38
Basic Clinician Training Module 6 Fibrinolysis and Hyperfibrinolysis TEG Analysis
| Date post: | 03-Jan-2016 |
| Category: |
Documents |
| Upload: | doreen-cori-horn |
| View: | 240 times |
| Download: | 3 times |

Basic Clinician TrainingModule 6
Fibrinolysis and Hyperfibrinolysis
TEG Analysis

Introduction
• Fibrinolysis is an essential component of hemostasis. Associated with wound healing Protective mechanism to clear thrombi from the
microvasculature• Excessive activation of the fibrinolytic pathway
(hyperfibrinolysis) can cause bleeding by several mechanisms, depending on the cause and magnitude: Breakdown of formed fibrin clot Degradation of coagulation factors (i.e. DIC) Impair clot formation due to excess generation of fibrin
degradation products • Interfere with fibrin cross-linking• Inhibit platelet function




Primary vs. Secondary HyperfibrinolysisTreatment & monitoring
• Identification of type of hyperfibrinolysis is crucial since therapies are different The wrong therapy can be fatal
• TEG analysis is able to distinguish between primary and secondary fibrinolysis.


Primary hyperfibrinolysisAs shown by TEG analysis
Common treatment:Antifibrinolytic agent

Secondary hyperfibrinolysisAs shown by TEG analysis
Common treatment:Anticoagulant

Disseminated intravascular coagulation (DIC)
Systemic and ongoingactivation of coagulation
Intravascular depositionof fibrin
Thrombosis of smalland midsize vessels
Tissue ischemiaand organ failure
Depletion of factorsand platelets
Bleeding
Levi, M & TenCate, H. NEJM. 1999;341:1999

DICCharacteristics• DIC is an acquired disorder that occurs in a
variety of clinical conditions Bacterial infections/sepsis Systemic infections Liver transplants Vascular disorders Severe trauma Solid tumors and hematological malignancies Obstetrical complications
• Placental abruptions• Amniotic fluid emboli
Reaction to toxins (snake venom, amphetamines, drugs)

DICDiagnostic characteristics• No single laboratory test can establish or rule out
diagnosis• Diagnosis requires a clinical presentation plus a
combination of test results Clinical presentation - bleeding and/or disease
state known to be associated with DIC Laboratory tests:
• Presence of soluble fibrin monomer complexes• Platelet count < 100,000/dL or rapidly decreasing
platelet count• Increased clotting times (PT, aPTT)• Presence of FDPs• Low levels of coagulation inhibitors (ATIII)
• TEG analysis also demonstrates progression of DIC

