58


ACS Management NSTEMI
Pro DTI “Hook-ster Hoekstra”
Pro Factor Xa “Knockdown Diercks”

James W. “Hook-ster”
Hoekstra, MD

Bivalirudin Use in the ED for NSTEMI:
Maximizing Our Choices to Maximize Our
Patients’ Benefit
James Hoekstra, MDProfessor and ChairmanDepartment of Emergency MedicineWake Forest University

80%
Diagnosis
Diagnosticcatheterization
60%
10%
20% 30%
PCI
CABG
Medicalmanagement
High risk
Low risk
CRUSADE Database.
Average time to catheterization = 21 hours
Current Management of NSTEMI ACS in the United States: Cath Happy!!
ACS, acute coronary syndrome; CABG, coronary artery bypass graft.ACS, acute coronary syndrome; CABG, coronary artery bypass graft.
Invasive Strategy Clinical Criteria (Class IA)– Recurrent chest pain– Elevated troponin level– ST depression– Signs of congestive heart failure– Sustained ventricular tachycardia– Hemodynamic instability– PCI in last month– High-risk noninvasive testing results– Prior CABG– TIMI >3– LVEF <40%– Diabetes
2007 ACC/AHA NSTE ACS Guidelines, available at acc.org.

EM Relevance: Medical Managementin the Pre-PCI Period
Concern Is Recurrent MI/Ischemia
ED PresentationED Presentation Catheterization Catheterization
D/CD/C
PCIPCI
Pre-PCI Period Pre-PCI Period Post-PCI PeriodPost-PCI Period
Cardiologists are vulnerable in the PCI and post-PCI period, where bleeding isa major concern
The Challenge: Balancing Efficacy and Safety
• Old guidelines (2002) emphasize reduction of ischemic risk in NSTE ACS—especially for upstream therapy initiated in the ED
• New guidelines (2007) include data on the harm that bleeding events cause, diminishing ischemic efficacy in some patients, and provide many more options for care upstream
• Emergency physicians are comfortable with the goal of reducing ischemic risk . . . and traditionally have left concern over bleeding to “downstream providers”; this paradigm is changing

IIaS
C
Direct antithrombin
LMWH
ATXa AT
Xa
Pentasaccharide
Bivalirudin and Fondaparinux
= saccharide unit.
Konkle BA, Schafer AI. In: Zipes DP, Libby P, Bonow RO, Braunwald E, eds.Braunwald’s Heart Disease. 7th ed. Volume 2. Philadelphia: Elsevier Saunders; 2005:2067–2092.
ATIIaIIa
UFH
LMWH, low-molecular-weight heparin.LMWH, low-molecular-weight heparin.

Moderate-high risk
ACS
Study Design: First Randomization• Moderate-high risk unstable angina or NSTEMI undergoing an
invasive strategy (N = 13,819)
An
gio
gra
ph
y w
ith
in 7
2 h
ou
rs
Aspirin in allAspirin in allClopidogrelClopidogrel
dosing and timingdosing and timingper local practiceper local practice
UFH orEnoxaparin+ GP IIb/IIIa
Bivalirudin+ GP IIb/IIIa
BivalirudinAlone
R*
*Stratified by preangiography thienopyridine use or administration.
ACUITY Design. Stone GW, et al. Am Heart J. 2004;148:764–775.
Medicalmanagement
PCI
CABG

Primary End Point Measures(Intent to Treat)
• Heparin* + IIb/IIIa vs Bivalirudin + IIb/IIIa vs Bivalirudin Alone
7.3%5.7%
11.7%
7.7%
11.8%
5.3%
3.0%
10.1%
7.8%
Net clinical outcome Composite ischemia Major bleeding (non-CABG)
30 d
ay e
ven
ts (
%)
Heparin+IIb/IIIa (N=4603) Bivalirudin+IIb/IIIa (N=4604) Bivalirudin alone (N=4612)
PNI <0.001PSup = 0.015
PNI = 0.011 PSup = 0.32
PNI <0.001PSup <0.001
*Heparin=unfractionated or enoxaparin. Stone GW, McLaurin BT. N Engl J Med. 2006;355:2203–2216.

0 1 2
ACUITY: Primary End Point Measures (Intent to Treat)
Bivalirudin Alone BetterBivalirudin Alone Better UFH/Enox + IIb/IIIa BetterUFH/Enox + IIb/IIIa Better
Risk Ratio±95% CI
Risk Ratio±95% CI
PrimaryEnd Point
Bivalalone
UFH/Enox+ IIb/IIIa
RR (95% CI)
Net clinical outcome
Ischemic composite
Major bleeding
Upp
er b
oun
dary
non
-infe
riorit
y11.7%10.1% 0.86 (0.77-0.97)
<0.0010.015
7.3%7.8% 1.08 (0.93-1.24)0.020.32
5.7%3.0% 0.53 (0.43-0.65)<0.001<0.001
P Value(noninferior)
(superior)
UFH/Enoxaparin + GPI vs Bivalirudin Alone
Stone GW, McLaurin BT. N Engl J Med. 2006;355:2203–2216.

