Association between the Apolipoprotein E4 andPostoperative Cognitive Dysfunction in ElderlyPatients Undergoing Intravenous Anesthesia andInhalation Anesthesia
Background: Intravenous and inhalation anesthesia are com-monly used in the clinical setting. Recovery of cognitive func-tion in elderly patients after surgery has received increased atten-tion. In this study, the authors compared recovery of cognitivefunction in patients after different anesthesia techniques, andinvestigated which technique is safer. The authors also exploredassociation between apolipoprotein E4 and postoperative cog-nitive dysfunction in patients undergoing general anesthesia.Methods: A total of 2,000 patients were equally and randomlydivided into intravenous and inhalation anesthesia groups. To-tal intravenous and inhalation anesthesia were used. Within 10days after surgery, cognitive function was assessed daily usingthe Mini-Mental State Examination (MMSE). Restriction frag-
ment length polymorphism of apolipoprotein E gene was ana-lyzed. The primary outcome was MMSE score, frequency dis-tribution of apolipoprotein E alleles and genotypes. P � 0.01was used as statistically significant.Results: MMSE score in inhalation preoperative baselinegroup significantly decreased at day 3 after surgery comparedwith the preoperational and intravenous anesthesia group. Theproportion of patients scoring less than 25 points was signifi-cantly greater in the inhalation anesthesia group than in theintravenous anesthesia group at 3 days after surgery. In the in-halation anesthesia group, the decrease in MMSE score wasclosely related with apolipoprotein E �4 allele. In the intrave-nous anesthesia group, the decrease in MMSE score was notcorrelated with apolipoprotein E �4 allele.Conclusions: There was a strong association between theapolipoprotein E �4 and postoperative cognitive dysfunctionin elderly patients undergoing inhalation anesthetics.
T OTAL intravenous anesthesia (TIVA) has been used longbefore propofol was introduced. TIVA has seen several
major developments since it was first introduced.1 Since thesynthesis of the first intravenous anesthetics, TIVA has evolveduntil the development of TIVA with target-controlled infusionpumps. The first pharmacokinetic model for the use of target-controlled infusion was described by Schwilden2 in 1981. Byusing propofol with the target-controlled infusion technique, itis possible to maintain constant concentration in blood. In ad-dition, due to the ultra- short effect of propofol, the anesthesi-ologist can accurately estimate the time of recovery. Because thedrug has a rapid onset of action, the plasma concentration ap-
* Associate Professor, Department of Anesthesia, Second Affili-ated Hospital, Medical College, Xi’an Jiaotong University, ShaanxiProvince, China. † Professor, Department of Neuroanatomy, Medi-cal College, Xi’an Jiaotong University. ‡ Professor, Department ofAnesthesia, Second Affiliated Hospital, Medical College, Xi’an Jiao-tong University. § Associate Professor, Department of Neuroanat-omy, Medical College, Xi’an Jiaotong University. � Associate Profes-sor, Department of Forensic Medicine, Medical College, Xi’an JiaotongUniversity. # Associate Professor, Department of Anesthesia, First Affil-iated Hospital, Medical College, Xi’an Jiaotong University. ** ResearchAssistant, Department of Psychology, Zhongxin Hospital, ShaanxiProvince, China. †† Research Assistant, Department of Forensic Medi-cine, Medical College, Xi’an Jiaotong University.
Received from the Department of Anesthesia, Second AffiliatedHospital, Medical College, Xi’an Jiaotong University, Xi’an, ShaanxiProvince, China, Department of Neuroanatomy, Medical College,Xi’an Jiaotong University, Xi’an, Shaanxi Province, China, Depart-ment of Forensic Medicine, Medical College, Xi’an Jiaotong Univer-sity, Xi’an, Shaanxi Province, China, Department of Psychology,Zhongxin Hospital, Xi’an, Shaanxi Province, China, and Departmentof Anesthesia, First Affiliated Hospital, Medical College, Xi’an Jiao-tong University, Xi’an, Shaanxi Province, China. Submitted for pub-lication May 18, 2010. Accepted for publication September 27, 2011.Supported by grants from National Nature Science Foundation ofChina (NSFC) (No. 30400515), Xi’an, Shaanxi Province, China 2004and NSFC (No. 30300395), Xi’an, Shaanxi Province, China 2003; andby Doctor funding Xi’an, Shaanxi Province, China 2003.
Address correspondence to Dr. Cai: Department of Anesthesia,Second Affiliated Hospital, Medical College, Xi’an Jiaotong University,Xi’an 710004, China. [email protected]. Information on pur-chasing reprints may be found at www.anesthesiology.org or on themasthead page at the beginning of this issue. ANESTHESIOLOGY’s articlesare made freely accessible to all readers, for personal use only, 6months from the cover date of the issue.
• Gene polymorphism of apolipoprotein E (ApoE) has been asso-ciated with development of dementia. Information on a possiblerole of ApoE in postoperative cognitive dysfunction is scarce.
What This Article Tells Us That Is New
• This study (single center, case-controlled) in 2,000 patientsshowed an association between ApoE4 and the developmentof transient postoperative dysfunction in elderly patients afterinhalational anesthesia.
Anesthesiology, V 116 • No 1 January 201284
Downloaded From: http://anesthesiology.pubs.asahq.org/pdfaccess.ashx?url=/data/journals/jasa/931114/ on 05/31/2018
proximates the target concentration and anesthesia can be fullycontrolled. Thus, TIVA became possible.
There have been many studies of cognitive function afteranesthesia and surgery.3,4 Potential mechanisms for either cog-nitive disorder or neurodegeneration after general anesthesia arenumerous, including N-methyl-D-aspartate-mediated excito-toxicity, oxidative stress, suppression of cholinergic signal trans-duction, and enhancement of protein oligomerization.5 Genepolymorphism of apolipoprotein E (ApoE) residing on chro-mosome 19 is associated with senile dementia.6–9 The ApoEgene contains three allele genes, �2, �3, and �4, which can makeup six genotypes of homozygote and heterozygote, and six typesof genetic phenotypes. In normal elderly people, the occurrencefrequency of ApoE �3 gene is the highest and the gene frequencyof ApoE �2 and �4 is lower, thus the genotype of �3/3 is mostcommon and �2/2, �4/4 are least common. The �4 allele genefrequency has been shown to be increased in patients with seniledementia, and the �4 allele genotype is correlated with the riskof senile dementia.10 However, little attention has been paid tothe relationship between ApoE and outcome after anesthesia.We hypothesize that there is an association between the ApoE �4and postoperative cognitive dysfunction in patients undergoinggeneral anesthesia. In the current study, we tested the hypothesisthat there was an association between transient postoperative cog-nitive dysfunction in elderly patients and general anesthesia, therewas an association between the ApoE �4 and transient postopera-tivecognitivedysfunction,andtherewasanassociationbetweentheApoE �4 and transient postoperative cognitive dysfunction in pa-tients undergoing intravenous or inhalation anesthesia. To test thehypothesis, we designed the clinical study presented here. In thisstudy, we focused our investigation on the association between theApoE �4 allele and postoperative cognitive dysfunction in patientsundergoing intravenous and inhalation anesthesia.
