24
Assessment of Clinical Performance Guidelines for Assessors and Applicants

Assessment ofClinical PerformanceGuidelines for Assessors and Applicants

ContentsGuidelines for Assessors and Applicants 3
> Introduction> Purpose of the ACP> Format> Clinical responsibility> Insurance> Role of the Assessor> Role of the Moderator> Role of the GOSC representative> Preassessment talk> Equality and diversity> Conduct> Questioning> Behaviour> Dealing with bias> ‘On the day’ performance> Risk> Decision making> Report writing
Appendix 1 10
> Osteopathic Practice Standards Checklist
Appendix 2 17
> Evaluation Form
Appendix 3 21
> Outcome Report
Assessment of Clinical Performance 2

Introduction
1. The Assessment of Clinical Performance(ACP) assesses an applicant’s ability to fulfilthe Osteopathic Practice Standards. Thesestandards can be accessed on the GeneralOsteopathic Council (GOsC) websitewww.osteopathy.org.uk
Purpose of the ACP
2. The ACP is the second part of theassessment required for registration with theGOsC. It is necessary to have completed theFurther Evidence of Practice Questionnairebefore progressing to this assessment.Details of this can be found on the GOsCwebsite.
Format
3. The ACP involves the applicant managingtwo new patients in a clinical setting over aperiod of around three hours. This includestaking a case history, performing anynecessary examinations and undertakingappropriate treatment (or referral).
4. Before the start of the ACP, all members ofthe assessment team will be provided withthe assessment summary from theapplicant’s Further Evidence of PracticeQuestionnaire.
5. A maximum of four applicants can beassessed in one day: two in the morning andtwo in the afternoon.
6. The assessment team comprises twoassessors and one moderator. They aresupported by a GOsC representative, who isacting in an administrative capacity only andwill not take part in the ACP.
7. Each assessor will observe the applicantwith one patient, and the moderator willsample all patients.
8. The assessor and the moderator willundertake a period of questioning of theapplicant in a separate room following thecase history and clinical examination.
9. After the applicant has seen both patients,the assessment team led by the moderatorwill discuss the findings and come to aconsensus agreement on whether theapplicant has passed or failed theassessment.
10. An evaluation form for recording the findingsof the assessments is attached as Appendix 2.This is supported by a checklist for guidancein Appendix 1.
Clinical responsibility
11. The GOsC assessment team of twoassessors and one moderator hold clinicalresponsibility for the patients seen/treated bythe applicants they assess.
12. One member of the assessment team mustbe present to observe the applicant with thepatients at all times in order to hold clinicalresponsibility, and that responsibility must beclear to all parties.
13. Assessors and moderators will be mindful toavoid excessive intrusion. In addition tobeing present to observe the applicant,assessors or moderators may need to speakwith the patient independently of theapplicant to cover all aspects of clinicalresponsibility.
14. Key aspects of clinical responsibility include:> The patient understands the content and
approach to the session.> The patients’ expectations of the session
are understood.> The patient is aware of how to raise
concerns and complaints.> The patient provides informed consent
throughout the session.> The patient understands what their next
steps are (relating to followup, treatment,referral and aftercare advice).
> The patient is offered a copy of theirpatient notes from the session. (The
Assessment of Clinical Performance - Guidelines for Assessors and Applicants 3

original notes will be stored at the clinic.The GOsC will hold a copy of the redactedpatient information.)
> Assessors and/or moderators have a dutyto intervene and stop the session if theapplicant is presenting a risk to thepatient.
> The patient must be given a patientinformation sheet.
Insurance
15. All assessors and moderators must beregistered with the GOsC and haveappropriate professional indemnity insuranceas required by the GOsC. The GOsCensures that the process is coveredseparately by its own insurance.
Role of the Assessor
16. The role of the assessor is to gain sufficientevidence to make a judgement on the clinicalcompetence of the applicant.
17. Each applicant will see two new patients.One assessor will take the lead during theconsultation with the first new patient; theother assessor takes the lead during theconsultation with the second new patient.There will generally only be two applicantsbeing assessed at any one time unless theGOsC has agreed otherwise.
18. Assessors are expected to collect sufficientevidence upon which to make a reliableevaluation of an applicant’s performance.
19. Assessors will have one major opportunity toquestion the applicant during the clinicalencounter with the patient, which is after thecase history and clinical examination havebeen performed.
20. The questioning will take place in adesignated room away from the treatmentroom and out of earshot of the patient.Questioning must be conducted in thepresence of a second person, preferably themoderator. It is the responsibility of the assessor to ensure that the moderator ispresent. The assessor must allow time for
the applicant to gather their thoughts prior to the initiation of the period of questioning.
21. The applicant will be required to present a briefsummary of the main features of the casehistory; the range of diagnostic hypotheses;the rationale for their clinical examinations; andthe significance of their clinical findings andhow these inform their diagnostic conclusionsand osteopathic diagnosis. Questioning willalso explore the proposed treatment andmanagement planning and any specific selfcare measures to be discussed with thepatient in the management of their complaint.It is important that the applicant is specific about their differential diagnoses, and can explain the rationale for their choices and the means by which they will try to differentiate between potential causes in their examination.
22. In simple cases, an assessor may ask a few‘hypothetical’ questions that link to thepatient, to enable the applicant todemonstrate the full extent of theirknowledge base. This section of questioningmay be quite lengthy, but should notnormally exceed 15 minutes. Assessorsshould observe a sample of delivery oftreatment by the applicant to ascertain howthe patient is involved in the management oftheir complaint.
23. Assessors may ask questions at other timesfor clarification, but should do so sparingly,especially if this is in front of the patient or isinterrupting the applicant’s progress with theconsultation/treatment. It is important thatthe questioning should not impinge on thepatient’s wellbeing. This should be thepriority of both the applicant and assessorsat all times.
24. Assessors must ensure that they adequatelyrecord any findings made in the periods ofobservation and questioning. Thisinformation will subsequently be used toinform the evaluation of the applicant duringmoderation. If there are any problemsencountered by the applicant or assessors atany point, or if they would like clarification,they can speak to the moderator or theGOsC representative.
Assessment of Clinical Performance - Guidelines for Assessors and Applicants 4

