Agenda Bay of Plenty Hospital Advisory Committee Venue: CEO Building, Cnr Cameron Road & 20 th Avenue, Tauranga Date and Time: Wednesday 2 July 2014 at 2:00pm Health Targets Shorter stays in emergency departments; Improved access to elective surgery; Shorter waits for cancer treatment/radiotherapy; Increased immunisation; Better help for smokers to quit; and More heart and diabetes checks Minister’s Expectations Better Public Services: Results for New Zealanders National Health Targets Care Closer to Home Shorter Waiting Times Health of Older People Regional and Clinical Integration Living within our means Board Priorities Health Targets Maori Health/Reducing Health Disparities Health of Older People Primary Health Wellness/Chronic Conditions Child and Youth Healthy, Thriving Communities
Transcript
Agenda
Bay of Plenty Hospital Advisory Committee
Venue: CEO Building, Cnr Cameron Road & 20th Avenue, Tauranga Date and Time: Wednesday 2 July 2014 at 2:00pm
Health Targets Shorter stays in emergency departments;
Improved access to elective surgery; Shorter waits for cancer treatment/radiotherapy;
Increased immunisation; Better help for smokers to quit; and
More heart and diabetes checks
Minister’s Expectations Better Public Services: Results for New Zealanders
National Health Targets Care Closer to Home
Shorter Waiting Times Health of Older People
Regional and Clinical Integration Living within our means
Board Priorities Health Targets
Maori Health/Reducing Health Disparities Health of Older People
Reports for Noting 6.1 Work Plan 6.2 Top Five Productivity Gains 2013-14
58
59
7
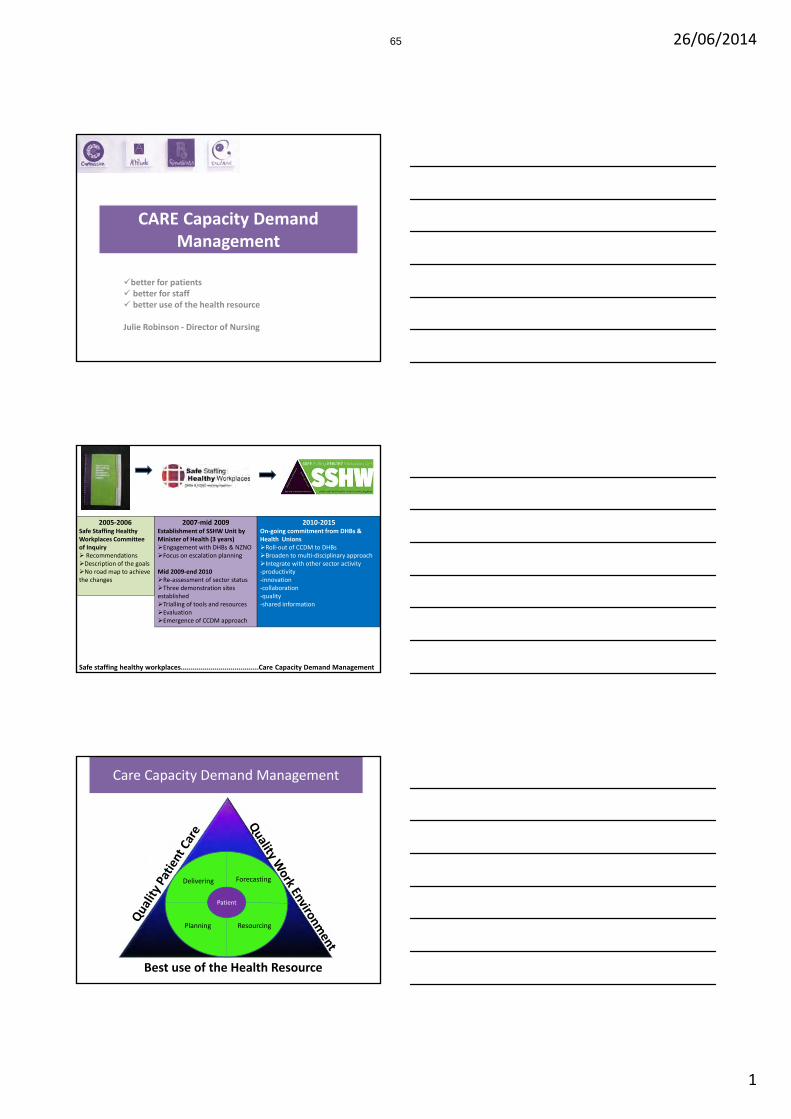
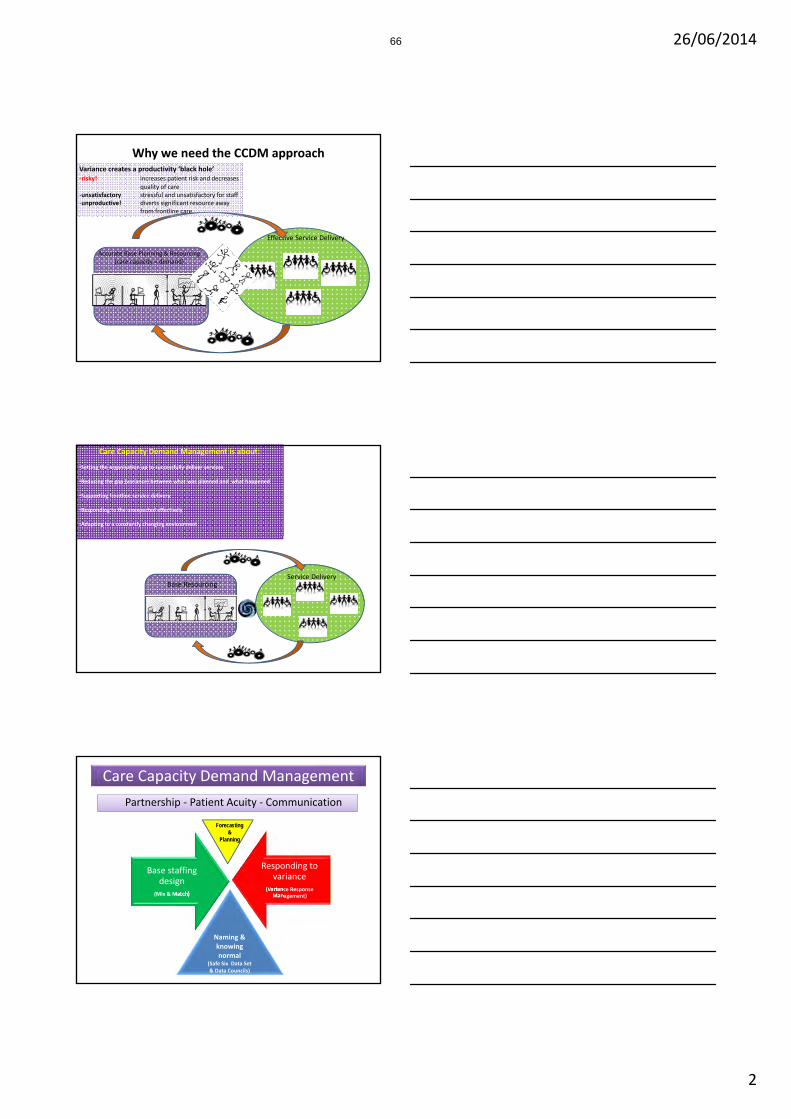
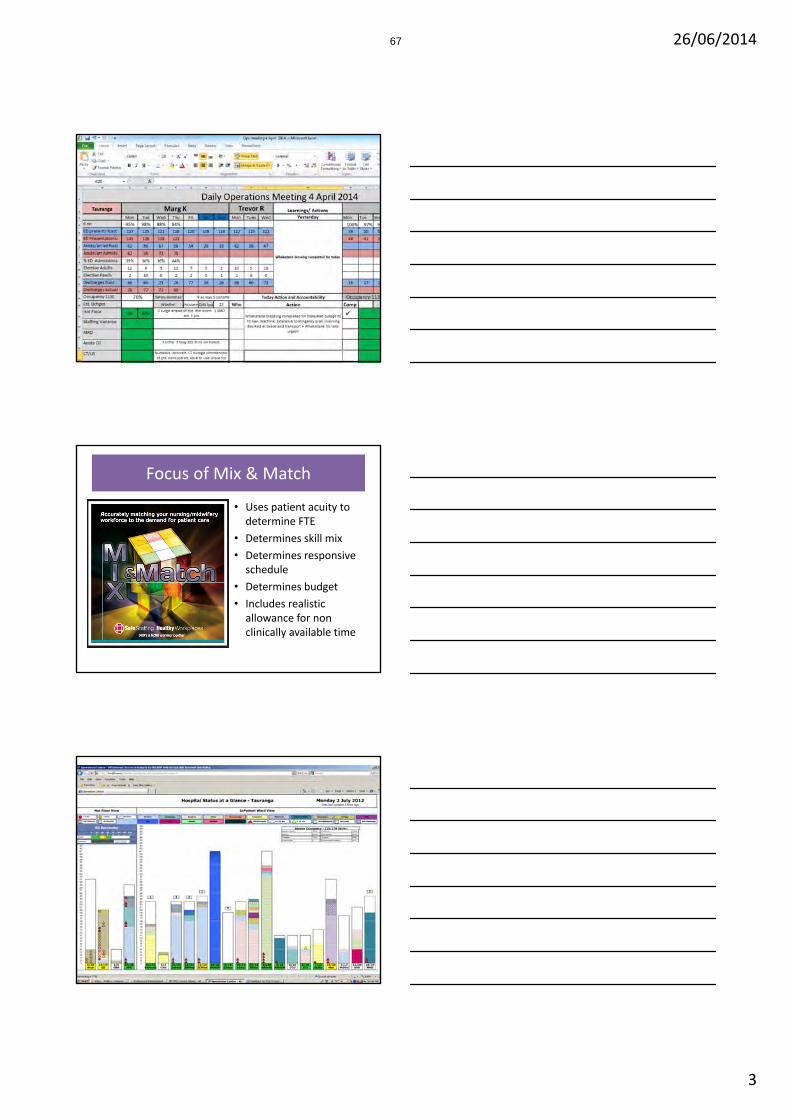
Presentations – Care Capacity Demand Management (CCDM) by Julie Robinson, Director of Nursing.
63
8
General Business
9
Resolution to Exclude the Public
10
Next Meeting – Wednesday 3 September 2014
Bay of Plenty District Health Board (open) Minutes
Minutes
Bay of Plenty Hospital Advisory Committee
Venue: Education Room 2, Education Centre, 889 Cameron Road Date and time: 23 April 2014 at 2:00pm
Committee: Mark Arundel (Chair), Sally Webb, David Stewart, Geoff Esterman, Jacob Te
Kurapa(left meeting at 3pm), Marion Guy Attendees: Janet McLean (Acting CEO), Gail Bingham (GM Governance & Quality), Helen Mason
(Chief Operating Officer), Julie Robinson (Director of Nursing).
Item No.
Item Action
1
Apologies
An apology was received from Stewart Ngatai Resolved that the apology from S Ngatai be received.
Moved: M Arundel Seconded: S Webb
2
Interests Register
The Committee were asked if there were any conflicts in relation to items on the agenda.
3
Minutes
Resolved that the minutes of the meeting held 26 February 2014 be confirmed as a true and correct record.
Moved: G Esterman Seconded: D Stewart
3
Bay of Plenty Hospital Advisory Committee (open) Minutes
Item No.
Item Action
4
Matters Arising
4.1 Matters Arising
There were no matters arising.
4.2 Committee Members Matters Arising
There were no matters arising.
5
Reports requiring decision
5.1 Chief Operating Officers Highlights Report The Committee discussed the report as circulated with the agenda.
Resolved that the Committee receive the report.
Moved: M Arundel
Seconded: M Guy
5.2
Chief Operating Officers Performance Report The Committee discussed the report as circulated with the agenda. Acutes remain an on-going challenge.
Resolved that the Committee receive the report.
Moved: D Stewart Seconded: M Guy
5.3 GM Property Services Monthly Report The Committee discussed the report as circulated with the agenda. Resolved that the Committee receive the report.
Moved: S Webb Seconded: D Stewart
4
Bay of Plenty Hospital Advisory Committee (open) Minutes
Item No.
Item Action
5.4
Draft Work Plan The Committee discussed the work plan as circulated with the agenda.
Resolved that the Committee endorse the work plan.
Moved: S Webb
Seconded: M Guy
6
Reports for Noting
6.1 Correspondence The Committee noted the information.
6.2 He Ritenga Audits The Committee noted the information.
7
Presentations
7.1 CIRCA by Suzanne Round (Change Manager) and Peter Bassett (Programme Manager), Service Improvement Unit, BOPDHB. Dr Sue Mackersey gave a presentation on the use of tele medicine in mental health and Dr Hugh Lees on the use of tele medicine.
8
General Business The Committee discussed communication with families once the HDC process has commenced. Communication with families has been added to the process.
GMGQ: Redact 6 complaints responses and place on the next agenda. Examples from DHB system, some SAC 1’s and general complaints.
9
Next Meeting – Wednesday 2 July 2014.
The meeting closed at 3:30pm. The minutes will be confirmed as a true and correct record at the next meeting.
5
Bay of Plenty Hospitals Advisory Committee
Matters Arising (open) – 2 July 2014
Meeting Date Item Action required Action Taken
23 April 14 8
GMGQ to redact 6 complaints responses and place on the next agenda. Examples from DHB system, some SAC 1’s and general complaints.
