BOARD OF DIRECTORS (Meeting held in Public) Monday 26 July 2021; 1300 –1410 Meeting to be held via Microsoft Teams AGENDA – PART 1 Please Note: During the COVID-19 pandemic, Board of Directors meeting agendas have been streamlined where possible to enable focus on the Trust’s incident response and recovery planning and other business critical issues. Items for discussion at Board of Directors meetings are highlighted in blue. All other items will not normally be discussed in detail, particularly those considered in advance by Board committees. Board members have the opportunity to raise questions with the relevant Director lead outside of the meeting with responses shared with all Board members and incorporated into meeting minutes as appropriate. ITEM FORMAT ACTION PRESENTED BY TIME 01 Welcome and Introductions Verbal To Note Rupert Nichols, Chair 1300 (15mins) 02 Apologies for Absence Verbal To Note Rupert Nichols, Chair 03 Declarations of Interest Verbal To Note All 04 Minutes of the Previous Meeting of the Board of Directors held 28 June 2021 Paper To Approve Rupert Nichols, Chair 05 Matters Arising and Action Log Verbal To Note Rupert Nichols, Chair 06 Chair’s Report Verbal To Note Rupert Nichols, Chair 07 Chief Executive’s Brief - July 2021 Paper To Discuss Neil Thwaite, Chief Executive QUALITY AND GOVERNANCE 08 COVID-19 and Recovery Briefing - Oversight Report (July 2021) Paper To Discuss Gill Green, Executive Director of Nursing and Governance and Deborah Partington, Director of Operations 1315 (10mins) OPERATIONAL PERFORMANCE 09 Board Performance Report (June 2021) Paper To Discuss Liz Calder, Director of Performance and Strategic Development 1325 (10mins) STRATEGY AND POLICY 10 Strategy – Progress Report Paper To Note Liz Calder, Director of Performance and Strategic Development 1335 (15mins)
Transcript
BOARD OF DIRECTORS (Meeting held in Public) Monday 26 July 2021; 1300 –1410 Meeting to be held via Microsoft Teams
AGENDA – PART 1
Please Note: During the COVID-19 pandemic, Board of Directors meeting agendas have been streamlined where possible to enable focus on the Trust’s incident response and recovery planning and other business critical issues. Items for discussion at Board of Directors meetings are highlighted in blue. All other items will not normally be discussed in detail, particularly those considered in advance by Board committees. Board members have the opportunity to raise questions with the relevant Director lead outside of the meeting with responses shared with all Board members and incorporated into meeting minutes as appropriate.
ITEM FORMAT ACTION PRESENTED BY TIME
01 Welcome and Introductions Verbal To Note Rupert Nichols, Chair 1300 (15mins) 02 Apologies for Absence Verbal To Note Rupert Nichols, Chair
03 Declarations of Interest
Verbal To Note All
04 Minutes of the Previous Meeting of the Board of Directors held 28 June 2021
Paper To Approve Rupert Nichols, Chair
05 Matters Arising and Action Log Verbal To Note Rupert Nichols, Chair
06 Chair’s Report Verbal To Note Rupert Nichols, Chair
07 Chief Executive’s Brief - July 2021 Paper
To Discuss Neil Thwaite, Chief Executive
QUALITY AND GOVERNANCE 08 COVID-19 and Recovery Briefing -
Oversight Report (July 2021) Paper To Discuss Gill Green, Executive Director
of Nursing and Governance and Deborah Partington, Director of Operations
1315 (10mins)
OPERATIONAL PERFORMANCE 09 Board Performance Report (June 2021) Paper To Discuss Liz Calder, Director of
Performance and Strategic Development
1325 (10mins)
STRATEGY AND POLICY 10 Strategy – Progress Report Paper To Note Liz Calder, Director of
11.01 – Minutes of the Meeting held on 10 June 2021 (Ratified) 11.02 – Committee Chair’s Assurance Report on the Meeting held 8 July 2021
Paper
To Note
Julie Jarman, Non-Executive Director and Chair
1350 (20mins)
12 Equality Diversity and Inclusion: 12.01 – Minutes of the Meeting held on 14 June 2021 (Ratified) 12.02 - Committee’s Chairs Assurance Report from the meeting held on 15 July 2021
Paper To Note Anthony Bell, Non-Executive Director and Chair
13 Charitable Funds Committee 13.01 – Minutes of meeting held 24 March 2021 (Ratified) 13.02 – Chair’s Report of the meeting held 5 July 2021 13.03 – Terms of Reference
Paper To Note Anthony Bell, Non-Executive Director and Chair
14 Audit Committee 14.01 – Minutes of meeting held on 8 June 2021 (Ratified) 14.02 – Committee’s Chairs Assurance Report from the meeting held on 5 July 2021
Paper Paper
To Note To Note
Andrea Harrison, Non-Executive Director and Chair
ANY OTHER BUSINESS 15 Any Other Business Verbal To Note All 1410
Meeting Ends Questions from the Public – Questions submitted in advance of the meeting to the Chair may be considered from public attendees
DATE AND TIME OF NEXT MEETING The next Board of Directors’ Meeting in public will take place on Monday 27 September 2021 at 1300. As it currently stands, the meeting will be held remotely via Microsoft Teams.
RESOLUTION The Board is invited to adopt the following - ‘That representatives of the press and other members of the public be excluded from the remainder of this meeting, having regard to the confidential nature of the business to be transacted’
1
Board of Directors – Part 1
TITLE OF REPORT: Minutes of the Previous Meeting of the Board of Directors held 28 June 2021
DATE OF MEETING: Monday 26 July 2021
AGENDA ITEM: 04
PRESENTED BY: Rupert Nichols, Chair
AUTHOR(S): Colin Reid, Interim Company Secretary
REPORT SUMMARY: The following report is a record of the Board of Directors meeting held in public on
Monday 28 June 2021.
THIS REPORT SUPPORTS ACHIEVEMENT OF THE FOLLOWING STRATEGIC OBJECTIVES:
Objective 1 – Work with service users and carers to achieve their goals by delivering high quality care x
Objective 2 – Create an outstanding place to work, ensuring staff feel valued and are supported to
reach their potential
x
Objective 3 – Continuously improve services for users through research, innovation and digital
technology
x
Objective 4 – Work in partnership with others to improve wellbeing and challenge stigma x
Objective 5 – Be a sustainable, well-led organisation that delivers social value x
REPORT CONSIDERED AT THE FOLLOWING COMMITTEES/SUB-GROUPS:
Committee/Sub-Group: Date:
Audit Committee -
Quality Improvement Committee -
Charitable Funds Committee -
Remuneration & Terms of Service Committee -
Council of Governors -
Executive Management Team -
LEGAL IMPLICATIONS: None identified
REGULATORY
IMPLICATIONS (CQC/NHSEI):
None identified
2
THIS REPORT PROVIDES ASSURANCE AGAINST A RISK ON THE BOARD ASSURANCE FRAMEWORK (BAF):
No
If ‘yes’:
RISK ID Strategic Objective Description (as per BAF)
PURPOSE OF REPORT – Please tick all relevant boxes
Information
Assurance x Approval/Decision x
RECOMMENDATIONS: The Board of Directors are asked to review and approve the minutes of the meeting
held on Monday 28 June 2021.
1
IN PUBLIC BOARD OF DIRECTORS MEETING – MONDAY 28 JUNE 2021 AT 1.00PM VIA
MICROSOFT TEAMS
PRESENT:
Board of Directors:
Rupert Nichols - Chair
Anthony Bell - Non-Executive Director
Liz Calder - Director of Performance and Strategic Development
Helen Dabbs - Non-Executive Director
Stephen Dalton - Non-Executive Director
Gill Green - Director of Nursing & Governance
Andrea Harrison - Non-Executive Director
Julie Jarman - Non-Executive Director
Pauleen Lane - Non-Executive Director
Andrew Maloney - Director of HR and Deputy CEO
Suzanne Robinson - Director of Finance and IM&T
Alice Seabourne - Medical Director
Neil Thwaite - Chief Executive
IN ATTENDANCE:
Colin Reid - Interim Company Secretary
OBSERVERS:
Maureen Burke - GMMH Governor
Avril Clarke - GMMH Governor
Dan Stears - GMMH Governor
Avril Allen - NHS Professionals
No. Item Action
130/21 Welcome and Introductions
The Chair welcomed members of the Board and observers to the meeting of the Board
of Directors held in public.
131/21 Apologies for Absence
There were no apologies.
132/21 Declarations of Interest
There were no declarations of interest in agenda items.
2
No. Item Action
133/21 Minutes of the Previous Meeting of the Board of Directors held 24 May 2021
The minutes of the meeting held on Monday 24 May 2021 were approved as a correct
record of the meeting, subject to the following amendment:
Paragraph 111/21, final sentence – remove “with the exception of the 4hr A&E
target.” and replace with “, noting that the information about the 4hr A&E
performance was in development.”
134/21 Matters Arising and Action Log
The Board reviewed and noted the Action Log.
135/21 Chair’s Report
The Chair commented on the appointment of the new Secretary of State for Health and
Social Care, Sajid Javid MP and the impending retirement of Sir Simon Stevens as Chief
Executive of NHS England in July 2021. He commented on the complex changes that
were required following the publication of the white paper whilst recovering from the
COVID-19 Pandemic and the pressures on the Executive Team and Trust Staff in
continuing to deliver the services in the mists of addressing the structural changes.
The Chair advised that subject to the lifting of the current COVID-19 Restrictions he
hoped that the next Board meeting would be held in person rather than through Teams.
136/21 Chief Executive’s Brief – June 2021
The Chief Executive shared the key headlines from his Chief Executive Brief with regards to: (i) Veterans Award: The Trust was delighted to have been named a Veteran Aware
Trust in recognition of its commitment to improving NHS care for veterans, reservists, members of the armed forces and their families.
(ii) GM ICS: Work continued across GM on establishing Integrated Care Systems (ICS) by April 2022 and transferring commissioning duties to them in line with the White Paper.
(iii) Health and Justice Tender: The Trust was putting together a tender to bid for the health and social care services, mental health services and secure children’s homes, the contract would be for 6 years, starting in April 2022 with the option to extend for an additional 3 years. The Chief Executive commented on the work being done by the Team to put the bids together.
(iv) New Park House Development: The Full Business Case was planned to be submitted following Board approval at the July 2021 Board meeting.
(v) Volunteers Week: Volunteers’ Week took place in June to recognise and thank volunteers. During an exceptionally difficult year, people from all walks of life around the UK have taken the time to volunteer and made a huge difference to people and their communities – just as they do every year. As a thank you and a chance to celebrate the work our volunteers do the Trust hosted its Annual Volunteer Celebration and Learning Event via Microsoft Teams on 22 June 2021. The Chief Executive, on behalf of the Board thanked all volunteers for their continued help and support to the Trust.
The Board noted the Chief Executive’s Brief for June 2021.
3
137/21 COVID-19 Briefing – Oversight Report (June 2021) The Director of Nursing and Governance, and the Director of Operations presented a briefing paper outlining the Trust’s response to the Covid-19 pandemic and the work of Gold Command and the Recovery Planning Group. Director of Nursing and Governance advised on the following matters: (i) Delta variant: Gold Command had continued to be alerted over the new Delta
variant, which was prominent in the North West and particularly in Greater Manchester.
(ii) Bolton Inpatient Visiting: In recognition of the Delta variant being very strong in Bolton, Gold Command had suspended visiting of inpatients at its Bolton Unit at Rivington, Honeysuckle Lodge and Woodlands in line with restrictions being put in place by Bolton NHS Foundation Trust. Any relaxation of restrictions would be taken in consultation with Bolton NHS Foundation Trust.
(iii) Bolton Staff: Guidance for staff living and working in Bolton on the latest status regarding vaccines and local advice had taken place with enhanced testing, vaccinations and lateral flow testing for staff working and living in Bolton.
(iv) Patient Vaccinations: On the 15th June it was confirmed that the Pfizer vaccination would be available to service users under the age of 40 at a number of Trust sites. A plan had been developed to deliver Pfizer vaccinations to Trust service users under 40 which commenced on 21st June 2021.
The Director of Operations provided an update on the work of the COVID-19 Recovery Planning Group. She advised that the Recovery Planning Group continued to co-ordinate the Trusts COVID-19 Recovery Plan and oversee the work of the Recovery Workstreams and Task and Finish Groups and highlighted the work being done in ROC, patient flow over a 7-day period, Manchester Safeguarding, Research and Innovation, CBU Waiting Lists and CAMHS. Anthony Bell, referring to the recent Windrush Celebration thanked the Director of Nursing and Governance for her attendance and contribution which was well received. He advised that throughout the day the need for individuals to be COVID-19 vaccinated was reinforced to those attending the event with particular emphasis on the promotion of the National Vaccination Programme. Anthony Bell referring to the benchmarking data that showed Trust BAME staff vaccination uptake falling behind other similar organisations in the North West asked whether there were any leanings that the Trust could take from those organisations. In response the Director of Nursing and Governance advised that in discussions with Manchester University NHS Foundation Trust (MFT) there was a suggestion that the Trust do more to promote the vaccination programme through MFT’s BAME leaders. The Director of Nursing and Governance agreed to discuss further with Anthony Bell how he could help support this initiative. With regards to a question on the Trust’s relationship with Care and Residential Homes, the Director of Nursing and Governance reported that at the beginning of the pandemic the relationship was not as it should have been particularly with regards to discharge. She advised that this did improve over the period following the outbreak. The Director of Nursing and Governance advised that the Trust continued to have very good professional relationship with Care and Residential Homes, particularly the specialist homes. The Director of Operations explained that before the pandemic, the Trust had in place care home liaison teams that supported a number of care homes but not all. For those where a liaison team were in place the relationship was good however not so for those where a liaison team was not in place. The Director of Operations advised that since the start of the pandemic relationships had improved particularly in relation to
4
discharge which saw a refining of processes to provide testing at the time of discharge and referred to the actions taken at Manchester and Trafford which saw the first testing service for discharging service users in the region. The Board noted the comprehensive work which had been undertaken by the Trust in response to the COVID-19 pandemic; the recovery planning work; and the priorities going forward.
138/21 GMMH Quality Account 2020/21 Final First Draft The Director of Nursing and Governance presented the Trust Quality Account 2020/21 for approval and reported that it had been reviewed at Quality Improvement Committee on 10 June 2021 with no suggested changes from the discussion. The Director of Nursing and Governance advised that this was the second year where the requirement for the Quality Account to be externally audited had been removed by NHSE/I. Referring to the responses from stakeholders, the Director of Nursing and Governance advised that the Trust had received some excellent and very positive feedback which was noted by the Board. The Director of Nursing and Governance referenced the Dragon’s Den programme which was due to be launched on 5th July 2021. The Trust’s communications team was currently developing materials which would be released across social media and in upcoming staff bulletins ahead of a communications campaign in the lead up to the launch. The Board approved the 2020/21 Quality Account for publication on the Trust’s website and NHS Choices, and thanked the Governance Team for their work in its production.
139/21 Mental Health Act (MHA) Annual Report: 1 January 2020 to 31 March 2021 The Medical Director presented the Trust Mental Health Annual report for 15months to 31 March 20211 for approval and reported that it had been reviewed at Quality Improvement Committee on 10 June 2021. The Medical Director advised that the extended report covers the unprecedented period following the onset of the COVID-19 pandemic and provides a summary of the Trust’s performance in relation to the MHA 1983 (as amended 2007) from 1 January 2020 to 31 March 2021, noting that future reports would be aligned to the financial, rather than calendar year. The Medical Director highlighted the key areas in the Report. Pauline lane referring to the section on Children and Young People was concerned that 16-18 year olds had been admitted to general adult wards and asked why this was the case. In response the Medical Director reported on the pressures in the system which had resulted in CAMHS beds not being free and explained that where this was the case 16-18 year olds would be admitted to an adult ward. The Director of Operations commented on the availability of CAMHS beds and reported that the usage fluctuated. The Director of Operations assured the Board that every step was taken to identify available CAMHS bed however if one was not available then 16-18 year olds would be placed in an adult ward. She advised that they would not remain on the adult ward for long and processes were in place to make sure they were moved to an appropriate CAMHS bed as soon as one was available. Whilst on an adult ward appropriate safeguarding arrangement were put in place to protect the Service user.
5
Julie Jarman commented on an action that came out of discussions at the QIC meeting relating to the “use of 136 suites” and explained that of all assessments made 63% resulted in discharge. The QIC were looking into whether there was any quality improvement work that could be done to reduce the number of service users being referred to the 136 suites earlier in the process, which would include the support of the police. Anthony Bell referred to the e-training packages and asked whether there was an improving picture in terms of compliance, and how does take up of the e-leaning compare regionally and nationally. It was noted that the data quoted in the Report was for internal training and which would be difficult to benchmark against national data as it was bespoke to the Trust. The Medical Director advised that she would check the position regarding the trajectory from last year and would advise Anthony Bell outside of the meeting. It was agreed that future reports would include comparable data from the previous year in relation to e-training packages and following further discussion on mental health tribunals to include, where information was available, benchmarking in relation to the number of tribunals and how many led to detention. The Board noted that the QIC would continue to review and receive assurance that actions arising out of the Report were being addressed. The Board approved the Mental Health Act 15-month Annual Report - 1 January 2020 to 31 March 2021.
140/21 Medical Revalidation and Appraisal Annual Report 2020/21 The Medical Director presented the Medical Revalidation and Appraisal Annual Report 2020/21 which sets out the key themes within the Trust’s Medical Appraisal Programme in order to provide evidence of the Trust’s compliance with national obligations. The Medical Director advised that the Report had been reviewed and received at Quality Improvement Committee on 10 June 2021. In response to a question on whether external assurance was obtained on the appraisal programme, the Board heard that assurance was provided via a peer review, the last one being undertaken in 2019. Consideration would be given to whether additional assurance was required from internal audit. The Board following review of the Medical Revalidation and Appraisal Annual Report 2020/21 received assurance that the Trust was compliant with The Medical Profession (Responsible Officers) regulations 2010 (amended 2013) and authorised the Chief Executive or Chair to sign of the Statement of Compliance at Appendix 1.
141/21 Research and Innovation Strategy 2021-2024 The Medical Director presented the Research and Innovation Strategy reminding the Board that the draft was discussed at a Board Development Session on 24th May 2021 and that the Strategy had been revised in line with feedback from that session. It was further noted that the Executive Management Team and Strategy Development Group had also reviewed the Strategy and was now presented to the Board for approval. Stephen Dalton commented that it was great to see that the Strategy focused on the contribution from the people the Trust serves but also that it focused on the people the Trust serves. With regard recruitment of medical staff, Stephen Dalton asked wither any consideration was being given to include research in the job description. In response the Medical Director advised that research was an important part of a clinical
6
role and if Medical staff wish to be involved in research, sessions would be made available to support them. Andrea Harrison felt that the Strategy was light on quantitative ambitions and would have liked to see included a suite of metrics that implementation of the strategy could be measured against. The Medical Director agreed and advised that future reports to the Board would include a suite of metrics that would enable the Board to receive assurance on implementation of the Strategy. The Chief Executive advised that financial metrics would also be included and advised that the Director of Finance and IM&T was looking at metrics of this nature which would be taken through the Finance and Investment Committee in due course. Helen Dabbs asked how the Strategy would be shared externally given the ambition was really good. In response the Medical Director advised that the Strategy was aligned to Manchester University’s strategy and would be included in the BRC bid. The Board approved the Research and Innovation Strategy 2021-2024, noting the formal launch date during July 2021.
142/21 Freedom to Speak Up Bi-Annual Update The Director of HR and Deputy Chief Executive presented the Freedom to Speak Up Bi-Annual Update on behalf of Juliette Tait, Freedom to Speak Up Guardian who was unable to attend the meeting. The Director of HR and Deputy Chief Executive advised that there was a total of 71 concerns raised during 2020/21, each of which had been addressed by either the Guardian or her Deputy who had commenced in post enabling an increased level of developmental work to support the growing of a positive speaking up culture. The Board recognised the positive contribution of Senior Leaders who continued to provide supportive and responsive feedback to those who raised concerns via the Freedom to Speak Up Guardian. The development of front-line leaders continued to be the priority of the Guardian and Deputy Guardian recognising that many concerns raised were because staff felt they were not being heard within their local services. In response to a question on whether there was any benchmarking information that could be obtained for Mental Health Trusts, the Director of HR and Deputy Chief Executive undertook to ask the Guardian to provide this in future reporting if available. Anthony Bell commented on the score below benchmarking average to the national survey question: “My organisation treats staff who are involved in an error, near miss or incident fairly” and asked whether this should be looked at in more detail. Helen Dabbs supported the comment explaining that there was evidence based data relating to safety culture in terms of reporting under freedom to speak up and learning from near misses and suggested this was something the Trust should reflect on as to how this leads into the Trust’s patient safety strategy. The Board noted the Freedom to Speak Up Bi-Annual Update and the positive assurance on the implementation, approach, and additional investment in Freedom to Speak Up.
143/21 Disciplinary Practices – A review of the Trust’s processes to improve experience. The Director of HR and Deputy Chief Executive presented the paper which provides findings of a review of the Trust’s disciplinary processes in response to a letter from Baroness Dido Harding and includes internal findings as a result of the 2019 WRES.
7
The Board noted the findings from the Review which indicated that significant improvements were required, particularly when considering the WRES indicator relating to BAME staff likelihood of entering a disciplinary process in comparison to white staff. Improvements would be facilitated through training for case managers and chairs of disciplinary panels, training for managers in general which focusses on a “just and learning” approach to decision making and the introduction of a system to support the efficient and effective handling of casework. The Board noted Disciplinary Practices – A review of the Trust’s processes to improve experience and that tracking data would be provided quarterly through the Strategic EDI Working Group.
144/21 Board Performance Report (May 2021) The Director of Performance and Strategic Development presented the Trust Performance Report for the period ended 31 May 2021. She explained that this was the second Performance Report for 2021/22 financial year. The Director of Performance and Strategic Development advised that as with last month’s Report, the Report includes Wigan Mental Health Services data following the transfer on 1 April 2021 and referred the Board to the Executive Summary and ran through some notable areas of performance. Julie Jarman referred to the indicator relating to temporary staff which showed performance at 14% against a target of 5%. She recognised that this had been a stubborn indicator for some time and asked what was being done to address it. The Director of HR and Deputy Chief Executive advised that this had been considered at the meeting of the Finance and Investment Committee this month along similar lines to the concern raised. He advised that it was key that the Trust stand back and look at the key drivers that results in the position the Trust finds itself. The Board noted that the Finance and Investment Committee would continue to review the underlying data and report its findings. The Board noted the performance position for the year to date and the actions being taken where variance was highlighted.
