Tazeen H. Jafar, M.D., M.P.H. Professor of Medicine Head, Section of Nephrology Department of Medicine and Community Health Sciences Aga Khan University, Karachi, Pakistan & Adjunct Faculty, Division of Nephrology Tufts Medical Center Boston, MA, US
Transcript
Tazeen H. Jafar, M.D., M.P.H.Professor of MedicineHead, Section of NephrologyDepartment of Medicine and Community Health SciencesAga Khan University, Karachi, Pakistan&Adjunct Faculty, Division of NephrologyTufts Medical CenterBoston, MA, US
ACE Inhibition in Progressive Renal Disease (AIPRD) Study Group Members of the AIPRD Study Group: Pietro Zucchelli, (Via P Palagi, Italy), Gavin Becker (Melbourne, Australia), Kym
Bannister (Adelaide, Australia), Paul Landais (Paris, France), Giuseppe Remuzzi (Bergamo, Italy), Piero Ruggenenti (Bergamo, Italy), Annelisa Perna (Bergamo, Italy), Annelise Kamper (Copenhagen, Denmark), Svend Strandgaard (Copenhagen, Denmark), Benno U. Ihle (Melbourne, Australia), Andres Himmelmann (Goteborg, Sweden), Lennart Hannson (Goteborg, Sweden), Jean-Pierre Grunfeld (Paris, France), Paul E de Jong (Groningen, Netherlands), Dick de Zeeuw (Groningen, Netherlands), Gabe G. Van Essen (Groningen, Netherlands), Alfred J. Apperloo (Groningen, Netherlands), Lamberto Oldrizzi (Verona, Italy), Carmelita. Marcantoni (Verona, Italy), Giuseppe Maschio (Verona, Italy), Ioannis Giatras, (Greece), Shahnaz Shahinfar (Westpoint, USA), Robert Toto (Dallas, USA), Barry M. Brenner (Boston, USA), Joseph Lau (Boston, USA), Nicolaos E. Madias (Boston, USA), Barbara Delano, (Brooklyn, USA), Tauqir Karim (Boston, USA), Ronald Perrone (Boston, USA), Christopher H. Schmid (Boston, USA), Tazeen H Jafar (Karachi, Pakistan and Boston, USA) and Andrew S. Levey (Boston, USA).
Funding: Dialysis Clinic, Inc. Paul Teschan Research Fund 1097-5 (Dr. Jafar), NEMC St. Elizabeth’s Hospital Clinical Research Fellowship, Boston, MA (Dr. Jafar), and an unrestricted grant from Merck Research Laboratories, West Point, NJ (Dr. Levey), Supported by grants from NIDDK RO1 DK53869A (Dr. Levey), AHCPR RO1 HS 10064 (Dr. Schmid),
Overview
AIPRD individual patient data meta-analysis (IPDMA) Main Objectives Methodology Results
Proteinuria as Surrogate During Treatment with ACE inhibitors
Benefit of ACE inhibitors independent of BP lowering effect could not be established in meta-analysis of group data
Giatras, I. et. al. Ann Intern Med 1997;127:337-345
Background-why AIPRD IPDMA?•Which antihypertensive agent to use?
AIRPD Individual Patient Data Meta- analysis 11 RCTS with 1860 patients with non-diabetic
kidney disease Anti-hypertensive regimens with ACE inhibitors vs. those
without ACE inhibitors on progression of kidney disease. Minimum follow-up of one year Database closed in 1999
Objectives:1) To determine whether antihypertensive regimens with
ACE inhibitors are superior to those without ACE inhibitors after accounting for patients’ baseline characteristics and change in BP during treatment.