In Progress
6
COO Highlights Report May 2014 1
CHIEF OPERATING OFFICER’S HIGHLIGHT REPORT PROVIDER ARM May 2014
SUBMITTED TO: Bay of Plenty Hospital Advisory Committee
Submitted by: Helen Mason, Chief Operating Officer
RECOMMENDED RESOLUTION: That Committee receive the report.
7
COO Highlights Report May 2014 2
CHIEF OPERATING OFFICER Good News
• Acting CMA/MD has commenced in role. Well received by staff. • Recruitment for permanent appointment to CMA/MD role will well underway, with good
engagement from SMOs on process, JD, etc. • Performance on acute flow continues to improve compared to previous periods. May saw total
achievement on the 6 hour target at 93% compared to 89% for May 2013. Tauranga performance was at 90% compared to 84% last May. There was high occupancy in May, with a high level of acutes. It was pleasing to continue to deliver elective services, particularly endoscopy.
MEDICAL DIRECTOR Good News MEDICAL STAFFING UNIT
• There are no current RMO vacancies at either sites. • Run changeover occurs Monday 26 May (House Officers/SHOs) and 9 June for
Registrars. During this period there are 21 departing/arriving HOs & Registrars (19 TGA & 2 WHK).
• National recruitment started early May. Strong response for HO/SHO roles. Registrars a little slower. All internal RMOs have been send an “expression of interest” request to indicate whether they are remaining at the DHB and what runs they wish to be considered for. Work with the services commences mid-June to start the shortlisting/interviewing/appointing processes. High interest for PGY1 posts.
Credentialling SMO Credentialling Applications received and reviewed Number of Applications Reviewed
Tga Open Term
Tga Fixed Term/Locums
Whk Open Term Whk Fixed Term/Locums
Jan - Mar 14 3 15 - 2 April 14 1 5 1 2 May 14 2 9 - 2 2014 Ongoing Re-Credentialling Programme for Senior Medical Officers Sexual Health 13 February 2014 2 Tauranga Medical Officers Sexual Health credentialed 1 Whakatane Medical Officer Sexual Health credentialed General Surgery
8
COO Highlights Report May 2014 3
29 & 30 May 2014 8Tauranga SMOs to be credentialed 2 Whakatane SMOs to be credentialed 2 Whakatane Medical Officers to be credentialed Locum Credentialling Exit Reports The Credentialling Committee have created evaluation forms of Locums once their tenure has ended. A Locum Feedback Exit Report will be completed by either the appropriate HOD or person who has had the most contact with the Locum. In addition, a Locum Exit Report has been set up to gauge feedback from the Locum’s perspective. Information from completed reports will be valuable if future re-employment is sought. Medical Officer Admitting Rights The Medical Leaders Group discussed the issue of Medical Officer Admitting Rights at their meeting held 25 March 2014. Their recommendations were subsequently endorsed by the Clinical Governance Group on 15 April 2014. Their recommendations were as follows: 1. That the Clinical Governance Committee approves the principle that MOSS can be accredited by
the Credentialling Committee to have admitting rights at BOPDHB Hospitals. 2. That MOSS admitting rights will be considered on a case by case basis. 3. An application for a MOSS to have admitting rights will be submitted to the Credentialling
Committee by the service to which they belong. 4. The Credentialling Committee shall determine the permissions and limitations that are appropriate
for each individual MOSS for whom an application has been received. 5. Any permission and limitations granted will apply to the individual MOSS for whom the application
has been submitted and will not serve as a precedent for other applications. This will particularly apply to MOSS working in the Emergency Department at Whakatane Hospital who if credentialed, can admit patients overnight to the Whakatane ED Observation SOP. If the patient is not discharged the following morning, the patient’s care will be transferred to the appropriate specialty. DIRECTOR OF NURSING Good News International WHO Hand Hygiene Day May 5 each year is a day on which there is an international focus on the “5 Moments of Hand Hygiene. As part of the campaign to improve and sustain compliance with the “5 Moments”, the Hand Hygiene Monday tee shirts were launched. Based on the success of the immunisation tee shirts, the Hand Hygiene Steering Group decided Monday would be the day for all auditors, champions and other key leaders to wear their hand hygiene tee shirts. The tee shirts have a choice of two different messages: “Clean hands save lives, protect patients, protect yourself” or “Ten out of ten patients prefer CARE from clean hands”. The Health Quality and Safety Commission wish to use the photo from the launch of the tee shirts to assist with national promotion of the message. International Nurses Day Each year International Nurses Day is celebrated on 12 May, Florence Nightingale’s birthday. The International Council of Nurses promotes a theme each year: this year it was “Nurses: A Force for Change. A Vital Resource for Health.”
9
COO Highlights Report May 2014 4
A range of activities took place to celebrate the day. An invitation was extended to all those nurses who trained at Tauranga and those nurses who provided information for the Tauranga Hospital centenary book to attend an afternoon tea. The feedback from those who attended was they would like the afternoon tea as an annual event. Mental Health provided an educational forum for staff to attend and the medical floor had a cultural lunch. The different groups brought food from their country of origin. Whakatane elected to celebrate with cake as they were settling into their new facility. Midland Nursing Leadership Forum The Midland Directors of Nursing (DON) provide two forums a year to encourage up and coming nursing leaders. A recent forum was hosted by Lakes DHB with a focus on Integrated Health. Helen Parker from the UK who currently works with Midland Health Network presented her experiences from her operational, management and academic roles in the UK. The BOPDHB DON presented her reflections on the recent Health Master Class in which she participated. SURGICAL, ANAESTHETICS & RADIOLOGY SERVICES Good News Faster cancer Treatment Tender – Initiative to Improve Patient Journey BOPDHB has been advised that this tender was successful – details of the funding and service specification being worked through (approximately $220k over 12 months). EOI for Service Improvement for Elective General Surgery BOPDHB has been advised that this EOI has been shortlisted for support – details of the funding and service specification being worked through (potentially $150k over 12 months). Midland Region Trauma Service (MRTS) The abstract submitted by the BOPDHB Trauma Service to the upcoming Australasian Trauma conference in Sydney has been accepted for presentation. Radiology Service Improvement Programme BOPDHB has taken the opportunity to join the national initiative to improve patient access to radiology. The project plan to implement this local Radiology initiative “Patients First” was completed for submission to the Ministry this month. This programme of work will be supported by specific MOH funding of approximately $160k over 18months. Staff
• Recruitment is in progress for the Associate CNM for ICU/CCU • Faster Cancer Treatment (FCT) Project Manager, Dorothy McKeown has commenced this
month. • Specialty FCT nurse, Morna Delany has been appointed as the Whakatane FCT Specialty
Nurse to provide the link across all FCT tumour streams for Whakatane based patients. • Management of change for Whakatane theatre staff around changes to shift length has been
completed. The outcome being the introduction of a variety of shifts (8, 9 & 10 hours) that form the roster to ensure service requirements are met.
Risks and Mitigating Actions High Acute Volumes for Orthopaedics The volume of orthopaedic acutes continues to be greater than forecast and is impacting on electives. Additional elective sessions have occurred this month and more planned for June. Additional volumes has also been outsourced to Orthopaedic Services.
10
COO Highlights Report May 2014 5
MEDICINE Good News Whakatane Hospital Opening For all services provided at Whakatane the opening of the new hospital was an exciting time but at the same time it was high pressure also. The building was successfully occupied over the couple of days of the move with all staff involved taking on the challenges of moving whole departments, wards and patients in a very positive approach. Although there were as was to be expected a number of hiccups and a few facility defects, on the whole the move took place relatively pain free. Our services in the Medical Cluster would like to thank all those involved in the facilitation and operation of the building design and move. Shorter Waits in Emergency Departments The April 2014 result of 94% is consistent with the dramatically improved performance from the prior two months. Earlier performance had ranged from 89% in July 2013 to a previous high of 92% in November. This improvement has been achieved even with volumes significantly up on last year’s activity, with health target qualifying attendances up 12.1% on the same month last year, and 8.1% for the YTD. Whakatane ED continues to deliver above target (99%), with Tauranga performance at 92% significantly improved from baseline results (85% July 2013). Out of hours activity continues to be identified as an area of high impact. A trial has been put in place for a third House Officer at night in the ED. This decision was driven by patient safety, however clearly this has had a positive impact on the breach numbers through the night and early morning. In addition there continues to be a focus at the front door through the redeveloped model of medicine to handle acute general medical patients more effectively. Presently, there is a project to look at the hospital at night, which will appraise the availability of all resources and their responsiveness to demand surge. This project will look at the tasks required at night and how these may be spread more effectively across all the available resources. Surges in patient numbers and high acuity have been contributing factors with weekend demand also influencing the result. In response, a third medical registrar is now rostered on to the weekends to assist in managing demand. The monitoring and measurement of demand continues to improve, with ‘breach’ reporting in place to identify individual ‘breaches’ with the cause and effect for daily analysis. The model of medicine introduced in mid-July continues to be developed to increase the focus on the front door. The Heads of Departments are now meeting on a regular basis to support improvement on this measure. The Standard Operating Procedure (SOP) for Acute Demand is currently out for consultation with all departments, and close to being finalised. Tauranga Hospital remains focused on achieving the whole of system action plan outlined in previously. Staff Recruitment The Cancer Co-ordinator for Lung/Chest has been appointed and will start in June. This post has been vacant for a number of months and is a key role in facilitating the FCT performance for this tumour stream. The vacancy for an Endocrinologist/General Physician has been filled with the successful candidate coming in September – she is a New Zealand graduate. Cardiology/Clinical Physiology One of Clinical Physiologists who holds the DMU (sonography qualification) will be working 0.3FTE to assist Radiology from 16 June 2014 for six months due to recruitment shortages in this area.
11
COO Highlights Report May 2014 6
The Implantable Cardioverter Defibrillator (ICD) support group previously reported have held their first meeting on Saturday 10 May for patients and their families. A five-strong patient-led committee has now been formed to oversee the group who have said “it is very useful for them to have a support network to help with useful advice or sometimes just someone to talk to”. The number of Bay residents who have had an ICD fitted has grown steadily to around 100 in recent years. The meeting, which was sponsored by two company ICD representatives, featured speakers Dr Dean Boddington, Sheryl Tait and Tracey Cumming from the pacemaker team. 13 May saw the first Evera MRI compatible ICD device implanted here in New Zealand by Dr Dean Boddington at Tauranga Hospital. The device enables those patient,s who in the future require an MRI, to have this safely (previously an MRI could not be performed on these patients)
http://www.sunlive.co.nz/news/71941-city-hospital-implants-nzfirst.html Diabetes Teleconferencing links allowing connection between Opotiki Clinics and the Nurse Practitioner are now fully operational and tested. We are planning to commence a Nurse Practitioner (diabetes) telehealth clinic at Opotiki in June as a pilot study. Renal Transplant - Currently we have another patient being worked up for first New Zealand three way kidney transplants in the paired kidney exchange program. Hopefully will take place in August. Video conference- Jabber accounts have been set up both in Tauranga and Whakatane Dialysis Units. This has facilitated daily teleconference with Whakatane and Clinical Nurse Manager, providing clinical leadership, follow ups and guidance to RNs on duty. In addition links to Waikato allow blood reviews done via teleconference/ video conference. Waikato Relationship Development – Waikato Renal Consultant has presented at Grand Round in Whakatane in May; plans for Grand Round presentation here in Tauranga also under way Risks and Mitigating Actions Dermatology – our current Dermatology (0.4 FTE) has resigned and will finish in July. The Medicine Cluster is currently negotiating with the skin centre for short term clinic coverage, and a medium to long term solution for providing medical dermatology clinics. Haematology – due to the current vacancy for a Haematologist at BOPDHB, services are still being provided by Waikato. However there a candidate from the UK who will be visiting the unit in June. WOMAN CHILD & FAMILY Good News Maternity Both maternity units have had a busy month with peaks and troughs but the staffing has been managed according to the variance demand. The SCBUs have both been busy with a noticeable increase of twin births in Whakatane. Pepi Pod programme has been steady. The additional funding that has been received from Maori Health has allowed more pods to be purchased to ensure the continuation of the programme.The robust follow up that is part of the programme is ensuring that the babies are being kept safe and the message of safe sleeping is being delivered. Smokefree pregnancy: the two Pepi Pod coordinators are continuing to deliver the message around smokefree pregnancy and Midland Maternity Action Group is looking at purchasing some monitors that can measure and demonstrate to the mothers what is happening to their babies when they smoke. The Tauranga Pepi Pod coordinator has also been to further training as she will be
undertaking the education to the midwives for the Bay of Plenty and Lakes district for the NZ College of Midwives. These two midwives are also going to a two day conference for Maori Women’s Health in Huntly. The Maternity Quality and Safety Governance group is to have Maternal Mental Health representation added to the group and an invitation is to be sent to the new Primary Birthing Unit to have representation on the group once they are established. The draft copy of the Maternity Report has been reviewed and there is a request for some very minor changes to the final report due in June Midwife Leader is meeting with the management of the Bethlehem Birthing Unit to establish guidelines around the process of transfer into the Tauranga Maternity Unit. The new Technical Skills workbook put together by the Midwifery Educators in the Midland Region has been accepted and a request has been made from Midwifery Council whether this workbook could be used around New Zealand. This is a credit to the Midland Educators which our educator is a part of and also contributed to the workbook. The first set of new technical skills for the midwives is going to be held next week in Tauranga. Changes to the Neonatal Life Support training is to be rolled out nationally and the two main midwife instructors for the Bay of Plenty DHB are having to attend a workshop in the South Island. They will then bring back the information to the other instructors . BFHI certification has been completed and arrangements are now being made for the NZ Breast Feeding Authority to come down to the Bay of Plenty and present the three facilities, Opotiki, Whakatane and Tauranga with their certificates and thank the staff for their contribution. Paediatrics The User group in Whakatane has met with Property services to look at options for Paediatric outpatients and the SMO office space that will be required as the existing space will be in the demolition zone when the Santon Block is being removed. The option to utilise the old CT suite for the clinics was positively received and there is agreement to progress some detailed design work for this. The Countdown Hospital Appeal is getting ready to launch its new round of fundraising again. Wish list items are being requested currently with the reminder that the items must be of benefit to the Children and babies in the area and it is not to replace the items that the DHB should be purchasing but should be items that would be nice to have. The announcement that Whakatane will be one of the next areas required to establish a Child Action team focused on developing services for vulnerable Children has been well received by the service who are looking forward to engaging in the planning process. Risks and Mitigating Actions Unaccepted Laboratory Reports: This has been entered onto the Risk register. The Midwifery Leader has been working with IT and Pathlab to look at what the issues are around so many of the Lab reports being escalated to the Midwifery Leader. Following an intensive look into the process it has been found.
