Page 1
M. BöhmInnere Medizin III (Kardiologie / Angiologie / Internistische Intensivmedizin)
Universitätsklinikum des Saarlandes
Homburg/Saar
[email protected]
Behandlung der systolischen
Herzinsuffizienz
Page 2
McMurray et al, Eur Heart J (2012) doi:10.1093/eurheartj/ehs104 AS-bb9-0512
Page 8
Faris et al, Int J Cardiol 82 (2002): 149-158 AS-af2-0616
Page 9
Withdrawal in Patients on ACE-Inhibitors
(Cross over)
Richards.pptRichardson et al., Lancet 1987;II:709-711
A 14 Pts.
- Captopril (3x25 mg)
- Furosemide (40 mg)
+ Amiloride (5 mg)
10 Pts.
(stable)
3 Months
stableCaptopril
4 Pts.
Pulmonary Edema
(11d, 33d, 8d, 16d)B 14 Pts.
- Furosemide (40 mg)
+ Amiloride (5 mg)14 Pts.
(stable)No Withdrawals
Page 10
Walma et al, BMJ 315 (1997): 464-468 AS-af-0102
Withdrawal of Diuretic inOlder Individuals without Ouvert CHF
2 4 6 8 10 12 14 16 18 20 22 24 260
0
0.2
0.4
0.6
0.8
1.0
Control group (n=100)
Withdrawal group (n=102)
P<0.001
Pro
po
rtio
n W
ith
ou
t R
ein
itia
tio
n
Weeks after withdrawal of diuretics
Page 11
Walma et al, BMJ 315 (1997): 464-468 AS-ag-0102
Withdrawal of Diuretics inOlder Individuals without Ouvert CHF
Criterion
All
Heart Failure
Hypertension
Subjective shortness of breath
Non-cardiac ankle oedema
Miscellaneous clinical conditions
Other
Withdrawal group(n=102)
50
25
9
6
4
3
3
Control group(n=100)
13
4
5
0
1
1
2
Risk difference (%)(95% CI)
36 (22 to 50)
21 (11 to 31)
4 (-3 to 11)
6 (1 to 11)
3 ( -1 to 8)
2 (-2 to 6)
1 (-3 to 5)
Page 15
Bisoprolol-first (o.d.)
Enalapril-first (b.i.d.)
Bisoprolol o.d.
Enalapril b.i.d.
Bisoprolol o.d.
Enalapril b.i.d
week Study end
1 - 2.5 years
0 2 4 6 8 10 26 28 30 32 34 36week Study end
1 - 2.5 years
First up-titration
First up-titration
Second up-titration
Second up-titrationMaintenance period
Maintenance period
Second maintenance period
22-100 weeks
Second maintenance period
16-94 weeks
1.252.5
3.755.0
7.5
1.252.5
3.755.0
7.5
2.5 5.0
2.5 5.0
* * * * * * * * * * * * * * * * ……….……. * * * * *
* = visits
10.0 mg
10.0 mg
10.0 mg
10.0 mg
Study design – CIBIS III
Bisoprolol o.d.
Enalapril b.i.d
0 2 4 6 8 10 26 28 30 32 34 36* * * * * * * * * * * * * * * * ……….……. * * * * *
DOI: 10.1161/CIRCULATIONAHA.105.582320
PP-A-0905.9
Page 16
Intention-to-treat (ITT)
50
60
70
80
90
100
0 6 12 18
Per-protocol (PP)
50
60
70
80
90
100
0 6 12 18
Primary endpoint – CIBIS III
% without
endpoint
% without
endpoint
B/E vs E/B
HR 0.97 (95% CI 0.78-1.21)
non-inferiority P=0.046
B/E vs E/B
HR 0.94 (95% CI 0.77-1.16)
non-inferiority P=0.019
503498
356353
265259
8073
505505
389388
291277
8776
months
months
For non-inferiority
P<0.025 denotes
statistical significance
(unilateral test)
DOI: 10.1161/CIRCULATIONAHA.
105.582320
Bisoprolol-first
Enalapril-first
Patients at risk
Patients at risk
Mean follow-up
1.25 years
PP-A-0905.15
Page 17
Worsening of CHF throughout study
Bisoprolol-first was associated with a trend
towards increased worsening of CHF in the
early phase of treatment.
