BCPFT-CLIN-POL-0114-154 – Management of Deliberate Self Harm Wolves CAMHS Policy Version 1.0 January 2014 Management of Deliberate Self Harm on Trust Presentation of Young People up to 18 th Birthday – Wolverhampton Policy Title State previous title where relevant. Management of deliberate self harm on hospital presentation of young people up to 18 th birthday - Wolverhampton State if Policy New or Revised New Policy Strand Org, HR, Clinical, H&S, Infection Control, Finance For clinical policies only - state index category CAMHS & paediatrics (RWHT) Links to National Regulatory Standards: Care Quality Commission(CQC) NHS Litigation Authority (NHSLA) National Institute for Health & Clinical Excellence (NICE) Mental Health Act (1983), (2007), Mental Capacity Act (2005), Children Act (1989), (2004), NICE (2004) Policy Lead/Author Job titles only CAMHS crisis team manager/ CAFS team manager/lead paediatrician (RWHT) Consultation State year and the individuals, groups, committees, service users, working partners etc. you have consulted with 2012 – self harm policy working group (Wolverhampton CAMHS & RWT Paediatric Unit and Designated Safeguarding Professionals) Ratification State ratified by whom - Policy Ratification Group, Executive Committee or Director Policy Ratification Group Equality Impact Assessment Yes Implementation Plan Yes Month/year policy first developed November 2013 Months/years policy reviewed Keep review dates in chronological order New Policy Next review due November 2016 Review details Revisions made, changes etc include page numbers and paragraphs New Policy For Corporate Executive Support use Date Policy First Uploaded to Intranet January 2014 Date Policy Revised & Reloaded to Intranet New Policy
Transcript
BCPFT-CLIN-POL-0114-154 – Management of Deliberate Self Harm Wolves CAMHS Policy
Version 1.0 January 2014
Management of Deliberate Self Harm on Trust Presentation of Young People up to 18th Birthday – Wolverhampton
Policy Title State previous title where relevant.
Management of deliberate self harm on hospital presentation of young people up to 18th birthday - Wolverhampton
State if Policy New or Revised New Policy Strand Org, HR, Clinical, H&S, Infection Control, Finance For clinical policies only - state index category
CAMHS & paediatrics (RWHT)
Links to National Regulatory Standards: Care Quality Commission(CQC) NHS Litigation Authority (NHSLA) National Institute for Health & Clinical Excellence (NICE)
Mental Health Act (1983), (2007), Mental Capacity Act (2005), Children Act (1989), (2004), NICE (2004)
Policy Lead/Author Job titles only
CAMHS crisis team manager/ CAFS team manager/lead paediatrician (RWHT)
Consultation State year and the individuals, groups, committees, service users, working partners etc. you have consulted with
2012 – self harm policy working group (Wolverhampton CAMHS & RWT Paediatric Unit and Designated Safeguarding Professionals)
Ratification State ratified by whom - Policy Ratification Group, Executive Committee or Director
Policy Ratification Group
Equality Impact Assessment Yes
Implementation Plan Yes
Month/year policy first developed November 2013
Months/years policy reviewed Keep review dates in chronological order
New Policy
Next review due November 2016
Review details Revisions made, changes etc include page numbers and paragraphs
New Policy
For Corporate Executive Support use
Date Policy First Uploaded to Intranet January 2014
Date Policy Revised & Reloaded to Intranet
New Policy
BCPFT-CLIN-POL-0114-154 – Management of Deliberate Self Harm Wolves CAMHS Policy
Version 1.0 January 2014 2
Ref. Contents Page
1.0 Introduction 3
2.0 Purpose 3
3.0 Objectives 3
4.0 Definitions 3
5.0 Duties 4
6.0 Committee/Group Responsible for Approval of this Policy 4
7.0 Process 4
8.0 Monitoring Compliance 11
9.0 Standards/Key Performance Indicators 11
10.0 Equality Impact Assessment 11
11.0 Training 11
12.0 Data Protection Act and Freedom of Information Act 11
13.0 References 12
13.1 Legislation 12
14.0 Links to other Policies and Procedures 12
Appendices
Appendix 1 13
Appendix 2 14
Appendix 3 15
Appendix 4 16
Appendix 5 17
Appendix 6 18
Appendix 7 19
Review and Amendment Log
Version Reason Status Date Description of Change
V1.0 New Policy Ratified Nov 2013 New Protocol with RWHT
Management of Deliberate Self Harm on Trust Presentation of Young People up to 18th Birthday – Wolverhampton
BCPFT-CLIN-POL-0114-154 – Management of Deliberate Self Harm Wolves CAMHS Policy
Version 1.0 January 2014 3
1.0 Introduction This policy has been jointly developed between Wolverhampton CAMHS (BCPFT) and New Cross Hospital (RWHT). It is intended to assist clinicians who provide care and treatment to children presenting to New Cross Hospital or the Phoenix walk in centre, following an act of self-harm, or where there are concerns about potential self-harm / risk to self. This policy is to apply irrespective of whether a child or young person is admitted to a children‟s, adolescent or adult ward. Adolescents between the ages of 16-18 years are given the choice in Accident and Emergency (A&E) Department of where they want to be admitted. An attempt at self-harm is a time of crisis for a child/young person and their family. The aim is that all such children/young people should be seen by a member of the Child and Family Service (CAMHS). The process of psychological assessment follows any necessary medical treatment. A time for reflection and discussion within the family is advantageous in all cases. Admission, whatever the medical status of the child/young person, allows for the above to occur. 2.0 Purpose This policy is intended to ensure that staff responsible for the care of children presenting to New Cross hospital in relation to self-harm, are aware of the specific care pathways for the management of this group of children. This policy has been developed in accordance with local and national safeguarding policy, The Mental Health Act (1983) (2007), The Mental Capacity Act (2005), NICE guidance on the management of deliberate self-harm in children and young people (2004) and The Children Act (1989) (2004). 3.0 Objectives This policy provides information regarding specific care pathways, and also provides practical guidance for the management of children and young people presenting with either actual self-harm, or risk of self-harm. This document has been developed jointly with lead paediatricians at New Cross Hospital, and is not intended to provide guidance for the management of children and self-harm in any setting other than New Cross Hospital or the Phoenix walk in centre. 4.0 Definitions For the purpose of this policy the reference to a „child‟ denotes a child or young person under the age of 18 years. „Self-harm‟ is a term used when someone injures or harms themselves on purpose rather than by accident. Self-harm is always a sign of something being seriously wrong‟ (Royal College of Psychiatrists, 2012). People self-harm in many different ways: some more obvious than others. Common methods of self-harm include overdosing, cutting parts of the body and scratching. Less common and less obvious acts of self-harm may include hair pulling, ingesting dangerous substances, inserting objects into the body, or placing oneself in dangerous situations. Assessing clinicians should use the patient‟s intent as a guide to whether or not someone‟s actions should be considered as self-harm.
