20
Approaches to Medicaid Managed Care: Experiences on the Ground John Koehn President, Amerigroup New Jersey Medicaid Business Unit, WellPoint Inc.

Approaches to Medicaid Managed Care: Experiences on the Ground
John Koehn President, Amerigroup New Jersey Medicaid Business Unit, WellPoint Inc.

Who We Are
2

About WellPoint
• WellPoint, Inc. was formed through the 2004 merger of WellPoint Health Networks, Inc. and Anthem, Inc.
• Purpose Statement: Together, we are transforming health care with trusted and caring solutions
• Vision: To be America’s valued health partner
• Values: Trustworthy; Accountable; Innovative; Caring; Easy-to-do Business With
• Serves more than 37 million people in our family of health plans and nearly 69 million people through our affiliated companies
• Ranks No. 38 on Fortune 500; No. 2 on Fortune 500 health care companies listing
3

The Government Business Division Serves 4.8 Million Medicaid Members
4

About Amerigroup New Jersey
By the Numbers
• Began operations in 1996
• 189,000 members
• 8,666 providers, 65 hospitals
• 249 associates
Who We Serve
• Children’s Health Insurance Program (CHIP)
• Temporary Assistance for Needy Families (TANF)
• Supplemental Security Income (SSI)
• Medicare Advantage
• Long-Term Services and Supports (LTSS)
Amerigroup counties
5

The Role of Medicaid Managed Care
6

Top 5 Percent of Enrollees Accounted for More Than Half of Total Spending
Medicaid Enrollees and Expenditures by Enrollment Group
Notes: KCMU/Urban Institute estimates based on data from FY 2009 MSIS and CMS‐64, 2012. MSIS FY 2008 data were used for MA, PA, UT, and WI, but adjusted to 2009 CMS‐64.
Source: Kaiser Family Foundation, May 2012.
Enrollees 62.6 million
Expenditures $346.5 billion
Bottom 95% of
Spenders
Bottom 95% of
Spenders
Top 5 Percent: • Seniors • People with
Disabilities • Adults • Children
7

Patient-Centered Medical Homes Reduce Avoidable Hospital Readmissions 30-day readmissions were reduced 10 percent for diabetic members and 77 percent for members with asthma
Predictive Models to Identify High-Risk Members Saved more than $134 per member per month
Independent Labs, Outpatient Surgery and Imaging Services as Cost-Effective Alternatives to Hospital Services Saved more than $500,000 in lab, ambulatory surgical and radiology services
Lower Health Care Costs Right Care, Right Time, Right Place
8
Higher Quality An Ounce of Prevention Is Worth a Pound of Cure
Text Message Reminders to Close Gaps in Care Scheduled appointments for 71 percent of the members
Home Telemonitoring Program Helps Members with Chronic Conditions 11 percent increase in Low-Density Lipoprotein (LDL) screenings; a 47 percent increase in LDL control; improvements eye exams and A1c testing; reduction of hospital readmissions
Encouraging Healthy Behaviors for Pregnant Mothers to Improve Birth Outcomes 30 percent more prenatal care visits; 888 additional obstetric screenings; 6 percent more completed a postpartum care visit; administrative expenses reduced by more than 80 percent
9

Expanded Access to Care Medicaid-Focused Innovations
Specialty and Behavioral Health Delivered Via Telemedicine to Members Living in Rural Areas Urgent Services Network Reduces Preventable Emergency Visits Infusion Services Delivered by Community Oncologists Health Homes for Members with Multiple Chronic Illnesses Community Health Workers Locate Difficult to Reach Members and Coordinate Their Care Financial Incentives Provided to Improve Quality of Care
10

Policy Issues to Consider
11
Shifting Populations Competing Delivery Models High Cost Drugs

Shifting Population Composition of the Medicaid pipeline is changing as higher-cost, higher-need populations enter managed care
Source: Health Management Associates, Sept .2011.
• Duals
• Additional LTSS
• Members with a Developmental Disability
• Members with a Serious or Persistent Mental Illness
Continued Shift to More Complex Programs 2013 and Beyond
Medicaid Pipeline Composition Shift Over Past Decade
12

