Outcome After Arthroscopic Reconstruction of the Coracoclavicular Ligaments Using a Double-Bundle Coracoid Cerclage Technique Nata Parnes, M.D., Darren Friedman, M.D., Cameron Phillips, M.D., and Paul Carey, M.D. Purpose: We report the outcome of an arthroscopic technique for coracoclavicular ligament reconstruction using an anatomic coracoid cerclage. Methods: Between March 2011 and September 2012, 12 consecutive patients with symp- tomatic chronic (>4 weeks from injury) type V acromioclavicular separation for which nonoperative treatment failed were treated with arthroscopic double-bundle reconstruction of the coracoclavicular ligaments using tendon allograft by the first author. The clinical records, operative reports, and preoperative and follow-up radiographs were reviewed. The visual analog scale score, Subjective Shoulder Value, Simple Shoulder Test score, and Constant-Murley score were evaluated preoperatively and at each follow-up appointment. Results: The study included 12 shoulders in 12 young active-duty soldiers with symptomatic high-grade acromioclavicular separation who were treated with a technique for arthroscopic reconstruction of the coracoclavicular ligaments. The mean age was 25 years (range, 20 to 35 years). The injury occurred during sports activity in 11 patients. One patient was injured in a motorcycle accident. The mean time from injury to surgery was 17.8 months (range, 1.5 to 72 months). The minimum length of follow-up was 24 months (mean, 30.4 months; range, 24 to 42 months). The mean preoperative and postoperative outcome scores were signifi- cantly different (P < .0001) for all subjective outcome measures. The mean Constant-Murley score improved from 58.4 (range, 51 to 76) to 96 (range, 88 to 100). The mean visual analog scale score improved from 8.1 (range, 7 to 10) to 0.58 (range, 0 to 2). The mean Subjective Shoulder Value improved from 32.9% (range, 10% to 70%) to 95% (range, 80% to 100%). The mean Simple Shoulder Test score improved from 6 (range, 5 to 8) to 11.83 (range, 11 to 12). All patients returned to their normal preinjury level of activity by 6 months. Radiographs at last follow-up showed no loss of reduction with maintenance of the coracoclavicular interval. There was 1 complication (8.5%), a postoperative superficial wound infection, that was treated accordingly. Conclusions: We present an arthroscopic technique for double-bundle tendon graft reconstruction of the coracoclavicular ligaments using the coracoid cerclage technique. This method showed good outcomes and maintenance of radiographic reduction with high patient satisfaction and a low complication rate. Level of Evidence: Level IV, therapeutic case series. A cromioclavicular (AC) joint separation is one of the most common shoulder injuries in high-level athletes. 1 Rockwood et al. 2 classified these injuries ac- cording to the magnitude of injury to the stabilizing ligaments. Low-grade injuries, types I and II, represent injury to the AC ligaments without coracoclavicular (CC) ligament injury. Typically, these are treated conservatively and most patients return to preinjury status. High-grade injuries, types IV through VI, result from injury to the CC and AC ligaments and typically require surgical reconstruction. 3 The optimal treat- ment for type III injuries is still controversial. Many different surgical techniques have been reported to reconstruct high-grade AC joint separation including screws; plates; muscle transfer; ligamentoplasty pro- cedures; and ligament reconstruction using autograft, allograft, or synthetic materials. 1,4 Carofino and Mazzocca 4 noted that the greatest chal- lenge of AC reconstruction has been postoperative loss of reduction. Synthetic materials are mostly effective in early reconstructions, during the first 4 weeks. In delayed and late reconstructions, multiple studies have shown that From Tri County Orthopedics (N.P.), Carthage, New York; Weill Cornell Medical College (D.F.), New York; New York Presbyterian Lower Manhattan (C.P.), New York; Kingsbrook Jewish Medical Center (C.P.), New York; and Department of Orthopaedic Surgery, Guthrie Army Health Clinic (P.C.), Fort Drum, New York, U.S.A. The authors report the following potential conflict of interest or source of funding: D.F. receives support from Arthrex and Allen Medical. Received October 17, 2014; accepted March 19, 2015. Address correspondence to Paul Carey, M.D., Department of Orthopaedic Surgery, Guthrie Army Health Clinic, 11050 Mt Belvedere Rd, Fort Drum, NY 13602-5004, U.S.A. E-mail: [email protected]Ó 2015 by the Arthroscopy Association of North America 0749-8063/14872/$36.00 http://dx.doi.org/10.1016/j.arthro.2015.03.037 Arthroscopy: The Journal of Arthroscopic and Related Surgery, Vol -, No - (Month), 2015: pp 1-8 1
Transcript
Outcome After Arthroscopic Reconstruction of theCoracoclavicular Ligaments Using a Double-Bundle
Coracoid Cerclage TechniqueNata Parnes, M.D., Darren Friedman, M.D., Cameron Phillips, M.D., and Paul Carey, M.D.
Purpose: We report the outcome of an arthroscopic technique for coracoclavicular ligament reconstruction using ananatomic coracoid cerclage. Methods: Between March 2011 and September 2012, 12 consecutive patients with symp-tomatic chronic (>4 weeks from injury) type V acromioclavicular separation for which nonoperative treatment failedwere treated with arthroscopic double-bundle reconstruction of the coracoclavicular ligaments using tendon allograft bythe first author. The clinical records, operative reports, and preoperative and follow-up radiographs were reviewed. Thevisual analog scale score, Subjective Shoulder Value, Simple Shoulder Test score, and Constant-Murley score wereevaluated preoperatively and at each follow-up appointment. Results: The study included 12 shoulders in 12 youngactive-duty soldiers with symptomatic high-grade acromioclavicular separation who were treated with a technique forarthroscopic reconstruction of the coracoclavicular ligaments. The mean age was 25 years (range, 20 to 35 years). Theinjury occurred during sports activity in 11 patients. One patient was injured in a motorcycle accident. The mean timefrom injury to surgery was 17.8 months (range, 1.5 to 72 months). The minimum length of follow-up was 24 months(mean, 30.4 months; range, 24 to 42 months). The mean preoperative and postoperative outcome scores were signifi-cantly different (P < .0001) for all subjective outcome measures. The mean Constant-Murley score improved from 58.4(range, 51 to 76) to 96 (range, 88 to 100). The mean visual analog scale score improved from 8.1 (range, 7 to 10) to 0.58(range, 0 to 2). The mean Subjective Shoulder Value improved from 32.9% (range, 10% to 70%) to 95% (range, 80% to100%). The mean Simple Shoulder Test score improved from 6 (range, 5 to 8) to 11.83 (range, 11 to 12). All patientsreturned to their normal preinjury level of activity by 6 months. Radiographs at last follow-up showed no loss of reductionwith maintenance of the coracoclavicular interval. There was 1 complication (8.5%), a postoperative superficial woundinfection, that was treated accordingly. Conclusions: We present an arthroscopic technique for double-bundle tendongraft reconstruction of the coracoclavicular ligaments using the coracoid cerclage technique. This method showed goodoutcomes and maintenance of radiographic reduction with high patient satisfaction and a low complication rate. Level ofEvidence: Level IV, therapeutic case series.
Acromioclavicular (AC) joint separation is one ofthe most common shoulder injuries in high-level
athletes.1 Rockwood et al.2 classified these injuries ac-cording to the magnitude of injury to the stabilizing
ligaments. Low-grade injuries, types I and II, representinjury to the AC ligaments without coracoclavicular (CC)ligament injury. Typically, these are treated conservativelyand most patients return to preinjury status.High-grade injuries, types IV through VI, result from
injury to the CC and AC ligaments and typicallyrequire surgical reconstruction.3 The optimal treat-ment for type III injuries is still controversial. Manydifferent surgical techniques have been reported toreconstruct high-grade AC joint separation includingscrews; plates; muscle transfer; ligamentoplasty pro-cedures; and ligament reconstruction using autograft,allograft, or synthetic materials.1,4
Carofino and Mazzocca4 noted that the greatest chal-lenge of AC reconstruction has been postoperative loss ofreduction. Synthetic materials are mostly effective in earlyreconstructions, during the first 4 weeks. In delayed andlate reconstructions, multiple studies have shown that
From Tri County Orthopedics (N.P.), Carthage, New York; Weill CornellMedical College (D.F.), New York; New York Presbyterian Lower Manhattan(C.P.), New York; Kingsbrook Jewish Medical Center (C.P.), New York; andDepartment of Orthopaedic Surgery, Guthrie Army Health Clinic (P.C.), FortDrum, New York, U.S.A.
The authors report the following potential conflict of interest or source offunding: D.F. receives support from Arthrex and Allen Medical.
Received October 17, 2014; accepted March 19, 2015.Address correspondence to Paul Carey, M.D., Department of Orthopaedic
Surgery, Guthrie Army Health Clinic, 11050 Mt Belvedere Rd, Fort Drum,NY 13602-5004, U.S.A. E-mail: [email protected]
� 2015 by the Arthroscopy Association of North America0749-8063/14872/$36.00http://dx.doi.org/10.1016/j.arthro.2015.03.037
Arthroscopy: The Journal of Arthroscopic and Related Surgery, Vol -, No - (Month), 2015: pp 1-8 1
anatomic reconstruction using a tendon graft is superior instability, load to failure, and reproduction of the native CCligaments’ function.5-7
Anatomic reconstruction using tendon graft has beendescribed by use of open and arthroscopic techniques. Inthe open approach, adequate access to the coracoid processfor graft fixation requires deltoid detachment from theclavicle, as well as extensive soft-tissue dissection, andplaces the neurovascular structures at risk because of sub-optimal visibility during graft transfer around the coracoid.Anarthroscopic techniquemayoffergreatervisibility in therelatively small safe zones around the coracoid with lessdissection of the deltotrapezial fascia.3 However, to ourknowledge, all but one of the described arthroscopictechniques require the use of bony tunnels in the coracoid,increasing the risk of coracoid fracture and graft fixationfailure while reconstructing only 1 of the 2 CC ligaments.8
We report the outcome of an arthroscopic technique forCC ligament reconstruction using an anatomic coracoidcerclage. This technique is an arthroscopic modification ofthe open anatomic reconstruction previously described byCarofino and Mazzocca.4 We hypothesize that this tech-nique will provide good clinical and radiologic results withhigh patient satisfaction and a low complication rate.
MethodsBetween March 2011 and September 2012, 12
consecutive patients with symptomatic chronic (>4weeks from injury) type V AC separation for whichnonoperative treatment failed were treated with arthro-scopic double-bundle reconstruction of the CC ligamentsusing tendon allograft by the first author (N.P.). Theclinical records, operative reports, and preoperative andfollow-up radiographs were reviewed.The inclusion criteria were (1) preoperative radiologic
confirmation of grade V AC joint separation, (2) morethan 4-week interval from initial trauma to surgery,and (3) severe pain localized to the AC joint or loss offunction. Only patients with previous shoulder injuriesor operations were excluded.Patients were evaluated preoperatively and at each
follow-up appointment with the visual analog scale score,Subjective Shoulder Value, Simple Shoulder Test score,and Constant-Murley score. Final follow-up ranged from24 to 42 months (mean, 30.4 months).The coracoclavicular distance (CCD) was measured as
the distance from the most superior aspect of the coracoidbase to the undersurface of the clavicle on Zanca-viewradiographs. Because the native relation of the coracoidand distal clavicle may vary between patients, the dif-ference in CCD between the operative and nonoperativeshoulders was used to assess the reduction.
Surgical TechniqueThe patient is placed in the beach-chair position using
an articulated arm positioner (Fig 1). A 30� arthroscopeis inserted into the glenohumeral joint through a pos-terior portal. An anterior rotator interval portal isestablished with an outside-in technique using a spinalneedle to verify the position. The needle is replacedwith an 8.25-mm arthroscopic cannula.
