55
An Update in Robotics in Outpatient Rehab Kristen Black-Bain PT, DPT, NCS

An Update in Robotics in
Outpatient Rehab
Kristen Black-Bain PT, DPT, NCS

Objectives
• Be familiar with various robotic devices for
both upper and lower extremities.
• Be familiar with current research on
various robotic devices for both upper and
lower extremities.
• Learn about advances in exoskeleton
development
If a robot does “the
robot”, is it still
called “the robot”?
Or just dancing??

• Robotics in Rehab
– Mobility aids
– Manipulation aids
– Evaluation tools
– Therapeutic aids
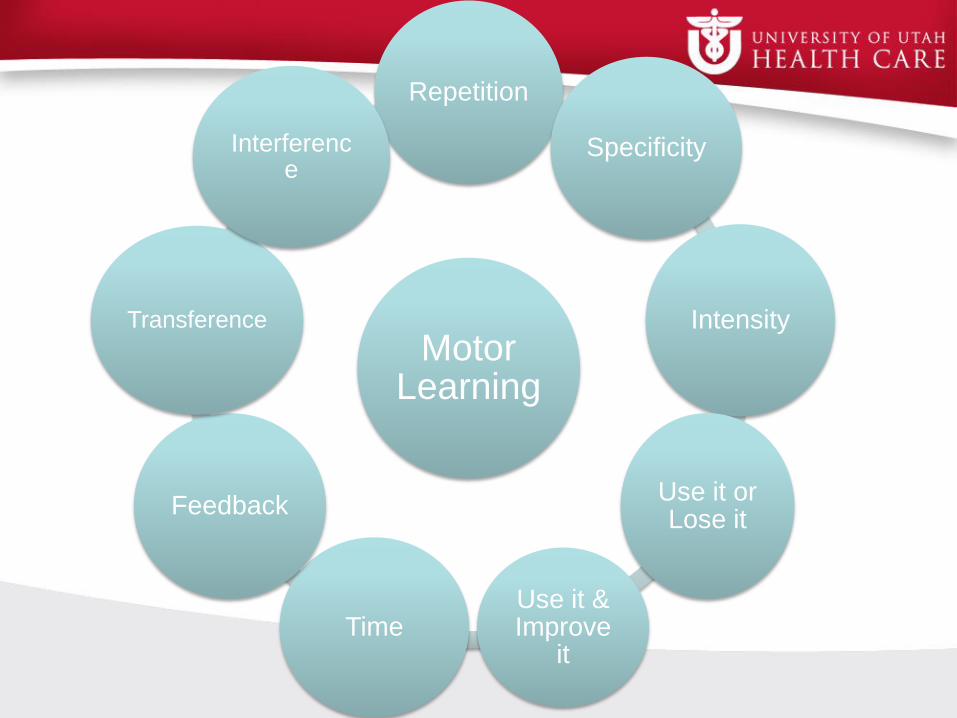
Motor Learning
Repetition
Specificity
Intensity
Use it or Lose it
Use it & Improve
itTime
Feedback
Transference
Interference

Robotics in Rehab
• Fewer therapists/staff
• Active participation with progression
• Reproducible
• Mental well being
Lower Extremity Robots