Materials and Methods
This study received the Institutional Review Board approvalfrom the Second Affiliated Hospital, Medical College, Xi’anJiaotong University, and all patients signed an informed con-sent form before the start of any procedures.
SubjectsBecause ApoE single nucleotide polymorphism varies amongpeople with different ethnic backgrounds and living in dif-ferent regions, only the data from the same ethnic group is ofscientific significance. Although China has a total of 56 eth-nic groups, Han represents more than 90% of the total Chi-nese population. In our hospital more than 95% patients areof Han ethnicity. Because research in gene polymorphismrequires a large sample size and our hospital cannot supplyenough cases for the minority ethnicities, the few non-Han pa-tients were excluded from our study. There were a total of 5,026elderly Han patients (approximately 70 yr old) who were sched-uled to undergo general anesthesia and screened for the study.
MethodologyThis is a single-site, case-controlled, 1:1 ratio, parallel-group,block-randomization study in the Second Affiliated Hospital,Medical College, Xi’an Jiaotong University. Eligible partici-pants were patients undergoing surgery in the Second AffiliatedHospital. Participants were randomly assigned after block ran-domization procedures (computerized random numbers) toone of two treatment groups. From 2005 to 2010, there were atotal of 5,026 elderly Han patients (approximately 70 yr old)who were scheduled to undergo general anesthesia and screenedfor the study. Among screened patients, 3,026 patients wereexcluded either because they did not meet the inclusion criteria,or did not consent to be enrolled in the study, or required post-operative intensive care (because of bleeding, inflammation, re-spiratory failure, heart failure, anastomotic leaks, etc.), or re-quired postoperative sedation, and as a result, were also excludedin the final data analysis (fig. 1). The 2,000 patients described inthis study represent only those who were enrolled and followedup for the entire duration of the study. A total of 2,000 patients,who were American Society of Anesthesiologists Physical StatusI–II, without genetic connection, were enrolled in this study.There were 1,140 males and 860 females, with a mean age of70.1 � 4.6 yr, and weight of 57.3 � 7.5 kg. Diagnoses for theenrolled patients included esophageal cancer, gastric cancer, re-nal carcinoma, and fracture (table 1). Patients with severe heartor lung diseases or hepatic or renal dysfunction were excluded.Elderly patients with symptoms of dementia were excluded ac-cording to diagnostic criteria for dementia of the third revisededition of the American Psychiatric Disease Diagnosis and Sta-tistics Handbook11 and Folstein MMSE.12 The rationale for theexclusion is that if elderly people with senile dementia were in-cluded, we would not be able to distinguish whether the postoper-ativecognitivedeficit arose frompreoperative seniledementiaor theinsultofgeneral anesthesia.PatientswithMMSEscore�25pointsand Hachinski ischemic score13 � 3 points have, at most, minimalcognitive dysfunction before general anesthesia. The test methodsweredescribedtoandacceptedbythepatientsaccording to the33rd
item of The Hospital Manage Regulations of State Council ofChina in 2005.14 Written preoperative informed consent, regard-ing anesthesia, was obtained from all patients. The patients wererandomized intoan intravenousanesthesiagroupandan inhalationanesthesia group. No statistical difference in baseline data of pa-tients in two groups was detected (P � 0.05) (table 2).
In our study, anesthesiologists treated the patients. Thepatients were blinded to the anesthetic technique. Psychia-trists did the postoperative mental state examination; bothpatients and psychiatrists were blinded to the anesthetic tech-nique. The examinations were performed once a day for 10days. The staff of forensic medicine analyzed ApoE gene.They were also blinded to the anesthetic technique.
The primary outcome was MMSE, frequency distributionof ApoE alleles and genotypes. The primary outcomes should beheld to a conservative type I error rate, and three primary out-comes should be interpreted at the 0.05/3 � 0.0167 level. P �0.01 was considered statistically significant.
PERIOPERATIVE MEDICINE
Anesthesiology 2012; 116:84 –93 Cai et al.85
Downloaded From: http://anesthesiology.pubs.asahq.org/pdfaccess.ashx?url=/data/journals/jasa/931114/ on 05/31/2018
This trial was overseen by the Department of Statistics,Medical College, Xi’an Jiaotong University.
Extraction of Genome DNABefore anesthesia, a blood sample (3 ml) from each patient wasplaced in ethylenediamine tetraacetic acid (1 mg/ml) for 1 h,and centrifuged to obtain plasma. Genomic DNA from wholeblood was extracted in accordance with instructions from theDNA extraction kit (Bocai, Shanghai, China). Genome DNAwas dissolved in tris EDTA buffer at �20°C for analysis.15
Amplification of ApoE Gene using Polymerase Chain ReactionThe amplification method was the same as previously pub-lished.16 Polymerase chain reaction conditions were as fol-lows: the amplified gene fragments were located in ApoEgene exon 4. ApoE gene primer was designed and synthesized
as follows: upstream: 5�-ACA GAA TTC GCC CCG CCGGCC TGG TAC AC-3�; downstream: 5�-TAA GCT TGGCAC GGC TGT CCA AGG A-3�. The total volume ofpolymerase chain reaction was 50 �l, including 50–100 ngtemplate DNA, 2 mM deoxynucleoside triphosphate, 20pmol upstream primer, 20 pmol downstream primer, 50 mM
KCl, 1.5 mM MgCL2, 10 mM Tris-HCl, pH 8.3, 1.5 UTaqDNA polymerase. The cycle profile was as follows: 95°C for3 min; 35 cycles of 94°C for 45 s, 62°C for 45 s, 72°C for 30 s;72°C for 10 min. The reactions were electrophoresed throughagarose gel. Products (244 base pairs) were generated.17
Restriction Fragment Length Polymorphism of ApoE GeneIn accordance with the previous study,16 5 �l amplified prod-ucts were electrophoresed through a 2% agarose gel to detecttarget DNA fragment. After purification, polymerase chain re-
Fig. 1. Flow diagram of a single-site trial of intravenous anesthesia versus inhalation anesthesia. The diagram includes detailedinformation on the excluded participants.