143/21 Annual Operational Plan 2021/22
The Director of Performance and Strategic Development presented the final version of the Trusts Annual Operational Plan 2021/22 for approval and reported that a 6-monthly report on performance against the Plan would be provided at the November Board meeting.
The Board approved the Annual Operational Plan 2021/22.
144/21 Update following the North West Boroughs Healthcare NHS Foundation Trust (NWBH) Transaction The Board received the updated position following the transfer from NWBH and noted: (i) the completion of the legal requirements for the Commercial Transfer of NWBH
services to the Trust; (ii) the safe landing of transferring services and continued integration within the Trust; (iii) the post transition governance arrangements including programme management,
delivery and monitoring of PTIP and collaborative arrangements with Wigan Borough CCG to monitor the joint service delivery plan and compliance with quality requirements; and
(iv) the key remaining risks and mitigations.
8
The Chair congratulated everyone involved in the transaction noting it was undertaken during a very difficult period.
145/21 Quality Improvement Committee:
Julie Jarman, Chair of the Quality Improvement Committee, presented two items from
the Quality Improvement Committee:
(i) Minutes of the Meeting held on 13 May 2021
The minutes of the meeting held on 13 May 2021 were received and noted.
(ii) Chair’s Assurance Report on the Meeting held 10 June 2021
Julie Jarman, Chair of the Quality Improvement Committee (QIC) briefed the Board on
highlights from the meeting including:
(i) As discussed during the meeting, the Committee received a number of Annual
Reports for review prior to being presented to the Board meeting today. The Chair
of the QIC thanked all who had contributed to each annual report. She advised that
a number of actions came out of the Mental Health Annual Report which the
Committee would be reviewing.
(ii) The Committee had heard of concerns regarding CAMHS safe staffing and had
requested that any risks are logged in the local risk register for escalation through
the Trust. The Chair of the QIC advised that it was important that these processes
were followed so that the risks can be fully investigated and mitigated.
(iii) The Committee heard of the delays in inquests taking place due to the pandemic
and noted that the Trust had seen a surge in inquests and the consequential
increase in work the Trust staff had to do to support the Courts. It was noted that
this not only causes stress to families but also to staff.
The Chair’s Quality Improvement Committee assurance report was noted.
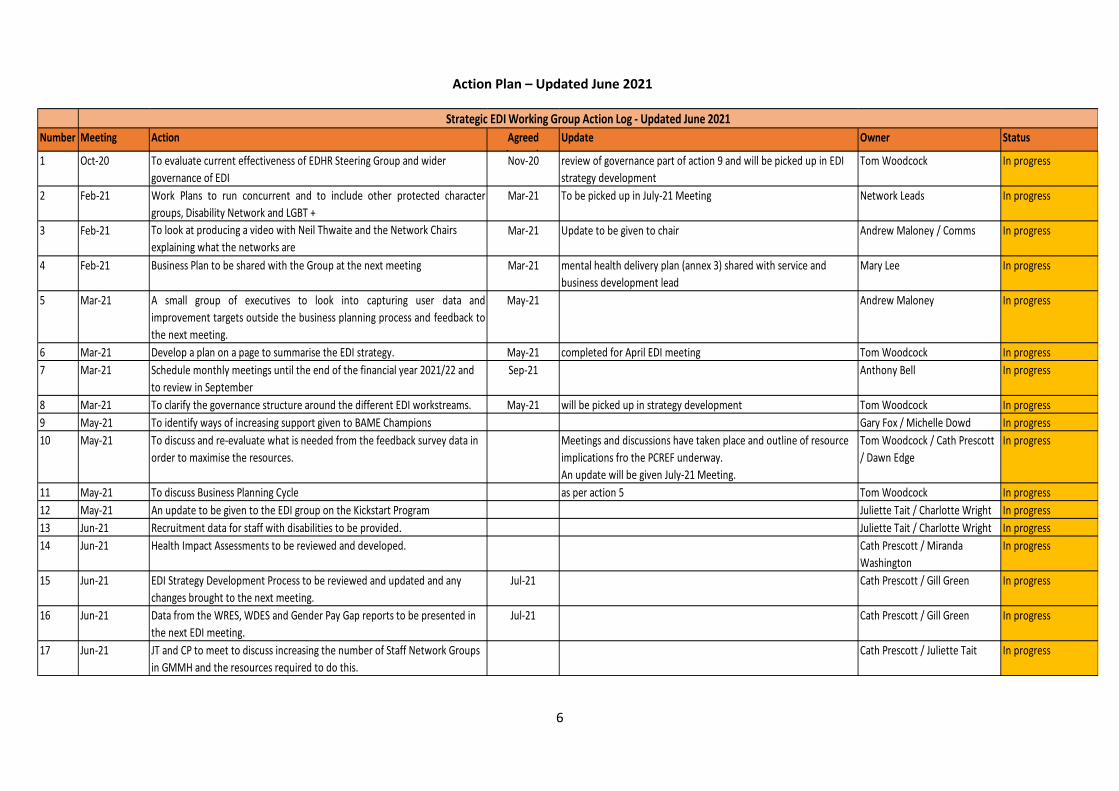
146/21 Strategic Equality, Diversity & Inclusion (EDI) Working Group:
(i) Minutes of the meeting held on 10 May 2021
The minutes of the meeting held on 10 May 2021 were received and noted.
(ii) Chair’s Assurance Report on the Meeting held 14 June 2021
Tony Bell, Chair of the Strategic Equality, Diversity and Inclusion (EDI) Working Group
briefed the Board on highlights from the meeting including:
(i) The group received a presentation on the development of the next organisational
EDI strategy and a draft timeline was scoped out which will have a refreshed
strategy for Board sign-off by March 2022.
(ii) The meeting received an update on the Patient and Carer Race Equality Framework
pilot and the engagement work currently in progress.
(iii) There was discussion about how to enable staff participation in networks given the
fact that many people are unable to engage during working hours. This issue
reduces the effectiveness and reach of the networks.
The chair of the Strategic EDI Working Group thanked Tom Woodcock for his help and
support, noting he had retired from the Trust.
The Chair’s Strategic EDI Working Group assurance report was noted.
9
147/21 Audit Committee:
Andrea Harrison, Chair of the Audit Committee, presented two items from the Audit
Committee:
(i) Minutes of the meeting held 26 April 2021
The minutes of the meeting held 26 April 2021 were received and noted.
(ii) Chair’s Report from the meeting held 8 June 2021
Andrea Harrison, Chair of the Audit Committee briefed the Board on highlights from the
meeting including the final review and approval of the Annual Report and Accounts
2020/21, referring to the delegation the Committee had received from the Board at its
May Board meeting. She advised that the Trust had received a clean external audit
opinion and with regard to value for money, with no significant control issues reported.
The Chair of the Audit Committee reported on the meeting of the Committee members
with the Internal and External Auditors and reported on the praise she received on the
work of the Finance Team and thanked the whole team for their hard work and
diligence in the production of the Financial Statements.
With regard to the Committee objectives for 2021/22, the Chair of the Audit Committee
advised that these had been agreed and included focus on ensuring sharing of lessons
learned and understanding the risk management plans for key strategic projects.
The Chair’s Audit Committee report was noted.
148/21 Any Other Business
None.
149/21 Date and Time of Next Meeting
The next Board of Directors meeting in public will take place on Monday 26 July 2021
at 1.00pm via Microsoft Teams.
150/21 Resolution
The Board of Directors approved the resolution ‘that representatives of the press and
other members of the public be excluded from the remainder of this meeting, having
regard to the confidential nature of the business to be transacted’.
Questions from the Public
No questions from the public had been submitted in advance. The chairman closed the
meeting.
Certified as a true record of the meeting.
………………………………………………………… ……………………………………………………………
Chair – Rupert Nichols Date
1
Board of Directors – Part 1
TITLE OF REPORT: Chief Executive’s Brief – July 2021
DATE OF MEETING: Monday 26 July 2021
AGENDA ITEM: 07
PRESENTED BY: Neil Thwaite, Chief Executive
AUTHOR(S): Communications and Marketing Team
Steph Neville, Head of Corporate Affairs
REPORT SUMMARY: The following CEO Brief brings together information on key national, regional and
local issues from other internal and external communications. Post-Board the CEO
Brief is updated with a summary of the Board’s key decisions and areas of discussion
and shared with the Trust’s Senior Leaders for wider cascade.
THIS REPORT SUPPORTS ACHIEVEMENT OF THE FOLLOWING STRATEGIC OBJECTIVES:
Objective 1 – Work with service users and carers to achieve their goals by delivering high quality care x
Objective 2 – Create an outstanding place to work, ensuring staff feel valued and are supported to
reach their potential
x
Objective 3 – Continuously improve services for users through research, innovation and digital
technology
x
Objective 4 – Work in partnership with others to improve wellbeing and challenge stigma x
Objective 5 – Be a sustainable, well-led organisation that delivers social value x
REPORT CONSIDERED AT THE FOLLOWING COMMITTEES/SUB-GROUPS:
Committee/Sub-Group: Date:
Audit Committee -
Quality Improvement Committee -
Charitable Funds Committee -
Remuneration & Terms of Service Committee -
Council of Governors -
Executive Management Team -
2
LEGAL IMPLICATIONS: None identified
REGULATORY
IMPLICATIONS (CQC/NHSEI):
None identified
THIS REPORT PROVIDES ASSURANCE AGAINST A RISK ON THE BOARD ASSURANCE FRAMEWORK (BAF):
No
If ‘yes’:
RISK ID Strategic Objective Description (as per BAF)
PURPOSE OF REPORT – Please tick all relevant boxes
Information
X Assurance Approval/Decision
RECOMMENDATIONS: The Board of Directors are asked to receive and note the Chief Executive’s briefing
This document identifies the key national, regional and local issues that are impacting upon or are relevant to the Trust
Action required / in progress
For information
Our Response to COVID-19
2
National and Regional Update• Publication of the Health and Care Bill• GMMH to be the Lead Provider for Adult Secure Services in GM• Supporting Urgent Care Across Our Health Systems
Chief Executive’s Monthly Brief – July 2021
• Perfect Week launches in Salford• Quarterly Staff Survey and Home Working Survey 2021• New Park House Development update• Video to promote our Staff Networks• Take part in a new Listen, Share, Hold, Respond study• World Hepatitis Day: Let's Talk About Hep C• 24/7 Helpline National Recognition• MCT Pathway Study Results Event• The Curve lit up blue to mark the NHS 73rd Birthday• NHS awarded the George Cross by Her Majesty The Queen• Sir Captain Tom’s Farewell Funding• The Dragons are back...• Adding Value Programme: Making Ideas Shine Brighter• Trust Strategy 2019-24• Finance Overview• Performance Overview
Local News
Our Response to COVID-19
Leads: Gill Green, Director of Nursing and Governance and Deborah Partington, Director of Operations
Gold Command / Recovery PlanningGold Command and the Recovery Planning Group continue to oversee the Trust’s response to COVID-19
Gold Command has recently provided:
• Close review of the suspension of visiting to Bolton inpatient units
• Clinical services business continuity• Outbreak review including in prison services• Oversight of LFT take up and weekly inpatient
swabbing• EU Settlement Scheme• Overview of vaccinations and plans for Autumn
Gold Command will remain in place as we closely monitor the impact of the ease in restrictions.
Recovery Group has recently reviewed:
• Long Covid update• Manchester PCN model and update• Priority workstream progress report• Recovery dashboards and performance by each
division• Recovery Academy update• Operational Plan Recruitment update• Overview of ROC activity and progress
Chief Executive’s Monthly Brief – July 2021
3
Delivering the COVID-19 Vaccination Programme
Lead: Gill Green, Director of Nursing and Governance
Our Response to COVID-19
To encourage BAME members of staff to have their vaccine, we shared a video of members of our BAME Staff Network from across the Trust, who teamed up to tell their story of why they have had the COVID-19 vaccination and encourage others to do the same.
Chief Executive’s Monthly Brief – July 2021
The vaccination team are concentrating their efforts across the Trust, delivering vaccines to inpatients. However, where staff still require a vaccine, this is being accommodated in the different areas when the team are in attendance.
GMMH are now able to offer the Pfizer vaccination to our service users, under the age of 40, who are currently receiving care and treatment in our bed bases. The vaccination administration follows national guidance. GMMH are taking a proactive approach to enable our service users to have a further option in accessing vaccinations.
The number of staff being vaccinated is steadily increasing across the Trust; however, the rate of staff vaccinated who are from a non-white ethnic background remains lower.
4
5
National Update
Lead: Neil Thwaite, Chief Executive
Publication of the Health and Care Bill
Chief Executive’s Monthly Brief – July 2021
The Health and Care Bill was published on the 6 July.
The Bill follows proposals for legislative change originally brought forward by NHS England and NHS Improvement (NHSE/I) in autumn 2019 in its Long Term Plan, while also incorporating valuable lessons learnt from the pandemic that will benefit both staff and patients.
The majority of the Bill is focused on developing system working, with integrated care systems (ICSs) being put on a statutory footing. This will result in CCGs being abolished.
It also formally merges NHS England and NHS Improvement, and gives the secretary of state a range of powers of direction over the national NHS bodies and local systems and trusts.
Other measures proposed include putting the Healthcare Safety Investigation Branch (HSIB) on a statutory footing; a new legal power to make payments directly to social care providers; the development of a new procurement regime for the NHS; and a new duty on the secretary of state to report on workforce responsibilities.
6
Regional Update
Lead: Liz Calder, Director of Performance and Strategic Development
GMMH to be the Lead Provider for Adult Secure Services in GM
Chief Executive’s Monthly Brief – July 2021
As part of the NHS Long Term Plan specialised mentalhealth services will become part of NHS-led ProviderCollaboratives. These are groups of providers working inpartnership to be responsible and accountable for theplacement and care of a cohort of patients, with overallaccountability to NHS England. They are clinically-led withpatient benefits at the centre of their approach. One of thepartners operates as the Lead Provider, taking overallresponsibility for the commissioning of the services.
GMMH will be the lead provider for the Greater ManchesterAdult Secure Services Provider Collaborative. Partnersinclude Pennine Care FT, Elysium Healthcare and CygnetHealthcare. We aim to be fully operational by 1 October2021.
GMMH is also a provider partner of the GM CAMHSProvider Collaborative, led by Pennine Care,
and working closely with the North West Eating Disorders.Provider Collaborative, led by Cheshire and Wirral PartnershipTrust.
7
Regional Update
Lead: Deborah Partington, Director of Operations
Supporting Urgent Care Across Our Health Systems
Chief Executive’s Monthly Brief – July 2021
Many accident and emergency departments across the country are currently undergoing high demand for their services.
Primary Care and mental health services are offering support to this by highlighting the different routes on offer to access healthcare other than attending A&E, such as NHS 111, walk in centres, minor injury units, pharmacies and mental health urgent care.
GMMH has been supporting health systems across Manchester, Trafford and Wigan by promoting the 24/7 GMMH helpline as well as the crisis cafes located in the centre of Manchester, Harpurhey and Atherleigh Park, Wigan, to ensure communities know mental health help is available at all times of day.
8
Local News
Perfect Week Travels to Salford
Chief Executive’s Monthly Brief – July 2021
Lead: Deborah Partington, Director of Operations
The Perfect Week, which is part of the Healthier Patient Programme is a five-day event which concentrates efforts on improving and delivering excellent care via enhanced patient flow. The week gives staff the opportunity to work together and test ideas, and challenge everyday practices to make lasting change.
Following on from Bolton's Perfect Week success at the end of June, the next place to host was Salford from 5 to 9 July 2021. The week exceeded all expectations, with great leadership, clinical involvement and patient flow resulting in timely, collaborative discharges.
With absolutely no compromise on quality, bed occupancy, patient flow, admission and discharge were all greatly improved.
Next stop – North and Central Manchester!
‘Every minute of a patient’s life is precious’.
9
Local News
National Quarterly Pulse Staff Survey
Chief Executive’s Monthly Brief – July 2021
Lead: Andrew Maloney, Deputy Chief Executive / Director of HR
During the unexpected challenges of the last 18months, it was agreed that the Staff Friends and Family Test (now termed the National Quarterly Pulse Survey) would be paused.
However, as things are gradually easing, we are keen to understand how staff are feeling about the organisation at this time.
The Picker Team, are currently writing to staff to ask them to take part in this quarter of the National Quarterly Pulse Survey. The survey asks for their views on our Trust, is very short and can be completed in less than 5 minutes. Staff also have the chance to provide comments.
Feedback will help the Trust design improvements to the care we provide and employees working experience.
Following the very informative Home Working Survey in 2020, we are keen to update our understanding of the experience of staff working from home at this point with a Home Working Survey for 2021.
We are currently seeking valued feedback regarding the home/hybrid working situation, as we are mindful that homeworking for many was something that happened as a necessity during COVID-19, rather than choice.
We have communicated the survey to all staff, but have said that it is targeted at staff who currently work from home or are in hybrid (partial home/ work based) working arrangement. The survey closes on Wednesday 21 July 2021.
Home Working Survey 2021
10
Local News
New Park House Development update
Chief Executive’s Monthly Brief – July 2021
Lead: Andrew Maloney, Deputy Chief Executive / Director of HR
The Full Business Case has been completed and is now proceeding through the necessary approvals and support from commissioning and other key stakeholder organisations.
We are on target for July's Board of Directors to consider the Business Case for onward submission to NHS England and NHS Improvement (NHSE/I).
There is much exciting work to do to prepare ourselves for the new building, and some of the development work with staff is already under way.
We are currently working on a new ‘care explainer' animation emphasising ways of changing care practices and how the new build will support this as well as assisting explanations about least restrictive practice and use of seclusion.
Work is continuing on the design of the new building with opportunities over the coming months for staff, service users, carers and localcommunities to take part in specific pieces of work looking at the interior design, feel and branding for the new development.
Video to promote our Staff Networks
11
Local News
Chief Executive’s Monthly Brief – July 2021
The Trust's Communications Team has been working with Staff Network Leads to produce a film to raise awareness of our three staff networks – BAME network, Disability network and LGBT+ network.
This 3-minute film, presented by Tracy Tsikai, Chair of the BAME Staff Network, Pete Smith, Chair of the LGBT Staff Network and Michelle Clarkson, Co-Chair of the Staff Disability Network, includes an overview of the vision behind our staff networks and the roles the different networks play in creating a safe, inclusive and diverse working environment that encourages respect and equality for all.
The aim was to create a film raising awareness of GMMH's staff networks and encouraging viewers to contact Staff Network Leads to join a staff network of their interest.
The final film will be housed on the Staff Networks page on the intranet and website, promoted in our all-staff bulletin and across our social network channels.
Lead: Andrew Maloney, Deputy Chief Executive/Director of HR
We are also exploring options for showing the film at Trust Welcome days and featuring it within the Executive welcome for senior leaders.
Take part in our new LiSHoRe study
12
Local News
Chief Executive’s Monthly Brief – July 2021
GMMH is taking part in a new consultation project called Listen, Share, Hold, Respond (LiSHoRe). LiSHoRe is a multi-site, participatory study being led by colleagues from Oxford Health NHS Trust and Oxford Brookes University.
The study aims to understand the psycho-spiritual experiences and support needs of Black, Asian and Ethnically Diverse NHS staff, who have been disproportionately affected by the pandemic.
A series of supportive Consultation Groups across 10 different NHS Trusts, including GMMH, are taking place (remotely via Microsoft Teams) over the next few months. These groups will provide an opportunity for staff to talk about their views and experiences of the pandemic and how it has impacted on them, their spiritual and religious experiences and needs.
Lead: Gill Green, Director of Nursing and Governance
We would like to invite Black, Asian and Ethnically Diverse colleagues to participate in one of these groups which should last between 60-90 minutes.
The Trust is supporting this initiative and it has been agreed that staff participating in the study are allowed to so within work time.
The first focus group meeting will take place on Thursday 19 August 13:30 –15:00. Other focus groups will also be held at later dates with 8-15 staff in each group.
For World Hepatitis Day on 28 July 2021, Achieve ran an online event to have an open discussion about Hep C. We covered what it is, how to get tested, what treatment involves, how to prevent it and how to spread the message.
Lead: Deborah Partington, Director of Operations
24/7 Helpline National Recognition
Our 24/7 helpline was rapidly mobilised in March 2020 to support people of all ages experiencing a mental health crisis or carers whose loved ones who needed urgent help with their mental health. Volunteers from across the Trust stepped up to ensure this support was available at a time when people needed it the most.
A case study about our helpline has been shared on the national NHS England website, as part of a piece about the national crisis lines response.
14
Local News
Chief Executive’s Monthly Brief – July 2021
Lead: Andrew Maloney, Deputy Chief Executive/Director of HR
NHS awarded the George Cross by Her Majesty The QueenOn Saturday 3 July, Greater Manchester Mental Health
NHS Trust (GMMH) lit up their headquarters, The Curve, in blue to mark the NHS’s 73rd birthday after a year like no other. The NHS’s birthday was a chance to reflect on the past year and celebrate the achievements and resilience of our NHS and local communities.
The Curve joined local landmarks and iconic buildings across England – particularly those who have been enlisted as vaccination sites – to be lit up blue on Saturday 3 July.
The Curve lit up blue to mark the NHS 73rd Birthday
On the NHS 73rd Birthday, Her Majesty The Queen announced that the NHS has been awarded the George Cross.
The award comes in recognition of 73 years of dedicated service, including all your courageous efforts in batting the COVID-19 pandemic.
We sent an email to all staff with the good news and to thank everyone for their hard work over the last few years.
15
Local News
Chief Executive’s Monthly Brief – July 2021
Lead: Andrew Maloney, Deputy Chief Executive/Director of HR
Sir Captain Tom’s Farewell FundingOn Monday 5th July, we sent an email to all staff with an update on the Sir Captain Tom's Farewell Funding bids for projects which would directly benefit staff and/or service user health and wellbeing.
We were inundated with bids and each and every one was amazing. We were so impressed with the creativity, the dedication to help each other and those we care for, and the innovative ideas which were presented. Examples are:
• Provision of outdoor furniture for staff and service users and other general improvements to outdoor areas such as garden and/or allotment equipment
• Updating of sensory rooms, both with equipment, general maintenance and redecoration
• Digital equipment to help service users keep in touch with friends and family
• Updating of staff rest rooms and facilities for refreshment• Team building activities
In acknowledgment of how important this agenda is especially in light of the last 18 months, we advised staff that the decision had been made to approve all bids as a testament to how much we value the effort and commitment our staff have shown.
16
Local News
Chief Executive’s Monthly Brief – July 2021
The Dragons are back...
