45
An Hour of Autism: Diagnosis, Treatment, What we do and don’t know Jennifer Bogin, M.S.ed, BCBA Director Division of Autism Spectrum Services
| Date post: | 18-Dec-2015 |
| Category: |
Documents |
| Upload: | sheryl-turner |
| View: | 213 times |
| Download: | 0 times |

An Hour of Autism:Diagnosis, Treatment, What we
do and don’t know
Jennifer Bogin, M.S.ed, BCBADirector
Division of Autism Spectrum Services
Today we will talk about
Defining ASD
Core Symptoms/ Co-occurring Disorders
Identification of ASD
New Numbers/Prevalence
DSM-5
Treatment of ASD Applied Behavior Analysis (ABA) Relationship-Based Methods
Anything else??????

Defining:Autism Spectrum Disorder
1943 – Leo Kanner – Infantile autism
1944 – Hans Asperger
1960s – Separation from schizophrenia
1970s – Biology / genetic underpinnings
1980 – DSM-III – Pervasive Developmental Disorders
1987 – DSM-III-R - Autistic Disorder / PDD-NOS
1994 – DSM-IV – Asperger’s Disorder
2013- DSM-5- Autism Spectrum Disorder

Jenn’s Recipe for Autism Eruption*
The Nature of the Disability (if one considers it a disability)
Actual increase in incidence
Increased identification
Better treatments = Hope
Insurance coverage (for hope)
The Jenny McCarthy, Doug Flutie, factor
Trending now….
So of course it’s controversial..
We can (kind of) define who has it
We have (almost) no idea what causes it
We don’t know IF it is increasing
IF it is then we don’t know why
We can make it better (if you consider it a problem)

The nature of Autism Spectrum Disorder
Stayed tuned for more on DSM-5 later!

Core Symptom DomainsPLUS Associated Medical Features
Social Impairment
& Restricted Interests
Speech/Communication
Deficits
Obsessive Compulsive
Disorder
AUTISMSPECTRUM
DISORDERS
Language DisordersIntellectual Disabilities
ADHDSocial Anxiety
OCD
AggressionEpilepsy-EEG abnormalities
Motor problems: Apraxia
Immune Dysfunction
Gastro-intestinal Dysfunction
Sleep Disturbance
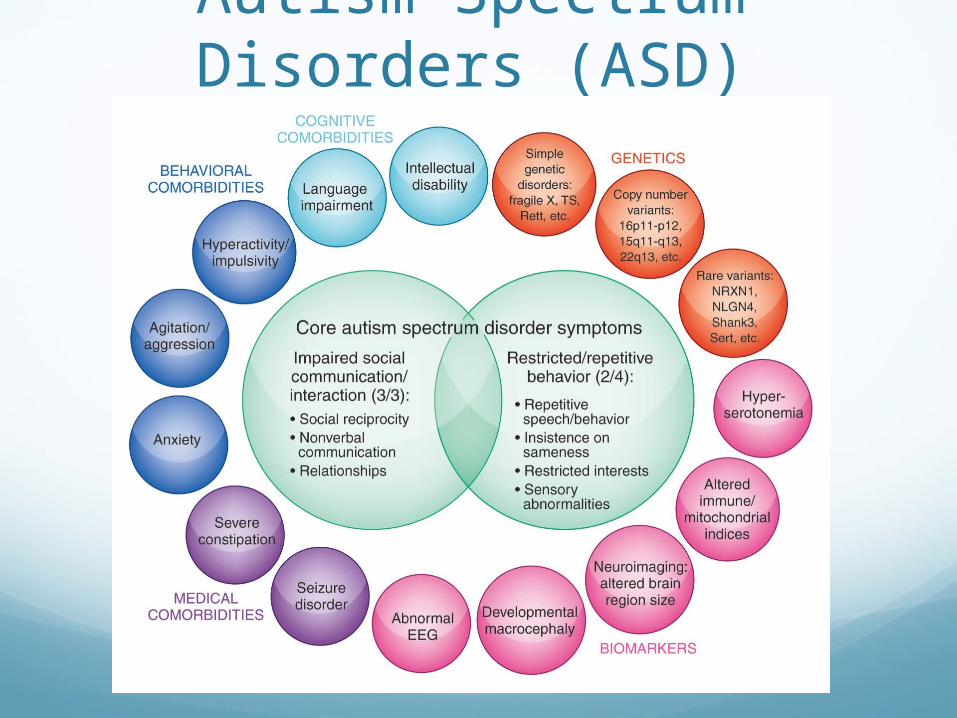
Autism Spectrum Disorders (ASD)