2) To assess the relationship of BP with progression of kidney disease across a wide range of urine protein excretion.(Jafar, TH et. al. Ann Intern Med 2001; Jafar, TH et. al. Ann Intern Med 2003)
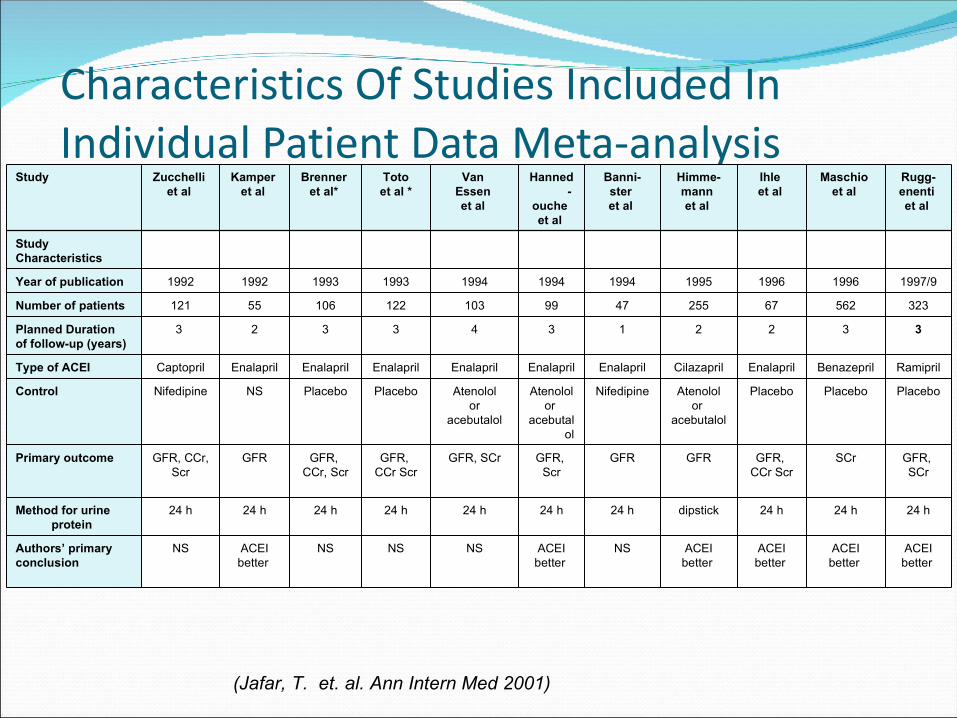
Characteristics Of Studies Included In Individual Patient Data Meta-analysis
Study Zucchelli et al
Kamper et al
Brenner et al*
Totoet al *
Van Essen et al
Hanned-
ouche et al
Banni-ster et al
Himme-mann et al
Ihle et al
Maschio et al
Rugg-enenti et al
StudyCharacteristics
Year of publication 1992 1992 1993 1993 1994 1994 1994 1995 1996 1996 1997/9
Number of patients 121 55 106 122 103 99 47 255 67 562 323
Planned Durationof follow-up (years)
3 2 3 3 4 3 1 2 2 3 3
Type of ACEI Captopril Enalapril Enalapril Enalapril Enalapril Enalapril Enalapril Cilazapril Enalapril Benazepril Ramipril
Control Nifedipine NS Placebo Placebo Atenololor
acebutalol
Atenololor
acebutalol
Nifedipine Atenololor