Time (months)
70
75
80
85
90
95
100
0 6 12 18
B/EE/B
All cause mortality at end of monotherapy phase
Bisoprolol-first showed a trend towards
improved survival during the early study
phase (which was maintained
during combined therapy).
Time (months)
75
80
85
90
95
100
0 1 2 3 4 5 6
B/EE/B
Bisoprolol-first achieved clinically
comparable survival and all-cause
hospitalization compared with enalapril-first.
Primary endpoint PP
40
50
60
70
80
90
100
0 6 12 18
B/EE/B
Time (months)
% event-free
DOI: 10.1161/CIRCULATIONAHA.105.582320
Food for Thoughts – CIBIS III
PP-A-0905.30
Page 19
Selye, Proc Soc Exp Biol Med 104 (1960): 109-111 AS-au2-0616
Page 20
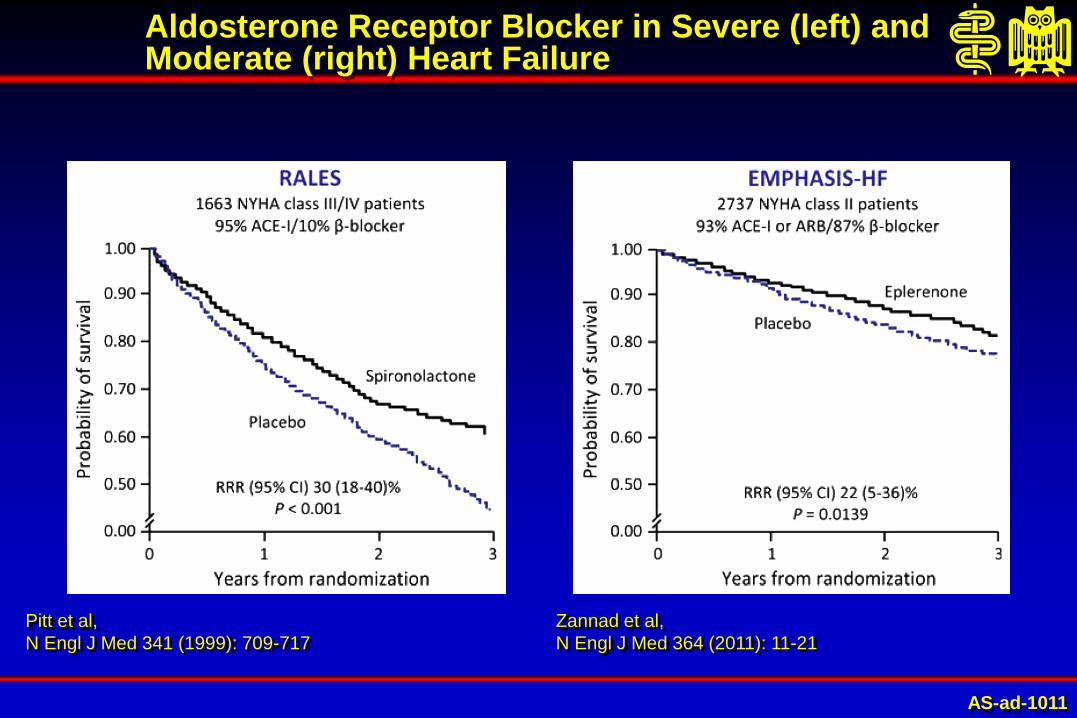
Pitt et al,
N Engl J Med 341 (1999): 709-717
AS-ad-1011
Aldosterone Receptor Blocker in Severe (left) andModerate (right) Heart Failure
Zannad et al,
N Engl J Med 364 (2011): 11-21
Page 21
Vardeny et al, Circ Heart Fail 7 (2014): 573-579
Page 22
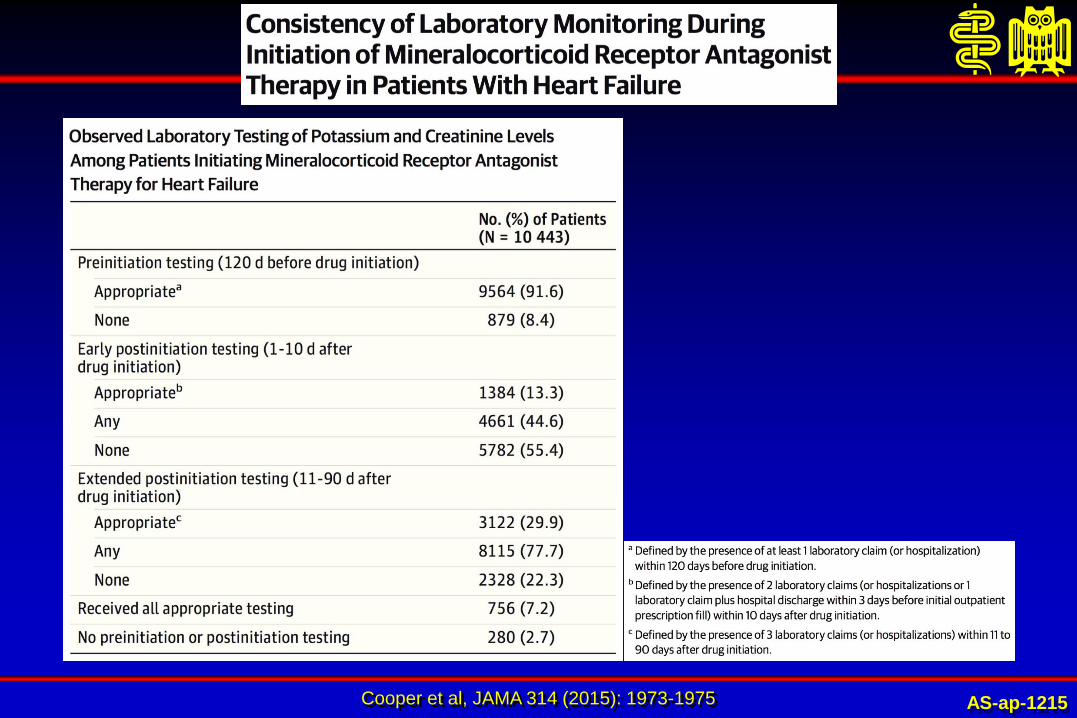
Cooper et al, JAMA 314 (2015): 1973-1975 AS-ap-1215
Page 23
AS-ah-0804Juurlink et al, N Engl J Med 351 (2004): 543-551
Hospitalizations due to Hyperkalemia after RALES
0.0
0.5
1994 1995 1996 1997 1998 1999 2000 2001
Study Year
Rate
of
In-H