Source: MetLife, “Market Survey of Nursing Home and Assisted Living Costs,” (October 2011), http://www.metlife.com/mmi/research/2011-market-survey-long-term-care-costs.html#graphic (accessed July 31, 2012).
Long Term Services and Supports Costs
• The cost of nursing facility care for one person was equivalent to providing home and community-based services to nearly three seniors and/or persons with disabilities (AARP Policy Institute)
• We estimate that if the nation’s population now eligible for Coordinated LTSS (CLTSS) but currently receiving care under a FFS Medicaid program were moved to a model of coordinated care total savings of $17 billion could be achieved over the first three-year period
• Almost two thirds of the total $210.9 billion spent on Long-Term Services and Supports (LTSS) in 2011 was paid for by the federal-state Medicaid program (National Health Policy Forum)
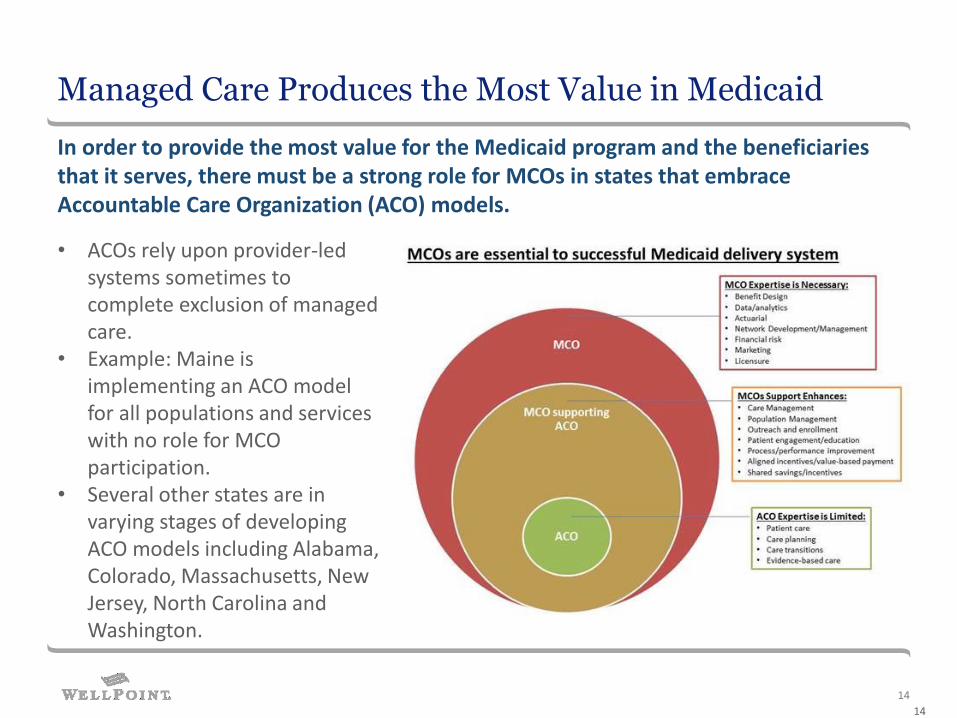
Managed Care Produces the Most Value in Medicaid
14
• ACOs rely upon provider-led systems sometimes to complete exclusion of managed care.
• Example: Maine is implementing an ACO model for all populations and services with no role for MCO participation.
• Several other states are in varying stages of developing ACO models including Alabama, Colorado, Massachusetts, New Jersey, North Carolina and Washington.
In order to provide the most value for the Medicaid program and the beneficiaries that it serves, there must be a strong role for MCOs in states that embrace Accountable Care Organization (ACO) models.
14

High-Cost Drugs are Not New… …but What is New is High-Cost Drugs for 3M People
15
About Gilead’s Various DTC Efforts Promoting Sovaldi
Sovaldi Manufacturer Gilead Sciences has begun launch an aggressive disease awareness campaign for the 4.1 million Americans with chronic hepatitis C.
• TV commercials featuring active people in open-air settings — imploring patients to “rethink your Hep C.”
• Print ads urge patients to get tested for the disease and to seek treatment, saying, “Don’t wait for your liver disease to progress. Talk to your physician today and visit www.sovaldi.com.”
• Multiple websites directing patients to “discount coupons” and offering advice on how best to speak with their physician, including:
• www.mysupportpath.com
• www.hepchope.com
• www.sovaldi.com.
16

Sovaldi Direct to Consumer (DTC) Advertising - Online
17

Potential Impacts of DTC Advertising
• Overall Impacts (From the Campaign for Sustainable Drug Pricing)
• While mass marketing is not necessarily negative, what makes Sovaldi different from any other mass-marketed drug is its inflated price tag at $84,000 for a 12-week course of treatment.
• The U.S. Centers for Disease Control and Prevention (CDC) estimates that 75 percent of those who are infected with hepatitis C are unaware of their status. However if with an aggressive marketing campaign all individuals infected with hepatitis C in America – an estimated 3.2 million people - were treated with Sovaldi, the cost of the Sovaldi alone would exceed the annual spend on all other brand name drugs combined.
• In the private sector, the California Technology Assessment Forum estimated that in order to pay for every person infected with hepatitis C to get Sovaldi, premiums would have to increase by $600 a year.
• Impact on Public Programs:
• According to Health Affairs, we assume that the 75,000 Part D enrollees get treated, equivalent to most of those who are aware they have the virus, but far less than the 350,000 infected beneficiaries, this would increase Part D drug spending by $6.5 billion, or an increase of about 8 percent in both federal Part D outlays and enrollee premiums.
• If 15 to 25 percent of people with Hepatitis C and covered by Medicaid are treated, the costs will be $7-$12.5 billion, based on population prevalence studies.
18

Short-Term Solutions: Options to Mitigate Risk for “Breakthrough” Drugs Needed adjustments to State Medicaid Rate Setting
19

Q-and-A
John Koehn President, Amerigroup New Jersey Medicaid Business Unit, WellPoint Inc.
20

















