 0-3), predose and for 6 h postdose in EEC on Day 1, andprior to EEC entry and for 4 h postallergen exposure on Day 8. AcR meas-urements were performed before subjects entered EEC; at 2, 4, 6 h in EEC(Day 1); and at 22, 24, 26 h postdose in EEC (Day 8). Subjects completedEEC-specific rhinoconjunctivitis QOL questionnaire (measuring non-nasal/eye symptoms, practical problems, emotions, overall QOL) beforeentry and at exit on Days 1 and 8. Spearman correlation analyses examinedthe correlation between nasal congestion with overall QOL. Results: Whennasal congestion was relieved with MFNS treatment, with onset of 6 h,nasal patency was high and NSS-C score was low. AcR and NSS-C corre-lated with overall QOL moderately (r=-0.45) to strongly (r=-0.5), respec-tively (both P<0.05), 6 h after single-dose MFNS and 26 h after 7 daysMFNS. When nasal congestion worsened and nasal patency was low withplacebo, AcR (r=-0.41) and NSS-C (r=0.33) correlated with overall QOLsignificantly (P<0.05) and moderately on Day 8 after 7 days placebo dos-ing. Conclusion: Objective AcR measurement shows that single dose MFNS200 mcg/day relieves nasal congestion as early as 6 h. Relief of nasal con-gestion measured subjectively or objectively correlates moderately tostrongly with overall improvements in QOL indicating that MFNS providesclinically meaningful relief of nasal congestion and improvements in QOL.
38QUALITY OF LIFE IN SUBJECTSWITHALLERGIC RHINITISDIFFERSBYDISEASE SEVERITYBUTNOTBYDISEASETYPE.
C. Garris*, R. Stanford, B. Prillaman, Research Triangle Park, NC.Introduction: Both seasonal (SAR) and perennial (PAR) allergic rhinitis
may affect patients’ physical, emotional, and social functioning. This analysisexamines differences in patient reported QoL between SAR and PAR and acrossdisease severity levels.Methods:The Rhinoconjunctivitis Quality of Life Ques-tionnaire (RQLQ), a 28-item, self-administered, disease-specific instrument,was administered to SAR and PAR subjects (≥12 years) in cross-sectional studyFFU108675. Study centers obtained IRB approval and written informed con-
sent from all subjects. Each RQLQ question is scored 0-6; higher scores indi-cate more QoL impairment.Mean changes in RQLQ score >0.5 indicate a min-imal important difference (MID). Subjects evaluated severity of their nasal con-gestion, rhinorrhea, nasal itching, sneezing, and post-nasal drip symptoms over24 hours using a scale of 0-3 (none to severe). Scores were totaled to determineTotal Nasal Symptom Score (TNSS). Subjects were grouped by sub-type (SARor PAR) and severity (TNSS 2-5=Mild; TNSS 6-15=Moderate/Severe[Mod/Sev]). RQLQ differences between groups were analyzed usingANOVAadjusting for sub-type or severity, where appropriate. Results: A total of 410subjects were enrolled (88 Mild SAR, 112 Mod/Sev SAR, 99 Mild PAR, 111Mod/Sev PAR). Mean age was 37 years, 61%were female, and 27%were His-panic. Overall mean RQLQ scores were 1.3, 1.4, 2.8, and 3.2 for Mild SAR,Mild PAR, Mod/Sev SAR, and Mod/Sev PAR subjects, respectively. The dif-ference in overall RQLQ between all Mild (1.3) and all Mod/Sev (3.0) sub-jects was statistically significant (p<0.001) and met MID criterion. The dif-ferences in overall RQLQ betweenMod/Sev SAR (2.8) andMod/Sev PAR (3.2)subjects and between all SAR (2.1) and all PAR (2.3) were statistically signif-icant (p=0.035 and 0.015, respectively), but did not meet MID. There was nostatistically significant or clinically meaningful difference in overall RQLQscore betweenMild SAR (1.3) andMild PAR subjects (1.4). Conclusion:Therewas no clinically meaningful difference in rhinitis-related QoL across subtypes,but rhinitis-related QoL was worse in patients with moderate to severe diseaseregardless of SAR or PAR subtype. These findings support the current viewthat QoL is related more to disease severity than disease type; thus providersshould be more mindful of patient symptoms than type of allergen.
39ANALYSIS OF RHINITIS OUTCOMES QUESTIONNAIRES(ROQ), TREE- GRASS-RAGWEED (RW) COUNTS, AND DIS-TANCE BETWEEN POLLEN COUNTING STATION AND RESI-DENCES.
D. Dalan*, E. Fenstad, Fargo, ND.Rationale: Monitoring pollen counts from a central station is the cur-
rent approach as a surrogate for aeroallergen exposure of sensitive indi-viduals. Studies on total pollen counts suggest distances between countingstations from 5.6 up to 30 km apart as significant for patients, without patientdata. We now report significant relationships between specific pollen sen-sitive patients’ ROQ, grass-RW pollen counts, and their residences’ distancefrom a National Allergy Bureau (NAB) counting station. Methods: We fol-lowed 68 tree, 309 grass, & 79 RW sensitive patients yearly from 2000-2005, using the ROQ (www.acaai.org), determined pollen counts fromMay—Sept, and then usedArcPad, geographic information software to deter-mine distance between pollen counter and patient residence. Results: RWpatients’ average ROQ scores were inversely related, as the distance increasedaway from the counter, p=0.03. Their average ROQ score of 35 was signif-icantly highest, p=0.02 only within patient zip codes adjoining the counter.The RW pollen counts correlated only with ROQ scores of residences within19 km away from the counting station, Spearman’s rho=0.9, and p=0.037.Grass patients’ average ROQ score of 25 was significantly highest (p=0.05),and positively correlated (r=0.89 p=0.03), with grass pollen counts, only atresidences’ zip codes adjoining and less than16 km from the counting sta-tion. Tree sensitive patients’ ROQ did not correlate with, distance, nor pollencounts. Conclusions: This analysis suggests grass and RW pollen counts arerelevant to patients’ ROQ within 16 & 19 km of the Fargo NAB station.Variability in patient sensitivity, space-time exposure, bioaerosol potency,geographical, and plant distributions helps explain prior discrepancies ofdistances. This new information may account for these confounding fac-tors in explaining meaning of specific, not just total pollen counts, and givesaeroallergen reporting added functional—patient relevant information. Thiswill assist in locating counting stations, interpretation of pollen counts, andimprove health outcomes studies in research and clinical care.
ABSTRACTS: CONCURRENT SESSIONS
A14 ANNALS OF ALLERGY, ASTHMA & IMMUNOLOGY
Figure 1. Location of Fargo NAB counting station and RW subjects.40 km out with 5 km rings. Red circles are patient residences, and central ofthe circle is location of the pollen counter.
40EFFECTOFEVAPORATIVE (SWAMP)COOLERSONSKINTESTSENSITIVITYTODUSTMITESANDMOLDS INADESERTENVI-RONMENT.N.W. Wilson*, C. Prasad, M.B. Hogan, Reno, NV.
Introduction: Dust mites and molds are usually not found in home environ-ments with low humidity and have a lower prevalence in desert areas. Evapora-tive (swamp) coolers are devices that cool air through the evaporation of water.They are relatively inexpensive and require less energy than other forms of cool-ing but are only efficient when the relative humidity is low, restricting its effec-tive use to very dry climates. The device increases indoor humidity signifi-cantly. One previous study found increased dust mite levels in Colorado homescooledwith evaporative coolers.Thepurpose of this study is to determinewhetherevaporative cooling affects the skin test rate to dust mites and molds in patientsin a desert environment.Methods: Patientswith symptoms consistentwith asthmaor allergic rhinitis who were undergoing routine skin testing for molds, indoorallergens, grasses, weeds and trees were asked about presence of central, win-dow and evaporative cooler air conditioning in their home. All were tested toAspergillus,Alternaria,Cladosporium,Penicillum,Dreschlera,Curvularia,MoldMix II,Rhodotorula, Smuts,D. pteryonyssinus andD. farinae (Alk-Abello,RoundRock, Tx) using the prick technique with controls. Patients who used humidi-fiers frequently or who recently moved to the Reno, NV area were excluded.Results: 190 patients between the ages of 1 and 42 years (mean 5.4 years) wereevaluated. 59 of 190 (31%) had an evaporative cooler in their home. 25 of 59(42%) of those with evaporative coolers had a positive skin test to at least onemold compared to 26 of 131 (19%) without such coolers (Chi-square 10.5,p=0.001). 20 of 59 (34%) of those with evaporative coolers had a positive skintest to at least one dust mite compared to 23 of 131 (17.5%) without such cool-ers (Chi Square 6.2, p=0.013). Conclusions: In the desert, patients who live inhomes cooled by evaporative coolers are significantly more likely to have posi-tive skin tests tomolds or dust mites.This is most likely due to increased humid-ity caused by these devices. Patients with asthma and allergic rhinitis in homeswith evaporative coolers should be counseled about the increased risk for moldand dust mite allergy. Humiditymonitoring, swamp coolermaintenance and fil-ter changes should be discussed.