Our Dragons are returning to the Den to hear ideas from our staff members about quality improvement initiatives to benefit our service users, careers and to improve staff experience.
The Dragons’ Den initiative launched on Monday 5th July to coincide with the NHS’s 73rd Birthday, signifying a time for hope when looking towards the future and to recognise and thank our extraordinary staff for their outstanding care and support during the difficulties of last year.
We are asking our colleagues to make a short, two-minute film to include brief details of their idea, which Quality Improvement Programme it relates to, how it improves quality and how it will benefit the care provided to our service users and carers or improve staff experience.
Lead: Gill Green, Director of Nursing and Governance
17
Local News
Chief Executive’s Monthly Brief – July 2021
Adding Value Programme: Making Ideas Shine Brighter
Lead: Suzanne Robinson, Director of Finance and IM&T
To support the Trust’s fifth strategic objective ‘Sustainable Services; Adding Value’, we will be launching our Adding Value programme during July.
This initiative will support staff to share their ideas on how we get best value from every pound we spend.
A Trust-wide multi-disciplinary group has been formed which will focus on the abundance of benchmarking data we hold, provided a unique space to challenge ourselves of why there is variation, exploring what the data is actually telling us, being inquisitive as to where we can improve, and looking at how we can be more productive, reduce waste and be more efficient.
An Adding Value Ideas Portal has been developed on the intranet which makes it very easy for all staff from across the Trust to submit their ideas.
These will then be assessed to make sure every great idea is considered and supported to make them become a reality.
3
Local News
Chief Executive’s Monthly Brief – July 2021
Trust Strategy 2019-24
Lead: Andrew Maloney, Deputy Chief Executive/Director of HR
In support of the GMMH's Trust Strategy, we will be launching a range of strategy focused resources, which staff can download from the Intranet's Trust Strategy Hub.
The first phase of resources include email signatures and MS Teams backgrounds, which highlight individual objectives, along with our strapline 'Our ambition is for people to have improved lived and optimistic futures'.
The Trust Strategy Hub can be found here: https://dearauahotmail.sharepoint.com/SitePages/Trust-Strategy-2019-24.aspx
Finance Overview
19Lead: Suzanne Robinson, Director of Finance and IM&T
Chief Executive’s Monthly Brief – July 2021Local Update
In 2021/22 we are still operating the financial year in 2 parts;H1 – which runs 1 April 2021 until 30th September 2021H2 – which runs 1 October 2021 until 31st March 2022
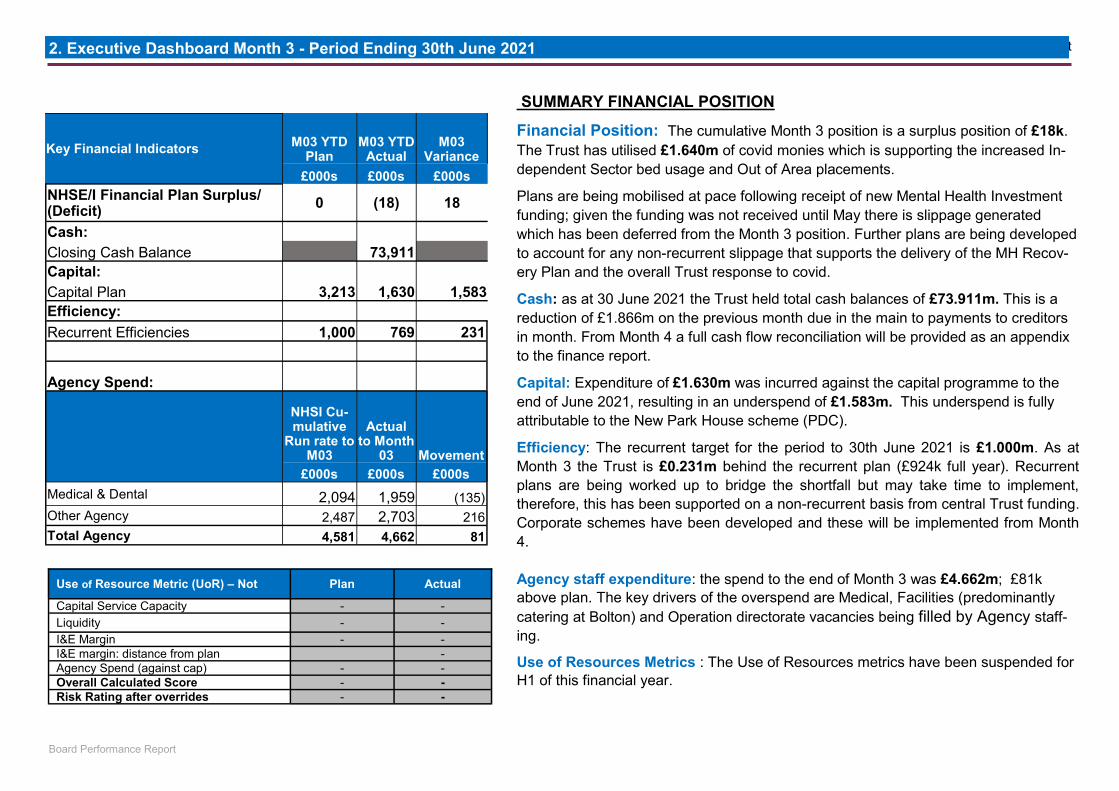
At Month 3 we are reporting a surplus of £18k above plan; within this is achievement of £769k of recurrent efficiencies which is £231k behind plan. GM ICS System Monies continue to support the additional cost of Independent Sector acute beds, demand for which has increased during the pandemic.
New Mental Health Funding was received in April to support the delivery of the Long Term Plan ambitions. Plans need to be developed at pace to ensure we get value from every pound received.
CapitalThe YTD plan required spend of £3.213m; as at Month 3 £1.630m was spent resulting in an underspend of £1.583m.
This underspend is fully attributable to the New Park House scheme (PDC); we’re updated the phasing of how much we’ll spend in 2021/22 as part of the FBC which is going to Board in July.
Better Payment Practice Code (BPPC)The BPCC requires us to pay 95% of our invoices within 30 days which is particularly important for local suppliers and keeps our local economy moving. In Month 3 we paid;
Value £ VolumeNHS 100% 100%
Non NHS 99.04% 98.51%
20
Local Update
Lead: Liz Calder, Director of Performance and Strategic Development
Performance Overview
Chief Executive’s Monthly Brief – July 2021
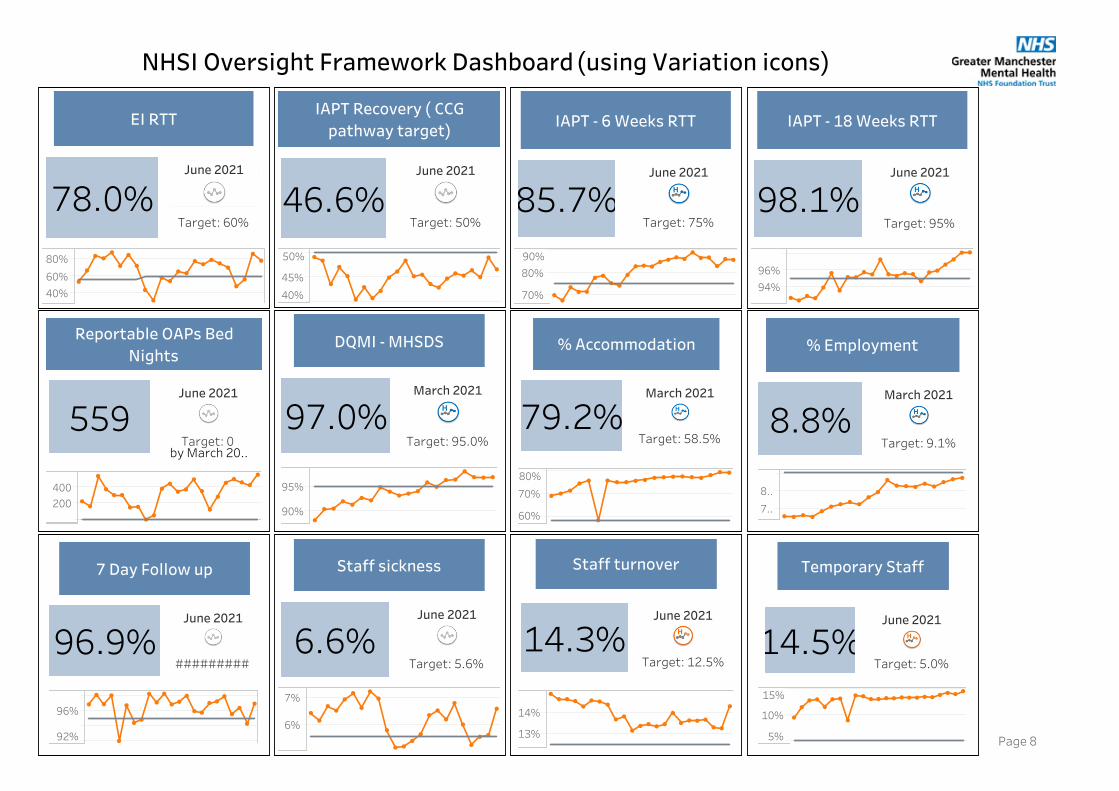
• The Trust continues to deliver good performance during the Covid-19 response.
• The good performance on IAPT access rates continue with both 6 and 18 week targets met at a Trust level.
• The access target for Early Intervention services have also continued to be met by all divisions
• The number of delayed discharges have increased in month. This reflects the impact of GM system wide work and a GMMH project ‘Healthier Patient Pathways’ to identify and prioritisedischarges, reduce length of stay and enhance patient flow. An initial increase was expected.
• Sickness levels have increased this month above the Trust target. This is due to an increase in short term absence and includes Covid related sickness. The overall trend for long term absence continues to reduce.
• There continues to be pressure on CAMHS services in Bolton due to increased referrals. Robust oversight of capacity and demand is in place inclusive of out of hours working. A multi agency referral pilot is also in progress to ensure referrals are directed appropriately to our partners.
‘Every minute of a patient’s life is precious’. It was Salford’s turn to host the Perfect Week from 5 to 9 July 2021. The Perfect Week is part of the Healthier Patient Pathway Programme and aims to provide a gold standard patient and service user experience. Using a ‘best care, every day’ approach, directly from our Trust’s long-term strategy, the purpose of the week is to adopt new approaches and challenge usual practices to make lasting change.
What did Salford’s Perfect Week look like?
The Perfect Week team in Salford developed a clear plan for admission which set out the rational for all admissions. Patient engagement was vital, with ‘me and my care plan’ and ‘your time to talk’ being used in ward rounds from the point of admission.
As with Bolton, Salford used a Bronze, Silver and
Gold approach, which meant that any barriers to discharge were escalated and prioritised.
Regarding discharge planning, a collaborative approach was taken, with the first ever ‘criteria-led discharge’ being carried out that weekend – more to follow!
How did it go?
The week was extremely successful with discharge plans being developed upon admission. There was a calm and collaborative team approach which included CMHT, theinpatient teams, review and commissioning teams and the patient’s family and carers involved. Patients who had been on a ward for a long period of time were provided with a transfer plan. Some patients who had
been waiting to move, were enabled to do so, and some admissions were signposted to other more suitable alternatives.
Highlights of the week included the participation of system wide partners and colleagues, the patient flow team, collective leadership and fantastic clinical involvement and leadership, teamwork, and enthusiasm. As with the Bolton
Salford Perfect Week Team
Cara Oates and Rebecca Billington
“Good escalation process improving patient care and not a burden to our workload.”
WHAT OUR STAFF SAID:
“There is quicker feedback regarding barriers, due to escalation.
WHAT OUR STAFF SAID:
21
experience, the senior management support – which has always been available – was fully utilised and helped enormously.
Ward teams identified that they were able to get on with the business of delivering great care, ably supported by local managers, meaning they were freed up to spend time with patients. This epitomises the essence of the perfect week!
We, of course have taken time to identify what we can learn and do better. Going forward we think there is an opportunity to look at the Perfect Week in our later life and community services so watch this space!!
Head of Operations for Salford, Karen Hodgetts said: “The week was a great success, with 17 people discharged over just five days. There was absolutely no compromise in quality and clinicians led the way, as they always do in Salford!
“I could not be prouder of everyone who took part in this week, from ward managers, community teams, the inpatient teams to the review team, home-based treatment and mental health liaison. You all knocked down barriers and continued to deliver exceptional care. Thank you all.”
John Walker, Associate Director said: “What has been great about Salford’s Perfect Week was that we did not ask staff to make huge changes to their usual practices as Salford is such a very highly functioning team. However, we made a few tweaks, which made a big difference and wow what a huge impact. I cannot congratulate the team enough, and of course expertly guided by Karen’s and Dr Bhandary’s expert leadership. A special thank you to Beccy for expertly chairing the meetings and a big well done #TeamSalford”
Click here to see Simon Glover, Lead Nurse for the Healthier Patient Pathway give his views on how remaining calm contributed to Salford’s success.
The Perfect Week has provided Salford with a wealth of evidence to embed change and continue to see improvements.
Next stop – North Manchester!
“First time PICU is clear since I started in June 2020!”
TITLE OF REPORT: COVID-19 and Recovery Briefing – Oversight Report (July 2021) DATE OF MEETING: Monday 26 July 2021 AGENDA ITEM: 08 PRESENTED BY: Gill Green Executive Director of Nursing and Governance and Deborah Partington
Executive Director of Operations AUTHOR(S): Clair Carson, Associate Director of Nursing and Governance
Juliette Tait, Associate Director of HR John Walker, Associate Director of Operations
REPORT SUMMARY: This briefing paper provides an update to the Board of Directors on GMMH’s
response to the Covid-19 pandemic. On 29th March 2021 the Trust Board of Directors considered a briefing report describing the work of Gold Command and the Recovery Planning Group. This paper now provides an update on developments and progress since 29th March 2021 and includes information for the month of July 2021 on the following: • Update on Gold Command • National and daily SitRep summary data • Staffing position • Infection, prevention, and control • Update from the Trust Mass Testing and Vaccine Group • Visiting and leave arrangements • Update on the work of the Recovery Planning Group
THIS REPORT SUPPORTS ACHIEVEMENT OF THE FOLLOWING CORPORATE OBJECTIVES: Objective 1 – Promote recovery by providing high quality care and delivering excellent outcomes
x Objective 4 – Invest in our environments
Objective 2 – Work with service users and carers to achieve their goals
x Objective 5 – Enable staff to reach their potential and innovate
Objective 3 – Engage in effective partnership working
x Objective 6 – Achieve financial strength and be well-governed
2
REPORT CONSIDERED AT THE FOLLOWING COMMITTEES/SUB-GROUPS: Committee/Sub-Group: Date: Audit Committee Quality Improvement Committee Charitable Funds Committee Remuneration & Terms of Service Committee Council of Governors Executive Management Team
LEGAL IMPLICATIONS:
REGULATORY IMPLICATIONS (CQC/NHSI):
THIS REPORT PROVIDES ASSURANCE AGAINST A RISK ON THE BOARD ASSURANCE FRAMEWORK (BAF):
No
If ‘yes’:
DATIX ID Strategic Objective Description (as per BAF)
PURPOSE OF REPORT – Please check all relevant boxes
Information
x Assurance x Approval/Decision
RECOMMENDATIONS: The Board of Directors are asked to note the comprehensive work which has been
undertaken by GMMH in response to Covid-19, the recovery planning work and the priorities going forward.
1
COVID-19 and Recovery Briefing – Oversight Report June 2021
1. Introduction This briefing paper provides an update to the Board of Directors on GMMH’s response to the Covid-19 pandemic. On 29th March 2021 the Trust Board of Directors considered a briefing report describing the work of Gold Command and the Recovery Planning Group. This paper now provides an update on developments and progress since 29th March 2021 and includes information on the following:
• Update on Gold Command • National and daily SitRep summary data • Staffing position • Infection, prevention, and control • Update from the Trust Mass Testing and Vaccine Group • Visiting and leave arrangements • Update on the work of the Recovery Planning Group
2. Update on Gold Command Gold Command has continued to closely monitor the position and the impact of Covid taking the appropriate action as required. An update of the work of Gold Command over the last month is provided below. 2.1 Daily National and Local SitRep Reporting
Gold Command continues to review the daily internal Situation Report (SitRep) for patients and staffing and signs off the daily National Mental Health and Specialist Services Situation reports. In addition, the Trust continues to submit the weekly Lateral Flow Testing returns along with the fortnightly Vaccine Programme submissions. By way of a reminder, the OPEL Report that was previously submitted to NHSE on a weekly basis was discontinued on 10th May 2021.
2
Table 1 – Summary of key National SitRep data for the period up to 6th July 2021
Figure 1 – Daily Covid-19 Activity for Inpatient and Community Services up to 6th July 2021
3
Figure 2 – Daily Covid-19 Activity for Inpatient Services only up to 6th July 2021
Figure 3 – Daily Covid-19 Staff Sickness up to 6th July 2021
2.2 Staffing Position
Those absent with Covid (Tested and Confirmed) has increased from 13th May 2021 to 6th July 2021. This has impacted on the overall Trust sickness absence level which increased during June from 5.69% to 6.34%. Sickness levels are above the Trust target (5.6%) and higher than the same month in the previous year (5.18% June 2020). Based on Health Roster data, 880 FTE days were lost during June due to Covid compared to 673 FTE days lost during May.
4
Absence continues to be managed locally within services, with support from the HR advisory team. Gold Command maintains oversight of the day-to-day staffing changes, informed by daily Sit Rep calls undertaken by senior representatives from the operational team.
2.3 Infection Prevention and Control (IPC) The Infection, Prevention and Control (IPC) Team continues to ensure that Trust policies and procedures are up-to-date and in line with the latest regional and national guidance. Senior members of the IPC Team also maintain contact with North West IPC Leads and represent the Trust on Greater Manchester Forums. The team work closely with operational and corporate colleagues so to ensure that IPC practice/standards are maintained. Since the last report monthly IPC audits on later life wards have been initiated which aim to provide further assurance. Later Life Wards
Area Wards Salford, Woodlands Hospital Delamere, Holly, and Hazelwood Wards North Manchester Maple Ward South Manchester Cavendish Ward Trafford Greenway and Bolin Wards
The IPC Team have also undertaken audits across 17 wards, feedback to each Ward Manager/Service Lead has been provided and an overarching report is in draft. Targeted visits have been completed with in-depth recovery plans put in place as required. 2.4 COVID-19 Outbreaks The Trust continues to manage and report on any outbreak in line with regional and national guidelines. Summary COVID-19 Outbreak Data (range) 01/04/2021 – 06/07/2021
Outbreak Area COVID-19 Positive Patients at peak of outbreak
COVID-19 positive staff at peak of outbreak
Status
Redwood Ward 3 0 Ended Delamere Ward 6 0 Ended Estates and Facilities N/A 3 Current
As previously outlined to members of the Board of Directors, once an outbreak has been confirmed the GMMH Outbreak Policy is activated and followed. Outbreak meetings are used to help identify root causes, review ward cohorting plans, and support staff with managing the outbreak. The extent of the outbreak determines the frequency of the meetings. GMMH submit outbreak data directly onto the national platform and daily SitRep reports are produced.
5
2.4.1 Learning from COVID-19 Outbreaks The Trust continues to use a continuous learning approach to preventing and managing COVID-19. This includes sharing good practice with the regional IPC Leads, and learning from our GM partners. Feedback on our management of outbreaks from Public Health England and NHSE/I have been positive to date. Learning continues to be shared through the daily Operational Leadership Team meetings by the Nursing and Governance Team. Specific outbreak summary reports have been co-produced for Gold Command detailing cluster or larger outbreaks, the learning from which has been shared. As we enter the next step of the Government’s response to the Pandemic COVID-19 Response: Summer 2021 - GOV.UK (www.gov.uk) the IPC Team will support the Trust to develop clear guidance on the following. 1) Vaccination strategy, including on-going COVID-19 vaccinations, boosters), and Influenza vaccine. 2) Ensure that the Trust is informed and kept up to date with national and regional guidance, including test,
track, and trace. 3) Monitor and respond to variants of concern (VOC) and variants of interest (VOI). 4) Retain contingency measures to respond to unexpected events, while accepting that further cases, and
surges will occur. 5) 2.5 Update from the Trust Mass Testing and Vaccine Group The Trust Mass Testing and Vaccine Group, chaired by the Director of Nursing, plans the Trust’s role in all patient and staff mass testing programmes as well as:
Specific updates from the GMMH Mass Testing and Vaccine Group are provided below. 2.5.1 Lateral Flow Testing The GMMH Mass Testing Group and Vaccine Group (MTAVG) continue to lead the implementation of the Lateral Flow Testing (LFT) programme across the organisation. It has been declared nationally that Trust will no longer directly receive lateral flow kits and instead must ensure their staff access the kits via recognised Government means- such as online or via local pharmacies. GMMH continue to provide kits via local PPE hubs as stock still remains in the Trust and communication messages are also regularly sent to all staff to source them through this route or via the Government schemes. Recording of tests is still encouraged via the GMMH app to provide support when required to hotspot/outbreak areas. 2.5.2 COVID-19 Vaccine The Trust vaccination team has been reduced overtime to meet the need of the service, it is based in Rooms 4 and 5 within the Curve.
The team is currently concentrating all its efforts on in- patients.
Following the JCVI announcement around age restrictions for the use of Astra Zeneca, GMMH has been successful in securing a small amount of Pfizer to be used as an AZ alternative for admissions under the age of 40 years. A new Pfizer specific SOP has been developed and following staff training, undertaken at MRI, the team started to deliver Pfizer on the 23rd of June 2021.
As of the 6th of July 2021, 1,229 doses of Astra Zeneca and 50 doses of Pfizer have been administered to in-patients at GMMH.
Of the current 841 occupied inpatient beds
• 113 (13.4%) have received a single dose • 461 (54.8%) have received two doses • 164 (19.5%) have actively declined to receive a vaccine. • 103 (12.2%) have neither received or declined a dose of vaccine (this group contains new admissions,
those not eligible for vaccine due to being under 18 years of age or for whom vaccine is clinically contra-indicated)
Therefore, 738 (88.7%) of current inpatients have had either 1 or 2 doses of the vaccine or have actively declined the vaccine at GMMH.
The Vaccination team continues to work with clinical colleagues and in-patients where there is a reluctance to accept the vaccine.
New starters within the Trust can access vaccination via the team as required, however, there are currently no planned large-scale clinics at this time.
Against a head count of 6,129 - 82.9% are known to have received a first dose of vaccine and 78.2% are known to have received a second dose. The discrepancy in 1st and 2nd doses is expected to be as a result of the vaccine being made more readily available via a number of outlets, as when staff have been contacted, following a failure to attend agreed appointments, they have largely stated they have attended an alternative location.
