20
Kinesiology of ankle joint 2016 Presented by : DR. ASER Mohamed kamal Physical therapist / cairo university DOCTOR OF EGYPTIAN TEAM OF HANDBALL
| Date post: | 13-Jan-2017 |
| Category: |
Health & Medicine |
| Upload: | egyptian-handball-federation |
| View: | 86 times |
| Download: | 2 times |

Kinesiology of ankle
joint
2016
Presented by :
DR. ASER Mohamed kamal
Physical therapist / cairo university
DOCTOR OF EGYPTIAN TEAM OF HANDBALL

ANKLE JOINT
Ankle-FOOT COMPLEX
The ankle-foot complex is structurally analogues to the wrist-hand complex of
the upper extremity.
The ankle-foot complex must meet the stability and mobility demands.
Stability demands-
1. Providing a stable base of support for the body in a variety of weight bearing
postures without undue muscular activity and energy expenditure.
2. Acting as a lever for effective push-off during gait.
Mobility demands-
1. Dampening of rotations imposed by more proximal joints of LL.
2. Being flexible enough as a shock absorber
3. Permitting the foot to conform to the changing and varied terrain on which foot
is placed.
The ankle and foot meet its requirements
through
28 bones
25 joints.
These include:
1. proximal and distal tibiofibular joints
2. Talo-crural or ankle joint
3. Talocalcaneal or subtalar joint
4. Talonavicular joint
5. Calcaneocuboid joint
6. 5 tarso-metatarsal joints
7. 5 metatarso-phalangeal joints
8. 9 inter-phalangeal joints
The bones of the foot are traditionally
divided into 3 functional segments :
• HIND OR REAR FOOT-posterior
segment composed of talus and
calcaneus
• MID FOOT-middle segment composed
of navicular ,cuboid, 3 cuneiforms
• FOREFOOT-anterior segment composed of metatarsals and phalanges.

ANKLE JOINT
The term ankle specifically refers to :
• Talocrural joint-The formation of the mortise (a hole)
by the medial malleoli (Tibia) and lateral malleoli
(fibula) with the talus lying in between them makes
up the talocrural joint.
• The ankle is a synovial Hinge joint with joint capsule
and associated ligaments.
• It is generally considered to have a single oblique axis
with 1°of freedom.
PROXIMAL ARTICULAR STRUCTURE
• The proximal segment of ankle is composed of concave surface of distal tibia
and of tibial and fibular malleoli.
• The structure of distal tibia and the two malleoli is referred to as a MORITSE.
• The mortise of the ankle is adjustable, relying on the proximal and distal
tibio-fibular joints.
PROXIMAL TIBIO-FIBULAR JOINT
• It is a plane synovial joint formed by articulation of
head of fibula with the postero-lateral aspect of
tibia.
• Although facets are flat, a slight convexity of tibial
facet and slight concavity of fibula is predominant.
• Each proximal tibiofibular joint is surrounded by a
joint capsule that is reinforced by anterior and
posterior tibiofibular ligaments.
DISTAL TIBIOFIBULAR JOINT
• It is a syndesmosis or fibrous union.
• It is in between the concave facet of tibia and convex facet of
fibula.
• Tibia and fibula do not come into contact with each other at
this point but are separated by fibro-adipose tissue.
• The ligaments of distal tibio-fibular joint are primarily
responsible for maintaining a stable mortise.
Tibia Fibula
<<<Talocrural joint Talus

Bony landmark:
Tibia: 1. Medial condyle – on proximal end of tibia, medial aspect. 2. Tibial tuberosity – on proximal end, anterior aspect just below patella. (insertion for quadriceps tendon) 3. Tibial spine – “Shin bone” - anterior ridge along tibia. 4. Medial malleolus – large protuberance on medial aspect of ankle. 5. Tibial plateau 6. Lateral condyle 7. Shaft Fibula: 1. Head – Move distally and posteriorly from lateral femoral condyle. 2. Lateral malleolus – Large protuberance on lateral aspect of ankle. 3. Shaft 4. Styloid process Tarsals: 1. Calcaneus – heel bone. 2. Naviculr tubercle – On medial border of foot, large bony prominence. 3. Head of the Talus– Just proximal to navicular tubercle, especially palpable in eversion. 4. Sustentaculum tali – Located between the head of the Talus and the medial malleolus.Feels like a small ridge. 5. Peroneal tubercle of the calcaneus – On lateral aspect of foot just distal to lateral malleolus. 6. Medial tubercle of calcaneus – lies on the medial plantar surface of the calcaneus (not usually sharp or distinct unless itis associated with a heel spur.