LE Robots
Alter G
Bionic Leg
G-EO
Lokomat Pro

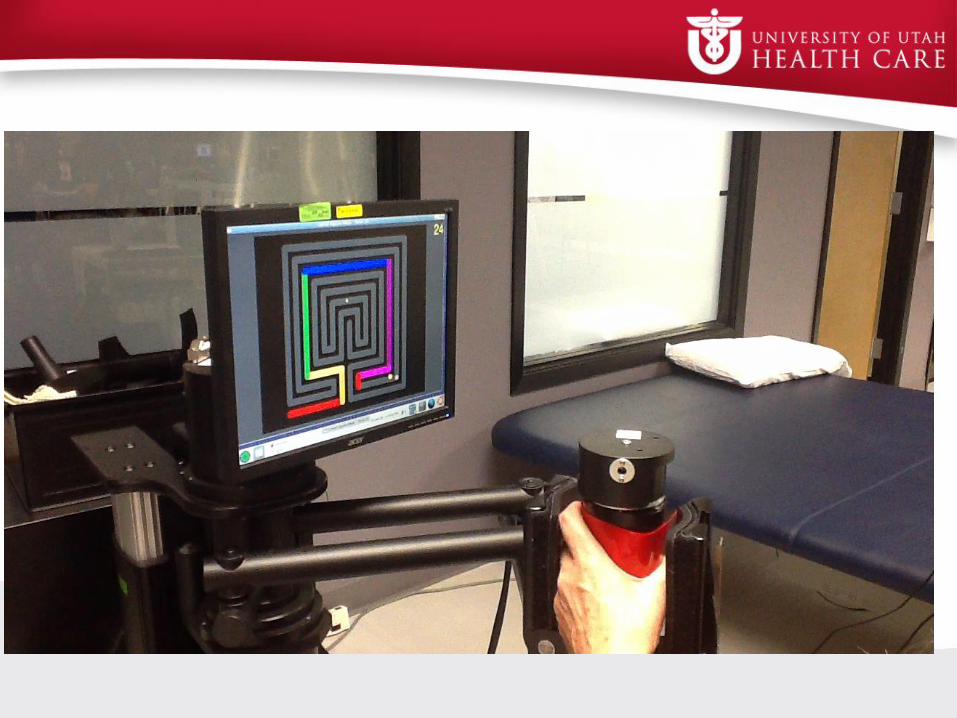
Upper Extremity Robots
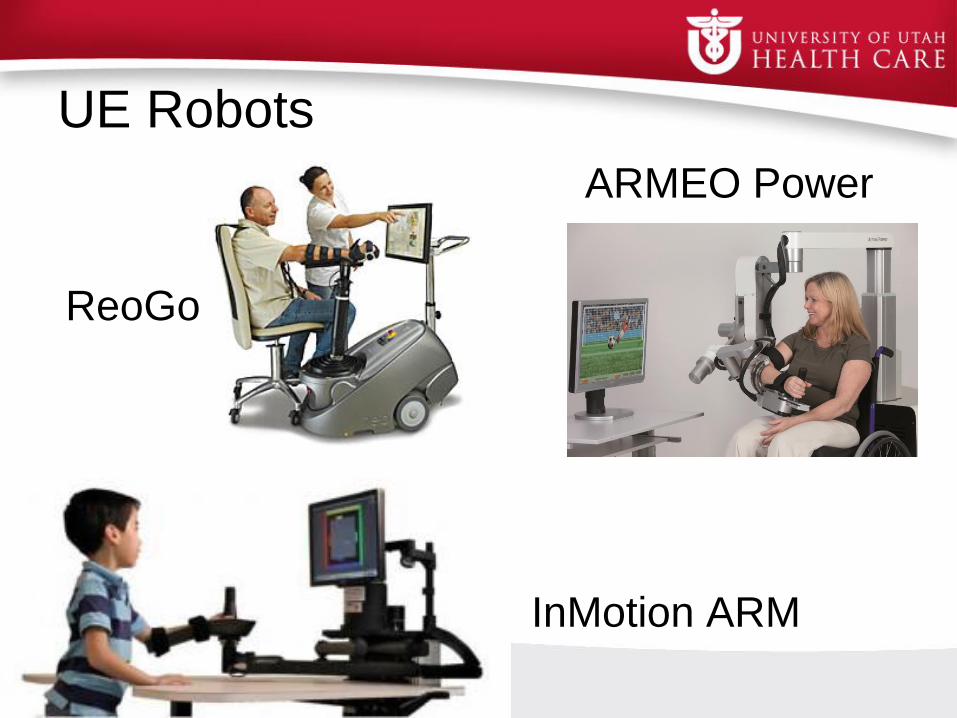
UE Robots
ARMEO Power
ReoGo
InMotion ARM