osp
ital D
eath
fro
m H
yp
erk
ale
mia
(pe
r 1000 p
ati
en
ts)
Online release
of RALES
1.0
1.5
2.0
2.5
Page 24
Vardeny et al, Circ Heart Fail 7 (2014): 573-579
Page 25
Vardeny et al, Circ Heart Fail 7 (2014): 573-579
Page 26
Pitt & Bakris, Hypertension 66 (2015): 731-738
Structure of ZS-9. Pore detail with potassium ion (A), sodium ion (B), and calcium ion
(C). Blue spheres indicates oxygen atoms; green spheres, silicon atoms; and red
spheres, zirconium atoms.
Reprinted from Stavros et al, PLoS One 9 (2014) e114686 with permission of the
publisher. Copyright © 2014, the Authors.
AS-aa4-1015
Page 27
Kosiborod et al, JAMA (2014): [doi: 10.1001/JAMA.2014.15688]
Page 28
Weir et al, N Engl J Med 372 (2015): 211-221
Time to First Recurrence of Hyperkalemia during the Randomized Withdrawal Phase
AS-aw3-0415
Page 29
What do we need?
- Randomised, prospektive Study
- GFR 15-45 ml/min
- Spironolactone plus Patiromir vs Standardtherapie
- planned
Page 31
COR LOE Recommendations
I ARNI: B-RIn patients with chronic symptomatic HFrEF NYHA class II or III who tolerate an ACE inhibitor or ARB,
replacement by an ARNI is recommended to further reduce morbidity and mortality (19).
See Online
Data Supplements
1 and 18.