0 1 2
UFH/Enoxaparin + IIb/IIIa vs Bivalirudin Alone
Yes (n = 3,197)No (n = 6,008)
Low (0–2) (n = 1,291)Intermed (3–4) (n = 4,407)
High (5–7) (n = 2,449)
Elevated (n = 5,368)Normal (n = 3,841)
Risk Ratio±95% CI
Risk Ratio±95% CI
BivalAlone
UFH/Enox+ IIb/IIIa
9.2%11.3%
12.2%11.1%
P Pint
0.76 (0.65–0.89)1.02 (0.86–1.21)
12.2%7.1%
13.3%9.4%
0.92 (0.80–1.06)0.75 (0.61–0.93)
0.230.01
<0.0010.83
0.35
0.02
0.18
13.0%8.6%
13.7%10.6%
0.96 (0.80–1.14)0.81 (0.69–0.95)
0.610.01 0.42
Biomarkers (CK/Trop)
ST deviation
TIMI risk score
Prethienopyridine
6.4% 10.2% 0.63 (0.43–0.91) 0.019.4% 10.2% 0.92 (0.77–1.10) 0.34
13.9% 15.2% 0.92 (0.76–1.11) 0.36
Yes (n = 5,192)No (n = 4,023)
RR (95% CI)
Bivalirudin Alone BetterBivalirudin Alone Better UFH/Enox + IIb/IIIa BetterUFH/Enox + IIb/IIIa Better
Stone GW, McLaurin BT. N Engl J Med. 2006;355:2203–2216.
ACUITY: Net Clinical Outcome Composite

Enoxaparin or UFH with antiplatelet agents
Fondaparinux or bivalirudin with antiplatelet agents
Invasive Therapy:Initial Antithrombin Therapies
II IIaIIa IIbIIb IIIIII
.

Upstream Hospital Care: Invasive RxAntiplatelet Therapy
A Platelet GP IIb/IIIa inhibitor in addition to ASA and heparin upstream for patients in whom PCI is planned
OR Clopidogrel 300 mg load and 75 mg/day upstream for a month up to a year
Bivalirudin instead of GPI/antithrombin upstream only if clopidogrel is used as well >6 hours prior to PCI
A Platelet GP IIb/IIIa inhibitor in addition to ASA and heparin upstream for patients in whom PCI is planned
OR Clopidogrel 300 mg load and 75 mg/day upstream for a month up to a year
Bivalirudin instead of GPI/antithrombin upstream only if clopidogrel is used as well >6 hours prior to PCI
II IIaIIa IIbIIb IIIIII

Bleeding Among Patients with ACSConclusions
• Antithrombotic therapies are cornerstone Rx– Must balance thrombosis and hemostasis
• Certain patient and PCI procedure characteristics predict bleeding– Age, female gender, chronic kidney disease,
procedure time, sheath dwell time
• Bivalirudin is a GREAT option in these patients

Deborah B. “Knockdown” Diercks, MD

XaBetter Living Through Chemistry
Deborah Diercks, MD
Associate Professor
Department of Emergency Medicine
University of California, Davis Medical Center

My Position
• Agents providing Xa inhibition are more desirable than UFH or direct thrombin inhibition– Xa inhibition is provided
• In balance with IIa (thrombin) inhibition– LMWH (enoxaparin)
• In isolation– Fondaparinux

My Position
• Part I: Enoxaparin and fondaparinux are superior to UFH
• Part II: ACUITY results do not support the superiority of bivalirudin
Part I
Enoxaparin and Fondaparinux Are Superior to UFH