2.6 Visiting and Leave Arrangements Supporting service users to maintain contact with their families and loved ones during their inpatient stay remains an important priority through the fluctuating lockdown restrictions. Due to the requirement to meet COVID-19 safe restrictions, GMMH have continued to support a risk assessed visiting policy with safeguards in place to ensure that those who are assessed as in clinical need to receive a visit, have been reviewed by the MDT and a safe plan put in place to support this.
The GMMH Visiting Policy continues to have oversight by a dedicated multi-disciplinary senior leadership Task and Finish Group. This group ensure the policy is updated to reflect regional/national guidance, taking into consideration community infection prevalence and the number of nosocomial infections. Visits continue to be booked and planned so that they can be managed in a COVID-19 safe way.
1. Visits continue to be planned by the MDT, are care planned and involve family/carers.
2. Visits are risk assessed so that they are COVID-19 safe.
3. Visits are generally limited to one person per family, but in special circumstances additional visitors are permitted.
7
Service users continue to be supported to take leave in order to maintain contact with family and loved ones.
During the last month in line with local restrictions and in agreement with the local clinical teams, due to the prevalence of the new Delta Variant in Bolton, visiting had been temporarily suspended on the inpatient units at Rivington, Honeysuckle Lodge and Woodlands. Previously employed processes to ensure contact is maintained with families are in place including Covid safe leave off site and use of technology. Risk assessed essential leave is still being supportive in cases such as End of Life care. This continued to be reviewed twice weekly via the MTAVG and Gold Command in conjunction with the local SLTs. A decision was made on 12th July 2021 to look to recommence leave from the week beginning the 19th July 2021 in line with other GMMH sites. RBH have been fully engaged in this decision and safe practices employed to manage this safely on the Bolton site.
3. Recovery Planning Group
The Trust Covid-19 Recovery Planning Group continues to co-ordinate the Trusts Covid-19 Recovery Plan and oversees the work of the Recovery Workstreams and Task and Finish Groups. The Recovery Planning Group receives regular update reports from each Workstream and Task and Finish Group in line with an agreed schedule of progress reporting. Since the last report to the Board of Directors in June 2021, the Recovery Planning Group has considered update reports from a number of workstreams, and task and finish groups and a summary of these reports is provided in Table 3 below:
Table 3 – Recovery Workstream Reports 12th May 2021- 6th July 2021
Workstream / Task and Finish Group
Summary Report Noted
ROC Team Update
Monthly update report summarising the month of June 2021 activity undertaken by the Resource Operational Cell (ROC), including data reports for the same time period. The report highlighted a number of key points including ongoing daily oversight and active support to services, developing key communication networks with Wigan and block placement booking to be reviewed with NHSP and services.
Service offer- 7-day patient flow summary
New format report shared- well received
Service offer- MATS and Later Life CMHT Final Report
A Trust wide review of MATs waiting lists was undertaken and the paper provided an overview of this and costs for any WLIs for Recovery to consider
Service offer- Manchester Safeguarding referrals
This paper was prepared to understand the safeguarding referral rates within MCC over the last 3 years and understand the divisional variation alongside the current picture. This information was noted to be particularly pertinent with regards to the review of the S.75 agreement with MCC.
Service offer- IAPT Update Report
Noted that that IAPT has undergone a period of unprecedented change over the last 12 months which has enabled services to evolve, innovate and become more
8
flexible. The onward plan is to deliver a varied service offer through a flexible demand lead model i.e. Hub and Spoke accommodation and a virtual remote (IM&T) infrastructure to deliver numerous types of remote therapy.
Service offer- CBU waiting lists
The combination of lockdown, increased access to RADAR during parts of 2020/21 (to support Acute Trust pressures), the unit Covid-19 outbreak in January and the national investment via PHE in medically managed inpatient detox treatment for 2021-22, have contributed to an increased demand for admission to CBU. This has resulted in a waiting list and higher waiting times than usual. This report made some provisional recommendations for consideration to address the position; many of these have since progressed with short and longer term actions to support current activity and also the longer term position of CBU given the varying arrangements in place regarding contracted occupancy.
Service Offer – CAMHs final report
Bolton CAMHS took timely and proportionate actions in line with the commencement of the C-19 pandemic to comply with the requirements of lockdown and maintain service delivery and made a number of positive changes, innovation and improvements over the past 12 months. It was noted that this work will be extended to include Wigan CAMHS and Community Eating Disorders (CED’s) given the recent transfer of these services – in shadow form – to the CAMHS division. A paper regarding CED’s is due for presentation at the next meeting on 27/07/21 given an increase in referrals and waiting times to the service.
Service Offer – SMS update
This T&F Group paper noted that service delivery changes across inpatient and community services, during the lockdown Phases of the pandemic, were in line with guidance from NHSE and PHE. Increases in community total caseload and treatment starts were evident and the service anticipated that additional funding during 2021-22 would alleviate some of this pressure (with the full findings and recommendations of the Dame Carol Black government commissioned review expected to provide strong support for future funding commitments via the Autumn comprehensive spending review).
Service offer- Long Covid support model proposal
This paper described the opportunity to develop a service pathway equipped to meet care for people experiencing post-COVID syndrome; the proposed model includes interfaces with existing services commissioned to address common mental health problems and creates a unique opportunity to monitor, evaluate and learn from service delivery. The service model is estimated as needing to deliver 2,200 new episodes of care (individual people) per year with a stepped care offer and liaison with partners in both primary and secondary care available at all levels.
Service offer- Manchester PCN Model and Update
Noting the aspiration of GMMH to work with commissioners to implement clinically effective roles as part of the developing transformed community mental health system, this paper described the need for development plans to take into account existing challenges regarding qualified staff and the need to avoid destabilising services. Future plans will need to take account of the workforce challenge and more explicitly link to the evolving community redesign plans and learning from existing models must be built into any model going forward.
9
Service offer- OAPs trajectory submission
GMMH continue to be part of a number of initiatives across the North West to support collaboration and learning between local mental health Trust providers. To date, there has been positive support from NHSE/I with collaboration across organisations and wider system support from key partners and stakeholders. There has been system wide support for mental Health trusts to work together to address capacity and demand issues, learn from colleagues, as well as support from NHSE with the North West Bed Bureau.
Service offer- Use of winter funds - ED front door pathways
This model proposed using slippage funds to bolster up the front door of ED and to support teams and departments in therapeutic risk taking and decision making at a time of increased challenge across the health system. Four 8C posts were originally proposed; two experienced practitioners have since been seconded and deployed across identified A&E departments within the organisation. The project will cease at the end of 6 months and a sustainable plan will be proposed to the Executive Director of Operations for each A&E Department.
. Service offer- DTOC summary paper
A small working group of GM partners was formed to review mental health delayed transfers of care (DTOC) and to progress a focussed project with the aim to reduce and eliminate DTOC’s. This paper presented detailed information on the GMMH and PCFT DTOC position on the 30th of April 2021 and identified system wide themes which will be used to support a system wide response to addressing and eliminating mental health DTOC’s. Deborah Partington is leading this project for GM mental health providers, who are working collaboratively to address this important issue.
Research and Innovation- Long Covid update
Presentation from Dr Elaine Maxwell – NIHR given to Recovery Board on latest research and proposed onward work
Workforce- Refreshed workforce strategy – People Plan
The People Plan proposal was shared and a number of actions in support of this identified including the development of a productivity plan through enhanced use of technology and to increase engagement in national and regional workforce networks to raise the profile of GMMH as a modern and model employer.
Workforce – Operational Plan Recruitment update
The Operational Plan was submitted on 30th June 2021 and operational services had developed high level business plans which outlined workforce requirements and other detail in relation to each of the funding streams. The need for a robust tracking process to monitor progress was noted as was the need for monthly update reports to be provided to the Recovery Board including a summary of key risks and issues.
Service User and Carer Monthly update
Update report on service user and carer activity provided with 4 key work areas identified and described.
Service User and Carer Recovery Academy Update
Presentation given that covered the key priorities and updates for the Academy including raising awareness of mental health and challenging stigma and plans were supported to develop income generation model to further support GMMH staff and service users/carers
10
Business Support –Digital Progress update provided; this noted a number of ongoing workstreams as well as planned actions for the future.
Business Support – Estates and Facilities update
This paper noted that Estates & Facilities Service were continuing to deliver services as normally as possible whilst adopting updated/ new ways of working to accommodate the issues within COVID 19 and safe working Practices. Key updates included:
• Staff vaccinations - since the mass vaccine element has been successful the large mobile vaccine centre has been replaced by a smaller hub in the Physical Healthcare Room.
• Facilities, Logistics, Transport, and Administration Teams continue to support clinical colleagues with the roving clinics enabling inpatients to receive the Pfizer Vaccination at Hospital Sites across the organization.
• Retaining sufficient PPE in storage for staff with over 6 weeks’ (1.1miliion individual items) stock consistently replenished as required via the Push Deliveries.
4. Conclusion and recommendation The Board of Directors are asked to note the comprehensive work which has been undertaken by GMMH in response to Covid-19, the recovery planning work and the priorities going forward.
1
Board of Directors – Part 1
TITLE OF REPORT: Board Performance Report (June 2021 performance)
DATE OF MEETING: Monday 26 July 2021
AGENDA ITEM: 09
PRESENTED BY: Elizabeth Calder, Director of Performance and Strategic Development
AUTHOR(S): Miranda Washington, Deputy Director of Performance & Business Development
REPORT SUMMARY: This report covers the period to end of June 2021. The report should be seen in
conjunction with the monthly Board Finance report and quarterly Quality report.
Key areas are highlighted in the Executive Summary of the Board report for review.
The Finance and Performance Group is meeting with divisions on a quarterly basis to review achievements and performance, supporting in depth discussions between the Executive Director team and services across a range of performance indicators. As previously reported national and local performance requirements have changed to
enable a comprehensive focus on COVID 19. In line with the national guidance this
report is shared for information rather than for assurance purposes. Some national
reporting remains suspended during this time. The latest nationally reported
information is included in the report and month of position noted.
System wide pressures continue due to Covid 19 and joint work with key stakeholders
to manage this remains a key priority.
THIS REPORT SUPPORTS ACHIEVEMENT OF THE FOLLOWING STRATEGIC OBJECTIVES:
Objective 1 – Work with service users and carers to achieve their goals by delivering high quality care
x
Objective 2 – Create an outstanding place to work, ensuring staff feel valued and are supported to reach their potential
x
Objective 3 – Continuously improve services for users through research, innovation and digital technology
Objective 4 – Work in partnership with others to improve wellbeing and challenge stigma
Objective 5 – Be a sustainable, well-led organisation that delivers social value x
2
REPORT CONSIDERED AT THE FOLLOWING COMMITTEES/SUB-GROUPS:
Committee/Sub-Group: Date:
Audit Committee
Quality Governance Committee
Charitable Funds Committee
Remuneration & Terms of Service Committee
Council of Governors
Executive Management Team 21st July 21
LEGAL IMPLICATIONS: N/A
REGULATORY
IMPLICATIONS (CQC/NHSI):
Compliance with NHSI targets, CQC standards and contractual KPIs
THIS REPORT PROVIDES ASSURANCE AGAINST A RISK ON THE BOARD ASSURANCE FRAMEWORK (BAF):
Yes
If ‘yes’:
DATIX ID Strategic Objective Description (as per BAF)
1490
Objective 1: Work with service users and carers to achieve their goals by delivering high quality care.
Performance - failure to meet national and local targets will impact on quality of care and could incur financial penalties and /or intervention from regulators.
PURPOSE OF REPORT – Please check all relevant boxes
Information
Y Assurance Y Approval/Decision
RECOMMENDATIONS: The Board of Directors is asked to:
• Consider the performance position for the year to date and note the actions
being taken where variance is highlighted.
• Advise as to any further areas where action or further assurance is required.
Board Performance ReportRegulatory and Workforce
v3.6.5
Report Month: June 2021
June Board Performance Report
Executive Summary
Finance Dashboard
Wigan Data Guidance
SPC Reference
NHSI Oversight Framework Metric List
Oversight Framework Dashboard
Additional Indicators List
Safe Domain
Effective Domain
Caring Domain
Well Led Domain
Responsive Domain 26
23
21
18
14
10
8
6
5
4
3
1
Contents
Executive Summary
Page 1
The Board Performance Report is shared for information in line with national guidance during Covid 19.The report shows the performance of the trust during the Covid response and recovery periods. It shouldbe noted that the reporting of a number of national indicators remains suspended at this time. The latestreported information is reflected in this report.
A summary of some notable areas of performance is provided below with further detail in thecommentary of the report.
Finance dashboard – The Month 3 dashboard provides a cumulative position in the June report coveringQ1. The financial position as at Month 3 is breakeven. National guidance for the Use of Resource metricshas confirmed that these will remain on hold for the first six months of 21/22.
IAPT referral to treatment access times – Positive performance continues with both 6 week and 18 weektargets met. Work remains ongoing in Manchester to ensure targets can be met consistently.
Out of Area bed nights - Reportable OAP bed nights showed an increase in month however the number ofnew placements made did reduce which reflects the continued work with our system wide partners todevelop alternatives for discharge. The GMMH Healthier Patient Pathways Project is also now in place.This work aims to support the reduction of OAPs by improving patient flow and supporting people as closeto home as possible.
The number of independent sector beds nights used in month reduced in June. This is in part due to theshorter month of June and also due to a decrease in independent sector PICU bed nights used.
The national target to reduce OAPs to zero is the end of Q2 2021/22. GMMH's ambition remains to reduceOAPs to zero as soon as possible and by Q3 at the latest.
Delayed discharges – The previous target shown of 7.5% has been updated to reflect the current targetfor acute trusts of 3.5% to ensure system wide consistency. This is shown as a local benchmark in thereport. There was an increase in month in all speciality areas. This reflects positive work withcommissioners and system partners on a Greater Manchester delayed discharge project aimed atidentifying and prioritising discharges, resolving delays and supporting delivery of a zero delayeddischarge position. We can expect to see an initial increase for the next few months before the reductioncan be achieved. Staff sickness – levels of sickness increased above the trust target this month. This is due to an increasein short term sickness for mental health and Covid reasons. HR managers are reviewing the position withservices to identify any support required.
Potential under reporting of patient safety incidents - the data is discussed monthly through the PostIncident Review Panel and remains subject to close weekly monitoring through the Associate Director ofNursing and Governance and relevant Associate Directors of Operations with a planned trajectory offurther improvement now established. Appraisals – Actions are in place to ensure improvement continues in the coming months.
Information Governance training – The target was not met in month. Work continues to raise theawareness of maintaining IG training compliance with staff and to highlight to senior managers wherestaff are outstanding with their training.
Executive Summary (Cont)
Page 2
Bolton CAMHS waiting times – Waiting times have increased in month. This reflects a continued increasein referrals which has impacted on ability to achieve this target. Robust oversight is being maintainedwhich includes out of hours working. A multiagency referral hub pilot is in place which should have apositive impact on the number of referrals accepted in the future. Wigan CYP Eating Disorder access times - As reported previously there has been an increase in referralswhich continues to impact on response times. The staffing model has now been reviewed and contractsfor staff employed on fixed term contracts have been extended to March 2022 to support the increase indemand. Three further additional staff will also be put in place to support the team over the comingweeks.
Domain Rating
Safe Requires Improvement
Effective Good
Caring Good
Well-Led Good
Overall Good
CQC Ratings(2)
1 Finance Report
Board Performance Report
SUMMARY FINANCIAL POSITION
Financial Position: The cumulative Month 3 position is a surplus position of £18k.
The Trust has utilised £1.640m of covid monies which is supporting the increased In-
dependent Sector bed usage and Out of Area placements.
Plans are being mobilised at pace following receipt of new Mental Health Investment
funding; given the funding was not received until May there is slippage generated
which has been deferred from the Month 3 position. Further plans are being developed
to account for any non-recurrent slippage that supports the delivery of the MH Recov-
ery Plan and the overall Trust response to covid.
Cash: as at 30 June 2021 the Trust held total cash balances of £73.911m. This is a
reduction of £1.866m on the previous month due in the main to payments to creditors
in month. From Month 4 a full cash flow reconciliation will be provided as an appendix
to the finance report.
Capital: Expenditure of £1.630m was incurred against the capital programme to the
end of June 2021, resulting in an underspend of £1.583m. This underspend is fully
attributable to the New Park House scheme (PDC).
Efficiency: The recurrent target for the period to 30th June 2021 is £1.000m. As at
Month 3 the Trust is £0.231m behind the recurrent plan (£924k full year). Recurrent
plans are being worked up to bridge the shortfall but may take time to implement,
therefore, this has been supported on a non-recurrent basis from central Trust funding.
Corporate schemes have been developed and these will be implemented from Month
4.
Agency staff expenditure: the spend to the end of Month 3 was £4.662m; £81k
above plan. The key drivers of the overspend are Medical, Facilities (predominantly
catering at Bolton) and Operation directorate vacancies being filled by Agency staff-
ing.
Use of Resources Metrics : The Use of Resources metrics have been suspended for
H1 of this financial year.
Use of Resource Metric (UoR) – Not Plan Actual
Capital Service Capacity - -
Liquidity - -
I&E Margin - - I&E margin: distance from plan - Agency Spend (against cap) - - Overall Calculated Score - - Risk Rating after overrides - -
2. Executive Dashboard Month 3 - Period Ending 30th June 2021
Key Financial Indicators M03 YTD
Plan M03 YTD
Actual M03
Variance
£000s £000s £000s
NHSE/I Financial Plan Surplus/(Deficit)
0 (18) 18
Cash:
Closing Cash Balance 73,911
Capital:
Capital Plan 3,213 1,630 1,583
Efficiency:
Recurrent Efficiencies 1,000 769 231
Agency Spend:
NHSI Cu-mulative
Run rate to M03
Actual to Month
03 Movement
£000s £000s £000s
Medical & Dental 2,094 1,959 (135)
Other Agency 2,487 2,703 216
Total Agency 4,581 4,662 81
Inclusion of Wigan data as from 1st April 2021
Page 4
Please note the main Board report now includes Wigan data for April 21 for all metricsreported from corporate information systems as indicated by (W). Information for Wigan canonly be reported from April 2021 when services transferred from North West BoroughsHealthcare NHS Foundation Trust to GMMH and not historically.
Information for metrics reported from non GMMH clinical information systems are attachedat the Wigan Appendix 1. This will continue until the move to GMMH systems is completed.
The metrics included in the Appendix are listed here:
· Early Intervention referral to treatment (RTT)· IAPT 6 week RTT· IAPT 18 week RTT· IAPT Recovery· OAP bed nights· CPA 7 day follow up from inpatient discharge· Under 16 admissions· Delayed Transfer of care· CAMHS referral to first appointment wait· CAMHS second to third appointment wait· Children & Young People Eating Disorder (routine cases) RTT· Children & Young People Eating Disorder (urgent cases) RTT
The only GMMH metric not presented for Wigan is A&E 4 hour waits. This reporting will bedeveloped. A new metric for Board included in the Wigan Appendix is the Children and YoungPeople Eating Disorder RTT as this is a service provided in Wigan that was not provided byGMMH prior to the transfer of services on 1 April 2021.
The Appendix presents the Wigan position and the position for the rest of GMMH. Thecombined Trust position is also shown. This ensures a Trust wide position for all Board levelmetrics can be seen for Board assurance. Commentary is provided as appropriate.
A trend line will be added when six months of data is available.
It should be noted that those metrics reported from national published figures will notinclude Wigan data until the April figures are published.
SPC Icon Reference (NHSI)
Page 5
Methodology adopted from https://improvement.nhs.uk/resources/making-data-count/
NHSI Oversight Framework Metric List
Variation Type IconCommon CauseConcern (High)
Concern (Low)Improvement (H..
Improvement (L..Page 6
Section Metric Name Latest Period Target/Benchmark Target Source Performance Wigan
Outcome EI RTT June 2021 60% National KPI 78.0% N
Data Quality Maturity Index (DQMI) -MHSDS dataset score
March 2021 95% National KPI 97.0% N
IAPT Recovery ( CCG pathway target) June 2021 50% National KPI 46.6% N
IAPT - 6 Weeks RTT June 2021 75% National KPI 85.7% N
IAPT - 18 Weeks RTT June 2021 95% National KPI 98.1% N
Outcome Reportable OAPs Bed Nights June 2021 0 GM Q3 Target 559 N
Quality ofCare
Staff Friends and Family Test %recommended - care
September2020
NullServiceBenchmark
78.2% N
Mental health scores from Friends andFamily Test - % positive
June 2021 80% Local Target 83.2% N
CPA - Proportion of discharges followedup within seven days
June 2021 95% National KPI 96.9% N
% clients in settled accommodation March 2021 59% National KPI 79.2% N
% clients in employment March 2021 9% National KPI 8.8% N
Quality ofCare
Admissions to adult facilities of patientsunder 16 years old
June 2021 0 National KPI 0 N
Assurance IconNo Target/Not Enough Data Points
Capable
Not capable
Unreliable
A V
NHSI Oversight Framework Metric List
Variation Type IconCommon CauseConcern (High)
Concern (Low)Improvement (H..
Improvement (L..Page 7
Section Metric Name Latest Period Target/Benchm.. Target Source Performance Wigan
Quality ofCare
Written complaints - rate June 2021 0.0ServiceBenchmark
0.01 Y
Occurrence of any Never Event June 2021 0.0 National KPI 0.00 Y
Patient Safety Alerts not completed bydeadline
June 2021 0.0 National KPI Null Y
CQC community mental health survey March 2020 8.0 Local Target 7.30 N
Potential under-reporting of patientsafety incidents
April 2021 Null National KPI 41.50 N
LeadershipandWorkforce
Staff sickness June 2021 5.6% National KPI 6.6% Y
Staff turnover June 2021 12.5% Local Target 14.3% Y
Proportion of temporary staff June 2021 5.0% Local Target 14.5% Y
Rapid Tranquillisation - GMMH (W) Exec Owner: Gill Green
The number of recorded incidents in June remainsconsistent with recent months.
The Positive and Safe Team continue to provideongoing support where needed.
The use of rapid tranquillisation in June has alsoremained consistent with recent months.
Ongoing support is provided by the Positive andSafe team as and when required.