Role of the Moderator
25. The role of the moderator is to ensure thatassessors on the team reach an informeddecision on the clinical competence of eachapplicant assessed. In order to do so, theywill need to collect evidence in the same way as assessors, to allow them to identifyareas that assessors may have missed and feed this in so that they have a clear understanding of the applicant’sperformance when it comes to moderatingthe decisions of the assessors.
26. The moderator’s role also includes:> acting as an applicant advocate to ensure
a fair assessment process for theapplicant, and ensuring that there is nounfair or harsh questioning from theassessors;
> ensuring that assessors are assessingagainst the GOsC’s Osteopathic PracticeStandards and not their own personalcriteria;
> facilitating discussion between assessorsduring moderation meetings and duringthe ACP, if necessary;
> sampling the assessors’ interaction withthe applicant, posing additional questionsif necessary, but not conducting their ownassessment of the applicant separately, toform their evaluation.
27. A moderator will have less time to spend witheach applicant and must allocate timeaccordingly in order to assess clinicalcompetence for each applicant.
28. The moderator will also be responsible forthe administration of the assessment team,including:> allocation of assessors to applicants;> ensuring the assessments keep to time;> conducting moderation meetings; > taking decisions relating to procedural
changes;> ensuring that the reports are finalised on
the day or to agreed timescales wherenecessary;
> ensuring that all the assessment teamhave reviewed the evaluation of the selfassessment questionnaire;
> summarising any areas in need ofexploration.
Role of the GOSCrepresentative
29. The role of the GOsC representative is tosupport the assessors and moderator inundertaking their functions. The GOsCrepresentative has no clinical responsibility.
30. The GOsC representative will:> make arrangements for the allocation of
applicants and patients;> provide assessors with all necessary
forms and information during theassessment;
> prepare the clinic rooms in advance of theassessment, including all special requestsfrom applicants;
> greet all applicants and show them to theclinic room;
> welcome patients on arrival;> show patients to the clinic room at the
appropriate time;> introduce patients to the assessment team
and the applicant at the appropriate times;> sit in on the period of questioning following
the case history taking and examination,and make notes on the discussion;
> show the patients back to the receptionarea;
> show the applicant out at the end of theprocess;
> observe the moderation sessions for allapplicants;
> make arrangements for lunch andrefreshments for assessors and applicants;
> ensure that there is a procedure in placeto arrange for a ‘backup’ patient as acontingency in case of a ‘no show’ on theday of the ACP. Alternatively, makearrangements for a candidate to undergoa viva voce with the assessment teamabout either question 7 from their FurtherEvidence of Practice Questionnaire orhypothetical cases;
> schedule another ACP when extremecircumstances dictate that it isunreasonable or impractical for anassessment, having started, to continue.
31. There should be no interaction/discussionbetween the GOsC representative and theapplicant during the assessment, unlessspecifically requested by an assessor ormoderator.
Assessment of Clinical Performance - Guidelines for Assessors and Applicants 5

Pre-assessment talk
32. Approximately 1015 minutes before the startof the assessment, the assessment teamshould introduce themselves to theapplicant, explain the process and clarify anyissues, such as identifying particular needs.
33. The following should be emphasised to theapplicant:> To focus on patient care, good
communication and developing patientrapport, and to remain professional andethical throughout the ACP;
> To demonstrate their reasoning skillsthroughout with clear justification fordecisions made;
> To keep to time and provide treatment,when appropriate;
> That they can take a few minutes togather their thoughts before presenting tothe assessors (and should inform theassessment team if they intend to do this);
> To discuss the working diagnosis beforestarting treatment;
> To ask for questions to be rephrased ifthey do not understand;
> To ask to discuss sensitive issues outsidethe treatment room if they feel that it is inthe best interests of the patient;
> To explain the rationale for their decisions,using relevant anatomical, physiologicaland osteopathic knowledge;
> To be accurate and specific when givingtheir differential diagnoses (for example,not to say ‘it is a gut problem’);
> To be accurate with terminology andrecognise the need to employ technicalterms with assessors, but to use lay termswhen explaining to patients.
Equality and diversity
34. The GOsC is committed to promotingequality of opportunity and access to theosteopathy profession. It therefore supportsan inclusive approach to applicants withparticular needs.
35. The responsibility is on the applicant toinform the GOsC, at the point of application,about any particular needs and providewritten evidence of these from a suitableauthority. This should include what
adjustments, adaptations or arrangementsthey require to be made. The GOsC, inconsultation with the applicant, willendeavour to accommodate theserequirements. The GOsC will inform theassessors of such arrangements.
36. In making their assessments, the assessorsshould ensure that their judgement is notaffected by their own personal beliefs andopinions, or by the applicant’s gender, ethnicorigin, sexual orientation, religious, culturaland political beliefs, physical disabilities orrequirements for reasonable adjustments.
Conduct
37. It is important that assessors are aware ofthe need to conduct themselves in a mannerthat is both professional and beyondreproach. Assessors should be aware of howtheir demeanour, actions and words may beperceived, and should take particular care inthis respect. They should particularly avoidbehaviours that may be interpreted as rude,discriminatory or aggressive and likely toundermine their integrity and that of theassessment process. The assessmentshould not be interrupted by theinappropriate use of mobile phones.
38. There should be no discussion betweenassessors regarding their evaluationfindings, in terms of the applicant’scompetence profile, while the examinationprocess is under way.
39. Discussion is permitted between assessorsregarding any competence areas where thelead assessor has been unable to locatesufficient evidence upon which to base anevaluation. The purpose of this discussionmust be to formulate a strategy to locatefurther evidence upon which to make adecision rather than to discuss any issueconcerning the applicant’s competence.This discussion must include the moderator.
Assessment of Clinical Performance - Guidelines for Assessors and Applicants 6