BCPFT-CLIN-POL-0114-154 – Management of Deliberate Self Harm Wolves CAMHS Policy
Version 1.0 January 2014 4
5.0 Duties Multi-agency Responsibility Meeting the needs of children and young people who self-harm, or those who are at risk of self-harm, will frequently require a multi-agency approach. The medical team is responsible for the physical health and well-being of the child/young person, including assessing and treating any physical health consequence from the act of self-harm. Appropriate plans are also needed for any other need identified in physical health, e.g. arranging investigation, follow-up or referral to an appropriate specialist. The CAMHS team is responsible for assessing the mental health of the child/young person, and in conjunction with any other agencies, to make appropriate plans for their future welfare. Each agency involved is to contribute to the discharge process: all need to be satisfied that discharge is appropriate before the child/young person is actually discharged. Prior to discharge, each agency is responsible for ensuring that appropriate plans and actions are in place to safeguard the child/young person from future harm, abuse or neglect and in the context of robust „Working Together‟ arrangements. The need for consultation with the Paediatrician On-Call for Child Protection (RWHT) must be considered in circumstances where there are Safeguarding concerns (contact via main switchboard New Cross Hospital 01902 307999 / internal ext. 0). The named nurse for Safeguarding Children Wolverhampton (BCPFT) can be contacted on either 01902 44663 or 07880 567 524. 6.0 Committee/Group Responsible for Approval of this Policy The Clinical Policies group is responsible for the approval of this policy. 7.0 Process Managing Risk and Communication Good communication is essential at all stages for medical and psycho-social safety of the child/young person. This communication must be reflected in the records kept by each department and agency. Records held by the CAMHS and the hospital wards must be consistent and where possible be reflected as shared record entries. Consideration must be given to the need for face-face meeting with relevant other party / parties if a case is complex or treatment / advice is refused, with a record being kept of the discussions that take place. Consideration must be given to applying Safeguarding Children procedures if immediate or on-going risk is suspected or presents as a concern. Occasionally a child/young person may have multiple admissions during a short period of time, as a result there may be several assessments undertaken by several different clinicians. These cases suggest a high level of complexity, and it is possible that the emotional presentation of the child/young person could vary widely from one
BCPFT-CLIN-POL-0114-154 – Management of Deliberate Self Harm Wolves CAMHS Policy
Version 1.0 January 2014 5
presentation to the next. Wherever possible the same clinician should attempt to carry out multiple assessments, where this is not possible all clinicians who have assessed the child/young person should collectively reflect on their individual assessments, and any perceived level of risk, to inform the planning of interventions and management of risk. Management within the Accident and Emergency Department (Appendices 1 to 4) The medical needs of the child/young person are to be assessed and any urgent treatment administered. All children/young people should then be referred for admission. Children under 16 years of age are to be referred to Ward A21 (Paediatric Assessment Unit). Older children aged 16-18 years have the option of admission to a Children‟s Ward or an Adult Medical Ward (former preferred – see Appendix 2). This is irrespective of the number of tablets taken and/or the medical seriousness or otherwise of the deliberate self-harm attempt (see Appendix 1). The clinical condition may necessitate referral elsewhere, e.g. to ITU. Admission needs to be presented as a positive step to allow the situation to settle. If a child/young person or their carer is unwilling for admission to occur even after full discussion, a discharge can only be taken as a self-discharge against medical advice. If discharge is considered dangerous to the child/young person or others, it can be prevented by use of the Mental Health Act (see Appendix 7). Practitioners within the Accident and Emergency Department are to liaise accordingly with the CAMHS on matters of risk and vulnerability and are to complete the Confirmation Record when admission does not take place (Appendix 3 and 4). Liaison with other agencies (Social Care / Police Services) is to be undertaken according to the severity of the presenting circumstances. If the child/young person self-discharges, the CAMHS team is to be informed via tel. 70-4021 or if out of hours, by a „safe haven‟ faxed message giving relevant information (see Appendix 3 and 4). The Accident and Emergency staff must inform the parent/carer of the process and of their need to be contactable until 10am the next working day (excluding Saturday, Sunday and Bank Holidays). Social care should be contacted in all cases especially those who are self- discharging against medical advice for information and consideration of a referral. If there is immediate concern about the child/young person, the details are to be discussed with the CAMHS team member (tel. 70-4021) during normal working hours. If out of working hours, a discussion with the Paediatric Registrar and/or CAMHS On-call Clinician is to take place. Alternative help is available from the Consultant Psychiatrist (Adult Mental Health Team), or the duty Consultant Paediatrician. Consideration is to be given to a need to use the Mental Health Act (Refer to Appendix 7). If admission is not possible because of bed shortages or ward closure, the clinical assessment should not differ due to lack of beds. The A&E staff are to make an assessment (as per usual procedure) and should offer immediate medical treatment for overdose or self-harm in the A&E department or another suitable area. If out of working hours, a discussion should be held with the Paediatric Registrar and CAMHS On-call