The Enemy and Our Weapons
• Weapons to stop the cascade:– Heparin– LMWH– Special forces
• Xa inhibitors• Direct thrombin
inhibitors
Cascade activation (intrinsic or extrinsic pathway)
Factor X Factor Xa
Prothrombin(factor II)
Thrombin(factor IIa)
Fibrinogen Fibrin
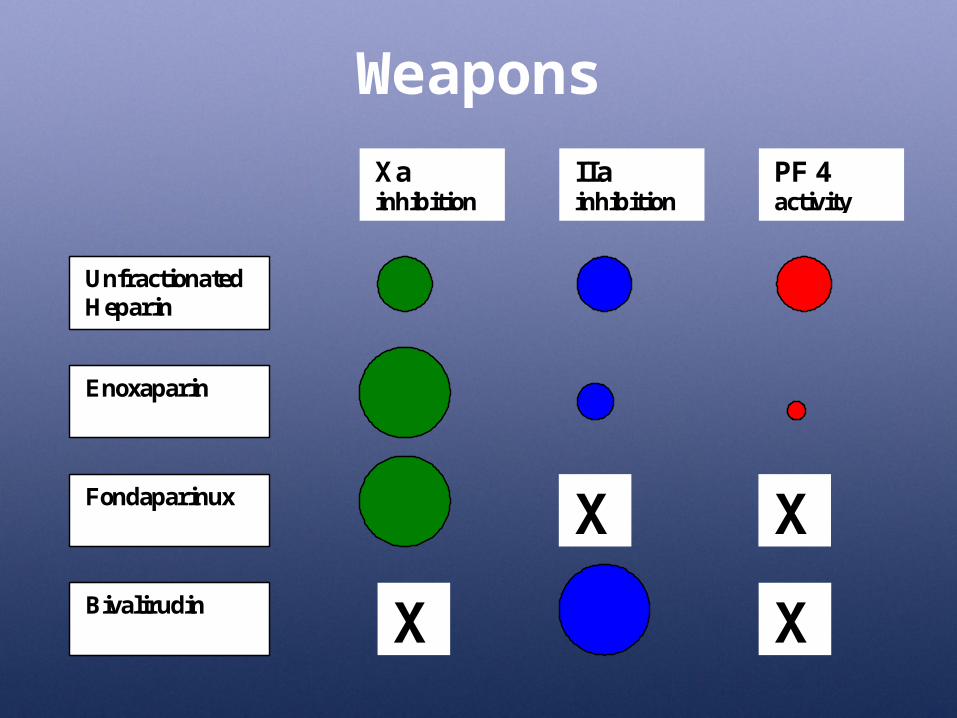
Weapons
Unfractionated Heparin
Enoxaparin
Fondaparinux
Bivalirudin
Xa inhibition
IIa inhibition
PF 4 activity
X X
X X

LMWH: Cleaner
• Dalteparin and enoxaparin– Animal derived– Smaller chains
more selective activity– Anti Xa >> anti IIa– Less PF4 binding
• Less HIT II

At least 2 of 3 required: Age 60 years ST (transient) or (+) CK-MB or troponin
IV Heparin
Primary end point: death or MI at 30 days
High-RiskACS Patients
Randomize(N = 10,027)
Early invasive strategyOther therapy per ACC/AHA guidelines
(ASA, -blocker, ACE-I, clopidogrel, GP IIb/IIIa)
60 U/kg 12 U/kg/hr (aPTT 50–70 seconds)
1 mg/kg SC every 12 hours
SYNERGY: Study Design
Mahaffey KW, et al, for the SYNERGY Investigators. JAMA. 2004;292:45–54.
Enoxaparin
aPTT, activated partial thromboplastin time.

SYNERGY: Primary End Point
0 5 10 15 20 25 300.8
0.85
0.9
0.95
1.0
Free
dom
from
Dea
th /
MI
Days from Randomization
UFHEnoxaparin
HR 0.96 (0.87-1.06)
30-Day Death/MI30-Day Death/MI
0.80.8 11 1.21.2
Hazard Ratio (95% CI)
EnoxaparinBetter
UFHBetter
Mahaffey KW, et al, for the SYNERGY Investigators. JAMA. 2004;292:45–54.