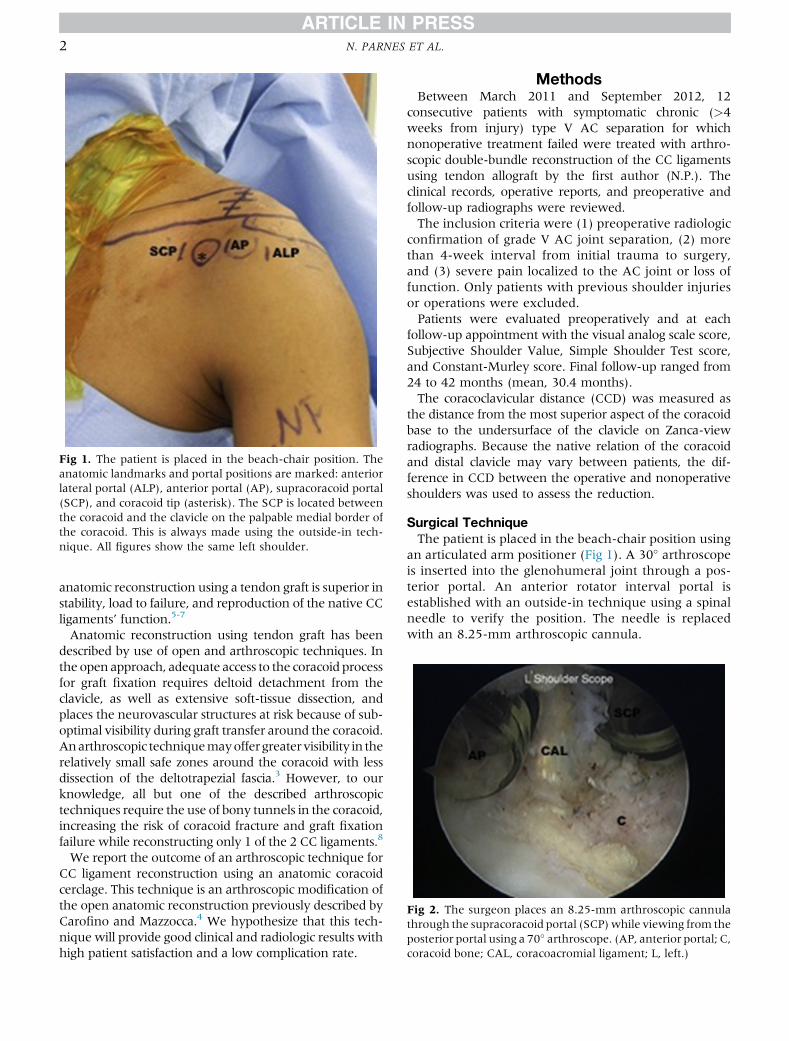
Fig 1. The patient is placed in the beach-chair position. Theanatomic landmarks and portal positions are marked: anteriorlateral portal (ALP), anterior portal (AP), supracoracoid portal(SCP), and coracoid tip (asterisk). The SCP is located betweenthe coracoid and the clavicle on the palpable medial border ofthe coracoid. This is always made using the outside-in tech-nique. All figures show the same left shoulder.
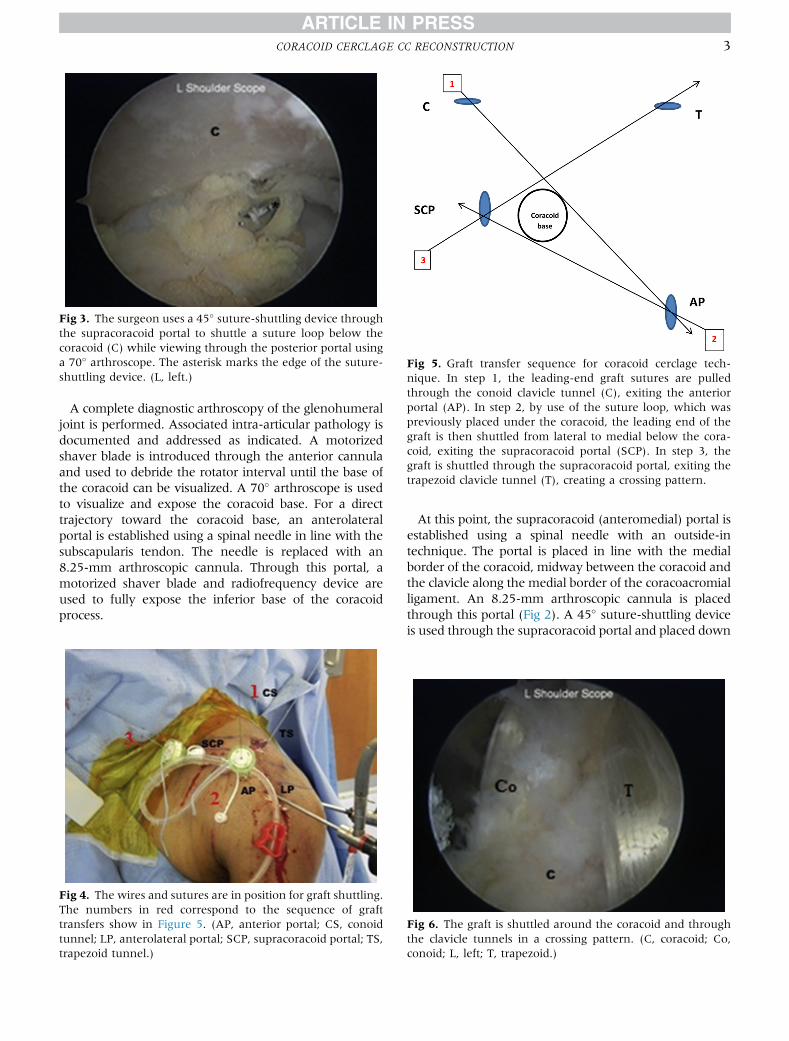
Fig 2. The surgeon places an 8.25-mm arthroscopic cannulathrough the supracoracoid portal (SCP)while viewing from theposterior portal using a 70� arthroscope. (AP, anterior portal; C,coracoid bone; CAL, coracoacromial ligament; L, left.)
2 N. PARNES ET AL.
A complete diagnostic arthroscopy of the glenohumeraljoint is performed. Associated intra-articular pathology isdocumented and addressed as indicated. A motorizedshaver blade is introduced through the anterior cannulaand used to debride the rotator interval until the base ofthe coracoid can be visualized. A 70� arthroscope is usedto visualize and expose the coracoid base. For a directtrajectory toward the coracoid base, an anterolateralportal is established using a spinal needle in line with thesubscapularis tendon. The needle is replaced with an8.25-mm arthroscopic cannula. Through this portal, amotorized shaver blade and radiofrequency device areused to fully expose the inferior base of the coracoidprocess.
At this point, the supracoracoid (anteromedial) portal isestablished using a spinal needle with an outside-intechnique. The portal is placed in line with the medialborder of the coracoid, midway between the coracoid andthe clavicle along the medial border of the coracoacromialligament. An 8.25-mm arthroscopic cannula is placedthrough this portal (Fig 2). A 45� suture-shuttling deviceis used through the supracoracoid portal and placed down
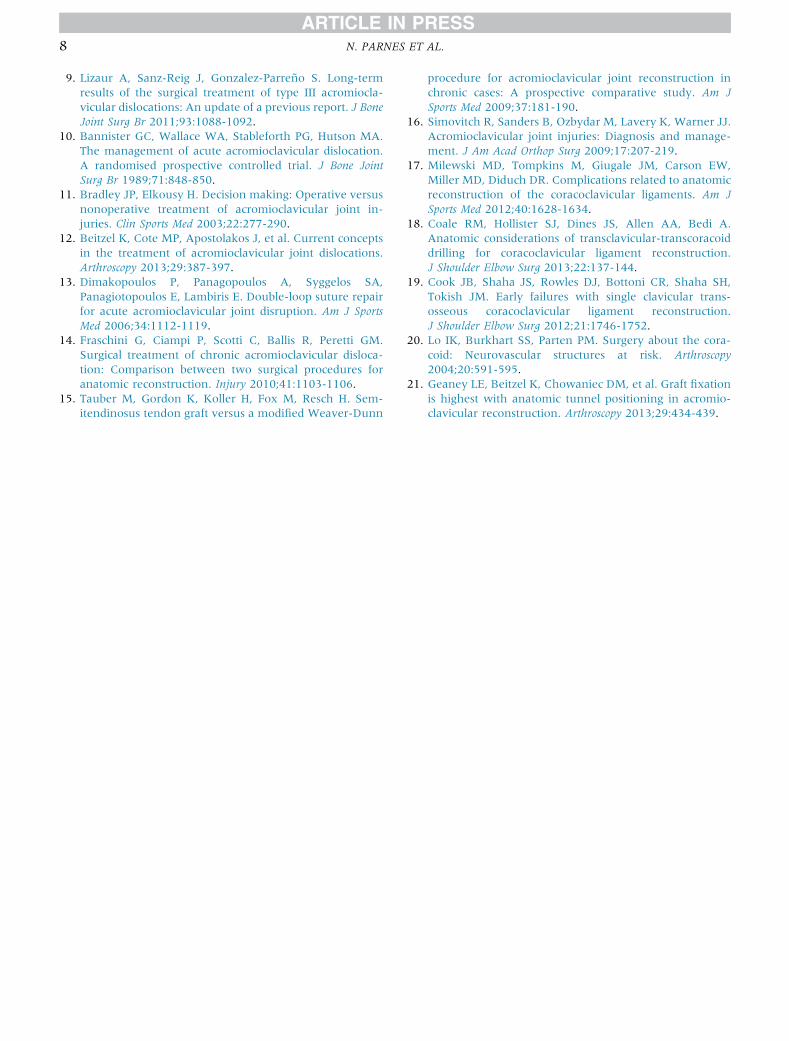
Fig 3. The surgeon uses a 45� suture-shuttling device throughthe supracoracoid portal to shuttle a suture loop below thecoracoid (C) while viewing through the posterior portal usinga 70� arthroscope. The asterisk marks the edge of the suture-shuttling device. (L, left.)
Fig 4. The wires and sutures are in position for graft shuttling.The numbers in red correspond to the sequence of grafttransfers show in Figure 5. (AP, anterior portal; CS, conoidtunnel; LP, anterolateral portal; SCP, supracoracoid portal; TS,trapezoid tunnel.)
Fig 6. The graft is shuttled around the coracoid and throughthe clavicle tunnels in a crossing pattern. (C, coracoid; Co,conoid; L, left; T, trapezoid.)
Fig 5. Graft transfer sequence for coracoid cerclage tech-nique. In step 1, the leading-end graft sutures are pulledthrough the conoid clavicle tunnel (C), exiting the anteriorportal (AP). In step 2, by use of the suture loop, which waspreviously placed under the coracoid, the leading end of thegraft is then shuttled from lateral to medial below the cora-coid, exiting the supracoracoid portal (SCP). In step 3, thegraft is shuttled through the supracoracoid portal, exiting thetrapezoid clavicle tunnel (T), creating a crossing pattern.