acebutalol
Placebo Placebo Placebo
Primary outcome GFR, CCr, Scr
GFR GFR, CCr, Scr
GFR, CCr Scr
GFR, SCr GFR, Scr
GFR GFR GFR, CCr Scr
SCr GFR, SCr
Method for urine protein
24 h 24 h 24 h 24 h 24 h 24 h 24 h dipstick 24 h 24 h 24 h
Authors’ primaryconclusion
NS ACEIbetter
NS NS NS ACEIbetter
NS ACEIbetter
ACEIbetter
ACEIbetter
ACEIbetter
(Jafar, T. et. al. Ann Intern Med 2001)
Methods Mean follow-up 2.2 years Visits=22,610 Primary Outcome (True Endpoints)
Composite outcome of doubling of baseline serum creatinine or onset of ESRD (true endpoint)
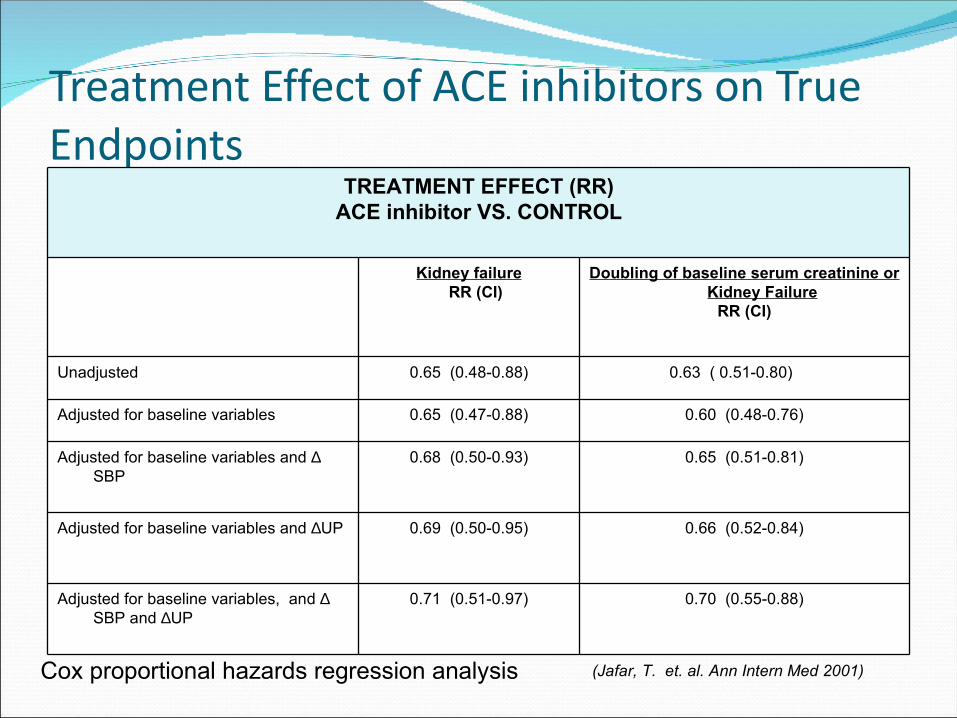
Onset of ESRD (true endpoint) Multivariable models adjusted for study centers Cox proportional hazards regression analysis Treatment effect (ACEI vs other antihypertensive agents) With and without adjustment for proteinuria (surrogate)
1) Change from baseline; 2) current level on treatment
Jafar TH et al. Annals Intern Med 2003
Definitions