Recommendations for Renin-Angiotensin System
Inhibition With ACE Inhibitor or ARB or ARNI
Yancy et al, Circulation 134 (2016) AS-bi6-0516
Page 32
Regulation of Natriuretic Peptides, Bradykinin and Angiotensin II
Kidney
Blood vessels
Heart
Angiotensin II
Inactive products
Inactive products
Angiotensin I
Bradykinin
Natriuretic peptides
(ANP, BNP, CNP)
ACE
NEP
Cardioprotection
Vasodilation
Sodium
excretion
Hypertrophy
Vasoconstriction
Sodium Retention
{
Page 33
Bayés-Genis et al, J Am Coll Cardiol 65 (2015): 657-665 AS-ag4-0415
Page 34
Bayés-Genis et al, J Am Coll Cardiol 65 (2015): 657-665 AS-ag5-0415
Page 35
Bayés-Genis et al, J Am Coll Cardiol 65 (2015): 657-665 AS-ag2-0415
Page 36
Bayés-Genis et al, J Am Coll Cardiol 65 (2015): 657-665 AS-ag6-0415
Page 37
Concept of ARNIs : Pharmacologic Actions
Kidney
Blood vessels
Heart
Angiotensin II
Inactive products
Inactive products
Angiotensin I
Bradykinin
Natriuretic peptides
(ANP, BNP, CNP)
ACE Inhibition
NEP Inhibition
Cardioprotection
Vasodilation
Sodium
excretion
Hypertrophy
Vasoconstriction
Sodium Retention
{
Page 38
LCZ696 comprises the anionic
forms of sacubitril and valsartan,
sodium cations and water2
Its smallest crystal structure unit
consists of:2
• 6 sacubitril and 6 valsartan
molecules in anionic form
• 18 sodium cations
• 15 water molecules
• LCZ696 is available in three doses:3– 50 mg (24 mg sacubitril / 26 mg valsartan)
– 100 mg (49 mg sacubitril / 51 mg valsartan)
– 200 mg (97 mg sacubitril / 103 mg valsartan)
2D LCZ696 structure1
6
Sacubitril Valsartan
LCZ696 is a salt complex
H2O=water; Na=sodium
1. Novartis Data on File: LCZ696 Investigator’s Brochure Edition 16, 25 March 2015;
2. Feng et al. Tetrahedron Lett 2012;53:275–6;3. Highlights of prescribing information (ENTRESTO);
http://www.pharma.us.novartis.com/product/pi/pdf/entresto.pdf Accessed 21 August 2015
AS-ab7-0116
1. Novartis Data on File: LCZ696 Investigator’s Brochure Edition 16, 25 March 2015;
2. Feng et al. Tetrahedron Lett 2012;53:275–6;3. Highlights of prescribing information (ENTRESTO); http://www.pharma.us.novartis.com/product/pi/pdf/entresto.pdf Accessed 21 August 2015
Page 39
At risk
Enalapril: 4212 3883 3579 2922 2123 1488 853 236
Cu
mu
lati
ve
Pro
po
rtio
n o
f P
ati
en
ts
wit
h P
rim
ary
En
d P
oin
t (%
)
Days after Randomization
0
10
20
30
40
0 180 360 540 720 900 1080 1260
HR: 0.80 (0.73, 0.87)
p < 0.001 1117Enalapril
(n=4212)
LCZ696
(n=4187)
914
PARADIGM-HF: Primary outcomeProspective comparison of ARNI with ACEI to Determine Impact on Global Mortality and morbidity in Heart Failure trial
LCZ696: 4187 3922 3663 3018 2257 1544 896 249
Page 40
Death from CV causes20% risk reduction
HF hospitalization21% risk reduction
693
558
658
537
McMurray, Packer et al NEJM 2014
P = 0.00004 P = 0.00004
PARADIGM-HFProspective comparison of ARNI with ACEI to Determine Impact on
Global Mortality and morbidity in Heart Failure trial
Page 41
Death from CV causes20% risk reduction
HF hospitalization21% risk reduction
693
558
658
537
McMurray, Packer et al NEJM 2014
P = 0.00004 P = 0.00004
PARADIGM-HFProspective comparison of ARNI with ACEI to Determine Impact on
Global Mortality and morbidity in Heart Failure trial
Page 42
Simpson et al., JACC 66: 2059-71, 2015
Page 43
Cardiomyocyte
Blood
What to do with Markers:NT pro BNP and BNP
Page 44
0 2 4 6 8
0
100
200
300
400
500
600
700
800
900
1000
1100
1200
1300
1400
0
50
100
150
200
250
300
350
400
450
500
NT
-pro
BN
P p
g/m
l
Months
BN
P p
g/m
l
LCZ696
Enalapril
NT-proBNP
BNP
PARADIGM-HF: NT-proBNP and BNP
Packer et al, Circulation (2014): [doi:10.1161/CIRCULATIONAHA.114.013748]
Page 45
Pro BNP/
NT proBNP
Pre- Post- Pre- Post-
BNP
Hemmung
des BNP
Abbaues
Reduzierte
Wandspannung
LCZ696 LCZ696
NT pro BNP and BNP Änderungenwith LCZ696 (schematisch)
Packer et al, Circulation (2014): [doi:10.1161/CIRCULATIONAHA.114.013748]
Page 46
How to Switch from an ACE
Inhibitor?