Questioning
40. The aim of questioning should be forassessors to observe the applicant’s clinicalperformance, and to seek evidence of therationale for their actions through questioningthat is relevant, fair, efficient and searching.
41. It is better to phrase questions simply and in‘bitesize’ chunks. Long and complexphrasing can be very unsettling and timewasting. It is usually less intrusive if oneassessor asks the majority of the questionsfor a given applicant, with the other assessor/moderator adding supplementary questions ifnecessary. It is important that questioning isclinically relevant and does not becomeskewed in favour of a particular assessor’sfavourite topic. Questions need to be askedthat sample the applicant’s underlyingknowledge base and clinical reasoning skills,but not to such an extent that the applicant’sinteraction with and management of theirpatient becomes adversely affected. Thisassessment needs to look globally at theapplicant’s clinical practice; it needs to bebalanced and not focus unduly on a specifictopic.
42. There should be progressively challengingbut not aggressive questioning, tempered bythe ability to recognise when an applicant is‘freezing’ owing to nervousness or istemporarily unsettled by direct questions. Ifan applicant is clearly having difficulties inreplying to questions it is better to moveaway from a particular line of questioning,and return to it later, perhaps framingquestions in a slightly different way. If directquestioning becomes too protracted, there isa possibility of distracting and underminingthe confidence of the applicant, which mayimpact on the rest of the assessment. This isparticularly so if there is intensivequestioning early in the assessment beforethe applicant has settled. It is oftennecessary to ‘ease into’ the questioning,covering some more basic concepts beforebuilding up to the more challengingquestioning.
43. It is also important to be aware of howapplicants are questioned in the presence oftheir patient. If the line of questioning is likelyto cause potential concern to the patient, orwill put the applicant in a difficult position, it
is always better to pursue this away from thepatient. The applicant should also beencouraged to ask to speak to the assessorsoutside the room if they feel the issues theyare discussing may upset the patient.
44. If it is deemed necessary to questionapplicants in front of the patient, care shouldbe taken to avoid undermining the patient’sconfidence in the applicant by questioningthat is too protracted or aggressive, or thatcauses the applicant to become obviouslyconfused and erratic.
45. If applicants appear not to understandparticular questions, the questions should beput again in another way.
46. It is important that applicants areencouraged to be specific and accurateabout their replies, especially wheredifferential diagnosis and the workingdiagnosis are concerned. It is not uncommonfor applicants to state vague diagnoses,such as ‘muscular problem’ or ‘heartproblem’, and in such cases the assessorneeds to ask the applicant to explain in moredetail what they are considering. Accuracywith terminology can sometimes be aproblem, and applicants need to be able toexplain in technical terms for the assessorsbut show an ability to use lay terms whengiving explanations to their patient.
Behaviour
47. Applicants who are under stress may behavein a range of different ways. Some becomevery quiet, some aggressive and otherspanic. It is necessary to be sensitive to thisand to reflect on why an applicant may bereacting in a certain way. Often somereassurance about the process may assistwith resolving such issues. It may benecessary for assessors to ‘take a deepbreath’ and ‘count to ten’ before reacting toovigorously to an applicant who initiallyappears aggressive or argumentative. Theoverriding consideration should be to givethe applicant the ‘benefit of the doubt’, butnot to a point where such behaviour becomes too obviously protracted, unreasonable or unprofessional.
Assessment of Clinical Performance - Guidelines for Assessors and Applicants 7

48. Assessors may find it helpful to reflect ontheir own personality and consider howcertain aspects may come across to anapplicant who will often be in a state ofheightened anxiety. This is not an attempt tomake assessors automatons, but isrecognising the potential for misinterpretationby applicants in a stressful situation. It isdesirable that assessors do not enter a clashof personality situation and should thereforeadopt, as far as is reasonable, a neutral butassertive approach.
49. Applicants who are behaving in a timidfashion may also be reacting to the stress ofthe situation. Assessors should look pasttheir initial impressions to seek evidence ofsuch an applicant’s ability. It is difficult forsome people to display overt confidence inan assessment situation, and someallowances can be made.
50. It is important to remember that assessorsare in a very much more powerful position inthe dynamics of this assessment. This bringswith it the responsibility to create theconditions, as far as is reasonable, forindividual applicants with varyingpersonalities and approaches to perform totheir potential.
Dealing with bias
51. Applicants should be reassured thatassessors are aware of the various forms ofpossible bias when assessing an individual’sperformance. The ACP is evaluated byconsidering the applicant’s performanceagainst each criterion (see Appendix 2)separately and making a judgement on eachaspect.
52. Assessors need to be sensitive to their ownbiases and preconceived ideas. This isespecially important during the ACP processwhere the ACP assessors will have theopportunity to review the outcomes of theprior written assessment, which may highlightareas of strengths and weaknesses. Thisstep is here to ensure that assessors areaware of any issues which may affect patientsafety and may need to be further exploredduring the assessment.
53. The assessment team should approach eachnew applicant with an open mind and shouldnot discuss the applicant prior to theassessment, as this may lead to assessorsmaking assumptions, either positive ornegative, about the likely performance of aparticular applicant. Applicants who areassumed to be poor in clinic may not begiven sufficient attention or opportunity toprove otherwise, while positive assumptionsabout applicants may lead to assessors notadequately sampling their underlyingknowledge, skills and rationale.
‘On the day’ performance
54. It is worth mentioning the potential inassessments for applicants who haveshown consistently borderline or poorperformance in the past to excel ‘on theday’. Conversely, applicants who mayperform consistently well in practice may dobadly in the assessment. It is necessary forassessors to be aware that sometimes‘good’ applicants are very selfcritical andcan be overanxious, leading to a poorperformance. This is exacerbated ifassessors pitch their questioning a little toorigorously too early on.
55. Assessors need to be aware also that someapplicants may give superficial responses toquestions, which may require challenging toascertain their underlying clinical reasoning.
Risk
56. If at any time an assessor thinks that anapplicant is presenting a risk to their patient,the applicant should be asked to leave theroom for discussion. If assessors feel that anapplicant is really unable to cope with theparticular patient and situation, it may benecessary to stop the assessment and toask the GOsC staff representative to liaisewith the clinic management to find someoneto take over the consultation.
Assessment of Clinical Performance - Guidelines for Assessors and Applicants 8