Progression of DICTEG analysis
Hypercoagulable phase• Secondary to an underlying disorder - Inflammatory state - Downregulation of physiological anti- coagulant mechanisms• Intravascular deposition of fibrin• Activation of fibrinolysis
Secondary fibrinolysis• Degradation of fibrin and fibrinogen• Generation of FDPs• FDP’s compromise clot formation and integrity• Consumption of factors and platelets
Hypocoagulable• Depletion of factors and platelets• Bleeding
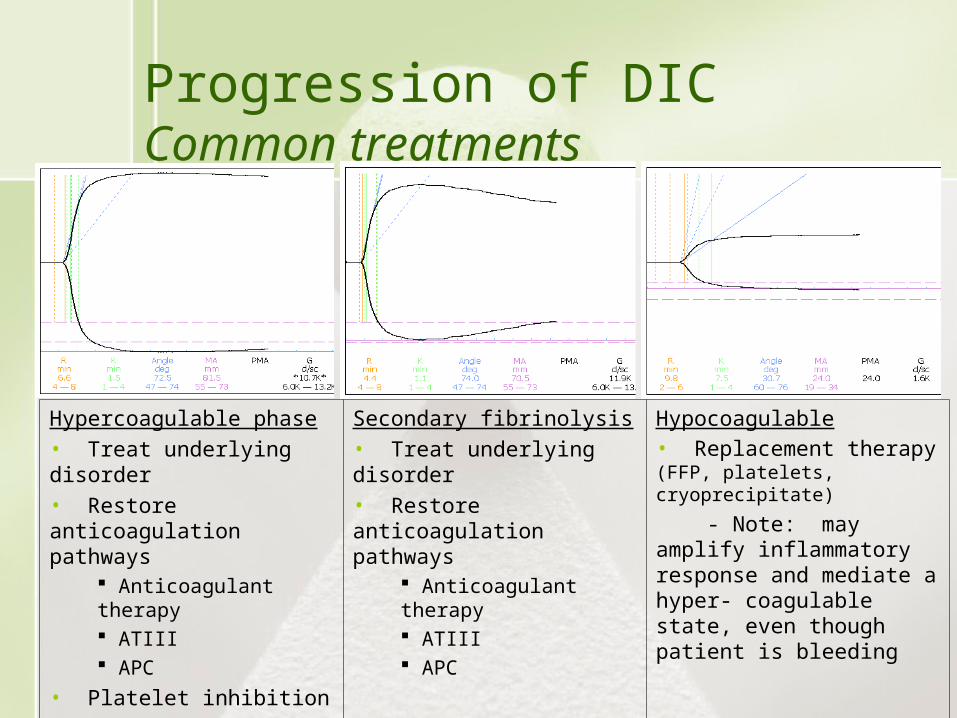
Progression of DICCommon treatments
Hypercoagulable phase• Treat underlying disorder• Restore anticoagulation pathways
Anticoagulant therapy ATIII APC
• Platelet inhibition
Secondary fibrinolysis• Treat underlying disorder• Restore anticoagulation pathways
Anticoagulant therapy ATIII APC
Hypocoagulable• Replacement therapy (FFP, platelets, cryoprecipitate)
- Note: may amplify inflammatory response and mediate a hyper- coagulable state, even though patient is bleeding

Interpretation exercises
Fibrinolysis

Exercise 1
Using the TEG Decision Tree what is a likely cause(s) of bleeding in this patient?[Select all that apply]a. Residual anticoagulantb. Surgical bleedingc. Primary fibrinolysisd. Secondary fibrinolysis
What treatment(s) would you consider for this patient?
Answer
Next

Exercise 2
Using the TEG Decision Tree what is a likely cause(s) of bleeding in this patient?[Select all that apply]a. Residual anticoagulantb. Surgical bleedingc. Primary fibrinolysisd. Secondary fibrinolysis
What treatment(s) would you consider for this patient?
Answer
Next

Exercise 3
Using the TEG Decision Tree what is a likely cause(s) of bleeding in this patient?[Select all that apply]a. Residual anticoagulantb. Surgical bleedingc. Primary fibrinolysisd. Secondary fibrinolysis
What treatment(s) would you consider for this patient?
Answer
Next
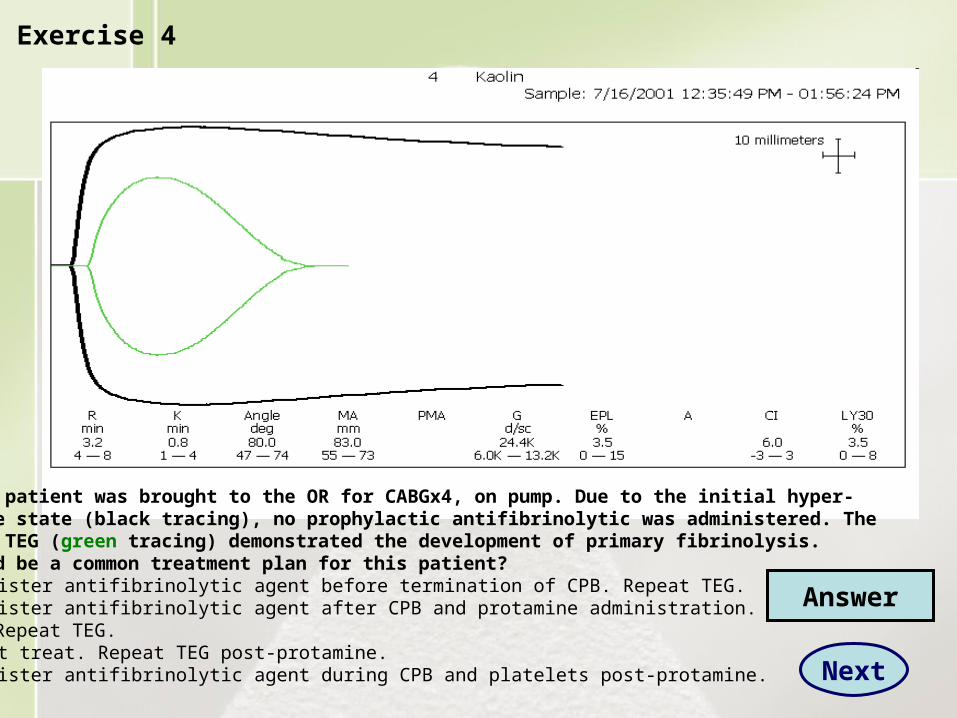
Exercise 4
The above patient was brought to the OR for CABGx4, on pump. Due to the initial hyper-coagulable state (black tracing), no prophylactic antifibrinolytic was administered. The rewarming TEG (green tracing) demonstrated the development of primary fibrinolysis.What would be a common treatment plan for this patient?a. Administer antifibrinolytic agent before termination of CPB. Repeat TEG.b. Administer antifibrinolytic agent after CPB and protamine administration. Repeat TEG.c. Do not treat. Repeat TEG post-protamine.d. Administer antifibrinolytic agent during CPB and platelets post-protamine.
Answer
Next