1. The LMC midwives were receiving paper copies so it was not necessary to go into éclair and check results.
2. If the LMC midwives needed an urgent result Pathlab was faxing these through to the midwives and then sending them a paper copy.
3. Some of the LMC midwives had up to five different numbers and the results were going to most of these different identification areas.
13
COO Highlights Report May 2014 8
4. Results from tests that were ordered by a doctor when the woman or the baby was an inpatient going into the LMCs results.
5. Results that are clearly a gynaecology test and not an obstetric one being sent to the LMC midwife instead of the Doctor.
6. Midwife and Doctor having the same surname so all the results were entered into the midwife’s results.
Following the discovery of the errors with the process further meetings have been held with IT and Pathlab and the following resolutions have been agreed:
• Midwives are to be notified that Pathlab are moving towards a paperless system. The plan is to activate this as 1st July 2014 following notification to all the midwives.
• Midwives have already been given remote access to the éclair system and it is their responsibility to ensure they are utilising the systems.
• Midwives have already been given an opportunity to complete the necessary training around the use of the remote access and had this programme added to their laptops.
• Midwives must let IT know if they have issues with access. • Midwife Leader to continue to monitor the report that she is now receiving on a weekly basis. • IT dept is ensuring that the midwives do not have more than one number/area for the results
to go into. • Staff ordering tests for women/babies as inpatients must ensure that they use the doctors
name on the request form that have ordered the tests • Pathlab are to monitor their data entry and not create a new number for the result, and ensure
they are checking the requestor on the form. It is felt that with these measures in place it will reduce the risk to the organisation and that it is noted that it was not the LMC midwives that were the cause of this risk but the actual process that was created by not consulting with the midwifery workforce at the time of the change over for the laboratory results and that the LMC midwives were very cooperative while the processes were being reviewed and investigated. REGIONAL MAORI HEALTH Good News The third Noho marae for the Rural Health Inter-professional Immersion programme was held on Sunday the 4th at Tanatana marae, Waimana, a rural town approximately 30 kilometres out from Whakatane. It commenced with a traditional pohiri followed by a Whakawhanaungatanga or introductions by the local people and visitors. This gave an opportunity for the students to ask about the different cultural perspectives and experiences given by the local people. Smoking cessation was also part of the discussions throughout the weekend. The Regional Māori Health team attended the Staff Service Recognition held at the Tauranga Yacht club on Wednesday 7th. Phillip Hikairo a local elder from Tauranga Moana commenced the evening with an opening karakia. A powhiri was held on Monday 12th in support to the International Nurses Day for the Mental Health forum. This was also followed by a whanau centred care presentation done by the Regional Director. The Treaty of Waitangi training was held on the 13th at the Education Centre in Tauranga. Through further discussions there will also be another training offered to all Whakatane and Tauranga staff on Thursday 18th and Friday 19th September held at the Clinical School in Whakatane. All staff are encouraged to attend. The Cultural Awareness training was held on the 16th May here at Regional Māori Health Services Whakatane with facilitator Pouroto Ngaropo. This gave a great opportunity for twelve attendees to visit the local sacred sites around Whakatane including Te Ana o Muriwai, Pohaturoa rock, Te Manuka Tutahi marae.
14
COO Highlights Report May 2014 9
REGIONAL COMMUNITY SERVICES Good News Stories Support Net Paid family care: The BOPDHB has implemented a policy to enable some family members to be paid as carers. There has been rapid policy development concerning this and is in place from 22 May 2014. Mental Health: Twice yearly meetings between Support Net staff and Mental Health staff are being arranged to improve understanding of roles, responsibilities, possible funding pathways and relationships. District Nursing International Nurses Day: staff enjoyed the cake supplied by the DHB and the soups from Watties. Allied Health Speech and Language Therapy (SLT) have been using two volunteers which has made a huge difference to the service and we hope to employ one as a volunteer. Great feedback received from the SLT Patient satisfaction audit. The team hosted the first regional SLT tele-health Team Leader meeting, with the attendance of six Team Leaders from across the Midlands DHBs, looking at a collaborative practice and regional standardisation of resources. Appointments of Natasha Grieg-Merritt to Acting Team Leader for Social Work (Tga) and Mark Gray to Acting Team Leader for Occupational Therapy (Tga), both positions are fixed term for 6 months. All Enable applications will now be online including housing alterations. Health Careers Expo held in Tauranga recently was well attended with high interest as compared to previous years, good feedback received from staff involved in Expo An organisational-wide farewell was held for Meg Hills, Social Worker Adult Rehab, who retired after 22 years of service to Whakatane Hospital . Risks and Mitigating Actions Support Net Staff Wellness There have been some significant amounts of sick leave taken in the last month for various reasons. With these absences the pressure on other staff increases and we continue to need to prioritise work for allocation, extend some waiting times for non-urgent work and increase the use of contracted workers. We have approached the pool of casual Social Workers in an attempt to get extra resource but there has been no interest from anyone in that group. Paid Family Care As noted above, the BOPDHB, as with other DHB’s, now has in place a paid family care policy. This risk is likely to include increased referrals for NASC assessment and /or coordination and consideration of family members for paid family care. There may be some cost increase as
15
COO Highlights Report May 2014 10
previously unfunded care becomes paid support by a family member. There may also be implications as current family members providing paid care who are no longer eligible under this policy, are transitioned to other arrangements. We are working to develop information and training for staff as it is unknown what the interest and uptake of this opportunity will be. District Nursing Tauranga currently have a waiting list off and on for the HITH patients due mostly to not being able to manage at the weekends. Extra staff are being rostered at the weekends to cope with extra workloads. Opotiki have never had budgeted FTE for weekends and we are continually having to roster staff to cover weekends. There is also someone rostered during the week to prevent the staff from doing overtime as there has been an increase in workloads for Opotiki. It appears that a GP practice is no longer doing ACC and is referring all wound care to the Opotiki DNs. The Practice Nurse clinics are full and they are unable to fit patients in so they refer to DN service. Whakatane workloads have increased and we are frequently rostering extra hours at the weekend in order to cope Allied Health Child Development Service, Whakatane has been unsuccessful in appointing a Physiotherapist. We currently have locums covering the service 2 days per week. The position has been re-advertised and we are liaising with Tga Physiotherapy for help with cover until this position is filled. SLT cover for Child Health to be reviewed in light of the MoH requirements for those children with feeding issues. A BOP Local Area Agreement (LLA) for Tauranga has been agreed. Whakatane is working to clarify what is needed and will include this into the LLA. There will be an increase Child Health volume. Over spending on Palliative Care patients continue. Social Work Department Whakatane now have vacant positions within Child Development Service and Adult Rehabilitation. The vacancies are being covered internally and with some support from Tga. Weekend cover of Physiotherapy services is reliant on volunteers, this is unsustainable. We will be looking at how to standardise this with assistance from HR. Podiatry Service has no succession plan in place; we need to consider a one year contract for a new graduate to assist in providing cover for planned and unplanned leave. MENTAL HEALTH & ADDICTION SERVICES Good News MENTAL HEALTH SERVICES FOR OLDER PEOPLE Ethics approval for Palliative Care Project Ethics approval for the palliative care project was granted – we wish to thank Dr Fiona Miller for all her work in completing this application to successful stage. The project group has completed a planning meeting for the project and with the Stage 3 (Athenree Rest Home and Hospital) and the Psychogeriatric (Althorp) facilities who are participants in this project. Midlands Regional Dementia Behavioural Support and Advisory Service
• Attended a Regional Dementia Advisory Service Coordinators meeting – enabling peer support and also confirming consistencies between the Midland and North regions. South was
16
COO Highlights Report May 2014 11
not represented and Mid-Central has used the South’s model employing an educator for the “Walking in Another Shoes’ programme.
• Attended my first Age Concern Elder Abuse and Prevention group as an advisory member – allowing for greater networking and awareness opportunities for the role, as well as guiding decisions regarding elder abuse cases.
International Nurses Day 2014 Nurses from MHSOP and Consultation Liaison Service presented key service developments that nurses are leading and/or are key contributors. The feedback from nurses attending was extremely positive regarding how nurses and the service in general is continually researching and developing new ways of improving care for our client groups and education other health professionals. As teams we should feel extremely proud of our continued contribution to health care development and the recognition received by other services for this. The programme presented on the day had informative content and highlighted nursing developments in other DHBs that we can also learn from. ADULT COMMUNITY MENTAL HEALTH AND ADDICTION SERVICE NGO meetings - Paula Abbey, Team Leader in Whakatane, has been vising the local NGOs to go over the MOUs’ and also discuss with the managers and members of the team how well they are all working together plus any concerns that they may have. The feedback from Whakatohea was very positive indeed. The feedback to Paula was that the case managers make themselves available; they are in regular contact and visit the services in Opotiki on a regular basis. This was fed back to the team who were also complimentary about Whakatohea services. It is a positive working relationship which of course goes a long way to assist and support clients of the service. Duly Authorised Officer (DAO) Forum was held in Hamilton on Thursday the 15th May. Most of our DAOs attended this forum. The staff who had attended reported that this session was useful and insightful learnings took place. Aspects such as conceptualising risk, positive risk taking and also competence, consent and coercion were discussed and learnings from these discussions will be implemented in practice. Crisis Respite – Discussions between the Adult Community Mental Health Service (ACMH) and Richmond NZ has taken place to explore possibilities regarding how Richmond may be able to support ACMH with crisis respite. At this present time there is only access to planned respite which makes it difficult should we have a crisis and need crisis accommodation. Excellent progress has been made and it is anticipated that the implementation of outcomes will commence over the next month. Development of a pathway for High and Complex Needs Clients - A meeting took place between Team Leaders, Clinical Co-ordinator and Dr David Chaplow to discuss how we could improve our pathway for the referrals for High and Complex Needs clients. The focus of future meetings will be on-
• Establishing an improved pathway for all high and complex clients referred to the service in order to ensure that this is done in a coordinated manner
• To identify what information is required from the referring agency before acceptance into the service
• To develop a robust continuum of care for the High and Complex Needs client group This group will continue to meet until the above has been accomplished. Getting clients to be more active - Dean Kerr, Occupational Therapist at Adult Community Mental Health has been working hard to find ways to help our clients get more active and socially involved and basketball has proved extremely popular. It is a collaborative venture between Adult Community Mental Health and the NGO housing and recovery providers, Te Tomika, Madison Centre and Bay of
17
COO Highlights Report May 2014 12
Plenty Community Homes Trust. The group has been running for 6 weeks and membership is now up to 25 plus spectators. Aside from enjoyment of the sport and the physical health benefits a great aspect of this group is that everyone contributes, there is karakia, shared lunch and everyone has a role. Clients who have come along just to watch have eventually picked up a ball and started playing. For some this is the first social activity they have been able to participate in a long time so effort will be made to support them to continue. Staff Recognition Programme - Each year staff who have served 10 years or more and match recognition criteria are invited to attend a celebratory event with family and friends. Staff are presented with a certificate for 10 and 15 years milestones. Those who have attained 20 years or more also receive a gift. Several staff from ACMHAS were acknowledged for their service to the BOPDHB – with years of service ranging from 10 years to 42 years. ADULT INPATIENT UNIT • Annual staff satisfaction survey has been completed for both units • TrendCare will be moving toward implementing the VRM process as a next stage • Double shifts are reducing and a semi-permanent recruitment campaign in both sites has
commenced.
Te Whare Maiangiangi • Remedial building repairs have commenced with the loss of 2 inpatient beds for the duration of
the work Te Toki Maurere • Approval for bathrooms to be refurbished is being progressed • Staff have coped well after a death on the ward – debrief was well attended and time was made
for interested staff to attend the Marae and the tangi on separate days. One staff member may need further assistance with the grief cycle and EAP and other support is being arranged.