Decision making
57. Assessors’ decisions need to be fair andconsidered. There needs to be anappreciation of the complexity of the clinicalpractice process and a good rationale forthose decisions. The weighting andbalancing of different aspects of the clinicalperformance process needs to be taken intoaccount. Assessors need to look at theoverall performance on balance and not beunduly influenced by discrete areas of goodor bad performance, especially if thisrelates to an assessor’s favourite subjectareas.
58. Assessors should not judge applicants toomuch by what they would do themselves,since applicants will have had input frommany different sources during their trainingand experience of practice. The importantpoint is that the applicant has a reasonedrationale for what they are doing and theconclusions they arrive at.
59. Assessors should be careful not to providedirect feedback to applicants on the day ofthe assessment that may indicate theoutcome of their assessment.
Report writing
60. The moderator will compile a report for eachapplicant after the moderation meeting, andthis should reflect the applicant's ability tofulfil the Osteopathic Practice Standards asevidenced by the assessors’ completion ofthe evaluation form (Appendix 2) for eachpatient seen. The report should be finalisedand signed by the whole assessment team.The report should reflect the outcome of themoderation meeting and include thefollowing specific details:
> Whether the applicant passed or failed,and the reasons for failing, if applicable.
> Feedback to the applicant onstrengths/good practice and areas fordevelopment, which could form the basisof future continuing professionaldevelopment.
The report template is provided in Appendix 3.
Assessment of Clinical Performance - Guidelines for Assessors and Applicants 9
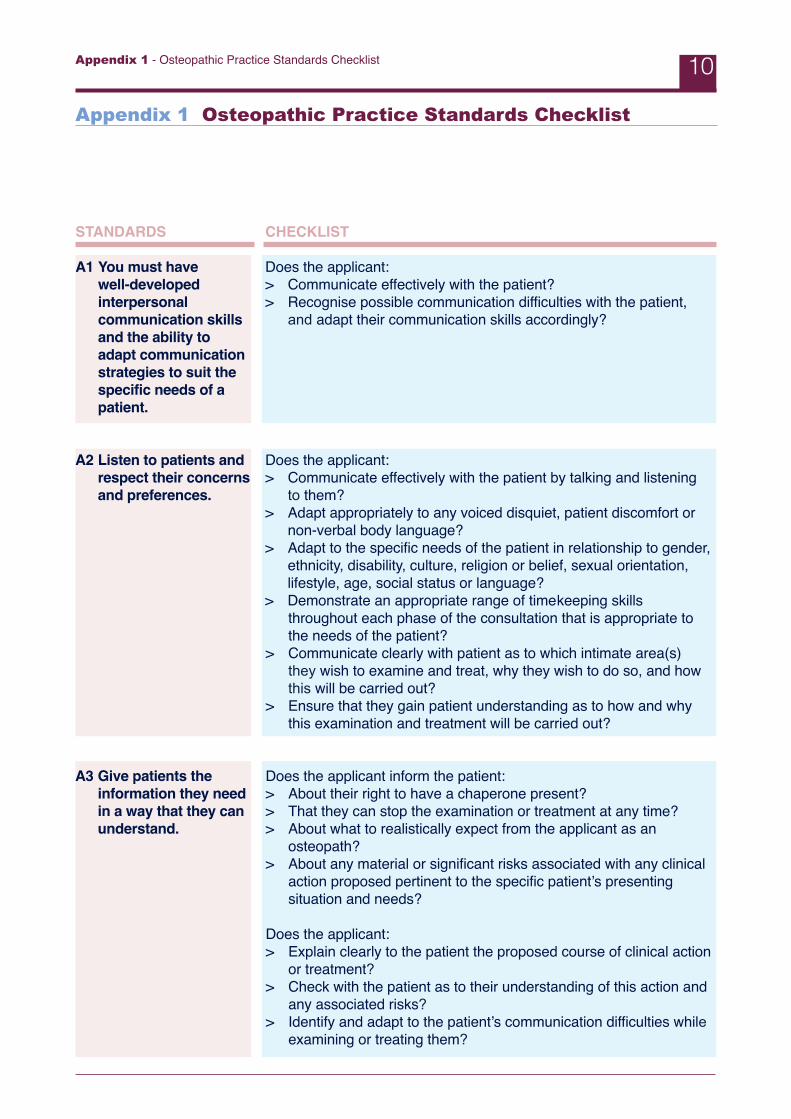
Appendix 1 - Osteopathic Practice Standards Checklist 10
STANDARDS
A1 You must have well-developedinterpersonalcommunication skillsand the ability toadapt communicationstrategies to suit thespecific needs of apatient.
A2 Listen to patients andrespect their concernsand preferences.
A3 Give patients theinformation they needin a way that they canunderstand.
CHECKLIST
Does the applicant: > Communicate effectively with the patient? > Recognise possible communication difficulties with the patient,
and adapt their communication skills accordingly?
Does the applicant: > Communicate effectively with the patient by talking and listening
to them? > Adapt appropriately to any voiced disquiet, patient discomfort or
non-verbal body language?> Adapt to the specific needs of the patient in relationship to gender,
ethnicity, disability, culture, religion or belief, sexual orientation,lifestyle, age, social status or language?
> Demonstrate an appropriate range of timekeeping skillsthroughout each phase of the consultation that is appropriate tothe needs of the patient?
> Communicate clearly with patient as to which intimate area(s)they wish to examine and treat, why they wish to do so, and howthis will be carried out?
> Ensure that they gain patient understanding as to how and whythis examination and treatment will be carried out?
Does the applicant inform the patient: > About their right to have a chaperone present?> That they can stop the examination or treatment at any time?> About what to realistically expect from the applicant as an
osteopath?> About any material or significant risks associated with any clinical
action proposed pertinent to the specific patient’s presentingsituation and needs?
Does the applicant:> Explain clearly to the patient the proposed course of clinical action
or treatment? > Check with the patient as to their understanding of this action and
any associated risks?> Identify and adapt to the patient’s communication difficulties while
examining or treating them?
Appendix 1 Osteopathic Practice Standards Checklist