41THE PREDICTIVE VALUE OF SKIN TESTING IN THE DIAG-NOSIS OF LOCALANESTHETICALLERGY.B. McClimon*, M. Rank, J. Li, Rochester, MN.
Introduction: The 2008 “Allergy Diagnostic Testing: An Updated PracticeParameter” states, “Skin testing for diagnosis of local anesthetic allergy is
limited by false-positive reactions. The gold standard for establishing a diag-nosis of local anesthetic allergy is the provocative challenge.” Herein we reportone of the largest series of skin tests and challenges to determine the utility ofskin testing for local anesthetic allergy. Methods: A retrospective chart reviewwas performed on patients undergoing local anesthetic skin testing. Approvalwas obtained from the IRB and patients declining research authorization wereexcluded. Patients were included if they underwent prick (neat) and intrader-mal skin testing (1:100) followed by incremental subcutaneous challenge dosesup to 1 ml of local anesthetic. Skin prick test, intradermal tests, and subcuta-neous challenges were defined as positive if they had wheals 3 mm larger thanthe negative control. Results: One hundred seventy-eight patients underwent227 local anesthetic skin tests (some patients were tested to multiple anesthet-ics) and 224 challenges. Two hundred twenty (97%) of the skin tests were neg-ative. Of the negative skin tests results, 214 (97%) had negative challenge orprobable non-IgE mediated events during challenge. Three patients with sixnegative skin tests subsequently had a positive challenge due to local skin reac-tion. None of these patients experienced systemic symptoms. Seven skin testson five patients met the criteria for a positive skin test with the local anesthet-ics. One patient had an equivocal local skin reaction with subcutaneous chal-lenge without systemic effects. Three patients had a negative subcutaneouschallenge and one patient did not undergo a challenge. More than 60% of skintests/challenges were performedwith lidocaine.A smaller number of tests wereperformed with other local anesthetics. Conclusion:The overwhelming major-ity of patients in our study had negative skin tests to local anesthetics. A moreaccurate statement regarding the role of skin testing in local anesthetic allergymay be, “skin testing for diagnosis of local anesthetic allergy has an excellentnegative predictive value. Skin testing in combination with provocative chal-lenge is a safe and effective means to evaluate patients with local anestheticallergy.”
Table 1-Local anesthetic agents used for skin testing/challenge
42PREHOSPITAL ADMINISTRATION OF EPINEPHRINE FORANAPHYLAXIS.R.J. Hyde*, R.J. Campbell,W.W. Decker, L. Stead, D. Hankins, Rochester,MN.
Introduction: Although there is no universal consensus on the diagnosticcriteria for anaphylaxis, there is agreement that epinephrine is the treatment ofchoice. Prehospital management of patients with anaphylaxis has not been wellstudied. The objectives for this study are 1) To study the frequency of epi-nephrine administration for anaphylaxis in patients entering the EMS system,and 2) To determine the outcome of patients who received prehospital epi-nephrine. Description of Methods: Using unique identifiers, the prehospitaldatabase at our institution was queried between 2000 and 2005 to identify allcases of allergic reactions and anaphylaxis that were transported to our Emer-gency Department (ED). Anaphylaxis was defined based on NIH/FAAN 2005Symposium criteria. Data &Results:A total of 200 calls were received for com-plaint of allergic reaction or anaphylaxis during the study period. Of these,107 patients were found to have had an allergic reaction, and within this sub-set, 53 patients met criteria for anaphylaxis. Thirteen percent were children.Paramedics administered epinephrine to 14 of the 53 (26%) patients with ana-phylaxis, and an additional 4 patients (8%) received epinephrine prior to EMSarrival. Of the 18 patients who met criteria for anaphylaxis and received pre-hospital epinephrine, 5 (28%) were admitted to the intensive care unit (ICU),2 (11%) were observed in the ED observation unit and later discharged, and 12(67%) were discharged directly from the ED. Of the 53 patients with anaphy-laxis, 3 (6%) required epinephrine in the ED but had not received prehospitalepinephrine.Two of the three were subsequently discharged from the ED. Noneof the patients returned to the ED with a biphasic reaction. Conclusions: Inour study population, allergic reaction and anaphylaxis represented approxi-mately 1% of the total EMS call volume during the five-year study period.Thirty-four percent of patients who met criteria for anaphylaxis received pre-
ABSTRACTS: CONCURRENT SESSIONS
VOLUME 102, JANUARY, 2009 A15
hospital epinephrine. Of patients who received prehospital epinephrine, 28%were admitted to the ICU. Epinephrine may be underutilized in the prehospi-tal management of anaphylaxis, although many patients who did not receiveprehospital epinephrine did not require epinephrine after arrival to the hospi-tal. This study leads the way for further work investigating the use and out-comes of prehospital epinephrine for patients with anaphylaxis.
43RAPID ORAL DESENSITIZATION TO FUROSEMIDE IN APATIENTWITH SULFONAMIDEALLERGY.N. Alim*, J.Y. Patel, Houston, TX.
Introduction:Many patients are allergic to sulfonamides, and all oral loopdiuretics contain sulfonamide groups.There are rare reports of hypersensitivity tofurosemide, but severe reactions, including anaphylaxis, havebeen reported. Intra-venous ethacrynic acid, the only non-sulfonamide loop diuretic, is impractical foroutpatientuse.Protocols fordesensitization to furosemidehave included rapid intra-venousadministrationandoralprotocols lasting3-10days.Theoralprotocolswereperformed inpatientswithnon-type Ihypersensitivity reactions.Wepresent a rapid,oral protocol for desensitization in a patient with type I furosemide allergy.Meth-ods: A patient with type I hypersensitivity to furosemide was desensitized tofurosemide in amonitored, inpatient setting. She received increasing doses of oralfurosemideevery20minutes, startingwitha1μgdoseandendingwitha finaldoseof 100 mg over a three-and-a-half hour period. Results:The patient experiencedmild, self-limited pruritus during the protocol with the 1mg dose, but she experi-enced no rash or urticaria.The 1mgdosewas repeated and her prurituswas treatedwith diphenhydramine with complete resolution of symptoms.After desensitiza-tion she was started on her oral maintenance regimen. She was observed in thehospital for another two days and did not have urticaria or other manifestations ofhypersensitivity. She continued on this therapy successfully as an outpatient withthe understanding that the desensitization procedure would have to be repeated ifshe discontinued the medication for more than twenty-four hours. Conclusions:Progress in the diagnosis and treatment of hypersensitivity to sulfonamide drugswill require identification of the major antigenic determinant and standardizationof skin testing and RAST. As the incidence of heart failure increases in an agingpopulation, the need for loop diuretics is on the rise. Rapid oral desensitization toa loop diuretic has not been previously described.The potential advantages of oraldesensitization are that it is probably safer than intravenous desensitization; it maybe more cost-effective in terms of monitoring and staff requirements; and it maybe possible to perform in an outpatient setting.We propose our protocol as a novelapproach to furosemide desensitization therapy in patients with non-life-threaten-ing reactions to furosemide.