CHILD AND ADOLESCENT MENTAL HEALTH SERVICES CAPA Team Days - Voyagers and CAMHS have both had their quarterly team days. The team came up with some ideas around improving current intake processes as well as crisis assessment and treatment pathways of clients at risk. We value these days as it gives us the opportunity to focus on service improvement. Secret Agent Society Social Skills Training - The Clinical Coordinators and the ADON met recently to discuss the training priorities and budget. We were hoping to send 15 staff members on an evidence base social skills training program (Australian) and were brainstorming ideas on how to progress this within the current fiscal constraints. As a service we were able to look at our collective budget and prioritize accordingly. We are looking forward to this training being delivered in July this year. Recruitment - After a considerable recruitment drive, CAMHS and Voyagers now have no vacancies. Developmental Paediatrician - David Jones, (developmental paediatrician) has now started clinics in CAMHS for a trial period of three months. David is mainly available for the infant-child team. We are confident that these clinics will assist us in providing better care for those children with not only mental health concerns but developmental delay. Sorted Model of Care and integration of services project - The youth AOD project is underway. We are currently in the stocktake phase where all stakeholders and NGO providers are asked to complete a questionnaire. The aim of the project is to develop a sector wide model of care, to establish pathways, a clinical governance structure and for SORTED to be utilized as a workforce development hub. Risks and Mitigating Actions
18
COO Highlights Report May 2014 13
Crisis Service - Provision of a crisis service has continued to be an issue this month with 3 staff unexpectedly going off sick for over 3 weeks. This left 29 shifts on reduced staffing and fortunately just 5 overnight on call shifts that had to be covered from within the team. Again stand down time has also had an impact as the 9 hour break after a call back has meant shifts running on 2 staff instead of the rostered 4 in addition to the shortage caused by sick leave. PACT staff have done extra on calls, overtime has been incurred as we have a very limited casual resource. It presents risk in terms of waiting times to be seen, ability to do follow up work, staff fatigue from working overtime after the shift as work cannot be completed in a timely manner during the shift and we also have to consider the financial cost. PACT formalised their concerns about the current situation in a letter to the Clinical Co-ordinator and Team Leaders which led to a meeting to discuss the issues. Despite the concerns it was a constructive meeting which should lead to positive outcomes. The Clinical Co-ordinator and Team Leaders, together with the staff will progress with the implementation of these outcomes. SERVICE IMPROVEMENT UNIT
Project Waka
Good News Stories
Following the extensive training and testing of clinical equipment over April the migration to the new facility was completed over the week of 5-9 May, with the majority of services moving on Wednesday 7th May, starting at 0500 hours. The covers were taken off the new signage by Matt Valentine, Medical Leader and the first ED patient arrived before 7 am. Firsts for theatre used by Orthopaedic surgery and Maternity have also been acknowledged. The first week had the new facility fully tested with high occupancy rates across all services. Staff are reporting that they are enjoying the space in their new units and it is great to see both staff and public utilising the courtyard.
Risks and Mitigating Actions There are a number of small defects being reported and changes being requested by the staff as they settle in and notice key aspects of their new units. A process is in place for these being reported and resolutions being managed. ERAS Orthopaedics Good News Stories This last month has had a change of focus, although the PDSA tests continue. Earlier in the month the group invited the Geriatricians to the meeting to discuss how together we could develop the ERAS principles for the #NOF patients. Work is ongoing regards this. Julie Palmer, the ERAS project manager from MoH visited on 14 May and attended a group meeting also attended by Helen Mason (COO and project executive). Julie was very pleased with the progress we were making. Both Helen and Julie advised that the project be presented to the board.
19
COO Highlights Report May 2014 14
Our patient advocate has been involved with attending meetings and providing patient experience advice. Physio resource has been accessed to allow reintroduction of the pre-op exercise classes for patients booked for hip and knee joint surgery at Tauranga. PDSAs started this month are the implementation of an electronic Notice For Admission form and use of a patient diary to record and monitor post-operative recovery.
Risks and Mitigating Actions
BOPDHB does not have the Geriatrician resource to provide consultation on admission for #NOF as is best practice so a protocol will need to be developed to guide practice of junior staff based on agreed principles. Currently 61% attendance at MDT education classes in Tauranga which we would like to increase through improved booking practices.
Hospital After Hours Project – Tauranga Hospital
Good News Stories
3 month trial of a Clinical Support Nurse (CSN) underway to provide clinical assistance to patients, advice and support to staff working after hours. This role works across the Hospital 7 days a week, 5pm to 1.30am, reporting to the Duty Manager, to improve our capacity to respond to the deteriorating patient after hours. The trial has completed the first month and feedback from the RMOs indicates that the CNS is filling an important function and improving patient safety, whilst also enabling the Duty Manager respond to variance. The addition of a night handover implemented on 3rd March, continues to be well attended and regarded by the majority of the required attendees. The RMOs representing the project team including Brian Corley (Med Reg), Brooke Vosper (Ortho Reg), Matt Aitken (Gen Sur Reg), and Jono Hoogerbrug (House Officer) have reviewed and updated the guidelines for the night handover, with a view to improving the delivery of the handover. These guidelines have been reviewed and endorsed by the Heads of Department and Acting Medical Director. Risks and Mitigating Actions Feedback has been provided to the Project Team indicting resistance to the night handover from some of the surgical service registrars, who have expressed that they do not see the benefit of attending and have not seen this being supported and led by their SMOs/HoDs and are therefore choosing to not attend the handover. The issue has been addressed with the Heads of Department at their inter-departmental meeting on 16th May. The Heads of Department have endorsed the project and are facilitating communication out to the RMOs. Duty Managers have requested support for training on how to chair the handover meeting at night. This has also been highlighted as an important issue to the successful delivery of the handover by Heads of Department for buy-in and usefulness. Julie Williams is coordinating a training day in June to support this training using peer-to-peer approach. Increased visibility of Hospital Status at a Glance (HSAAG) Good News Stories Nurse Leaders are conducting training sessions with their wards on the features of the HSAAG using a fact sheet developed to support education. Risks and Mitigating Actions There is no agreed plan to provide additional training to the doctors or other clinical and non-clinical staff. This will need to be agreed at CCUG. Communications Team are involved and have been asked for their advice.
20
COO Highlights Report May 2014 15
IHI Open School Good News Stories Over 100 staff have now made a start on the Quality Improvement Capability course. In addition to this the DHB Executive Team and 10 staff from Planning and Funding have now been given access to start the course. All of the COO direct reports are committed to completing the course by the end of June. The course has been publicised in the latest version of Check Up magazine alongside a feature story on Clinical Physiology team who are now starting to see outcomes from the training. One member of staff has completed an improvement activity to reduce the time it takes to report an outcome of a clinical assessment – reducing it from 12 days down to 2 days, a saving of 10 days per patient. The Service Improvement Unit facilitated a planning day for the Respiratory Service using the IHI Open School as a basis for improvement. Access to the course will be provided to members of the team wishing to take improvement activity forward. Risks and Mitigating Actions Trevor Richardson has approached the Clinical School requesting their involvement in the administration of the training, as this is currently being managed within the Service Improvement Unit. There are still many staff who have requested access to the course but are not yet underway with the training. The Service Improvement Unit are working with these individuals to see how they can be supported through their training. CIRCA & OTHER PROJECTS UPDATE: CIRCA 1 Two CIRCA 1 projects have started; E –ordering of labs and Community Pharmacy to Éclair. Currently the PIDs and governance structures are being established. CIRCA 2 Patient Education Resource Centre (PERC) was presented to Clinical Governance Group. Service Improvement Unit has been invited to represent the BOPDHB on the eHealth Alliance group based on the CIRCA 2 activity under the Patient Education Framework. eHealth Alliance Group under the lead of Health Navigator are interested in looking at the development of the PERC at the BOPDHB as a resource that could be used by other DHBs and nationally. Approach has been made to Krames (licensed product used to deliver the PERC) to discuss funding options to support a regional/national approach. Risks and Mitigating Actions There are some issues to be resolved with key internal stakeholders and their explicit role in supporting the pilot at the BOPDHB. This has led to delays in progressing the implementation plan; however this has not hindered the first step of localising the content which continues. The activity is heavily linked to the Integrated Healthcare Strategy, specifically under the theme of Health Literacy and both are working together to address these issues and progress the activity. Microster A presentation on Microster was made to the doctors in Mental Health. The group appeared to be happy with the proposed changes. The second Microster business rules group meeting was held with further basic rules governing the roll out being discussed. The latest version of Microster has now been installed and is being tested. The roll out of the new version will coincide with the roll out of the new version of the intranet which will contain Microster Self Service. Microster Self Service allows electronic leave applications and call back claims and the remote viewing of work rosters.
21
COO Highlights Report May 2014 16
Volunteers
With the IHI Improvement Advisor course now completed the remaining focus is on the business as usual processing of volunteer applications.
In addition work has been going onto looking at working with St John over the role of managing the volunteer service on behalf of the BOPDHB.
Bay Navigator
Good News Stories
Map of Medicine
Meeting held here with Graham Guy and Damian Tomic to discuss progress. Identified functionality of MoM currently underway whereby pathways are directly integrated into the PMS system. This would make MoM much more user-friendly. Damian is going to provide Phil Back with some costing on this. Also discussed; a sidebar option which could be implemented in the hospital setting to avoid passwords. They have identified the need to provide pathways which are more concise, which is in line with our thinking. They have asked that we transfer our current pathways to the MoM structure with this in mind. Overall we seem to be ‘bridging the gap’ with regard to the future for MoM. Also attended a MoM Benefit’s Realisation meeting in Hamilton Website redesign Content is ready to be uploaded. The digital team are enthusiastic with regard to a new look site which will be more user-friendly and comprehensive. Pathways
Progress continues. No pathways completed in the last month but many nearing completion. New pathways are due to start and some have reconvened to address issues.
Risks and Mitigating Actions
Map of Medicine
Now that MoM and BN have been running alongside each other for a few months it is now becoming clearer with regard to the future direction/integration of the two projects. I believe it is important to identify a 2year/5 year plan to ensure that time and effort is put into the right initiatives within these projects. (CD)
SUPPORT SERVICES Good News Stories Formal confirmation of a NZQA process to develop orderlies and remunerate them subsequently – this gives them a sense of value and worth. 4 applicants for a coding position advertised. Previously we have attracted nil applicants however these coders are working in other DHBs and want to move to the BOP – so location does matter. Permanent flexi working out really well and have flexi nursing considering doing the same.
22
COO Highlights Report May 2014 17
Risks and Mitigating Actions Paging Whakatane but this is being address by Jeff and Owen and work arounds are in place to mitigate risk
23
COO Service Report – March 2014 Page 1 of 13
CHIEF OPERATING OFFICER’S PERFORMANCE REPORT PROVIDER ARM May 2014
SUBMITTED TO: Bay of Plenty Hospital Advisory Committee 2 July 2014
Submitted by: Helen Mason, Chief Operating Officer
RECOMMENDED RESOLUTION: That the Committee receives the report.
24
COO Service Report – March 2014 Page 2 of 13
HIGHLIGHTS SUMMARY CHIEF OPERATING OFFICER CWDs • Elective CWD are 85 below the phased plan for May 2014 and 492 below YTD.
• Acute CWDs were 56 under the revised plan in for May (estimate due to un-coded cases) and 5 over plan YTD.
• A comparison in the graph below with YTD April of prior years’ shows the significant increase in acute CWD delivered and the crowding out impact on electives.
Discharges • Surgical discharges are 46 above plan for the month of May 2014 and 149 ahead YTD. • For the month there were 117 more patient discharges when compared with May 2013 and YTD
compared to 2012-13 there have been 1,678 more discharges. ED attendances • When comparing May 2014 with 2013 ED attendances at Tauranga and Whakatane were 2.7%
and 2.8% higher respectively. YTD there are 8.2% more attendances than in the previous year at Tauranga and 3.2% more attendances at Whakatane (see below).
25
COO Service Report – March 2014 Page 3 of 13
Shorter stays six hour target results are closely monitored. Whakatane Hospital continues to perform very well. Recent Tauranga results are encouraging despite high throughput. The six hour target result for May at 93% was still the best May result on record.
Theatre • Provider Arm Performed 68 fewer main theatre operations during May 2014 compared to May
2013. Year to date there have been 55 fewer main theatre operations performed in total than for 2012-13 and 254 less elective procedures.
Other activity • During May hospital occupancy was 94.77% at Tauranga and 83.25% at Whakatane
• Outpatients are 8.7% or 170 First Specialist Assessments (FSA) above plan for the month and 1,025 or 5.2% ahead YTD.
• Follow-up visits are 2.0% or 93 ahead of contract for the month and 1,854 or 3.9% ahead YTD.
Efficiency • Acute ALOS per CWD recorded a record low level in May. Electives recorded the second lowest
ALOS per CWD in history, just above the 2013 result. Graphs below illustrate the increased discharges and ALOS combined across both sites.
Electronic Inpatient Discharge Summaries sent within 24 hours 0.0% 51.1% 95.0% (43.9%) 52.0% 95.0% (43.0%)
KEYN/A = Not availableU/D = Under Development
Month Year to date Month Year to dateBEST VALUE FOR HEALTH SYSTEM RESOURCES
Note: ESPI figures include ungraded. This will be reviewed and they maybe excluded in future* Due to changed criteria, no comparison to last year is available
28
May-14
Key: Trend Arrows shows improvement, shows deterioration, shows no change, from previous month
Target Achieved (A), Target Not Achieved (NA)
Experience of Care: Service Result Target Variance Comment & Action Plan
Outpatient DNA Rate Provider 6.5% 5.0% (1.5%)Surgical 7.4% 5.0% (2.4%)
Medical 3.6% 5.0% 1.4%
WCF 7.5% 8.0% 0.5%
Outpatient DNA Maori Provider 15.4% 5.0% (10.4%)Surgical 16.3% 5.0% (11.3%)
Slight reduction from a poor result in April. Reducing Maori DNA's is an ongoing project.Continued focus on patient centered bookings for all outpatient clinics - ongoing work to identify and remove barriers to clinic attendance, e.g. use of telehealth diabetes clinics for Opotiki primary care.