Angioedema?
Page 47
LCZ696 actively inhibits Neprilysin and the AT1 receptor, thus
enabling alternative degradation pathways for bradykinin
Active
bradykinin
Inactive
bradykinin
ACE APP NEP DPP-4
Bradykinin breakdown
Omapatrilat inhibits ACE, APP and NEP2
LCZ696 inhibitsonly NEP1,4,5
Active
bradykinin
Inactive
bradykinin
Bradykinin is a substrate of Neprilysin and other vasopeptidases (ACE,
APP, DPP-4) – its elevation has been associated with cough and
angioedema2,3
Omapatrilat inhibits three enzymes (ACE, APP, NEP) involved in the
breakdown of bradykinin, which is likely to be responsible for the
development of angioedema2
Page 48
LCZ696 actively inhibits Neprilysin and the AT1 receptor, thus
enabling alternative degradation pathways for bradykinin
Active
bradykinin
Inactive
bradykinin
ACE APP NEP DPP-4
Bradykinin breakdown
Omapatrilat inhibits ACE, APP and NEP2
LCZ696 inhibitsonly NEP1,4,5
Active
bradykinin
Inactive
bradykinin
Bradykinin is a substrate of Neprilysin and other vasopeptidases (ACE,
APP, DPP-4) – its elevation has been associated with cough and
angioedema2,3
Omapatrilat inhibits three enzymes (ACE, APP, NEP) involved in the
breakdown of bradykinin, which is likely to be responsible for the
development of angioedema2
Take Care of Wash Out, ie at least 36 hours!
Page 49
OMAPATRILAT
Natriureticpeptides Bradykinin
Angiotensin I
Angiotensin II
NEP ACE
ACE-NEP Inhibition: Omapatrilat
AS-cs8-0409
Page 50
AS-bb-0511
Quincke-Ödem
Page 51
What do we need?
- PARAGON: LCZ in HFPEF
- Single application
- Resistent hypertension. Impaired renal function
Page 52
McMurray JJV | Session 412-08
McMurray et al. NEJM 2016: http://www.nejm.org/doi/pdf/10.1056/NEJMoa1514859
In reducing the risk of the primary composite outcome of
cardiovascular death or heart failure hospitalization …
• Aliskiren added to enalapril is superior to enalapril
• Aliskiren monotherapy is superior to enalapril
• Aliskiren monotherapy is non-inferior to enalapril
Superiority
hyptheses
Non-inferiority
hyptheses
Primary outcome: CV death or heart failure hospitalization(event driven: target 2318 patients, 2369 occurred)
Enalapril 5-10mg bid* (N=2336)
Aliskiren 300mg qd# (N=2340)
Enalapril 5-10mg bid + Aliskiren 300mg qd (N=2340)
Enalapril
5-10mg bid
Aliskiren
300mg qd
Open-label run-in
4-12 weeks
Double-blind
median FU 36.6 months
Prior ACEi use dicontinued
*89% 10 mg#target dose (titrated from 150mg qd)
R
ATMOSPHERE
Methods
AS-ap48-0416
Page 53
McMurray JJV | Session 412-08
McMurray et al. NEJM 2016: http://www.nejm.org/doi/pdf/10.1056/NEJMoa1514859
Cu
mu
lati
ve
eve
nt
rate
(%
of
pa
tie
nts
)
0 360 1800
Primary composite endpoint
Combination vs. enalaprilHR 0.93 (95% CI 0.85-1.03), P=0.17