Background: Odontogenic infections commonly present to the emer-gency department (ED). The combination of penicillin (PCN) and metron-
idazole is effective but patient-reported PCN allergy often requires substi-tution with clindamycin, a more expensive medication with more potentialside effects. Previoulsy, we found that patients presenting to the ED with aPCN allergy history had a 91.3% false-positive rate of self-reported PCNallergy confirmed by PCN skin testing. Although PCN skin testing was fea-sible in the ED setting it was unclear whether it would be cost-effective ifused routinely. The purpose of this study was to determine the cost-effec-tiveness of ED-based PCN skin testing in patients with odontogenic infec-tions reporting a PCN allergy. Methods: A decision analytic model was con-structed evaluating the cost-effectiveness of two possible strategies inpatients with odontogenic infections self-reporting a PCN allergy: 1) skintesting using PCN major and minor determinants and antibiotic treatmentguided by results; and 2) empiric treatment with clindamycin. The 2007Medicare costs and National Physician Fee Schedule were used to captureED and hospital costs, including costs associated with complications anddeath. Analyses were conducted using Decision Maker® software. Results:In the base case analysis, PCN skin testing was the dominant strategy, beingboth more effective and less costly. Sensitivity analysis demonstrated PCNskin testing continued to have a marginal cost-effectiveness ratio less than$50,000 per quality adjusted life year until skin testing costs increased to> $657.10/patient. Similarly an increase in the % of patients with true PCNallergy >47.7%, a PCN anaphylaxis rate >82.5%, an anaphylaxis mortalityrate >12.6%, or an increase in the cost of a course of PCN and metronida-zole to >$723.37 would each independently increase the cost of the PCNskin testing strategy above a willingness to pay threshold of $50,000 perquality adjusted life year. Conclusion: PCN skin testing for ED patients pre-senting with odontogenic infections and self-reported PCN allergy is moreeffective and less costly than treating empirically with clindamycin.
Analysis of ED antibiotic treatment strategies
45PREDNISONE HYPERSENSITIVITY: WHAT IS THE ALTER-NATIVE DRUG?
T.M. Nsouli*, C.D. Schluckebier, E.J. McSorley-Gerard, Burke, VA.Background: Prednisone is commonly utilized for the treatment of severe
asthma andmany other allergic conditions because of its excellent anti-inflam-matory and immunomodulatory properties. Although immediate-type hyper-sensitivity to prednisone is rare, in some cases it could be confused with treat-ment failure. Objective: In this presentation we report three patients who wereallergic to prednisone and were able to well tolerate dexamethasone as an alter-native steroid preparation. Methods: We evaluated three patients necessitatingthe use of prednisone for severe asthma and urticaria.The first patient, a 38 y/oWFwith severe asthma, developed urticaria, facial angioedema, and increasedwheezing when treated with prednisone. The second patient, a 35 y/o BF withrecalcitrant urticaria, experienced flushing, angioedema, intense pruritus, andexacerbation of her urticaria after starting prednisone. The third patient, a 48y/oWFwith severe asthma, developed urticaria, facial angioedema, and pruri-tiswith the use of prednisone.Worsening of the patients’symptoms during pred-nisone therapy suggested treatment failure. However, the allergy evaluation thatincluded clinical history, allergy skin testing and provocative oral challengescollectively confirmed immediate hypersensitivity to prednisone. We substi-tuted dexamethasone as an alternative steroid to prednisone in order to treat notonly the patients’ initial allergic chief complaints but also to treat allergy symp-toms induced by prednisone. Of interest, all three patients had a history of sen-sitivity toASAandNSAIDS.Conclusion:Although prednisone-induced hyper-sensitivity is rare, clinicians should be aware of this possibility and should havea high index of suspicion in case of worsening of patient’s symptoms while onprednisone therapy, especially in individuals with ASA/NSAIDS sensitivity.Dexamethasone is an excellent steroid alternative in prednisone allergic patients.
ABSTRACTS: CONCURRENT SESSIONS
A16 ANNALS OF ALLERGY, ASTHMA & IMMUNOLOGY
Evaluation of 3 Patients with Prednisone Sensitivity
WT= Well toleratedPred= Prednisone, Dex= DexamethasoneASA : Aspirin, NSAID: nonsteroidal anti-inflamatory drug x= number of chal-lenges
46THE USE OF PENICILLIN SKIN TESTING TO ASSESS THEPREVALENCEOFPENICILLINALLERGY INANEMERGENCYDEPARTMENT SETTING.
J.A. Bernstein*, A. Raja, C. Lindsell, C. Codispoti, I.L. Bernstein,J. Moellman, Cincinnati, OH.
Background: Patient-reported penicillin (PCN) allergy can result in usingless effective and more expensive antibiotics that may contribute to the increas-ing prevalence of multi-drug resistant pathogens and increased costs to ourhealth care system, respectively. The objective of this study was to performPCN skin testing in the ED to assess the prevalence of PCN allergy and to per-form a decision cost analysis for treatment based on this testing. Methods: Aprospective observational cohort study enrolled a convenience sample of EDpatients with self-reported a PCN allergy at triage. All patients signed ainformed consent approved by an IRB. Patients were evaluated by skin pricktesting followed by intracutaneous testing, if necessary, to major and minorPCN determinants prepared according to previously published methods. Theproportion of false positive self-reported PCN allergies was computed and95% confidence intervals (CI95) were calculated using the score method.Groups were compared using Fisher’s Exact test or Student’s t-test. Results:150 patients were enrolled without adverse reactions. The average ED physi-cian testing time was 30 minutes. The false positive rate for self-reported PCNallergy was 137/150 (91.3%, CI95 85.3% to 95.1%). Among patients whomthe first choice antibiotic was not given due to a false positive PCN allergy(n=21), the mean antibiotic cost increased from $64.92 to $141.12 (meanincrease of $76.21, CI95 $18.21 to $134.21; p=0.013). Conclusions: PCN skintesting can be completed within 30 minutes and is therefore feasible in theED setting. A substantial number of patients with self-reported PCN allergyhave negative PCN skin testing indicating they do not produce specific IgEPCN antibodies and are not at increased risk for an IgE-mediated reaction.PCN skin testing may allow the use of first line, less expensive PCN antibi-otics in these patients, leading to substantial health care savings.
47ANAPHYLAXISWHILE CARVINGA PUMPKIN.
M. La Shell*1, C. Calabria1, B. Whisman1, A. White2, 1. San Antonio, TX;2. San Diego, CA.
BACKGROUND: IgE-mediated allergy to pumpkin is rare with data lim-ited to case reports. These cases describe systemic reactions after ingestion ofpumpkin soup (n = 1) and of pumpkinseed (n = 2). We present the first case ofa systemic reaction associatedwith cutaneous only exposure to pumpkin.METH-ODS: An 8 year old male with moderate-persistent asthma and known foodallergy to peach and soy developed ocular pruritus, swelling, nasal pruritus,sneezing and chest tightness while carving a pumpkin. He had no previous reac-tions to pumpkin. He had not ingested any of the pumpkin but did rub his eyesafter putting his hand inside the pumpkin. No other foods were eaten around thistime. His symptoms were treated at home with albuterol only and resolved withno further sequelae. RESULTS: Percutaneous skin testing was performed tofresh pumpkin and pumpkin seed demonstrating wheal and flare sizes of10mm/40mm and 4mm/20mm respectively. Antigen extract (excluding seedsand skin) was prepared from fresh pumpkin. Electrophoresis of the extract wasperformed by the sodium dodecylsulfate polyacrylamide gel electrophoresis(SDS-PAGE) technique to identify specific pumpkin proteins, and immunoblot-tingwas performed to determine if the patient had pumpkin specific IgE to theseproteins. SDS-PAGE revealed several protein bands, ranging from approximately
6-150 KDa. Immunoblotting revealed specific IgE to approximately seven ofthese bands ranging from 15-50KDa. CONCLUSION:This is the first reportedcase of pumpkin anaphylaxis due to cutaneous only exposure. Seven proteinsranging from 15-50 KDa in weight are the relevant antigens in this patient.
48PENICILLIN ALLERGY PATIENTS WITH A POSITIVE PENI-CILLIN SKIN TEST EXHIBIT INCREASED ADVERSE REAC-TIONSTO CEPHALOSPORINS.A. Harish*, C.A. Koch, P. Klemawesch, J.T. Li, M.A. Park, Rochester, MN.