CORACOID CERCLAGE CC RECONSTRUCTION 3
the medial border of the coracoid until identified aboutthe coracoid base. The shuttle suture is retrieved throughthe anterior portal to shuttle a suture loop below thecoracoid (Fig 3).A 2-cm incision is made perpendicular to the clavicular
axis, 3.5 cm medial to the AC joint. The deltotrapezialfascia is released off the clavicle to obtain access to thesuperior cortex. Up to 10 mm of the distal clavicle may beremoved using an arthroscopic or open technique only ifthere is evidence of AC joint arthrosis or hyperostosis onpreoperative radiographs.The arthroscope is placed through the anterolateral
portal to improve visualization of the coracoid base. Thetarget end of the drill guide for the clavicle bone tunnelsis placed through the anterior portal just lateral to thebase of the coracoid. The drill sleeve of the guide ispositioned over the posterior third of the clavicle,approximately 4.5 cm medial to the distal clavicle edge.A guide pin is used for placement of the “conoid”tunnel. Once the guide pin is inserted in the direction ofthe eventual bone tunnel and its tip is visualized at thedesired position, a 5.5-mm cannulated headed reameris used over the guide pin to fashion the bone tunnel.The guide pin is removed, and the nonlooped end of aflexible nitinol passing wire is delivered through thecannulated reamer and retrieved through the anteriorportal before removal of the reamer.The target end of the drill guide is then placed
through the supracoracoid portal or anterior portal justsuperior to the coracoid. The drill sleeve of the guide ispositioned over the middle third of the clavicle,approximately 2.5 cmmedial to the distal clavicle edge.A guide pin is used for placement of the “trapezoid”tunnel. Once the guide pin is inserted in the direction ofthe eventual bone tunnel and its tip is visualized atthe desired position, the 5.5-mm cannulated headedreamer is used over the guide pin to fashion the bonetunnel. The guide pin is removed, and a flexible nitinolpassing wire is delivered through the reamer andretrieved through the supracoracoid portal beforeremoval of the cannulated reamer. Figures 4 and 5
show the technique for passing wires and suturesbefore graft passage.A soft-tissue autograft or allograft (commonly nonir-
radiated semitendinosus) is prepared on the back table.Several running locked sutures are placed in the leadingfree end of the graft. The graft length should be aminimum of 10 cm, and the graft should pass through a5.5-mm sizing block.The leading-end graft sutures are loaded on the
flexible loop on the previously placed passing wire. Thegraft is first pulled through the conoid clavicle tunnel,exiting the anterior portal. By use of the suture loopthat was previously placed under the coracoid, theleading end of the graft is then shuttled from lateral tomedial below the coracoid, exiting the supracoracoidportal. The graft is then shuttled through the supra-coracoid portal, exiting the trapezoid clavicle tunnel,creating a crossing pattern (Fig 6).Simultaneous superior displacement of the scap-
ulohumeral complex and inferior displacement of theclavicle reduce the AC joint. At this point, both graft endsare advanced superiorly through the tunnels, confirmingmaximal tightness. Once reduction is confirmed with anintraoperative Zanca-view radiograph, a 5.5-mm� 8-mmPEEK (polyether ether ketone) tenodesis screw is placed inthe conoid bone tunnel. After verification that initial screwfixation has been successful, a second PEEK tenodesisscrew is placed in the trapezoid bone tunnel (alternatively,a square knot tied with both free graft ends can be used).The remaining portions of the tendon graft are then sewnto each other using No. 2 nonabsorbable braided suture.The graft ends are placed laterally and secured with No. 2nonabsorbable braided suture to the AC joint capsule. Thearthroscopic portals are closed with interrupted subcu-taneousmonofilament sutureswhile the clavicularwoundis closed in layers. Figure 7 shows a typical completedreconstruction with the anatomic tunnel location refer-enced from the distal end of the clavicle. Figure 8 showspreoperative, immediate postoperative, and 2-year post-operative radiographs of a reconstructed chronic type VAC joint separation. Figure 5 is a schematic representationof the sequence used for graft passage in the technique.Postoperatively, the patients are placed in a gun-
slinger brace for 6 weeks. The patients are allowedelbow range of motion in the supine position. Activeand passive motion is allowed after 6 weeks. From 6 to12 weeks, rehabilitation is focused on gradual regainingof normal shoulder mechanics and range of motion.Resistance exercises are allowed after 12 weeks. Con-tact athletics are allowed after 6 months.
ResultsThe study included 12 shoulders in 12 active-duty
male patients, with a mean age of 25 years (range, 20to 35 years). The minimum length of follow-up was 24months (mean, 30.4 months; range, 24 to 42 months).
All the included patients were available for clinical andradiologic assessment.The injury occurred during sports activity in 11 pa-
tients (3 during football, 3 during wrestling, 3 duringsnowboarding, and 2 from a fall on the shoulder whilerunning). One patient was injured in a motorcycle ac-cident. The mean time from injury to surgery was 17.8months (range, 1.5 to 72 months). The right shoulderwas involved in 4 patients and the left shoulder in 8,and the dominant extremity was involved in 7 patients.All patients had returned to their preinjury job ac-
tivity in the army and recreational sports by 6 monthsafter surgery. We found no significant clinical orradiologic loss of reduction and there was no need forrevision surgery in any patient.The mean preoperative and postoperative outcome
scores were significantly different (P < .0001) for all sub-jective outcome measures: The mean visual analog scalescore improved from 8.1 � 1.3 (range, 7 to 10) to 0.58 �0.79 (range, 0 to 2), the mean Subjective Shoulder Valueimproved from 32.9% � 17.9% (range, 10% to 70%) to95% � 6.56% (range, 80% to 100%), the mean SimpleShoulder Test score improved from6� 0.95 (range, 5 to 8)to 11.83� 0.39 (range, 11 to 12), and themean Constant-Murley score improved from 58.4� 7.25 (range, 51 to 76)to 96 � 4.53 (range, 88 to 100) (Table 1).At final follow-up, the mean difference in CCD was
1.02 mm (range, 0 to 3 mm). There was no significantloss of reduction and no evidence of clavicle or coracoid
bone fracture. In 1 patient who had a 3-mm loss ofreduction, the trapezoid bone canal was also slightlywidened, raising suspicion that the tenodesis screw mayhave loosened. On review of the radiograph, ourimpression was that the canal was placed lateral to theanatomic position in the clavicle. At final follow-up, 28months postoperatively, the patient stated that he hadno pain and had returned to military duty and hispreinjury activity level of recreational sports participa-tion. He was satisfied with the cosmetic result.In our group of 12 patients, there has been 1 complica-
tion (8.5%). A postoperative superficial wound infectiondeveloped in 1 case at the supraclavicular incision site. Thecausative organism was identified as methicillin-sensitiveStaphylococcus aureus. The patient was treated with serialwound irrigations followed by delayed closure. Hisallograft-tenodesis screw construct was left intact. Hereceived intravenous clindamycin and ciprofloxacintreatment for 6 weeks as recommended by an infectiousdisease specialist. Sixmonths after surgery, the patientwasasymptomatic and the reconstruction remained clinicallyand radiologically stable. The patient returned to recrea-tional sports and full-time military duty and remained inthe same condition at his last follow-up visit 3.5 years aftersurgery.
DiscussionThis study describes arthroscopic anatomic recon-
struction of the CC ligaments using the supracoracoid
Fig 8. (A) Preoperative radiograph showing chronic grade V acromioclavicular joint separation. (CCD, coracoclavicular dis-tance.) (B) The immediate postoperative radiograph shows reduction. (C) The follow-up radiograph at 2 years shows no loss ofreduction.
CORACOID CERCLAGE CC RECONSTRUCTION 5
portal. This technique was developed to avoid some ofthe complications reported with current arthroscopictechniques. The clinical and radiologic outcomes in thisstudy are comparable with the outcomes of openanatomic CC ligament reconstruction reported by Car-ofino and Mazzocca.4
AC joint separation is a common injury among youngathletes and motorcycle riders.9 With 1 exception, all ofthe patients included in our study were young militarymen in their 20s. Eleven of the patients were injuredduring sports activity and one in a motorcycle accident.Young active patients who sustain a high-grade AC jointseparation have better outcomes regarding function andpain relief with surgical treatment than patients who aretreated conservatively.10,11
Anatomic reconstructions of the CC ligaments usingfree tendon grafts have shown greater stability and loadto failure than nonanatomic ligamentoplasty proceduressuch as the traditional Weaver-Dunn procedure andnonanatomic allograft, anatomic suture, and GraftRopetechniques (Arthrex, Naples, FL).7 They also more closelyreproduce the function of the native CC ligaments. In arecent systematic review, Beitzel et al.12 found a lack ofevidence in the literature to support a single technique asthe “gold standard” for CC reconstruction. However, onthe basis of their research, they favor techniques thatrespect the bony anatomy and restore the native functionof both the conoid and trapezoid.12 Our study reinforcesthe findings of other clinical reports that also support suchanatomic reconstructions.13-16
Carofino and Mazzocca,4 in a case series of 17 patientswho underwent anatomic open CC ligament recon-struction with free tendon graft, reported significantimprovement in pain levels and function. The meanAmerican Shoulder and Elbow Surgeons scoreincreased from 52 preoperatively to 92. The Constant-Murley score rose from 66.6 to 94.7. There were 3failures in this series, and 2 required revision surgery.The open anatomic CC ligament reconstruction tech-
nique described by Carofino and Mazzocca4 has severalrisks and disadvantages, including extensive soft-tissuedissection and detachment of the deltoid from the clav-icle for graft transfer around the coracoid base. In addi-tion, suboptimal visibility around the coracoid processduring the graft transfer, especially in muscular patients,may place the neurovascular structures at risk.3
To overcome the aforementioned challenges, severalarthroscopic techniques have been developed and arewidely used today. These techniques permit greater visi-bility of the base of the coracoid with less soft-tissuedissection.3 However, to our knowledge, all but one ofthe published arthroscopic reconstruction techniques use asingle clavicular tunnel and require drilling of the coracoidbase for graft fixation.8 This creates the risk of coracoidfracture because the high load to failure of the graft orfixation device may exceed the load to failure of theT
able
1.Dem
ograp
hic
DataofPatients
Treated
WithArthroscopic
Double-Bundle
Rep
air
Age
,yr
Tim
eto
Surgery
Follow-up,
mo
VASScore
SSV
Constan
tScore
SSTScore
Mea
nDifference
inCCD
Postoperatively,
mm
Preoperative
Postoperative*
Preoperative
Postoperative*
Preoperative
Postoperative*
Preoperative
Postoperative
25
6wk
42
80
10%
90%
51
100
512
224
6mo
36
80
50%
100%
58
100
612
1.2
27
6mo
35
60
30%
100%
52
95
612
135
2mo
31
60
40%
100%
56
100
612
027
6mo
31
10
230%
80%
55
88
511
122
18mo
29
91
20%
95%
55
94
512
026
3mo
29
90
10%
100%
52
100
512
124
18mo
28
70
50%
100%
76
100
812
322
72mo
27
82
25%
90%
60
93
711
0.5
20
30mo
26
81
40%
90%
63
90
612
124
48mo
24
81
70%
90%
67
92
712
0.5
21
3mo
24
10
020%
100%
56
100
612
1Mean,24.75
17.8
mo
30.4
8.1
0.58
32.9%
95%
58.41
96
611.83
1.01
CCD,coracoclav
iculardistance;SST,Sim
ple
Shoulder
Test;SSV,Subjective
Shoulder
Value;
VAS,visual
analogscale.
*Differencesarestatisticallysign
ificant(P
<.0001).
6 N. PARNES ET AL.
cortical bone before device breakage. Milewski et al.17
reported an 80% complication rate in the coracoid-tunnel group of 10 patients, including coracoid fracturesin 20% and intraoperative failure of the coracoid buttonfixation in 10%. In comparison, there was a 35% totalcomplication rate in the coracoid-loop group. In theirgroup of 106 patients who underwent open anatomic CCreconstruction by the coracoid cerclage technique, Car-ofino andMazzocca4 did not report any coracoid fractures.Coale et al.18 found in their study that transclavicular-
transcoracoid reconstructive techniques cannot restorethe footprint of the conoid and trapezoid ligamentswithout significant risk of cortical breach and fracture.Cook et al.19 reported an 80% early failure rate in 10active-duty patients who underwent CC ligament recon-struction with the GraftRope technique. Four patientsrequired revision surgery.VanSice and Savoie8 presented the findings in 12
patients who were treated with arthroscopic AC jointreconstruction with transfer of the graft around ratherthan through the coracoid. In 2 patients inflammationdeveloped from the nonabsorbable suture placed abovethe clavicle, which required removal in the clinic. Onepatient had a 5-mm loss of reduction, and one patientrequired revision because of a fall in the postoperativeperiod. At 2 to 4 years of follow-up, loss of reduction orrevision surgery did not otherwise occur in any patient.In our group of young active-duty patients, there has
been 1 complication (8.5%), a postoperative woundinfection that required debridement and intravenousantibiotics. This did not affect the reconstruction sta-bility or the final clinical or radiographic outcome. All ofthe reconstructions remained stable at final follow-up,and no patient required revision surgery.An advantage of the described surgical technique is that
it can be performed through small arthroscopic portals,thus avoiding deltoid detachment and extensive soft-tissuedissection while enabling excellent visualization of thecoracoid base during the graft transfer. The technique usesthe supracoracoid portal, which is located midwaybetween themedial border of the coracoid and the clavicle.Lo et al.20 showed in their study on neurovascular struc-tures around the coracoid that this area is safe. We use anoutside-in technique to optimize the placement of thisportal.Geaney et al.21 found that the optimal bone density of
the clavicle is in the anatomic insertion area of the CCligaments between 20 mm and 50 mm from the lateraledge of the clavicle. In our technique the tendon graft isfixed to the clavicle using 2 bone tunnels that are located25mmand 45mm from the lateral end of the clavicle. Thepresent technique reproduces the anatomic insertion ofthe 2 CC ligaments on the clavicle without drilling thecoracoid process. This potentially explains the lack of bonefractures and the maintenance of fixation stability in ourgroup of patients.