Dementia and Inhalational Anesthesia
Anesthesiology 2012; 116:84 –93 Cai et al.86
Downloaded From: http://anesthesiology.pubs.asahq.org/pdfaccess.ashx?url=/data/journals/jasa/931114/ on 05/31/2018
action products were digested with 6 U HhaI endonuclease andbuffer solution at 37°C for 4 or 5 h, and then electrophoresedthrough a 15% polyacrylamide gel. After ethidium bromidestaining, DNA type was observed with an ultraviolet transmis-sion reflectometer. ApoE genotyping was performed by restric-tion fragment length polymorphism analysis using DNA ex-tracted from buffy coats of whole blood samples. DNA sampleswere amplified with polymerase chain reaction and digestedwith the appropriate restriction enzymes.18
Anesthetic MethodAll patients received 10 mg diazepam and 0.5 mg atropine,intramuscularly, 30 min before general anesthesia. A three-lu-men venous catheter was used for infusion of fentanyl, propofol,
and muscle relaxant. A catheter was put into the left radial arteryto collect blood samples. The three-lumen central venous cath-eter was used for measuring central venous pressure. In the in-travenous anesthesia group, the fentanyl target level was 5.12ng/ml.19 The loading dose of fentanyl was 4 �g/kg, followed bycontinuous infusion at a rate of 0.03 �g/kg/min; propofol targetlevel was 3 �g/ml,19 the loading dose of propofol 3 mg/kg,followed by continuous infusion at a rate of 53.8 �g/kg/min,which was injected by 6 steps with gradual increase in concen-tration: the initial target level was 1 �g/ml, and increased by 0.4�g/ml with an interval of 150 s; vecuronium bromide targetlevel was 2.0–2.5 �g/ml, the loading dose of vecuronium bro-miode 0.08 mg/kg, followed by continuous infusion at a rate of0.5 �g/kg/min. Neuromuscular monitoring was obtained withforce displacement transducers attached to each adductor polli-cis. Tracheal intubation was performed once adductor pollicismuscular response obtained with train-of-four at 0.05 Hz wasabolished20 and the bispectral index reached 40–60.
In the inhalation anesthesia group, the loading dose of fen-tanyl 4 �g/kg, followed by continuous infusion at a rate of 0.03�g/kg/min; the loading dose of propofol 3 mg/kg, followed bycontinuous inhalation 2–3% end-tidal concentration of isoflu-rane, which was used for maintenance of anesthesia. The end-tidal concentration of isoflurane was administered to maintain anormal depth of anesthesia using the BIS™ monitor (Aspect,Newton, MA) and traditional signs of anesthetic depth. Theloading dose of vecuronium was 0.08 mg/kg, followed by con-tinuous infusion at a rate of 0.5 �g/kg/min. Neuromuscularmonitoring was obtained with force displacement transducersattached to each adductor pollicis. Tracheal intubation was per-formed once adductor pollicis muscular response obtained withtrain-of-four at 0.05 Hz was abolished and the bispectral indexreached 40–60. Lactated Ringer’s solution and hetastarch wereused during surgery.
Respiration was assisted by ventilation via mask in case ofincreasing respiratory depression, and mechanical ventila-tion maintained to achieve a specific end-tidal carbon diox-ide after intubation. Ventilation was adjusted to maintain theend-tidal carbondioxide at 35 � 5 mmHg.
Patient MonitoringThe Model 883 Multi-function Monitor (Hewlett-Packard,Palo Alto, CA) was used to monitor heart rate, electrocardio-gram, blood pressure, oxygen saturation, and neuromuscularmonitoring. Model A-2000 Monitor (Aspect, Newton, MA)was used to measure bispectral index. Within 10 days aftersurgery, cognitive function was assessed using MMSE daily.
Main Outcome MeasuresCorrelation of ApoE gene frequency and ApoE�4 allele toMMSE score was measured.
Statistical AnalysisTwo-tailed tests were used. The data of physiologic and bio-chemical index were compared by the Z test. The data of
Table 1. Diagnosis and Frequencies in Intravenous andInhalation Groups
P value is greater than 0.05, thus no statistical difference be-tween the two groups.HIS � Hachinski ischemic score; MMSE � Mini-Mental StateExamination.
PERIOPERATIVE MEDICINE
Anesthesiology 2012; 116:84 –93 Cai et al.87
Downloaded From: http://anesthesiology.pubs.asahq.org/pdfaccess.ashx?url=/data/journals/jasa/931114/ on 05/31/2018
MMSE examined across groups by day were analyzed by two-way ANOVA with repeated measures, and the multiple meansof MMSE were compared with multiple comparison. P � 0.05was considered as no statistical difference between the twogroups, whereas P � 0.01 was considered significant. Genefrequency was obtained by gene count. Genotype and gene fre-quency were analyzed using the chi-square test. In two groups,the patient whose MMSE score was less than 25 points at day 1was selected to perform the statistical comparison. This studywas powered to detect clinically significant differences in theprimary outcome. An a priori power calculation revealed that tohave power of 80%, with a two-tailed � level of 0.05, a samplesize of n � 2,000 would allow detection of odds ratios (OR) assmall as 1.4. Differences smaller than this magnitude are notlikely to be clinically meaningful. The association of ApoE �4allele frequency and ApoE �4 allele to MMSE score was mea-sured through calculating OR and 95% CI. P � 0.05 was con-sidered as no statistical difference between the two groups,whereas P � 0.01 was considered significant. The STATA4.0medical statistic software (Stata Corporation, College Station,TX) was supplied by Department of Statistics, MedicalCollege,’Xi’an Jiaotong University, China.
Results
Quantitative Analysis of ParticipantsA total of 2,000 patients were included in final analysis, of atotal of 5,026 patients that were screened for the study.