Introduction: Up to 10% of patients with a history of penicillin allergy canhave an adverse reaction to cephalosporins. Recent studies state that it may besafer to administer cephalosporins to penicillin allergic patients than previouslybelieved.We conducted a case control study to determine whether patients withpenicillin allergy were at increased risk for adverse drug reactions when chal-lenged with a cephalosporin. Methods: A case control study was conducted.Patients with a history of a penicillin allergy and a positive penicillin skin testwho received a cephalosporin from February 1991 to June 2005 served as cases(N=85). Patients with a history of penicillin allergy and a negative penicillinskin test who received a cephalosporin from July 1, 2002 to September 16, 2003served as controls (N=682).The Institutional Review Board approved the studyand all subjects signed a written informed consent. Results: Five (5.9%) of 85cases had an adverse drug reaction to a cephalosporin as compared to five(0.7%) of 682 controls {Chi square test; OR = 8.5; 95% CI (2.4 to 30.0); P =0.0024}.We further stratified the adverse drug reactions to cephalosporins intolikely IgE-mediated reactions versus non-IgE-mediated reactions. The rate oflikely IgE-mediated adverse drug reactions to the cephalosporins was 2 (2.4%)of 85 amongst the cases compared to 1 (0.1%) of 682 amongst the controls{Fischer’s exact test, OR = 16.4; 95% CI (1.5 to 183.0); P = 0.0338}. Conclu-sion: A cautious approach is warranted in prescribing a cephalosporin in sub-jects with a history of penicillin allergy with a positive penicillin skin test asthere appears to be a greater risk for adverse drug reaction. Patients with a his-tory of penicillin allergy needing a cephalosporin would benefit from penicillinskin testing.
ADR: adverse drug reationCeph: cephalosporin
49WHY NEWBORN SCREENING FOR SEVERE COMBINEDIMMUNODEFICIENCY IS ESSENTIAL:A CASE REPORT .M. Adeli*, R. Buckley, Durham, NC.
Objectives: The importance of educating primary care physicians, espe-cially pediatricians, about normal ranges for ALC at different ages cannot beoveremphasized. This is especially true for those caring for infants in the firstfew months of life. During this time, any ALC <2500/mm3 is pathogenic andshould be evaluated. Patient : We report a 4 1/2 month old white female infantwith a 2 month history of a chronic oral ulcer, intermittent fever, recurrent oti-tis media, decreased appetite with weight loss, and an acute respiratory illnesswith hypoxemia. Since birth, she had been in an in-home daycare run by hermother. She had been seen frequently by her PCP and, in retrospect, persistentlymphopenia had been present in all blood counts performed, but this abnor-mality had not been appreciated by her caregivers. She was ultimately diag-nosed to have T- B- NK+ RAG 2 deficient SCID. However, because she hadalready developed two very difficult to treat viral infections, i.e. with parain-fluenza 3 and adenovirus, she did not survive long enough to be treated by abone marrow transplant. Within 5 days of the diagnosis of SCID, the adenovi-ral infection led to fulminating liver failure and a diffuse intravascular coagu-lopathy which led to her rapid demise. Until the time when neonatal screening
ABSTRACTS: CONCURRENT SESSIONS
VOLUME 102, JANUARY, 2009 A17
for SCID becomes available for all neonates (either by looking for lymphope-nia or CD3 or CD4 proteins in cord bood or by using Guthrie spots to quantifyT cell receptor excision circles) all physicians who care for infants should knowthe normal range for ALC at that age. If lymphopenia is present, the infantshould immediately be studied by flow cytometry and, if there are few or no Tcells, T cell function tests should be ordered immediately. Recognition of thecharacteristic lymphopenia can result in early diagnosis of SCID—even at birthand protect the infants from becoming infected before they can be transplanted.Newborn screening will not only give all SCID patients a chance to receive theearliest, most effective and economical treatment, but it will also reveal the trueincidence of SCID and define the range of conditions characterized by severelyimpairedT-cell development. Key words: Severe combined immunodeficiency(SCID), Absolute Lymphocyte Count (ALC)
Chest X ray revealed the absence of a thymic shadow and patchy atelectasis
50INCIDENCE & TEMPORAL TRENDS OF PRIMARY IMMUN-ODEFICIENCY IN OLMSTED COUNTY, MINNESOTA, USA: APOPULATION BASED COHORT STUDY.
Background: Although Primary Immunodeficiencies (PID) are oftendescribed as rare disorders, the true incidence of these diseases is not known.Methods: We undertook a historical cohort study to describe the epidemi-ology of PID in Olmsted County, MN,USA over a 31 year period( Jan.1,1976to Dec.31,2006) using the Rochester Epidemiology Project. All study pro-cedures & ethics were approved by the Institutional Review Board of MayoClinic & Olmsted Medical Center. The informed consent requirement waswaived by the IRB as this was a historic chart review study,only those chartswhere research authorization was provided were reviewed. Incidence andtrends over time, frequency of complications, other co-morbid conditions,and risk factors for mortality were determined. Results: Over the 31 yearstudy period, 158 new cases of PID were diagnosed with an overall inci-dence rate of 4.6 per 100,000 person-years.The rate of PID from 2001-2006(10.3 per 100,000 person-years) was nearly 5 times higher than from 1976-1980 (2.4 per 100,000 person-years) and nearly twice as high as from 1996-2000 (5.5 per 100,000 person-years). Older age at diagnosis was signifi-cantly associated with mortality (P=0.01).Longer delay in diagnosis was asignificant predictor of subsequent treatment with immune globulin(P<0.001), recurrent sinusitis (Wilcoxon Rank Sum test, P <0.0001) andrecurrent pneumonia (Wilcoxon Rank Sum test, P=0.03).Using Kaplan-Meier survival curves,the proportion of patients surviving at 10 years fromdiagnosis was nearly 95% which was comparable to the survival of age, sex& race matched referent subject from MN without PID (P=0.132). Con-clusion: With the first ever population-based study on the incidence of PIDin USA, we have found that the diagnosis of PID increased over the pastthree decades. This kind of epidemiological data is fundamental to raise theawareness of the medical community to primary immunodeficiency dis-
eases. Clinical Implications: Frequent, severe, or unusual infections shouldprompt a thorough immunodeficiency evaluation, because early recogni-tion may avoid considerable morbidity.
Overall and Age-Specific Incidence of Primary Immunodeficiency (PID) inOlmsted County, Minnesota, USA from 1976 to 2006.
51HYPOGAMMAGLOBULINEMIA AND HYPOCOMPLE-MENTEMIA ASSOCIATEDWITH AUTOIMMUNE NEPHRITISSUCCESSFULLYTREATEDWITH RITUXIMAB.A. Sreedharan*, S. Chegini, Hershey, PA.
Introduction: Secondary immunodeficiency must be excluded as the etiol-ogy of hypogammaglobulinemia and hypocomplementemia. In patients withsecondary immunodeficiencies, all attempts should be made to reverse theunderlying pathologic process to improve the immunologic status of the patient.Case: A 23 year-old female with seronegative systemic lupus erythematous,recurrent episodes of nephritis, undetectable C4 levels, and repeated sinopul-monary infections was referred for evaluation of immunodeficiency. Herglomerulonephritis was classified as stage IV/V mixed, diffuse proliferative.Therapeutic interventions had failed due to intolerable side effects with aza-thioprine and methotrexate, and increased frequency of sinopulmonary infec-tions with adalimumab and etanercept.Work up revealed an IgG of 280mg/dL,with normal IgM and IgA levels. Diphtheria and tetanus titers showed excel-lent responses post-vaccination. Urinary protein excretion was 2.53 g/ 24 hours,and urine immunofixation confirmed urinary loss of immunoglobulins. Sub-cutaneous IgG replacement was initiated, which decreased the frequency ofinfections; however increased doses were required due to urinary loss. Her pro-teinuria, C4 hypocomplementemia and arthralgias persisted.Methods: In com-parison to cyclophosphamide, the standard treatment for stage IV/Vmixed dif-fuse proliferative glomerulonephritis, rituximab is more targeted and avoidsbroad immunosuppression in a patient already affected by recurrent infections.We reviewed literature using the PubMed search engine using the terms “lupusnephritis” and “rituximab.” Treatment with rituximab 500 mg and methyl-prednisilone 100 mg was administered weekly to treat the underlying cause ofher immune deficiency. Results: We identified multiple case series of patientswith lupus nephritis successfully treated with rituximab. After three weeks ofrituximab, successful B cell depletion was accomplished. Two weeks follow-ing the fourth infusion of rituximab, the C4 level was within normal range andserum IgG increased by 35%. Urine protein excretion decreased to approxi-mately 900mg/24 hours. Conclusion:Treatment of autoimmune nephritis withrituximab reduced proteinuria, normalized C4 and increased IgG levels. Asproteinuria continues to decrease, the need for subcutaneous immunoglobulinmay be alleviated.