Appendix 1 - Osteopathic Practice Standards Checklist 11
STANDARDS
A4 You must receive validconsent beforeexamination andtreatment.
A5 Work in partnershipwith patients to findthe best treatment forthem.
A6 Support patients incaring for themselvesto improve andmaintain their ownhealth.
B1 You must understandosteopathic conceptsand principles, andapply them critically topatient care.
CHECKLIST
In gaining valid consent from the patient, does the applicant ensureor take all steps to consider:> That the patient is competent, and has the capacity to give
consent?> That, if the patient appears not to be competent to understand,
they do not proceed further?> That any information given to the patient is contextually sensitive
and takes into consideration age, disability, and culturalbackground?
> That the patient is able to give consent voluntarily without beingmade to feel under pressure?
> That consent is an ongoing process during treatment?
Does the applicant: > Interact with and involve the patient during the examination and
treatment phases of the consultation?> Involve the patient in treatment and management planning?> Demonstrate a reasoned and appropriate course of management
action for this specific patient?
Does the applicant:> Provide sufficient information for the patient to be able to make an
informed choice as to which course of action they wish to proceedwith?
> Offer the patient the opportunity to inform their GP or otherhealthcare professionals about receiving osteopathic treatment?
Does the applicant: > Apply osteopathic principles and concepts in their clinical decision
making?> Justify and critique their understanding and application of
osteopathic principles and concepts in the evaluation andmanagement specific to the patient?
> Apply a range of osteopathic approaches that are informed bytheir analysis of the context of the presenting patient?
> Consider the patient as whole in the context of the presentingcomplaint?
> Use palpation as an evaluation, diagnostic, treatment and re-evaluation tool?

Appendix 1 - Osteopathic Practice Standards Checklist 12
STANDARDS
B2 You must havesufficient knowledgeand skills to supportyour work as anosteopath.
B3 Recognise and workwithin the limits ofyour training andcompetence.
B4 Keep yourprofessionalknowledge and skillsup to date.
CHECKLIST
Does the applicant demonstrate an underpinning knowledge basesufficient to: > Recognise the clinical signs of dysfunction and interpret their
significance given the context of the specific patient and theirpresenting complaint?
> Develop treatment and rehabilitation strategies given theirunderstanding of the specific context of the patient?
> Inform their clinical judgement and generation of diagnostichypotheses throughout each phase of the consultation?
> Recognise where there might be underlying pathology andfacilitate the onward referral of the patient for additional oralternative investigations and/or treatment?
> Recognise any pertinent psychosocial issues and the impactthese might have on the specific context of the presenting patient?
> Apply osteopathic technique safely and effectively given thecontext of the presenting patient?
Does the applicant demonstrate: > Welldeveloped palpatory skills? > The effective use of palpation as an evaluation tool?> How they interpret the findings of palpation to inform their clinical
reasoning through the examination and treatment phases of theconsultation?
> The ability to carry out, and interpret, an evaluation of the patientthat is informed by the presenting signs and symptoms, ismodified to the needs of the patient, and includes observation,palpation and motion evaluation (both active and passive)?
> Problem-solving and thinking skills, in their evaluation of thepatient through the different phases of the consultation, thatinforms clinical reasoning and decision-making processes?
> Good physical practitioner handling skills, being mindful of theirown and patient’s morphology?
> The application of suitable strategies to protect themselvespsychologically in any interaction with the patient?
Does the applicant:> Have the skills and competence to treat a patient?> Consider the need to seek advice or assistance for ongoing
patient care?
Does the applicant demonstrate:> How they integrate contemporary advice related to osteopathic
healthcare into their practice? (For example, guidelines, risks andadverse reactions.)