MMSE Score in Patients of Both GroupsWith an ANOVA test, two groups were found significantlydifferent regarding time and group factor (P � 0.01). For thatreason, two groups were analyzed with the Bonferroni correc-tion post hoc test to address the three stages at different timepoints that made a significant difference inside a group and toaddress the three stages at the same time point that made asignificant difference between the two groups (P � 0.01). Be-fore the surgery, there was no difference in MMSE scores be-tween inhalation group and intravenous group. After the sur-gery, the MMSE score in the intravenous group remainedunchanged during the entire 10 days of monitoring. For pa-tients with inhalation anesthesia, however, the MMSE score atdays 1, 2, and 3 after surgery decreased significantly (P � 0.01)when compared with its own preoperative value, and also sig-nificantly (P � 0.01) when compared with the intravenousgroup value for the corresponding date. Interestingly, by day 10,MMSE score in the inhalation group recovered to preoperativelevel. P � 0.01, versus before surgery; P � 0.01, versus theintravenous anesthesia group (fig. 2).
Proportion of Patients of Various Scores in Both GroupsThe proportion of patients scoring less than 25 points was signifi-cantly greater in the inhalation anesthesia group than in the intra-venous anesthesia group 3 days after surgery (P�0.01) (fig. 3). It isworth noting that more than 10% of patients in the inhalation
anesthesia group received a MMSE score of less than 20 points,compared with 0% in the intravenous anesthesia group.
Frequency Distribution of ApoE Genotypes in Both GroupsApoEalleles andgene frequencywerecalculated inaccordancewiththeHardy-Weinbergequilibriumlawinpatientsof the intravenousanesthesia and inhalation anesthesia groups. As figure 4 displayed,the frequency of �3/�3 was the highest, followed by �2/�3, and�2/�4 was the lowest. No statistically significant effect in gene fre-quency was found between the two groups.
Frequency Distribution of ApoE Genotypes in Patients ScoringVarious MMSE Scores of the Inhalation Anesthesia GroupAs figure 5 shows, in patients scoring � 25 points, �3/�3 fre-quency was the highest, followed by �3/�4, and �4/�4 was the
Fig. 2. Comparison of Mini-Mental State Examination (MMSE)score in patients of the intravenous anesthesia group and theinhalation anesthesia group. Errors refer SD. *P � 0.01, versusbefore surgery; #P � 0.01, versus the intravenous anesthesiagroup. The results show that MMSE examination scores weresignificantly decreased day 1, 2, and 3 after surgery in theinhalation anesthesia group, compared with the intravenousanesthesia group and before surgery. Decreased MMSE scoresindicated deficits in cognitive function. The proportion of pa-tients scoring less than 25 points was significantly greater in theinhalation anesthesia group, compared with the intravenousanesthesia group 3 days after surgery.
Fig. 3. Proportion of patients of various Mini-Mental StateExamination (MMSE) scores in both groups (n/%). *P � 0.01,versus the intravenous anesthesia group. It is worth notingthat more than 10% of patients in inhalation anesthesia groupreceived a MMSE score of less than 20 points, comparedwith 0% in the intravenous anesthesia group.
Dementia and Inhalational Anesthesia
Anesthesiology 2012; 116:84 –93 Cai et al.88
Downloaded From: http://anesthesiology.pubs.asahq.org/pdfaccess.ashx?url=/data/journals/jasa/931114/ on 05/31/2018
lowest. In patients scoring less than 25 points, �3/�3 frequencywas the highest, followed by �3/�4, and �2/�2 was thelowest. Z test results revealed that �4 allele (Z � 3.15, P �0.01) and �4/�4 gene (Z � 2.61, P � 0.01) were greaterin patients scoring less than 25 points than in the patientsscoring � 25 points.
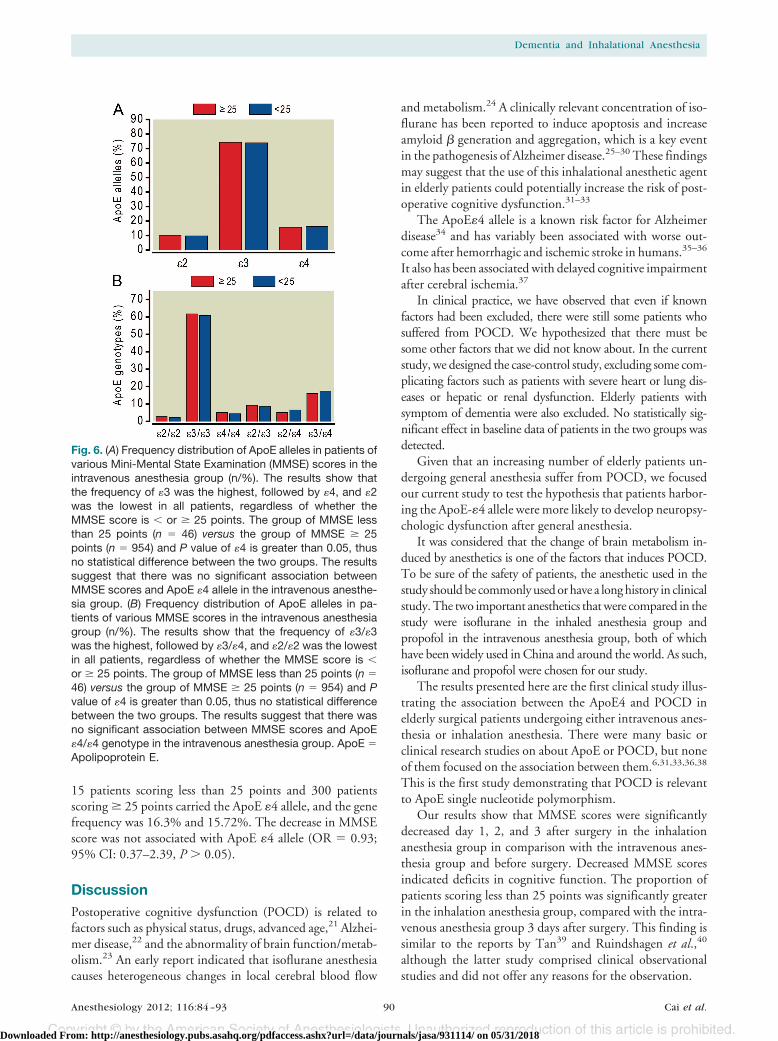
Frequency Distribution of ApoE Genotypes in PatientsScoring Various MMSE Scores of the IntravenousAnesthesia GroupAs figure 6 exhibited, the frequency of �3/�3 was thehighest, followed by �3/�4, and �2/�2 was the lowest inall patients, regardless whether the MMSE score is � or �25 points.