Aliskiren vs. enalaprilHR 0.99 (95% CI 0.90-1.10), P=0.91
Days since Randomization
720 1080 1440
0 360 1800720 1080 1440 0 360 1800720 1080 1440
0 360 1800720 1080 1440
100
90
80
70
60
50
40
30
20
10
0
100
90
80
70
60
50
40
30
20
10
0
100
90
80
70
60
50
40
30
20
10
0
100
90
80
70
60
50
40
30
20
10
0
Cu
mu
lati
ve
eve
nt
rate
(%
of
pa
tie
nts
)
Cu
mu
lati
ve
eve
nt
rate
(%
of
pa
tie
nts
)C
um
ula
tive
eve
nt
rate
(%
of
pa
tie
nts
)
Combination vs. enalaprilHR 0.93 (95% CI 0.82-1.05), P=0.23
Aliskiren vs. enalaprilHR 1.06 (95% CI, 0.94–1.19) P=0.34
Days since Randomization
Death from CV causes
Death from any cause
Combination vs. enalaprilHR 0.91 (95% CI 0.82-1.02), P=0.12
Aliskiren vs. enalapril
HR 1.04 (95% CI 0.93-1.16), P=0.46
Days since Randomization
First heart failure–related hospitalization
Combination vs. enalaprilHR 0.93 (95% CI 0.82-1.06), P=0.29
Aliskiren vs. enalaprilHR 0.99 (95% CI 0.87-1.13), P=0.91
Days since Randomization
Combination
Aliskiren
Enalapril
Combination
Aliskiren
Enalapril
Combination
Aliskiren
Enalapril
Combination
Aliskiren
Enalapril
ATMOSPHERE
Results – superiority hypothesis
AS-ap50-0416
Page 56
Cleland et al, Eur Heart J 34 (2013): 3547-3556 AS-al3-0616
Page 57
Cleland et al, Eur Heart J 34 (2013): 3547-3556 AS-al2-0616
Page 59
Baseline heart rate is a predictor of endpoints on placebo
Primary composite endpoint: risk increases by 2.9% per 1-bpm increase, and by 15.6% per 5-bpm increase
50
40
30
20
10
0
0 6 12 18 24 30Months
≥87 bpm
80 to <87 bpm
75 to <80 bpm
72 to <75 bpm
70 to <72 bpm
P<0.001
Patients with primary composite endpoint (%)
Böhm et al, Lancet 2010; 376: 886-894.
Stable CHF, SR > 70 bpm
Page 60
Ivabradine n=793 (14.5%PY) Placebo n=937 (17.7%PY)
HR = 0.82 p<0.0001
0 6 12 18 24 30
Months
40
30
20
10
0
Ivabradine
Placebo
- 18%
Cumulative frequency (%)
Primary composite endpoint
Swedberg et al, Lancet 376 (2010): 875-885
NNT=26 (annualized)
NYHA II-IV, SR > 70 bpm
Page 61
Endpoints Hazard ratio 95% CI p value
Primary composite endpoint 0.82 [0.75;0.90] p<0.0001
CV death 0.91 [0.80;1.03] p=0.128
Hospitalization for HF 0.74 [0.66;0.83] p<0.0001
All-cause death 0.90 [0.80;1.02] p=0.092
Death from HF 0.74 [0.58;0.94] p=0.014
Hospitalization for any cause 0.89 [0.82;0.96] p=0.003
Hospitalization for CV reason 0.85 [0.78;0.92] p=0.0002
Effect of ivabradine on outcomes
Swedberg et al. Lancet 2010; 376: 875-885.
Page 62
Primary composite endpoint according to heart rate achieved at D28* in the ivabradine group
≥75 bpm
70-<75 bpm
60-<65 bpm
65-<70 bpm
<60 bpm
Patients with
primary
endpoint (%)
Months0 6 12 18 24 30Day 28
50
40
30
20
10
0
Böhm et al, Lancet 2010; 376: 886-894.