Appendix 1 - Osteopathic Practice Standards Checklist 13
STANDARDS
C1 You must be able toconduct an osteopathicpatient evaluationsufficient to make aworking diagnosis andformulate a treatmentplan.
C2 You must be able toformulate and delivera justifiableosteopathic treatmentplan or an alternativecourse of action.
CHECKLIST
Does the applicant demonstrate the ability to: > Take and record a detailed case history? (This should include any
problems and symptoms reported by the patient; general healthacross all body systems; relevant medical, surgical and traumatichistory; and family and social history.)
> Make and record an analysis of the presenting complaint giventhe context of the case history?
> Adapt their interview and enquiry skills to their perception of thespecific needs of that patient? (For example, pain levels,psychosocial issues and communication ability.)
> Take into consideration the significance of possible predisposingfactors, such as physiological, psychological and social issues, intheir analysis of the presenting complaint?
> Select and conduct a range of clinical examinations/investigations that are initiated from the case history analysis andare adapted or modified to the needs of the patient?
> Formulate diagnostic hypotheses informed by the analysis of thecase history, observation of the patient, and the examinationfindings?
> Develop a working osteopathic diagnosis?
In developing a treatment and management plan, does the applicant: > Select and justify a treatment and management approach that is
developed from the information gathered from the different phasesof the consultation, and informed by the working diagnosis?
> Take into consideration the specific needs and expectations of thepatient?
> Consider their personal limits of competence?> Consider and discuss with the patient the likely effects of
treatment?> Identify the suitability of, modification of, or contra-indication to
using specific osteopathic techniques given the needs of thepatient, the context of their presenting complaint and their history?
In applying treatment, does the applicant:> Monitor the effects of treatment during and after its application?> Adapt the application of either technique or treatment approach in
response to ongoing palpation?> Evaluate posttreatment response?> Justify the continuance, modification or cessation of osteopathic
treatment?> Recognise, and take appropriate remedial action to deal with, an
adverse reaction to osteopathic treatment?
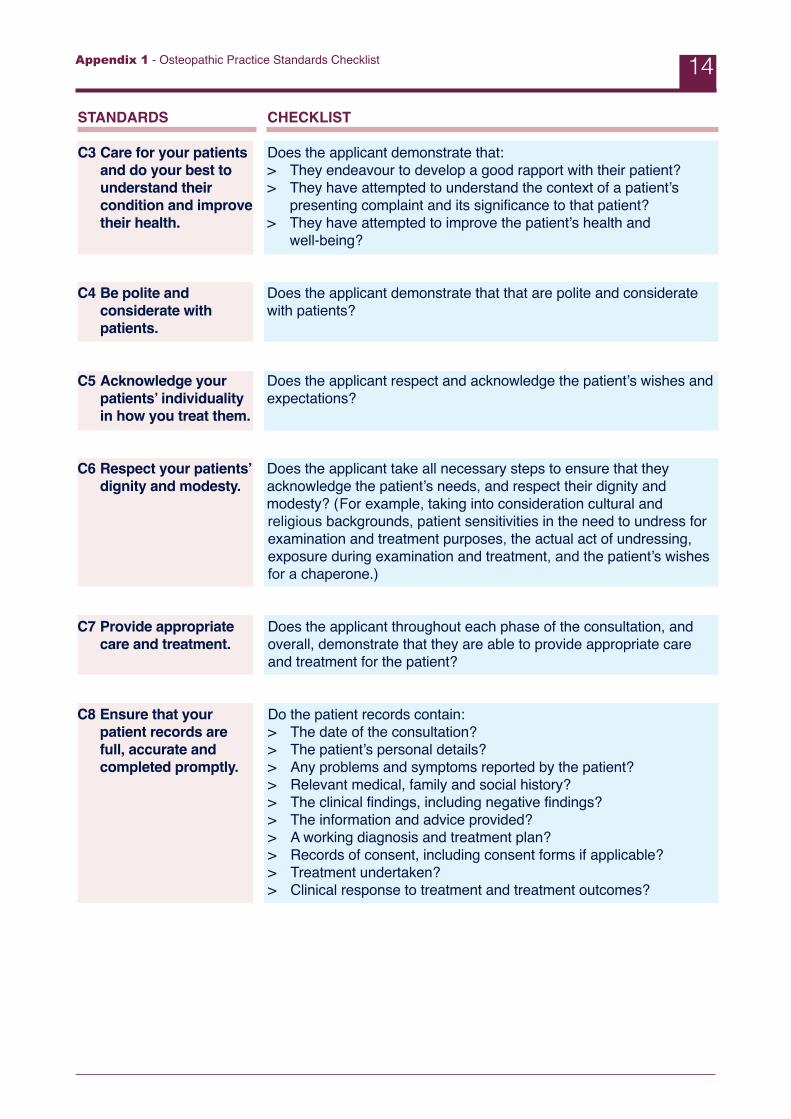
Appendix 1 - Osteopathic Practice Standards Checklist 14
STANDARDS
C3 Care for your patientsand do your best tounderstand theircondition and improvetheir health.
C4 Be polite andconsiderate withpatients.
C5 Acknowledge yourpatients’ individualityin how you treat them.
C6 Respect your patients’dignity and modesty.
C7 Provide appropriatecare and treatment.
C8 Ensure that yourpatient records arefull, accurate andcompleted promptly.
CHECKLIST
Does the applicant demonstrate that: > They endeavour to develop a good rapport with their patient? > They have attempted to understand the context of a patient’s
presenting complaint and its significance to that patient?> They have attempted to improve the patient’s health and
well-being?
Does the applicant demonstrate that that are polite and consideratewith patients?
Does the applicant respect and acknowledge the patient’s wishes andexpectations?
Does the applicant take all necessary steps to ensure that theyacknowledge the patient’s needs, and respect their dignity andmodesty? (For example, taking into consideration cultural andreligious backgrounds, patient sensitivities in the need to undress forexamination and treatment purposes, the actual act of undressing,exposure during examination and treatment, and the patient’s wishesfor a chaperone.)
Does the applicant throughout each phase of the consultation, andoverall, demonstrate that they are able to provide appropriate careand treatment for the patient?
Do the patient records contain: > The date of the consultation?> The patient’s personal details?> Any problems and symptoms reported by the patient?> Relevant medical, family and social history?> The clinical findings, including negative findings?> The information and advice provided?> A working diagnosis and treatment plan?> Records of consent, including consent forms if applicable?> Treatment undertaken?> Clinical response to treatment and treatment outcomes?

Appendix 1 - Osteopathic Practice Standards Checklist 15
STANDARDS
D1 You must considerthe contributions ofother healthcareprofessionals toensure best patientcare.
D12 Take all necessarysteps to control thespread ofcommunicablediseases.
CHECKLIST
Does the applicant:> Provide any evidence of consideration of other healthcare
approaches in the management plan of the patient?> Understand the contribution of osteopathic treatment in context of
primary care provision?> Consider referral to other disciplines in order to request further
investigations as appropriate?> Understand the indications for referral?
Does the applicant demonstrate an awareness of infection control andthe impact this has upon their professional practice?