Ligaments (lateral)
Lateral ligament It consists of 3
bands
Anterior talofibular ligament
Posterior talofibular
ligament
Calcaneofibular ligament
Distal articular surface
TALUS
3 Articular Surfaces
• Larger lateral facet-triangular shaped
• Smaller medial facet-comma shaped
• Superior facet- TROCHLEAR
Ligaments (medial)
• Fibrous capsule
• Deltoid or medial ligament- strong triangular
Superficial part
Deep part
Superficial part-
Deep Part
It is also called as Anterior tibio-talar ligament.
Attached to the anterior part of medial surface of talus.
ANTERIOR TIBIONAVICULAR
MIDDLE TIBIOCALCANEAN
POSTERIOR TIBIOTALAR

Ankle joint function:
• The primary ankle motion of dorsi-flexion and plantar-flexion occurs around
an oblique axis that causes the foot to move across all 3 planes. AXIS
• In neutral position of the ankle, the joint axis passes approximately through
the fibular malleolus and the body of the talus and through or just below the
tibial malleolus and posteriorly.
• Supination = PF + Adduction + Inversion
• Pronation = DF + Abduction + Eversion
• The distal tibia is twisted laterally compared with its proximal
portion accounting for toe-out position of the foot in normal
standing.
• The axis of angle is considered to be rotated laterally 20°-30°
in the transverse plane and inclined 10° down on the lateral
side.
Talar
rotation(7°
med and 10°
lat rotation)
Abduction-
adduction
Transverse
plane
Vertical axis
Talar
tilt(5°)
Inversion-
eversion
Frontal
plane
Anteroposterior
axis
Dorsiflexion-
plantar flexion
Antero-
posterior plane
Frontal axis
ARTHROKINEMATICS
• The shape of the body of talus is complex.
• The trochlea is wider anteriorly than posteriorly.
• The lateral (fibular) facet is substantially larger than the medial (tibial) facet
and its surface is oriented slightly obliquely to that of medial facet.
• This resembles a truncated cone.
• This causes greater displacement of fibular malleolus on lateral facet of talus
than the tibial on medial facet.
• The greater excursion of the lateral malleollus results in the imposition of
motion on the fibula in several directions through the ankle ROM.
• This motion is found to be small in magnitude and variable in direction
among individuals and with different loading conditions.
• This is related to the orientation of the proximal tibiofibular facet,with more
mobility available in those facets that are more vertical.
• It may depend on the tibiofibular ligamentous elasticity.
Dorsiflexion
1. Tibialis anterior
2. Extensor digitorum longus
3. Peroneus longus
4. Peroneus brevis
5. peroneus tertius (usually very close to extensor digitorum longus and often
considered as part of this muscle)
6. extensor halluces Longus (deep to ext. Digitorum longus)
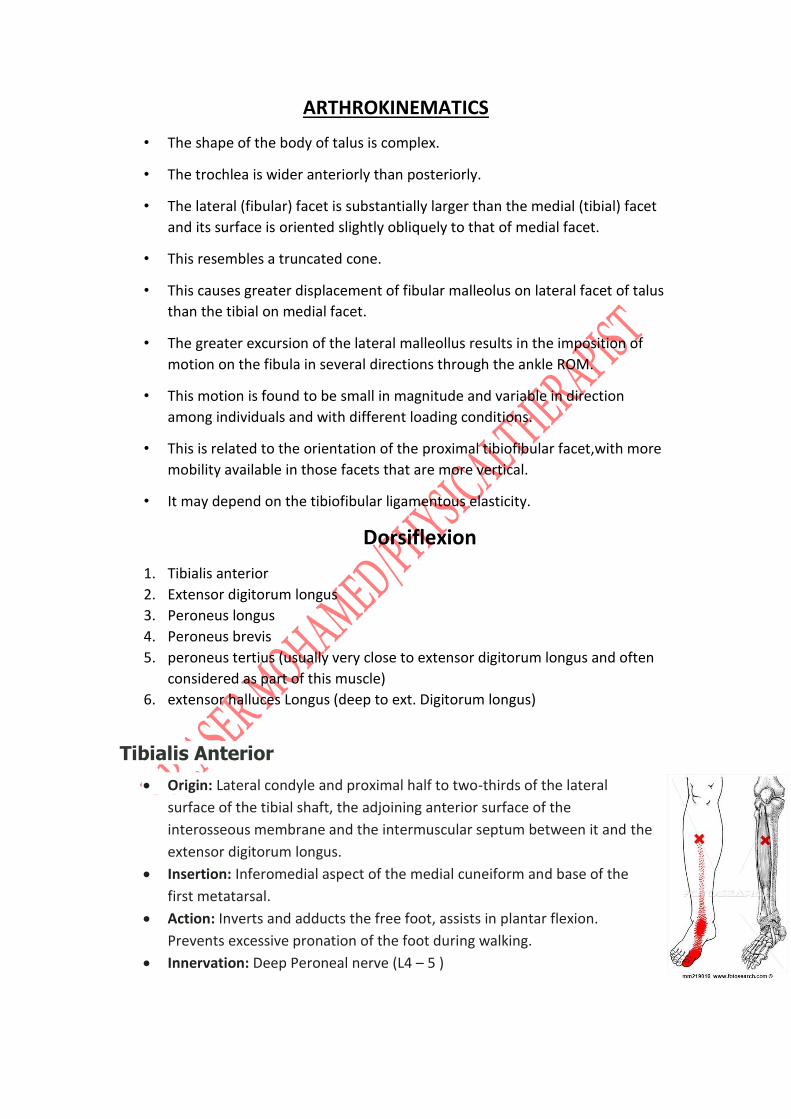
Tibialis Anterior
Origin: Lateral condyle and proximal half to two-thirds of the lateral
surface of the tibial shaft, the adjoining anterior surface of the
interosseous membrane and the intermuscular septum between it and the
extensor digitorum longus.
Insertion: Inferomedial aspect of the medial cuneiform and base of the
first metatarsal.
Action: Inverts and adducts the free foot, assists in plantar flexion.
Prevents excessive pronation of the foot during walking.
Innervation: Deep Peroneal nerve (L4 – 5 )

