46
Acute Small Bowel Obstrction BY PROF/ GOUDA ELLABBAN SCU HOSPITAL/ EGYPT
| Date post: | 11-Aug-2015 |
| Category: |
Health & Medicine |
| Upload: | scu-hospital |
| View: | 132 times |
| Download: | 0 times |

Acute Small Bowel Obstrction
BYPROF/ GOUDA ELLABBAN
SCU HOSPITAL/ EGYPT

Objectives :• Definition of acute small bowel obstruction• Surgical anatomy of small bowel• Pathophysiology & etiology• Initial management
Exclusion Criteria :• Sub-acute small intestinal obstruction• Acute on chronic small intestinal obstruction • Chronic obstruction of small bowel• Obstruction of large bowel
• An obstruction of the intestine is a blockage that completely stops or seriously impairs the passage of intestinal contents.
• AN OBSTRUCTION IS DEVIDED INTO
Obstruction
Mechanical Non-Mechanical

Definitions :• Ileus :• an absence of muscular contractions
of the intestine which normally move the food through the system; can result in an intestinal obstruction
Anatomy ! Applied -
1. Embryology
2. Gross Anatomy
3. Histology

embryology :• Foregut : esophagus ,stomach , pancrease ,
liver , duodenum , PAIN WILL BE LOCALIZED IN EPIGASTRIC AREA
• Midgut :small intestine distal to bile duct , cecum , appendix , ascending colon , transverse colon , PAIN WILL BE LOCALIZED IN UMBLICAL REGION
• • Hindgut : distal part of transverse colon ,
descending colon sigmoid colon , rectum , PAIN WILL BE LOCALIZED IN HYPOGASTRIC REGION

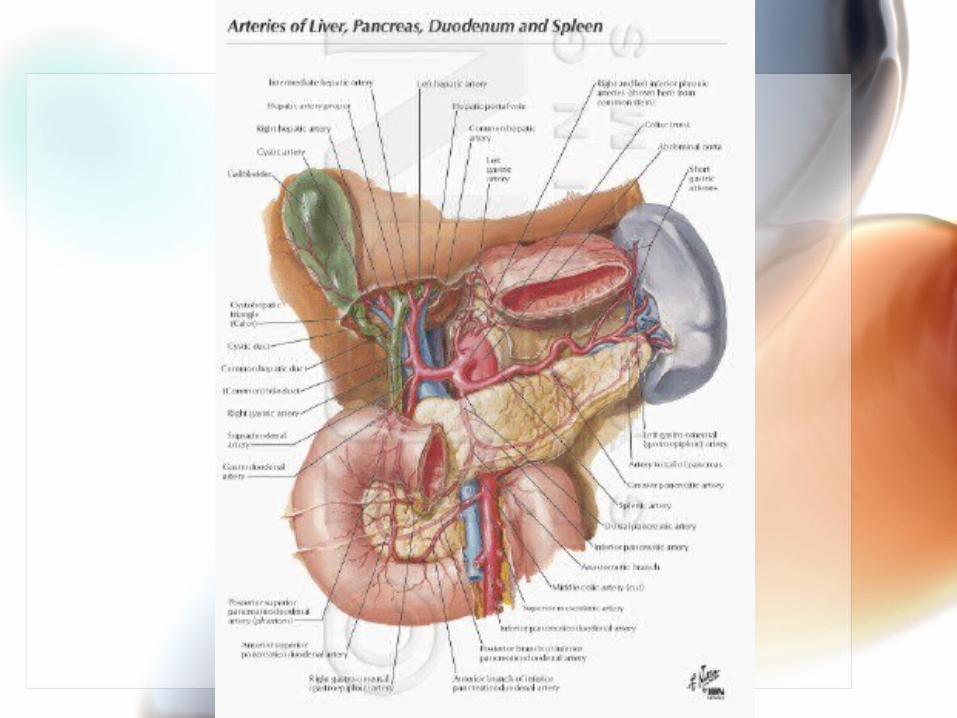
Vascular anatomy :• Duodenum
• Arterial : 1. celiac artery through superior
pancreatecodudenal artery abranch of gastroduodenal artery. ( it supplies duodenum proximal to entry of CBD)
2. Superior mesentric artery through inferior pancreatecoduodenal artery (it supplies duodenum distal to entry of CBD)
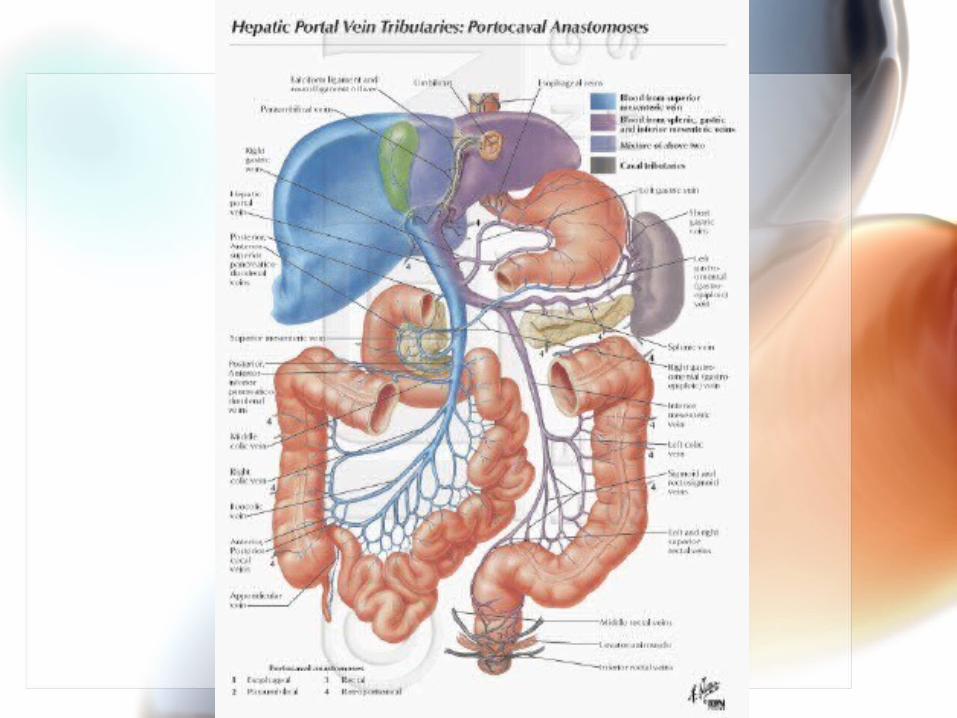
• Veinous :
follows the arteries and drain into Portal vein (through superior mesenteric & splenic veins)
WWW.SMSO.NET