Appendix 1 - Osteopathic Practice Standards Checklist 16
Mapping of Assessment of Clinical Performance to OPS
A1A2A3A4A5A6 B1B2B3B4C1C2C3C4C5C6C7C8D1D12
Communication Case History
XXXXXX
X
XXX
X
DifferentialDiagnosis
XX
ClinicalExamination OsteopathicEvaluation
XXX
XX
X
XXXXXX
Treatment Management
Plan
XXXXXX
XX
X
XXXXXXX

Appendix 2 Evaluation Form
Applicant’s name: Date:
Examiner’s name: Moderator’s name:
Case 1 summary:
CASE HISTORY/COMMUNICATION (A1, A2, A3, A4, A5, A6, C1, C3, C4, C5, C8)
> Occupation> Psychosocial context> Symptoms and progression> Onset> Aggravating factors> Relieving factors> NA factors> Daily pattern> Sleep> Past history> Past medical history> Family history> Logical progression and sequencing of questions> Sufficiency of information gathered> Recording> Communication: risks and benefits> Sensitivity/manner
Appendix 2 - Evaluation Form 17

DIFFERENTIAL DIAGNOSIS/INTERPRETATION/CLINICAL REASONING/KNOWLEDGE BASEBIOMEDICAL SCIENCES AND OSTEOPATHIC PRINCIPLES(B1, B2)
> Knowledge of pathology> Applied anatomy> Clinical biomechanics> Tissue differential> Safety awareness
Proposed Differential Diagnosis: Reasoning1
2
3
4
5
CLINICAL EXAMINATION/OSTEOPATHIC EVALUATION (A3, A4, A5, B1, B2, C1, C3, C4, C5, C6, C7, C8)
> Appropriate/effective> Consent> Postural examinations:
> Gait> A/P and lateral curves> Bony landmarks> Tissue quality
> Standing exam – active ROM> Sitting exam> Recumbent exam> Peripheral joint exam> Clinical tests: selection> Clinical methods effective> Orthopaedic special test> Neurological screen> Vascular screen> Osteopathic evaluation:
> responsive to patient> palpation> patient handling/operator position> logical sequence/omissions> patient comfort> recording
Applicant’s name:
Appendix 2 - Evaluation Form 18

FORMATION OF DIAGNOSTIC CONCLUSIONS, TREATMENT PLAN & MANAGEMENT PLANS(A1, A2, A3, A4, A5, A6, B2, B3, C2, C4, C5, C6, C7, C8, D1, D12)
> Reasonable conclusions> Clinical reasoning/justification> Awareness of current evidence> Knowledge and application of osteopathic principles> Decision to treat/refer> Understanding other disciplines> Shortterm aims> Longterm aims> Application of osteopathic principles> Formation of prognosis> Treatment observed> Modification of techniques> Depends on palpation to monitor change> Awareness of contra-indication> Re-evaluates change> Advice and exercises
Applicant’s name:
Applicant’s grade (please circle): Pass Fail
Areas of strength
Areas for development
Areas of significant weakness/reasons for failure
Appendix 2 - Evaluation Form 19

Other comments
Appendix 2 - Evaluation Form 20

Appendix 3 Outcome Report
Applicant’s name: Date:
Recommendation: (Please circle) PASS FAIL
Summary:
1 Strengths and areas for development identified by the Further Evidence of Practice Questionnaire
2 ACP outcomes
Strengths/good practice
Areas for development
Reasons for failure (if applicable)
Assessor 1: Signed: Date:
Assessor 2: Signed: Date:
Moderator: Signed: Date:
Appendix 3 - Outcome Report 21
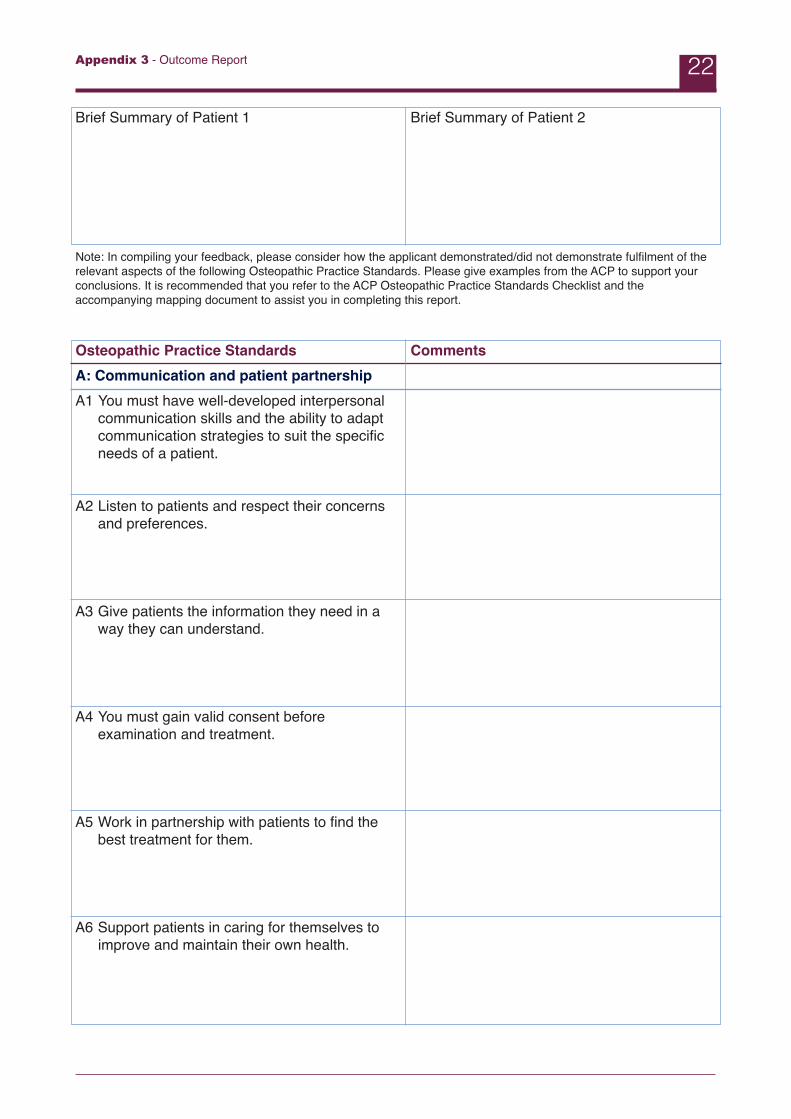
Brief Summary of Patient 1 Brief Summary of Patient 2
Note: In compiling your feedback, please consider how the applicant demonstrated/did not demonstrate fulfilment of therelevant aspects of the following Osteopathic Practice Standards. Please give examples from the ACP to support yourconclusions. It is recommended that you refer to the ACP Osteopathic Practice Standards Checklist and theaccompanying mapping document to assist you in completing this report.
Osteopathic Practice Standards CommentsA: Communication and patient partnershipA1 You must have well-developed interpersonal
communication skills and the ability to adapt communication strategies to suit the specific needs of a patient.
A2 Listen to patients and respect their concerns and preferences.
A3 Give patients the information they need in a way they can understand.
A4 You must gain valid consent before examination and treatment.
A5 Work in partnership with patients to find the best treatment for them.
A6 Support patients in caring for themselves to improve and maintain their own health.
Appendix 3 - Outcome Report 22