Page 14
July 2019
August 2019
September 2019
October 2019
November 2019
December 2019
January 2020
February 2020
March 2020
April 2020
May 2020
June 2020
July 2020
August 2020
September 2020
October 2020
November 2020
December 2020
January 2021
February 2021
March 2021
April 2021
May 2021
June 2021
60
80
100
LCL 43.77
UCL 104.1
Mean 73.96
Benchmark 85
Seclusion - GMMH (W) Exec Owner: Gill Green
Variation TypeCommon Cause
Safe - Seclusion and Deaths
June 2019
July 2019
August 2019
September 2019
October 2019
November 2019
December 2019
January 2020
February 2020
March 2020
April 2020
May 2020
June 2020
July 2020
August 2020
September 2020
October 2020
November 2020
December 2020
January 2021
February 2021
March 2021
April 2021
May 2021
50
100
150
LCL 44.46
UCL 125.9
Mean 85.17 Benchmark 93
Deaths - GMMH (W) Exec Owner: Gill Green
Seclusion figures in June are within the averagemonthly range.
Ongoing support is provided by the Positive andSafe team as and when required.
Please note the number of deaths is reported amonth in arrears.
The number of deaths recorded in May and theprevious months are showing as comparable withyears prior to the COVID19 pandemic and withinexpected parameters for the Trust.
Page 15
April 2020
May 2020
June 2020
July 2020
August
2020
Septembe
r 2020
October
2020
November
2020
December
2020
January
2021
February
2021
March
2021
April 2021
May 2021
June 2021
20.0%
40.0%
60.0%
80.0%
LCL 48.8%
UCL 77.7%
Mean 63.2%
Target 85.0%
Supervision completed in line with Trust policy - GMMH (W) Exec Owner: Gill Green
Variation TypeConcernImprovement
Safe - Supervision and Mandatory Training
July 2019
August 2019
September 2019
October 2019
November 2019
December 2019
January 2020
February 2020
March 2020
April 2020
May 2020
June 2020
July 2020
August 2020
September 2020
October 2020
November 2020
December 2020
January 2021
February 2021
March 2021
April 2021
May 2021
June 2021
80.0%
82.0%
84.0%
86.0%
88.0%
LCL 81.2%
UCL 87.6%
Mean 84.4%Target 85.0%
Mandatory Training - GMMH (W) Exec Owner: Andrew Maloney
The Trust's position on supervision complianceincreased to 77.4% in June. There has been asustained improvement in supervision compliancesince August 2020. Focused work is ongoingthrough the Improving Access and Quality ofSupervision Breakthrough Series Collaborative.
Following a pause in training during wave 1 ofCovid the Trust position continues to improve. Thisis the 7th consecutive month of performance abovetarget.
Page 16
July 2019
August 2019
September 2019
October 2019
November 2019
December 2019
January 2020
February 2020
March 2020
April 2020
May 2020
June 2020
July 2020
August 2020
September 2020
October 2020
November 2020
December 2020
January 2021
February 2021
March 2021
April 2021
May 2021
June 2021
50
100
LCL 18.82
UCL 111.3
Mean 65.08 Benchmark 62
Assaults on Staff - GMMH (W) Exec Owner: Gill Green
Variation TypeCommon Cause
Safe - Assaults on Staff
In June the number of violence and aggressionincidents resulting in harm to staff reduced to 62.There are no particular areas requiring furtherinvestigation at this stage.
Page 17
July 2019
August 2019
September 2019
October 2019
November 2019
December 2019
January 2020
February 2020
March 2020
April 2020
May 2020
June 2020
July 2020
August 2020
September 2020
October 2020
November 2020
December 2020
January 2021
February 2021
March 2021
April 2021
May 2021
June 2021
0
200
400
600
LCL -18.0
UCL 645.0
Target 0
Mean 313.5
Reportable OAPs Bed Nights - GMMH Exec Owner: Deborah Partington
Variation TypeCommon Cause
Concern
Improvement
Effective - Reportable OAPS Bed Nights and Independent Sector Contracted Beds
Reportable OAP bed nights showed an increase inmonth however the number of new placements didreduce which reflects the continued work with oursystem wide partners to develop alternatives fordischarge. The GMMH Healthier Patient PathwaysProject is also now in place. This work aims tosupport the reduction of OAPs by improving patientflow and supporting people as close to home aspossible.
The national target to reduce OAPs to zero is theend of Q2 2021/22. GMMH's ambition remains toreduce OAPs to zero as soon as possible and by Q3at the latest.
Please note the title of the chart has been updatedto ensure it accurately reflects the data included.The chart shows all OAPs placed locally, inclusive ofthe contracted beds which are part of the NorthWest Bed Bureau.
There has been a decrease in the occupied bednights in June. This is in part due to the shortermonth of June and also due to a decrease inindependent sector PICU bed nights used.Please note these figures do not include Wiganpatients in Independent Sector Contracted beds asfrom April 1st 21, these are reported in theAppendix.
Page 18
August 2019
October 2019
December 2019
February 2020
April 2020
June 2020
August 2020
October 2020
December 2020
February 2021
April 2021
June 2021
5.0..
10...
LCL 4.1%
UCL 10.7%
Mean 7.4%
Target 3.5%
Delayed Transfers of Care - GMMH - Adult of Working AgeExec Owner: Deborah Partington
August 2019
October 2019
December 2019
February 2020
April 2020
June 2020
August 2020
October 2020
December 2020
February 2021
April 2021
June 2021
10..
20..
30..
LCL 5.3%
UCL 23.9%
Mean 14.6%
Target 3.5%
Delayed Transfers of Care - GMMH - RehabExec Owner: Deborah Partington
August 2019
October 2019
December 2019
February 2020
April 2020
June 2020
August 2020
October 2020
December 2020
February 2021
April 2021
June 2021
4.0%
6.0%
8.0%
10...
12...
LCL 4.2%
UCL 9.3%
Mean 6.8%
Target 3.5%
Delayed Transfers of Care - GMMH - (All Trust DToCs)Exec Owner: Deborah Partington
Variation TypeConcernImprovement
Effective - Delayed Transfers of Care
August 2019
October 2019
December 2019
February 2020
April 2020
June 2020
August 2020
October 2020
December 2020
February 2021
April 2021
June 2021
5.0..
10...
15...
LCL 2.5%
UCL 16.1%
Mean 9.3%
Target 3.5%
Delayed Transfers of Care - GMMH - Older AdultExec Owner: Deborah Partington
The previous target of 7.5%has been updated to reflectthe current target for acuteTrusts of 3.5%. This is shownas a local benchmark forGMMH.There was an increase in allspeciality areas. This reflectspositive work with systempartners on a GreaterManchester project aimed atsupporting delivery of a zerodelayed discharge position.An initial increase isexpected. This work formspart of the GMMH HealthierPatient Pathways project.
The previous target of 7.5%has been updated to reflectthe current target for acuteTrusts of 3.5%. This is shownas a local benchmark forGMMH.There was an increase in anumber of divisions inrelation to access toresidential and nursing homeplacements. Work continueswith system partners on a GMproject aimed at supportingdelivery of zero delayeddischarges. An initial increaseis expected. This work formspart of the GMMH HealthierPatient Pathways project.
The previous target of 7.5%has been updated to reflectthe current target for acuteTrusts of 3.5%. This is shownas a local benchmark forGMMH.There was an increase in allspeciality areas. This reflectspositive work with systempartners on a GreaterManchester project aimed atsupporting delivery of a zerodelayed discharge position. Aninitial increase is expected.This work forms part of theGMMH Healthier PatientPathways project, aimed atimproving patient experienceby enhanced patient flow andreduced length of stay.
The previous target of 7.5%has been updated to reflectthe current target for acuteTrusts of 3.5%. This isshown as a local benchmarkfor GMMH.There was an increase in allspeciality areas. This reflectspositive work with systempartners on a GreaterManchester project aimed atsupporting delivery of a zerodelayed discharge position.An initial increase isexpected. This work is partof the GMMH HealthierPatient Pathways project,aimed at improving patientexperience by reducinglength of stay.
Effective - 4 Hour Breaches in A&E and Time to recruit
July 2019
August 2019
September 2019
October 2019
November 2019
December 2019
January 2020
February 2020
March 2020
April 2020
May 2020
June 2020
July 2020
August 2020
September 2020
October 2020
November 2020
December 2020
January 2021
February 2021
March 2021
April 2021
May 2021
June 2021
80
100
120
LCL 72.7
UCL 125.4
Mean 99.0Target 91
Time to recruit - GMMH (W) Exec Owner: Andrew Maloney
GMMH have maintained performance over the past12 months.
All mental health liaison teams are working withacute partners to deliver Emergency Departmentstreaming to mental health urgent care centres.Where this pathway is established there is clearcorrelation of improved performance and serviceuser experience. GMMH is working with partners toexplore options where the acute site estate remainschallenged to support this pathway.
The figures exclude newly qualified candidates andthose where commencement is delayed due tomaternity leave/long term sickness. The overalltime to hire with these groups included is 104 days.
Overall time to hire has increased due to the timetaken to undertake interviews. The time taken tocomplete pre-employment checks also increasedslightly due to the volume of candidates and rolesbeing recruited to. In addition there were 32 postsat band 7 or above with notice periods of 8 weeksor longer. This delays start dates and lengthenstime to recruit. Further additional resource iscontinuing to support the Recruitment Team on atemporary basis to assist with the volume ofrecruitment, and to support an NHSE/I project forrecruitment to Healthcare Support Worker roles.
Page 20
July 2019
August 2019
September 2019
October 2019
November 2019
December 2019
January 2020
February 2020
March 2020
April 2020
May 2020
June 2020
July 2020
August 2020
September 2020
October 2020
November 2020
December 2020
January 2021
February 2021
March 2021
April 2021
May 2021
June 2021
40
60
80
100
LCL 32.26
UCL 100.5
Mean 66.38Benchmark 74
Complaints - GMMH (W) Exec Owner: Gill Green
Variation TypeCommon Cause
Caring - Complaints and Pressure Ulcers
July 2019
August 2019
September 2019
October 2019
November 2019
December 2019
January 2020
February 2020
March 2020
April 2020
May 2020
June 2020
July 2020
August 2020
September 2020
October 2020
November 2020
December 2020
January 2021
February 2021
March 2021
April 2021
May 2021
June 2021
-2
0
2
4
LCL -1.96
UCL 4.29
Mean 1.17 Benchmark 1
Pressure Ulcers - GMMH (W) Exec Owner: Gill Green
The number of complaints recorded in Juneremained below the benchmark. The CustomerCare Team continues to triage an increasedproportion of initial enquiries as concerns ratherthan complaints.
There were no reported GMMH acquired pressureulcers in June.
Page 21
July 2019
August 2019
September 2019
October 2019
November 2019
December 2019
January 2020
February 2020
March 2020
April 2020
May 2020
June 2020
July 2020
August 2020
September 2020
October 2020
November 2020
December 2020
January 2021
February 2021
March 2021
April 2021
May 2021
June 2021
50
100
LCL 45.51
UCL 127.2
Mean 86.33 Benchmark 88
Falls - GMMH (W) Exec Owner: Gill Green
Variation TypeCommon CauseImprovement
Caring - Falls
The number of inpatient falls recorded in Juneremained below the mean.
Page 22
July 2019
August 2019
September 2019
October 2019
November 2019
December 2019
January 2020
February 2020
March 2020
April 2020
May 2020
June 2020
July 2020
August 2020
September 2020
October 2020
November 2020
December 2020
January 2021
February 2021
March 2021
April 2021
May 2021
June 2021
5.0%
6.0%
7.0%
LCL 5.1%
UCL 7.4%
Mean 6.2%
Target 5.6%
Staff sickness - GMMH (W) Exec Owner: Andrew Maloney
Variation TypeCommon CauseConcernImprovement
Well Led - Sickness and IG Training
July 2019
August 2019
September 2019
October 2019
November 2019
December 2019
January 2020
February 2020
March 2020
April 2020
May 2020
June 2020
July 2020
August 2020
September 2020
October 2020
November 2020
December 2020
January 2021
February 2021
March 2021
April 2021
May 2021
June 2021
92.0%
94.0%
96.0%
LCL 92.7%
UCL 95.7%
Mean 94.2%Target 95.0%
IG training compliance - GMMH (W) Exec Owner: Suzanne Robinson
Levels of sickness increased during June. This isthe first time absence has been above target sinceFebruary. This is due to an increase in short termabsence (from 1.57% to 2.45%).
Absence levels are higher than the same month inthe previous year (5.18% in June 2020). Whilstthere are monthly variances with long termabsence, the trend over 24 months is reducing.There has been an increase in absence due toCOVID and mental health related absence. TheTrust sickness level excluding COVID was 5.92%during June, which is an increase from 5.37% inMay.
HR Managers will review the position in more detailat a local level to ensure appropriate support plansare in place.
The Trust is required to maintain a level of 95%compliance for IG training, at any point during theyear.
The position at the end of June is below therequired target. Work is continually ongoing toidentify which staff need to complete their training.This is then brought to the attention of linemanagers to address.
Page 23
July 2019
August 2019
September 2019
October 2019
November 2019
December 2019
January 2020
February 2020
March 2020
April 2020
May 2020
June 2020
July 2020
August 2020
September 2020
October 2020
November 2020
December 2020
January 2021
February 2021
March 2021
April 2021
May 2021
June 2021
75.0%
80.0%
85.0%
LCL 73.2%
UCL 79.4%
Mean 76.3%
Target 85.0%
Appraisal Rate - GMMH (W) Exec Owner: Andrew Maloney
Variation TypeConcernImprovement
Well Led - Appraisal Rate and Bank and Agency Use
July 2019
August 2019
September 2019
October 2019
November 2019
December 2019
January 2020
February 2020
March 2020
April 2020
May 2020
June 2020
July 2020
August 2020
September 2020
October 2020
November 2020
December 2020
January 2021
February 2021
March 2021
April 2021
May 2021
June 2021
10.0%
12.0%
14.0%
16.0%
18.0%
LCL 9.5%
UCL 17.0%
Mean 13.3%
Bank and Agency Use - GMMH (W) Exec Owner: Suzanne Robinson
The Trust position on appraisal has improved fromOctober 20, and there continue to be steadyincreases across some services. It should be notedthat appraisals were put on hold as part of theCOVID response however have now resumed.
Agency costs are £81k overspent against plan.Agency nursing and support to clinical staff costsare impacting on this due to increased pressureswithin inpatient services.
There are 36.81wte vacancies across NHSinfrastructure Support roles. Engaging agency staffto cover these vacancies has resulted in a pressureof £161k to the end of month 3.
Bank costs are £214k overspent against plan. Themain area of pressure is on support to clinical staffdue to increased pressures within inpatient servicesand staff sickness rates.
The cost of temporary staff as a percentage of totalstaff costs is 14.19%. The percentage by staffnumber is reflective of the number of vacancieswithin the Trust, and the additional staff used tocover for staff affected by Covid. The percentagestaff cost is higher than staff numbers as a largeproportion of agency spend (46% of total) is onmedical locums.
Page 25
July 2019
August 2019
September 2019
October 2019
November 2019
December 2019
January 2020
February 2020
March 2020
April 2020
May 2020
June 2020
July 2020
August 2020
September 2020
October 2020
November 2020
December 2020
January 2021
February 2021
March 2021
April 2021
May 2021
June 2021
40.0%
60.0%
80.0%
100.0%
LCL 35.8%
UCL 100.0%
Mean 67.9%Target 60.0%
EI RTT - Division - GMMH Exec Owner: Deborah Partington
The target is 60% of new assessments to becompleted within 2 weeks of referral and careco-ordinator allocated.
The target was met in month by all divisions. As inprevious months reasons for breaches includeDNAs by service users and some delays in referralon to Early Intervention services from other Trustservices that did not meet the two week target.Services continue to reinforce the need for earlyreferral to EI services and are following up allservice users referred.
The reduction in performance from March - May20 was a direct result of the COVID 19 response.This reduced face to face assessments andincreased remote assessments which do not meetthe referral to treatment clock stop requirements.
The Division continues to report a compliantposition for access to services within 6 weeks ofreferral. Work continues across Manchester, inparticular North of the borough, to build upon theimprovements in accessibility to achieve the RTTtarget consistently.
GMMH achieved the 18-week target in month andare expected to continue this consistently. Thesuccess of the Manchester waiting list initiativesover the past year to improve accessibility has beena divisional focus. Attention is now focussed onsustaining access into the future.
It should be noted that the recovery target appliesto the whole IAPT pathway provided within adistrict. This includes Step 2 and Step 3 providers.GMMH provide both Step 2 and Step 3 services inBolton and Trafford which are monitored againstthe 50% recovery target. For Salford andManchester, GMMH provides Step 3 only servicesand whilst aiming to support as much recovery aspossible, 40-42% is considered a more realisticrecovery rate for Step 3 services to reflect thehigher level of complexity in clients at Step 3.
Recovery for June ended with 46.6%, a minorreduction from May. Work continues withinManchester to maintain an improving position inaccessibility which will have a positive impact uponfuture patient outcomes.
Page 27
August 2019
October 2019
December 2019
February 2020
April 2020
June 2020
August 2020
October 2020
December 2020
February 2021
April 2021
June 2021
0.0%
50.0%
100.0%
150.0%
LCL 12.0%
UCL 134.7%
Mean 73.4%Target 60.0%
EI RTT - Division - Bolton Exec Owner: Deborah Partington
Variation TypeCommon CauseConcern
Responsive - EI RTT - Divisions
August 2019
October 2019
December 2019
February 2020
April 2020
June 2020
August 2020
October 2020
December 2020
February 2021
April 2021
June 2021
60.0%
80.0%
100.0%
LCL 44.3%
UCL 102.4%
Mean 73.4%
Target 60.0%
EI RTT - Division - Salford Exec Owner: Deborah Partington
The target was met in month.
The reduction in performanceMarch to May 2020 was adirect result of the COVID 19response with a reduction inface to face assessments andan increase in remoteassessments. Face to facecontact is required to stopthe clock.
The target has been met thismonth. The additionalassessment rota remains inplace to support ongoingachievement.
The reduction inperformance from March2020 was a direct reflectionof the COVID 19 responsewith an increase in remoteassessments. Face to facecontact is required to stopthe clock when measuringreferral to treatment timesfor EI services.
August 2019
October 2019
December 2019
February 2020
April 2020
June 2020
August 2020
October 2020
December 2020
February 2021
April 2021
June 2021
0.0%
50.0%
100.0%
150.0%
LCL 0.2%
UCL 131.1%
Mean 65.6% Target 60.0%
EI RTT - Division - Trafford Exec Owner: Deborah Partington
The target has been met thismonth. The lower number ofassessments in Trafford doesmean there is fluctuation inachieving this target.
The reduction inperformance March - May2020 directly reflects COVID19 with the reduction in faceto face assessments andincrease in remoteassessments. Face to faceassessment is required tostop the clock for EI referralto treatment targets.
August 2019
October 2019
December 2019
February 2020
April 2020
June 2020
August 2020
October 2020
December 2020
February 2021
April 2021
June 2021
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%100.0%
LCL 33.4%
UCL 86.0%
Mean 59.7% Target 60.0%
EI RTT - Division - Manchester Exec Owner: Deborah Partington
The service met the target inmonth. The servicecontinues to encourage earlyreferral on from other Trustservices.
The reduction inperformance from March2020 was a direct result ofthe COVID 19 response.Remote assessmentscontinued however these didnot meet referral totreatment clock stoprequirements.
The service is achieving thetarget. No further action atthis time is required.
The Manchester service wasbelow target, achieving71.6%. This is attributed tothe discharges from longestwaiter initiative in Q42020/21 which are comingto completion of therapy.This is an expectedtemporary, short termimpact.
The chart shows consistentachievement of the targetby the service. No furtheraction required.
Abc
The chart shows consistentachievement of the target bythe service. No further actionrequired.
The service is maintainingthe previous significantimprovements in 18-weekaccessibility following aconcerted waiting listinitiative aimed at reductionof longest waiters fromOctober 2020.
Plans are in place to ensurefuture compliance canremain consistent, with thesupport of additionalinvestment.
Abc
The chart shows consistentachievement of the target.No further action requiredat this time.
The target has beenachieved in June. The teamhave identified areas forimprovement including areview of the currentpathway, system processesand procedures. The teamare also recruiting againstadditional investment. Areview of the skill mixrequirements has informedthis to ensure the servicecan best meet the localpopulation need.
It should be noted that thistarget applies to the wholeIAPT pathway providedwithin a division. Salfordprovide recovery figures inline with those expected fora Step 3 only service atbetween 40-42%. Step 2services contribute to theoverall CCG pathway targetin addition to the GMMHStep 3 service. Salfordachieved 40.6% recovery inmonth.
This is a target for the wholeIAPT pathway in a division.Manchester services providesrecovery figures in line withthose expected for a Step 3only service at between40-42%. Step 2 alsocontributes to the CCGoverall pathway target.Manchester continue toshow a sustained overallimprovement. This reflectswork to reduce waiting timesresulting in improvedoutcomes. Work is focusedon ensuring the expectedtarget for Step 3 isconsistently met.
The target has beenachieved. No further actionsrequired at this time.
Page 31
May 2019
June 2019
July 2019
August 2019
September 2019
October 2019
November 2019
December 2019
January 2020
February 2020
March 2020
April 2020
May 2020
June 2020
July 2020
August 2020
September 2020
October 2020
November 2020
December 2020
January 2021
February 2021
March 2021
April 2021
10.00
20.00
LCL 1.41
UCL 15.56
Mean 8.48Target 6.00
CAMHS - Waiting Time (Weeks) - Referral to First Appointment Exec Owner:Deborah Partington
Variation TypeCommon CauseConcernImprovement
Responsive - CAMHS Waiting Times (Weeks) - Referral to First Appointment and Second to Third A..
May 2019
June 2019
July 2019
August 2019
September 2019
October 2019
November 2019
December 2019
January 2020
February 2020
March 2020
April 2020
May 2020
June 2020
July 2020
August 2020
September 2020
October 2020
November 2020
December 2020
January 2021
February 2021
March 2021
April 2021
0.00
10.00
20.00
LCL -2.04
UCL 16.51
Mean 7.23
CAMHS - Waiting Time (Weeks) - Second to Third Appointment Exec Owner:Deborah Partington
There continues to be an increase in referrals tothe service which has impacted on waiting timesfrom referral to first appointment. In additionthere is also a residual fluctuation in waiting timesdue to the transfer to Paris in December 2020.
The service continues to maintain robust oversightof capacity and demand with provision of additionalcapacity (including out of hours working). Themulti-agency referral hub pilot is in progress andshould have a positive impact on the amount ofreferrals accepted. A proportion of referrals arenow being directed towards the appropriateTHRIVE partners.
There has been a slight increase in waiting timesfor second to third appointment.
As noted above, there is likely to be some ongoingfluctuation in this and the other referral totreatment measures due to the impact of thetransfer to Paris.