ABSTRACTS: CONCURRENT SESSIONS
A18 ANNALS OF ALLERGY, ASTHMA & IMMUNOLOGY
52RESULTS OF OPEN-LABELADMINISTRATION OF NANOFIL-TEREDC1-INHIBITORFORTHETREATMENTOFACUTEHAEATTACKS.B. Zuraw*1, W. Lumry2, D. Hurewitz3, J. Baker4, R. Levy5, M. White6,K. Anderson7, A. Grant8, M. Manning9, M. Riedl10, M. Davis-Lorton11,L. Bielory12,T. Craig13, P. Patel14, H. Li6, I. Kalfus15, P. Busse15, 1. La Jolla,CA; 2. Dallas, TX; 3. Tulsa, OK; 4. Lake Oswego, OR; 5. Atlanta, GA; 6.Wheaton, MD; 7. Bemidji, MN; 8. Galveston, TX; 9. Scottsdale, AZ; 10.Los Angeles, CA; 11. Mineola, NY; 12. Newark, NJ; 13. Hershey, PA; 14.Altamonte Springs, FL; 15. NewYork, NY.
Rationale: Two randomized controlled trials of nanofiltered C1 inhibitorconcentrate (C1INH-nf; Cinryze®, Lev Pharmaceuticals) for the acute andlong-term prophylactic treatment of HAE were recently completed. To obtainadditional information about the efficacy and safety of C1INH-nf for HAE, anopen-label extension study was initiated and is ongoing. Methods: 88 subjectswith documented HAEwere screened and enrolled in an acute treatment open-label extension protocol. Subjects were eligible to receive open-label injectionsof C1INH-nf (1,000 units i.v.) for acute attacks of angioedema occurring at anylocation. Subjects could receive a second open-label injection of 1,000 unitsC1INH-nf 60 minutes after the first injection if they had not begun to improve.24 subjects have been followed for greater than one year. Results: 447 attackswere treated in 82 subjects (32.9% male) who had at least one attack. Numberof attacks ranged from 1-57 with a mean of 5.45 ± 8.28 and amedian of 3. Sub-jects received 1 injection for 287 attacks and 2 injections for 160 attacks. Theprimary location of treated attacks was: extremities – 68; facial – 48; gas-trointestinal – 272; genitourinary – 9; and laryngeal – 50. The median time toimprovement was 30minutes in the 447 attacks with 93.4% reporting improve-ment within 4 hours. This was irrespective of whether subjects received open-label C1INH-nf <4 times, ≥4 times, or ≥10 times. Responses were similar inall attack locations. None of the subjects in this study treated for laryngealattacks required hospitalization or intubation. There were no serious adverseevents secondary to C1 INH-nf administration. Conclusions: C1INH-nf waseffective and safe for the treatment of all types of acute HAE attacks. Theseresults are consistent with clinical experience in Europe and support use ofC1INH-nf as the gold standard for the treatment of acute HAE attacks.
53EFFECTSOFDESLORATADINEONHUMANSKINMASTCELLACTIVATIONAND MEDIATOR RELEASE.K.Weller1, M. Maurer1, G. Gopalan*2, 1. Berlin, Germany; 2. Kenilworth,NJ.
Introduction. Mast cell (MC) activation and subsequent release of media-tors (eg, histamine) are responsible for most symptoms of allergic disease.Although current therapies are typically directed toward blocking the H1-his-tamine receptor, inhibition of mediator release from MCs may offer anotherapproach. Recent research has suggested that some antiallergic effects of deslo-ratadine (DL)may be due toMC stabilization.Methods. Human skinMCswerepreincubated with different concentrations of DL (ranging from 1 x 10–8 to 1x 10–4 M) or vehicle prior to stimulation with anti-immunoglobulin E (IgE),Ca-ionophore, and substance P. Expression of CD107a (a marker of MC acti-vation and degranulation) was assessed, and histamine release was quantified.Cell toxicity was determined via trypan blue staining. Two-tailed Student’s ttest for unpaired samples was used for statistical analysis. Results. Comparedwith vehicle, pretreatment with DL markedly inhibited CD107a expression onhuman skin MCs after stimulation with all test substances (P<0.05). Thestrongest inhibitory effect of DL on this marker occurred in response to stim-ulation with anti-IgE (50.7%; P<0.05), followed by substance P (48.0%;P<0.005) and Ca-ionophore (26.7%; P<0.01). The inhibitory action of DLwas dose dependent with all 3 substances. In addition, preincubation with DL,as opposed to vehicle, was associated with profound inhibition of IgE-depend-ent histamine release by MCs. The inhibitory effect was 42.6% (P<0.005) atthe highest DL concentration (1 x 10–4 M). Compared with vehicle, DL pre-treatment also reduced histamine release in response to Ca-ionophore; the effectwas 39.9%, achieved at the highest DL dose (P<0.005). The inhibitory effectof DL on substance P-induced histamine release was 53.7% at the highestconcentration (P<0.01); however, even the lower concentrations (1 x 10–6 Mand 1 x 10–8 M) led to significant inhibition (9.8% and 13.0%, respectively;P<0.005 for both). DLwas not cytotoxic at the concentrations used in this study.Conclusion. DL strongly inhibits activation of human skin MCs as well as
subsequent histamine release. These inhibitory effects are not limited to IgE-dependent stimulation but also extend to IgE-independent pathways.
54HUMANMASTCELLS STIMULATEBRONCHIALEPITHELIALCELLSTOPRODUCEPLASMINOGENACTIVATOR INHIBITOR-1VIATGF-BETAANDACTIVINA.S.H. Cho*, S. Shin, A. Kato, R. Schleimer, Chicago, IL.
Introduction: Mast cells (MC) have been known to be associated with theairway remodeling in asthma. We previously reported that human MC are animportant source of plasminogen activator inhibitor (PAI)-1 and PAI-1 pro-ducing MC are associated with fatal asthma.We hypothesized that MC are notonly an important source of PAI-1 in the airways in asthma but also influenceother resident cells such as epithelial cells (EC) to produce PAI-1 to promoteairway fibrosis in asthma. Methods: We cultured the human mast cell line,LAD2, and stimulated the cells with IgE-receptor cross-linking, substance P(SP), and compound 48/80 (48/80) for 30 minutes and 24 hours. We collectedthe supernatants from the resting and stimulated MC and incubated the humanbronchial epithelial cell line, BEAS-2B with the MC supernatant for 24 hours.Supernatants from BEAS-2B were harvested and the level of PAI-1 was meas-ured. We further tested the role of TGF-beta and activin A in the MC super-natants using specific neutralizing antibodies. Results: Resting BEAS-2B pro-duced 10 to 100 fold higher amounts of PAI-1 compared to human MC.Whenthe supernatants from restingMC andMC stimulated for 30 minutes with IgE,SP, and 48/80 were added to BEAS-2B, there was no significant change in PAI-1 production. However, when the supernatants from LAD2 stimulated for 24hours with IgE, SP, and 48/80 were added to BEAS-2B, there was more than2 fold enhancement of PAI-1 production fromBEAS-2B.TGF-beta and activinA, members of theTGF-beta superfamily, have been known to be released fromMC and stimulate bronchial EC to produce PAI-1. To investigate the role ofTGF-beta and activin A among the newly formed MC mediators in the pro-duction of PAI-1 from EC, we pre-incubated BEAS-2B supernatants with neu-tralizing antibodies for TGF-beta and activin A for 1 hour, added the super-natants to BEAS-2B, and incubated for 24 hours. Both TGF-beta or activin Aneutralizing antibodies significantly reduced the MC-induced production ofPAI-1 from BEAS-2B and this blocking effect was greater when both TGF-beta and activin A antibodies were added. Conclusions: This study suggeststhat humanMCmay have an important role in the airway remodeling of asthmanot only as a source of PAI-1 but also by influencing other resident cells suchas bronchial EC to produce PAI-1.