Research
• Veterans Administration/Department of Defense, regarding UE
robotics, “recommend robot-assisted movement therapy as an
adjunct to conventional therapy in patients with deficits in arm
function to improve motor skill” (Krebs, 2012).
• “American Heart Association suggests that robot-assisted therapy
for the UE has achieved Class I level of evidence for stroke care in
outpatient and chronic care setting… Class IIa for stroke care in
inpatient setting” (Krebs, 2012).
• Study of 10 chronic SCI (C4-C6) participating in 6 wk study
showed clinically significant improvements in aim and smoothness
of movement in UE kinematics (Cortes, 2013).

Research
• RCT; Subacute (30 + 7 days) stroke patients; showed significant
improvement in Fugl-Meyer, MAS, and PROM after robot-assisted
upper limb rehab tx (Sale, 2014).
– Control group performing standard therapy also showed
significant improvement in Fugl-Meyer but experimental group
had higher improvement
• Single-blind RCT; children with CP improved significantly in
manual dexterity assessed by Box and Block test compared with
control group (Gilliaux, 2015).
• Single-blind RCT; chronic stroke patients had significant
improvement in task-oriented arm training after six months
(Timmermans, 2014)

Device Function Cost Features
ARMEO Intelligent arm support in
3D workspace, 6
actuated DOF,
augmented feedback,
provides objective data
$190,000 Pediatric option,
more degrees of
freedom
Reo-Go 3D gyro mechanism;
performance feedback,
collects objective data
$85,000 Mobile/easy to
move; lock out
specific motions
InMotion 2 active DOF at
shoulder;
$110,000- ARM and
Hand.
Additional $90,000 for
InMotion Wrist
Optional InMotion
Hand and Wrist for
combined
coordination of
movement.
Pediatric option



Hybrid UE Robot Research
• MAHI-EXO II
– Upper extremity exoskeleton
– 5 degrees of freedom
– Hard stop at elbow
– Currently conducting validation studies
for patients with Stroke and SCI
MAHI-EXO II + BCI (Brain Computer Interface)
– Currently recruiting subacute and chronic
stroke participants
https://clinicaltrials.gov/ct2/show/NCT01948739
Photo courtesy of www.neurogadget.com

Lower Extremity Exoskeletons

Exoskeletons
ReWalk Ekso Rex

Ekso• Formerly called “E-Legs”
• Wearable bionic suit that enables user to stand and walk over
ground
• Battery powered motors move limbs in reciprocal gait pattern
• Progressing walking modes
– Training mode with audio feedback for appropriate weight shifting
• Variable assist
– Various settings that
allow range of passive
to actively assisted
stepping from user
• Bilateral Max Assist
• Adaptive Assist
• Fixed Assist Photo courtesy of www.prescouter.com

Research• Clinical trials out of Kessler showing positive results from training with
Ekso exoskeleton (presented at ASCIP 2012, 2014 conference by Gail
Forrest, PhD)
– Increased oxygen consumption, ventilation, and heart rate showing
potential cardiovascular benefit
– Increased muscle firing in lower leg muscles during Ekso assisted
walking
– Increase gait speed and decreased stance time on single limb with
increased training
– Increased loading on LEs

Research• Clinical trials out of Mount Sinai (presented at ASCIP 2014 by Allan
Kozlowski, PT)
– Ekso walking is safe (no adverse events occurred)
– Level of assistance varies
– HR, RPE, METs comparable to light exercise
– Secondary benefits: reports of improved pain, spasticity, posture,
sleep, and bowel function
– Psychosocial benefits