Association between ApoE �4 Allele and MMSEScores in Inhalation Anesthesia and IntravenousAnesthesia GroupsIn the inhalation anesthesia group, 113 patients scoring lessthan 25 points and 146 patients scoring � 25 points carriedthe ApoE �4 allele, and the gene frequency was 25.69% and9.36%, respectively. The decrease in MMSE score wasclosely related with the ApoE �4 allele (OR � 3.31; 95% CI:1.25–6.39, P � 0.05). In the intravenous anesthesia group,
Fig. 4. (A) Frequency distribution of apolipoprotein E (ApoE)alleles in patients of the intravenous anesthesia group (n �1,000) and the inhalation anesthesia group (n � 1,000) (n/%).P value of �4 is greater than 0.05, thus no statistical differ-ence between the two groups. The results show that thefrequency of �3 was the highest, followed by �2, and �4 wasthe lowest. However, no significant difference in gene fre-quency was found between the two groups. The resultssuggest that the difference in distribution frequency ofApoE alleles was excluded in the comparisons betweenthe inhalation and intravenous anesthesia groups. (B) Fre-quency distribution of ApoE genotypes in patients of theintravenous anesthesia group (n � 1,000) and the inhala-tion anesthesia group (n � 1,000) (n/%). P value of �4/�4 isgreater than 0.05, thus no statistical difference betweenthe two groups. The results show that the frequency of�3/�3 was the highest, followed by �3/�4, and �4/�4 wasthe lowest. However, no significant difference in gene fre-quency was found between the two groups. The resultssuggest that the difference in distribution frequency ofApoE genotypes was excluded in the comparisons be-tween the inhalation and intravenous anesthesia groups.
Fig. 5. (A) Frequency distribution of apolipoprotein E (ApoE)alleles in patients of various Mini-Mental State Examination(MMSE) scores in the inhalation anesthesia group (n/%).*P �0.01, the group of MMSE less than 25 points (n � 220) versusthe group of MMSE � 25 points (n � 780). The results showthat in patients scoring � 25 points, �3 frequency was thehighest, followed by �2, and �4 was the lowest. In patientsscoring less than 25 points, �3 frequency was the highest,followed by �4, and �2 was the lowest. Z test results revealedthat �4 allele (Z � 3.15, P � 0.01) were greater in patientsscoring less than 25 points than in the patients scoring � 25points. The results suggest that the �4 allele was a risk factorfor cognitive dysfunction in elderly patients who received aninhalation anesthetic. (B) Frequency distribution of ApoE ge-notypes in patients of various MMSE scores in the inhalationanesthesia group (n/%). *P � 0.01, the group of MMSE lessthan 25 points (n � 220) versus the group of MMSE � 25points (n � 780). The results show that in patients scoring �25 points, �3/�3 frequency was the highest, followed by�3/�4, and �4/�4 was the lowest. In patients scoring less than25 points, �3/�3 frequency was the highest, followed by�3/�4, and �2/�2 was the lowest. Z test results revealed that�4/�4 genotype (Z � 2.61, P � 0.01) were greater in patientsscoring less than 25 points than in the patients scoring � 25points. The results suggest that the �4/�4 genotype was arisk factor for cognitive dysfunction in elderly patients whoreceived an inhalation anesthetic.
PERIOPERATIVE MEDICINE
Anesthesiology 2012; 116:84 –93 Cai et al.89
Downloaded From: http://anesthesiology.pubs.asahq.org/pdfaccess.ashx?url=/data/journals/jasa/931114/ on 05/31/2018
15 patients scoring less than 25 points and 300 patientsscoring � 25 points carried the ApoE �4 allele, and the genefrequency was 16.3% and 15.72%. The decrease in MMSEscore was not associated with ApoE �4 allele (OR � 0.93;95% CI: 0.37–2.39, P � 0.05).
DiscussionPostoperative cognitive dysfunction (POCD) is related tofactors such as physical status, drugs, advanced age,21 Alzhei-mer disease,22 and the abnormality of brain function/metab-olism.23 An early report indicated that isoflurane anesthesiacauses heterogeneous changes in local cerebral blood flow
and metabolism.24 A clinically relevant concentration of iso-flurane has been reported to induce apoptosis and increaseamyloid � generation and aggregation, which is a key eventin the pathogenesis of Alzheimer disease.25–30 These findingsmay suggest that the use of this inhalational anesthetic agentin elderly patients could potentially increase the risk of post-operative cognitive dysfunction.31–33
The ApoE�4 allele is a known risk factor for Alzheimerdisease34 and has variably been associated with worse out-come after hemorrhagic and ischemic stroke in humans.35–36
It also has been associated with delayed cognitive impairmentafter cerebral ischemia.37
In clinical practice, we have observed that even if knownfactors had been excluded, there were still some patients whosuffered from POCD. We hypothesized that there must besome other factors that we did not know about. In the currentstudy, we designed the case-control study, excluding some com-plicating factors such as patients with severe heart or lung dis-eases or hepatic or renal dysfunction. Elderly patients withsymptom of dementia were also excluded. No statistically sig-nificant effect in baseline data of patients in the two groups wasdetected.
Given that an increasing number of elderly patients un-dergoing general anesthesia suffer from POCD, we focusedour current study to test the hypothesis that patients harbor-ing the ApoE-�4 allele were more likely to develop neuropsy-chologic dysfunction after general anesthesia.
It was considered that the change of brain metabolism in-duced by anesthetics is one of the factors that induces POCD.To be sure of the safety of patients, the anesthetic used in thestudy should be commonly used or have a long history in clinicalstudy. The two important anesthetics that were compared in thestudy were isoflurane in the inhaled anesthesia group andpropofol in the intravenous anesthesia group, both of whichhave been widely used in China and around the world. As such,isoflurane and propofol were chosen for our study.
The results presented here are the first clinical study illus-trating the association between the ApoE4 and POCD inelderly surgical patients undergoing either intravenous anes-thesia or inhalation anesthesia. There were many basic orclinical research studies on about ApoE or POCD, but noneof them focused on the association between them.6,31,33,36,38
This is the first study demonstrating that POCD is relevantto ApoE single nucleotide polymorphism.