BCPFT-CLIN-POL-0114-154 – Management of Deliberate Self Harm Wolves CAMHS Policy
Version 1.0 January 2014 6
(07900-226390 until 8 pm). Out of hours, the medical /mental health assessment can be discussed respectively with the Paediatric Registrar and the CAMHS on-call team via Penn Hospital switchboard. Consideration can be given to the need to use the Mental Health Act (Refer to Appendix 7). As recommended by the NICE guidance on self-harm (2004), all children and young people presenting with self-harm should be referred for admission. The NICE guidance does not make a distinction between self-injury and self-poisoning and recommends a comprehensive psychosocial and risk assessment in all cases. Referral for admission should be routine in cases of attempted self-strangulation, drowning, carbon monoxide poisoning, shooting, setting fire, mutilation and cutting and overdose. Cases of illicit drug ingestion or dangerous alcohol ingestion should be referred for admission for medical assessment. If there are immediate concerns „out of hours working‟ about a child/young person in A&E who is refusing admission, the CAMHS Crisis & Home Treatment Team (CAHTT) on-call Clinician is to be contacted for advice and consultation ( 07900 226390 until 8pm only). The CAMHS CAHTT do not routinely cover or conduct out of hours assessments in the A&E department, but do assess those children and young people admitted to the Children‟s Ward. Management on the Ward (Appendix 5) The child/young person should be admitted under the On-call Consultant Paediatrician or Consultant Physician (if placed on an Adult Ward). Any further medical treatment as necessary is the first priority. In cases of substance misuse, the medical team should re-assess the child or young person once they are no longer intoxicated or withdrawing from substances. Outpatient referral can be made to the SUBS team if substance misuse is a significant concern. Outpatient or, occasionally, inpatient referral can be made to CAMHS if significant mental health concerns are identified. If the child/young person is on the Children‟s Ward, the CAMHS referral form is to be completed and contact by CAMHS awaited. Any additional information that maybe relevant for the CAMHS assessment (such as details of social care involvement) should be attached to the referral form. If the young person is on an Adult Ward, a referral is to be accepted by the Adult Mental Health Crisis Team (who are to inform CAMHS of the outcome of their risk assessment). Practitioners working in EAU are to follow these procedures. The referral to the CAMHS / Adult Mental Health Crisis Team should be recorded in the medical notes. It is essential that the carer/guardian and the child/young person are informed that a referral has been made. The child/young person needs to be medically fit prior to undertaking the mental health assessment. Children/young people, who require medical treatment that is likely to last overnight, should be seen and assessed on the day that they are likely to be medically fit for discharge, rather than being assessed by CAMHS at the beginning of their admission. This practice will avoid unnecessary duplication of assessments.
BCPFT-CLIN-POL-0114-154 – Management of Deliberate Self Harm Wolves CAMHS Policy
Version 1.0 January 2014 7
Response to Referrals by CAMHS Routine enquiry with Social Care Services As routine practice, CAMHS are expected to make enquiries to ascertain if the child/young person is known to Social Care services when engaging with the child/young person and their family. An understanding of the level of need or concern relating to a child/young person that has necessitated the involvement of Social Care services and relating to whom a CAMHS assessment is required, is considered fundamental for analysis of vulnerability and risk and for on-going care planning and multi-agency service delivery. During office Hours (Monday to Friday 9am to 5pm) Referrals made to CAMHS by 12 noon are likely to be seen the same day by the CAMHS worker. Referrals made after 12 noon may be seen the next working day.
Out of office hours (Evening, Weekends and Bank Holidays) The CAMHS on-call Clinician contacts the ward at 9am, children / young people already on the ward will be seen the same day. Children / young people who are admitted after 9am will be seen the following day, unless there are immediate concerns about risk, safety, and / or management. Under such circumstances the ward should contact the CAMHS On-call Clinician (tel 07900 226390 until 8pm only) to discuss concerns. If an out of hours assessment is required, the ward staff should inform the child / young person and their carer of the CAMHS referral and arrange for a parent/carer to be available for the assessment.
After seeing the child/young person and their carer(s), the CAMHS clinician is to inform either the ward Sister or the ward Registrar as to „if‟ and „when‟ the child/young person is suitable for discharge. There should be an entry in the hospital records to this effect in addition to relevant background information that might help staff support the child/young person.
Out of hours or at weekends, if a child/young person needs to be discharged before a CAMHS assessment, discharge is to be at the discretion of the supervising Consultant Paediatrician (or Physician, if on an Adult Ward). The Consultant should only agree to discharge if it is considered safe and with the agreement of the child/young person and their parent/carer that there will be continuous responsible adult supervision of the child/young person until a CAMHS assessment can take place. The CAMHS On-call Clinician can be contacted (07900 226 390) to discuss the situation and advise on when a CAMHS assessment is likely to be offered.