WWW.SMSO.NET

• Lymphatics :
anterior lymphatic vessels pancreatecoduodenal LN pyloric LN
posterior lyphatic vessels superior mesenteric LN
efferent lymphatics will drain into celiac LN.

• Jejunum & ileum :– Arterial : superior mesenteric artery
sending 15 – 18 branches to both of themarteries unite to form loops and arches
called -arterial arcades- that give rise to straight arteries called -vasa recta- .– Venous : superior mesenteric veinwhich
ends posterior to the head of pancrese and joins the splenic vein to form the portal vein

WWW.SMSO.NET
WWW.SMSO.NET

– Lymph nodes :
Lacteals that absorb fat will secrete into the plexuses around the jejunum & ileum, then te lymphatic vessels will pass between the mesentery and drain into the following nodes :
• Close to the intestinal wall• Among the arterial arcades• Along the proximal part of the superior mesenteric
artery.
Efferent lyphatic vessels from the mesenteric LN will drain into superior mesenteric LN
Lymphatic vessels from the terminal ileum follow the ileal branch of the ileocolic artery to the ileocolic LN


Nerve Supply• Nerves supply of duodenum :
– Vagus nerve – Sympathetic nerves through theceliac and superior
mesenteric plexuses on the pancreatecoduodenal arteries
• Nerve Supply of jejunum & ileum :
Sympathetic supply T5 through T9 segments of the spinal cord Reach the celiac plexus by the sympathatic trunks & thoracic splanchnic nerves
Parasympathetic supply originally comes from posterior vagal trunk then synapse on cell bodies of postsynaptic sympathetic neurons in the celiac & superior mesenteric ganglia.

• NB :• The small intestine is insensitive to
most of the pain stimuli including cutting and burning, however, it is sensitive to distension which is perceived as colicky pains ( spasmodic pains ).

Histology :• Briefly about the layers

Etiology
Causes
Mechanical Non-Mechanical
Intraluminal
Intramural
Extramural
Displacement
1.
2.
3.
4.