55INPATIENTCONSULTATIONOFALLERGY/IMMUNOLOGY INATERTIARY CARE SETTING FROM 2001-2007.H.F. Otto*, R.W. England, J.M. Quinn, Lackland AFB, TX.
Introduction: Few studies have examined inpatient referral patterns for fel-lowship training programs. Only two studies have looked at the inpatient consul-tations for allergy/immunology (AI). Since that time, significant changes in bothmedicine and the military have occurred but no further AI inpatient studies havebeen conducted. Methods: Our protocol was approved by our IRB.We performedaretrospectivechart reviewofall inpatientAIconsultations from1July2001 through30 June 2007. Our primary endpoint was the reason for consultation and second-aryendpoints includedAIdiagnosismade,AI recommendationandAIunique test-ing offered. This study incorporated 14 years of data from the previous studieswithanadditional6yearsofdata for analysisof trendsandchanges.Results:A totalof 254AI inpatient consults were reviewed.Thirty six percent (92 of 254) of inpa-tient consultswere forevaluationofadversedrug reactions (ADR),22%(55of254)miscellaneous reasons, 17%(43of254)angioedema/urticaria, 13%(32of254) forpossible immunodeficiency, 9% (23 of 254) for anaphylaxis and 3% (8 of 254) forasthma. Forty six percent (42 of 92) of the ADR consults were due to penicillin.Compared to the previously reported data, we found an 85% and 23% decrease inasthma and penicillin-related consults, respectively.Themost common reason forconsultingAI varies by age group; immunodeficiency was themost common rea-son in thepediatricagegroup(32%;20of63)whilepenicillin-relatedconsultswerethe most common reason in the adult age group (19%; 36 of 191). AI inpatientconsults show a continued decline over the 6 years studied despite stable total hos-pital admissions since 1998. Conclusions: Identifying consultation trends pro-vides a guide for education of AI fellows and primary care residents. The periodstudied shows a continued decline in the total number of consults, specificallyasthmaandpenicillinconsults,overourstudyperiodcomparedtopreviouslyreporteddata. The lack of penicilloyl skin test is associated with diminished consults for
ABSTRACTS: CONCURRENT SESSIONS
VOLUME 102, JANUARY, 2009 A19
penicillin allergy. Inpatient consultation is playing a diminishing but still impor-tant role inAI training as it provides unique opportunity for evaluation and treat-ment of serious life threatening diseases.
56MARKERS OF IMMUNE TOLERANCE IN SUCCESSFULLYTREATED EOSINOPHILIC ESOPHAGITIS.
N. Reshamwala*, J. John, J. Huang, K. Nadeau, Palo Alto, CA.
Introduction: Eosinophilic esophagitis(EE) is an allergic inflammatory con-dition of the esophagus in children and adults. The pathophysiological basis ofthe condition is not well understood, but the intake of certain foods may playa role.Treatment strategies include removal of the offending food,proton pumpinhibitors,swallowed steroids, anti-histamines,and, in investigational reports,the anti-IL5 monoclonal antibody mepolizumab. Methods: 35 subjects (n=20with EE treated with dietary changes and oral budesonide whowent into remis-sion, n=10 with GERD, n=5 with refractory EE)with mild to severe disease and5 healthy controls (HC)were analyzed using esophageal biopsy immunohisto-chemistry (IHC),ELISA studies on plasma, and FACS analysis of peripheralblood for markers associated with remission. Remission was determined bylack of symptoms and 0-1 eosinophils per high powered field upon re-biopsy.Approval was obtained from the Stanford IRB and written informed consentobtained from all research subjects. Results: Molecular markers associated withimmune tolerance such as Foxp3+CD4+CD25hiCD127lo (naturalTreg),TGF-beta, and IL-10 were decreased by up to 5 fold in the esophagus, peripheralblood cells,and plasma in EE subjects compared to HC. In addition, after lon-gitudinal studies in the same EE subjects, naturalTreg were found in the esoph-agus during remission but not during relapse. Dietary changes that includedonly an elemental diet were associated with higher numbers ofTreg in the esoph-agus (by 50%) and with higher levels of TGF-beta and IL-10 in plasma (up to2 fold) of EE patients as compared to dietary changes that included only exclu-sion of some food items. Swallowed budesonide in combination with dietarychanges was associated with the most increase in Treg numbers in the esoph-agus as compared to swallowed inhaler-steroids with dietary changes. Refrac-tory EE subjects were found to have decreasedTGF-beta and IL-10 in the plasmacompared to treated EE subjects. Refractory EE subjects had increased Th2cytokines and fibrotic factors in their plasma compared to treated EE subjects.Conclusion: The data suggest that natural Treg, TGF-beta and IL-10 are asso-ciated with EE disease in remission.Thesemarkers could be helpful in the man-agement and assessment of treatment progress in EE.
57RETROSPECTIVE POPULATION PHARMACOKINETICS OFLEVOCETIRIZINE IN CHILDREN FROM 6 MONTHS TO 6YEARS.
Introduction: the objectives of this study were: 1) identify the importantcovariates affecting the pharmacokinetic (PK) parameters of the antihistaminelevocetirizine; 2) recommend dosing regimens for children aged 6 months to6 years. Method:A retrospective population pharmacokinetic analysis was car-ried out by nonlinear mixed-effect modeling using NONMEM VI. Levoceti-rizine concentration-time data were obtained in 324 adult and pediatric sub-jects from nine clinical trials, following single or multiple doses for a durationranging from 4 weeks to 18 months. The influence of the following factors onpharmacokinetics was examined: gender, weight, BSA, age, creatinine clear-
ance, health condition, and fasted or fed intake. Monte-Carlo simulations ofdifferent dosing regimens were then performed to compare the concentrationsin children to those in adults receiving the approved dose of 5 mg once daily.A two-compartment model parameterized in terms of absorption rate (KA),clearance (CL/F), volumes of distribution of the central (V2) and peripheral(V3) compartments, and intercompartment clearance (Q) was fitted to the data.Weight was incorporated as a covariate on CL/F, V2, V3 and Q. Two dosingregimens, 1.25 mg once daily and 1.25 mg twice daily, were simulated in 6-12months old children. Results: 181 patients were under the age of 6 (median:3.2 years); 18 patients were between the age of 6 and 16 (median: 8.0 years)and 124 patients were adults above 16 years of age (median 34.7 years). Themedian Cmax of a 1.25 mg once daily dosing regimen remained within therange of concentrations in adults (199 to 462 ng/mL) whereas the ones fol-lowing 1.25 mg twice daily exceeded the adult range for the youngest childrenfrom 6 to 8 months of age with values reaching 516 ng/mL. For 1-6 years oldchildren, simulations of a 1.25 mg twice daily regimen indicated that concen-trations remained in the adult range. Body weight was the only covariate foundto influence significantly the PK parameters. Conclusion: Levocetirizine’s phar-macokinetics is mainly dependent on body weight. The recommended dosingregimen of levocetirizine is 1.25 mg once daily in 6-12 month old children and1.25 mg twice daily in 1-6 year old children.
58BEPOTASTINE BESILATE OPHTHALMIC SOLUTION 1%REDUCES NASAL CONGESTION AT 8 HOURS FOLLOWINGDOSING IN A CLINICAL MODEL OF ALLERGIC CONJUNC-TIVITIS.
G.L. Torkildsen*1, P.J. Gomes2, J.I. Williams3, J.A. Gow3, M.B. Abelson2,T.R. McNamara3, 1. North Andover, MA; 2. Andover, MA; 3. Irvine, CA.