Death or MI to 30 Days C
umul
ativ
e %
of P
atie
nts
Days from Randomization0 5 10 15 20 25 30
UFH
Enoxaparin
HR = 0.8295% CI: 0.72, 0.94
15.9
13.3P = 0.004RRR = 16.4
20
15
10
5
0
J Am Coll Cardiol. 2006;48:1346–1354.
SYNERGY: Consistent Therapy
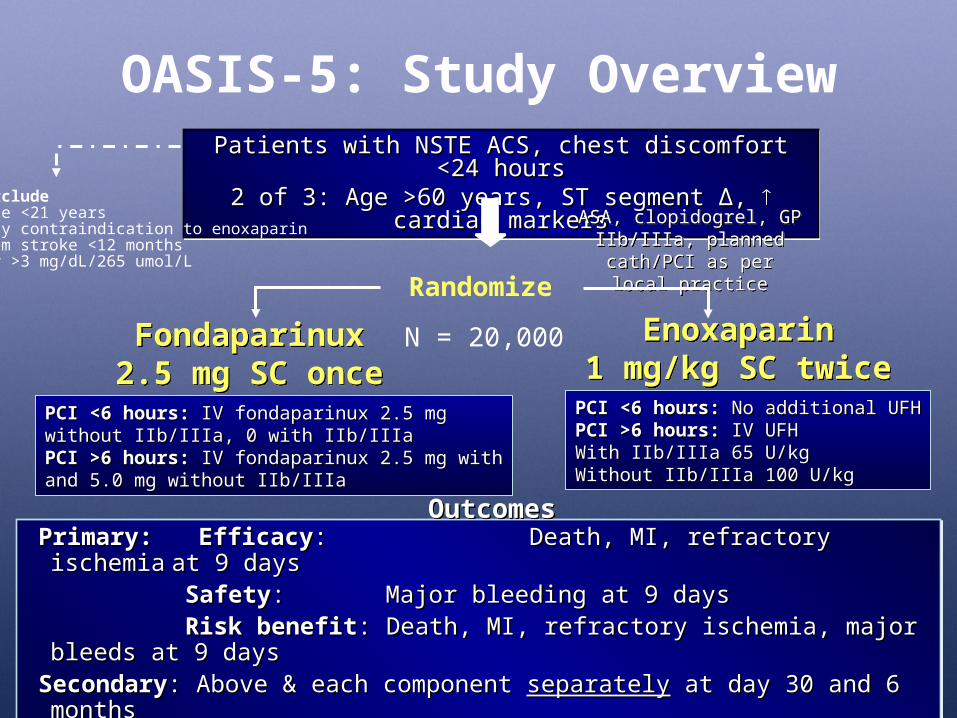
Patients with NSTE ACS, chest discomfort <24 hoursPatients with NSTE ACS, chest discomfort <24 hours2 of 3: Age >60 years, ST segment 2 of 3: Age >60 years, ST segment ΔΔ, , cardiac markers cardiac markers
Patients with NSTE ACS, chest discomfort <24 hoursPatients with NSTE ACS, chest discomfort <24 hours2 of 3: Age >60 years, ST segment 2 of 3: Age >60 years, ST segment ΔΔ, , cardiac markers cardiac markers
Fondaparinux2.5 mg SC once daily
Fondaparinux2.5 mg SC once daily
OASIS-5: Study Overview
ASA, clopidogrel, GP IIb/IIIa, planned cath/PCI
as per local practice
ASA, clopidogrel, GP IIb/IIIa, planned cath/PCI
as per local practice
Randomize
Enoxaparin1 mg/kg SC twice daily
Enoxaparin1 mg/kg SC twice daily
Primary: Primary: EfficacyEfficacy: : Death, MI, refractory ischemiaDeath, MI, refractory ischemia at 9 days at 9 days
SafetySafety: : Major bleeding at 9 daysMajor bleeding at 9 daysRisk benefitRisk benefit: Death, MI, refractory ischemia, major bleeds at 9 days: Death, MI, refractory ischemia, major bleeds at 9 days
SecondarySecondary: Above & each component : Above & each component separatelyseparately at day 30 and 6 months at day 30 and 6 monthsHypothesisHypothesis: First test noninferiority, then test superiority: First test noninferiority, then test superiority
Primary: Primary: EfficacyEfficacy: : Death, MI, refractory ischemiaDeath, MI, refractory ischemia at 9 days at 9 days
SafetySafety: : Major bleeding at 9 daysMajor bleeding at 9 daysRisk benefitRisk benefit: Death, MI, refractory ischemia, major bleeds at 9 days: Death, MI, refractory ischemia, major bleeds at 9 days
SecondarySecondary: Above & each component : Above & each component separatelyseparately at day 30 and 6 months at day 30 and 6 monthsHypothesisHypothesis: First test noninferiority, then test superiority: First test noninferiority, then test superiority
OutcomesOutcomes
PCI <6 hours:PCI <6 hours: No additional UFH No additional UFHPCI >6 hours:PCI >6 hours: IV UFH IV UFHWith IIb/IIIa 65 U/kgWith IIb/IIIa 65 U/kgWithout IIb/IIIa 100 U/kgWithout IIb/IIIa 100 U/kg
PCI <6 hours:PCI <6 hours: IV fondaparinux 2.5 mg IV fondaparinux 2.5 mgwithout IIb/IIIa, 0 with IIb/IIIawithout IIb/IIIa, 0 with IIb/IIIaPCI >6 hours:PCI >6 hours: IV fondaparinux 2.5 mg with IV fondaparinux 2.5 mg withand 5.0 mg without IIb/IIIa and 5.0 mg without IIb/IIIa
ExcludeAge <21 yearsAny contraindication to enoxaparinHem stroke <12 monthsCr >3 mg/dL/265 umol/L
N = 20,000