Detailed review being undertaken to identify where variances are as some parts of the service are performimg better than others. WHK Maori DNA rate is higher and Patient cnetrered booking process needs to be reviewed. The new system for reception/ administration for paediatrics and acute care at wahakatane is impacting on the scheduling component of the paediatric admin scheduler
Consistent result however there is a large amount of uncoded activity which may have further bearing on this result.
Achieved
achievedachievedAchieved
Monthly reports by NHI being reviewed by HOD's. The majority of cases sit within Paediatrics with on average 30% of these being arranged admissions.
29
Service Result Target Variance Comment & Action Plan
Medical 47.3% 95.0% (47.7%)WCF 40.7% 95.0% (54.3%)
6 Hour Target Provider 92.7% 95.0% (2.3%)
NA
LOS Outlier Provider 1.9% 1.5% (0.4%)Surgical 1.3% 1.5% 0.2%
Medical 2.7% 1.5% (1.2%)
WCF 1.7% 1.5% (0.2%)
Smokers Referred to Cessation
Provider 91.5% 95.0% (3.5%)
NA
NA
NA
NA
A
A
NA
A
A
NA
NA
Lower demand in Paediatrics at both Tga and Whakatane for the period. Numbers starting to increase esp. in TGA. Maternity birthing numbers have been lower in TGA slightly higher in WHK YTD.
Currently acheived although there are 651 acute cases sti l l uncoded for the month
Several eating disorder patients requiring treatment impacting on length of stay
No further improvement this month however an increase in transfer to the transit loung will impact on this target. Continued work on flow through of acute work load - the area that is achieving this is HIA ward however other areas are sti l l experiencing delay due to prioritisation of acute work load before discharge. Transit lounge use remains
There are 196 + 8 Dental procedures that are uncoded. There are 108 uncoded elective cases.
There are 278 uncoded acute episodes uncoded.
Expected for this time of the year. All beds openAs noted above - the medical wards have been particularly busy with acute demand from mid-May. We await completion of coding to identify impact of LOS ( t l ti LOS t b hi h h hi h % f l ti k t d d
Close to target continue to review. Service consistently sits between 20% and 30% with TGA performing better than WHK generally.
Within range of +/- 2%Negative variances in actual to required NHPPD noted particularly in last week of May which impacted on overall variance. This was due to high bed util isation and acuity over this time with l imited capacity to variance respond to demand. Results impacted by Whakatane baseline staffing requirements and high speciall ing requirements
February Elective C Sections at 26.1% which pushes ALOS rate higher.
Achieved
Achieved
Achieved
Below target for two months now. Non DOSA patients are closley scrutinised by CNM's and Duty Managers prior to admission. Suggest case type.
As for medicine the breaches reported have not imapacted on the 6 hour tagte with l i h b h d d
Achieved
Performance slipped slightly in May due to some very high attendance days and high inpatient workload during the end of the month. Result has improved since
Achieved however acknowledge impact of uncoded activity on the eventual result.
Impacted on by Project Waka and preparations for migration.
result affected by reduced cases holding for C-sections on gyne l ists
Unrecorded entries need to be addressed in order to accurately measure this performance.
Variance caused mainly to the unrecording of this measure
This measure is impacted by 759 acute and elective uncoded cases - LOS outliers continue to be identified and management plans util ised where possible. The majority of LOS outliers are acutely unwell - with very few patients 'stranded' by process or unmet demand. The service is consistently within the outlier target of 1.5%
Continued attention to identification of smokers and documentation of cessation care. Key initiative this month has been the inclusion of smoking information as a mandatory reporting field in ED electronic discharge which is starting to increase documentation. We are currently reporting performance to MOH weekly
30
System: Service Result Target Variance Comment & Action Plan
Sick Leave Provider 3.1% 3.1% (0.0%)Surgical 3.3% 3.1% (0.2%)Medical 3.1% 3.1% (0.0%)WCF 2.1% 3.1% 1.0%Support Service 2.5% 3.1% 0.6%Maori Health 4.2% 3.1% (1.1%)RCS 3.4% 3.1% (0.3%)Mental Health 3.0% 3.1% 0.1%
Mandatory Training completed Provider 87.7% 100.0% (12.3%)within 3m of start date Surgical 93.3% 100.0% (6.7%)
OP FSA Provider 20,618 19,593 1025Surgical 11,438 10,601 837
Medical 5,901 5,995 -94
WCF 3,279 2,997 282
OP FU Provider 48,852 46,998 1,854Surgical 24,930 24,489 441Medical 14,197 14,072 125WCF 9,725 8,438 1,287
NA
NA
NA
NA
A
A
A
A
Not unexpected result for May.Within targetAchieved
high number particularlly for Whakatane. Team Leaders managing
All Nursing mandatory training up to date. Plan in place for Whakatane staff
Team leaders to manage compliance achieved
Results improving
Some long term sick leave in some areas affecting resultAchieved
Improving overallReport received monthly for followup, mainly RMO run changes influencing this months resultMain issue is RMO orientation team leaders to review result
Ahead in both Paed Med & Gynae FSA's - attributed to fall ing F/Up ratio and demand
Gynaecology volumes slightly ahead on contract YTD
Demand driven and one factor that has impacted on elective CWD.Continued demand
Mainly due to Paed Med CWD activity, contract volumes being adjusted in 14/15 yr, very low birth numbers in the current year esp. TGA
Gynaecology volumes slightly ahead on contract YTD. Sl ightly ahead of target YTD,
Under delivery in: Haemtology due to the service being provided through Waikato given vacancy at BOPDHB, Gastroenerology due to first half of the year being down two Gastroenterologists and also a focus on colonoscopy delivery, Dermatology due to ratio to FU issues. These are offset sl ightly with overdelivery in Virtual FSAs
Achieved. Additional elective service contracted by MoH. Also does not include uncoded elective activity (approx. 150)
At low levels. Majority of impact is from a small number of part timers accumulating leave. RCS has a 50:50 part time / full time ratio.
Plans are in place for the majority of staff exceeding 200hours , some difficulties with staff being released at present.
Usual strategies are employed however signficant struggle to achieve reducing in leave balances to this extent across the board and maintain BAU.
Some leave buy outs have are taking place; along with continued identification and management of individual staff with high AL balances.
Despite leave being planned and taken some areas sti l l struggling to reduce given
Managing in usual way with leave plans. Always find it dificult to manage this one
Shortfalls known and plans in place however unlikely to address extent of variance in time for year end. Focus is to minimise extent and impact.
Overdelivery however required to generate treatment l ist.
Ahead of targetWithin target
108 elective uncoded events for May - the result therefore contain an estimation.
Mainly in Paed Med and Obstetric (specialist)
31
Service Result Target Variance Comment & Action Plan
Operating Expenses Provider 10,993 9,713 -1,280
Surgical 4,031 3,516 -515
Medical 2,580 2,227 -353
WCF 502 337 -165
Support Service 114 81 -33 Maori Health 11 14 2RCS 989 965 -24
Mental Health 405 321 -84
Personnel Costs Provider 18,064 16,661 -1403
Surgical 5,705 4,849 -856
Medical 4,576 4,249 -327
WCF 1,686 1,534 -152
Support Service 590 548 -42 Maori Health 365 303 -63 RCS 2,266 2,247 -19 Mental Health 2,185 2,208 23
FTE's Provider 2,346 2,162 -184
Surgical 637 562 -75
Medical 570 507 -63
WCF 176 157 -19
Support Service 147 136 -11 Maori Health 62 50 -12 RCS 380 384 4
Mental Health 302 297 -5
NA
NA
NA
FTE's associated with MHSOP inpatient staffing budget, overtime costs associated with specials and adult inpatient staffing shortages..
Mainly due to DNS backpays in the monthMedical variance 635k offset by outsourced SMO of -342k.
CC breakdown of variances not available at time fo report. Drivers for variances known including additional theatre resourcing. For Nursing, HPPD are within range which suggests much of variance is demand driven. Includes SMO 1.5 FTE in change of leave l iabil ity.
Communications, Professional Fees Transport and facil ities (whanau houses)
$166K of increase in leave l iabil ity ; $104K over spend to budget in entitled CME; 3 FTE HO & 1 FTE Reg required for roster but not budgeted ( See narrative I month end report for detail)
Mainly due to LOS/Vacancy Factor adjusters in Budget not being fulfi l led plus high number of specials required esp. in TGA Paeds with anorexia patients
$301K overspend in minor purchases (Waaka and increase in minor capital lower l imit)Patient meals, Laundry & Cleaning $124K ovespend (See narrative in month end report for more details)
O&G locum costs in WHK plus SMO placement fee; Increasing patient volumes pushing up consumables
Range of variance across expensesPall iative Care External Beds (YTD ($117k) - to be flagged with P&F
Mainly due to LOS/Vacancy Factor adjusters in Budget not being fulfi l led plus high number of specials required esp. in TGA Paeds with anorexia patients
Court Liason, Nurse Leader position, professional staff over Nursing adjuster
Change in minor capex levels not budgeted resulting in overspend in minor equipment as well as significant project waka expenses incurred. MRI/CT scans $84k over and Outsourced Medical Locums $68k over. Project Waka cleans and patient meal contract variation impacting the month result.
Nursing $247k over due to one l ine adjuster and safety watches unbudgeted, also high acute demand - demonstrated by negative variance in NHPPD. Medical personnel $90k overbudget, new resource approved but not budgeted, Afterhours Registrar in ED, Model of Medicine
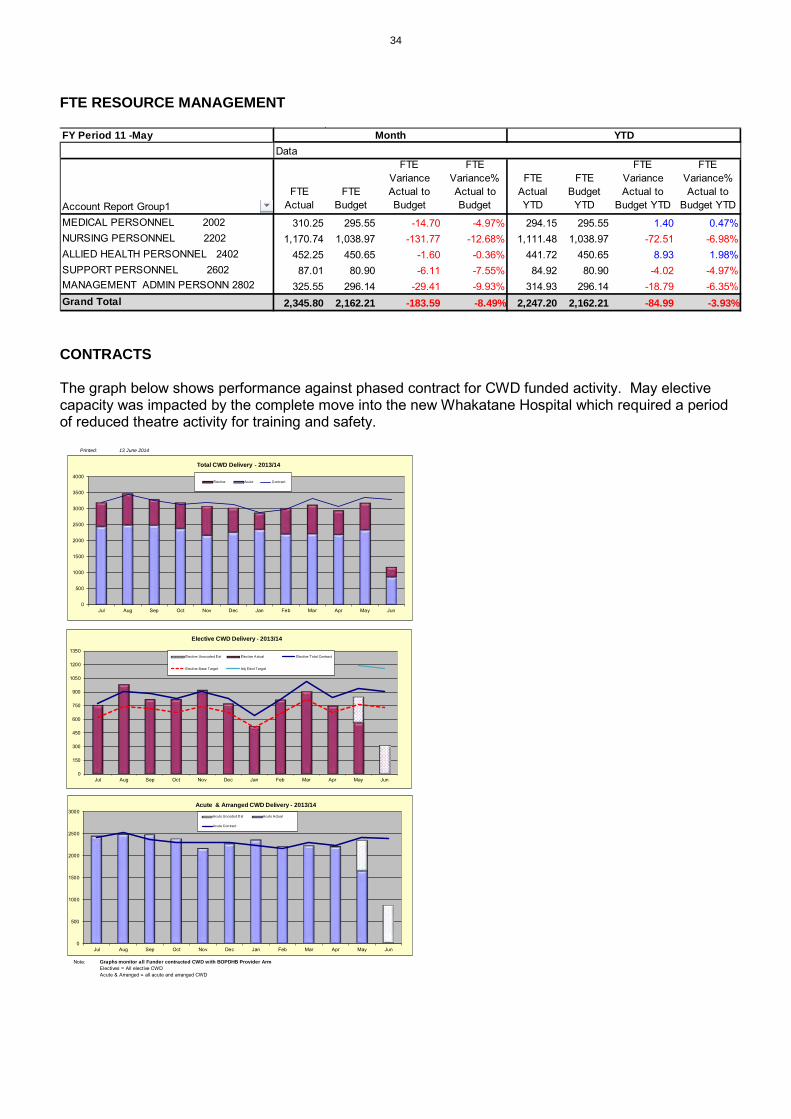
CONTRACTS The graph below shows performance against phased contract for CWD funded activity. May elective capacity was impacted by the complete move into the new Whakatane Hospital which required a period of reduced theatre activity for training and safety.