Our results show that MMSE scores were significantlydecreased day 1, 2, and 3 after surgery in the inhalationanesthesia group in comparison with the intravenous anes-thesia group and before surgery. Decreased MMSE scoresindicated deficits in cognitive function. The proportion ofpatients scoring less than 25 points was significantly greaterin the inhalation anesthesia group, compared with the intra-venous anesthesia group 3 days after surgery. This finding issimilar to the reports by Tan39 and Ruindshagen et al.,40
although the latter study comprised clinical observationalstudies and did not offer any reasons for the observation.
Fig. 6. (A) Frequency distribution of ApoE alleles in patients ofvarious Mini-Mental State Examination (MMSE) scores in theintravenous anesthesia group (n/%). The results show thatthe frequency of �3 was the highest, followed by �4, and �2was the lowest in all patients, regardless of whether theMMSE score is � or � 25 points. The group of MMSE lessthan 25 points (n � 46) versus the group of MMSE � 25points (n � 954) and P value of �4 is greater than 0.05, thusno statistical difference between the two groups. The resultssuggest that there was no significant association betweenMMSE scores and ApoE �4 allele in the intravenous anesthe-sia group. (B) Frequency distribution of ApoE alleles in pa-tients of various MMSE scores in the intravenous anesthesiagroup (n/%). The results show that the frequency of �3/�3was the highest, followed by �3/�4, and �2/�2 was the lowestin all patients, regardless of whether the MMSE score is �or � 25 points. The group of MMSE less than 25 points (n �46) versus the group of MMSE � 25 points (n � 954) and Pvalue of �4 is greater than 0.05, thus no statistical differencebetween the two groups. The results suggest that there wasno significant association between MMSE scores and ApoE�4/�4 genotype in the intravenous anesthesia group. ApoE �Apolipoprotein E.
Dementia and Inhalational Anesthesia
Anesthesiology 2012; 116:84 –93 Cai et al.90
Downloaded From: http://anesthesiology.pubs.asahq.org/pdfaccess.ashx?url=/data/journals/jasa/931114/ on 05/31/2018
To determine the reason why some patients’ MMSE scorewere less than 25 in the inhalation anesthesia group whereasno patient with a score less than 25 was observed in theintravenous anesthesia group, we measured the ApoE geno-types for both groups of patients. Our results demonstratedthat there were no statistically significant effects in frequencydistribution of ApoE genotypes between the inhalation andintravenous anesthesia groups, suggesting that ApoE distri-bution itself is not a contributing factor. However, furtheranalysis of ApoE distribution and MMSE score revealed thatthe frequency of the �4 allele (Z � 3.15, P � 0.01) and�4/�4 gene (Z � 2.61, P � 0.01) was greatest in patientswith a score less than 25 points than in patients with ascore � 25 points. Therefore, the presence of the �4 alleleand �4/�4 gene is of great importance and should receivemore attention in the clinic. To further confirm the associa-tion between ApoE �4 and postoperative cognitive dysfunc-tion, the OR and 95% CI were calculated to analyze thecorrelation between the ApoE �4 allele and MMSE scores.Results indicated that lower MMSE scores correlated withthe presence of the ApoE �4 allele in the inhalation anesthe-sia group (OR � 3.31, P � 0.05). These results provide thedirect evidence for a strong association between the ApoE4 andtransient postoperative cognitive dysfunction in patients under-going inhalation anesthesia. In contrast, presence of the ApoE�4 allele did not correlate with reduced MMSE scores in theintravenous anesthesia group (OR � 0.93, P � 0.05).
No statistically significant effect was found with regard togenotype and allele frequency in the inhalation and intravenousanesthesia groups. However, there was a statistically significanteffect in the number of patients who developed cognitive dys-function after surgery. In the intravenous anesthesia group,some patients suffered from cognitive dysfunction, and theirMMSE scores ranged from 20 to 25 points. These patientsrecovered over 10 days. There was no statistically significanteffect in genotype and allele frequency between the previouslymentioned patients and patients who scored � 25 points inthe intravenous anesthesia group. There was no significantcorrelation between MMSE scores and ApoE single nucleo-tide polymorphism. However, there was a statistically signif-icant effect in the number of cognitive dysfunction patientsbetween the inhalation and intravenous anesthesia groups. Inthe inhalation anesthesia group, there was a statistically sig-nificant effect in ApoE genotype and gene frequency in pa-tients with various MMSE scores. Specifically, the greatestdifferences were detected between the �4 allele and genefrequency. The correlation analysis between the ApoE �4allele and MMSE scores indicated that the �4 allele was a riskfactor for cognitive dysfunction in elderly patients who re-ceived an inhalation anesthetic. The incidence rate of cogni-tive dysfunction in patients who received inhalation anesthe-sia was greater compared with intravenous anesthesia. Thereis a strong association between the ApoE4 and transient post-operative cognitive dysfunction in patients undergoing inha-lation anesthesia.
In our study, the cognitive decline was seen 3 days postop-eratively in the inhalation anesthesia group, but this decline wasreversed at 10 days. Neither anesthesia technique is associatedwith long-term cognitive dysfunction. The risk of short-termcognitive decline, however, as determined by MMSE evalua-tion, is higher with an inhalation anesthetic, particularly in pa-tients with the E4 allele. Although such kind of “short-termcognitive decline” could be recovered in approximately 10 days,we still could not ensure that there are any morphologic changesin certain areas of the patient’s brain, or no changes in the phys-iologic and biochemical index. A recent study41 illustrates thatexposure of naïve mice to less than 2% isoflurane for only 2 hcan induce caspase activation and increase amyloid � levels.Therefore, there is thepotential risk thatuseof inhalationanesthesiacould cause detrimental effect to the brain, at least in elderlypatients with certain genotype. Whether this detrimental effectcould cause long-lasting changes requires further investigation.
In the current study, only isoflurane was investigated.However, there are other volatile anesthetics that are com-monly used in the clinical setting, such as sevoflurane anddesflurane. It has been reported that sevoflurane and isoflu-rane have similar anesthetic properties but different poten-cies.41 Sevoflurane and desflurane were found to be less po-tent than isoflurane in altering intracellular calcium, andproduced less apoptosis.41 In addition, sevoflurane may pro-mote Alzheimer disease neuropathogenesis.42 From litera-ture reports and our study here, we do not know whether allvolatile anesthetics will have a similar effect in causingPOCD in patients with certain genetic background, andwhether any particular volatile anesthetics may be more suit-able to elderly people than to others. Apparently, furtherresearch is warranted to answer these intriguing questions.