Intraluminal causes are relatively unusual.
• Fecal (indigestible vegetable material impacted in the terminal ileum)
• Foreign body (the small bowel is already compromised by postoperative adhesions. )
• Worms ( Ascaris lumbricoides .)• Polyps• Gallstone ileus (occur with a cholecystenteric
fistula)• Bezoars are possible factors. • Inspissated meconium resulting in obstruction of
the distal ileum may be seen with cystic fibrosis in patients of any age.

intramural causes • T.B• Crohn’s disease• Tumors• Congenital• Strictures
• Neonatal atresias and strictures may be causes. • Thickening of the bowel wall with luminal compromise may be seen, as in patients with
Crohn disease. This thickening may occur with recurrent episodes of partial or incomplete obstruction.
• Small-bowel tuberculosis is not uncommon in certain parts of the world. • Strictures may occur following the ulceration induced by potassium tablets, nonsteroidal
anti-inflammatory agents, and therapeutic irradiation for bladder or cervical cancer. • An intramural hematoma may occur in trauma or in patients receiving higher doses of
anticoagulant agents than are necessary. • Lipomatas, leiomyomatas, and carcinoid tumors rarely result in obstruction, but these
have been reported in association with small-bowel lymphoma and the rare adenocarcinoma.
• Secondary tumors, notably gastric and colonic carcinomas, ovarian cancers, and malignant melanomas, may occasionally compromise the lumen of the small bowel.
• Any polypoid mucosal or submucosal lesion may form the head of an intussusception, which in turn can result in SBO.
• Intussusception in children younger than 2 years is a common abdominal emergency and usually idiopathic, although Meckel diverticulum, polyps, duplication cysts, and Henoch-Schönlein purpura have been implicated.
Extramural causes may be the most common.
• Bands• Adhesions• Abscess• Compression• Volvoulus
• Adhesions related to previous surgery or peritonitis are frequently implicated. Adhesive bands occur between loops of bowel and the wound and operative site. These adhesions can obstruct the small bowel by causing acute angulation and kinking, often many years after the initial procedure is performed.
• Congenital intraperitoneal bands may result in obstruction. • Congenital malrotation results in a short mesenteric attachment, and the entire midgut may undergo torsion or volvulus, which
leads not only to obstruction but also rapid progression to ischemia and death. • Hernias may cause SBO. A loop of small bowel may enter any form of hernia and become obstructed because of the narrow
neck of the hernia, which compromises the caliber of the bowel from without. – Most frequently, hernia-induced obstruction may occur as a complication of femoral, indirect inguinal, or umbilical hernias. Such
obstruction is a recognized complication of incisional and epigastric hernias and of the rare spigelian hernia. – Clearly, development of the obstruction is related to the width of the neck of the hernia, which to some degree reflects the nature of
the boundaries of the hernial defect. Obstructions resulting from a femoral hernia are particularly unwieldy. – Initially, the venous return of the bowel is compromised, leading to congestion and edema, which progresses to localized tissue
anoxia with frank ischemia; necrosis; and, in some patients, perforation. – The site of the obstruction is at the neck of the hernial sac, but any dead bowel is usually within the sac, which contains transudate;
this sac is often tender. – In large, multiloculated umbilical and incisional hernias, obstruction and its sequelae may arise in a single locus if the neck is
sufficiently tight. – A Richter hernia occurs when only part of the circumference of the small bowel is trapped at the hernial neck (usually femoral). This
type of hernia may not result in a complete obstruction and is easy to overlook, particularly in patients with obesity, until perforation has occurred.
– Obstruction occasionally results from incarceration of a loop of small bowel through congenital defects in the mesentery or omentum.
– Other so-called internal hernias may arise as a result of various degrees of malrotation occurring during fetal development. The most common are right and left paraduodenal hernias.
– Obstruction due to an internal hernia is clinically indistinguishable from obstruction due to postoperative adhesions.

Displacement• Internal hernia• External hernia• Intussusceptions

Non-mechanical Cause :• Peritonitis• Vascular occlusion• Drugs, electrolyte, toxemia• Truma• Post operative• Retroperitoneal causes.• Mega colon (dilatation and
lengthening of the colon)

ALL TUBES ARE THE SAME.

FUNCTIONAL RESERVE CAPACITY OF TUBES ?