OASIS-5: Efficacy Outcomes at Day 9
Enox Fonda
Death/MI/RI 5.8% 5.9%
Death/MI 4.1% 4.1%
Death 1.9% 1.8%
MI 2.7% 2.7%
Refractory ischemia
1.9% 2.05%
0.8 1 1.2
NoninferiorityMargin = 1.185
Hazard RatioFondaparinux Better Enoxaparin Better

OASIS-5: Bleeding Rates at Day 9
Outcome Enox(%)
Fonda(%)
HR (95% CI) P value
No. randomized 10,021 10,057
Total bleed 7.0 3.2 0.44 (0.39-0.51) <<0.0001
Major bleed 4.0 2.1 0.53 (0.45-0.62) <<0.0001
TIMI major bleed 1.3 0.7 0.54 (0.41-0.73) <<0.0001
Minor bleed 3.1 1.1 0.35 (0.28-0.43) <<0.0001

OASIS-5: Mortality at 6 Months
Days
Cu
mu
lati
ve H
azar
d0.
00.
020.
040.
06
0 20 40 60 80 100 120 140 160 180
HR = 0.8995% CI: 0.79, 0.99
P = 0.037
Enoxaparin
Fondaparinux

Oasis-5
• Summary of Oasis-5– Fondaparinux has similar efficacy to enoxaparin– Fondaparinux (as used in this study) has less
bleeding than enoxaparin (as used in this study)– This lower bleeding rate translated into fewer
adverse outcomes at 6 months
• Critique– Enoxaparin was not used appropriately?

Part II
ACUITY Results Do Not Support the Superiority of Bivalirudin

Moderate-high risk
ACS
ACUITY Study Design• Moderate-high risk unstable angina or NSTEMI undergoing an invasive
strategy (N = 13,800)
An
gio
gra
ph
y w
ith
in 7
2 h
ou
rs
Aspirin in allClopidogrel
dosing and timingper local practice
UFH orenoxaparin+ GP IIb/IIIa
Bivalirudin+ GP IIb/IIIa
Bivalirudinalone
R*
*Stratified by preangiography thienopyridine use or administration.
ACUITY Design. Stone GW, et al. Am Heart J. 2004;148:764–775.
Medicalmanagement
PCI
CABG
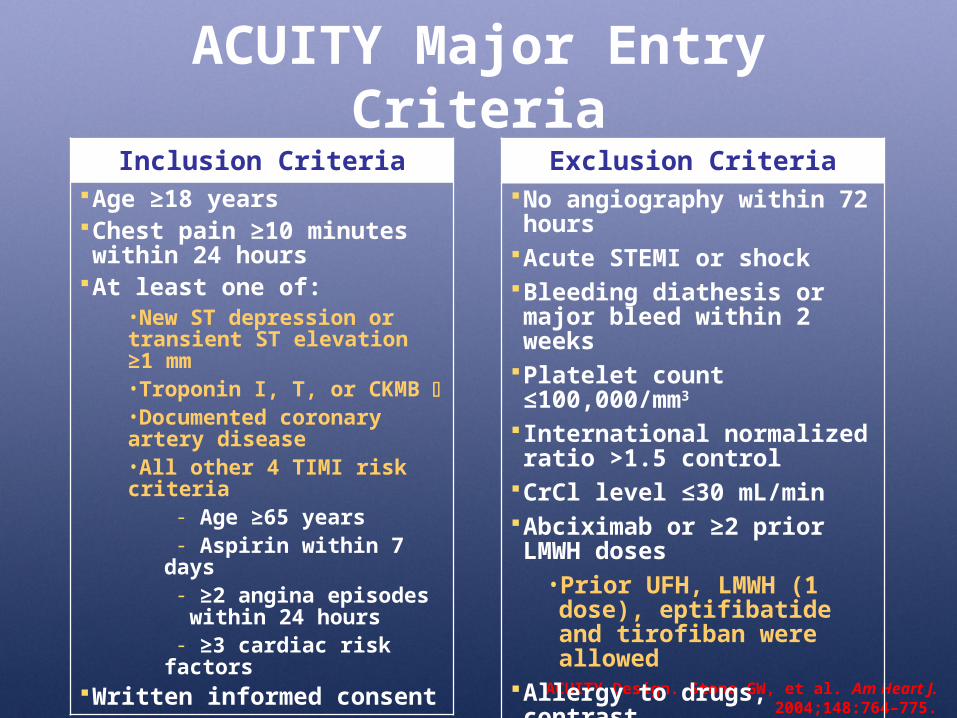
ACUITY Major Entry Criteria
ACUITY Design. Stone GW, et al. Am Heart J. 2004;148:764–775.
Inclusion CriteriaAge ≥18 yearsChest pain ≥10 minutes within 24 hours
At least one of:•New ST depression or transient ST elevation ≥1 mm•Troponin I, T, or CKMB •Documented coronary artery disease•All other 4 TIMI risk criteria
- Age ≥65 years- Aspirin within 7 days- ≥2 angina episodes
within 24 hours- ≥3 cardiac risk factors
Written informed consent
Exclusion CriteriaNo angiography within 72 hours
Acute STEMI or shockBleeding diathesis or major bleed within 2 weeks
Platelet count ≤100,000/mm3
International normalized ratio >1.5 control
CrCl level ≤30 mL/minAbciximab or ≥2 prior LMWH doses
• Prior UFH, LMWH (1 dose), eptifibatide and tirofiban were allowed
Allergy to drugs, contrast