Extensor Digitorum Longus
Origin: Lateral condyle of the tibia, the proximal two-
thirds of the medial surface of the fibula, the adjacent
anterior surface of the interosseous membrane, the
anterior intermuscular septum, and the septum
between it and tibialis anterior.
Insertion: Divides into four slips and inserts at the base
of each of the lateral four proximal phalanges. Each
tendon then divides into three slips: an intermediate
slip which attaches to the base of the middle phalanx,
and two collateral slips which attach to the base of the
distal phalanx.
Action: Extension of the four lateral toes, assists with dorsiflexion of the foot
at the ankle.
Innervation: Deep Peroneal nerve (L5 – S1 )
Peroneus Longus Muscle
Origin: Head and proximal two-thirds of the lateral surface of the
fibula, and the anterior and posterior intermuscular septa of the
leg. Insertion: Passing behind the lateral malleolus, running obliquely
across the sole of the foot from lateral to medial, and ending on
the base of the first metatarsal and the medial cuneiform bones
Action: Eversion of the foot at the subtalar joint Innervation: Superficial Peroneal Nerve (L5, S1)
Peroneus Brevis Muscle
Origin: Distal two-thirds of the lateral surface of the
fibula, and the anterior and posterior intermuscular
septa
Insertion: Tubercle on the base of the lateral aspect of
the fifth metatarsal.
Action: Eversion of the foot at the subtalar joint
Innervation: Superficial Peroneal Nerve (L5, S1)