Our results presented here raise potential concerns regardingthe use of isoflurane, a commonly used anesthetic.43 In addi-tion, to carry out the study to investigate under what conditionsthat isoflurane is safe to use, there are other alternatives. Onealternative is to use those inhalation anesthetics that do not causePOCD, or design better and safer anesthetics. Another alterna-tives is that, based on our study, total intravenous anesthesia ismore suitable for elderly patients because it has no observableeffect on cognitive function of elderly patients after surgery,especially those carrying the ApoE �4 allele. ApoE single nucle-otide polymorphism varies among people with different ethnicbackground and living in different regions. The current study wasconducted in patients who are of Han ethnicity residing in north-west China; thus, inevitable limitation exists in our research find-ings. The scientific results would be more universal if performedand verified in much more diversified territories and ethnic groups.
Conclusions
There is a strong association between ApoE4 and transientPOCD in patients undergoing inhalation anesthesia. Com-pared with inhalation anesthesia, TIVA is more suitable forelderly patients because it has no observable effect on cogni-
PERIOPERATIVE MEDICINE
Anesthesiology 2012; 116:84 –93 Cai et al.91
Downloaded From: http://anesthesiology.pubs.asahq.org/pdfaccess.ashx?url=/data/journals/jasa/931114/ on 05/31/2018
tive function of elderly patients after surgery, especially thosecarrying the ApoE �4 allele.
References1. Nora FS: Total intravenous anesthesia as a target-controlled infu-
sion. An evolutive analysis. Rev Bras Anestesiol 2008; 58:179–92
2. Schwilden H: A general method for calculating the dosagescheme in linear pharmacokinetics. Eur J Clin Pharmacol1981; 20:379 – 86
3. Kostopanagiotou G, Markantonis SL, Polydorou M, PandaziA, Kottis G: Recovery and cognitive function after fentanyl orremifentanil administration for carotid endarterectomy.J Clin Anesth 2005; 17:16 –20
4. Heyer EJ, Gold MI, Kirby EW, Zurica J, Mitchell E, Halazun HJ,Teverbaugh L, Sciacca RR, Solomon RA, Quest DO, Maldonado TS,Riles TS, Connolly ES Jr: A study of cognitive dysfunction inpatients having carotid endarterectomy performed with regionalanesthesia. Anesth Analg 2008; 107:636–42
5. Eckenhoff RG, Johansson JS, Wei H, Carnini A, Kang B, WeiW, Pidikiti R, Keller JM, Eckenhoff MF: Inhaled anestheticenhancement of amyloid-beta oligomerization and cytotox-icity. ANESTHESIOLOGY 2004; 101:703–9
7. Ancelin ML, de Roquefeuil G, Ledesert B, Bonnel F, CheminalJC, Ritchie K: Exposure to anaesthetic agents, cognitivefunctioning and depressive symptomatology in the elderly.Br J Psychiatry 2001; 178:360 – 6
8. Findeis MA: Approaches to discovery and characterization ofinhibitors of amyloid beta-peptide polymerization. BiochimBiophys Acta 2000; 1502:76 – 84
9. Duda JE, Lee VM, Trojanowski JQ: Neuropathology of sy-nuclein aggregates. J Neurosci Res 2000; 61:121–7
10. Romas SN, Tang MX, Berglund L, Mayeux R: APOE genotype,plasma lipids, lipoproteins, and AD in community elderly.Neurology 1999; 53:517–21
11. American Psychiatric Association Diagnostic and StatisticalManual Disorders, Third Edition-Revised. Washington, DC:American Psychiatric Association; 1987
12. Grace J, Nadler JD, White DA, Guilmette TJ, Giuliano AJ,Monsch AU, Snow MG: Folstein vs modified Mini-MentalState Examination in geriatric stroke. Stability, validity, andscreening utility. Arch Neurol 1995; 52:477– 84
13. Newton JR, Parkinson D, Clench MR: Strategies for exami-nation of Alzheimer’s disease amyloid precursor protein iso-forms. Anal Bioanal Chem 2006; 385:692–9
14. State Council of the People’s Republic of China. Administra-tive Regulations on Medical Institution. 1994-09-01
15. Kang TJ, Yang MS: Rapid and reliable extraction of genomicDNA from various wild-type and transgenic plants. BMCBiotechnol 2004; 4:20
16. Pandey P, Pradhan S, Mittal B: LRP-associated protein gene(LRPAP1) and susceptibility to degenerative dementia. GenesBrain Behav 2008; 7:943–50
18. Hixson JE: Apolipoprotein E polymorphisms affect athero-sclerosis in young males. Pathobiological Determinants ofAtherosclerosis in Youth (PDAY) Research Group. Arterio-scler Thromb 1991; 11:1237– 44
19. Smith C, McEwan AI, Jhaveri R, Wilkinson M, Goodman D,Smith LR, Canada AT, Glass PS: The interaction of fentanyl onCp50 of propofol for loss of consciousness and skin incision.ANESTHESIOLOGY 1994; 81:820 – 8, discussion 26A
20. de Quattro A, Gardaz JP, Bissonnette B: Intubation condi-
tions: Importance of the rate of repetition of the train-of-four. Ann Fr Anesth Reanim 1996; 15:1032– 6
21. Boos GL, Soares LF, Oliveira Filho GR: Postoperative cogni-tive dysfunction: Prevalence and associated factors. Rev BrasAnestesiol 2005; 55:517–24
22. Wei H, Xie Z: Anesthesia, calcium homeostasis and Alzhei-mer’s disease. Curr Alzheimer Res 2009; 6:30 –5
23. Tsai TL, Sands LP, Leung JM: An update on postoperativecognitive dysfunction. Adv Anesth 2010; 28:269 – 84