Primary Results by Treatment Arm (30 Day)Heparin* + IIb/IIIa vs Bivalirudin + IIb/IIIa vs Bivalirudin Alone
7.3%5.7%
11.7%
7.7%
11.8%
5.3%
3.0%
10.1%
7.8%
Net clinical outcome Composite ischemia Major bleeding (non-CABG)
30 d
ay e
ven
ts (
%)
Heparin+IIb/IIIa (N=4603) Bivalirudin+IIb/IIIa (N=4604) Bivalirudin alone (N=4612)
PNI <0.001PSup = 0.015
PNI = 0.01 PSup = 0.32
PNI <0.001PSup <0.001
*Heparin=unfractionated or enoxaparin. Stone GW, et al. N Engl J Med. 2006;335:2203–2216.

Non–CABG-related bleeding
– Intracranial bleeding or intraocular bleeding– Retroperitoneal bleeding– Access site bleed requiring intervention/surgery– Hematoma ≥5 cm– Hemoglobin ≥3 g/dL with an overt source or ≥4 g/dL without overt source– Blood product transfusion– Reoperation for bleeding
1. Superiority was driven by decreased bleeding– Trend toward higher ischemic events– Hematoma does not equal death
7.3%5.7%
11.7%
7.7%
11.8%
5.3%
3.0%
10.1%
7.8%
Net clinical outcome Composite ischemia Major bleeding (non-CABG)
30 d
ay e
ven
ts (
%)
Heparin+IIb/IIIa (N=4603)
Bivalirudin+IIb/IIIa (N=4604)
Bivalirudin alone (N=4612)
*Heparin=unfractionated or enoxaparin. Stone GW, et al. N Engl J Med. 2006;335:2203–2216.

2. An unusual and unimportant bleeding scale was used– TIMI-major bleeding rates were low in all arms
TIMI-Major bleeding
0
2
4
6
8
ACUITY
Treatment arm
% o
f p
atie
nts
Bival
Bival + GP
H + GP

3. TIMI major bleeding rates in ACUITY are similar to those seen in all other trials– Superiority due to the “innovative” bleeding scale
0
0.5
1
1.5
2
2.5
3
SYNERGY OASIS-5 ACUITY
Enox
UFH
Fonda
Bival
Bival + GP
H + GP
Comparison of major bleeding rates by arm, by study

4. ACUITY does not reflect practice in the United States– Biomarker-negative patients were receiving
heparin + GPI
Newby KL, et al. Circulation. 2001;103:2891-2896.
TnT-NegativeTnT-Positive
PARAGON-B
PRISM
CAPTURE
Combined
0.125 1 20.5 0.125 1 20.5GP IIb/IIIa
BetterGP IIb/IIIa
WorseGP IIb/IIIa
BetterGP IIb/IIIa
Worse