At a minimum follow-up of 24 months, we have foundmarked improvement in the Constant score, SimpleShoulder Test score, and level of pain. There was also agood cosmetic result in all patients, and all patientsreturned to preinjury levels of sports and job activity.
LimitationsAlthough this study is limited in that it includes a small
homogeneous cohort of young active-duty military malepatients, the cohort size compares favorably with similarpublished studies.8,18 However, the findings may not beapplicable to the broader population because of differencesin general health condition and bone quality, as well asother anatomic considerations. In addition, although thefollow-up period is sufficient to assess the outcome afterthe described procedure, a longer-term study includingmore patients may identify additional potential compli-cations. Lastly, the lack of a comparison group in thepublished literature with high similarity to our patientgroup confounds our ability to fully evaluate the outcome.
ConclusionsWe present an arthroscopic technique for CC liga-
ment reconstruction using an anatomic coracoid cerc-lage. This method showed good outcomes andmaintenance of radiographic reduction with high pa-tient satisfaction and a low complication rate.
References1. Mazzocca AD, Arciero RA, Bicos J. Evaluation and treat-
ment of acromioclavicular joint injuries. Am J Sports Med2007;35:316-329.
2. Rockwood CJ, Williams G, Young D. Disorders of theacromioclavicular joint. In: Rockwood CJ, Matsen FA III,ed. The Shoulder. Ed 2. Philadelphia: WB Saunders, 1998:483-553
3. DeBerardino TM, Pensak MJ, Ferreira J, Mazzocca AD.Arthroscopic stabilization of acromioclavicular jointdislocation using the AC graftrope system. J ShoulderElbow Surg 2010;19:47-52.
5. Lädermann A, Gueorguiev B, Stimec B, Fasel J, Rothstock S,Hoffmeyer P. Acromioclavicular joint reconstruction: Acomparative biomechanical study of three techniques.J Shoulder Elbow Surg 2013;22:171-178.
6. Mazzocca AD, Santangelo SA, Johnson ST, Rios CG,Dumonski ML, Arciero RA. A biomechanical evaluationof an anatomical coracoclavicular ligament reconstruc-tion. Am J Sports Med 2006;34:236-246.
7. Thomas K, Litsky A, Jones G, Bishop JY. Biomechanicalcomparison of coracoclavicular reconstructive techniques.Am J Sports Med 2011;39:804-810.
8. VanSice W, Savoie H. Arthroscopic reconstruction of theacromioclavicular joint using semitendinosus allograft:Technique and preliminary results. Tech Shoulder ElbowSurg 2008;9:109-113.
9. Lizaur A, Sanz-Reig J, Gonzalez-Parreño S. Long-termresults of the surgical treatment of type III acromiocla-vicular dislocations: An update of a previous report. J BoneJoint Surg Br 2011;93:1088-1092.
11. Bradley JP, Elkousy H. Decision making: Operative versusnonoperative treatment of acromioclavicular joint in-juries. Clin Sports Med 2003;22:277-290.
12. Beitzel K, Cote MP, Apostolakos J, et al. Current conceptsin the treatment of acromioclavicular joint dislocations.Arthroscopy 2013;29:387-397.
13. Dimakopoulos P, Panagopoulos A, Syggelos SA,Panagiotopoulos E, Lambiris E. Double-loop suture repairfor acute acromioclavicular joint disruption. Am J SportsMed 2006;34:1112-1119.
14. Fraschini G, Ciampi P, Scotti C, Ballis R, Peretti GM.Surgical treatment of chronic acromioclavicular disloca-tion: Comparison between two surgical procedures foranatomic reconstruction. Injury 2010;41:1103-1106.
15. Tauber M, Gordon K, Koller H, Fox M, Resch H. Sem-itendinosus tendon graft versus a modified Weaver-Dunn
procedure for acromioclavicular joint reconstruction inchronic cases: A prospective comparative study. Am JSports Med 2009;37:181-190.
16. Simovitch R, Sanders B, Ozbydar M, Lavery K, Warner JJ.Acromioclavicular joint injuries: Diagnosis and manage-ment. J Am Acad Orthop Surg 2009;17:207-219.
17. Milewski MD, Tompkins M, Giugale JM, Carson EW,Miller MD, Diduch DR. Complications related to anatomicreconstruction of the coracoclavicular ligaments. Am JSports Med 2012;40:1628-1634.
18. Coale RM, Hollister SJ, Dines JS, Allen AA, Bedi A.Anatomic considerations of transclavicular-transcoracoiddrilling for coracoclavicular ligament reconstruction.J Shoulder Elbow Surg 2013;22:137-144.
19. Cook JB, Shaha JS, Rowles DJ, Bottoni CR, Shaha SH,Tokish JM. Early failures with single clavicular trans-osseous coracoclavicular ligament reconstruction.J Shoulder Elbow Surg 2012;21:1746-1752.
20. Lo IK, Burkhart SS, Parten PM. Surgery about the cora-coid: Neurovascular structures at risk. Arthroscopy2004;20:591-595.
21. Geaney LE, Beitzel K, Chowaniec DM, et al. Graft fixationis highest with anatomic tunnel positioning in acromio-clavicular reconstruction. Arthroscopy 2013;29:434-439.
Arthroscopic Transtendinous Double-PulleyRemplissage Technique in the Beach-Chair Position
for Large Hill-Sachs LesionsNata Parnes, M.D., MAJ Paul A. Carey, M.D., MC, USA, Christopher Schumacher, M.D.,
and Mark D. Price, M.D., Ph.D.
Abstract: Hill-Sachs lesions are a common finding in patients with glenohumeral instability. There have been numerousmethods described for addressing Hill-Sachs deformity. One popular method includes transferring a portion of theinfraspinatus muscle into the posterior-superior defect (remplissage) to prevent the lesion from engaging and the resultantinstability. We present a method of arthroscopic remplissage whereby the lesion is addressed through transtendinousinsertion of arthroscopic anchors. Once 2 anchors have been inserted, 1 limb of each suture is tied to the other anchor, theso-called pulley repair technique. This can be performed either under direct visualization in the subacromial space orblindly while the surgeon is viewing from the articular side. Once both limbs have been tied, the infraspinatus tendonnicely spans the defect, and there has been minimal morbidity to the tendon itself. We have found this method to be usefulfor addressing a large Hill-Sachs deformity.
Posterosuperior humeral head impaction fractures(Hill-Sachs lesions) occur in up to 88% of patients
with recurrent anteroinferior glenohumeral instability.1
Large Hill-Sachs lesions of the humeral head can engageover the anterior glenoid rim when the arm is abductedand externally rotated, resulting in recurrent anteriorinstability and failure of an isolated labral repair.A variety of open and arthroscopic techniques have
been described to treat engaging Hill-Sachs lesionsincluding humeral head and/or anterior glenoid rimaugmentation, rotational humeral osteotomies, partialarthroplasties, capsular shifts, and tissue-filling tech-niques. In 2004 Wolf and Pollack2 described the
arthroscopic technique of Hill-Sachs remplissage (Frenchfor “filling”) performed in combination with Bankartrepair with the patient in the lateral decubitus position.This technique has gained in popularity because of itssimplicity, short surgical time, good biomechanical andclinical outcome, lack of need for graft augmentation, andlow rate of complications. Multiple variations of thistechnique have been describedwith patients in the lateraldecubitus and beach-chair positions.In 2009 Koo et al.3 described an arthroscopic double-
pulley remplissage technique with the patient in thelateral decubitus position,which provides a large footprintfixation but requires alternate visualization of the gleno-humeral joint and the subacromial space. We present amodification of this technique performedwith the patientin the beach-chair position using Healix Transtend an-chors (Mitek, Raynham, MA) to achieve all-internalremplissage fixation.
nique is similar to an arthroscopic transtendinous double-pulley repair of a partial-thickness, articular-surfacesupraspinatus tendon repair. It essentially consists of fix-ation of the infraspinatus tendon and posterior capsule tothe abraded surface of the Hill-Sachs lesion. The techniquedescribed in this report was developed by the firstauthor (N.P.) and simplifies the double-pulley remplissage
From Tri County Orthopedic Center (N.P.), Carthage; Fort Drum ArmyHospital (P.A.C.), Fort Drum, New York; and University of MassachusettsMedical School and UMass Memorial Medical Center (C.S., M.D.P.),Worcester, Massachusetts, U.S.A.
The authors report the following potential conflict of interest or source offunding: M.D.P. receives support from American Academy of OrthopaedicSurgeons Anatomy and Imaging Evaluation Subcommittee, DePuy Mitek,and Arthrex.
Received December 29, 2014; accepted March 5, 2015.Address correspondence to Mark D. Price, M.D., Ph.D., UMass Memorial
Medical Center, Division of Sports Medicine, 281 Lincoln St, Worcester MA01605, U.S.A. E-mail: [email protected]
� 2015 Arthroscopy Association of North America. Published by ElsevierInc. All rights reserved.
technique of Koo et al.3 by using the Healix Transtendanchor system. Video 1 demonstrates this method in itsentirety. The steps of the procedure are outlined in Table 1,and pearls, pitfalls, key points, and indications are shownin Table 2.Under general anesthesia, the patient is placed in a
modified beach-chair position and the arm is placed intoa Spider articulated arm holder (Tenet Medical, Calgary,Alberta, Canada) that allows for free positioning in space.The arthroscope is introduced into the glenohumeraljoint through a posterolateral portal that is placed at thelateral aspect of the convexity of the humeral head sothat it is centered directly over the Hill-Sachs lesion. Thisportal will allow visualization of the joint during theanterior labral repair, as well as working access to abradethe surface of the Hill-Sachs lesion and suture manage-ment during the transtendinous double-pulley repair. Ananteroinferior portal is made in the rotator interval,whichwill be the primary working portal for the anteriorlabral repair. By use of a spinal needle, an anterosuperiorportal is placed immediately posterior to the bicepstendon by an outside-in technique. This portal will allowsuture management during the anterior labral repairand visualization of the Hill-Sachs lesion during theremplissage procedure.We first perform diagnostic glenohumeral arthroscopy
through the posterior portal and then through the ante-rosuperior portal. We assess the anterior labral lesion, theamount of glenoid bone loss, and the size of the Hill-Sachslesion, and we determine whether the Hill-Sachs lesion isengaging while the arm is in abduction and externalrotation.Our indications for the remplissage procedure include
a moderate to large Hill-Sachs defect (>3mm in depth)associated with bony glenoid loss of less than 25% or asmall to moderate Hill-Sachs defect associated withglenoid bone loss close to 25%. Any Hill-Sachs lesion
associated with glenoid bone loss greater than 25% isaddressed with the Latarjet procedure.A subacromial bursectomy is performed with special
attention to the posterior and posterolateral gutters toprevent interposition of bursal tissue during the knot-tying
Table 1. Step-by-Step Remplissage Technique
1. Position the patient in the beach-chair position.2. Perform diagnostic arthroscopy through the posterolateral portal
and the anterolateral portal.3. Clear the subacromial space posteriorly and posterolaterally.4. Place and pass glenoid sutures/anchors without tying them.5. Prepare the Hill-Sachs bony bed.6. Insert the trocar-tipped guidewire for the Healix Transtend anchor
through the posterior cannula, infraspinatus tendon, andposterior capsule, locating it at the inferior aspect of the Hill-Sachs lesion, next to the articular margin.