24. Maekawa T, Tommasino C, Shapiro HM, Keifer-Goodman J,Kohlenberger RW: Local cerebral blood flow and glucoseutilization during isoflurane anesthesia in the rat. ANESTHESI-OLOGY 1986; 65:144 –51
25. Tanzi RE, Bertram L: Twenty years of the Alzheimer’s diseaseamyloid hypothesis: A genetic perspective. Cell 2005; 120:545–55
26. Vassar R, Bennett BD, Babu-Khan S, Kahn S, Mendiaz EA, Denis P,Teplow DB, Ross S, Amarante P, Loeloff R, Luo Y, Fisher S, FullerJ, Edenson S, Lile J, Jarosinski MA, Biere AL, Curran E, Burgess T,Louis JC, Collins F, Treanor J, Rogers G, Citron M: Beta-secretasecleavage of Alzheimer’s amyloid precursor protein by the trans-membrane aspartic protease BACE. Science 1999; 286:735–41
27. Gu Y, Misonou H, Sato T, Dohmae N, Takio K, Ihara Y:Distinct intramembrane cleavage of the beta-amyloid precur-sor protein family resembling gamma-secretase-like cleavageof Notch. J Biol Chem 2001; 276:35235– 8
28. Sastre M, Steiner H, Fuchs K, Capell A, Multhaup G, Condron MM,Teplow DB, Haass C: Presenilin-dependent gamma-secretase pro-cessing of beta-amyloid precursor protein at a site correspondingto the S3 cleavage of Notch. EMBO Rep 2001; 2:835–41
29. Yu C, Kim SH, Ikeuchi T, Xu H, Gasparini L, Wang R, SisodiaSS: Characterization of a presenilin-mediated amyloid precur-sor protein carboxyl-terminal fragment gamma: Evidence fordistinct mechanisms involved in gamma-secretase processingof the APP and Notch1 transmembrane domains. J Biol Chem2001; 276:43756 – 60
30. Xie Z, Dong Y, Maeda U, Moir RD, Xia W, Culley DJ, CrosbyG, Tanzi RE: The inhalation anesthetic isoflurane induces avicious cycle of apoptosis and amyloid beta-protein accumu-lation. J Neurosci 2007; 27:1247–54
31. Bohnen NI, Warner MA, Kokmen E, Beard CM, Kurland LT:Alzheimer’s disease and cumulative exposure to anesthesia:A case-control study. J Am Geriatr Soc 1994; 42:198 –201
32. Muravchick S, Smith DS: Parkinsonian symptoms during emer-gence from general anesthesia. ANESTHESIOLOGY 1995; 82:305–7
33. Xie Z, Dong Y, Maeda U, Alfille P, Culley DJ, Crosby G, TanziRE: The common inhalation anesthetic isoflurane inducesapoptosis and increases amyloid beta protein levels. ANESTHE-SIOLOGY 2006; 104:988 –94
34. Horsburgh K, McCarron MO, White F, Nicoll JA: The role ofapolipoprotein E in Alzheimer’s disease, acute brain injury andcerebrovascular disease: Evidence of common mechanisms andutility of animal models. Neurobiol Aging 2000; 21:245–55
36. Mori T, Town T, Kobayashi M, Tan J, Fujita SC, Asano T:Augmented delayed infarct expansion and reactive astrocy-tosis after permanent focal ischemia in apoliporprotein E4Knock-in mice. J Cereb Blood Flow Metab 2004; 24:646 –56
37. Ballard CG, Morris CM, Rao H, O’Brien JT, Barber R, StephensS, Rowan E, Gibson A, Kalaria RN, Kenny RA: APOE epsilon4and cognitive decline in older stroke patients with earlycognitive impairment. Neurology 2004; 63:1399 – 402
38. Robson MJ, Alston RP, Andrews PJ, Wenham PR, Souter MJ, DearI: Apoliporotein E and neurocognitive outcome from coronaryartery surgery. J Neural Neurosury Psychiatry 2002; 72:675–6
Dementia and Inhalational Anesthesia
Anesthesiology 2012; 116:84 –93 Cai et al.92
Downloaded From: http://anesthesiology.pubs.asahq.org/pdfaccess.ashx?url=/data/journals/jasa/931114/ on 05/31/2018
39. Tan R: Effect of propofol and isoflurane on surgical stress responseand postoperative cognitive function in elderly patients. Nan FangYi Ke Da Xue Xue Bao 2009; 29:1247–8
40. Rundshagen I, Schnabel K, Schulte am Esch J: Recovery ofmemory after general anaesthesia: Clinical findings and somato-sensory evoked responses. Br J Anaesth 2002; 88:362–8
41. Wang J, Meng F, Cottrell JE, Kass IS: The differential effectsof volatile anesthetics on electrophysiological and biochemicalchanges during and recovery after hypoxia in rat hippocampalslice CA1 pyramidal cells. Neuroscience 2006; 140:957–67
42. Dong Y, Zhang G, Zhang B, Moir RD, Xia W, MarcantonioER, Culley DJ, Crosby G, Tanzi RE, Xie Z: The commoninhalational anesthetic sevoflurane induces apoptosis and in-creases beta-amyloid protein levels. Arch Neurol 2009; 66:620–31
43. Xie Z, Culley DJ, Dong Y, Zhang G, Zhang B, Moir RD,Frosch MP, Crosby G, Tanzi RE: The common inhalationanesthetic isoflurane induces caspase activation and increasesamyloid beta-protein level in vivo. Ann Neurol 2008; 64:618–27
ANESTHESIOLOGY REFLECTIONS
Oxygenated Nitrous Oxide at Ruffner’s Dental Parlors
George S. Bause, M.D., M.P.H., Honorary Curator, ASA’s Wood Library-Museum of Anesthesiology,Park Ridge, Illinois, and Clinical Associate Professor, Case Western Reserve University, Cleveland, [email protected].
PERIOPERATIVE MEDICINE
Anesthesiology 2012; 116:84 –93 Cai et al.93
Downloaded From: http://anesthesiology.pubs.asahq.org/pdfaccess.ashx?url=/data/journals/jasa/931114/ on 05/31/2018























![INDEX [ebooks.asmedigitalcollection.asme.org]ebooks.asmedigitalcollection.asme.org/pdfaccess.ashx?url=/data/...INDEX Actual Mating ... ASME Y14.43-2003 Dimensioning and Tolerancing](https://static.documents.pub/doc/80x56/5a9ff5fb7f8b9a89178d5fd2/pdfindex-actual-mating-asme-y1443-2003-dimensioning-and-tolerancing-principles.jpg)