5. Who is the enemy?
• Cost effectiveness of bivalirudin– GP IIb/IIIa
• Is this an issue for emergency physicians?– New guidelines suggest not every patient
needs one– Registry data says that not every patient is
getting one
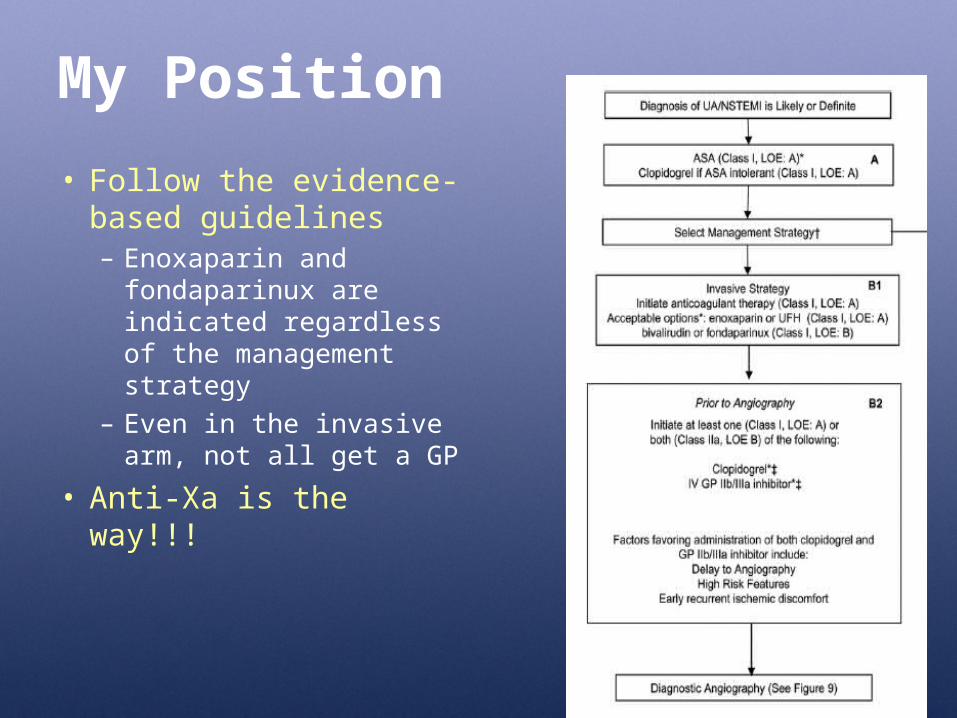
My Position
• Follow the evidence-based guidelines– Enoxaparin and
fondaparinux are indicated regardless of the management strategy
– Even in the invasive arm, not all get a GP
• Anti-Xa is the way!!!

BLEEDING IS IMPORTANT
ONE SIZE DOES NOT FIT ALL!!!
Pro DTI “Hook-ster Hoekstra”
Selection of Therapy in the ED Must Include Consideration of
Bleeding Risk
• Age
• Gender
• Renal insufficiency
• Baseline anemia
• Expectation of prolonged medical therapy

0 1 2 3
P valueRR (95% CI)Risk Ratio ± 95% CIRisk Ratio ± 95% CI
Results: The ACUITY Trial PCI PopulationPredictors of Major Bleeding
Age >75 years (vs 55–75)
Anemia
CrCl level <60 mL/min
Diabetes
Female gender
High risk (ST/biomarkers)
Hypertension
Prior PCI
Prior antithrombotic therapy
Heparin(s) + GPI (vs bivalirudin)
1.56 (1.19–2.04) 0.0009
1.89 (1.48–2.41) <0.0001
1.68 (1.29–2.18) <0.0001
1.30 (1.03–1.63) 0.0248
2.08 (1.68–2.57) <0.0001
1.42 (1.06–1.90) 0.0178
1.33 (1.03–1.70) 0.0287
1.47 (1.15–1.88) 0.0019
1.23 (0.98–1.55) 0.0768
2.08 (1.56–2.76) <0.0001