Note: Graphs monitor all Funder contracted CWD with BOPDHB Provider ArmElectives = All elective CWDAcute & Arranged = all acute and arranged CWD
0
500
1000
1500
2000
2500
3000
3500
4000
Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun
Total CWD Delivery - 2013/14
Elective Acute Contract
0
500
1000
1500
2000
2500
3000
Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun
Acute & Arranged CWD Delivery - 2013/14Acute Uncoded Est Acute Actual
Acute Contract
0
150
300
450
600
750
900
1050
1200
1350
Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun
Elective CWD Delivery - 2013/14
Elective Unocoded Est Elective Actual Elective Total Contract
Elective Base Target Adj Elect Target
34
WAITLISTS
Medical FSA
Gastro Procedures
Surgical FSA
691 730 704 716627
766 754 697794
533642 582
449541 501
724
546654
0
200
400
600
800
1000
1200
1400
0
200
400
600
800
1000
1200
Ref
s -R
ec'd
/ Ac
cc'd
/ A
pp't
Tota
l Num
ber
Wai
ting
Bay of Plenty - Medical FSA
Bay of Plenty Waiting > 5 Months Waiting < 5 months Referrals Received BOP" Referrals Accepted BOP"BOP Total Seen - FSA
Graph shows numbers waiting longer than five months for a Medical FSA and compares this to total numbers waiting.Target: Comments:
0
500
1000
1500
2000
2500
3000
3500
Dec-12
Jan-13
Feb-13
Mar-13
Apr-13
May-13
Jun-13
Jul-13
Aug-13
Sep-13
Oct-13
Nov-13
Dec-13
Jan-14
Feb-14
Mar-14
Apr-14
May-14
Tota
l Num
ber W
aitin
g
Bay of Plenty Gastro Procedures
Bay of Plenty Waiting > 5 Months Waiting < 5 monthsBay of Plenty Surveillance Proc Out of Time Surveillance Procedures Waiting
Graph shows numbers waiting longer than five months for a Gastroenterology procedure compared to total numbers waiting.Target: Comments:
0
500
1000
1500
2000
2500
0
500
1000
1500
2000
2500
3000
3500
Ref
rec'
d/Ac
cept
/See
n
Tota
l Num
bers
Wai
ting
Bay of Plenty - Surgical FSA
Bay of Plenty Waiting > 5 Months Waiting < 5 months Referrals Rec'd BOP
Referrals Accepted BOP Total Seen - FSA BOP
Graph shows numbers waiting longer than five months for a Surgical FSA compared to total numbers waiting.Target: Comments:
35
Surgical Procedures
WCF FSA
WCF Procedures
Graph shows numbers waiting longer than five months for a WCF FSA compared to total numbers waiting.Target: Comments:
Graph shows numbers waiting longer than five months for a Surgical procedure compared to total numbers waiting.Target: Comments:
0200400600800
100012001400160018002000
Dec-12
Jan-13
Feb-13
Mar-13
Apr-13
May-13
Jun-13
Jul-13
Aug-13
Sep-13
Oct-13
Nov-13
Dec-13
Jan-14
Feb-14
Mar-14
Apr-14
May-14
Tota
l Num
bers
Wai
ting
Bay of Plenty - Surgical Procedures
Bay of Plenty Waiting > 5 Months Waiting < 5 months
Graph shows numbers waiting longer than five months for a WCF procedure compared to total numbers waiting.Target: Comments:
0
100
200
300
400
500
600
700
0
200
400
600
800
1000
1200
Ref
rec'
d/Ac
cept
/See
n
Tota
l Num
bers
Wai
ting
Bay of Plenty - WCF FSA
Bay of Plenty Waiting > 5 Months Waiting < 5 months Referrals Rec'd BOP
Referrals Accepted BOP Total Seen - FSA BOP
020406080
100120140160180200
Dec-12
Jan-13
Feb-13
Mar-13
Apr-13
May-13
Jun-13
Jul-13
Aug-13
Sep-13
Oct-13
Nov-13
Dec-13
Jan-14
Feb-14
Mar-14
Apr-14
May-14
Tota
l Num
bers
Wai
ting
Bay of Plenty - WCF Procedures
Bay of Plenty Waiting > 5 Months Waiting < 5 months
36
Property Services General Manager Monthly Report
June 2014
1. Red Flags
Nothing to report Highlights Project Waka - Fletchers Final Account The final account has been settled with Fletchers, within four weeks of completing the project. There is a positive variance of $121,600. Property Services Computerised Maintenance Management System (BEIMS) Property Services was recently awarded two excellence awards by the Melbourne based vendor. One, for the deployment of the system, and the other for the management of the system by our Super User.
2. General
Tauranga Campus Site Designation The document has been signed by the Minister and subsequently advertised by TCC. The Final objections close on 26 June.
3. Project Waka
General The final account has been agreed with Fletchers. The project remains $121,600 under budget. This positive variance is likely to be used for additional post-project completion works.
Project Works Summary The contractor is still completing the defect works. These works are being completed without disruption to the hospital operations. The major learning moment arising, post the move to the new premises, has been the need to install additional “hold open” controls to corridor fire doors. These works could have been undertaken as part of the main build, had the architect, service improvement team and the various clinical areas spent more time during the design stage, assessing the flow of patients. Furniture Fixtures and Equipment We are yet to complete the learning moment review, and apply the learning moments to how we can do B50 L2 project better.
37
GM Monthly Report – June 2014 DocMan/Management
4. Other Major Projects Tauranga MSB 5 (MSB3 Replacement) Electrical Work We have successfully completed the preparation work. There will be two further service impacts on ED, before we are ready for the final commissioning and cut-over to the new switchbaord in late July. The project remains on budget. Planned Commencement Date April 2014 Planned Completion Date August 2014 - Percentage complete last month 45% - Percentage complete this month 75%
Whakatane – New Water Tanks The additional funding required to construct two new tanks (potable and fire water) was declined by AMC. Therefore, we will now only proceed to design and construct a potable water tank. Planned Commencement Date July 2013 Planned Completion Date February 2015 - Percentage complete last month 10% - Percentage complete this month 10%
Whakatane – Santon Demolition and Post Demolition Strategy Two sign-off meetings are required:
• Paediatricians as to their clinic and office locations • RMO/SMO rooms etc
The paediatrician meeting was very successful. The final Dawson accommodation plans will be presented to the SMO and RMOs in July for sign-off. Following sign-off, the Dawson refurbishment documentation will be completed. Planned Completion Date December 2014 - Percentage complete last month 80% - Percentage complete this month 80% Whakatane – Relocation of Pathlab to a Stand-alone Facility Pathlab have signed off the construction contract, hence we can now award the contract to the builder. We are awaiting the consent approval from Whakatane District Council before construction can commence. Revised Planned Completion Date December 2014 - Percentage complete last month 15% - Percentage complete this month 18%
38
GM Monthly Report – June 2014 DocMan/Management
Tauranga ED UPS Upgrade This work will be complete in June. Now that the MSB 5 preparation has been completed, the cut-over to the new UPS will be undertaken in the first week of July. Completion Date February 2014 Revised Completion Date July 2014 - Percentage complete last month 85% - Percentage complete this month 85%
Tauranga Theatre UPS Upgrade The decision has been made to delay this work until post the go-live of MSB 5. The delay has been based on availability of resources and spreading the operational impacts. The additional tier for the switchboard has been ordered. This tier will allow the work to be completed with minimal disruption to the theatres. Planned Completion Date January 2014 - Percentage complete last month 25% - Percentage complete this month 25%
Tauranga Boiler House Seismic Upgrade We obtained competitive pricing and the additional tender came in more expensive than the original quotation. We will now revert back to the original tender who is more qualified to complete the works.
Planned Completion Date August 2014 - Percentage complete last month 10% - Percentage complete this month 10% Tauranga Cancer Centre The preliminary concept plan has been signed off. The project will be funded from the trust account. Planned Completion Date January 2015 - Percentage complete last month 10% - Percentage complete this month 10% Tauranga Campus – Energy Management Programme The report will be delivered to the DHB in late June.
Security Access System Upgrade 1000 Whakatane and Tauranga staff have been loaded onto the new system. Due to the delay in completing the Stage 2 work, above, Stage 3 will now be moved into 2014/15 financial year.
Stage 3 Tauranga Campus Planned Completion Date 30 June 2014 - Percentage complete last month 5% - Percentage complete this month 5%
39
GM Monthly Report – June 2014 DocMan/Management
Tauranga – Emergency Lighting Upgrade Good progress continues to be made by the contractor. Planned Completion Date August 2014 - Percentage complete last month 30% - Percentage complete this month 75% Tauranga – Demolition of Jacaranda House Work is complete. Minor damage to the residential houses opposite the demolition site has been reported. We reacted to the initial advice from the property owners by undertaking a photographic inspection and record. We have also installed accelerometers to record the vibration for the demolition activity. The contractor has been advised of the potential claim for damages.
5. Third Party Projects Radiotherapy Development (KKC)
Preparation work for occupation by the cancer centre of the office area is underway.
Northern Campus Development (NCD) Nothing to report.
6. Risk, Compliance & OHS
Nothing to report
7. Facilities Management Update This Month
Fire Alarms Activation (false) TGA - Site General 1 - Acute Mental Health 0 WHK - Site General 0 - Ward 8 0 Fire Alarms Activation (real) TGA - Site General 0 - Acute Mental Health 0 WHK - Site General 0 - Ward 8 0
40
GM Monthly Report – June 2014 DocMan/Management
Reportable Events TGA 0 WHK 0 Power interruption TGA 0 Power interruption WHK 0 Lost time injury TGA 0 Lost time injury WHK 0 After Hours Call-outs TGA this month 11 WHK this month 5
8. Property Management Nothing to report.
9. National & Regional Facilities Management Initiative Regional Nothing to report. National The bench mark site visit to Mid Central DHB was very useful in assessing the resource level for the Tauranga facilities management team.
41
BOPDHB QUALITY AND PATIENT SAFETY WALK-ROUNDS
SUBMITTED TO: Bay of Plenty Hospital Advisory Committee 2 July 2014 Prepared by: Averil Boon and Debbie Brown; Quality and Patient Safety
Endorsed by: Gail Bingham; General Manager Governance and Quality
RECOMMENDED RESOLUTION: That the Committee endorses the introduction of quality and patient safety walk rounds. ATTACHMENTS:
ATTACHMENTS:
• Appendix 1: Process
• Appendix 2: Sample Quality and Safety Walk-round Schedule
• Appendix 3: Sample Executive/Senior Leadership Team
• Appendix 4: Sample Questions – Patients and staff
• Appendix 5: Sample Communication – Prior to planned visit
• Appendix 6: Sample Walk-round Leaflet
• Appendix 7: Sample Preparation for the Senior Managers Leading the Quality and Patient Safety Walk-round
• Appendix 8: Sample Communication after the Quality and Safety Walk-round
• Appendix 9: Sample Final communication after the Quality and Safety Walk-round
• Appendix 10: Sample Quality and Safety Walk-round Action Plan Template
42
BACKGROUND:
Leadership walk-rounds is an improvement tool that connects senior leaders with their frontline staff to help build a culture of safety within the organisation.
The tool was developed by Allan Frankel, MD, (Director of Patient Safety, Partners Health Care System, Boston, Massachusetts, USA) as a way both to educate senior leadership about safety issues and to signal to front line workers the senior leaders’ commitment to creating a culture of safety. The Brigham and Women’s Hospital, Boston, USA was able to demonstrate a significant improvement in safety culture by undertaking walk-rounds.
Why Do Walk-Rounds?
Generally, the resources required for walk-rounds are meagre, but the returns are significant. Benefits include:
1. Improved understanding between frontline providers and senior leaders 2. Better-educated leadership about frontline concerns 3. Increased responsiveness of the organization to problems 4. Faster implementation of improvements 5. More efficient use of capital and operating expenses.
Justification - Benefits of Walk-Rounds
• Leadership walk-rounds allow senior leaders to have a structured conversation around patient safety with frontline staff, and enquire as to the barriers to caring for patients as safely as possible.
• They provide an opportunity to connect senior leadership with frontline staff. • They increase awareness of safety issues among all clinicians and establish a strong
commitment by senior leadership to a culture that encourages patient safety. • They allow senior leaders to obtain and act on information gathered that identifies
opportunities for improvement. • They connect senior leaders with staff in a way that educates senior leadership about
safety issues and also signals to staff senior leaders’ commitment to a patient safety culture.
• They educate staff about patient safety concepts and improvement as well as incident reporting systems.
• Process will allow consistent feedback to frontline providers and leadership about the process and the actions taken.
Resource Analysis
Quality and Patient Safety walk-rounds can be conducted in any setting such as wards, departments, operating theatres, clinics, general practice and community settings, but are not limited to these. They are also useful in services such as laboratory and orderlies or other areas that may affect patient care or the safety of the organisation such as information technology and
43
finance. They provide a formal process for members of the executive/senior management team/members of the board to talk with staff about safety issues in their unit or team and show their support of staff for reporting errors/near misses.
• Time commitment – senior leadership and staff • To ensure continuity, it is advised that a named person be identified to coordinate all
Quality and Patient Safety walk-rounds. It is important for the individual to have appropriate authority, resources and time to effectively manage the process.
Seven steps are required for effectively implementing Walk-Rounds:
1. Preparation — Ensure commitment and regular participation by leadership, secure dedicated resources from quality and patient safety department, and clearly communicate process, scheduling, and feedback mechanisms for the rest of the organization.
2. Scheduling — Set Walk-Rounds months in advance and accommodate schedules of senior leaders, supporting patient safety staff, and other participants.
3. Conducting Walk-Rounds — decide where to conduct the sessions. Sessions should include opening and closing statements and a series of specific questions.
4. Tracking — set up a robust process for tracking and ranking collected data. 5. Reporting — share walk-rounds data with a multidisciplinary committee so that action
items may be assigned to management personnel. 6. Feedbacks — establish a clearly delineated and formal structure for feedback to frontline
providers who participate in Walk-Rounds and to executive boards about findings and actions taken to address them.