Peroneus Tertius
Origin: Distal third or more of the anterior surface of the fibula, the
adjoining anterior surface of the interosseous membrane and the
anterior intermuscular septum
Insertion: Inserts into the medial part of the dorsal surface of the base
of the fifth metatarsal and usually sends an expansion along the medial
border of the shaft the metatarsal
Action: Assists with dorsiflexion of the foot at the ankle
Innervation: Deep Peroneal (L5, S1)
Extensor Hallucis Longus Muscle
• Origin: Middle half of the medial surface of the fibula, medial to extensor digitorum longus, and adjacent anterior surface of the interosseous membrane
• Insertion: Dorsal aspect of the base of the distal phalanx of the great toe
• Action: Extension of the great toe, assists with dorsiflexion of the foot at the ankle.
• Innervation: Deep Peroneal nerve (L5 – S1-2 )
Plantar Flexors
1. Calf muscle (gastrocnemius and soleus)
2. Flexor hallucis longus
3. Flexor digitorum longus
4. Tibialis posterior
5. Plantaris
Gastrocnemius Muscle
Origin: Medial head: the depression at the upper and posterior part of the medial condyle of the femur and continuing behind the adductor tubercle to a slightly raised area on the popliteal surface of the femur, just above the medial condyle. Lateral head: area on the lateral surface of the lateral condyle of the femur and to the lower part of the corresponding supracondylar line.
Insertion: Receives the tendon of soleus on its deep surface to form the Achilles tendon to attach to the middle of three facets on the posterior surface of the calcaneus

Action: Plantarflexion of the foot at the ankle, assists with flexion of the leg at the knee.
Innervation: Tibial nerve S1-2
Soleus
Origin: Posterior surface of the head and proximal quarter of
the shaft of the fibula, spanning over to the soleal line and the
middle third of the medial border of the tibia, and a fibrous
band, which arches over the popliteal vessels and tibial nerve,
between the tibia and fibula
Insertion: Joins with the tendon of the gastrocnemius to form
the tendo calcaneus to attach to the middle of three facets on
the posterior surface of the calcaneus. The muscle is covered
proximally by gastrocnemius and is accessible on both sides.
Actions: Plantarflexion of the foot at the ankle
Innervation: Tibial nerve (S1 – 2 )
Flexor Hallucis Longus
Origin: Distal two-thirds of the posterior surfaces of
the fibula, the adjacent interosseus membrane, the
posterior intermuscular septum, and the lateral part of
the fascia covering tibialis posterior
Insertion: Plantar aspect of the base of the distal
phalanx of the great toe after traveling between the
two sesamoids associated with the first metatarsal
head.
Action: Flexion of the great toe, assists with
plantarflexion of the foot at the ankle.
Innervation: Tibial nerve (L5 – S1-2 )
Flexor Digitorum Longus
Origin: Posterior surface of the tibia, just below the soleal line to within
7 or 8 cm of the distal end of the bone, and to the medial part of the
fascia covering the tibialis posterior
Insertion: Plantar surfaces of the bases of the distal phalanges of the
four lateral toes
Action: Flexion of the four lateral toes, assists with plantarflexion of the
foot at the ankle.
Innervation: Tibial nerve (L5 – S1-2 )