70 %
Has To Be Obstructed !!
Symptoms :• Vomiting, colicky abdominal pain,
abdominal • distention, absolute constipation ( i.e.
neither• faeces nor flatus can pass ) .• Dehydration and loss of skin turgor .• Hypotension, tachycardia.• Abdominal distention and increased bowel
sounds .• Empty rectum on digital examination .• Tenderness, rebound or guardness
indicates• peritonitis .

Pathophysiology• An Obstruction Could Be :
– Simple– Closed Loop– Strangulated

Simple obstruction• Above the obstruction
Obstruction peristalsis is increased dilates reduction in peristaltic strength flaccidity and paralysis
(This is a protective phenomenon to prevent vascular damage secondary to increased intraluminal pressure.)
• Below- the obstruction.
the bowel exhibits normal peristalsis and absorption until it becomes empty when it contracts and becomes immobile.

Distention of the intestine is caused by the accumulation of
1. Gas.
2. fluid.

Gasdue to:1.swallowed air (atmospheric air).2.overgrowth of both aerobic and
anaerobic organisms.3.Diffused from blood into the bowel
lumen. When O2 & CO2 has been absorbed into the
blood stream, the resultant mixture is made up of nitrogen & hydrogen sulphide.

Fluid:results from: 1.ingested fluid.2.swallowed saliva. 3.gastric juice. 4.biliary and pancreatic secretions.There will be interference with normal sodium
and water transport. i.e., water & electrolytes excretion into the lumen & absorption depletion of water & electrolytes

Dehydration and electrolyte loss (especially potassium) are therefore due to:
reduced oral intake defective intestinal absorption vomiting sequestration in the bowel lumen.

• During the first 12 to 24 h:marked depression of sodium flux
from lumen to blood depression of water.
• After 24 h: there is movement of sodium and
water into the lumen further distention and fluid losses.
Closed loop obstructionSingle mechanism:• a hernial ring or • adhesive band,complete obstruction of the colon +
presence of a competent ileocecal valve (85% of individuals).
the blood supply is often obstructed at the same time.

StrangulationMay be due to:
1. external compression
2. rising intraluminal pressure
3. interruption of mesenteric flow
4. primary obstruction of intestinal circulation.

Mechanism of strangulation : Distention The venous return is compromised
increase in capillary pressure loss of intravascular fluid and red blood cells the arterial supply is impaired infarction the wall of the intestine becomes partly devitalized systemic exposure to aerobic and anaerobic organisms with their associated toxins accumulation of bacteria & their toxins in the obstructed part. So, it is believed, the relived the obstruction will cause movement of the bacteria & their toxic products into the part of bowel with good absorption function absorption of toxins which may cause death.
Interruption of the blood supply will lead to:
impairment of the intramural blood supply e.g., In the colon it will lead to gangrene of the cecal wall (usually anteriorly).

The systemic effects include:
1. elevation of the diaphragmi. restricted ventilation and ii. subsequent atelectasis.
2. Impaired Venous return i. sequestration of fluid into the edematous intestinal wall and peritoneal
cavity the intestine becomes severely congested blood begins to seep into the intestinal lumen.
ii. may lead to decrease C.O.
3. The loss of fluids and electrolytes:i. Increase blood viscosity.ii. Hypovolemiaiii. renal insufficiencyiv. shock, and death.
Shock may be accelerated by bacteria and their toxins in the strangulated obs.

Initial managment

• Picture 1. Small-bowel obstruction. Plain abdominal radiograph in a 6-year-old boy who presented with vomiting and acute pain in the right iliac fossa. The loops of the small bowel are dilated, and this is associated with small calcific nodules in the right iliac fossa. These findings are suggestive of appendicoliths. At laparotomy, an appendiceal mass was found; this caused the small-bowel obstruction.

• Picture 2. Small-bowel obstruction. Plain abdominal radiograph in a 9-year-old patient with a past history of appendicitis complicated by peritonitis who presented with abdominal pain and vomiting. The clinical diagnosis was small-bowel obstruction due to adhesions. Radiograph shows markedly distended loops of small bowel with effacement of the valvulae in the mid abdomen. The child recovered with conservative treatment.

• Picture 34. Small bowel obstruction. Nonenhanced CT scan at the level of the umbilicus in a 67-year-old man who presented with features of small bowel obstruction. Scan shows dilated loops of fluid-filled small bowel with a small amount of air (same patient as in Images 33-35). Note the collapsed right colon and beak-shaped transition of the small bowel (arrow).

