Measures of ProteinuriaCollection: 24 hours urine specimens in 10 studies and dipstick
in oneAnalyte: Total Urinary Protein (in g/d)Analytical methods: Total protein –automated precipitation assays in
10, dipstick in one
Threshold: continuous. All values of urine protein <0.1 g/d converted to 0.1 g/d)
Outcomes Doubling of baseline serum creatinine or onset of kidney
failure Onset of kidney failure
Measures for validating proteinuria as surrogate endpoint in IPD-MA1) Assessed individual-level association
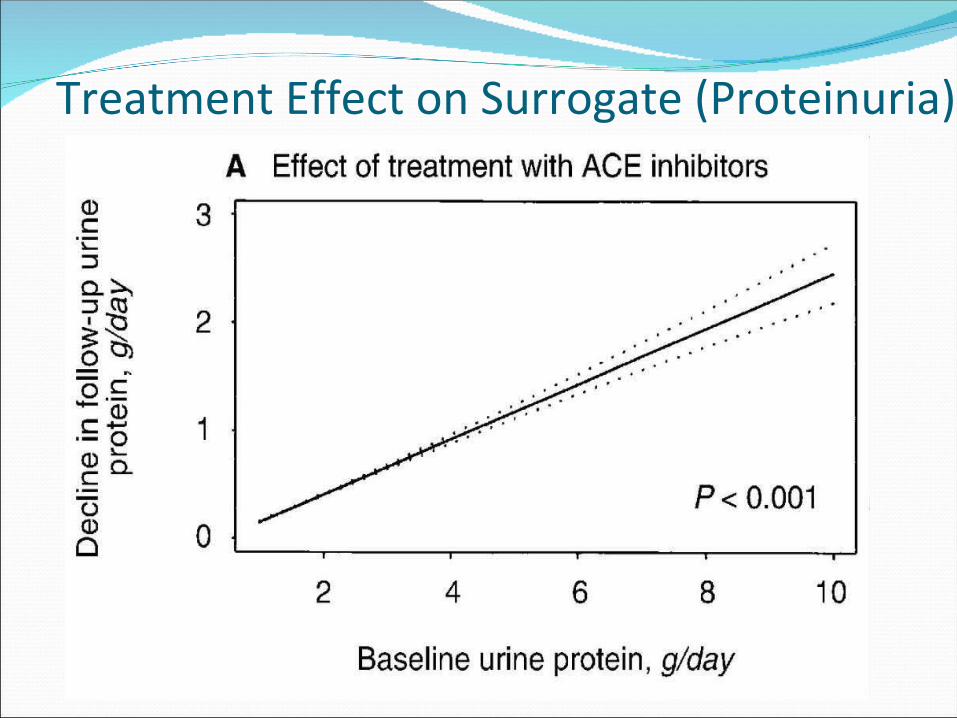
1) treatment affects the surrogate endpoint (UP)2) treatment affects the true endpoint (Doubling of
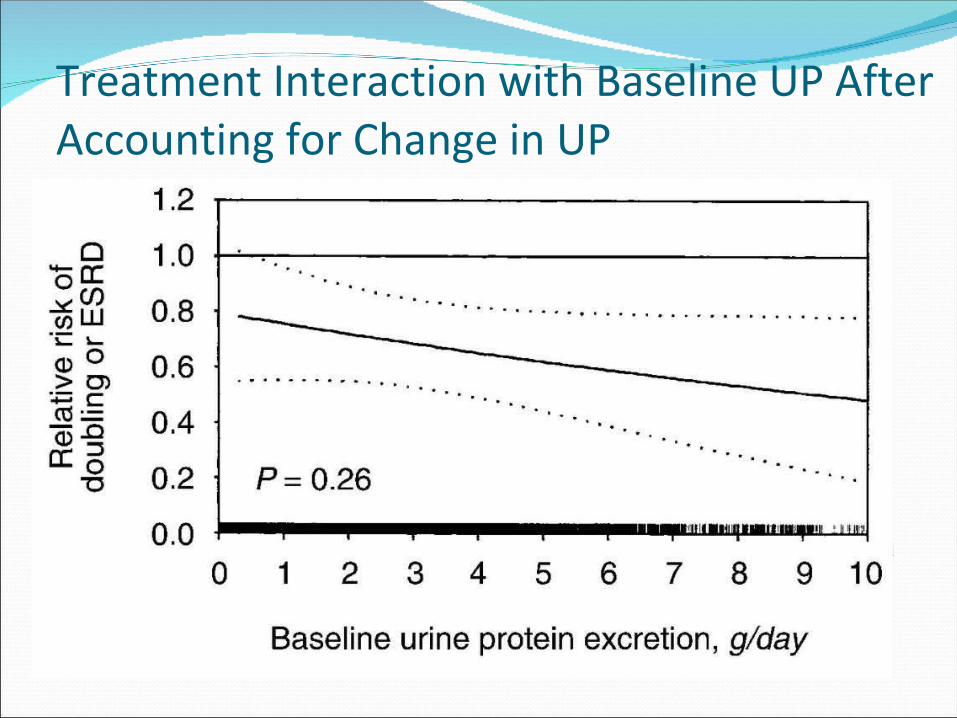
serum Creatinine/ onset of kidney failure) 3) “adjusted association”: association treatment and
true endpoint after accounting for treatment effect on surrogate and for center effect