During office hours if the child / young person or their carer threatens premature discharge from the ward, the CAMHS team is to be informed and a face to face meeting is to take place to discuss the best options for the child/young person‟s safety and wishes. If needed, a multi-agency strategy meeting is to be convened with comprehensive details of the discussion and outcomes recorded. The CAMHS clinician is to ensure that any documentation sited within the hospital records is consistent with that held separately by the CAMHS. Clear entries should be made by all parties in the existing clinical health records. If a child/young person or their parent/carer threatens premature discharge out of hours, the CAMHS on-call Clinician is to be contacted to discuss the situation.
BCPFT-CLIN-POL-0114-154 – Management of Deliberate Self Harm Wolves CAMHS Policy
Version 1.0 January 2014 8
If the child/young person absconds from the ward during office hours, the CAMHS team is to be notified to discuss the next steps. During out of hours, the CAMHS On-call Clinician is to be contacted for a discussion on the next steps. A possible outcome may be to inform the Police service of the self-discharge by a vulnerable child/young person who may be considered „at risk‟. If it is considered that an urgent psychiatric assessment is needed: During normal hours 9am to 5pm- contact the CAMHS team
Out of hours - For those admitted to the Children‟s Ward the CAMHS On-call Clinician is to be contacted 07900 226 390.
Young people admitted to an Adult Ward remain the responsibility of the Adult Mental Health Crisis Team until handover to the CAMHS, and are to be contacted on Tel. 70-5810 / 4141 or bleep 1704).
All cases assessed as high risk are to be brought to the attention of the appropriate CAMHS manager by the CAMHS clinician undertaking the initial assessment. High risk cases requiring a transfer to a specialist CAMHS unit or an admission to Charlemont Ward at Hallam Street Hospital in the absence of an available CAMHS bed need to be discussed with the On-call clinician from CAMHS and the On-call manager from BCPFT. The duty On-call manager for BCPFT can be contacted via Penn-hospital reception 01902-444141 The management of high risk cases is to be discussed and reviewed at the weekly CAMHS senior clinicians‟ multidisciplinary meeting until such time as the risks are considered to have reduced. Discharge and Follow-up by CAMHS (Appendix 7) Most children/young people admitted after an act of self-harm are discharged the same day after being seen by the CAMHS practitioner. Discharge should only be with CAMHS agreement and no in-patient medical treatment needed. Any current involvement of a key agency e.g. Children‟s Social Care services, also need to agree to the discharge before it takes place. Discharge is to be co-ordinated by the medical team who are to ensure that they know CAMHS‟ (and any other agency‟s) recommendations on discharge. Arrangements are to be made regarding any medical follow-up if needed.
For all admissions, prior to discharge, the CAMHS team and ward medical team should consider the need to hold a multi-agency pre-discharge planning meeting. Examples for need for such a meeting would be repeated risky self-harm behaviours, life-threatening self-harm act, and possible safeguarding concern. This list cannot be comprehensive; the expertise of experienced practitioners is needed to arrive at appropriate judgment. If either team considers a multi-agency meeting desirable then a written entry should be made in both hospital and CAMHS records of this view and, if meeting not held, clear reasons why not.
BCPFT-CLIN-POL-0114-154 – Management of Deliberate Self Harm Wolves CAMHS Policy
Version 1.0 January 2014 9
Understanding the views of the child/young person Records held by both the CAMHS and the hospital service must reflect the dialogue that has taken place directly with the child and their perspective on their needs, their opinions on care planning and management of their needs and their impression of the impact on their well-being as a result of service intervention.
If there is disagreement on the needs of the child/young person, senior practitioners (e.g. Consultant for the medical team) from all involved agencies should engage to find a solution. If a referral has been made to Social Care services (Children‟s Services) the actions that Social Care are taking must be clearly understood and documented in the records.
In circumstances where the mental health status of the child/young person is assessed
as „high risk‟, a full mental health assessment and closer follow-up is required, e.g. telephone contact or home visit every day or two. The child/young person should not be discharged by CAMHS for non-attendance. There must be liaison with other key agencies (e.g. social worker, school nurse, school) involved to exchange information and ascertain risk.
In circumstances where there is more than one CAMHS practitioner engaged in repeat/on-going assessments and review of the child/young person‟s progress (whilst hospitalised or in the community setting), robust communication between all CAMHS practitioners as involved must be maintained, to ensure that full appraisal of needs and risks are informed by the contributions of all associated clinicians.
Any medication prescribed for the child/young person must be supported with written guidance and parents/carers who are overseeing the administration of medication must be made aware of such guidance prior to hospital discharge.
Parents/carers are to be provided with relevant information and guidance by CAMHS regarding how to maintain the child/young person‟s safety and reduce further risk of acts of self-harm when discharged back into the community. Any concerns regarding the ability to keep the child/young person safe as expressed by the parents/carers are to be duly addressed and the management of their concerns documented. A follow-up appointment with CAMHS is to be offered within seven days, unless there are exceptional circumstances i.e.:
i. The child/young person remains on the ward for further assessment by the local Child and Adolescent Psychiatrist (to be completed within 24 – 48 hours).
ii. The child/young person remains on the ward for further assessment by a specialist colleague from the regional tier 4 CAMHS unit.
iii. The child/young person remains on the ward until further assessed by
Social Care and/or Police services.
BCPFT-CLIN-POL-0114-154 – Management of Deliberate Self Harm Wolves CAMHS Policy
Version 1.0 January 2014 10
If the child/young person fails to attend their follow-up appointment with CAMHS the family should be contacted the same day. If the family persistently fails to engage consider a home visit and inform the GP, associated hospital clinicians and (if involved) the Social Care team.