Exercise 5
The above patient was brought to the OR for CABGx4, on pump. While opening the chest, the surgeon commented that the patient was ‘oozy’. What is the mostly likely cause of this condition?a. Fibrinogen deficiencyb. Platelet deficiency/defectc. Fibrinolysisd. Hemodilution
Would treatment with an antifibrinolytic agent be contra-indicated? Yes or No.If no, which antifibrinolytic agent would you use?
Answer
Next

Exercise 6
Using the TEG Decision Tree what is a likely cause(s) of bleeding in this patient?[Select all that apply]a. Residual anticoagulantb. Surgical bleedingc. Primary fibrinolysisd. Secondary fibrinolysis
What treatment(s) would you consider for this patient?
Kaolin
Answer
Next

Exercise 7
Kaolin
Using the TEG Decision Tree what is a likely cause of bleeding in this patient?[Select all that apply]a. Factor deficiencyb. Platelet deficiency/dysfunctionc. Primary fibrinolysisd. Secondary fibrinolysis
What treatment(s) would you consider for this patient?
Answer
Next

Exercise 8
Kaolin
Using the TEG Decision Tree, what is your interpretation of this tracing?(select all that apply)a. Primary fibrinolysisb. Secondary fibrinolysisc. Fibrinolysisd. Surgical bleedinge. Platelet adhesion defect
Answer
Next

Exercise 9 Kaolin
Using the TEG Decision Tree, what is your interpretation of this tracing?(select all that apply)a. Primary fibrinolysisb. Secondary fibrinolysisc. Factor deficiencyd. Surgical bleedinge. Platelet adhesion defect Answer
Next

Exercise 10 Exercise
Using the TEG Decision Tree, what is your interpretation of this tracing?(select all that apply)a. Primary fibrinolysisb. Secondary fibrinolysisc. Normald. Factor deficiencye. Platelet deficiency/dysfunction
If this patient were bleeding, what treatment(s) would you consider using?
Answer
Next
Kaolin

Exercise 1
Using the TEG Decision Tree what is a likely cause(s) of bleeding in this patient?[Select all that apply]a. Residual anticoagulantb. Surgical bleedingc. Primary fibrinolysisd. Secondary fibrinolysis
What treatment(s) would you consider for this patient? Consider treating theunderlying disorder plus an anticoagulant to inhibit or reduce thrombin generation.
Back
Next

Exercise 2
Using the TEG Decision Tree what is a likely cause(s) of bleeding in this patient?[Select all that apply]a. Residual anticoagulantb. Surgical bleedingc. Primary fibrinolysisd. Secondary fibrinolysis
What treatment(s) would you consider for this patient? Antifibrinolytic agent
Back
Next