Rex Bionics
• Hands free, self supported device controlled by joystick
• Can be used by people with cervical injuries
as high as C-4
• Can navigate up/down stairs and ramps
• Rehab and personal units available (UK only)
• Fast adjustability
Update:
• Clinical trials starting in early 2015
• Goal is to secure pre-market notification, 501(k)
from FDA by end of second quarter of 2016
leading to at-home use late 2016. Photo courtesy of www.proactiveinvestors.co.uk


ReWalk• Stepping is controlled by wt shifting and subtle trunk movements that
trigger tilt sensors
• Adjustability for varying levels of user (beginner – advanced)
– Joint range, step speed, delay between steps, tilt angle, current
threshold
• Battery held in backpack
• Able to ascend/descend stairs
• Used with forearm crutches
• Mode is determined by watch
controller worn by user
Only FDA approved device in US for personal usePhoto courtesy of www.medicalplasticnews.com

Research
• 6 Chronic SCI volunteer participants with thoracic level (T5- T12)
complete injuries participated in average 13 training sessions did
not show any increase in pain or adverse effects (Esquenazi, 2012)
– One participant with chronic high-level neuropathic pain (VAS 8-9)
showed repeated improvement after training (VAS 4-6).
• In a nonrandomized single intervention trial, 12 subjects with
chronic thoracic level (T3-T12) motor complete SCI reported
positive emotional/psychological benefits on survey (Zeilig, 2012)
– 3/11 reported improved spasticity, 0/11 reported increase in pain, 5/11
reported improved bowel regulation

Research
• Improved bowel function in 5 motor complete SCI participating in
15-20 sessions of ReWalk exoskeleton training (Fineberg, 2012)
– Decreased average time of evacuation
– reduction of dependency for manual stimulation, laxatives, or stool
softeners
• Early data out of Bronx VA (Ann Spungen, presented at ASCIP
2014); 7 ReWalk users walking 1-2 hours 3 days a week
– Improved skill level (decreased assistance, varied terrain outdoors, community
mobility)
– potential positive lean tissue mass changes in users with lower motor partial
zones of preservation
– No changes in bone mineral density
– Loss of fat mass
– Report of significant improvement in bowel function
– Increased energy expenditure but sustainable
– Improved QOL

Case Report
• Female 27 years old; Chronic T-10 AIS-C SCI, 10 years post injury
• Goal: to walk around home with braces (KAFO/AFO)
• Previously attempted ambulation with braces and FWW
– Subjective report: required assistance, relied heavily on UEs
allowing only 5-10 ft of gait with FWW
• Measurements before ReWalk training
– TUG: 52 sec; wearing R KAFO and L AFO in parallel bars
– LE MMT
• R hip flex 4-/5 L hip flex 4+/5
• R hip ext 2-/5 L hip ext 3-/5
• R knee ext 3-/5 L knee ext 5/5
• R knee flex 2/5 L knee flex 3/5
– Pain: daily nerve pain in B LEs L > R, worst 9/10 on VAS

Case Report
• Intervention
– 2-3 days/ week X 6 weeks
• 15 sessions total; 11 ReWalk, 4 gait training with braces
started after first 3 weeks
• Measurements after 6 weeks
– TUG: 23.72 sec (52.36 sec)
– Ambulate 77 (5-10) ft with FWW
– LE MMT
• R hip flex 4-/5 (4-) L hip flex 4+/5 (4+)
• R hip ext 2+/5 (2-) L hip ext 3-/5 (3-)
• R knee ext 3/5 (3-) L knee ext 5/5
• R knee flex 2/5 (2) L knee flex 3+/5 (3)
• Pain: daily nerve pain in B LEs; worst 8/10 VAS (9/10)

“When using the ReWalk I could feel my
abs starting to work and I hadn’t felt that
before.”
“Using it definitely helped with my sitting
balance”.
“Using the ReWalk has helped my trunk to
get stronger with other things I do”.