7. Use a 4-mm designated cannula over the guidewire to place theHealix Transtend anchor at the desired location.
8. Repeat steps 6 and 7 with a second Healix Transtend anchor, andplace it at the superior aspect of the Hill-Sachs lesion.
9. Viewing from the anterosuperior portal and working through theanteroinferior portal, tie the glenoid sutures.
10. Through the posterior 8.5-mm cannula, tie the sutures from the 2anchors using the double-pulley technique.
11. Verify the quality of the repair on both intra-articular andsubacromial views.
Table 2. Pearls, Pitfalls, Key Points, and Indications
PearlsThe procedure can be performed with the patient in the beach-
chair or lateral decubitus position.It is important to perform preliminary subacromial bursectomy
with special attention to the posterior and posterolateralgutters to prevent interposition of bursal tissue during theknot-tying stage.
When the surgeon is performing arthroscopy through theanterosuperior portal, a 70� arthroscope allows better viewingof the Hill-Sachs lesion, although a 30� arthroscope can stillprovide adequate visualization.
While the surgeon is preparing the bony bed of the Hill-Sachsdefect, it is important to be gentle and remove a minimalamount of surface bone.
During the procedure, the cannula has to be withdrawn from theposterior capsule and the infraspinatus tendon but not throughthe deltoid.
The arm should be positioned in slight abduction and neutralrotation.
While the surgeon is inserting the anchors, it is important to anglethe guide perpendicular to the lesion or slightly from medial tolateral to reduce the risk of penetrating the articular surface.
The 70� arthroscope should be used through the anterosuperiorportal and the anterior portal to verify that the first anchor hasbeen placed in the most inferior area of the Hill-Sachs defect.
The second anchor should be placed in the most superior area ofthe Hill-Sachs defect.
The surgeon should verify that the sutures on both anchors slideeasily.
While tying the sutures from the 2 anchors in the double-pulleytechnique, the surgeon should verify that the first knot is stableand does not slip before pulling it into the subacromial space.
The final tissue fixation to the Hill-Sachs defect should beperformed by tying arthroscopic nonsliding knots in thesubacromial space and should be confirmed on both intra-articular and subacromial views.
At the end of the procedure, the humeral head should be centeredon the glenoid when viewing through the anterosuperiorportal.
PitfallsFailure of 1 of the 2 anchors will lead to failure of the double-
pulley fixation.If the choice is made to view the knots being tied in the
subacromial space, the surgeon must be sure to perform thesubacromial bursectomy before anchor insertion; otherwise,damage to the sutures is possible or even likely.
Key pointsThis technique simplifies the double-pulley technique of Koo
et al.3 by using the Transtend anchor system.The double-pulley technique provides a large footprint fixation.The technique is simple and less time-consuming than previously
described techniques for remplissage.Indications
Intraoperative evidence of engagement of Hill-Sachs defectModerate to large Hill-Sachs defect (>3 mm in depth) associated
with bony glenoid loss <25%Borderline arthroscopic cases in which bone defect is close to 25%
but Hill-Sachs defect is small to moderate in size
e306 N. PARNES ET AL.
stage. Once the subacromial space has been prepared, thearthroscope is again placed intra-articularly.Viewing from the posterior portal and instrumenting
through the anteroinferior and anterosuperior portals,the surgeon mobilizes the labral tear and inferior gle-nohumeral ligament and repairs the labrum with sutureanchors. The sutures are passed through the ante-roinferior portal and left untied.The camera is switched from the posterior portal to the
anterosuperior portal; we have found that a 70� arthro-scope allows better viewing of the Hill-Sachs lesion at thispoint. An 8.5-mm threaded cannula is placed over aswitching stick in the posterior portal. Through the
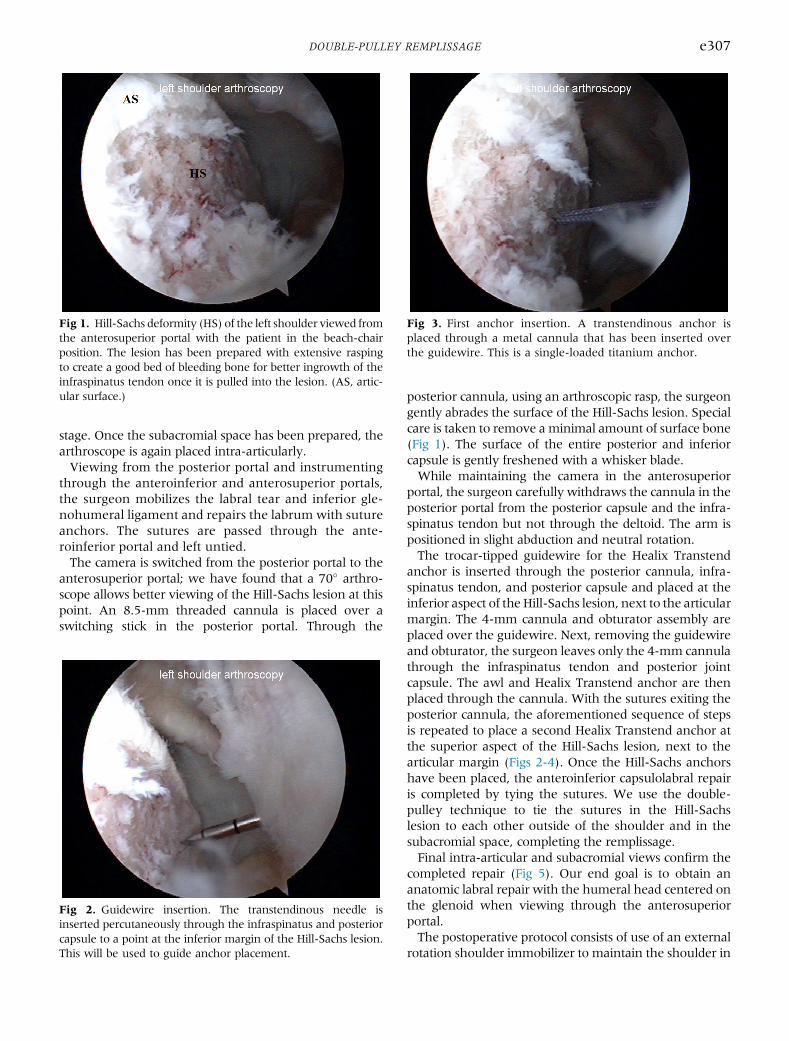
posterior cannula, using an arthroscopic rasp, the surgeongently abrades the surface of the Hill-Sachs lesion. Specialcare is taken to remove aminimal amount of surface bone(Fig 1). The surface of the entire posterior and inferiorcapsule is gently freshened with a whisker blade.While maintaining the camera in the anterosuperior
portal, the surgeon carefully withdraws the cannula in theposterior portal from the posterior capsule and the infra-spinatus tendon but not through the deltoid. The arm ispositioned in slight abduction and neutral rotation.The trocar-tipped guidewire for the Healix Transtend
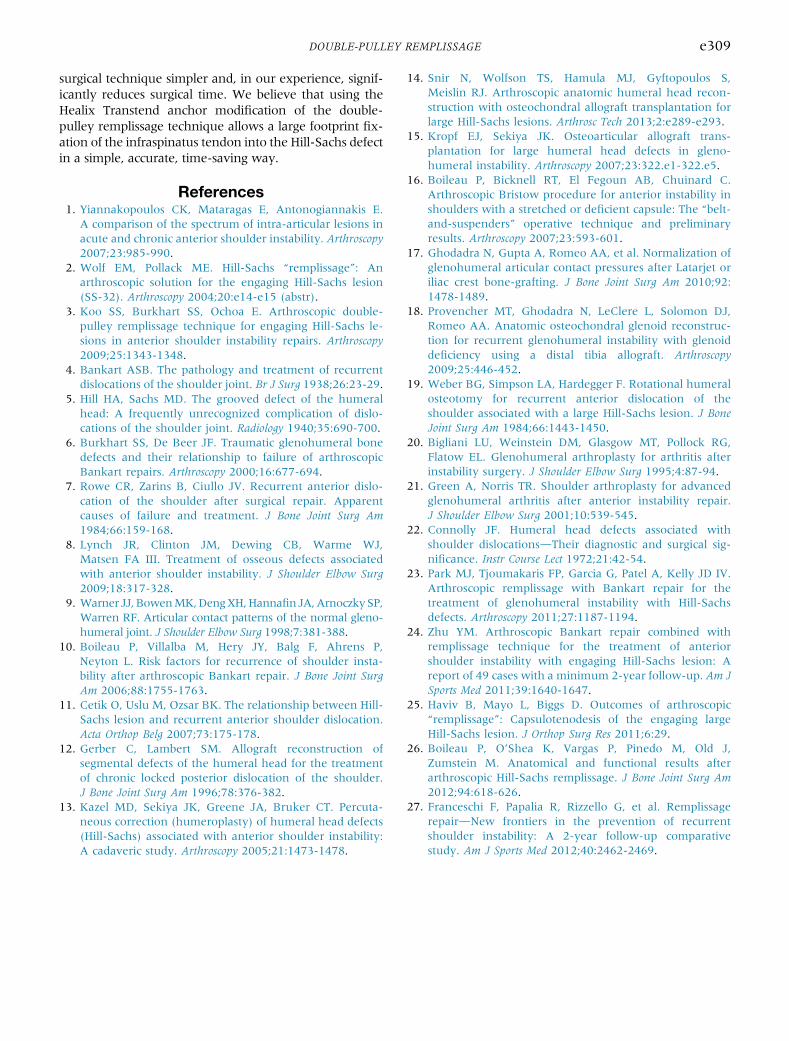
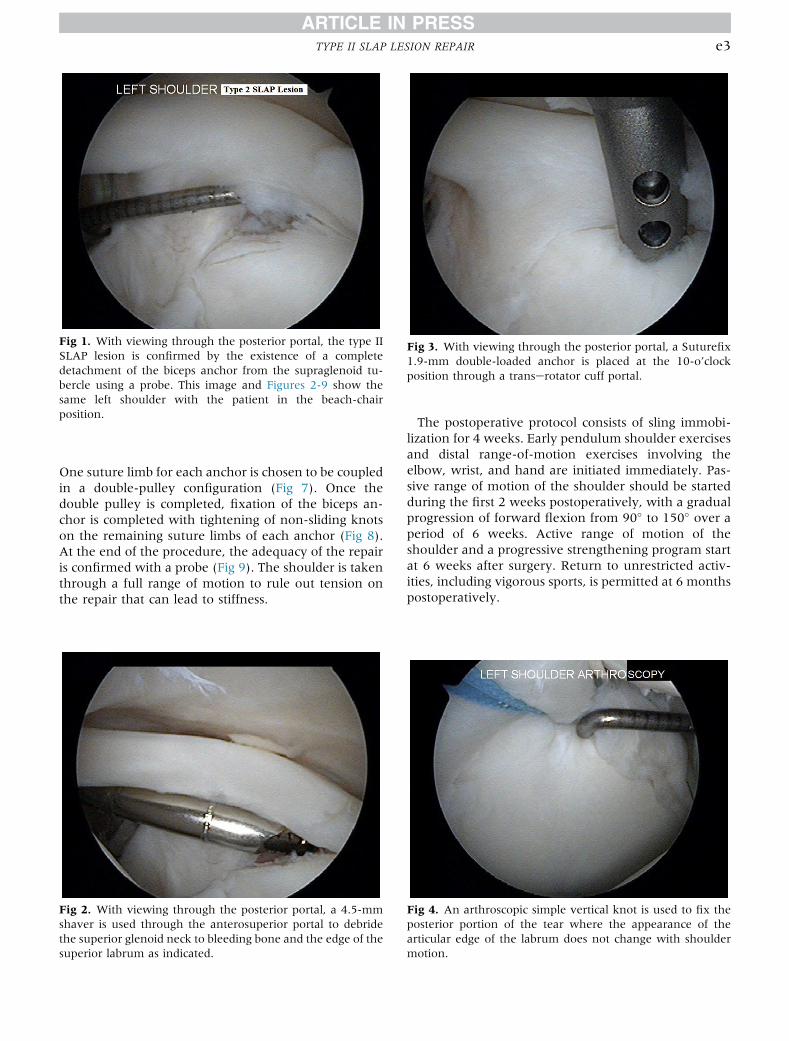
anchor is inserted through the posterior cannula, infra-spinatus tendon, and posterior capsule and placed at theinferior aspect of theHill-Sachs lesion, next to the articularmargin. The 4-mm cannula and obturator assembly areplaced over the guidewire. Next, removing the guidewireand obturator, the surgeon leaves only the 4-mm cannulathrough the infraspinatus tendon and posterior jointcapsule. The awl and Healix Transtend anchor are thenplaced through the cannula. With the sutures exiting theposterior cannula, the aforementioned sequence of stepsis repeated to place a second Healix Transtend anchor atthe superior aspect of the Hill-Sachs lesion, next to thearticular margin (Figs 2-4). Once the Hill-Sachs anchorshave been placed, the anteroinferior capsulolabral repairis completed by tying the sutures. We use the double-pulley technique to tie the sutures in the Hill-Sachslesion to each other outside of the shoulder and in thesubacromial space, completing the remplissage.Final intra-articular and subacromial views confirm the
completed repair (Fig 5). Our end goal is to obtain ananatomic labral repair with the humeral head centered onthe glenoid when viewing through the anterosuperiorportal.The postoperative protocol consists of use of an external
rotation shoulder immobilizer to maintain the shoulder in
Fig 1. Hill-Sachs deformity (HS) of the left shoulder viewed fromthe anterosuperior portal with the patient in the beach-chairposition. The lesion has been prepared with extensive raspingto create a good bed of bleeding bone for better ingrowth of theinfraspinatus tendon once it is pulled into the lesion. (AS, artic-ular surface.)