Introduction: To establish the efficacy and safety of bepotastine besilateophthalmic solution 1%, an investigational anti-histamine eye drop, comparedto placebo in reducing nasal congestion using the ConjunctivalAllergen Chal-lenge (CAC) clinical model of allergic conjunctivitis at 8 hours after ophthalmicdosing. Methods: Single center, double-masked, randomized, placebo-con-trolled, 7 week clinical trial using the CACmodel of allergic conjunctivitis.Theclinical trial was approved by an Institutional Review Board (IRB). Eligiblesubjects were assigned randomly to either bepotastine besilate ophthalmic solu-tion 1% (n=36) or placebo (n=36). Results: Bepotastine besilate ophthalmicsolution 1% was clinically superior to placebo (P ≤ 0.012) at all observationtime points 8 hours after dosing for reducing CAC-induced nasal congestion,with no incidence of treatment emergent ocular adverse events. Clinical supe-riority was defined as both clinical significance and statistical significanceaccording to predetermined criteria, including recognition of the need for sta-tistical multiplicity corrections as a result of the unique clinical trial design.One subject in the placebo treatment group was withdrawn because of non-compliance. No subjects were withdrawn from the bepotastine besilate oph-thalmic solution 1% treatment group during the clinical trial. Additional fol-low-up visits were not needed for any of the enrolled subjects. Conclusions:Bepotastine besilate ophthalmic solution 1%was clinically superior to placeboin reducing nasal congestion in the CAC model of allergic conjunctivitis at 8hours after ophthalmic dosing. The positive 8 hour dosing schedule resultsstrongly suggest that bepotastine besilate ophthalmic solution 1%may be dosedeffectively for reducing nasal congestion associated with allergic conjunctivi-tis when used twice daily.
59EFFICACYANDTOLERABILITYOFSECONDANDTHIRDGEN-ERATION ANTIHISTAMINES IN THE TREATMENT OFACQUIRED COLD URTICARIA.
M.E. Weinstein*1, L. Bielory2, 1. Montclair, NJ; 2. Newark, NJ.
Introduction: Acquired cold urticaria (ACU) is a rare form of physicalurticaria that has been treated with first generation antihistamines (1AH), andrecently with better tolerated, non-sedating second (2AH) and third generationantihistamines (3AH). Effective suppression of symptomswith the 1AH cypro-heptadine is well documented, but there is a paucity of data regarding selec-tive antihistamines.We performed a meta-analysis in order to demonstrate theefficacy and tolerability of 2AH and 3AHmedications in the treatment ofACU.Methods: Data were extracted via MEDLINE search of literature from 1950through July 2008. Double-blind randomized controlled studies comparingthe treatment ofACU patients with 2AH and 3AHmedications versus placebo
ABSTRACTS: CONCURRENT SESSIONS
A20 ANNALS OF ALLERGY, ASTHMA & IMMUNOLOGY
were included. Results: Using the terms “cold urticaria” and “antihistamine”,68 articles were mapped, of which 6 clinical trials involving 2AH and 3AHmedications were identified. Four trials were included, with 2 trials excludedbecause they were not double-blinded. Three trials looked at the effect of 2AHmedications (ebastine, acrivastine and mizolastine) and one trial looked at theeffect of a 3AH medication (desloratadine). Overall, 79 subjects were identi-fied, ranging in age from 15 to 70, with females outnumbering males 72% to28% (pooledOdds Ratio (OR) 5.06, 95%Confidence Interval (CI)=2.39, 10.71).Two trials indicated that 2AH and 3AH medications significantly eliminatedthe presence of wheals after treatment versus placebo (OR 27.11, 95%CI=10.47,70.2).Three trials demonstrated a significant elimination of pruritus with 2AHand 3AH treatment versus placebo (OR 10.53, 95%CI=4.91, 22.61).There wasno significant reduction in the presence of erythema after cold stimulation withAH treatment versus placebo. Two studies assessed the tolerability of a 2AHversus placebo and found no significant increase in adverse events. Moreover,one trial compared a 2AH to both placebo and 1AH, demonstrating a signifi-cant increase in tolerability to both (p=0.013 and p=0.021, respectively). Con-clusions: The newer, non-sedating antihistamines appear to be effective in thetreatment of ACU in terms of their ability to significantly reduce the presenceof wheals and pruritus after cold exposure. These medications are well toler-ated, and in some cases, better tolerated than their first generation counterparts.
60INHIBITORY EFFECTS OF FLAVONOIDS EXTRACTED FROMLICORICEON IPOPOLYSACCHARIDE-INDUCEDACUTEPUL-MONARY INFLAMMATION IN MICE.X.Yicheng, D. Xinwei,W. Ximei,Y. Xiaofeng, X. Qiang-min*,Hangzhou,China.
Airway inflammation plays important roles in the pathogenesis of acute res-piratory distress syndrome (ARDS), asthma and chronic obstructive pulmonarydisease (COPD), and anti-inflammatory treatment effectively improves thesymptoms of these diseases.To develop the potentially therapeutic compoundsfor the treatment of pulmonary inflammation, we investigated the effects oflicorice flavonoids (LF) extracted from the roots of Glycyrrhiza uralensis(licorice) on lipopolysaccharide (LPS)-induced acute pulmonary inflammationin mice.Acute pulmonary inflammation was induced by intracheal instillationwith LPS, treatment with LF at dosages of 3, 10 and 30 mg/kg significantlyreduced the LPS-induced inflammatory cells, including neutrophils,macrophages and lymphocytes accumulation in bronchoalveolar lavage fluids(BALF), among these inflammatory cells, LF predominately inhibited neu-trophil infiltration, and the maximal effect (30 mg/kg) was as comparable asdexamethasone treatment at 1 mg/kg. Consistent with its effects on neutrophilinfiltration, LF treatment significantly increased LPS-induced BALF super-oxide dismutase activity, and significantly decreased lung myeloperoxidaseactivity as well. Furthermore, treatment with LF at 30 mg/kg significantlyreduced LPS-induced lung TNF and IL-1 mRNA expression at 6 h and 24 hafter LPS instillation, respectively. Finally, LF at different dosages not only sig-nificantly decreased the elevation of lung water content, but also markedlyattenuated LPS-induced histological alteration. Therefore, we suggest that LFeffectively attenuates LPS-induced pulmonary inflammation through inhibi-tion of inflammatory cells infiltration and inflammatorymediator release whichsubsequently reduces neutrophil recruitment into lung and neutrophil-medi-ated oxidative injury, and this study provides with the potential rationale fordevelopment of anti-inflammatory compounds from flavonoid extracts oflicorice. * Corresponding author: Xie Qiang-min
61THE HIGH-RESOLUTION STRUCTURE OF MOMETASONEFUROATE BOUND TO HUMAN GLUCOCORTICOID RECEP-TOR.W.D.Tolbert1, H.E. Xu1, H.Wang2, C.A. Lesburg*2, R.Aslanian2, K. Suino-Powell1, 1. Grand Rapids, MI; 2. Kenilworth, NJ.
Mometasone furoate (MF) is the active pharmaceutical ingredient inmarketed drugs such as Nasonex®, Elocon®, and Asmanex®. It is a potentcorticosteroid anti-inflammatory prescribed for relief of nasal allergy symp-toms, skin conditions such as eczema, and asthma. MF is the first drug toincorporate a C17 furoate group to improve its binding and pharmacolog-ical and pharmacokinetic properties. In order to understand the molecularbasis of MF binding to its receptor – and the role of the C17 furoate group
in particular – we determined the crystal structure of MF bound to the lig-and-binding domain (LBD) of the human glucocorticoid receptor (GR). At2.0 Å, this structure represents the highest-resolution GR/ligand complexsolved to date. Details of ligand binding and the surrounding water mole-cules are well defined in this high-quality structure. The GR/MF complexis bound to a peptide derived from steroid receptor coactivator-1 (SRC-1),unlike previously-published GR-LBD structures. An analysis of this struc-ture is presented together with a comparison to other GR/ligand complexes.