First lets look at Identification…We were pretty good at picking up this guy… (Early Onset)
But now we’re picking up this one…. (Regression)
What are the implications?

Hot of the press…(March 27, 2014) – Today, the Centers for
Disease Control and Prevention (CDC) released new data on the prevalence of autism in
the United States. This surveillance study identified 1 in 68 children (1 in 42 boys and 1 in
189 girls) as having autism spectrum disorder (ASD).
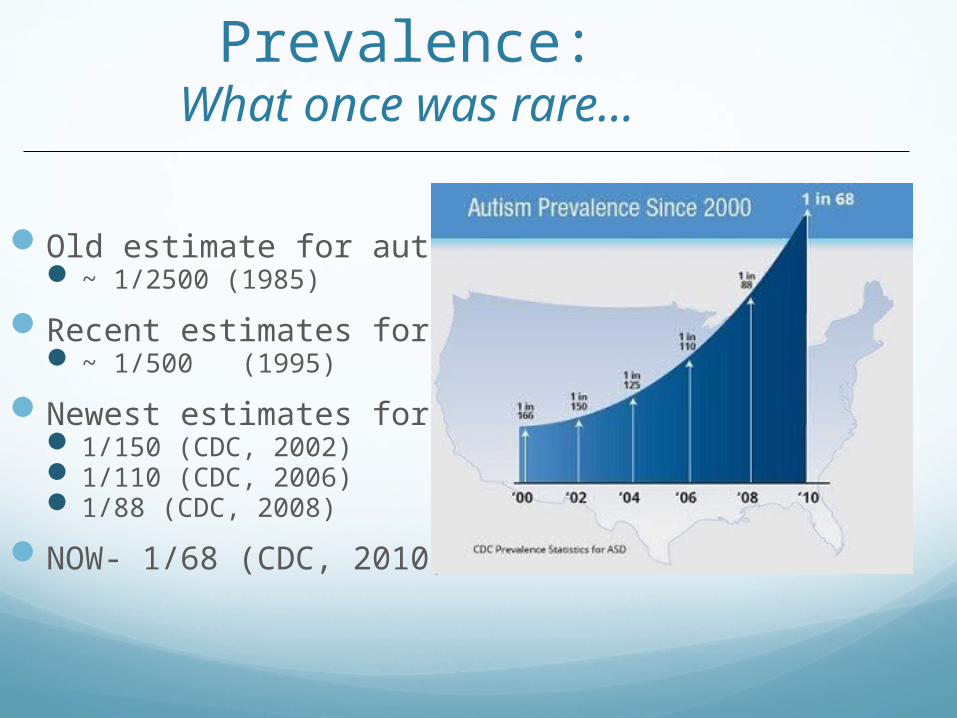
Prevalence:What once was rare…
Old estimate for autism: ~ 1/2500 (1985)
Recent estimates for autism: ~ 1/500 (1995)
Newest estimates for ASD: 1/150 (CDC, 2002) 1/110 (CDC, 2006) 1/88 (CDC, 2008)
NOW- 1/68 (CDC, 2010)

New diagnostic measuresAutism Diagnostic Interview (1989, 1994)Autism Diagnostic Observation Schedule
(1989, 2000)
Screening tools/algorithms/instruments in wide use:MCHAT / AAP guidelinesSCQSRS
Why are numbers increasing: Better tools?

Diagnostic changes Categories Broadening
Better tools and identification process
Awareness Mental health providers, pediatricians, schools Media, parents
Other factors: Previous underestimates
Methodology for obtaining epidemiological data
What else???
Why are numbers increasing: Lots of reasons?