Page 32
July 2019
August 2019
September 2019
October 2019
November 2019
December 2019
January 2020
February 2020
March 2020
April 2020
May 2020
June 2020
July 2020
August 2020
September 2020
October 2020
November 2020
December 2020
January 2021
February 2021
March 2021
April 2021
May 2021
June 2021
80.0%
90.0%
100.0%
110.0%
LCL 75.6%
UCL 106.4%
Mean 91.0%
Target 100.0%
H&J - CPA annual health check Exec Owner:Deborah Partington
Variation TypeCommon Cause
Responsive - Health & Justice - CPA Annual Health check and 13 Week Review
88% of CPA annual health checks took place inJune as some residents declined their health check.These have now been seen.
All sites reported 100% compliance on 13 weeksubstance misues reviews.
Page 33
July 2019
August 2019
September 2019
October 2019
November 2019
December 2019
January 2020
February 2020
March 2020
April 2020
May 2020
June 2020
July 2020
August 2020
September 2020
October 2020
November 2020
December 2020
January 2021
February 2021
March 2021
April 2021
May 2021
June 2021
70.0%
80.0%
90.0%
100.0%
LCL 85.6%
UCL 101.5%
Mean 93.5%
Target 100.0%
H&J - Alcohol screening on reception Exec Owner:Deborah Partington
Variation TypeConcernImprovement
Responsive - Health & Justice - Alcohol Screening and GP Wait
July 2020 Augus..Septem..Octobe..Novemb..Decemb..Januar..Februar.. Marc.. Apri.. Ma.. Jun..
10
15
20
LCL 923.3%
UCL 1395.3%
Mean 11.6
Target 21
UCL 13.95
Target 21.0
H&J - GP wait for routine care Exec Owner:Deborah Partington
Compliance in June was 100% for alcoholscreening on reception
At all sites, the waiting time for GP care was lessthan 21 days in June.
Page 34
Division
2018-06
2018-09
2018-12
2019-03
2019-06
2019-09
2019-10
2019-11
2019-12
2020-01
2020-02
2020-03
2020-04
2020-05
2020-06
2020-08
2020-09
2020-10
2020-11
2020-12
2021-01
2021-02
2021-03
2021-04
Bolton
Bury
Cumbria
Lancashire
Salford
Trafford 8.3%
8.4%
4.2%
4.6%
4.5%
8.8%
8.4%
4.9%
4.6%
5.0%
9.5%
7.8%
5.1%
4.9%
5.0%
10.2%
8.7%
5.1%
4.5%
4.7%
10.5%
8.6%
5.4%
4.7%
4.3%
11.0%
8.4%
6.0%
4.5%
5.1%
10.6%
8.5%
5.8%
4.8%
4.6%
10.6%
8.2%
5.8%
5.0%
4.3%
11.1%
7.9%
5.6%
4.6%
3.6%
10.9%
9.1%
6.4%
4.9%
3.8%
11.8%
9.6%
6.9%
5.7%
3.9%
12.7%
10.5%
6.8%
5.5%
3.8%
11.8%
10.6%
6.7%
6.2%
4.1%
11.5%
10.7%
6.3%
6.5%
4.3%
9.7%
10.4%
6.7%
7.1%
4.5%
9.5%
10.4%
6.1%
6.4%
4.2%
9.2%
10.0%
6.3%
7.3%
4.2%
9.7%
10.3%
5.8%
6.4%
3.7%
10.2%
10.8%
5.1%
3.3%
9.2%
10.6%
4.7%
3.3%
9.4%
11.0%
4.9%
3.0%
8.7%
11.0%
6.9%
4.9%
3.0%
6.1%
10.9%
6.9%
4.7%
3.2%
SMS services - Successful completions of opiate users - All Exec Owner: Deborah Partington
Responsive - SMS Successful Completions
These figures are reported 3 months in arrears to allow for partnership figures to be reflected. Successful completion percentages are generated nationally via an algorithm that is based on clusters ofdeprivation. There are 23 Local Authorities in the North West. The April data shows Bolton, Cumbria and Trafford all slightly reduced percentages but with Trafford remaining green. Bury and Salford havestayed the same. Salford remains green. The treatment of opiate users during the pandemic continues to focus on harm reduction, retention and engagement, thus impacting on service users beingdischarged from the treatment system. This is fully supported by local commissioners and Public Health England and has been reflected in the new, universal funding allocation for 2021-22 which has aspecific focus on harm reduction interventions.
Rest of GMMH Performance 17.78Combined Performance 6 11.61
The target was not achieved in month by Wigan with 6 breaches. The target was achieved by the Trust overall.
There were no U16 admissions to adult facilities.
The target has been refreshed to reflect the target used for acute Trusts of 3.5%. This will be used as a local benchmark for GMMH services. This was achieved in month by Wigan however not Trustwide.
This measure was not previously reported by NWB. Steps are in place to develop new Standard Operating Procedures for the service that should enable the development of this reporting.
There were 120 Independent Sector Contracted bednights used in June.
Please note the Wigan figures are local service reported access times rather than MHSDS reported figures. The change in the provider code (from North West Boroughs to GMMH) in April 21 means that there are significant DQ issues with MHSDS reported access times for Wigan. This reflects the position when Bolton CAMHS transferred to GMMH. Appointments for patients that have been seen whilst under the care of NWBH are not being reported by MHSDS hence showing as long waiters and skewing data. This will continue until the patient has been seen appointments recorded on Paris by GMMH and submitted under the GMMH provider code. A note has been placed on the data by NHS Digital to note the impact of the change in provider code on the quality of data. Plans will be put in place by the service to monitor the impact of this. Local service access times in June were reported as 2.86 weeks and within target.
CAMHS Referral to First Appt.
The target was achieved in month by Wigan and Trustwide.
The target was achieved in month by Wigan and Trustwide.
The target was achieved in month by Wigan and Trustwide.
The target was achieved in month by Wigan and Trustwide.
There were no reportable OAP bednights used by Wigan in month.
U16 Admissions
DToC
A&E 4 Hour
Independent Sector
Contracted Bednights
Out
com
eQ
ualit
y of
Car
eEf
fect
ive
EI RTT
IAPT Recovery
IAPT 18 Weeks
IAPT 6 Weeks
Reportable OAP Bednights
CPA 7 Day Follow Up
Wigan Performance 5.43 2.86 3.86Rest of GMMH Performance 4.76Combined Performance N/A 5.10Wigan Performance 83.3% 100.0% 100.0%Rest of GMMH Performance
The Wigan figures are local service reported access times. Pleaes see above comment.
There has been a significant increase in referrals to which has impacted on response times. The staffing model has been reviewed and contracts for staff employed on fixed term contracts have been extended to March 2022 to support the increase in demand. NHSP have also been approached for 3 additional staff to support the team over the coming weeks.
There is currently 1 CYP waiting outside of the target and has an appointment on 27th July.
CAMHS Second to Third Appt.
CYP ED Routine Completed
Within 4 Weeks
CYP ED Urgent Completed
Within 1 Week
Resp
onsi
ve
1
Board of Directors – Part 1
TITLE OF REPORT: Trust Strategy Update DATE OF MEETING: 26 July 2021 AGENDA ITEM: 10 PRESENTED BY: Elizabeth Calder, Director of Performance and Strategic Development AUTHOR(S): Mary Lee, Associate Director of Performance and Strategic Development
REPORT SUMMARY: The Trust Strategy 2019 – 2024 takes forward the Trust’s vision of working with
service users and carers to have improved lives and optimistic futures with a clear focus on delivering excellent care and supporting wellbeing. The strategy set out five strategic objectives based on the Trust values:
Best Care Every Day - Work with service users and carers to achieve their goals by delivering high quality care and excellent outcomes. Compassionate, supported, motivated staff - Create an outstanding place to work, ensuring staff feel valued and are supported to reach their potential. Best outcomes - Continuously improve services for users through Research, Innovation and Digital Technology. Person-centred, seamless services - Work in partnership with others to improve wellbeing and challenge stigma. Sustainable services, adding value - Be a sustainable, well-governed organisation that delivers social value.
This paper provides an update on progress with implementing the strategy, following the last update to the Board of Directors in November 2020. The update gives an overview of work that has been undertaken by strategic objective in the context of a further Covid-19 national lockdown. The Trust’s priorities for the year ahead to take forward the Trust’s Strategy were set out in the Annual Plan 2021/22 agreed by the Board of Directors in June 2021. The Trust’s Strategy has been further developed through key supporting strategies set out in the report. The update sets out how implementation of the Trust’s priorities for 2021/22 and supporting strategies will be overseen and proposes that each of the support strategies will be discussed at the Board of Directors throughout
2
the year. This is in addition to the update on progress with the Annual Plan 2021/22 in Autumn 2021.
A further update of the overall Trust Strategy will be undertaken for 2022/23, taking into account Covid-19, progress with developing and implementing key trust supporting strategies and the implementation of the White Paper.
THIS REPORT SUPPORTS ACHIEVEMENT OF THE FOLLOWING STRATEGIC OBJECTIVES: Objective 1 – Work with service users and carers to achieve their goals by delivering high quality care
√
Objective 2 – Create an outstanding place to work, ensuring staff feel valued and are supported to reach their potential
√
Objective 3 – Continuously improve services for users through research, innovation and digital technology
√
Objective 4 – Work in partnership with others to improve wellbeing and challenge stigma
√
Objective 5 – Be a sustainable, well-led organisation that delivers social value
√
REPORT CONSIDERED AT THE FOLLOWING COMMITTEES/SUB-GROUPS: Committee/Sub-Group: Date: Audit Committee Quality Improvement Committee Charitable Funds Committee Remuneration & Terms of Service Committee Council of Governors Executive Management Team 14 July 2021
THIS REPORT PROVIDES ASSURANCE AGAINST A RISK ON THE BOARD ASSURANCE FRAMEWORK (BAF):
No
If ‘yes’:
DATIX ID Strategic Objective Description (as per BAF)
PURPOSE OF REPORT – Please check all relevant boxes
Information
√ Assurance Approval/Decision
3
RECOMMENDATIONS: The Board of Directors is asked to:
• Consider the Trust Strategy progress update report and the achievements since the last update to Board in November 2020.
• Note the priorities for taking forward the Trust Strategy in 2021/22 set out in the Annual Plan 2021/22 and supporting strategies.
• Note the proposed update on the priorities in the Annual Plan 2021/22 in Autumn 2021 and proposal for the development/implementation of key supporting strategies to be discussed at the Board of Directors through the year.
Trust Strategy 2019 – 2024 - Progress Update
1. Introduction The Trust Strategy 2019 – 2024 takes forward the Trust’s vision of working with service users and carers to have improved lives and optimistic futures with a clear focus on delivering excellent care and supporting wellbeing. The strategy set out five strategic objectives based on the Trust values: Best Care Every Day - Work with service users and carers to achieve their goals by delivering high quality care and excellent outcomes. Compassionate, supported, motivated staff - Create an outstanding place to work, ensuring staff feel valued and are supported to reach their potential. Best outcomes - Continuously improve services for users through Research, Innovation and Digital Technology. Person-centred, seamless services - Work in partnership with others to improve wellbeing and challenge stigma. Sustainable services, adding value - Be a sustainable, well-governed organisation that delivers social value.
In November 2020, the Board of Directors received an update report providing an overview of progress against each of the five strategic objectives. The report acknowledged, due to the impact of the pandemic and the suspension of many business as usual requirements, the anticipated reporting schedule for the Trust Strategy for the first half of 2020/21 was replaced by regular monthly reports to the Board of Directors on the Trust response to Covid-19 describing the Trust priorities and focus of work throughout the pandemic. The strategy update report in November commenced the formal strategy reporting schedule and provided an overview of progress and work completed by the Trust over the period March 2020 to September 2020. This report now provides a further update to members of the Board on progress against each of the five strategic objectives over the period since the last Board update.
2. Achievements against each Strategic Objective
A review of our achievements against the priorities we said we would achieve in the latter 6 months of 2020/21 needs to be considered in the context of the ongoing impact of Covid. Our plans to move our attention back to our original strategic priorities were superseded as the country faced a further wave of Covid and a further period of lockdown. It was important that the trust remained focused on meeting both the demands of the pandemic and also the increased mental health demands as a consequence.
Despite the challenges of the pandemic, and as part of our Covid-19 response, the Trust delivered a number of significant achievements to contribute to the Trust’s strategic objectives and these achievements are summarized in Table 1 below:
Table 1 - Key Achievements against each Strategic Objective – October 2021 onwards
Objective Progress Best Care Every Day
• Recommenced phase 2 of Quality Improvement (QI) Strategy including the establishment of a dedicated QI team and expert posts to lead QI programmes.
• Reviewed and improved the Quarterly Board Quality Report • Rolled out our Quality of Care programme to support the development of a clinical
quality assurance system • Further enhanced the GMMH crisis offer including expanding the crisis helpline
offering enhanced 24/7 help and support linked to the GM CAS & 111 service and the establishment of urgent care centres, crisis cafés and crisis beds.
• Expansion of the community mental health offer including introduction of seven day working across Community Mental Health Teams (CMHTs) and increase of the IAPT workforce, in addition to enabling both a digital response and continuing face to face contact during the pandemic to ensure core clinical services continued to operate.
• Continued the focused work on patient flow which included the implementation of a Surge Policy to support bed management and the development of the Healthier Patient Pathways improvement programme.
• Expanded the GMMH Homelessness offer to support the MH homeless team with drug and alcohol dependence and established a core MDT Homeless Team in Salford.
• Completed a comprehensive review of community models for our adult eating disorder services and ADHD services. This review has supported the development of 7 business cases across our localities (of which 4 are approved and 3 are under discussion with commissioners) and agreed support for the implementation of a waiting list initiative for ADHD.
Compassionate, supported, motivated staff
• Agreed a new trust People Plan for 2021/22 approved by the Board of Directors. • Drafted a new Leadership Strategy based on principles of compassion and collective
leadership • Revised and launched a new appraisal framework with fundamental objectives for
everyone on Equality Diversity and Inclusion. • Implemented ESR Establishment Control across the Trust. • Increased wellbeing of staff demonstrated by the reduced number of days lost due to
sickness. • Increased opportunities for organisational learning through revising our approach on
how we mange staff misconduct using just and learning principles as a foundation for decision making.
• Supported the transfer of approx. 800 staff from North West Boroughs into GMMH.
Best Outcomes
• Agreed a 3-year Research and Innovation Strategy aligned with GMMH strategy. • Engaged in specific research trials relating to the impact of the pandemic upon service
users. This has included SMI, IAPT, CAMHS, CMHTs, SMS, Perinatal and Inpatient services.
• Launched the EDI Research Group with Professor Dame Edge as lead. • Supported our workforce to become digitally enabled with full rollout of Teams and IT
equipment. • Completed the migration of Bolton CAMHS to Paris. • Completed the roll out of MaSt across CMHTs. • Designed and implemented a new Trust intranet and SharePoint site. • Increased the use of the booking functionality on teams which has been rolled out
across all relevant outpatient/community type services resulting in significant increase in the numbers of virtual consultations.
• Promoted the use of the GM Shared Care Record across the Trust resulting in increased usage.
• Implemented a new integration solution to enable improved connectivity between systems.
• Negotiated and established a new SLA arrangement with Mersey Care for Wigan Services.
• Implemented a new bed flow solution to replace IPFM. • Gained re-accreditation of Cyber Essentials+. • Negotiated a new Civica contract agreed December 2020.
Individualised Seamless Services
• Recruited service users to join programme groups for service developments at Park House redevelopment.
• Completed an evaluation of Manchester Wellbeing Fund with future options being considered.
• Played a key role in the GM COVID-19 integrated care partnerships arrangements and the GM COVID-19 system response.
• Completed the Full Business Case (FBC) and statutory transaction to formally transfer services from North West Boroughs to GMMH from 1st April with a clear Post Transaction Implementation Plan (PTIP) in place identifying key service priorities.
• Established our role as a system partner in Wigan. • Completed the FBC for the Provider Collaborative for Adult Secure Service. The FBC was
approved by GMMH Board of Directors and the NHSE and GMHSCP approval panel for go live from 1st October 2021.
• Worked collaboratively with partners to agree the clinical model for the Provider Collaborative and established a North West Network of Provider Collaboratives to share best practice and work with NHSE on cross cutting issues.
Sustainable Services, Adding Value
• Agreed a Financial Sustainability Plan for 21/22. • Supported the development of the FBCs for the Provider Collaborative and Park House. • Developed a financial separation plan for Wigan services from North West Boroughs. • Implemented new Financial Engagement Strategy including delivery of efficiencies. • Maintained cash balances to support working capital, delivered Cost Improvement Plans
and implemented financial tracking system to identify Covid spend. • Completed the alignment of ESR and finance systems. • Completed the Strategic Outline Case and Outline Business Case for Park House gaining
approval to proceed to FBC. • EPMA business case agreed and approved internally. • Completed a desktop review of Edenfield accommodation to support redevelopment
plans. • Established Urgent Care Centres across key localities. • Development of schemes to eliminate dormitory provision in South Manchester. • Undertook commercial review of all Estates and Facilities SLA’s. • Commenced scoping of metric around social value including workforce and procurement
information.
3. Looking Forward – 2021/22 The Trust’s priorities for the year ahead to take forward the Trust’s Strategy were set out in the Annual Plan 2021/22 agreed by the Board of Directors in June 2021. These priorities have been considered in the context of the impact of Covid-19, the national guidance that has been issued to date, the implications of the White Paper ‘Integration and Innovation: working together to improve health and social care for all’ and the partnership work underway across Greater Manchester and our localities. The Trust’s Strategy has been further developed through key supporting strategies set out in Table 2 below. The Strategic Development Group will continue to oversee the implementation of the Trust Strategy internally and review delivery of the supporting strategies. It is proposed to bring each of the support strategies to the Board of Directors throughout the year for a more detailed discussion and review. This is in addition to the update on progress with the Annual Plan 2021/22 in Autumn 2021. A further update of the overall Trust Strategy will be undertaken for 2022/23, taking into account Covid-19, progress with developing and implementing key trust supporting strategies and the implementation of the White Paper.
Table 2 - Key Supporting Strategies
Best Care QI Strategy – Year 2 Transformation Programmes – Community Teams Transformation, Healthier Patient Pathways, Responding to Crisis for Adults
Supported Workforce
GMMH People Plan
Best Outcomes Research and Innovation Strategy Digital Strategy refresh Equality, Diversity and Inclusion Strategy*
Individualised, seamless care
Implementing the White Paper Developing Provider Collaboratives, including Lead Provider for Greater Manchester Adult Secure Services GMMH Housing Strategy
Sustainable services, adding value
Finance Strategy Estates Strategy*, Park House Productivity Social Value*
*In development
4. Conclusion and Recommendation
The Board of Directors is asked to: • Consider the Trust Strategy progress update report and the achievements since the last update to Board
in November 2020. • Note the priorities for taking forward the Trust Strategy in 2021/22 set out in the Annual Plan 2021/22
and supporting strategies. • Note the proposed update on the priorities in the Annual Plan 2021/22 in Autumn 2021 and proposal
for the development/implementation of key supporting strategies to be discussed at the Board of Directors through the year.
1
Board of Directors – Part 1
TITLE OF REPORT: Quality Improvement Committee
11.01 Minutes of the Meeting held on 10 June 2021 (Ratified)
11.02 Committee Chair’s Assurance Report on the Meeting held 08 July 2021
DATE OF MEETING: Monday 26 July 2021
AGENDA ITEM: 11
PRESENTED BY: Julie Jarman, Non-Executive Director and Committee Chair
AUTHOR(S): Rachel Wedge, Nursing, Governance and Risk Admin. Team Manager
REPORT SUMMARY: The Board of Directors are asked to note the ratified minutes of the Quality
Improvement Committee held on 10 June 2021 and the Committee Chair’s Assurance
Report from the Quality Improvement Committee on the meeting held on 08 July
2021.
THIS REPORT SUPPORTS ACHIEVEMENT OF THE FOLLOWING STRATEGIC OBJECTIVES:
Objective 1 – Work with service users and carers to achieve their goals by delivering high quality care x
Objective 2 – Create an outstanding place to work, ensuring staff feel valued and are supported to
reach their potential
Objective 3 – Continuously improve services for users through research, innovation and digital
technology
Objective 4 – Work in partnership with others to improve wellbeing and challenge stigma
Objective 5 – Be a sustainable, well-led organisation that delivers social value x
REPORT CONSIDERED AT THE FOLLOWING COMMITTEES/SUB-GROUPS:
Committee/Sub-Group: Date:
Audit Committee -
Quality Improvement Committee
Charitable Funds Committee -
Remuneration & Terms of Service Committee -
Council of Governors -
2
Executive Management Team -
LEGAL IMPLICATIONS: None identified
REGULATORY
IMPLICATIONS (CQC/NHSEI):
None identified
THIS REPORT PROVIDES ASSURANCE AGAINST A RISK ON THE BOARD ASSURANCE FRAMEWORK (BAF):
No
If ‘yes’:
RISK ID Strategic Objective Description (as per BAF)
PURPOSE OF REPORT – Please tick all relevant boxes
Information
x Assurance x Approval/Decision
RECOMMENDATIONS: The Board of Directors are asked to review and note the minutes from the meeting
held on 10 June 2021 and the Chair’s report from the meeting held on 08 July 2021
2021.
1
Thursday 10 June 2021
Virtual via Microsoft Teams 9.30am until 12:00am
RATIFIED Chair Julie Jarman Non- Executive Director Corporate Dr Alice Seabourne Medical Director Corporate Gill Green Director of Nursing and Governance Corporate Deborah Partington Director of Operations Corporate Jane Wilson Director of Pharmacy Pharmacy Clair Carson Associate Director of Nursing and Governance Nursing and Governance John Walker Associate Director of Operations Operations Caroline Cain Associate Director of Operations Wigan Tony Morrison Associate Director of Research and Innovation Research and Innovation Bridget Hughes Head of Operations Central & Citywide Caroline Cain Head of Operations Wigan Kate Hall Head of Operations SMS Karen Morley Head of Operations H&J Matt Patterson Head of Operations AFS Dr Sandeep Mathews Consultant AFS Dr Neeti Singh Consultant Rehab Dr Rosie Clarke Consultant Manchester Central Dr Kishen Neelam Consultant Bolton Dr Parveen Sharma Consultant Wigan Helen Cutts CMHT Transformation Lead Trustwide Patrick Cahoon Head of Quality Improvement Nursing and Governance Christine Diamond Head of Mental Health Act Legislation Nursing and Governance Tom Woodcock Strategic Lead for Community Asset Nursing and Governance Zoe Dent Head of Operations North Manchester Kathleen Inglott Consultant AFS
2
1. Apologies
Apologies were noted from: Deborah Partington, Helen Dabbs, Paula Solomon, Chris Dale, Dale Huey, Emma Nazurally
2. Minutes of Previous Meeting
The minutes from the previous Quality Improvement Committee held on Thursday 10 June 2021 were agreed as an accurate record. The outstanding actions were discussed and the action log updated.