Cause of Kidney Disease Glomerular diseases 32.9% Hypertensive nephrosclerosis 33.0% Tubulointerstitial diseases 11.8% PKD 7.6% Others 14.7%
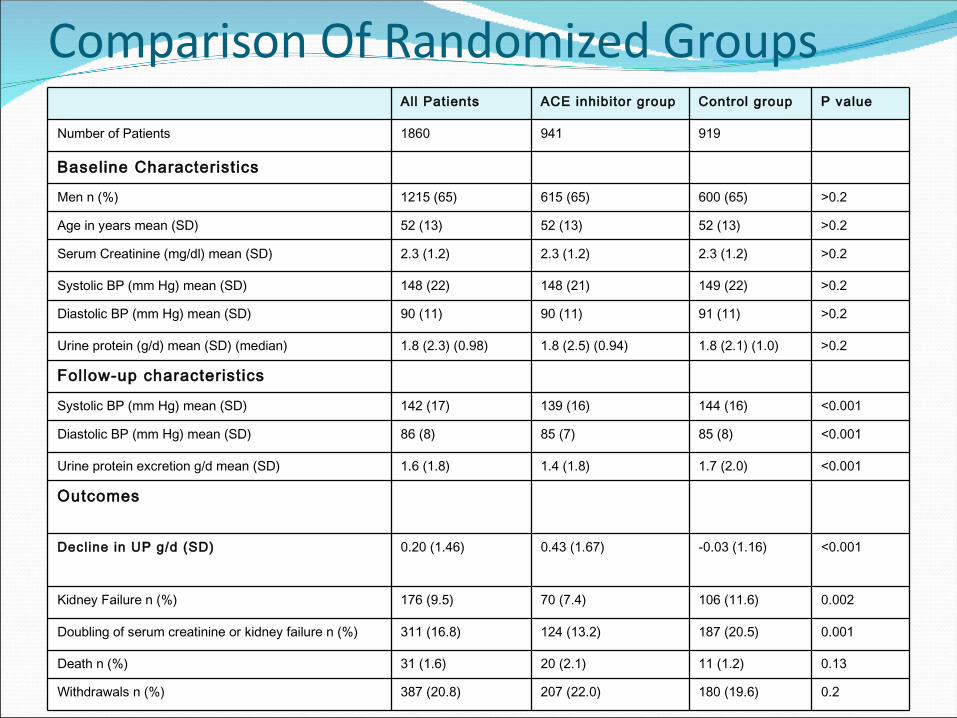
Comparison Of Randomized Groups
Outcomes
<0.001-0.03 (1.16)0.43 (1.67)0.20 (1.46)Decline in UP g/d (SD)
All Patients ACE inhibitor group Control group P value
Number of Patients 1860 941 919
Baseline Characteristics
Men n (%) 1215 (65) 615 (65) 600 (65) >0.2
Age in years mean (SD) 52 (13) 52 (13) 52 (13) >0.2
Decline in proteinuria (each 1 g/d decrease) 0.84 (0.80-0.87)
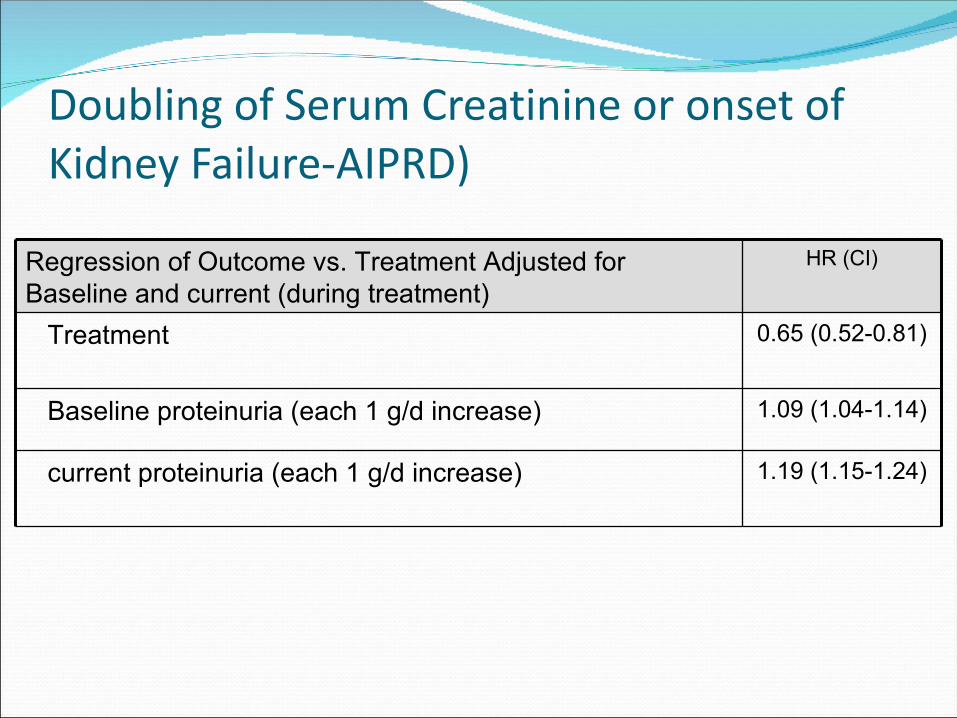
Note: If treatment is effective, HR for treatment will be <1.0. If proteinuria is a surrogate marker for treatment effect, HR for treatment effect will increase from <1.0 to closer to 1.0 in adjusted models.
Treatment Effect According to Current UP
Doubling of Serum Creatinine or onset of Kidney Failure-AIPRD)
Regression of Outcome vs. Treatment Adjusted for Baseline and current (during treatment)