DSM-5Distinctions can be difficult both within the spectrum and across
other disorders
Autism Spectrum Disorder
Autistic D/O Asperger’s PDD-NOS
DSM-5Deficits in social communication (all 3):
Deficits in nonverbal communicationDeficits in social and emotional reciprocity Deficits in maintaining relationships
Restricted, repetitive patterns of behavior, interest, and activities (2)Stereotyped motor or verbal behaviorUnusual sensory behaviorExcessive adherence to routines and ritualized bhxRestricted, fixated interests
Symptoms present in early childhood (manifest when social demands exceed capabilities)
Neurodevelopmental UnderpinningsCore and associated vulnerabilities
likely have complex neurogenetic
origins:
Evidence:
Maleness (3:1 to 4:1)
Familial loading/risk: MZ twins: 58-96% DZ twins: 0-31% Sibs: 5-20%
(18.7% - Ozonoff et al., Pediatrics, 2011) 1% - Population

299.00 Autism Spectrum Disorder
A. Persistent deficits in social communication and social interaction across multiple contexts, as manifested by the following, currently or by history (examples are illustrative, not exhaustive; see text):
1. Deficits in social- ‐emotional reciprocity, ranging, for example, from abnormal social approach and failure of normal back- ‐and- ‐forth conversation; to reduced sharing of interests, emotions, or affect; to failure to initiate or respond to social interactions.
2. Deficits in nonverbal communicative behaviors used for social interaction, ranging, for example, from poorly integrated- ‐ verbal and nonverbal communication; to abnormalities in eye contact and body- ‐language or deficits in understanding and use of gestures, to a total lack of facial expression and nonverbal communication.
3. Deficits in developing, maintaining, and understanding relationships, ranging, for example, from difficulties adjusting behavior to suit various social contexts; to difficulties in sharing imaginative play or in making friends; to absence of interest in peers

299.00 Autism Spectrum Disorder
B. Restricted, repetitive patterns of behavior, interests, or activities, as manifested by at least two of the following, currently or by history (examples are illustrative, not exhaustive; see text):
1. Stereotyped or repetitive motor movements, or use of objects, or speech (e.g., simple motor stereotypies, lining up toys or flipping objects, echolalia, idiosyncratic phrases).
2. Insistence on sameness, inflexible adherence to routines, or ritualized patterns of verbal or nonverbal behavior (e.g., extreme distress at small changes, difficulties with transitions, rigid thinking patterns, greeting rituals, need to take same route or eat same food every day).
3. Highly restricted, fixated interests that are abnormal in intensity or focus (e.g., strong attachment to or preoccupation with unusual objects, excessively circumscribed or perseverative interests).
4. Hyper- ‐or hypo- ‐reactivity to sensory input or unusual interest in sensory aspects of environment (e.g., apparent indifference to pain/temperature, adverse response to specific sounds or textures, excessive smelling or touching of objects, fascination with lights or spinning objects).
299.00 Autism Spectrum Disorder
C. Symptoms must be present in early developmental period (but may not become fully manifest until social demands exceed limited capacities, or may be masked by learned strategies in later life).
D. Symptoms cause clinically significant impairment in social, occupational, or other important areas of current functioning.
E. These disturbances are not better explained by intellectual disability (intellectual developmental disorder) or global developmental delay. Intellectual disability and autism spectrum disorder frequently co- ‐occur; to make comorbid diagnoses of autism spectrum disorder and intellectual disability, social communication should be below that expected for general developmental level.
(important) Note:Individuals with a well-established DSM-IV diagnosis of autistic disorder, Asperger’s
disorder, or pervasive developmental disorder not otherwise specified should be
given the diagnosis of autism spectrum disorder. Individuals who have marked
deficits in social communication, but whose symptoms do not otherwise need criteria for autism spectrum disorder, should be
evaluated for social (pragmatic) communication disorder
The Importance of Effective Early Diagnosis and Treatment:
A public health perspective
Earlier diagnosis = More intervention opportunities
More opportunities = Optimal intervention benefitCore features: social communication / atypical behaviorsCognitive and adaptive functioning Fully integrated classroom placements Potentially promoting optimal adaptive independence Potentially reducing considerable lifetime cost and service system
demands associated with ASD and related care