3. Matters Arising All matters arising are covered within the agenda
4. Conflicts of Interest No conflicts of interested were declared at the Committee.
5. Annual Quality Report The Committee noted the Annual Quality Report. The report describes the progress on quality improvement across GMMH and celebrates the breadth of activity that has been undertaken over the last year. The report also highlights efforts to strengthen our overall approach to quality, including our steps to rapidly progress our improvement capability, through delivery of the phase one GMMH QI strategy. There is a wide range of ongoing QI and assurance initiatives taking place across the Trust. These include the QI programmes and collaboratives, clinical audit and effectiveness, the new Quality of Care programme and learning from incidents. The Committee will receive regular updates. A varied and comprehensive range of reports was received at Quality Improvement Committee throughout the course of 2020/21. These reports reflect the extensive breadth of the developing total quality system across GMMH and the subsequent assurance that this provides. Approximately 350 members of GMMH staff have participated in QI training across a wide range of areas ranging from our beginner’s guide and measurement, Lean in healthcare and appreciative enquiry training, through to human factors, improvement practitioner and measurement masterclass training. Following discussions, the following actions were agreed
• For the Annual Quality Report to be shared with the Audit committee for consideration at their Committee meeting.
6. Board Assurance Framework (BAF)
The Committee approved the Board Assurance Framework (BAF). The Committee approved the Board
Assurance Framework. The 3 risks aligned to QIC for review are:
• S01/01 Safe Staffing (2252)
• SO1/02 Physical Heath (2816)
• SO1/03 Positive and Safe (2817)
3
The risks have been reviewed to reflect the current status and measures in place during the pandemic.
Timescales have been reviewed to reflect the current stage of the pandemic and in particular the
additional national guidance issued for IPC.
Safe Staffing has been regularly reported as per the restart of national reporting and the quarterly
reports to the Committee on Safe Staffing have included the additional measures in place to maintain
safety of both service users and staff during the pandemic. Notable is the commencement of the major
project of Healthier Patient Pathways in May 2021 in the acute bed bases of GMMH.
Discussions were held on safe staffing within the community teams. It was advised that any concerns
regarding safe staffing within the community teams needs to be discussed at local SLT’s and added to
their local risk register and discussed at the Risk Management Committee. A plan on a page on how to
report such risks in Datix with be shared with members.
Following discussions, the following actions were agreed
• For SLT’s to discuss safe staffing with the community teams and where issues identified this to be added to the local risk register
7. Community Transformation Programme update & Healthier Patient Pathway update
Community Transformation Programme update
The Committee noted the Community Transformation Highlight Report. The report outlines the
workstream objectives for year one, key developments within May, which include:
• A new GM governance structure has been implemented. Key to this are enabling groups such as
the West Change Leadership Group which brings together a small number of key representatives
alongside the Core Team to ensure there is collaboration, a shared understanding of the vision
and a high degree of standardisation alongside some ability for a flexible locality offer. These
enabling sessions are facilitated by the Innovation Unit.
• Regular meetings have been set up with the East Sector to ensure that both East and West are
aligned
• The first GM and GMMH Physical Health SMI ODG has been held which has outlined the
expectations for year 1 in supporting those on GP SMI registers to access annual; health checks,
vaccinations and support for healthier lifestyles.
• Work continues on GMMH branding and a digital strategy. The workforce strategy is complete.
• A locality planning meeting has been set with Wigan and support given to the SLT to begin the
setting up of Wigan programme, starting with attendance at the Wigan Activation Board. SMS
integration agenda into the core offer has been built into the implementation plan across all
localities.
The report also outlines key activities that are planned for June, this included the recruitment of an 8A
Operational Development post to lead on the locality planning and programme development. An
update will be provided to the Committee in June
Discussions were held regarding peer workforce across the Trust, Claire Watson to be invited to the next
QIC.
Following discussions, the following action was agreed
• Claire Watson to be invited to QIC in June to update the Committee on Peer Workforce across the Trust
4
Healthier Pathways update
The Committee received an update on the Healthier Patient Pathways Transformation Programme. The
programme commenced on 7 June and will run until 10 October. The aims are to :
• Improve patient experience
• Improve staff well being
• Create a sustainable flow
• Reduce the length of stay
A provisional timeline has been created for each division to take part in The Perfect Week, which will also
include Wigan services. Bolton will be the first to participate starting week commencing 21 June followed
by Salford.
Updates will be provided to QIC in accordance with project outcomes.
The Committee discussed how the Later Life services could be included. It was agreed that Later Life
services workstream will be discussed separately.
8. Mental Health Act Annual Report – 1 January 2020 to 31 March 2021 The Committee approved the Mental Health Act Annual Report. The report offers an overview of activity for both the calendar year, 1 January to 31 December 2020 and the financial year, 1 April 2020 to 31 March 2021 and provides comparative data against MHA activity in 2019 where appropriate. This will allow future reports to be aligned to the financial, rather than calendar year. Highlights from the report include:
• There was a 14% decrease in formal admissions under Part II of the MHA from 1 January to 31 December 2020 when compared with 2019. When the period between 1 April 2020 and 31 March 2021 is compared to 2019, this shows an 11% decrease in formal admissions.
• In 2020 there were 1444 admissions under s.2, which is a 18% increase against 2019. There were 237 admissions under s.3 during this period, which is significant decrease of 57% in comparison to 2019. A further 24% increase in s.2 admissions is also noted when comparing data for 1 April 2020 to 31 March 2021 to 2019.
• During the calendar year 2020, 65% of those detained under s.2 were from a white background and 29% were from an ethnic background. In terms of detentions under s.3, 70% of those detained were from a white background and 27% were from an ethnic background. Information in respect of ethnicity was missing from 6% of s.2 records and 3% of s.3 records
• There was an overall 38% increase in the use of s.5 Holding Powers across the Trust between 1 January and 31 December 2020. This trend continued across the period between 1 April 2020 and 31 March 2021, with a 39% increase when compared with 2019
• There was a 20% increase in the use of s.136 during the 2020 calendar year in comparison with 2019. The period between 1 April 2020 and 31 March 2021 saw a further 5% increase when compared with the data for 2020.
5
• 63% of detentions under s.136 resulted in discharge between 1 January and 31 December 2020, with 37% resulting in admission to hospital. 27% of those requiring admission were admitted under a section of the MHA, which is an increase of 4% against 2019.
Following discussions, the following actions were agreed
• The Quality Improvement Team to support with a QI project and look at the issues
• It was also agreed that the use of S136 needs to be re-visited, a meeting will be arranged with the appropriate professionals involved
9. MHA CQC Thematic Review The Committee received a presentation on the MHA CQC thematic review. This presentation outlines key themes arising from the CQC Mental Health Act Monitoring Visits and the ensuing Provider Action Statements from 1 January 2020 to 31 March 2021. The CQC announced that it would be stopping routine inspections of services during the Coronavirus pandemic from 16 March 2020 and introduced a new remote method of review from mid-April 2020 as a result of the pandemic. The revised CQC review process takes place remotely and includes the reviewer gathering information and speaking with ward managers, advocacy, staff, patients and their families via phone or other virtual methods. A letter to summarise the review is then sent to the service and outlines further actions as required. Between 1 January 2020 and 31 March 2021, the CQC undertook 26 Mental Health Act monitoring visits, with 20 of these taking place in 2020 and 6 in 2021. This is a significant reduction in comparison to the 34 reviews undertaken in 2019 alone. Of the reviews, 20 were under the new, remote arrangements whilst 6 had taken place between January and early March 2020 under previous inspection arrangements. Feedback following the visits include:
• Objective reports from CQC unannounced MHA reviews provide valuable compliance assurance
• Planned CQC remote reviews allow for rich feedback from service users, carers and IMHAs
• Provision of earlier CQC reports and PAS’ ahead of remote inspections has facilitated review of actions and focus on key areas,
• Staff feedback - remote inspections have been useful and positive
• Sustainability review in MHAQI allows for cross-service discussion and spread of innovative solutions
10. LeDer Policy Summary The Committee noted the LeDer Policy Summary. In March 2021 NHSE published the ‘learning from Lives
and deaths - people with a learning Disability and autistic people’ (LeDeR policy 2021)
LeDeR is a service improvement programme which aims to improve care, reduce health inequalities, and
prevent premature mortality of people with a learning disability and autistic people by reviewing
information about the health and social care support people received.
6
The policy has been co-produced with bereaved family members, people with a learning disability, health
and social care professionals and people from across the LeDeR workforce and sets out for the first time
for the NHS, the core aims and values of the LeDeR programme and the expectations of different parts of
the health and social care system in delivering the programme from June 2021.
The policy highlights clear staffing structures and roles and responsibilities for the implementation of LeDer
teams with a timeline that these are introduced by Integrated Care systems by 1 April 2022.
Following discussions, it was agreed
• A QI piece of work to be undertaken in relation to the recording of LD diagnosis, this will involve the LD Teams supporting with the implementation of this.
11. Nosocomial Reporting The Committee noted the Nosocomial Report. In May 2020, the National sitrep for reporting Covid
positive patients within all NHS Trusts changed to include two new questions. This was to report all
patients diagnosed after a swab either 8 or 15 days post admission. GMMH were able to report this
accurately given the enormous work that had already been achieved in reporting and developing the
SitRep process for the pandemic.
Unfortunately, the answers to these two questions were then added together as a total and an
assumption made through the analysis process that if the infection was acquired at this point after
admission it must have been acquired in a hospital setting and was therefore classed as Nosocomial.
This assumption did not allow for the nuances of Mental Health Trusts, including AWOL, leave, failure
to comply to isolation, social distancing, mask wearing when out on leave and a whole other host of
circumstances unique to this speciality.
The submission of this dataset was then ultimately reported through a weekly Nosocomial Reporting
Pack for all GM NHS Trusts and immediately had GMMH as a very noticeable outlier. This in turn was
picked up by the MEN and reported in large headlines of the risk to being admitted to the Trust and
risked the reputation of the organisation as a result.
Since this time (Dec 2020) the IPC team in Nursing and Governance have kept a local spreadsheet
detailing all cases diagnosed post 8 or 15 days from admission with a full clinical review of each case
allowing a validated conclusion if the case was in fact nosocomial or acquired as a result of other contact.
The team have also clinically reviewed all those cases reported pre-Dec 2020 to validate their
nosocomial status.
The current validated nosocomial position for GMMH shows 290 positive patients since 28th March 2020,
86 cases clinically validated as nosocomial – given this was not recorded or expected to be recorded
prior to 1st May 2020 - this should be now recorded as our actual position being 29.6% - 17% less than
the GMMH position currently being reported by Region.
Gill Green, on behalf of the Trust, wrote a letter to NHS England to formally request that the national
submission was revised to reflect the accurate picture for GMMH. A response has now been received
and although the data already submitted cannot be amended, they have commended GMMH in regard
to reporting and also how the episodes had been clinically managed in a positive way.
7
12. Use of Force Action Plan - update
The Committee held discussions on the Use of Force Action Plan. The DHSC have launched a
consultation Mental Health Units (Use of Force) Act 2018 statutory guidance. The guidance will provide
information for NHS and independent mental health providers on how they should meet the legal
obligations placed on them by the Act. The consultation ends on 17 August 2021 and it was agreed to
add as an agenda item for discussion at the next meeting in order to update the current action plan.
Following discussions, the following actions were agreed:
• Use of Force Action Plan to be discussed at QIC in September
13. Nursing and Governance briefing for April
The Committee noted the Nursing and Governance Briefing for April 2021. The report summarises
high level information monitored by the Nursing and Governance team. This relates to complaints and
and safeguarding activity. There is also a summary of Mental Health Act and Mental Capacity Act
related information.
Complaints
• No high level complaints was received
• Six level 4 and 5 complaints are currently open
• No high-level claims were received Serious Incidents
• Three serious Incident was identified in April 2021, initial fact finding reviews are currently being undertaken
Inquests
• 20 Inquests we concluded in April
• One regulation 28 reports were issued The Committee were informed of the increase in Inquest activity following the re-commencement of
Inquests and backlog due to the pandemic and the impact this could potentially have on clinicians
involved.
NHSE Independent Homicide Investigations
• One Independent Homicide Investigations has been commissioned in April
Mental Health Act Compliance and Mental Capacity Act
• No remote CQC MHA monitoring visits took place in April
• 49 MHA tribunal hearings took place Safeguarding
• Three Serious Case Reviews were commissioned in April
• One prevent referral was made in April
8
14. Quality Account 2021/2022 The Committee approved the Quality Account for 2021/2022. The format of the Quality Account follows strict mandated contents, as set out in guidance. Guidance has remained unchanged from 2019/20. As per 2019/20, there was no requirement to include a quality report in the annual report and no requirement to undertake auditor assurance work on the Quality Account. In addition, the Council of Governors was not required to select a local data indicator and there was no need for external testing of data indicators for this year’s Quality Account. For 2021/22, it was decided to maintain the existing Quality Improvement Priorities (QIPs), which were agreed and set out in last year’s Quality Account. This will allow GMMH to continue with the significant progress already made, and to develop and implement further additional improvement and sustainability programmes that relate to these areas. The QIPs for 2021/22, will therefore continue to be:
• To improve outcomes • To Minimise harm • To integrate care around the person
Once approved, the Quality Account will undergo minor branding by the communications department and will be uploaded onto the NHS Choices website on 30th June. The Dragon’s Den programme will launch on 5th July 2021. The Trust’s communications team is currently developing materials which will be released across social media and in upcoming staff bulletins ahead of a comms campaign in the lead up to the launch.
15. Quality Improvement Operational Delivery Group The Committee noted the minutes from the Quality Improvement Operational Delivery Group. The meeting was held on Tuesday 25 May. The members discussed the regulatory standards, NHSE Older Adult 2020 Stocktake, Physical Healthcare Strategy, Positive and Safe Programme, Medicines Management, NHS Benchmarking. The Group will continue to monitor action and escalate to QIC if necessary.
16. Items for Escalation There were no items raised for escalation
17. Any Other Business
Gill Green briefed Committee members in regard to how the vaccination programme for staff had been
rolled out within GMMH since January 2021.
The update included:
• Confirmation of the vaccination centres and access to the vaccination in outreach clinics across
GMMH.
• Monitoring arrangements on uptake including the National system of recording which is
undertaken centrally within the NHS.
9
• Shared practice and learning across GM
• Communications strategy to encourage uptake of the vaccine, available information and access
to trusted and confidential conversations as needed.
18. Date and Time on Next Meeting
The next meeting is scheduled for:
Thursday 8 July 2021
at
9.30am until 12:00
Via Microsoft Teams
1
Committee Chair’s Report to the Board of Directors
QUALITY IMPROVEMENT COMMITTEE
Date of Board Meeting: Monday 26 July 2021
Date of Committee Meeting: Thursday 8 July 2021
Committee Chair: Julie Jarman, Non-Executive Director
Date of Chair’s Report: Thursday 8 July 2021
Date of Next Committee Meeting: Thursday 9 September 2021
Key
Developments
Service User and Carer Engagement Update The Committee received a presentation on Service User and Carer Engagement. Highlights include:
• Recent CMHT Care Plan Audit showed an increase in service user involvement up from 75% in 18/19 to 96% in 20/21. The team are doing a follow up deep dive into care planning and carer engagement because this statistic hides the fact that there are very high levels of exceptions noted on the system – including one team which had a 91% exception rate.
• An increase in carer contribution to care planning up from 61% in 18/19 to 73% in 20/21. Only 39% of carers were offered a copy of the care plan
• Recent Trust wide learning event re: carer engagement as a result of NICHE review into 10 serious incidents. Lack of carer engagement highlighted, in addition to high level of complaints from carers and high numbers of carer exemptions identified in Paris.
• Recovery Academy Team supporting the delivery of education and training via Learning Hub including taught sessions and e-learning, Trust Welcome Day, Preceptorship Programme and EPIC.
• Service User and Carer engagement continues in various projects across the Trust, including the Park House Development, AFS LPC and Community Transformation.
• The Trusts feedback process has been reviewed and new processes implemented this includes the use of QR codes.
• The World Health Organisation are interested in GMMH’s Strategy and Engagement Scheme model. Claire Watson had an initial meeting with France in June 2021.
2
• Look at how service staffing, performance indicators and service user views and outcome monitoring can all be triangulated
Peer Workforce Update The committee received a presentation on Peer Workforce. Highlights include:
• There are currently 40 Peer Mentor volunteers across the Trust footprint
• GMMH have secured funding for Level 2 Peer Support award matched to the National Peer Support Competency Framework
• There are 26 Peer Support Roles across the Trust
• We are in the process of recruiting into 8 Peer Support Worker roles, placements to commence July 2021
• Peer Support Apprenticeships will start in January 2022 There was significant support for the value of increasing the peer workforce and the committee held discussions on what the Peer Support Workforce Target should be set at, currently it stands at 0.5%. It was agreed the target should be staggered over the next 3 years, aiming for at 1% at the end of 2021/2022 then 2% for 2022/23 with the final target of 5%. This to be monitored at the Quality Improvement Operational Development Group and also to be added as a quality metric going forward. It was agreed to add questions on the peer workforce into the Quality of Care Programme. Community Transformation Highlight Report The Committee noted the Community Transformation Highlight Report. The report outlines the workstream objectives for year one, key developments within June, which include:
• Project Leads are representing at a range of GM groups supporting transformation programme. Focus on establishing elements that will be common in GM, and West Sector, and which elements will be subject to more extensive local tailoring.
• Lead consultants’ group have now been arranged.
• Development of model and diagrams to support discussions internally and externally.
• First workshop for community lead consultants and Heads of Operations was held at the end of June
• Arrangements for financial governance have been established including budget clinic.
• Request for staff engagement events received, these are currently being arranged
• SLTs are being supported to engage with local partners to form locality planning meetings which will be the for the development of the model and implementation in each locality. These groups are critical for VCSE, PCN/ GP and EBE engagement and participation.
• Baseline locality plans have been drawn up for all five localities – in process of being shared out with HoOps and lead consultants/ SLTs for ongoing work.
• Core group clarifying phasing arrangements for Core/ Specialist teams per locality.
The Committee received an update on the Healthier Patient Pathways Transformation Programme. The Perfect week for Bolton took place week commencing 21 June, this went extremely well. Highlights of the week include
• One DTOC patient with a 263 day LoS had placement agreed by the CCG via Gold escalation
• One DTOC patient transferred to Rehab earlier following Gold escalation due to revised IPC guidance (reducing LoS a further 2 weeks)
• Excellent team work to effectively reduce the level of admissions and maintain the level of discharges
Key change ideas included
• MH Liaison/ HBT to document purpose of admission and communicate to patient/ carer
• Comprehensive handover to ward from admitting team • Junior Doctors to commence treatment following initial contact • Community care coordinator & carer to be invited to first MDT Review • Implement countdown discharge spreadsheet
There were lots of positive feedback received from staff taking part with the majority saying it has been a positive experience. Following discussions, it was agreed to include feedback from a service user of their experience of the Perfect week. Quality of Care Review - Trafford The Committee received a presentation with an update on actions following the Quality-of-Care Review that was undertaken at Trafford. A number of recommendations were identified following the QoC review, these were:
• Care Planning
• Physical Health
• Mental Health Act
• Restrictive Practices
• Infection Prevention The Committee received assurance that the Inpatient Services at Trafford have worked extremely hard and have systems in place to support with the actions identified, and welcomed the enthusiasm of the team to improve the quality of care and the way they have embraced QI methods
4
The Use of Force Action Plan The Committee held discussions on the Use of Force Action Plan. A draft consultation for the update to the statutory guidance for the Mental Health Units (Use of Force) Act 2018 was published on 25 May 2021. This draft statutory guidance provides further information about how the Act should be implemented and, like the MHA, there would need to be cogent reasons for departure from the statutory guidance or organisations could face legal challenge. It is also intended that case studies and good practice examples will be included in the final version of the guidance. GMMH has reviewed the statutory guidance and have provided comments for consideration to be submitted to the consultation on this guidance. The consultation closes on 17 August 2021, if any comments could be sent to Clair Carson prior to the closing date. Once this has been completed the Use of Force will be re-launched. Nursing and Governance Briefing for May 2021 The Committee noted the Nursing and Governance Briefing for May 2021. The report summarises high level information monitored by the Nursing and Governance team. This relates to complaints and claims; serious incidents; newly commissioned and ongoing Independent Homicide Reviews; inquests; safeguarding activity and a summary of Mental Health Act and Mental Capacity Act related information. The Committee received assurance about the level of psychological support being offered to staff who have been involved in a difficult incident or are required to attend inquests. Briefing in regard to future Public Enquiry for the C19 pandemic
The Committee noted the briefing in regard to future public Enquiry for the C19 Pandemic. The Government has recently announced the formation of a Public Enquiry regarding response to the C19 pandemic. This will involve all public organisations, experts and members of the public. Further scope and detail have yet to be published. However, the Greater Manchester NHS Provider Federation Board has recently developed a proposal for reviewing the Collective GM response to the pandemic which will particularly identify areas of good practice, lessons learned and how the learning is taken forward, understood and actioned. Once the summary report has been published this will be circulated and discussed at the next QIC in September
Any Risks
Identified and
Agreed Actions
5
Other Items for
the Board’s
Attention
The Committee noted the minutes of the Quality Improvement Operational
Delivery Group held on Tuesday 2021.
It was noted in the meeting that Dame Carol Black’s independent review has
been launched, Kate Hall will review and update the committee in September.
It was noted that we are anticipating service user reps on the Committee.
1
Board of Directors – Part 1
TITLE OF REPORT: Equality Diversity and Inclusion Strategic Group:
12.01 Minutes of the meeting held 14 June 2021
12.02 Committee Chair’s Assurance Report form the meeting held on
15 July 2021
DATE OF MEETING: Monday 26 July 2021
AGENDA ITEM: 12.01-12.02
PRESENTED BY: Anthony Bell, Non-Executive Director
AUTHOR(S): Cath Prescott Head of Equality Diversity & Inclusion
REPORT: The Board of Directors are asked to note the Strategic Equality Diversity and Inclusion
Group minutes of the meeting held 14 June 2021 and the Chair’s Assurance Report
the meeting held on 15 July 2021.