Fig 2. Guidewire insertion. The transtendinous needle isinserted percutaneously through the infraspinatus and posteriorcapsule to a point at the inferior margin of the Hill-Sachs lesion.This will be used to guide anchor placement.
Fig 3. First anchor insertion. A transtendinous anchor isplaced through a metal cannula that has been inserted overthe guidewire. This is a single-loaded titanium anchor.
DOUBLE-PULLEY REMPLISSAGE e307
neutral rotation. This helps decrease tension on the pos-terior repair. Immobilization is maintained for 4 to6 weeks. Immediate isometric and elbow range-of-motionexercises are allowed. At the 6-week mark, a program ofactive and active-assisted motion exercises is begun.Increased active strengthening exercises are implementedat the 12-week mark. Return to full activity and sports isallowed at approximately 5 to 6 months after surgery.
DiscussionOver 95%of shoulder dislocations are anterior.4 During
anterior shoulder dislocation, the head of the humerusforcefully displaces out of the glenoid socket, avulsinganterior bony and soft-tissue structures in the process(Bankart lesion).4 As the posterior part of the humeralhead exits the joint and the soft cancellous bone of theposterosuperior humeral head collides with the densecortical anterior rim of the glenoid, a bony indentation atthe back of the humeral head may be created (Hill-Sachslesion).5 These bony lesions are an important causeof recurrent shoulder instability and failure of Bankartrepairs.6-8 In particular, lesions that engage the rim of theglenoid when the shoulder is in a position of abductionand external rotation, so-called engaging Hill-Sachs le-sions, are associated with recurrent instability.6,9-11 Avariety of anatomic and nonanatomic surgical techniqueshave been described to address Hill-Sachs lesions that arelarge, engaging, or associated with recurrent instability,including humeral head augmentation, disimpaction,and resurfacing12-15; glenoid bone augmentation16-18;and rotational humeral osteotomy.19 These techniquesmight achieve good stabilization of the shoulder, but theyalso are associated with complications includingnonunion, neurovascular damage, implant malfunction,
disease transmission by allograft, glenohumeral arthritis,and increased cost.20,21
Connolly22 in 1972 described an open surgical tech-nique to insert the infraspinatus muscle into aHill-Sachs defect to eliminate the engagement of theHill-Sachs deformity. In 2004 Wolf and Pollack2
described an arthroscopic approach to insert the infra-spinatus muscle into a Hill-Sachs deformity and usedthe term “remplissage” (French for “filling”) for thisprocedure. Their technique quickly gained in popularitybecause of its simplicity, good clinical outcome, lowcomplication rate, low cost, and lack of requirement foradditional implant or graft material.23-27 The remplis-sage technique uses a nonanatomic solution to treat theHill-Sachs lesion and stabilize the glenohumeral joint.The technique requires tethering of the infraspinatus,which has raised the concern of loss of internal rotation.Despite this concern, no significant loss of internalrotation has been found in patients who have under-gone this procedure.23-27
Koo et al.3 described a modification of the classicremplissage procedure using the double-pulley technique.This technique potentially offers the advantage ofproviding a large footprint fixation and firmly setting theinfraspinatus tendon into the Hill-Sachs defect. Theirgroup of patients showed good outcomes with no loss ofinternal rotation.The technique described in our report is a modification
of the double-pulley technique using Healix Transtendanchors through the posterior cannula. This modificationhas several advantages, including the ability to perform theentire technique while viewing in the glenohumeral joint,thus eliminating the need to alternate the view betweenthe glenohumeral joint and the subacromial space. This inturn eliminates the need to use spinal needles andmultipleportals, which potentially make this procedure more ac-curate. Most importantly, this modification makes the
Fig 4. Second anchor insertion. This anchor is inserted in thesame manner as the first but at the superior aspect of the Hill-Sachs lesion. One limb from each suture is tied together in adouble-pulley fashion to fill the Hill-Sachs defect with theinfraspinatus tendon.
Fig 5. After both limbs have been tied together, the infra-spinatus tendon in nicely positioned into the Hill-Sachs defect.Joint congruency and stability have been restored.
e308 N. PARNES ET AL.
surgical technique simpler and, in our experience, signif-icantly reduces surgical time. We believe that using theHealix Transtend anchor modification of the double-pulley remplissage technique allows a large footprint fix-ation of the infraspinatus tendon into the Hill-Sachs defectin a simple, accurate, time-saving way.
References1. Yiannakopoulos CK, Mataragas E, Antonogiannakis E.
A comparison of the spectrum of intra-articular lesions inacute and chronic anterior shoulder instability. Arthroscopy2007;23:985-990.
2. Wolf EM, Pollack ME. Hill-Sachs “remplissage”: Anarthroscopic solution for the engaging Hill-Sachs lesion(SS-32). Arthroscopy 2004;20:e14-e15 (abstr).
3. Koo SS, Burkhart SS, Ochoa E. Arthroscopic double-pulley remplissage technique for engaging Hill-Sachs le-sions in anterior shoulder instability repairs. Arthroscopy2009;25:1343-1348.
4. Bankart ASB. The pathology and treatment of recurrentdislocations of the shoulder joint. Br J Surg 1938;26:23-29.
5. Hill HA, Sachs MD. The grooved defect of the humeralhead: A frequently unrecognized complication of dislo-cations of the shoulder joint. Radiology 1940;35:690-700.
6. Burkhart SS, De Beer JF. Traumatic glenohumeral bonedefects and their relationship to failure of arthroscopicBankart repairs. Arthroscopy 2000;16:677-694.
7. Rowe CR, Zarins B, Ciullo JV. Recurrent anterior dislo-cation of the shoulder after surgical repair. Apparentcauses of failure and treatment. J Bone Joint Surg Am1984;66:159-168.
8. Lynch JR, Clinton JM, Dewing CB, Warme WJ,Matsen FA III. Treatment of osseous defects associatedwith anterior shoulder instability. J Shoulder Elbow Surg2009;18:317-328.
9. Warner JJ, BowenMK,DengXH,HannafinJA,ArnoczkySP,Warren RF. Articular contact patterns of the normal gleno-humeral joint. J Shoulder Elbow Surg 1998;7:381-388.
10. Boileau P, Villalba M, Hery JY, Balg F, Ahrens P,Neyton L. Risk factors for recurrence of shoulder insta-bility after arthroscopic Bankart repair. J Bone Joint SurgAm 2006;88:1755-1763.
11. Cetik O, Uslu M, Ozsar BK. The relationship between Hill-Sachs lesion and recurrent anterior shoulder dislocation.Acta Orthop Belg 2007;73:175-178.
12. Gerber C, Lambert SM. Allograft reconstruction ofsegmental defects of the humeral head for the treatmentof chronic locked posterior dislocation of the shoulder.J Bone Joint Surg Am 1996;78:376-382.
13. Kazel MD, Sekiya JK, Greene JA, Bruker CT. Percuta-neous correction (humeroplasty) of humeral head defects(Hill-Sachs) associated with anterior shoulder instability:A cadaveric study. Arthroscopy 2005;21:1473-1478.
14. Snir N, Wolfson TS, Hamula MJ, Gyftopoulos S,Meislin RJ. Arthroscopic anatomic humeral head recon-struction with osteochondral allograft transplantation forlarge Hill-Sachs lesions. Arthrosc Tech 2013;2:e289-e293.
15. Kropf EJ, Sekiya JK. Osteoarticular allograft trans-plantation for large humeral head defects in gleno-humeral instability. Arthroscopy 2007;23:322.e1-322.e5.
16. Boileau P, Bicknell RT, El Fegoun AB, Chuinard C.Arthroscopic Bristow procedure for anterior instability inshoulders with a stretched or deficient capsule: The “belt-and-suspenders” operative technique and preliminaryresults. Arthroscopy 2007;23:593-601.
17. Ghodadra N, Gupta A, Romeo AA, et al. Normalization ofglenohumeral articular contact pressures after Latarjet oriliac crest bone-grafting. J Bone Joint Surg Am 2010;92:1478-1489.
18. Provencher MT, Ghodadra N, LeClere L, Solomon DJ,Romeo AA. Anatomic osteochondral glenoid reconstruc-tion for recurrent glenohumeral instability with glenoiddeficiency using a distal tibia allograft. Arthroscopy2009;25:446-452.
19. Weber BG, Simpson LA, Hardegger F. Rotational humeralosteotomy for recurrent anterior dislocation of theshoulder associated with a large Hill-Sachs lesion. J BoneJoint Surg Am 1984;66:1443-1450.
21. Green A, Norris TR. Shoulder arthroplasty for advancedglenohumeral arthritis after anterior instability repair.J Shoulder Elbow Surg 2001;10:539-545.
22. Connolly JF. Humeral head defects associated withshoulder dislocationsdTheir diagnostic and surgical sig-nificance. Instr Course Lect 1972;21:42-54.
23. Park MJ, Tjoumakaris FP, Garcia G, Patel A, Kelly JD IV.Arthroscopic remplissage with Bankart repair for thetreatment of glenohumeral instability with Hill-Sachsdefects. Arthroscopy 2011;27:1187-1194.
24. Zhu YM. Arthroscopic Bankart repair combined withremplissage technique for the treatment of anteriorshoulder instability with engaging Hill-Sachs lesion: Areport of 49 cases with a minimum 2-year follow-up. Am JSports Med 2011;39:1640-1647.
25. Haviv B, Mayo L, Biggs D. Outcomes of arthroscopic“remplissage”: Capsulotenodesis of the engaging largeHill-Sachs lesion. J Orthop Surg Res 2011;6:29.
26. Boileau P, O’Shea K, Vargas P, Pinedo M, Old J,Zumstein M. Anatomical and functional results afterarthroscopic Hill-Sachs remplissage. J Bone Joint Surg Am2012;94:618-626.
27. Franceschi F, Papalia R, Rizzello G, et al. RemplissagerepairdNew frontiers in the prevention of recurrentshoulder instability: A 2-year follow-up comparativestudy. Am J Sports Med 2012;40:2462-2469.
The Double-Pulley Anatomic Technique for Type IISLAP Lesion Repair
Nata Parnes, M.D., Mario Ciani, D.C., Brian Carr, M.D., and Paul Carey, M.D.