From Concern to Effective Treatment
Effective Treatment
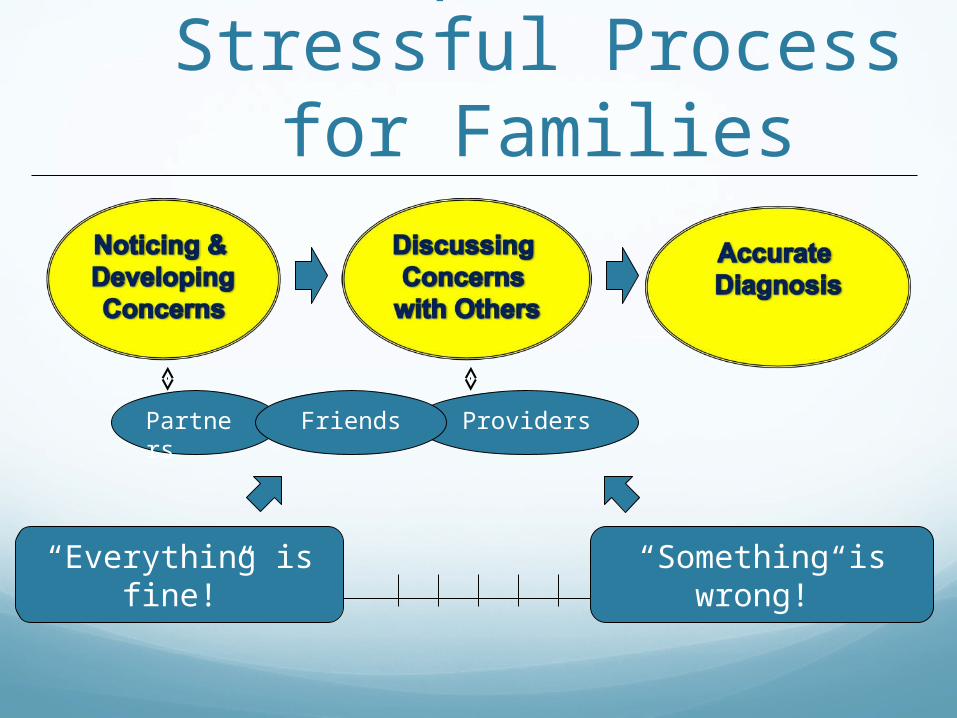
Complex and Stressful Process for Families
Partners ProvidersFriends
“Everything is fine!” “Something is wrong!”

Partners PediatricianProvidersFriends
Social Media
CDCGoogleDAN AAP TV BlogosphereAutism Speaks
Science in Context
Costs of ASDRecent estimates of annual incremental costs
(see Amendah et al., 2011) $2,100 – $11,200 medical expenditures $13,000 educational costs $40,000-$60,000 intensive behavioral tx $60,000-$128,000 residential costs for adults w/ASD Productivity loss, overall lifetime costs, quantification of impact of early
intervention programs
Most quoted total lifetime costs = $3.2 million (Ganz, 2007)
Mean medical expenditures for Medicaid enrolled children 6 times greater for children with ASD: $10,709 to $1,816 (Peacock, 2012)

Historical PerspectiveNot far removed from an “untreatable” era
Rutter (1970):<2% functioning “normally”60% requiring institutional placement/support
Lovaas (1987): UCLA Young Autism Project Intensive ABA = 9 / 19 (47%) “recovered” or
“normal functioning”A breakthrough with major methodological
concerns

Over short periods of time findings related to:language acquisitionnonverbal communicationreduction in challenging behaviorssocial skills
Over longer periods of time:cognitive ability / IQeducational success
Suggestions of medications and complementary agents:primarily associated symptomsclaims of broad effects
Two decades of research findings:

Why Are We Doing This?Our fundamental assumption…
Accurate early identification of a specific common neurodevelopmental disorder in
childhood should help us connect to specific intervention and treatment options that
optimize functioning for children and families

Promise of ‘recovery’ (AKA HOPE) Actual randomized controlled studies
‘optimal outcome’ studies
www.talkaboutcuringautism.org
http://www.newautism.com/ (how I learned to cure autism)
The ‘Bonding Hormone’ That Might Cure Autism
Jenny McCarthy: My son's recovery from autism
If Autism is your question, The Son-Rise Program is your answer!
http://www.vitamindcouncil.org
Can Clay Baths Cure Autism? Yes!
http://www.earthclinic.com/CURES/autism.html


Treatments and Therapies 78,300,000 results (0.08 seconds) Auditory Integration
Sensory Integration
ABA
Discrete Trial Training
Lovaas/UCLA Intervention
Early Start Denver Model
Holding Therapy
Dolphin Assisted Therapy
Facilitated Communication
Augmentative Communication
Vision Therapy
Vitamins
Hyperbaric Oxygen
Psychopharmacological treatments
Floortime
Music Therapy
Social Skills Training
Incidental Teaching
TEACCH
PECS
Pivotal Response Therapy
Son-Rise
RDI
Chelation
Diets
Drugs
Supplements

Evidence-Based Interventions*

Applied Behavior Analysis (ABA)
What is ABA?
How is it different from other approaches?
How is it done?
Baer, Wolf, & Risley (1968)
APPLIED—strives to produce rapid and clear benefit to problems of social importance;
BEHAVIORAL—uses objective and accurate measurement of the behavior of interest;
ANALYSIS—uses controlled (single-case) methods to understand the environmental variable(s) that influence an individual’s behavior.

Outcomes of ABA for Autism
0
5
10
15
20
25
30
35
0 5 10 15 20 25 30 35 40 45
Hours per Week of Treatment
Incr
ease
s in
IQ
Sco
res
r = .79p < .02
Cost-Benefit Analysis of Early,
Intensive ABA for AutismAverage lifetime cost for a person
with autism is over $4 million
Average cost of Early, Intensive ABA is $150,000 over about 3 years
Average lifetime savings from ABA Treatment is between $1.6 and $2.7 million

Examples of ABAEdward and “go find”
Small group instruction “hoping frogs”

Examples of Relationship-Based Methods
Early Start Denver Model ‘Paddy Feet’ Bubbles
Early Intensive Behavioral and Developmental Interventions (EIBDI)
Comprehensive (see Rogers and Vismara, 2008)Focus on several areas of functioning vs. skill specific
intervention
Draw from principles of Applied Behavior Analysis (ABA)Method and setting
ABA umbrella term for learning principles/techniquesTeach new behaviors, reduce challenging behaviors Systematic reinforcement
ABA is a term existing for decades prior to specific adoption within autism intervention literature

Early intensive behavioral and developmental interventions
UCLA/Lovaas model & variants: Intensive intervention (18-36 hr) utilizing operant conditioning,
emphasis on structure and discrete trial toward generalization of skills Variants of Early Intensive Behavioral Intervention (EIBI) Is this a category?
Comprehensive approaches for children under 2: ABA principles within a developmental and relational framework Early Start Denver Model (ESDM) / Early social communication
training : Range: Intensive intervention (15-20 hours) to lower levels
Parent-training: Pivotal Response Training, Social Pragmatic Intervention, More than
Words, etc.
Where does this leave us now?

Methodology is limiting our understandingof intervention impact / potential
Lack of current evidence does not equal lack of effect or potential effect of treatment
Some current and available ASD interventions do make a tremendous impact for some children
How do we best serve children in our backyards?

How do we choose and value treatments?Individualized intervention:
• What works for which children and why?• What is the meaningful social and functional impact?
• Range of outcomes to be expected ?• How do we value therapeutic changes?
A changing landscape:• Improved understanding of disorder• Improved study and improved interventions• Methodologically rigorous and meaningful investigation

Questions?

