If the child/young person refuses a follow-up appointment at the time of assessment, they and their carer(s) are to be given a card detailing CAMHS address and telephone number in the event that they need to make contact in the future. If necessary, this arrangement should be discussed beforehand with the Consultant Child and Adolescent Psychiatrist/Psychologist.
The Children‟s Liaison Service is to ensure that the „named‟ health practitioner (e.g. School Nurse/Looked After Children Nurse) for the child/young person is notified of key details relating to the hospital presentation and stay. The Children‟s Liaison Service is to ensure that the Named Nurse for Safeguarding Children who is responsible for supporting local CAMHS/Adult Mental Health Services (for. BCPFT) is notified of all presentations/admissions of children/young people who present at the hospital following an act of self-harm. Looked After Children and Young People All staff should be aware that Looked After Children and young people (children and young people voluntarily accommodated via Section 20 Children Act 1989 or where a court order is in place enabling the Local Authority to exercise Corporate Parenting responsibilities via Section 31 Children Act 1989), are a particularly vulnerable group who may be more likely to present to the Accident and Emergency Department with either thoughts or actual acts of self-harm. Looked After Children and young people have experienced change and instability in their lives: they are also likely to be less emotionally resilient than those children and young people who have not had contact with the care system. Staff caring for such children and young people should be aware that there are often multiple professionals involved in their care, and in a number of cases, the Local Authority may share parental responsibility with the parents. Staff should ensure that they inform all relevant professionals of the child/young person‟s admission, the presenting circumstances and any risks. Training and Knowledge of Procedures As part of any induction programme, practitioners working within the CAMHS, Accident and Emergency Department, Children‟s Ward, EAU and the Adult Wards on which young people may be admitted, are to become familiar with this policy.
Initiated July 1998/updMay08/updApr09/updJun1/updMarch2012/updFeb13/updMarch2013
BCPFT-CLIN-POL-0114-154 – Management of Deliberate Self Harm Wolves CAMHS Policy
Version 1.0 January 2014 11
8.0 Monitoring compliance Monitoring compliance to this document will be through an annual review of the patients documentation and journey and their adherence to the policy. This will be based on BCPFT responsibilities regarding this policy. The monitoring will form part of the annual record keeping audit. The outcomes of the audit will be shared with the Directorate Risk Action group. Any shortfalls will be presented as part of an action learning set and at team meetings to ensure wider learning is cascaded. This policy and subsequent audits are to be monitored within governance structure of RWT and also through the JHSCC. 9.0 Standards / key performance indicators
Key Performance Indicator Method of Assessment
1. Number of patients with CAMHS involvement and adherence to policy
A random audit annually to determine a selection of patients who are affected by this policy and the adherence by a review of their clinical notes and documentation
10.0 Equality Impact Assessment “The Black Country Partnership NHS Foundation Trust is committed to ensuring that the way we provide services and the way we recruit and treat staff reflects individual needs, promotes equality and does not discriminate unfairly against any particular individual or group. The Equality Impact Assessment for this policy has been completed and is readily available on the Intranet. If you require this in a different format e.g. larger print, Braille, different languages or audio tape, please contact the Equality & Diversity Team on 0121-612-8067 or email [email protected]”
11.0 Training All new clinical staff are directed to familiarise themselves with this policy as part of the standard induction process to Wolverhampton CAMHS. Specialist training on risk assessment is conducted internally as required, the need for this training and frequency is decided by the appropriate service manager.
12.0 Data Protection Act and Freedom of Information Act All staff have a responsibility to ensure that they do not disclose information concerning the Trust‟s activities or about service users in its care to unauthorised individuals. This responsibility applies whether you are currently employed or after your employment ends and in certain aspects of your personal life e.g. use of social networking sites etc. The Trust seeks to ensure a high level of transparency in all its business activities but reserves the right not to disclose information where relevant legislation applies.