Abstract: The annual incidence and number of repairs of SLAP lesions in the United States are constantly increasing.Surgical repairs of type II SLAP lesions have overall good success rates. However, a low satisfaction rate and low rate ofreturn to preinjury level of play remain a challenge with elite overhead and throwing athletes. Recent anatomic studiessuggest that current surgical techniques over-tension the biceps anchor and the superior labrum. These studies suggestthat restoration of the normal anatomy will improve clinical outcomes and sports performance. We present a “double-pulley” technique for arthroscopic fixation of type II SLAP lesions. In this technique the normal anatomy is respected bypreserving the mobility of the articular aspect of the superior labrum while reinforcing the biceps anchor and its posteriorfibers medially.
High physical demands and training requirementsmake SLAP tears a common cause of shoulder pain
and disability among athletes involved in overhead activ-ities.1 The annual incidence andnumber of repairs of SLAPlesions in the United States are constantly increasing.2
Multiple arthroscopic type II SLAP lesion repairtechniques have been described, with good to excellentoutcomes in most cases. However, the results inthrowing or overhead athletes are much less satisfyingespecially because of residual pain, stiffness, and a poorreturn to preinjury level of performance.3
Most of the arthroscopic repair techniques focus onthe stability of the superior labrum fixation and less onrestoration of the patient’s anatomy. Better under-standing and restoration of the native anatomy willprobably improve clinical outcomes and rates of returnto preinjury level of performance.4
Recent anatomic studies have improved our under-standing of the anatomic alterations that result from
SLAP tears and the normal anatomy of the long head ofbiceps tendon footprint insertion to the upper labrumand supraglenoid tubercle. These studies have drawnsome guidelines for optimal SLAP lesion repair tech-nique.5,6 In this article we describe a “double-pulley”technique for anatomic repair of the superior labrumand biceps anchor using these guidelines (Tables 1 and2).
Surgical TechniqueThis technique was developed by the first author
(N.P.). It uses the double-pulley suture configurationfor type II SLAP lesion repair. The patient is placed inthe beach-chair position using a Spider Limb Positioner(Tenet Medical, Calgary, Alberta, Canada) to hold thearm in the desired position. A 30� arthroscope isintroduced into the glenohumeral joint through astandard posterior portal. An anterosuperior portal isestablished high in the rotator interval region using aspinal needle by an outside-in technique. The needle isreplaced with an 8.25-mm arthroscopic shouldercannula.A complete diagnostic arthroscopy of the gleno-
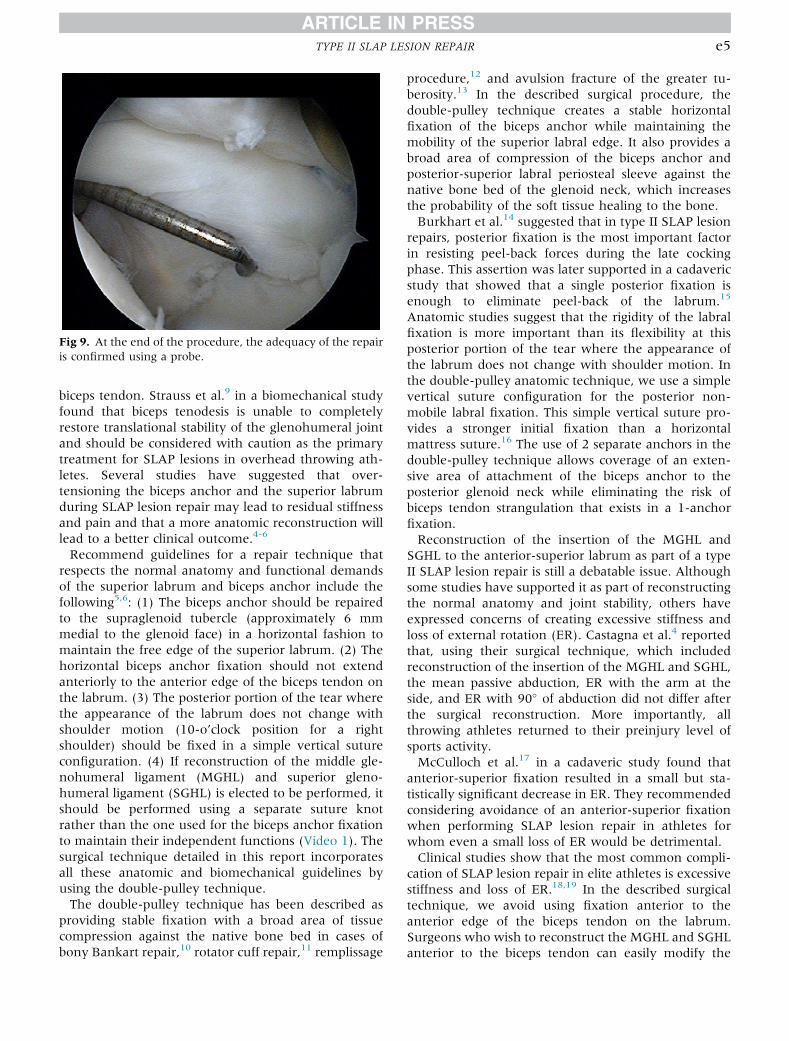
humeral joint is performed. Associated intra-articularpathology is documented and addressed as indicated.Then, by use of a probe, the type II SLAP lesion isconfirmed by the existence of a complete detachmentof the biceps anchor from the supraglenoid tubercle(Fig 1). Once the lesion is verified, a transerotator cuffportal is created medial to the rotator cuff cable (at themusculotendinous junction) using a spinal needle asdescribed by O’Brien et al.7
From the Tri County Orthopedic Center (N.P.), Carthage, New York;Clarkson University (M.C.), Potsdam, New York; and Department of Ortho-paedic Surgery, Guthrie Army Health Clinic (B.C., P.C.), Fort Drum, NewYork, U.S.A.
The authors report that they have no conflicts of interest in the authorshipand publication of this article.
Received February 16, 2015; accepted May 21, 2015.Address correspondence to Paul Carey, M.D., Department of Orthopaedic
Surgery, Guthrie Army Health Clinic, 11050 Mt Belvedere Rd, Fort Drum,NY 13602-5004, U.S.A. E-mail: [email protected]
Published by Elsevier Inc. on behalf of the Arthroscopy Association of NorthAmerica
With the arthroscope placed in the posterior portal, a4.5-mm shaver is used through the anterosuperiorportal to debride the superior glenoid neck to bleedingbone and the edge of the superior labrum as indicated(Fig 2). Through a smooth cannula placed in the transerotator cuff portal, a Suturefix 1.9-mm double-loadedanchor (Smith & Nephew, Andover MA) is placed atthe 10-o’clock position for a right shoulder (Fig 3). Thesurgeon retrieves 3 suture arms through the ante-rosuperior portal, leaving 1 suture end in the transerotator cuff portal. Viewing through the transerotatorcuff portal, the surgeon uses a 45� right lasso-loop devicethrough the posterior portal to shuttle the remainingsuture arm through the superior-posterior labrum. Thesuture is passed at a point where the position of thelabrum does not change with shoulder motion. With thearthroscope placed in the posterior portal, an arthro-scopic simple vertical knot-tying technique is used
through the transerotator cuff portal (Fig 4). The 45�
right lasso-loop device is used again through the poste-rior portal to shuttle the other 2 arms of the secondsuture on the anchor through the superior-posteriorlabrum (Fig 5). The arthroscope is transferred to theposterior portal. Then, by use of the anterosuperiorportal, a Suturefix 1.7-mm single-loaded anchor (Smith& Nephew) is placed on the glenoid rim in line with theanterior edge of the biceps insertion (Fig 5). Both suturearms are retrieved through the transerotator cuff portal.A 45� left lasso-loop device is used through the ante-rosuperior portal to shuttle the 2 arms through thesuperior-anterior labrum in line with the anterior edgeof the biceps tendon.Using a suture manipulator, the surgeon retrieves the
4 limbs of the 2 sutures through the transerotator cuffportal, taking care to retrieve the suture limbs from theanterior anchor superior to the biceps tendon (Fig 6).
1. Position the patient in the beach-chair position.2. Perform diagnostic arthroscopy through the posterior portal and anterior portal (place 8.5-mm cannulas in both portals).3. Use a spinal needle and No. 11 blade to place a trans-cuff portal medial to the rotator cuff cable while viewing from posterior (place a 5.5-mm
smooth cannula over a switching stick).4. Use a rasp and 4.5-mm shaver to prepare the superior glenoid neck and superior labrum.5. Through the trans-cuff portal, place a Suturefix 1.9-mm double-loaded anchor at the 10-o’clock position (right shoulder).6. Use a shuttling device to retrieve 1 arm of the suture from the anchor through the superior-posterior labrum.7. Through the trans-cuff portal, use an arthroscopic simple vertical knot-tying technique to fix the superior-posterior labrum.8. Through the posterior portal, use a shuttling device to retrieve the 2 arms of the other suture on the anchor through the superior-posterior
labrum.9. Through the anterior portal, place a Suturefix 1.7-mm single-loaded anchor in line with the anterior edge of the biceps tendon.10. Through the anterior portal, use a shuttling device to retrieve the 2 arms of the suture on the anchor through the superior-anterior labrum.11. Retrieve the 4 limbs through the trans-cuff portal (superior to the biceps tendon).12. Through the trans-cuff cannula, tie the sutures from the 2 anchors using the double-pulley technique.
Table 2. Indications, Advantages, Disadvantages, Pearls, and Pitfalls of Arthroscopic Double-Pulley Type II SLAP Lesion Repair
IndicationsSymptomatic type II SLAP lesions in patients aged <40 yr with normal biceps tendons.
AdvantagesStable horizontal fixation is achieved while maintaining the freedom of the superior labral edge.The technique provides a broad area of compression of the biceps anchor and posterior-superior labral periosteal sleeve against the native
bone bed of the glenoid neck.The technique is suitable for large and complex type II SLAP tears.A watertight repair of the posterior-superior labral periosteal sleeve is produced; this is especially important when a paralabral cyst is present.Using 2 separate anchors eliminates the risk of biceps tendon strangulation.
DisadvantagesThe procedure is longer and has higher costs than a single-anchor repair.Failure of 1 of the 2 anchors will lead to total failure of the double-pulley fixation.
PearlsUse a spinal needle in an outside-in technique to place the transerotator cuff portal medial to the supraspinatus cable to avoid damage to the
tendon.Place the posterior anchor on the glenoid rim at a point where the appearance of the labrum does not change with shoulder motion
(10-o’clock position for a right shoulder) and not at the biceps base.Remember that the horizontal biceps anchor fixation should not extend anteriorly to the anterior edge of the biceps tendon on the labrum.Verify that both sutures are sliding freely before performing the double-pulley part of the technique.
PitfallsWhen drilling the glenoid rim for the anterior anchor placement, be careful not to drill into the posterior anchor.If MGHL and SGHL reconstruction is elected, avoid fixing them with the same suture used for the biceps fixation.
MGHL, middle glenohumeral ligament; SGHL, superior glenohumeral ligament.
e2 N. PARNES ET AL.
One suture limb for each anchor is chosen to be coupledin a double-pulley configuration (Fig 7). Once thedouble pulley is completed, fixation of the biceps an-chor is completed with tightening of non-sliding knotson the remaining suture limbs of each anchor (Fig 8).At the end of the procedure, the adequacy of the repairis confirmed with a probe (Fig 9). The shoulder is takenthrough a full range of motion to rule out tension onthe repair that can lead to stiffness.
The postoperative protocol consists of sling immobi-lization for 4 weeks. Early pendulum shoulder exercisesand distal range-of-motion exercises involving theelbow, wrist, and hand are initiated immediately. Pas-sive range of motion of the shoulder should be startedduring the first 2 weeks postoperatively, with a gradualprogression of forward flexion from 90� to 150� over aperiod of 6 weeks. Active range of motion of theshoulder and a progressive strengthening program startat 6 weeks after surgery. Return to unrestricted activ-ities, including vigorous sports, is permitted at 6 monthspostoperatively.