Tibialis Posterior Origin: Proximal two-thirds of the posterior surfaces of the tibia and the
fibula and the interosseus membrane.
Insertion: Passing behind the medial malleolus to attach to the bones
that form the arch of the foot: the navicular, each cuneiform and cuboid
the calcaneus and metatarsals 2,3,4
Action: Inverts and adducts the free foot, assists in plantar flexion.
Prevents excessive pronation of the foot during walking.
Innervation: Tibial nerve (L4 – 5 )
Plantaris Origin: Lateral supracondylar ridge of the femur above the lateral head of
the gastrocnemius.
Insertion: Medial aspect of the posterior surface of the calcaneus, medial to
the Achilles tendon.
Action: Assists with flexion of the knee. Assist with plantarflexion of the foot
at the ankle
Innervation: Tibial Nerve (S1,2)
Invertors
A- Primary:
1- tibialis anterior
2- tibialis posterior
B- secondary :
1- extensor halluces Longus
2- Flexor digitorum longus
3- Flexor hallucis longus
Evertors
A- Primary:
1- Peroneus longus
2- Peroneus brevis
B- secondary :
1- peroneus tertius
2- Extensor digitorum long
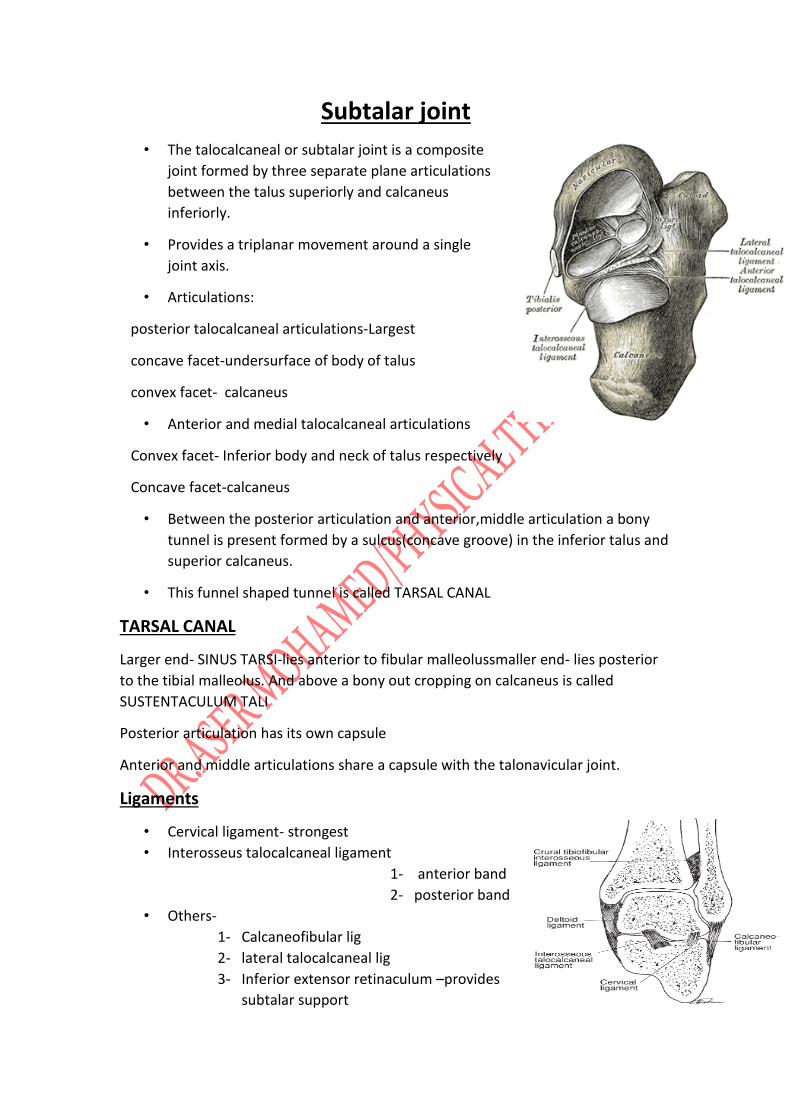
Subtalar joint
• The talocalcaneal or subtalar joint is a composite
joint formed by three separate plane articulations
between the talus superiorly and calcaneus
inferiorly.
• Provides a triplanar movement around a single
joint axis.
• Articulations:
posterior talocalcaneal articulations-Largest
concave facet-undersurface of body of talus
convex facet- calcaneus
• Anterior and medial talocalcaneal articulations
Convex facet- Inferior body and neck of talus respectively
Concave facet-calcaneus
• Between the posterior articulation and anterior,middle articulation a bony
tunnel is present formed by a sulcus(concave groove) in the inferior talus and
superior calcaneus.
• This funnel shaped tunnel is called TARSAL CANAL
TARSAL CANAL