Hybrid-Exoskeletons
Indego HAL Kinesis/H2

H2-Exo / Kinesis
• Exoskeleton developed by Technaid out of Spain
• Bilateral lower extremity equipped with active
actuators at knee hinges
– Passive elastic actuators at ankles
• EMS: PC controlled stimulator delivers
biphasic current to knee ext/flex
• Can manually trigger steps
• Wearer uses walker for UE support

Research
• Pilot study; 3 motor incomplete SCI using FES hybrid
exoskeleton
– able to complete 6 minutes of walking after one day (Del Ama,
May 2014)
– After only one week of training, improved gait measures (10m
and 6MWT), but also continued to improved one week after
intervention.
• HYPER project
– Recruiting for clinical trial: Subacute or chronic stroke patients
– https://clinicaltrials.gov/ct2/show/NCT02114450

H2-Exo

Cyberdyne HAL
• Hybrid-Assistive-Limb
• “World’s First Cyborg type robot that
interfaces man, machine, and information”
• Assistance triggered by EMG
from surface electrodes
• Single LE, Bilateral LE, or whole body
UE/LE combo
• Currently only in Japan and Germany
• Submitted application for FDA
clearance in U.S. Photo courtesy of www.cyberdyne.jp

Research
• After 16 training sessions, patients with various
neurological diagnoses (Stroke, SCI) improved gait
speed, number of steps, and cadence (Kubota, 2013).
• HAL was found to be safe when used for gait training in
acute stroke patients (Nilsson, 2014)
– All 7 participants improved gait measured by 10MWT


Indego
• Lightweight at only 27 lbs
• Breaks down to smaller pieces for easy travel/transportation
• Functional electrical stimulation component
• Adapts to user input with varying levels of
power provided
• Requires use of AFO to be worn with device
Photo courtesy of www.mdtmag.com

Indego
• Slim profile that allows sitting in most standard wheelchairs
• Wireless operation through app
on mobile device
• Single handed strapping
• Not yet approved by FDA
• Commercial release expected
in 2016 in US
Photos courtesy of www.indego.com


Research
• Single subject case study showed exoskeleton powered
locomotion to have faster gait speed and also reduced
exertion compared with KAFO use (Farris, 2013).
• Single subject case study with T10 complete SCI using
exoskeleton combined with FES showed 34% reduction
in electrical power required at hip joints during stance
phase of gait (Ha, 2012)

Research
• Preliminary data presented at ASCIP 2014
– Potential for multiple dxs (SCI, CVA, TBI, MS, etc)
– Easy to learn for staff and family/caregivers
– Self report of reduced spasticity during and up to 4 hrs after
– Reduced pain and time for bowel care
• Recruiting for multi center clinical trial
– https://clinicaltrials.gov/show/NCT02202538

Device Function Cost Availability
Ekso Can balance indep, Sit to
stand, gait, progressing
level of independence
settings
Rehab Unit: approx-
$150,000
Currently only
rehab unit
available.
Indigo E-stim, sit to stand, gait,
stair climbing
Projected estimate:
approx- $30,000
Expecting FDA
approval 2016
HAL,
Cyberdyne
Sit to stand, gait, upper
and lower limb
assistance,
Facility contract rental
agreement: $5000
initial then approx-
$1400-$1600 per mo
Japan and
Germany, has
applied for FDA
approval in US
ReWalk Sit to stand, gait,
direction change, stair
climbing
Rehab Unit: approx-
$85,000
Personal Unit:
projected approx-
$65,000
Currently rehab
unit available.
Available for
purchase. VA has
covered one P unit
Rex Bionics Sit to stand, gait, stairs,
ramps up/down, no
assistive device
Both rehab and
personal units:
$150,000
Rehab unit avail
worldwide;
Personal- UK

3D Printing
Photo courtesy of www.dezeen.com

MindWalker Project
Photo courtesy of www.damngeeky.com

Walk Again

Criteria for Exoskeleton use
• Healthy weight
• Range of motion within normal limits
• Orthopedically stable
• Upright tolerance
• Device specific requirements
Contraindications:
- fractures, uncontrolled spasticity, pregnancy, skin breakdown, DVT,
low blood pressure, psychiatric/cognitive issues, contractures

Good Physical Health is the Key!!