7. Measurement — Evaluate whether Walk-Rounds are effective in improving the organisation’s culture. A number of validated surveys are available to quantify caregivers’ attitudes and perceptions of their working environments.
Communication
A strong communication plan is essential to the success of the Quality and Patient Safety Walk-round initiative. This is informed by the approach adopted by the organisation. Briefing staff so they know about the initiative and understand the aims is really important. General staff briefings, newsletters, notice boards, team meetings, and intranet communication may be used to promote the initiative.
Tracking Mechanism
For effective use and follow up, the executive/senior management team normally commits to maintaining a record of the process. A tracking mechanism (electronic) can then be used to monitor progress while at the same time providing reports on issues identified, actioned, escalated and resolved. The nominated Quality and Patient Safety Walk-round person will be responsible for maintaining the record.
IMPACTS ON BAY OF PLENTY DHB GOALS AND OUTCOMES
44
In summary, walk-rounds can:
• Demonstrate top level commitment to improving patient safety and quality of care; • Provide opportunity for direct engagement and communication with patients about safety
and their experience; • Establish lines of communication about patient safety among frontline staff and senior
leaders throughout all departments within the organisation; • Provide opportunities for staff to raise concerns and suggest improvements; • Identify opportunities with staff concerned for improving safety; • Encourage reporting of issues, errors, and near misses; • Promote a culture for change pertaining to patient safety; • Establish local solutions to minimise risk; and • Demonstrate accountability.
45
BAY OF PLENTY DISTRICT HEALTH BOARD
Page 1 of 12
Appendix 1 - Process
AIMS Demonstrate senior leader’s commitment to quality and patient safety for patients, staff and the public, increase staff engagement and a culture of open communication, identify, acknowledge and share good practice, support a proactive approach to minimising risk, timely reporting and feedback, strengthen commitment and accountability for quality and patient safety
SETTING THE SCENE Agreed and confirmed at the start of the walk-round, the walk-round is an opportunity for an open discussion on quality and patient safety and is not an assessment or inspection. All information discussed in a walk-round is confidential
COMMUNICATION A clear communication plan for the Quality and Safety Walk-round initiative, all staff are briefed about the initiative and the aims. General staff briefings, newsletters and intranet communication should be used to promote the initiative, providing feedback and follow up with the unit/team within agreed time frames
HOW The team in the area being visited are asked to think of a recent example of a patient safety incident they have experienced and share this at the meeting so that discussion can take place on - what is working well, how this was managed by the team and how the senior management team can help
WHERE Walk-rounds start with a tour of the unit and meeting with patients and staff, a meeting venue close to the patient /service area (office or meeting room) is used for the discussion
WHEN The Walk-rounds occur at an agreed frequency, dates and times are arranged, in consultation with area, and communicated by the named person coordinating the Quality and Patient Safety Walk-round, who will schedule all dates and areas to be visited for the year
WARD/DEPARTMENT/UNIT TEAM Ward/Department/Unit manager (identified lead), on the day there may be a number of other staff present e.g.:
• Doctors (SMO – RMO) • Allied health staff • Administration Support Staff • Catering Staff • Nurses/Midwives, Health Care
Assistants • and other Support Staff
SENIOR LEADER WALK-ROUND TEAM
One of the following will be designated lead: • Senior Leadership representative • Quality and Patient Safety
representative • A member of the board • Volunteer Patient Advisor
representative • A scribe/note taker
46
BAY OF PLENTY DISTRICT HEALTH BOARD
Page 1 of 12
Appendix 2: Sample Quality and Safety Walk-round Schedule REPRESENTATIVE SERVICE UNIT /
TEAM / DEPT
DATE DAY OF WEEK
TIME SENIOR LEADER
VOLUNTEER PATIENT ADVISOR
QUALITY & PATIENT SAFETY
NOTE TAKER
47
BAY OF PLENTY DISTRICT HEALTH BOARD
Page 1 of 12
Appendix 3: Sample Executive/Senior Leadership Team Walk-round Members Example Senior Leadership Team (one lead for each walk-round): NAME TITLE POINT OF CONTACT [insert details] Chair & Board Members [insert email and phone
contact details] CEO Chief Operating Officer Chief Medical Officer Director of Nursing General Managers
(Governance & Quality, Planning & Funding, Maori Health, Finance, Information Management, Property Services etc.
Service Leaders Others Others may be involved in the visit or provide advice and support in follow up to the visit e.g. Risk Management / Health and Safety / Technical Services / Property Services etc. NAME TITLE POINT OF CONTACT NAME TITLE POINT OF CONTACT NAME TITLE POINT OF CONTACT Volunteer Patient Advisors: NAME TITLE POINT OF CONTACT NAME TITLE POINT OF CONTACT
48
BAY OF PLENTY DISTRICT HEALTH BOARD
Page 2 of 12
Appendix 4: Sample Questions Sample Guide for Discussion with Patients
The prompts below are examples that may be used in the walk-round conversation with patients.
SAMPLE QUESTIONS Talk With, Not About Patients Direct your conversation, patient report, questions and answers directly to patients and their family members using first person language. Be mindful of your body language and convey warmth and friendliness in your interactions with them.
1. How are we doing today? 2. Is there anything that we could do better? 3. If you were in-charge here, what would you do to make things work
better?AME Outpatient:
1. Did you staff explain your rights as a patient when you came to the hospital or clinic?
2. Did you experience any long waits during your visit today? If so, where? 3. Did you have any issues scheduling your visit today? 4. Have you been able to find your way in the hospital/clinic? 5. Are you being kept informed of the status of your business at the
hospital/clinic? 6. Has the hospital/clinic staff been helpful to you? 7. Will you speak positively about your experience at Parkland today? 8. If we could make one thing easier for you at Parkland, what would it be?
Sample Guide for Discussion with Staff
The topics below are examples that may be used to guide the discussion. Not all areas can be covered at each visit. It is helpful for the walk-round members to meet in advance to prepare for the specific walk-round. The walk-round leader in consultation with the group makes a decision based on engagement with the unit/team on which areas to focus on. The aim is to take a discursive rather than a formulaic approach.
TOPIC SUGGESTED QUESTIONS 1. Introduction “We are moving as an organisation to open communication
because we believe that doing so will make your work environment safer for you and your patients. The discussion we are interested in having with you is confidential and purely for patient safety and improvement. We are interested in focusing on the systems you work in each day rather than on blaming specific individuals. The questions we might ask you will tend to be general ones, and you might consider how these questions might apply in your work areas in regards to medication errors, communication or teamwork problems, distractions, inefficiencies, problems with protocols, etc. We are happy to discuss any issues of concern to you. Our goal is to take what we learn in these conversations and use them to improve your work environment and our overall delivery of care.” • What do you do well – what are you most proud of here? Could this
practice be of benefit elsewhere? • Can you tell us one thing you are happy with and one that might
49
BAY OF PLENTY DISTRICT HEALTH BOARD
Page 3 of 12
cause you concern? • Would you be happy for yourself or a member of your family to be
treated in this area? (Good starting question which can be profoundly indicative of a serious problem).
• What patient or staff safety issues keep you awake at night? • Is there anything we could do to help you or your staff to further
minimise risk? 2. Communication • Can you describe how communication among staff either enhances
or inhibits safe care on your unit/team? o shift handovers o between teams e.g., doctors, nurses, health and social care
professionals o support staff (clerical, catering, cleaning, orderlies)
• Have you discussed patient safety issues with patients or their families?
• Do patients and families raise any safety concerns? • How legible are the patient’s healthcare records? • Have you any problems accessing patients’ healthcare records?
3. Teamwork • Can you tell us how your team works? • Can you tell us how the team works with other teams? • What is staff morale like?
4. Risk Management • Tell us about the last time a patient was harmed here/about the most recent near miss? What happened? (Good starting question to get the discussion going).
• When you make a mistake, do you report it? What makes you do that?
• If you prevent/intercept a mistake, do you report it? • If you make or report an error, are you concerned about personal
consequences? • Do you know what happens to the information that you report?
5. Prevention and Control of Health Care Associated Infection
• What were your last hand hygiene audit results? Were there areas to be improved and what are you doing to improve them?
• What is the standard of cleaning of clinical equipment - pumps, commodes, drip stands, trolleys, etc? Are they cleaned regularly?
• Do you know how often different items should be cleaned? If not do you know how to find out (e.g. Cleaning And Disinfection - A-Z Of Clinical Equipment policy)?
• What percentage of patients on antibiotics has a review date documented in their medication record?
• What percentage of your patients with peripheral intravenous lines or urinary catheters has the care bundle components recorded today?
6. Environment • What aspects of the environment are likely to lead to the next patient harm? Examples:
o Broken sinks, taps, bedpan washers, scales, ligature points, etc.
o Not enough information available (e.g. building works affecting care)
7. Equipment • Do you have regular maintenance of your equipment? • Do you have service notices on your equipment? • Do you have access to all the equipment you need to care for your
patients safely? 8. Process • What audits (both clinical and non-clinical) does your area undertake
or lead? • Today, are you able to care for your patients as safely as possible?
If not, why not? • Have there been any near misses that nearly caused patient harm
but didn’t? Examples: o Taking a drug to give to a patient and then realising it is
50
BAY OF PLENTY DISTRICT HEALTH BOARD
Page 4 of 12
incorrect o Mis-programming a pump, but having an alert that warns
you o Incorrect prescriptions/orders caught by nurses/midwives or
other staff 9. Continuing professional
development • What incident, risk management, quality improvement and clinical
governance training have you had? • What infection prevention and control and medication management
training have you had? • Are your team up to date with mandatory training, for example, Basic
Life Support, Moving and Handling, Fire Training, Hand Hygiene? 10 Leadership • Do you feel supported when you make a mistake or things go
wrong? • Who leads your team? • What specific intervention from senior management would make the
work you do safer for patients and staff? Examples: o Organise multi-disciplinary groups to evaluate a specific
problem o Facilitate in changing the attitude of a particular group o Facilitating interaction between two specific groups
• What would make these Quality and Patient Safety Walk-rounds more effective?
• Have you found participation in these Quality and Patient Safety Walk-rounds beneficial?
11 Sample Closing Statement
“We appreciate the time and effort you put into taking care of patients and making their experience in our organisation remarkable. Our job is to take the information you have given us, analyse it carefully, figure out what actions we might take to fix problems, assign those responsibilities to individuals, and hold their feet to the fire until the problems are solved. We promise to let you know how we’re doing and we will come back and elicit your opinion. We will work on the information you have given us. In return we would like you to tell two other people you work with about the concepts we have discussed in this conversation. As you see or think of other adverse events or are concerned about potential harm to a patient please report it through the Reportable Event System (QCMS). Near misses and adverse events are windows that we can all use to improve the safety of care we deliver. We can only address the issues if we know and talk about them openly.”
51
BAY OF PLENTY DISTRICT HEALTH BOARD
Page 5 of 12
Appendix 5: Sample Communication – Prior to planned visit
[insert date]
Dear all
XXXX ward has been scheduled for a Quality and Patient Safety Walk-round on the dd/mm/yyyy from XX:XX am to XX:XX am.
XXXX (Senior Manager) will be accompanied by XXXX Plus any other member
The aim of the walk-round is to allow the senior management team to learn about safety issues on the unit/team that are of concern to staff or patients.
They will ask questions to which there are no right or wrong answers. The senior team would like to use the visit as an opportunity to speak to all staff of any grade or profession. Please inform staff members of the walk-round and their opportunity to engage in the process. The senior managers would also welcome the opportunity to speak with patients if possible, at the start of the visit, and would therefore appreciate it if you could kindly arrange this on the day (if appropriate).
If you have any queries or require further clarification, please contact me via email or contact details below.
Attached is a leaflet, which explains the purpose and process of the visit. You may wish to bring it to the attention of all your team to help them understand the purpose of the visit. A notice is also attached.
Many thanks and kind regards,
52
BAY OF PLENTY DISTRICT HEALTH BOARD
Page 6 of 12
Appendix 6: Sample Walk-round Leaflet
Quality and Patient Safety Walk-rounds What is the aim of the Walk-round? The aims in introducing Quality and Safety Walk-rounds are:
• Demonstrate senior managers’ commitment to quality and patient safety for patients, staff and the public;
• Increase staff engagement and develop a culture of open communication;
• Identify, acknowledge and share good practice;
• Support a proactive approach to minimising risk, timely reporting and feedback; and
• Strengthen commitment and accountability for quality and patient safety.
How do they fit in with the quality and patient safety programme? Our aim is to minimise harm – that is, we want to ensure that all preventable harm is eliminated and this will need the help of all members of staff and of patients and the public. Quality and Patient Safety Walk-rounds will assist in demonstrating our commitment to staff engagement, building relationships, trust and patient centred service quality and safety. Who is involved? You and a member of the senior management team will visit each area accompanied by a volunteer patient representative/advisor (where possible) as well as a Quality and Patient Safety representative and an administration support person to record key issues discussed. Where does the walk-round take place? It is useful for the walk-rounds to start with a tour of the unit/department and meeting with patients (where possible). It is better to focus on the walk-round rather than a formal meeting. The walk-round team and the staff can then meet and hold the discussions in any area that suits the local team. This may be in the patient areas or in a quiet room within the main clinical area.