Larger end- SINUS TARSI-lies anterior to fibular malleolussmaller end- lies posterior
to the tibial malleolus. And above a bony out cropping on calcaneus is called
SUSTENTACULUM TALI
Posterior articulation has its own capsule
Anterior and middle articulations share a capsule with the talonavicular joint.
Ligaments
• Cervical ligament- strongest
• Interosseus talocalcaneal ligament
1- anterior band
2- posterior band
• Others-
1- Calcaneofibular lig
2- lateral talocalcaneal lig
3- Inferior extensor retinaculum –provides
subtalar support
4- Cervical,interosseus,collaterals-talocalcaneal stability
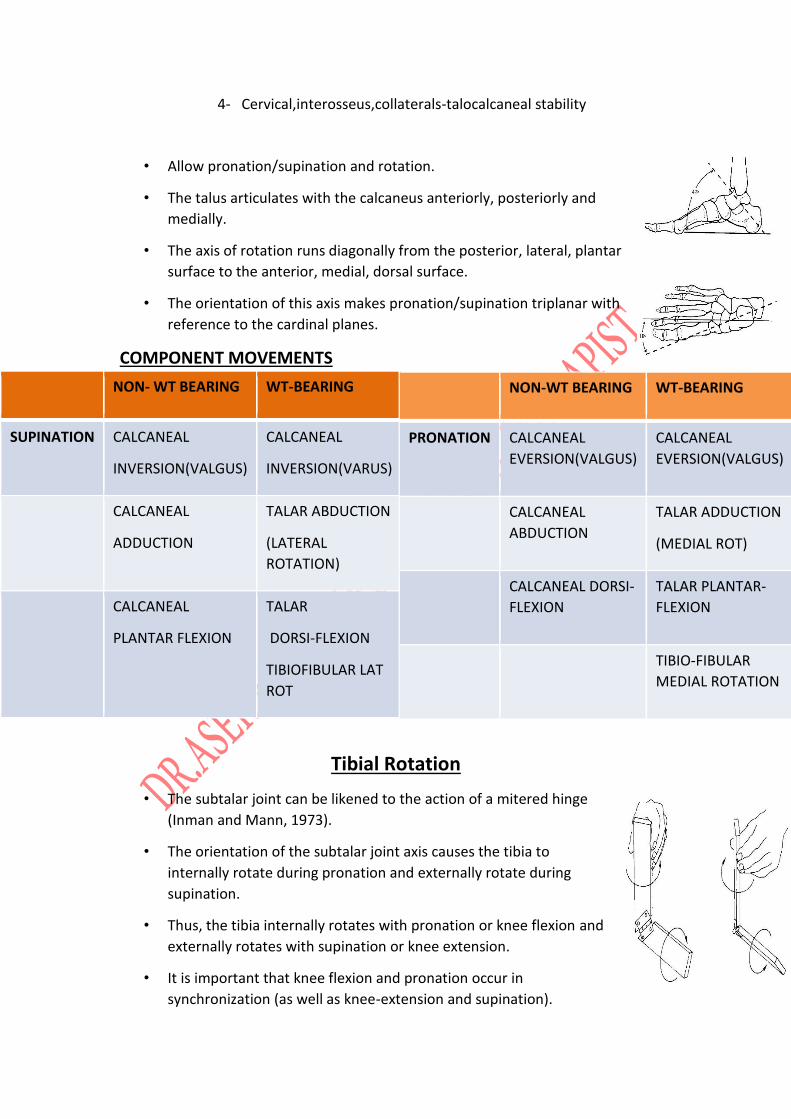
• Allow pronation/supination and rotation.
• The talus articulates with the calcaneus anteriorly, posteriorly and
medially.
• The axis of rotation runs diagonally from the posterior, lateral, plantar
surface to the anterior, medial, dorsal surface.
• The orientation of this axis makes pronation/supination triplanar with
reference to the cardinal planes.
COMPONENT MOVEMENTS
Tibial Rotation
• The subtalar joint can be likened to the action of a mitered hinge
(Inman and Mann, 1973).
• The orientation of the subtalar joint axis causes the tibia to
internally rotate during pronation and externally rotate during
supination.
• Thus, the tibia internally rotates with pronation or knee flexion and
externally rotates with supination or knee extension.
• It is important that knee flexion and pronation occur in
synchronization (as well as knee-extension and supination).
NON- WT BEARING WT-BEARING
SUPINATION CALCANEAL
INVERSION(VALGUS)
CALCANEAL
INVERSION(VARUS)
CALCANEAL
ADDUCTION
TALAR ABDUCTION
(LATERAL
ROTATION)
CALCANEAL
PLANTAR FLEXION
TALAR
DORSI-FLEXION
TIBIOFIBULAR LAT
ROT
NON-WT BEARING WT-BEARING
PRONATION CALCANEAL
EVERSION(VALGUS)
CALCANEAL
EVERSION(VALGUS)
CALCANEAL
ABDUCTION
TALAR ADDUCTION
(MEDIAL ROT)
CALCANEAL DORSI-
FLEXION
TALAR PLANTAR-
FLEXION
TIBIO-FIBULAR
MEDIAL ROTATION