BCPFT-CLIN-POL-0114-154 – Management of Deliberate Self Harm Wolves CAMHS Policy
Version 1.0 January 2014 12
13.0 References Self-Harm – The short-term physical & psychological management & secondary prevention of self-harm in primary & secondary care (NICE, 2004) The Mental Health Act (1983), (2007) The Children Act (1989), (2004) Working Together to Safeguard Children (2010) 13.1 Legislation The Mental Health Act (1983), (2007) The Children Act (1989), (2004) Working Together to Safeguard Children (2010)
14.0 Links to other Policies and Procedures Local & National Safeguarding procedures Department of Health Confidentiality: NHS Code of Practice
BCPFT-CLIN-POL-0114-154 – Management of Deliberate Self Harm Wolves CAMHS Policy
Version 1.0 January 2014 13
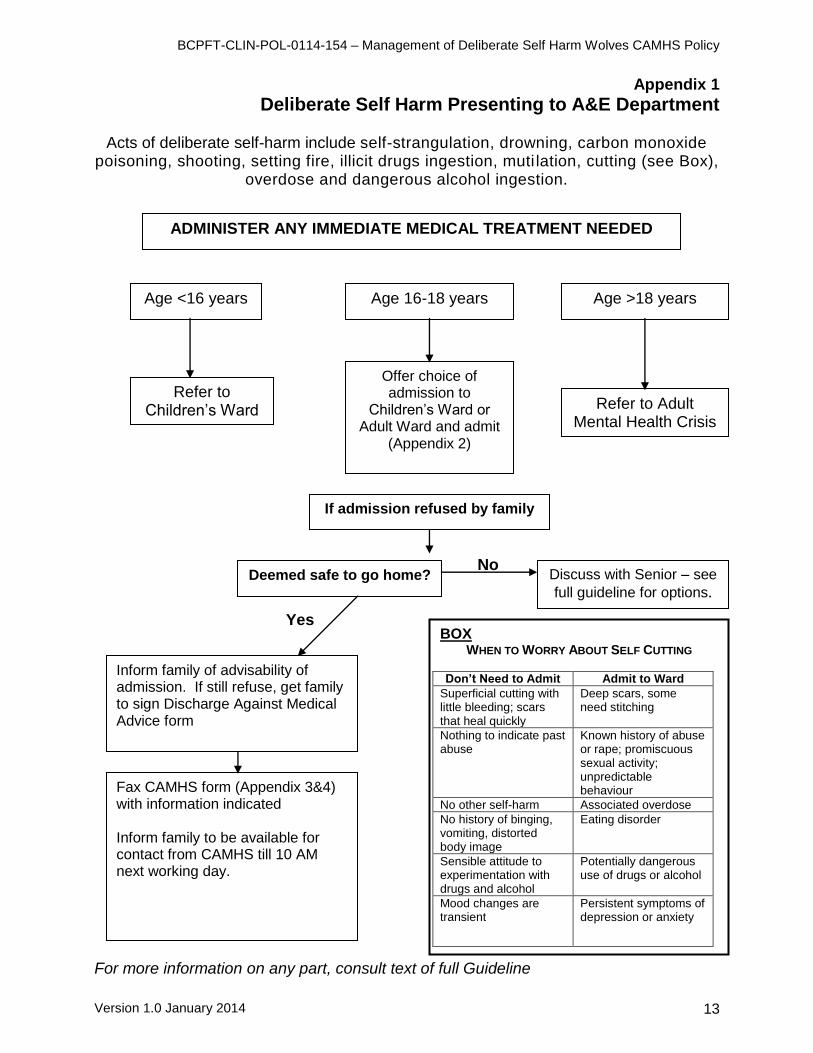
Appendix 1
Deliberate Self Harm Presenting to A&E Department
Acts of deliberate self-harm include self-strangulation, drowning, carbon monoxide poisoning, shooting, setting fire, illicit drugs ingestion, muti lation, cutting (see Box),
overdose and dangerous alcohol ingestion.
No
Yes For more information on any part, consult text of full Guideline
Age 16-18 years Age >18 years
Refer to Adult Mental Health Crisis
Worker
Age <16 years
Refer to Children‟s Ward
ADMINISTER ANY IMMEDIATE MEDICAL TREATMENT NEEDED
Offer choice of admission to
Children‟s Ward or Adult Ward and admit
(Appendix 2)
If admission refused by family
Deemed safe to go home?
Fax CAMHS form (Appendix 3&4) with information indicated Inform family to be available for contact from CAMHS till 10 AM next working day.
Discuss with Senior – see
full guideline for options.
Inform family of advisability of admission. If still refuse, get family to sign Discharge Against Medical Advice form
BOX WHEN TO WORRY ABOUT SELF CUTTING
Don’t Need to Admit Admit to Ward
Superficial cutting with little bleeding; scars that heal quickly
Deep scars, some need stitching
Nothing to indicate past abuse
Known history of abuse or rape; promiscuous sexual activity; unpredictable behaviour
No other self-harm Associated overdose
No history of binging, vomiting, distorted body image
Eating disorder
Sensible attitude to experimentation with drugs and alcohol
Potentially dangerous use of drugs or alcohol
Mood changes are transient
Persistent symptoms of depression or anxiety
BCPFT-CLIN-POL-0114-154 – Management of Deliberate Self Harm Wolves CAMHS Policy
Version 1.0 January 2014 14
Appendix 2
Where to Admit 16 – 18 Year Olds 1. Under 16s are admitted to Children‟s Wards regardless of which medical or surgical team is in charge of the patient. 2. Between ages of 16 and 18 years there is discretion where to admit the patient based on their clinical needs (e.g. needs specialist medical or nursing care not available on children‟s ward), wishes of the patient, and the needs of the other patients in the children‟s wards or adult wards. 3. The suggestions below are a guidance to help decide where to place such patients. If shortage of beds in adult wards or children‟s wards, flexibility may be needed to meet patient needs. 4. Deliberate Self Harm patients age 16-18 years (who will also be seen by CAMHS team within 24 hours) should preferably be admitted to children‟s ward UNLESS they are anticipated to be disruptive in which case they should be referred to adult team for admission. [If admitted to children‟s ward there is otherwise risk to others on the ward who can include babies without resident parent]. If admitted to adult ward, the adult mental health liaison worker will pass on the admission information to the CAMHS team. NB: 16-18 year olds admitted to children‟s ward can be looked after by the relevant (adult) medical or surgical team on this ward, without need for paediatrician to be involved.
BCPFT-CLIN-POL-0114-154 – Management of Deliberate Self Harm Wolves CAMHS Policy
Version 1.0 January 2014 15
Appendix 3
FAX Confirmation Record
DELIBERATE SELF HARM IN UNDER 18’s
To be faxed with the NON-ADMISSION NOTIFICATION FORM (Appendix 4) TO CAMHS FROM EMERGENCY DEPARTMENT
SENDER NAME
DATE &TIME
YOUR CONTACT
DETAILS
TOTAL NUMBER OF
SHEETS FAXED
THIS RECORD SHOULD THEN BE SCANNED WITH ALL OTHER DOCUMENTATION INTO THE MSS SYSTEM FOR CONFIRMATION OF
SENDING
CAMHS FAX NUMBER – 70-6633 INTERNAL 01902 446633 IF OUTSIDE NEW CROSS HOSPITAL
BCPFT-CLIN-POL-0114-154 – Management of Deliberate Self Harm Wolves CAMHS Policy
Version 1.0 January 2014 16
Appendix 4
DELIBERATE SELF HARM IN UNDER 18s NON-ADMISSION NOTIFICATION FORM TO CAMHS FROM A&E DEPT
(OR BY PAEDIATRIC OR LIAISON HV TEAM)
Date Time Taken By
Name
DOB/AGE MALE / FEMALE
NHS No
Address
Postcode
Tel No:
Name of Parent/Carer
Name / Address of
School / College
Name / Address
of GP
Was Young Person Accompanied
by Parent / Carer?