Fig 1. With viewing through the posterior portal, the type IISLAP lesion is confirmed by the existence of a completedetachment of the biceps anchor from the supraglenoid tu-bercle using a probe. This image and Figures 2-9 show thesame left shoulder with the patient in the beach-chairposition.
Fig 2. With viewing through the posterior portal, a 4.5-mmshaver is used through the anterosuperior portal to debridethe superior glenoid neck to bleeding bone and the edge of thesuperior labrum as indicated.
Fig 4. An arthroscopic simple vertical knot is used to fix theposterior portion of the tear where the appearance of thearticular edge of the labrum does not change with shouldermotion.
Fig 3. With viewing through the posterior portal, a Suturefix1.9-mm double-loaded anchor is placed at the 10-o’clockposition through a transerotator cuff portal.
TYPE II SLAP LESION REPAIR e3
DiscussionThe disappointing outcomes of type II SLAP lesion
repair in elite athletes motivated surgeons to furtherinvestigate alternative solutions for this injury. Patientsubjective satisfaction levels and rates of return toprevious level of sports activity have been found to bebetter with biceps tenodesis8 when compared withSLAP lesion repair using suture anchor fixation. Pre-viously described techniques for type II SLAP lesion
repair mostly addressed labral stability and not theanatomic restoration of the biceps anchor and superiorlabrum.Recent anatomic and biomechanical studies have
improved our understanding of the pathologic changesthat occur with a SLAP tear and the normal anatomyand function of the superior labrum and long head of
Fig 5. The 2 arms of the second suture on the anchor areshuttled through the superior-posterior labrum. By use of theanterosuperior portal, a Suturefix 1.7-mm single-loaded an-chor is placed on the glenoid neck in line with the anterioredge of the long head of the biceps tendon.
Fig 6. A shuttling device is used to retrieve the 2 arms of thesuture on the anterior anchor through the superior-anteriorlabrum. The surgeon retrieves the 4 limbs of the 2 suturesthrough the transerotator cuff portal, paying attention toretrieve the suture limbs from the anterior anchor superior tothe biceps tendon to prevent entanglement.
Fig 7. One suture limb for each anchor is chosen to becoupled in a double-pulley configuration.
Fig 8. Fixation of the long head of the biceps tendon anchor iscompleted with tightening of non-sliding knots on theremaining suture limbs of each anchor. As viewed fromabove, the completed double-pulley construct secures thebiceps anchor fibers medially between 2 suture anchors.
e4 N. PARNES ET AL.
biceps tendon. Strauss et al.9 in a biomechanical studyfound that biceps tenodesis is unable to completelyrestore translational stability of the glenohumeral jointand should be considered with caution as the primarytreatment for SLAP lesions in overhead throwing ath-letes. Several studies have suggested that over-tensioning the biceps anchor and the superior labrumduring SLAP lesion repair may lead to residual stiffnessand pain and that a more anatomic reconstruction willlead to a better clinical outcome.4-6
Recommend guidelines for a repair technique thatrespects the normal anatomy and functional demandsof the superior labrum and biceps anchor include thefollowing5,6: (1) The biceps anchor should be repairedto the supraglenoid tubercle (approximately 6 mmmedial to the glenoid face) in a horizontal fashion tomaintain the free edge of the superior labrum. (2) Thehorizontal biceps anchor fixation should not extendanteriorly to the anterior edge of the biceps tendon onthe labrum. (3) The posterior portion of the tear wherethe appearance of the labrum does not change withshoulder motion (10-o’clock position for a rightshoulder) should be fixed in a simple vertical sutureconfiguration. (4) If reconstruction of the middle gle-nohumeral ligament (MGHL) and superior gleno-humeral ligament (SGHL) is elected to be performed, itshould be performed using a separate suture knotrather than the one used for the biceps anchor fixationto maintain their independent functions (Video 1). Thesurgical technique detailed in this report incorporatesall these anatomic and biomechanical guidelines byusing the double-pulley technique.The double-pulley technique has been described as
providing stable fixation with a broad area of tissuecompression against the native bone bed in cases ofbony Bankart repair,10 rotator cuff repair,11 remplissage
procedure,12 and avulsion fracture of the greater tu-berosity.13 In the described surgical procedure, thedouble-pulley technique creates a stable horizontalfixation of the biceps anchor while maintaining themobility of the superior labral edge. It also provides abroad area of compression of the biceps anchor andposterior-superior labral periosteal sleeve against thenative bone bed of the glenoid neck, which increasesthe probability of the soft tissue healing to the bone.Burkhart et al.14 suggested that in type II SLAP lesion
repairs, posterior fixation is the most important factorin resisting peel-back forces during the late cockingphase. This assertion was later supported in a cadavericstudy that showed that a single posterior fixation isenough to eliminate peel-back of the labrum.15
Anatomic studies suggest that the rigidity of the labralfixation is more important than its flexibility at thisposterior portion of the tear where the appearance ofthe labrum does not change with shoulder motion. Inthe double-pulley anatomic technique, we use a simplevertical suture configuration for the posterior non-mobile labral fixation. This simple vertical suture pro-vides a stronger initial fixation than a horizontalmattress suture.16 The use of 2 separate anchors in thedouble-pulley technique allows coverage of an exten-sive area of attachment of the biceps anchor to theposterior glenoid neck while eliminating the risk ofbiceps tendon strangulation that exists in a 1-anchorfixation.Reconstruction of the insertion of the MGHL and
SGHL to the anterior-superior labrum as part of a typeII SLAP lesion repair is still a debatable issue. Althoughsome studies have supported it as part of reconstructingthe normal anatomy and joint stability, others haveexpressed concerns of creating excessive stiffness andloss of external rotation (ER). Castagna et al.4 reportedthat, using their surgical technique, which includedreconstruction of the insertion of the MGHL and SGHL,the mean passive abduction, ER with the arm at theside, and ER with 90� of abduction did not differ afterthe surgical reconstruction. More importantly, allthrowing athletes returned to their preinjury level ofsports activity.McCulloch et al.17 in a cadaveric study found that
anterior-superior fixation resulted in a small but sta-tistically significant decrease in ER. They recommendedconsidering avoidance of an anterior-superior fixationwhen performing SLAP lesion repair in athletes forwhom even a small loss of ER would be detrimental.Clinical studies show that the most common compli-
cation of SLAP lesion repair in elite athletes is excessivestiffness and loss of ER.18,19 In the described surgicaltechnique, we avoid using fixation anterior to theanterior edge of the biceps tendon on the labrum.Surgeons who wish to reconstruct the MGHL and SGHLanterior to the biceps tendon can easily modify the
Fig 9. At the end of the procedure, the adequacy of the repairis confirmed using a probe.
TYPE II SLAP LESION REPAIR e5
surgical technique by using a double-loaded anchorinstead of the single-loaded anchor at the anterior-superior glenoid area. The extra suture on the anchorcan be used to perform a vertical simple stitch at thelevel of the insertion of the MGHL and SGHL.There is no consensus regarding the use of a transe
rotator cuff portal during SLAP lesion repair. Thedouble-pulley anatomic technique can be performed asdescribed or without the use of the transerotator cuffportal depending on the surgeon’s preference. Ifavoiding the use of the transerotator cuff portal iselected, we recommend tying the double-pulley knotsthrough the anterior portal while viewing from theposterior portal so that the knot will be medial to thebiceps tendon insertion. This knot position reduces therisk of rotator cuff impingement against it.This report describes an arthroscopic double-pulley
technique to repair type II SLAP lesions. This tech-nique is based on recent anatomic and biomechanicalfindings. Further clinical outcome studies are requiredto validate the theoretical benefits of this technique.
AcknowledgmentThe authors thank Itai Parnes for technical support.
References1. Knesek M, Skendzel JG, Dines JS, Altchek DW, Allen AA,
Bedi A. Diagnosis and management of superior labralanterior posterior tears in throwing athletes. Am J SportsMed 2013;41:444-460.
2. Onyekwelu I, Khatib O, Zuckerman JD, Rokito AS,Kwon YW. The rising incidence of arthroscopic superiorlabrum anterior and posterior (SLAP) repairs. J ShoulderElbow Surg 2012;21:728-731.
3. Park JY, Chung SW, Jeon SH, Lee JG, Oh KS. Clinical andradiological outcomes of type 2 superior labral anteriorposterior repairs in elite overhead athletes. Am J SportsMed 2013;41:1372-1379.
4. Castagna A, De Giorgi S, Garofalo R, Tafuri S, Conti M,Moretti B. A new anatomic technique for type II SLAPrepair. Knee Surg Sports Traumatol Arthrosc in press, avail-able online 21 November, 2014. doi:10.1007/s00167-014-3440-4.
5. Arai R, Kobayashi M, Harada H, et al. Anatomical studyfor SLAP lesion repair. Knee Surg Sports Traumatol Arthrosc2014;22:435-441.
6. Bain GI, Galley IJ, Singh C, Carter C, Eng K. Anatomicstudy of the superior glenoid labrum. Clin Anat 2013;26:367-376.
7. O’Brien SJ, Allen AA, Coleman SH, Drakos MC. Thetrans-rotator cuff approach to SLAP lesions: Technicalaspects for repair and a clinical follow-up of 31 patients ata minimum of 2 years. Arthroscopy 2002;18:372-377.
8. Boileau P, Parratte S, Chuinard C, Roussanne Y, Shia D,Bicknell R. Arthroscopic treatment of isolated type IISLAP lesions: Biceps tenodesis as an alternative to rein-sertion. Am J Sports Med 2009;37:929-936.
9. Strauss EJ, Salata MJ, Sershon RA, et al. Role of the su-perior labrum after biceps tenodesis in glenohumeralstability. J Shoulder Elbow Surg 2014;23:485-491.
10. Zhang J, Jiang C. A new “double-pulley” dual-row tech-nique for arthroscopic fixation of bony Bankart lesion.Knee Surg Sports Traumatol Arthrosc 2011;19:1558-1562.
11. Arrigoni P, Brady PS, Burkhart SS. The double-pulleytechnique for double-row rotator cuff repair. Arthroscopy2007;23:675.e1-675.e4.
12. Koo SS, Burkhart SS, Ochoa E. Arthroscopic double-pulley remplissage technique for engaging Hill-Sachs le-sions in anterior shoulder instability repairs. Arthroscopy2009;25:1343-1348.
13. Murena L, Canton G, Falvo DA, Genovese EA, Surace MF,Cherubino P. The “double-pulley” technique for arthro-scopic fixation of partial articular-side bony avulsion ofthe supraspinatus tendon: A rare case of bony PASTAlesion. Arthrosc Tech 2012;2:e9-e14.
14. Burkhart SS, Morgan CD, Kibler WB. The disabledthrowing shoulder: Spectrum of pathology. Part II: Eval-uation and treatment of SLAP lesions in throwers.Arthroscopy 2003;19:531-539.
15. Seneviratne A, Montgomery K, Bevilacqua B, Zikria B.Quantifying the extent of a type II SLAP lesion required tocause peel-back of the glenoid labrumdA cadavericstudy. Arthroscopy 2006;22:1163.e1-1163.e6.
16. Yoo JC, Ahn JH, Lee SH, et al. A biomechanical com-parison of repair techniques in posterior type II superiorlabral anterior and posterior (SLAP) lesions. J ShoulderElbow Surg 2008;17:144-149.
17. McCulloch PC, Andrews WJ, Alexander J, Brekke A,Duwani S, Noble P. The effect on external rotation ofan anchor placed anterior to the biceps in type 2 SLAPrepairs in a cadaveric throwing model. Arthroscopy2013;29:18-24.
18. Brockmeier SF, Voos JE, Williams RJ III, Altchek DW,Cordasco FA, Allen AA. Outcomes after arthroscopicrepair of type-II SLAP lesions. J Bone Joint Surg Am2009;91:1595-1603.
19. Provencher MT, McCormick F, Dewing C, McIntire S,Solomon D. A prospective analysis of 179 type 2 superiorlabrum anterior and posterior repairs: Outcomes andfactors associated with success and failure. Am J Sports Med2013;41:880-886.