Considerations when choosing a device
• Patient population
• Cost
• How will it be used/ Reimbursement
• The company providing and manufacturing the device.
• Space/ceiling height in your facility

Motor Learning
Repetition
Specificity
Intensity
Use it or Lose it
Use it & Improve
itTime
Feedback
Transference
Interference
Be Creative !
Think outside the box!

REFERENCES:• Bishop L, Stein J, Wong CK. Robot-aided gait training in an individual with chronic spinal cord injury: a
case study. JNPT. 2012;36: (138-143).
• Byl NN. Mobility training using a bionic knee orthosis in patient in a post-stroke chronic state: a case
series. Journ of Medical case report. 2012; 6:216.
• Cortes M, et al. Improved motor performance in chronic spinal cord injury following upper-limb robotic
training. Neuro Rehabil. 2013; 33 (57-65).
• del-Ama AJ, Gil-Agudo A, Pons JL, Morena JC. Hybrid FES-robot cooperative control of ambulatory gait
rehabilitation exoskeleton. J Neuroeng Rehabil. 2014 Mar 4; 11:27.
• del-Ama AJ, Gil-Agudo A, Pons JL, Moreno JC. Hybrid gait training with an overground robot for people
with incomplete spinal cord injury: a pilot study. Front Hum Neurosci. 2014 May 13; 8:298.
• Esquenazi A, Packel A. Robotic-Assisted gait training and restoration. Am J Phys Med Rehabil. 2012; 91
(Suppl), 217-231.
• Esquenazi A, Talaty M, Packel A, Saulino M; The ReWalk powered exoskeleton to restore ambulatory
function to individuals with thoracic-level motor-complete spinal cord injury. Am Journ Phys Med Reh.
2012 Nov; 91: 11 (911-21).
• Farris R, et al. A preliminary assessment of legged mobility provided by a lower limb exoskeleton for
persons with paraplegia. IEEE Trans Neural Syst Rehabil Eng. 2013; 18.
• Fineberg DB, et al. Improvements in bowel function in paraplegics using ReWalk for overground
ambulation. Poster presentation. Academy of spinal cord injury professionals. Annual conference 2012.
• Fineberg DB, Asselin P, Harel NY, Agranova-Breyter I, Kornfeld SD, Bauman WA, Spungen AM. Vertical
ground reaction force-based analysis of powered exoskeleton-assisted walking in persons with motor-
complete paraplegia. Journ Spinal Cord Med. 2013, 36:4, 313-321.
• Gilliaux M, Renders A, Dispa D, Holvoet D, Sapin J, Dehez B, et al. Upper limb robot-assisted therapy in
cerebral palsy: a single-blind randomized controlled trial. Neurorehabil Neural Repair. 2015 Feb; 29(2):
183-92.
• Ha KH, Quintero HA, Farris RJ, Goldfarb M. Enhancing stance phase propulsion during level walking by
combining FES with a powered exoskeleton for persons with paraplegia. IEEE Eng Med Biol Soc. 2012;
2012:344-7.
• Herr H. Exoskeletons and orthoses: classification, design challenges and future directions. Journ of
NeuroEng and Rehab. 2009, 6:21.
• Hesse S, Werner C, Bardeleben A. Electromechanical gait training with functional electrical stimulation:
case studies in spinal cord injury. Spinal Cord. 2004.
• Hesse S, Waldner A, Tomelleri C. Innovative robot for the repetitive practice of floor walking and stair
climbing up and down in stroke patients. J Neuroeng Rehabil. 2010 Jun. 7:30.
• Hidler J, et al. Multicenter randomized clinical trial evaluating the effectiveness of the Lokomat in
subacute stroke. Neurorehabil Neural Repair. 2009; 23(1), 5-13.