• CLOSED PACKED POSITION:- FULL SUPINATION
• POSITION OF RELATIVE MOBILITY: – PRONATION
Transverse tarsal joint
• The transverse tarsal joint, also called the midtarsal or Chopart joint
It is a compound joint formed by the talonavicular and calcaneocuboid
joints .
• The two joints together present an S-shaped joint line that transects
the foot horizontally, dividing the hindfoot from the midfoot and
forefoot.
• The navicular and the cuboid bones are considered, immobile in the
weight-bearing foot.
Talonavicular joint
• The proximal portion of the talonavicular articulation is formed by the
anterior portion of the head of the talus, and the distal portion of the
articulation, by the concave posterior aspect of the navicular bone.
• A single joint capsule encompasses the talonavicular joint facets and the
anterior and medial facets of the subtalar joint.
Ligaments
• Inferior aspect of the joint capsule-plantar
calcaneo-navicular lig/spring lig
• Medially- deltoid lig
• Laterally-bifurcate lig

Calcaneo-cuboid joint
• The calcaneo-cuboid joint is formed proximally by the anterior calcaneus and
distally by the posterior cuboid bone
• The calcaneocuboid articulation has its own capsule that is reinforced by
several important ligaments.
The capsule is reinforced
• Laterally - lateral band of the bifurcate ligament (also known as the
calcaneocuboid ligament)
• Dorsally –dorsal calcaneocuboid ligament,
• Inferiorly -plantar calcaneocuboid (short plantar) and the long plantar
ligaments
Midtarsal Joint
• During pronation, the axes of these two joints are
parallel, this unlocks the joint and creates a
hypermobile foot that can absorb shock.
• During supination the axes are not parallel and this
joint becomes locked allowing efficient transmission
of forces.
• Actually consists of two joints: the calcaneocuboid
on the lateral side and the talonavicular on the
medial side.
Tarsal transverse joint axis
• The transverse joint is considered to have two axis around which the talus
and calcaneus moves on the relatively fixed naviculo-cubiod unit.
1- LONGUTUDINAL AXIS
2- OBLIQUE AXIS
Longitudinal axis-
• Motion around this axis is triplanar producing supinaion /pronation with
coupled components similar to those seen in subtalar joint.
• It approaches a true A-P axis producing inversion and eversion component
predominate.

Oblique axis
• This triplanar axis also provides supination/pronation with coupled
component movements of the talus and calcaneus segments moving
together on the navicular and cuboid bones.
• The dorsiflexion/plantarflexion and abduction/adduction components
predominate over inversion/eversion motions.
• Motions about the longitudinal and oblique axes are difficult to separate and
quantify.
• The longitudinal axis of the transverse tarsal joint
• Inclined 15° superiorly from the transverse plane
• Inclined 9° medially from the sagittal plane.
Oblique axis
• This triplanar axis also provides supination/pronation with
coupled component movements of the talus and calcaneus
segments moving together on the navicular and cuboid bones.
• The dorsiflexion/plantarflexion and abduction/adduction
components predominate over inversion/eversion motions.
• Motions about the longitudinal and oblique axes are difficult to
separate and quantify.
• The oblique axis of the transverse tarsal joint .
• Inclined 57° from the sagittal plane
• Inclined 52°superiorly from the transverse plane.
15°
9°
57°
52°