Achiewed Heart Rate at Day 28
Relevance
Page 63
Comorbidities in Chronic Heart Failure
Dickstein et al, Eur Heart J 29 (2008): 2388-2442
Detect Co-morbidities and
Precipitating Factors
Non-cardiovascular
Anaemia
Pulmonary disease
Renal dysfunction
Thyroid dysfunction
Diabetes
Cardiovascular
Ischemia / CAD
Hypertension
Valvular dysfunction
Diastolic dysfunction
Atrial fibrillation
Ventricular dysrhythmias
Bradycardia
Diabetes
Page 64
Silverman M, Turner RJ. In: Windhager EE, ed. Handbook of Physiology, Vol. II. New York, NY: Oxford University Press; 1992:2017-2038.
0
200
400
600
0 200 400 600 800
Plasmaglukose (mg/dL)
Glu
ko
se
(m
g/m
in)
11070
Normale
Plasma-
glukose
Fast die gesamte filtrierte Glukose wird
beim Gesunden reabsorbiert
Page 65
Bei normaler Plasmaglukose (70-110 mg/dL), wird Glukose fast komplett reab-sorbiert
Bei hoher Plasma-glukose, wie bei Diabetes, wird Glukose weiter tubulär reabsor-biert
Tubuläre Reab-sorption unterhält Hyperglykämie
Wenn TmG über-schritten wird (~180–200 mg/dL), kommt es zur Glukosurie
Silverman M, Turner RJ. In: Windhager EE, ed. Handbook of Physiology, Vol. II. New York, NY: Oxford University Press; 1992:2017-2038.
0
200
400
600
0 200 400 600 800
Plasmaglukose (mg/dL)
Tubuläre
Reabsorption
TmGGlu
ko
se
(m
g/m
in)
11070
Normale
Plasma-
glukoseUrin
Glukose
Schwelle
kaum
Glukose
im Urin
Glukose im
Urin
Erhöhte Plasmaglukose
Fast die gesamte filtrierte Glukose wird
beim Gesunden reabsorbiert
Page 66
Distales S3 Segment des
proximalen Tubulus
~10% Glukose reabsorbiert
Transport durch SGLT1
S1 Segment des proximalen
Tubulus
~90% Glukose reabsorbiert
Transport durch SGLT2
Keine Glukoseim Filtrat
Sammelrohr
Glomerulus filtriert
Proximaler Tubulus reabsorbiert
Silverman M, Turner RJ. In: Windhager EE, ed. Handbook of Physiology, Vol. II. New York, NY: Oxford University Press; 1992:2017-2038.
Bakris GL, et al. Kidney Int. 2009;75:1272-1277.
Glukose
Glukose- Reabsorption findet im
proximalen Tubulus statt
SGLT: sodium glucose transporter
Page 67
EMPA-REG OUTCOME®: Trial design
67
• Study medication was given in addition to standard of care
• The trial was to continue until at least 691 patients experienced an
adjudicated primary outcome event
• 97.0% of patients completed the study and final vital status was available for
99.2% of patients
Randomized and
treated
(n=7020)
Empagliflozin 10 mg
(n=2345)
Empagliflozin 25 mg
(n=2342)
Placebo
(n=2333)
Screening
(n=11531)
Zinman B et al. N Engl J Med 2015 DOI: 10.1056/NEJMoa1504720.
Page 68
Zinman et al., New Engl J Med (2015): [doi:10.1056/NEJMoa1504720]
Page 69
Zinman et al., New Engl J Med (2015): [doi:10.1056/NEJMoa1504720]
Page 70
Patients
hospitalized
for
heart failure
(%)
HR 0.75
(95% CI 0.48, 1.19)
HR 0.59
(95% CI 0.43, 0.82)
Cox regression analysis.
HR, hazard ratio; CI, confidence interval.
Hospitalization for heart failure
in patients with vs without heart failure at baseline
Zinman et al, N Engl J Med (Suppl.) [doi: 10.1056/NEJMoa1504720]
Page 74
AS-bn-0709Home et al, Lancet 373 (2009): 2125-2135
Page 76
Leitlinien Sind lesenswert!
… sollten nur auch gelesen werden!
Guide-
lines
Page 77
M. Böhm
Klinik für Innere Medizin III
Universitätsklinikum des Saarlandes
Homburg/Saar, Germany
Tel. 06841-16-23372
Fax. 06841-16-23369
[email protected]
Thank you
for your attention!