• Hornby TG, et al. Enhanced gait-related improvements after therapist-versus robotic-assisted locomotor
training in subjects with chronic stroke: A randomized controlled study. Stroke. 2008; 39(6), 1768-92.
• Krebs HI, Hogan N. Robotic therapy: the tipping point. Am J Phys Med Rehabil. 2012 Nov. 91: 11 03,
(S290-S297).
• Kubota S, et al. Feasibility of rehabilitation training with a newly developed wearable robot for patients
with limited mobility. Arch Phys Med Rehabil. 2013 Jun. 94: 6 (1080-7).
• Mayr A, Kofler M, Qirbach E, et al. Prospective, blinded, randomized crossover study of gait
rehabilitation in stroke patients using the Lokomat gait orthosis. Neurorehabil Neural Repair. 2007;
21:307-14.
• McCabe J, Monkiewicz M, Holcomb J, Pundik S, Daly JJ; Comparison of Robotics, FES, and Motor
Learning Methods for Treatment of Persisten Upper Extremity Dusfunction after Stroke: a Randomized
Controlled Trial. Arch Phys Med Rehabil. 2014 Nove 15.
• Nilsson A, Vreede KS, Haglund V, Kawamoto H, Sankai Y, Borg J. Gait training early after stroke with a
new exoskeleton- the hybrid assistive limb: a study of safety and feasibility. J Neuroeng Rehabil. 2014
June 2; 11:92.
• Nooijen CF, et al. Gait quality is improved by locomotor training in idividuals with SCI regardless of
training approach. J Neuroeng Rehabil. 2009; 6:36.
• Norouzi-Gheidari N, et al. Effects of robot-assisted therapy on stroke rehabilitation in upper limbs:
systematic review and meta-analysis of the literature. JRRD. 2012; 49:4 (479-496).
• Sale P, et al. Robot-assisted walking training for individuals with Parkinson’s disease: a pilot randomized
controlled trial. BMC Neurol. 2013; 13: 50.
• Sale P, Franceschini M, Mazzoleni S, Palma E, Agosti M, Posteraro F. Effects of upper limb robot-
assisted therapy on motor recovery in subacute stroke patients. Journ Neuroeng and Rehabil. 2014,
11:104.
• Talaty M, Esquenazi A. Differentiating ability in users of the rewalk powered exoskeleton. IEEE Int Conf
Rehabil Robot. Jun, 2013; 1-5.
• Tefertiller C. et al. Efficacy of rehabilitation robotics for walking training in neurological disorders: A
review. Journ Rehabil Res & Dev. 2011; 48: 387-416.
• Timmermas AA, Lemmens RJ, Monfrance M, Geers RP, Bakx W, Seelen HA. Effects of task-oriented
robot training on arm function, activity, and quality of life in chronic stroke patients: a randomized
controlled trial. J Neuroeng Rehabil. 2014 Mar 31;11:45.
• Toyo Keizai. Cyberdyne Inc.- the robot suit obtains certification in Europe. Translated from Ueraburu
Tanmatsu mo Zokuzoku Tojo- Donaru Nihon no Denshibuhin. Weekly, Sept 2013: 54-57.
• Westlake KP, Patten C. Pilot study of Lokomat versus manual-assisted treadmill training for locomotor
recovery post-stroke. J Neuroeng Rehabil. 2009; 6:18.
• Wirz M, et al. Effectiveness of automated locomotor training in patients with chronic incomplete spinal
cord injury: a multicenter trial. Arch Phys Med Rehabil. 2005;86:4, 672-80.
• Wong CK, Bishop L, Stein J. A wearable robotic knee orthosis for gait training; a case-series of
hemiparetic stroke survivors. Prosthet Orthot Int. 2012;36(1):113-120.
• Zeilig G, et al. Safety and tolerance of the ReWalk exoskeleton suit for ambulation by people with
complete spinal cord injury: a pilot study. Journ of Spin Cord Med. 2012; 35:2.

