62MEASURING AND COMPARING THE CONCENTRATION OFEXHALEDNITRICOXIDE (FENO)AMONGOBESENON-ASTH-MATIC ADOLESCENTS (ONA), OBESE ASTHMATIC ADOLES-CENTS (OA), EUTROPHIC NON ASTHMATIC ADOLESCENTS(ENA)AND EUTROPHICASTHMATICADOLESCENTS (EA).K.M.Aguilar Albavera*, J.J. Sienra Monge, B.E. Del Rio Navarro, J. DelRio Chivardi, Mexico City, Mexico.
Introduction:Asthma is a chronic inflammatory disease of the respiratorytract. It is suggested that adipose tissue leads to an inflammatory state. In recentyears, FeNO has been used to measure respiratory tract inflammation.The aimwas to measure and compare FeNO concentrations between obese adolescentswith and without asthma and eutrophic adolescents with and without asthmaMethods: A descriptive, transversal study in a group of adolescents ages 10to 16 years, obese and eutrophic, with and without asthma. Approval wasobtained from the Hospital IRB and written informed consent obtained fromthe parents of all research subjects. The quantity of FeNO was measured bychemoluminiscence using a standardized technique approved by the Ameri-can Thoracic Society. Measurements of central trend (mean and median) anddispersion (standard deviation and confidence interval) were estimated. Results:A total of 334 subjects were enrolled. The OA: n=87, mean FeNO: 37.07 ppb(SD 31.63 and 95%CI 30.07-44.49); the ONA group: n= 149 mean FeNO:26.73 ppb, (SD 20.05 and 95%CI 23.48- 29.97); the EA group: n=38 meanFeNO: 63.58 (SD 31.04 and 95%CI 53.36- 72.77); and the ENA group: n=50mean FeNO: 39.47 (SD 28.30 and 95%CI 31.42-47.51). The ANOVA analy-sis observed a significant difference between the groups (p=<0.001). In thepost hoc correction, we observed that the OA group has a significant differ-ence from the ONA group (p=0.026) and with the EA group (p<=0.001), butnot with the ENA group (p=1.00). Both the ONA group and the EA grouphave a significant difference from the other three groups (p<=0.05). Conclu-sions: In both groups (obese and eutrophic) we observed that FeNO levels arehigher in the asthmatic group, which correlates with previously published lit-erature. It was in the eutrophic asthmatic group that we observed the highestFeNO levels. The explanation for this phenomenon may be varied and is attrib-uted to possible causes: Mechanical: low lung volumes, reduced airway cal-iber, and increase of respiratory tract wall thickness. Metabolic: alteration inoxide-reduction of NO secondary to oxidative stress produced by obesity. Con-sequently, there are more variables to analyze to arrive at a possible explana-tion of this phenomenon.
ABSTRACTS: CONCURRENT SESSIONS
VOLUME 102, JANUARY, 2009 A21
63VALVED-HOLDING CHAMBER TECHNIQUE IN PEDIATRICHOUSESTAFF: STRUCTURED VERSUS CONVENTIONALTRAINING.S. Kaipa1, M. Reddy*1, D. Strom1, R. Neugebauer2, 1. Bronx, NY; 2. NewYork, NY.
BACKGROUND: Proper technique when using a metered-dose inhalerwith a valved-holding chamber (MDI/VHC) is a critical patient self-manage-ment skill. Providers learn the demonstration (DEMO) of this technique dur-ing medical training via conventional methods (observation, modeling, on-the-job training). Objectives of this study were to: 1) survey pediatric housestaff(HS) skill and experience with MDI/VHC; 2) conduct structured, one-on-onetraining to HS on the correct DEMO of MDI/VHC use to patients; and 3)observe differences between HS receiving conventional versus structured train-ing.METHODS: (see table for characteristics of study groups) 31 pediatric HSat varying training levels completed a brief survey to assess past experiencewithMDI/VHC. Using a validated 9-point scale, a faculty allergist scored eachHS’s DEMO skills at t=1. Group B recieved structured training (one-on-one,step-by-step re-DEMO) at t=1 then DEMO re-scoring at t=2. Analyses weredone by SPSS 16.0. Approval was obtained from the BLHC IRB; informedconsent was waived for this quality improvement (QI) study. RESULTS: All31 HS were foreign medical graduates with diverse educational/national expe-riences in treating asthma. 77% reported previously prescribing MDI/VHC toa patient; 67% reported conducting previous MDI/VHC DEMO to a patient;32% reported having previous, formal one-on-one training on properMDI/VHCDEMO. Group B (mean=5.08) at t=2 scored higher than groupA (mean=4.17)at t=1 (p=0.07 on a two-tailed t-test), suggesting that structured training couldbe more beneficial than conventional training in retaining the steps of thisDEMO skill. In addition, group B scores (mean=2.91) for the DEMO portionat t=1 drastically improved by t=2 (mean=5.08), suggesting a successful inter-vention (p<0.05 on a paired sample t-test). Ongoing QI studies will include alarger sample size withmultiple intervention points of structured training. CON-CLUSIONS: In order to maximize patient self-management skills, HS musthave the expertise to confidently apply the up-to-date evidence and teach effec-tive device utilization. Training programs should consider including struc-tured instruction in order for HS to develop important outreach, education andcommunication skills, especially when working with populations (e.g. inner-city, new immigrants) historically at high-risk for poor disease control.
Methods: Conventional versus Structured Training
In the interest of quality improvement, groupA also received structured train-ing at t=1, though this was not relevant to the study design.
64EFFICACYANDSAFETYOFMOXIFLOXACIN 5-DAYTHERAPYVS PLACEBO INACUTE BACTERIAL SINUSITIS.J.A.Hadley*1, R.Mosges2,M. Poole3,M.Desrosiers4, D.Haverstock5, D. vanVeenhuyzen5, Z. Herman-Gnjidic6, 1. Rochester, NY; 2. Cologne, Germany;3. Savannah, GA; 4. Montreal, Canada; 5. West Haven, CT; 6. Toronto,Canada.
Objectives: To evaluate the efficacy and safety of moxifloxacin (MXF)400mg q.d. for 5 days in the treatment of acute maxillary bacterial sinusitis(ABS).Methods:This was a prospective, multi-center, 2:1moxifloxacin:placeborandomized, double-blind, Phase III trial. Subjects with ABS defined by clin-ical, radiological and bacteriological criteria received MXF 400mg PO or amatching placebo q.d. for 5 days. Concomitant symptom-relief medicationswere allowed. A sinus tap was performed at baseline to obtain a sample forculture. The ethical review panel from each centre approved the protocol andwritten informed consent was obtained from all study subjects. The primaryendpoint was clinical response at test-of-cure (TOC), 1–3 days after the end oftherapy in the modified intent to treat (mITT) population (subjects with posi-tive culture for one of five pre-specified pathogens). Time to symptom reliefwas based on the Sinonasal Outcome Test-16 (SNOT-16). Results: The ITTpopulation consisted of 374 subjects (MXF n=251, placebo n=123) of whom118 (n=73MXF, n=45 placebo) were in the mITT population. Clinical successrates were numerically higher in the MXF arm at TOC than in the placebo arm(n=57/73 [78.1%] vs n=30/45 [66.7%]); P=0.189). Clinical failure rates were19.2% (14/73) forMXF-treated subjects and 33.3% (15/45) for placebo-treatedsubjects. MXF-treated subjects also experienced significantly greater meanreductions in SNOT-16 scores than placebo-treated subjects at TOC (–17.54vs –12.83; P=0.032). At TOC, overall concomitant medication use was lowerin theMXF vs the placebo arm (n=28/73 [38.4%] vs n=25/45 [55.6%], respec-tively). Overall, premature discontinuation due to insufficient therapeutic effectwas significantly lower in the MXF vs the placebo arm (n=21/251 [8.4%] vs20/123 [16.3%]; P=0.022).The rate of treatment-emergent adverse events (AE)was similar between arms (MXF n=96/251 [38.2%], placebo n=50/123 [40.7%])as was the rate of serious adverse events (SAE) (MXF n=1/251 [0.4%], placebo1/123 [0.8%]). No new safety signals were seen. Conclusions:Whilst MXF 5-day therapy for ABS was not statistically superior to placebo at the primaryendpoint, subjects who received MXF had significantly greater improvementsin health outcomes and used fewer concomitant medicines than subjects treatedwith placebo, while experiencing no increase in AE or SAE.