What happens at the Walk-round? A member of the walk-round team will explain and introduce the process including the agreements for confidentiality and patient safety disclosures. Members of the visiting walk-round team will then ask some questions to start a dialogue. All members of staff are welcome to participate and are encouraged to respond and participate in the discussion. Issues that can be raised may include:
• Good practice and safety developments; • Your key patient safety concerns; • What can we do together to improve? • How does your local team operate? • Communication – within teams and with
patients; • How can the senior management team help?;
and • Incident reporting & safety culture in the
organisation. At the end of the process, we will agree the actions to be taken forward together to make the area safer for patients. We ask staff to think of an example of good practice and a patient safety experience that they have addressed and bring this to the meeting to share with us, e.g. patients not getting their medications on time, patients not being reviewed when required, etc. What will happen to the information we gather? Senior managers will respond to the local team within an agreed time frame, thanking all individuals for their participation and highlighting the main areas discussed actions agreed. References Frankel, A., Graydon-Baker, E., Neppl, C., Simmonds, T., Gustafson, M., and Gandhi, T. (2003) “Patient Safety Leadership Workarounds” Joint Commission Journal on Quality and Safety 29 (1):16-26 Leonard M, Frankel A, Simmonds T, Vega K.: Achieving (2004) Safe and Reliable Healthcare Strategies and Solutions. Chicago: Health Administration Press. For Information Contact: [Insert details]
53
BAY OF PLENTY DISTRICT HEALTH BOARD
Page 7 of 12
Appendix 7: Sample Preparation for the Senior Managers Leading the Quality and Patient Safety Walk-round
[insert date]
Dear All ,
The Quality and Patient Safety Walk-round visit which you are leading is scheduled to visit XXXX unit/team on dd/mm/yyyy from xx:xx am to xx:xx am.
Please find attached a sample question guide. This information serves as background material to assist you in preparing for the conversation with the unit/team. Following this rigidly, on the walk-round may distract from the flow of the discussion. An open dialogue is more effective.
The information you might consider reviewing, in existing reports, in preparation for visit might include:
• Relevant quality and performance indicators; • Unit/Department/team risk register; • Infection prevention and control issues; • Complaints/compliments; • Incidents/near misses; • Quality improvements; • Staffing complements/absenteeism; and • Health and safety issues.
If you require any further details or clarification about the visit, please do not hesitate to contact me.
Best wishes,
Attach the Action Plan report from the last walk-round (if relevant) and the Quality and Safety Walk-round Discussion Guide.
54
BAY OF PLENTY DISTRICT HEALTH BOARD
Page 8 of 12
Appendix 8: Sample Communication after the Quality and Safety Walk-round A copy of the draft Action Plan is circulated to all those present at the walk-round for comment and approval. All positive feedback and suggestions for improvements are also noted and these are included in the email sent to the team following the walk-round (see below).
In some instances, it can be useful to focus on a small number of high priority issues identified on a Quality and Patient Safety Walk-round.
A suggested email template is as below:
[insert date]
Dear XXXX,
Thank you for investing the time and participating in the Quality and Patient Safety Walk-round to XXXX unit/team on dd/mm/yyyy.
As agreed, please find attached a draft version of the action plan that highlights safety action points that together we will take forward with the intention of resolving or raising further awareness on the issue.
In addition, we would like to note the positive feedback we received during the visit:
1.
2.
3.
Suggestions for unit/team to consider as part of promoting further good practice are:
1.
2.
3.
If you wish to make any amendments to the attached report or to the comments above, I would be grateful if you could please let me know by XXX 20XX. The final action plan will then be emailed to all concerned to ensure agreed actions are taken forward.
Kind regards and many thanks
It is good practice to distribute the draft action plan within an agreed time frame.
55
BAY OF PLENTY DISTRICT HEALTH BOARD
Page 9 of 12
Appendix 9: Sample Final communication after the Quality and Safety Walk-round The final action plan is circulated to all participants in the walk-round within an agreed timeframe. An example email template is as below:
[insert date]
Dear All,
Thank you for participating in the Quality and Patient Safety Walk-round to XXXX unit/department/team on dd/mm/yyyy. Further to my email (dated XXX) please find attached the final action plan that takes account of your comments and highlights the agreed priority issues that will be taken forward.
Again, we would like to note the positive feedback we received during the visit:
1.
2.
3.
Suggestions for unit/team to consider as part of promoting further good practice are:
1.
2.
3.
Our agreed time scale for addressing the issues is dd/mm/yyyy. Please keep me briefed on the progress to enable me to update the Quality and Safety Walk-round database.
Thank you.
Kind regards,
The named person for coordinating the Quality and Safety Walk-rounds takes responsibility for following up progress on the action plans as the deadlines approach. Progress on all other issues are normally captured at the next walk-round visit for that particular area (or as agreed by the executive/senior management team).
56
BAY OF PLENTY DISTRICT HEALTH BOARD
Page 1 of 12
Appendix 10: Sample Quality and Safety Walk-round Action Plan Template TOPIC ISSUE OR CONCERN
RAISED WHAT HAS ALREADY BEEN DONE TO ADDRESS ISSUE
ACTION TO BE TAKEN FOLLOWING WALK_ROUND
PERSON RESPONSIBLE
DUE DATE
Areas: Incident Reporting; Communication; Environment; Equipment; Process; Teamwork; Prevention and control of HCAI; Continuing Professional Development; Leadership.
FEEDBACK SUGGESTIONS Areas: Incident Reporting; Communication; Environment; Equipment; Process; Teamwork; Prevention and control of HCAI; Continuing Professional Development; Leadership
57
Updated 20/3/2014
Bay of Plenty Hospitals Advisory Committee Work Plan 2014
Month Activity Documentation Source
January • No meeting February • Monthly COO Report
• General Manager Property Services Report
• COO • GMPS
March • No Meeting April • Focus Topic: Quality & Safety
Top Five Productivity Gains 2013-14 SUBMITTED TO: Bay of Plenty Hospital Advisory Committee 2 July 2014 Prepared by: Trevor Richardson, Decision Support Manager, Provider Arm Endorsed by: Helen Mason, Chief Operating Officer BACKGROUND: During the 2013-14 financial year BOPDHB Provider Arm achieved a number of efficiency gains. The top five based on total impact are highlighted in this paper During the year high growth in acute demand has been one of our key challenges. The graphs below show ED attendance growth and associated inpatient discharge growth.
Although acute demand has been higher, our significant reduction in ALOS has resulted in less overnight inpatient beds being used than four years ago. The quantitative impact is 10 less beds on average in Tauranga and 7 less in Whakatane.
ALOS reductions saved 4,000 bed days @ $500 each totalling $2m compared to prior year. In addition to the savings attained, the cost of building the next inpatient bed floor at Tauranga has been safely delayed, pushing the $5m cost further into the future. Some key contributing factors to ALOS reductions have been:
• Full implementation and maintenance of the Stroke Unit in Health in Aging • Implementation of the new model of medicine • Focus on discharge barriers which still has further potential • ERAS and other elective pathway developments • CCDM focus • CIRCA programme of projects
2. Six Hour Target Tauranga Hospital Financial year-to-date 2013-14 six hour target result at Tauranga Hospital has improved from 86% to 89%. This 5% improvement in performance has been made with the challenge of an 8.2% growth in attendances. This improvement is a significant efficiency gain for the Tauranga
10
20
30
40
50
60
70
Whakatane Hospital Bed Usage Med/Surg/Paeds/ICU
2010
2011
2012
2013
201450
100
150
200
250
300
TGA Hospital Bed Usage Med/Surg/Paeds/ICU/CCU/HIA
2010
2011
2012
2013
2014
1.00
1.20
1.40
1.60
1.80
2.00
2.20
LOS / CWD Electives excludes daycase & maternity
2006 2007 2008 2009 2010
2011 2012 2013 2014
3.00
3.20
3.40
3.60
3.80
4.00
4.20
4.40
4.60
4.80
LOS / CWD Acute & Arr excluding daycase & maternity
2006 2007 2008 2009 2010
2011 2012 2013 2014
60
public with the average arrival time to discharge reducing from 234 minutes in 2012-13 to 222 minutes in 2013-14 for the 35,000 Health Target qualifying Tauranga ED attendances.
3. Bed Days ATR The Stroke Unit locating in the HIA ward at Tauranga and the clinical staff focus on patient outcomes has seen some reduction in MOH funded bed days but an increase in ACC funded bed days. The impact of this is to bring more revenue into the BOPDHB. As can be seen in the graphs the ALOS for health of older persons has reduced. The reduction is from 20 days average to 17 days average YTD to the end of May 2014.
4. Operating Expense Reduction Although we have experienced significantly higher inpatient volumes our operating expenses excluding salary and wages have remained the same as last financial year (until Waka opening). Total YTD spend on clinical supplies and outsourced services are $69.3m which is the same as 2 years ago. One single key operating expense efficiency gain has been blood product usage reductions. Below are usage reports for Intragam and Red Cells which together account for annual expenses of $3.2m. These reductions have been achieved through the Transfusion Committee which is a clinically lead group with the aim of enhancing patient safety and optimising blood product use. Several key initiatives lead to these reductions.
10
20
30
40
50
60
July
Augu
st
Sept
embe
r
Oct
ober
Nov
embe
r
Dece
mbe
r
Janu
ary
Febr
uary
Mar
ch
April
May
June July
Augu
st
Sept
embe
r
Oct
ober
Nov
embe
r
Dece
mbe
r
Janu
ary
Febr
uary
Mar
ch
April
May
2013 2014
Health of Older Person
Discharges Count
Average LOS Days
61
5. Non-Contact FSA Increases There has been an increase of 273 or 25% in non-contact FSAs year to date compared to 2012-13. This process enables a care plan to be provided by the specialist and is more efficient for the patients as they don’t need to take up half a day of their time to attend a clinic. DEFINITIONS USED: Term Definition ALOS Average length of stay
CWD Case weighted discharge ERAS Enhanced recovery after surgery DNW Did not wait CCDM Care capacity demand management FSA First Specialist Assessment HIA Health In Aging
62
Care Capacity Demand Management (CCDM) SUBMITTED TO: Bay of Plenty Hospital Advisory Committee 2 July 2014 Prepared by: Julie Robinson, Director of Nursing Endorsed by: Helen Mason, Chief Operating Officer RECOMMENDED RESOLUTION: That the committee note the contents of the presentation ATTACHMENTS: Presentation: Care Capacity Demand Management BACKGROUND: In September 2009 Bay of Plenty District Health Board was one of three DHBs invited by the Safe Staffing Healthy Workplaces (SSHW) Unit to become a demonstration site to test strategies and to develop tools to support change under the SSHW agenda. Four years ago I think most of us involved thought that the task was to develop a staffing formula for nursing. What we have come to understand and to encompass is that a staffing methodology and indeed a single professional group does not exist in isolation from the rest of the context in which it operates. The outcome has been the development of a unique programme that is being progressively implemented into DHBs. Entry into the programme requires that the DHB has a suitable data platform that includes a validated patient acuity system. This system provides one of the essential metrics that are required. There are currently 15 DHBs who have this capability through a software programme called TrendCare. This is possibly one of the most consistent IT programmes that exist across DHBs and provides us with real opportunities for cross DHB collaboration. CCDM is established under the bipartite industrial partnership model with governance and operational structures. The key components of the programme are:
• Forecasting • Mix & Match – an approach that enables a service to match its FTE, skill mix, schedule
and budget to demand • VRM - variance response management tools (variance boards, variance response
actions and standard operating procedures) • Monitoring metrics – critical to sustainability
63
ANALYSIS: The health sector demands quality, quantity, efficiency, workforce stability and fiscal restraint – simultaneously. There are inevitable and constant tensions between what are often competing priorities but this is the reality and the context from within which the CCDM programme has emerged. Organisations have to establish equilibrium within three competing performance boundaries: Financial failure, we cannot spend more than we have; unacceptable workload and unacceptable outcomes. One of our key learnings has been that to get gain in this context, we need to operate in a way that balances and prioritises all of these imperatives. One of the key challenges under CCDM has been showing the positive impacts given the timeframe for full implementation and to date no DHB has fully implemented all the components. BOPDHB has completed most with only two acute inpatient wards remaining to complete the Mix and Match process. The monitoring metrics were also agreed at a recent care capacity user group. Under the CCDM umbrella a reduction in the variance between nursing hours required and nursing hours provided has shown a positive trend at Tauranga. Constant scrutiny at the daily operations centre meetings and the acute patient flow projects under the CCDM work streams has seen a reduction in length of stay and throughput increased. Also of note is the reduction in the use of casual registered nurses since CCDM began. This can be attributed to the work on variance responses and the redeployment of staff from areas of less to need to areas of greater need. As a balancing measure sick leave rates have remained relatively stable over this timeframe.
64
26/06/2014
1
CARE Capacity Demand Management
better for patients better for staff better use of the health resource
Julie Robinson ‐ Director of Nursing
2005‐2006Safe Staffing Healthy Workplaces Committee of Inquiry RecommendationsDescription of the goalsNo road map to achieve the changes
2007‐mid 2009Establishment of SSHW Unit by Minister of Health (3 years)Engagement with DHBs & NZNOFocus on escalation planning
Mid 2009‐end 2010Re‐assessment of sector statusThree demonstration sites establishedTrialling of tools and resourcesEvaluationEmergence of CCDM approach
2010‐2015On‐going commitment from DHBs & Health UnionsRoll‐out of CCDM to DHBsBroaden to multi‐disciplinary approachIntegrate with other sector activity‐productivity‐innovation‐collaboration‐quality‐shared information