Yes No Please Tick
If No, Please Indicate who Accompanied
the Young Person
Was the Young Person Informed that
CAMHS will Make Contact?
Yes Please Tick
(Please inform if possible)
Details of Deliberate Self Harm
Details of social care involvement with child and/or family
Name: Contact No or Bleep:
Designation:
Please Fax form to 70-6633 (or 01902 446633 if from outside New Cross)
Section Group Code
White British A
Irish B
Other White Background C
Mixed White & Black Caribbean D
White & Black African E
White & Asian F
Any other mixed background G
Asian /Asian British Indian H
Pakistani J
Bangladeshi K
Any other Asian background L
Black/Black British Caribbean M
African N
Any other Black background P
Other Ethnic Group Chinese R
Any other Ethnic group S
Not Stated Not given/Refused Z
BCPFT-CLIN-POL-0114-154 – Management of Deliberate Self Harm Wolves CAMHS Policy
Version 1.0 January 2014 17
Appendix 5
Deliberate Self Harm Patient on Ward
(Children’s Ward or Adult Medical Ward)
ADMINISTER ANY MEDICAL TREATMENT NEEDED
Inform patient / carer(s) of need to see CAMHS worker to look at reasons behind self-harm act, and interventions that may help.
Children’s Ward: complete CAMHS referral form (see Appendix 6) and await contact from CAMHS
CAMHS will usually see within one working day and when medically fit
Discharge patient once CAMHS (and any other involved agency) say safe to do so, and medically no need to remain in-patient. Ensure family have follow-up plan with CAMHS and any medical follow-up needed.
If patient threatens premature discharge, inform Senior – see full guideline for options
Out of hours, if patient in need of urgent psychiatric assessment, see Paragraph 6 for options
Adult Mental Health Crisis Team will arrange further assessment and intervention as available.
If patient absconds from ward inform CAMHS or, if out of hours, consider informing Police (see full guideline)
Adult Ward: Adult Mental Health Crisis Worker will assess and liaise with CAMHS team.
BCPFT-CLIN-POL-0114-154 – Management of Deliberate Self Harm Wolves CAMHS Policy
Version 1.0 January 2014 18
Appendix 6
Deliberate Self Harm – Action for CAMHS Team
For more information on any part, consult text of full Guideline and consult Departmental guideline
Referral received from Children‟s Ward or Adult Medical Ward of Deliberate Self Harm patient awaiting CAMHS assessment
Contact ward to inform Nurse in Charge when patient will be seen. Ask for main carer / guardian to also be present at that time As routine practice, make enquires to ascertain if the patient is in receipt of Social Care services
Patient Assessed
Safe for Discharge Arrange follow-up for patient.
Inform medical team. Not Safe for Discharge Arrange further psychiatric assessment as needed (see full guideline for options).
If Safeguarding Children concern: Use existing inter-agency Safeguarding Children procedures
Patient does not attend follow-up: Contact patient by phone to determine risk. Discuss further with senior if needed.
Patient / Carer threatens own discharge: Meet face to face with medical team to lay best plan available. Consider multi-agency strategy meeting. Consult senior if needed.
BCPFT-CLIN-POL-0114-154 – Management of Deliberate Self Harm Wolves CAMHS Policy
Version 1.0 January 2014 19
Appendix 7
Uses of relevant Mental Health legislation for paediatric patients
1) The Mental Health Act 1983, amended by the Mental Health Act 2007, can be used on any paediatric patient who has a mental disorder and who may be a risk to themselves or others. There is no lower age limit. Mental disorder is defined as: „any disorder or disability of mind‟. Risks to self may include suicide or deterioration in health. If there is a risk of significant harm to others, it may be more prudent to let the young person leave hospital, rather than prejudice the care of other young patients by trying to keep him or her on the children‟s ward.
2) A & E: The only way someone can be kept in A & E once they are there is by a section 2 (28-day assessment order), which requires a psychiatrist, a second doctor, an Approved Mental Health Practitioner (the new name for an Approved Social Worker) and an inpatient bed (which can be paediatric if there are no adolescent psychiatric beds immediately available; beds on adult psychiatric wards should not in general be used for under-18s – see (5) below). This takes some time (usually over an hour) to set up – but it can be quicker if the young person freely consents to psychiatric admission. The young person can be kept in A & E under parental consent or common law in the meantime. If the young person tries to run away, the senior clinician present has to balance the young person‟s need for constraint against the risks of exercising constraint (to other patients and those doing the constraining). The majority of young people will however stay in one place if they are told they have to.
3) If a young person has run out of A & E, the police can be requested to bring them back, utilising the powers of section 136 (police holding order) if there is reason to suspect a mental disorder (no diagnosis is necessary) and risk to self or others. The police are not allowed to do this for someone in their own home or in A & E. They may take them to the police station rather than back to A & E – for instance if the senior clinician present thinks the risks of waiting in A & E is too great. The police should then stay with the young person in A & E until a section 2 assessment has been completed, which should lead either to the young person being allowed to leave, or to being admitted (possibly to a children‟s ward).