ACUITY: Impact of 30-Day Events on 1-Year Mortality
3.4
8.6
12.5
28.9
0
5
10
15
20
25
30
No MI ormajor bleed
MI only Major bleedonly
Both MI andmajor bleed
Events in first 30 days
1-ye
ar m
ort
alit
y (%
)
Stone GW, McLaurin BT. N Engl J Med. 2006;355:2203–2216.Stone et al. American College of Cardiology Annual Scientific Session; March 24–27, 2007; New Orleans, La.
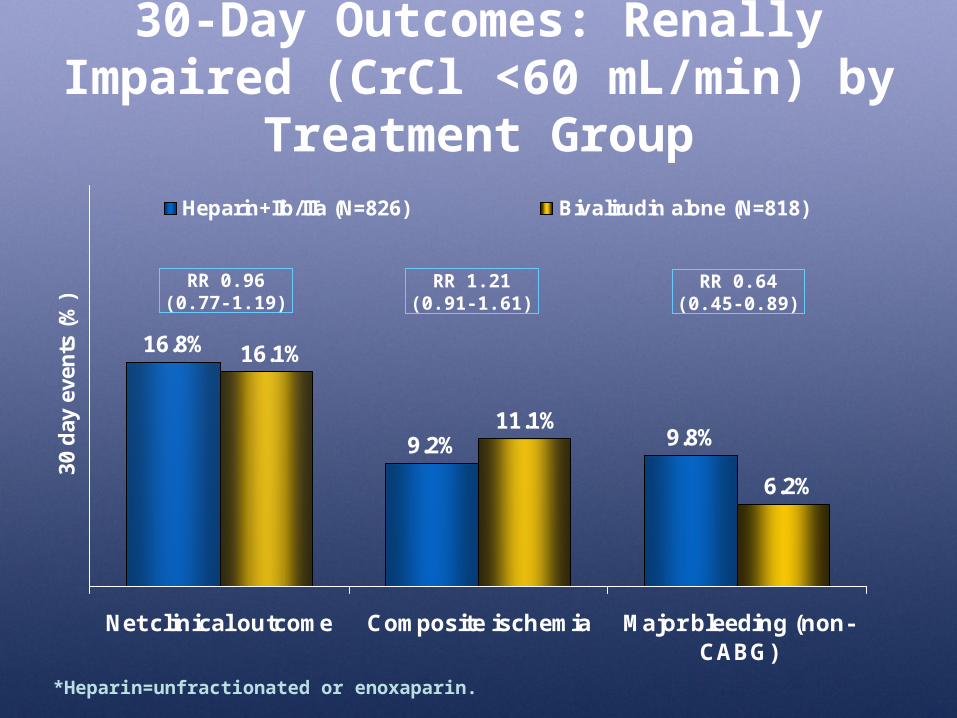
30-Day Outcomes: Renally Impaired (CrCl <60 mL/min) by Treatment Group
9.2% 9.8%
16.8%
11.1%
16.1%
6.2%
Net clinical outcome Composite ischemia Major bleeding (non-CABG)
30 d
ay e
ven
ts (
%)
Heparin+IIb/IIIa (N=826) Bivalirudin alone (N=818)
*Heparin=unfractionated or enoxaparin.
RR 0.64(0.45-0.89)
RR 1.21(0.91-1.61)
RR 0.96(0.77-1.19)

Bivalirudin 30-Day Outcomes in Diabetic Patients: ACUITY Substudy
15.2
9.58.5
4.6
12.1
8.3
0
5
10
15
20
Net clinical outcome Composite ischemia
Heparin(s) + GP IIb/IIIa (n=703) ANGIOMAX alone (n=721)
P = 0.08
P = 0.42P < 0.003
30-D
ay E
ven
ts (
%)
Major bleeding (non-CABG)
Data on file. The Medicines Company, Parsippany, NJ.

Seamless Transition to the Cath Lab: The Ideal Scenario???
Presentation
Early Treatment in the ED
Catheterization
D/C
PCI
Drug Administration

• Bivalirudin is a good antithrombin agent
• It should be used in the patient population that was studied– That is what evidence-based medicine
is all about
Pro Factor Xa “Knockdown Diercks”

Let’s Take a Closer Look

1. Patients were on study drug for a very short time
- Patients were on study drug a median of 3.9–4.1 hours prior to PCI
2. Majority of the patients were treated with a UFH or anti-Xa inhibitor prior to randomization
3. All patients were to undergo an invasive management strategy
Time
Arrival Randomization PCI
0 h 6.1 h 10.1 h
(Median times used for H + GPI arm) (Stone et al., Bival for patients with ACS. NEJM, 2006)

4. Broad inclusion criteria
Inclusion Criteria Age ≥18 years Chest pain ≥10 minutes within 24 hours At least one of:
• New ST depression or transient ST elevation ≥1 mm
• Troponin I, T, or CKMB • Documented coronary artery disease• All other 4 TIMI risk criteria
- Age ≥65 years- Aspirin within 7 days- ≥2 angina episodes within 24 hours- ≥3 cardiac risk factors
• High risk???• Does this reflect
current practice?• What is the
appropriate treatment for this group?

My Final Position
• In high-risk patients:– Enoxaparin or fondaparinux are recommended agents
in patients who will be managed with a conservative or invasive strategy
• In intermediate-risk patients or patients at higher risk for bleeding, who are rapidly going on to cardiac intervention (no long ED stay), who have been treated with an anti-Xa agent prior to initiating bivalirudin, it is a reasonable agent
Why You Should Use Enoxaparin
• Enoxaparin– Similar rates of bleeding to UFH
• Improved clinical outcomes
– Benefit persists regardless of whether invasive or conservative approach used
– Lower resource consumption– Proven
Why You Should Use Fondaparinux
• Fondaparinux– Less bleeding than enoxaparin and bivalirudin
(even in a higher-risk population)– Similar clinical outcomes (to enoxaparin)– Low cost– Ease of dosing

Why Would You Choose Bivalirudin?
• Uncertain performance in high-risk patients– What would ACUITY have looked like if it was
done in the same patient population as SYNERGY or OASIS-5?
• Requires continuous infusion
• $$$$$


