Exercise 3
Using the TEG Decision Tree what is a likely cause(s) of bleeding in this patient?[Select all that apply]a. Residual anticoagulantb. Surgical bleedingc. Primary fibrinolysisd. Secondary fibrinolysis
What treatment(s) would you consider for this patient? Explore surgical area(s) forpossible sites of bleeding and repair as needed.
Back
Next

Exercise 4
The above patient was brought to the OR for CABGx4, on pump. Due to the initial hyper-coagulable state (black tracing), no prophylactic antifibrinolytic was administered. The rewarming TEG (green tracing) demonstrated the development of primary fibrinolysis.What would be a common treatment plan for this patient?a. Administer antifibrinolytic agent before termination of CPB. Repeat TEG.b. Administer antifibrinolytic agent after CPB and protamine administration. Repeat TEG.c. Do not treat. Repeat TEG post-protamine.d. Administer antifibrinolytic agent during CPB and platelets post-protamine.
Back
Next

Exercise 5
The above patient was brought to the OR for CABGx4, on pump. While opening the chest, the surgeon commented that the patient was ‘oozy’. What is the mostly likely cause of this condition?a. Fibrinogen deficiencyb. Platelet deficiency/defectc. Fibrinolysisd. HemodilutionWould treatment with an antifibrinolytic agent be contra-indicated? Yes or No.If no, which antifibrinolytic agent would you use? Consider aprotinin for potentialplatelet protecting effects.
Back
Next

Exercise 6
Using the TEG Decision Tree what is a likely cause(s) of bleeding in this patient?[Select all that apply]a. Residual anticoagulantb. Surgical bleedingc. Primary fibrinolysisd. Secondary fibrinolysisWhat treatment(s) would you consider for this patient? Consider treating first withantifibrinolytic agent. If patient continues to bleed, repeat TEG to determineneed for platelets or factors.
Kaolin
Back
Next

Exercise 7
Kaolin
Using the TEG Decision Tree what is a likely cause of bleeding in this patient?[Select all that apply]a. Factor deficiencyb. Platelet deficiency/dysfunctionc. Primary fibrinolysisd. Secondary fibrinolysis
What treatment(s) would you consider for this patient? Consider treating with platelet transfusion. If patient continues to bleed, repeat the TEG to determinepossible contribution of fibrinolysis.
Back
Next

Exercise 8
Kaolin
Using the TEG Decision Tree, what is your interpretation of this tracing?(select all that apply)a. Primary fibrinolysis (cannot rule out)b. Secondary fibrinolysis (cannot rule out)c. Fibrinolysis d. Surgical bleedinge. Platelet adhesion defectAlthough fibrinolysis is present, the CI value is outside the values indicated for the designation as primary or secondary. Knowledge of patient history, drughistory, other laboratory tests, and bleeding status would be required to make a definitive diagnosis. A clinical presentation of DIC would suggest secondaryfibrinolysis, and treatment with an anticoagulant. If patient continues to bleed,repeat the TEG and consider treatment with an antifibrinolytic agent.
Back
Next

Exercise 9 Kaolin
Using the TEG Decision Tree, what is your interpretation of this tracing from a patient who isbleeding? (select all that apply)a. Primary fibrinolysisb. Secondary fibrinolysis (cannot rule out)c. Factor deficiency (Present, but not primary cause of bleeding. Consider treatment withantifibrinolytic agent first. Monitor patient bleeding status. If patient still bleeding, repeatthe TEG to determine extent of factor deficiency in the absence of fibrinolysis. a. Surgical bleedingb. Platelet adhesion defect
Back
Next

Exercise 10 Exercise
Using the TEG Decision Tree, what is your interpretation of this tracing?(select all that apply)a. Primary fibrinolysis (cannot rule out)b. Secondary fibrinolysis (cannot rule out)c. Normald. Factor deficiencye. Platelet deficiency/dysfunctionIf this patient were bleeding, what treatment(s) would you consider using?Although some fibrinolysis is present, it is still within normal range. Considerchecking for surgical bleeding or treatment with DDAVP. Also, check patienthistory of platelet inhibitors or possible presence of DIC. Treat accordingly.
Back
Next
Kaolin

End of Module 6

