4) If a young person agrees to come onto the children‟s or adult ward, and then changes their mind, they can be kept in against their will, using either:
a) Common law (for limited periods of a few hours);
b) Parental consent (for limited periods of a few days) – not recommended for those who are thought to be Gillick competent to refuse admission.
c) The Children Act (1989). Those looking after a child or young person on a children‟s ward may do „what is reasonable in all the circumstances of the case for the purpose of safeguarding or promoting the child‟s welfare‟ (section 3(5)). Whether the intervention is reasonable or not will depend
BCPFT-CLIN-POL-0114-154 – Management of Deliberate Self Harm Wolves CAMHS Policy
Version 1.0 January 2014 20
upon the urgency and gravity of what is required and the extent to which it is practicable to consult a person with parental responsibility. For instance, if an 11-year-old is being treated on a children‟s ward, becomes distressed and attempts to leave, then he can be prevented from leaving by any member of staff involved in his care, if it is thought that he is vulnerable to harm beyond the safety of the hospital ward. The maximum period during which a child or young person‟s liberty may be restricted without either parental consent ((b) above) or a Mental Health Act order ((d) and (4) below) or the authority of a court (section 25 Children Act 1989) is 72 hours, either consecutively or in aggregate in any period of 28 days.
d) A Mental Health Act section 5(2). This is a holding order for 72 hours. This is signed by the responsible consultant (paediatrician) and the duty administrator / manager. The necessary papers are usually kept in A & E or on any psychiatric ward (for instance, Penn Hospital). The expectation is that a section 2 assessment will be arranged before the 72 hours is over – but sometimes the section 5 order is simply allowed to lapse.
5) A young person can be kept on a children‟s ward under a section 2, if necessary with agency Registered Mental Health Nurses (requiring special funding from the commissioners). This should in general only be necessary until an appropriate adolescent psychiatric bed can be found. Residence for any length of time on the children‟s ward may be inadvisable if the young person presents a risk to other paediatric patients – despite the extra nursing. The Mental Health Act 2007 effectively makes admission of under-18s to adult psychiatric wards illegal – unless there is a professional consensus that this is the best option for the young person. This would usually be only if a young person is very nearly 18 years old, or in exceptional circumstances. The need to avoid admission of under-18s to an adult psychiatric ward puts pressure on commissioners to fund emergency adolescent psychiatric provision, on inpatient units to provide emergency access to beds, and on community CAMHS services to provide out-of-hours services to enable more young people to be managed in the community – but in the absence of any of these, on children‟s wards and staff!
6) The Mental Capacity Act (2005) applies to over-16s. It can be used to enable decisions to be made on behalf of a young person – usually by someone with parental responsibility, but sometimes by professionals. An over-16 can be considered unable to make a particular decision only if: a) He or she has „an impairment of, or disturbance in, the functioning of the
mind or brain‟, whether permanent or temporary; AND b) He or she is unable to undertake any of the following steps:
i. Understand the information relevant to the decision; ii. Retain that information; iii. Use or weigh that information as part of the process of making the
decision; iv. Communicate the decision made (whether by talking, sign language
or other means). Decision-making capacity is decision-specific and time-specific. When decisions are made on behalf of someone who lacks capacity, they must be
BCPFT-CLIN-POL-0114-154 – Management of Deliberate Self Harm Wolves CAMHS Policy
Version 1.0 January 2014 21
made in his / her best interests. In practice, most such patients encountered by paediatricians will have learning difficulties, and should have carers who can make appropriate decisions for them. It should be noted that the Mental Capacity Act cannot be used if a deprivation of liberty is involved (such as keeping a child on a children‟s ward against their expressed wishes) – in which case another route must be taken.
7) The Code of Practice to the Mental Health Act (2007) introduces the concept of The Zone of Parental Control. This means what an adult can decide about a child under 16 or a young person of 16 or 17 for whom she or he has parental responsibility. Medical procedures on children under 16 would normally fall within the zone of parental control, providing: a) The decision is one that a parent would normally be expected to make.
More extreme interventions are likely to fall outside the zone. b) There are no indications that the parent might not act in the best interests
of the child. If there could be a conflict of interest for the parent (as might occur after an acrimonious divorce), or if the child has alleged abuse by the parent, then professionals may decide to restrict the zone of parental control.
c) There is no reason to suppose the parent lacks the capacity to consent (for instance due to substance misuse or learning disability).
d) The young person agrees with the treatment proposed. If the young person is resisting, then more justification is needed to use parental consent alone.
Decisions regarding 16- and 17-year-olds are likely to fall within the zone of parental control only if the young person lacks the ability to consent for themselves (see previous section).
8) Recent changes in legislation, and its interpretation by case law, have had the effect of giving more power to the child: there are hoops to jump through to admit or treat a 16- or 17-year-old without their own consent; and the views of under-16‟s must be sought. A Gillick-competent under-16 should in general not be admitted or treated on parental consent alone.
9) The exception to this is in an emergency: if the failure to treat is likely to lead to the child or young person‟s death or to severe permanent injury the child or young person may be treated without any consent. Treatment under these circumstances is limited to what is necessary to save the child or young person‟s life or prevent an irreversible serious deterioration of their condition. Once the child or young person‟s condition is stabilised, the legal authority for providing any further treatment must be clarified.
10) Legal advice should be sought in any situation where the best way forward is unclear. While waiting for this, you are unlikely to be criticised for choosing what appears – after discussion with colleagues – to be the safest option.
Prepared by
Dr Quentin Spender, Consultant CAMHS, February 2009