TRANSVERSE TARSAL JOINT FUNCTION
• Any weight-bearing subtalar motion includes talar abduction/adduction-
dorsiflexion/plantarflexion that also causes motion at the talonavicular
joint
• calcaneal inversion/eversion that causes motion at the calcaneocuboid joint.
• As the subtalar joint supinates, its linkage to the transverse tarsal joint causes
both the talonavicular joint and the calcaneocuboid joint to begin to supinate
also.(CLOSE PACKED POSITION)
• When the subtalar joint is pronated and loose-packed, the transverse tarsal
joint is also mobile and LOOSE PACKED .
• The transverse tarsal joint is the transitional link between the hindfoot and
the forefoot, serving to
(1)add to the supination/pronation range of the subtalar joint and
(2) compensate the forefoot for hindfoot
position.
• Weight-Bearing Hindfoot Pronation and Transverse Tarsal Joint Motion
In the weight-bearing position, medial rotation of the tibia
for example-pivoting on a fixed foot
• Weight-Bearing Hindfoot Supination and
Transverse Tarsal Joint Motion
• A lateral rotatory force on the leg will create
• subtalar supination in the weight-bearing subtalar joint with a relative
pronation of the transverse tarsal joint (opposite motion of the forefoot
segment) to maintain appropriate
• weight-bearing on a level surface Supination of the subtalar joint, however,
can proceed to only a certain point before the transverse
• tarsal joint also begins to supinate.

PRONATION
With pronation occurring at the subtalar joint through medial rotation of the
leg, the transverse tarsal joint is free to
(A) supinate slightly to maintain the relatively fixed position of the forefoot
segment;
(B) pronate slightly as occurs in normal standing; or
(C) supinate substantially to maintain appropriate weight-bearing of the forefoot
segment on uneven terrain
SUPINATION
With supination occurring at the subtalar joint through lateral rotation of the
leg, the transverse tarsal joint has limited ability to pronate to maintain the
relatively fixed position of the forefoot segment
(A) will begin to supinate with a greater range of subtalarsupination and
lateral rotation of the leg

(B) or will fully supinate along with a fully supinated subtalar joint and
maximal lateral rotation of the superimposed leg .
TARSOMETATARSAL JOINTS
• The tarsometatarsal TMT joints are plane synovial joints formed by the distal
row of tarsal bones (posteriorly) and the bases of the metatarsals.
• LIGAMENT
Deep transverse metatarsal ligament
• This spans the heads of the metatarsals on the plantar surface and is similar
to that found in the hand.
• Contribute to stability of proximal located TMT joints by preventing excessive
motion and splaying of metatarsal heads.
Axis
• A ray is defined as a functional unit formed by a metatarsal and (for the first
through third rays) its associated cuneiform bone.
• The cuneiform bones are included as parts of the movement units of the
TMT rays because of the small and relatively insignificant amount of motion
occuring at the cuneonavicular joints.
• The axis of the first ray is inclined in such as way that dorsiflexion of the first
ray also includes inversion and adduction, whereas plantarflexion is
accompanied by eversion and abduction.
• The abduction/adduction components normally are minimal.
• Movements of the fifth ray around its axis are more restricted and occur
with the opposite arrangement of components.
• Dorsiflexion is accompanied by eversion and abduction, and
plantarflexion is accompanied
*by inversion and adduction.
• The axis for the third ray nearly coincides with a coronal axis; the
predominant motion, therefore, is dorsiflexion/plantarflexion.
• The axes for the second and fourth rays were not determined
FUNCTION
• In weightbearing,the TMT joints function primarily to augment the function
of the transverse tarsal joint; that is, the TMT joints attempt to regulate

position of the metatarsals and phalanges (the forefoot) in relation to the
weight-bearing surface.
SUPINATION TWIST
• When the hind foot pronates substantially in wt-bearing position.
• The TTJ Joint counter acts the forefoot to keep the plantar aspect of the foot
in contact with the ground.
• TMT –medial forefoor will press the ground
lateral foot will lift off the ground
1st and 2nd ray -dorsiflexion
4th and 5th ray-plantarflexion
• the entire forefoot undergoes an inversion rotation around a hypothetical
axis at the second ray.
• PRONATION TWIST
• When the hind foot and TTJ are locked in supination ,the adjustment of
forefoot position will be left entirely to TMT Joints.
• TMT-forefoot medial –lift off the ground
• lateral-press to the ground
1st and 2nd-plantarflex
4th and 5th –dorsiflexion
• Eversion accompanies
Arches
• Needed for traction between the floor & foot’s wt bearing structures.
• Tensed throughout stance phase.
• Compared to a tie rod.
• Plantar plates of mtp resist compressive & tensile forces transferred through
plantar aponeurosis.
• In toe extension- mt heads act as pulleys that pull this fascia– supination.

