B: Knowledge skills and performanceB1 You must understand osteopathic concepts
and principles, and apply them critically topatient care.
B2 You must have sufficient knowledge and skillsto support your work as an osteopath.
B3 Recognise and work within the limits of yourtraining and competence.
B4 Keep your professional knowledge and skillsup to date.
C: Safety and quality in practice C1 You must be able to conduct an osteopathic
patient evaluation sufficient to make a workingdiagnosis and formulate a treatment plan.
C2 You must be able to formulate and deliver ajustifiable osteopathic treatment plan or analternative course of action.
C3 Care for your patients and do your best tounderstand their condition and improve theirhealth.
C4 Be polite and considerate with patients.
Appendix 3 - Outcome Report 23
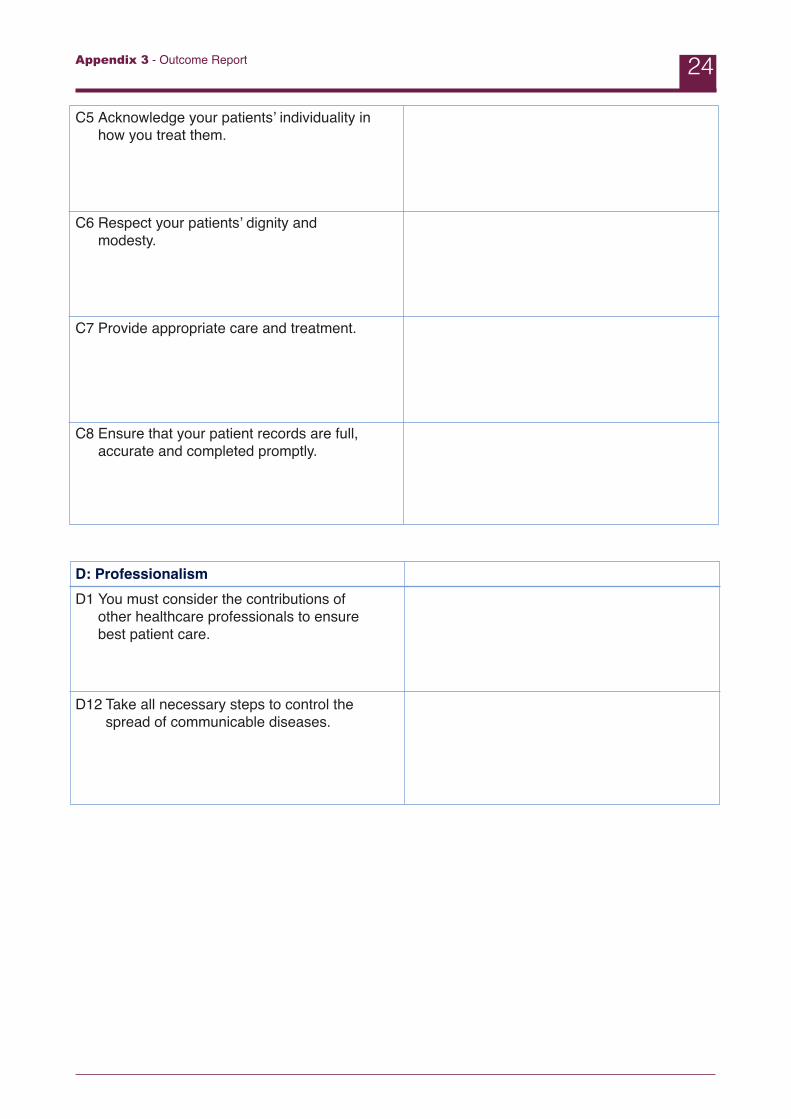
C5 Acknowledge your patients’ individuality inhow you treat them.
C6 Respect your patients’ dignity andmodesty.
C7 Provide appropriate care and treatment.
C8 Ensure that your patient records are full,accurate and completed promptly.
D: ProfessionalismD1 You must consider the contributions of
other healthcare professionals to ensurebest patient care.
D12 Take all necessary steps to control thespread of communicable diseases.
Appendix 3 - Outcome Report 24

