THIS REPORT SUPPORTS ACHIEVEMENT OF THE FOLLOWING STRATEGIC OBJECTIVES:
Objective 1 – Work with service users and carers to achieve their goals by delivering high quality care yes
Objective 2 – Create an outstanding place to work, ensuring staff feel valued and are supported to
reach their potential
yes
Objective 3 – Continuously improve services for users through research, innovation and digital
technology
yes
Objective 4 – Work in partnership with others to improve wellbeing and challenge stigma yes
Objective 5 – Be a sustainable, well-led organisation that delivers social value yes
2
REPORT CONSIDERED AT THE FOLLOWING COMMITTEES/SUB-GROUPS:
Committee/Sub-Group: Date:
Audit Committee
Quality Improvement Committee
Charitable Funds Committee
Remuneration & Terms of Service Committee
Council of Governors
Executive Management Team
LEGAL IMPLICATIONS: As a public sector organisation GMMH Foundation Trust is subject to legal duties
as an employer and as a provider of goods and services under the Equality Act
2010.
REGULATORY
IMPLICATIONS (CQC/NHSI):
THIS REPORT PROVIDES ASSURANCE AGAINST A RISK ON THE BOARD ASSURANCE FRAMEWORK (BAF):
Yes
If ‘yes’:
SO2/01 Recruitment and retention
SO4/01 Engagement
DATIX ID Strategic Objective Description (as per BAF)
PURPOSE OF REPORT – Please tick all relevant boxes
Information
Y Assurance Y Approval/Decision
RECOMMENDATIONS: That the Board notes the development of the Trust approach to EDI in line with
national strategic priorities and local needs.
1
STRATEGIC EQUALITY, DIVERSITY & INCLUSION WORKING GROUP
Minutes
Monday 14 June 2021
09:00 – 11:00 via MS Teams
RATIFIED Attendees: Job Role Anthony Bell Non-Executive Director - Chair Catherine Prescott Head of EDI Charles Kwaku-Odoi Caribbean & African Health Network Charlotte Wright Head of HR Clair Carson Associate Director Colin Reid Trust Executive Gill Green Director of Nursing and Governance Dawn Edge Manchester University Hambeleleni Abisai BAME Staff Network Juliette Tait Associate Director of HR & OD Michelle Clarkson Disability Staff Network Miranda Washington Deputy Director Performance and Business Development Peter Smith Chair of LGBT + staff network Rupert Nichols Chair of the Board Sandeep Matthews Consultant – Adult Forensic Tom Woodcock Strategic Lead for Community Asset Development Tracy Tsikai BAME Staff Network Minutes Molly Entwisle Nursing, Governance and Risk Team Administrator
2
1. Apologies Apologies were noted from:
Andrew Maloney Deborah Partington Dr Sodi Mann Janine Taylor Kim Saville Marie Coulton Neil Thwaite Sabaa Mahmud
2. Minutes of Previous Meeting
The minutes from the previous Strategic Equality, Diversity and Inclusion Working Group held on Monday 10 May 2021 were agreed as an accurate record. 3. Update on action log
4. GMMH EDI Strategy Development The group received a presentation on the GMMH EDI Strategy Development.
The current GMMH EDI strategy runs from 2019 – 2021 therefore a refresh is due and will reflect the
increased focus within the Trust on supporting Equality Diversity and Inclusion and addressing health
inequalities in our communities. The national Addressing Mental Health Equalities Strategy (Sept 2020)
provides direction and the outline position described in the slide presentation identifies cross cutting
themes and synergies with other strategic workstreams in the Trust.
Following discussions, it was agreed that the process would be evaluated, with any feedback being taken
into account and the process further developed. An update would be given in the next meeting.
5. Action Plan 4.1 Workstream 1 – Supporting Local Health Systems 4.1.2 Patient and Carer Race Equality Framework update The group received an update on the Patient and Carer race Equality Framework. GMMH have continued to implement the pilot PCREF in conjunction with NHSE and other sites (SLAM, East London, and Birmingham and Solihull) and participate in the relevant steering groups at a national level. The GMMH project group meets fortnightly and is supported by operational and corporate colleagues. The PCREF survey has been circulated and promoted across the organisation and there is work to look at more accessible formats and translated versions. Engagement with VCSE groups needs further development with relatively low uptake of the offer to facilitate group discussions around the survey. Resource implications for the longer term engagement with community groups and data analysis are being scoped.
3
It was raised that the participation from community groups has been low. It was agreed that TW and CKO would discuss how this can be improved. HA raised that it would be beneficial if the group liaised with other local research and data collection similar to PCREF in order to learn from their methods. GG has raised to the National PCREF Steering group the accessibility issues of the PCREF survey. 4.2 Work Stream 2 – Data and Information 4.2.1 Health Inequalities and business planning The group received an update on Health Inequalities and business planning.
1. Equality Impact Assessments have been requested as part of all operational and corporate business plans. There is a section of the business plan that each Directorate / Division completes that includes an Equality Impact Assessment and each Directorate is asked to align plans to the GMMH equality objectives. The deadline for completion of the Business Plans has been extended to end of June. The Plans will be used to feed into the Trust Operational Plan, with a section on inequalities.
2. The Provider Collaborative Programme for GM Adult Secure Services – we have recently commissioned Niche to undertake a simulation-modelling led review of mental health services for adult forensic populations in GM, the scope includes “The need to address health inequalities for the population based within each locality/network.” Following the completion of this work a full Commissioning Strategy will be developed, with a clear emphasis on advancing equality, in line with the national ‘Advancing Mental Health Equalities Strategy’ and taking into consideration the opportunities to advance equalities summarised in the Mental Health Delivery Plan 2021-22, Advancing equality for the local population is a key underpinning principle of the PC approach, achieved via a population health based approach to planning services, the central role of Experts by Experience and clinicians leading improvements in care pathways and more joined up pathways of service delivery, achieved by collaboration. There are great opportunities with the PC approach to drive forward equality.
3. The mental health delivery plan Annex 3 which describes opportunities for mental health services to address inequalities was discussed at the last Strategic EDI group and is intended to be shared with services to set a baseline and identify priorities.
Following discussions, it was agreed that Health Impact Assessments would be reviewed and
developed.
4.3 Work Stream 3 - Workforce 4.3.1 HR update The group received a HR update. The Workforce Race Equality Standard, Workforce Disability Equality Standard and the Gender Pay Gap Reports information will be extracted and presented at the next Strategic EDI meeting. The following reports are due to be submitted and will be provided for further discussion to the Strategic EDI Group:-
4
o Workforce Race Equality Standard & Workforce Disability Equality Standard – national reporting deadline of 31st August 2021 (WRES & WDES Action Groups have been established in readiness)
o Gender Pay Gap Report – national reporting deadline to be confirmed (but due imminently).
There is due to be a reengagement with the Staff Network groups with HR.
TT highlighted that it would be beneficial for the outcome of the previous data collection collected by
the Staff Network groups to be shared with these groups prior to the reengagement. TT advised that
this would keep motivation up and it would encourage further data collection by these groups.
MC raised that recruitment data for staff with disabilities had not been received. It was agreed that this
recruitment data would be collated and provided to the meeting and to the Staff Network group.
It was raised that there is no LGBTQ+ data for GMMH staff. There is LGBTQ+ data for service users.
Following discussions, the following actions were agreed
• Data from the WRES, WDES and Gender Pay gap reports to be brought to the next meeting.
• Recruitment data relating to staff with disabilities would be collated and provided to the Strategic EDI Group and the Disability Staff Network group.
6. Network updates & EDHR Update The group received an update on the BAME Staff Network. The BAME Network continues to support the service by facilitating the following: 1. The BAME committee manages to recruit 4 committee members, consisting two consultants, which make up 8 members and is in the process to recruit the BAME Chair with the support from HR. Time is still a major constrain in order for the network to provide quality service to its members and to the organisation. 2. We continue to support the PCREF research project by encouraging the BAME Network members to complete the survey. We plan to help focus group workshop with Catherine’s support. 3. We had initial meeting with Oxford Listen, Share, Hold, Respond (LiSHoRe) to start the research project on Spiritual Care. Oxford need a letter of authorisation for the project to go ahead. We need to know who will prepare this letter from the GMMH. Will it be the Research and Development or EDI? It was raised that the term ‘BAME’ is being revised due to it not being a fully inclusive term. Discussions and surveys are taking place in regards to developing a more inclusive term. The group received an update on the LGBTQ+ Staff Network Group. The LGBTQ+ Staff network group were hoping to attend various Pride events but are awaiting Public Health guidance on the attendance of these events. It was raised that there is not currently a GMMH Staff Network group for every required group. It was
agreed that JT and CP would meet to discuss this further.
MC raised that staff members who are in the Staff Network have no protected time to complete work
relating to the Staff Network group and are often having to complete this in their own time and on top
of their current job role. MC advised that this often deters new staff members from joining the Staff
Network Groups.
5
AB highlighted the importance of Staff Network Groups and felt that they should be supported.
It was raised that information and changes are not being fed back to the Disability Staff Network and it
is felt that issues are being raised in their meetings, but no feedback and resolution is received relating
to these issues.
Following discussions, the following actions were agreed
• JT and CP to meet to discuss increasing the number of Staff Network Groups in GMMH and the resources required to do this.
7. Any other Business GG raised to the meeting that it was TW’s last Strategic EDI meeting. The group thanked Tom for all his hard work and commitment to the group and the organisation. 8. Date and time of next meeting The next meeting is scheduled for:
Thursday 15 July 2021
14:00 – 16:00
Virtual via MS Teams
6
Action Plan – Updated June 2021
Number Meeting Action Agreed
timescale
Update Owner Status
1 Oct-20 To evaluate current effectiveness of EDHR Steering Group and wider
governance of EDI
Nov-20 review of governance part of action 9 and will be picked up in EDI
strategy development
Tom Woodcock In progress
2 Feb-21 Work Plans to run concurrent and to include other protected character
groups, Disability Network and LGBT +
Mar-21 To be picked up in July-21 Meeting Network Leads In progress
3 Feb-21 To look at producing a video with Neil Thwaite and the Network Chairs
explaining what the networks are
Mar-21 Update to be given to chair Andrew Maloney / Comms In progress
4 Feb-21 Business Plan to be shared with the Group at the next meeting Mar-21 mental health delivery plan (annex 3) shared with service and
business development lead
Mary Lee In progress
5 Mar-21 A small group of executives to look into capturing user data and
improvement targets outside the business planning process and feedback to
the next meeting.
May-21 Andrew Maloney In progress
6 Mar-21 Develop a plan on a page to summarise the EDI strategy. May-21 completed for April EDI meeting Tom Woodcock In progress
7 Mar-21 Schedule monthly meetings until the end of the financial year 2021/22 and
to review in September
Sep-21 Anthony Bell In progress
8 Mar-21 To clarify the governance structure around the different EDI workstreams. May-21 will be picked up in strategy development Tom Woodcock In progress
9 May-21 To identify ways of increasing support given to BAME Champions Gary Fox / Michelle Dowd In progress
10 May-21 To discuss and re-evaluate what is needed from the feedback survey data in
order to maximise the resources.
Meetings and discussions have taken place and outline of resource
implications fro the PCREF underway.
An update will be given July-21 Meeting.
Tom Woodcock / Cath Prescott
/ Dawn Edge
In progress
11 May-21 To discuss Business Planning Cycle as per action 5 Tom Woodcock In progress
12 May-21 An update to be given to the EDI group on the Kickstart Program Juliette Tait / Charlotte Wright In progress
13 Jun-21 Recruitment data for staff with disabilities to be provided. Juliette Tait / Charlotte Wright In progress
14 Jun-21 Health Impact Assessments to be reviewed and developed. Cath Prescott / Miranda
Washington
In progress
15 Jun-21 EDI Strategy Development Process to be reviewed and updated and any
changes brought to the next meeting.
Jul-21 Cath Prescott / Gill Green In progress
16 Jun-21 Data from the WRES, WDES and Gender Pay Gap reports to be presented in
the next EDI meeting.
Jul-21 Cath Prescott / Gill Green In progress
17 Jun-21 JT and CP to meet to discuss increasing the number of Staff Network Groups
in GMMH and the resources required to do this.
Cath Prescott / Juliette Tait In progress
Strategic EDI Working Group Action Log - Updated June 2021
Committee Chair’s Report to the Board of Directors
STRATEGIC EDI WORKING GROUP
Date of Board Meeting: Monday, 26 July 2021
Date of Committee Meeting: Thursday, 15 July 2021
Committee Chair: Anthony Bell, Non-Executive Director
Date of Chair’s Report: Thursday, 15 July 2021
Date of Next Committee Meeting: Monday, 9 August 2021
Key
Developments
• Strategy. The group received a presentation confirming how the
organisational EDI strategy development will proceed. The Strategy will be
developed in three key sprints and identify our priorities in relation to our
community, our services and our workforce. Eight pillars of an effective
approach have been identified, which include governance, research, co-
production, health equality impact assessments, inclusive and accessible
environments, data and performance indicators and the Trust as an anchor
institution. It was agreed that initial discussions around each of these key
pillars would take place at future meetings and that a series of small sub-
groups will be established to drive forward development
• Governance. A discussion took place on current and future governance
arrangements for EDI and members of the group were invited to share
their views on what an effective structure would include. It was noted that
the Trust’s governance arrangements were also being reviewed and that
this piece of work could feed into discussions. It was agreed that a small
sub-group would consult further and develop a proposal.
• Co-production. A discussion took place on current activity taking place with
service users, carers, service providers, community groups and the
workforce. It was noted that whilst a lot of excellent work has taken place
to develop supportive vehicles for co-production in respect of service
users, carers and the workforce there remain areas for improvement. It
was also noted that an area lacking at present is co-production activity with
our community. It was agreed that a small sub-group would scope future
action required to support the strategy development and ongoing activity.
2
• Build Back Fairer in Greater Manchester: Health Equity and Dignified Lives.
An overview of the recent GM Marmot report was presented, and a
discussion took place on ‘What does being a Marmot City mean for GMMH
Trust? It was proposed that this be picked up as part of the discussion on
the Trust as an Anchor Institution and that consideration should be given
to the production of a series of informative videos and webinars. It was
noted that this has links with the social value work currently taking place
across Trust and it was agreed that links should be made to ensure a
joined-up approach.
• Patient and Carer Race Equality Framework (PCREF). An update on
progress against the PCREF was provided. It was noted that action was
currently taking place against all three arms of the framework including
legal and regulatory duties, co-production of core competencies and the
assessment tool. Feedback from the national PCREF group was provided
and an overview of potential inclusion of the PCREF in the QCC KLOE’s
given.
Any Risks
Identified and
Agreed Actions
• A series of small sub-groups, based on the eight pillars of an effective
approach, will be established to drive forward development of the EDI
Strategy.
Other Items for
the Board’s
Attention
NA
1
Board of Directors – Part 1
TITLE OF REPORT: Charitable Funds Committee:
13.01 Minutes of the Meeting held 24 March 2021 (Ratified)
13.02 Committee Chair’s Report on the Meeting held 5 July 2021
13.03 Terms of Reference
DATE OF MEETING: Monday 26 July 2021
AGENDA ITEM: 1301-13.03
PRESENTED BY: Anthony Bell, Non-Executive Director and Charitable Funds Committee Chair
AUTHOR(S): Diana Paul, Executive PA
REPORT SUMMARY: The Board of Directors are asked to note the ratified minutes of the Charitable
Funds Committee meeting held on 24 March 2021 and the Committee Chair’s
Report on the meeting held on 5 July 2021.
Terms of Reference approved at the meeting on 5 July 2021 are also attached.
THIS REPORT SUPPORTS ACHIEVEMENT OF THE FOLLOWING STRATEGIC OBJECTIVES:
Objective 1 – Work with service users and carers to achieve their goals by delivering high quality care
Objective 2 – Create an outstanding place to work, ensuring staff feel valued and are supported to
reach their potential
Objective 3 – Continuously improve services for users through research, innovation and digital
technology
Objective 4 – Work in partnership with others to improve wellbeing and challenge stigma
Objective 5 – Be a sustainable, well-led organisation that delivers social value x
REPORT CONSIDERED AT THE FOLLOWING COMMITTEES/SUB-GROUPS:
Committee/Sub-Group: Date:
Audit Committee -
Quality Improvement Committee -
Charitable Funds Committee -
Remuneration & Terms of Service Committee -
Council of Governors -
Executive Management Team -
2
LEGAL IMPLICATIONS: None identified
REGULATORY IMPLICATIONS
(CQC/NHSI):
None identified
THIS REPORT PROVIDES ASSURANCE AGAINST A RISK ON THE BOARD ASSURANCE FRAMEWORK (BAF):
No
If ‘yes’:
DATIX ID Strategic Objective Description (as per BAF)
PURPOSE OF REPORT – Please tick all relevant boxes
Information
Assurance x Approval/Decision x
RECOMMENDATIONS: The Board of Directors are asked to receive and note the following:
• Minutes of the Charitable Funds Committee meeting held 24 March 2021
(Ratified)
• Committee Chair’s Report on the meeting held 5 July 2021.
• Terms of Reference
RATIFIED CHARITABLE FUNDS COMMITTEE 24 MARCH 2021 AT 11AM VIA MICROSOFT OFFICE PRESENT: Anthony Bell Non-Executive Director (Chair) Julie Jarman Non-Executive Director Suzanne Robinson Director of Finance and IM&T Gill Green Director of Nursing & Governance Adele McKie Assistant Director of Finance, Financial Services & Procurement Diana Paul Executive PA IN ATTENDANCE: Juliet Tait Associate Director of HR (attended for 06/21) Colin Reid Interim Company Secretary
No. Notes Action
01/21 Apologies for Absence There were no apologies of absence.
Noted
02/21 Declaration of Interest There were no declarations of interests in agenda items,
03/21 Minutes of Previous Meeting held 4 December 2020 The minutes of the previous meeting held on 4 December 2020 were agreed as a true and correct record.
Approved
04/21 Matters Arising from Previous Meeting Committee members agreed all action have been closed.
Noted
05/21 Finance Report: Summary Report until 28 February 2021 Adele McKie, Assistant Director of Finance informed the meeting the paper outlines the charity held funds as at 28 February which total £372,414.38 having received income (including interest on investments) of £147,440.83 and incurred expenditure of £30,026.12. The Charity currently has further committed expenditure against these funds totally £183,944.35. Adele McKie explained in more detail regarding the breakdown of the income, expenditure, committed and uncommitted funds within the report. She highlighted part of the uncommitted funds is regarding the current contribution to the psychiatric nurses’ fund which staff have paid into, a meeting is due to take place in March as to how these monies can be spent and as of 1 April any monies donated by these staff will be allocated to the staff benefit fund. Suzanne Robinson, Director of Finance & IM&T stated going forward there will be an additional standard agenda item to show what the £30,026.12 monies have been spent on and the impact it has made.
Noted
2
There may also be opportunity to look at larger projects which the Trust could undertake which could encompass Charitable Funds monies as well as looking to see if there are any grants which could be accessed. The Trust also has £15k legacy monies specifically allocated for Later Life services. Adele McKie to investigate with the Charity Commission regarding closing this account, findings to be brought back to the next meeting for a decision to be made regarding the future of the Later Life fund. Gill Green, Director of Nursing & Governance stated the importance of including Wigan services and providing them the same opportunity to request monies from the Charitable Funds. Suzanne Robinson stated the Trust is expected a share of NWB’s Charitable Funds monies will be transferred with the Wigan services, some of these monies will be specifically designated for Wigan services and a portion will be incorporated within the Trust’s main Charity Fund. Details of these monies will be brought to the next meeting. Tony Bell, Non-Executive Director enquired as to whether the 3 areas which the fund is split into Staff, Patient and General is still appropriate. It was agreed for the Committee to look at this at a future meeting, however it was acknowledged that the Trust would have more options regarding expenditure if it were part of a general fund. The Committee noted the report and thanked Adele for the clear and informative report.
Adele McKie
Adele McKie
06/21 NHS Charities Together Fund Juliet Tait, Associate Director of HR informed the meeting that in February 2021, the Trust received confirmation of a successful bid for second wave Covid 19 funding and £50k was allocated. These funds were designated for enhancing the wellbeing of NHS staff, patients and volunteers. A scoping meeting with Staff Network Leads, Trade Union representatives and other key stakeholders was held and agreed for staff across the Trust to put in bids for these monies, similar to the process for Dragon’s Den. A communication and engagement plan will be launched week commencing 12 April 21. A Panel comprising of staff will be pulled together to hear and make decisions on the bids presented. Suzanne Robinson, Director of Finance & IM&T stated the importance of having a criteria for which bids are scored against for reporting back to NHS Charities including incorporating what the monies have been spent on and evidence what the impact/benefit has been. National communications regarding the benefits received from the monies also to be looked at when reporting to NHS Charities. Julie Jarman, Non-Executive Director, stated this exercise could also be a springboard for spending the £6k which is within the staff benefit fund. Juliette Tait and Adele McKie to discuss outside of the meeting.
Noted
Adele McKie/
Juliet Tait
3
Suzanne Robinson, Director of Finance & IM&T agreed this is a positive approach for engaging the Trust and for this approach to be looked to be integrated into the spending across the Charitable Funds. The meeting agreed for an update to come to the next meeting and for this to be delivered in a multi-faceted way, pictures, videos, hearing direct from people who have benefited instead of a hand written report coming to the Committee. This could also be shared with Governors and included within the Chief Executive’s Brief and Internet. The Committee noted the report.
Juliet Tait
07/21 Communication Regarding the Charity Discussion was had regarding communicating the work of the Charity. Suzanne Robinson, Director of Finance & IM&T informed the meeting that Caroline Pickwell, Head of Communications had forwarded the Communication Strategy which had been put on hold due to Covid, within this there is recognition of the importance of communicating and engaging with staff around the Charitable Fund. The meeting agreed the importance to communicating with staff/patients and volunteers the good news stories of what Charitable Fund monies spent and how this has impacted the particular areas. Tony Bell, Non-Executive Director enquired as to the next steps regarding the Fund and how to generate more monies. Tony Bell asked for members to consider ideas to be brought to the next meeting for discussion. Suzanne Robinson stated NHS Charities will still receive monies from the public for at least the next 12 months which will give the Trust opportunity to look at the future of the Fund beyond this point.
Noted
08/21 Any Other Business There was no other business raised.
09/21 Date and Time of Next Meeting 5 July 2021, 1pm, via Microsoft Teams
Noted
4
CHARITABLE FUNDS COMMITTEE ACTION LOG
No Meeting Minute No.
Item Action Agreed Timescale
Forecast Completion
Update Owner Status
19 22/3/21 05/21 Finance Report Details of Wigan Charitable Funds monies to come to next meeting
July 21 Adele McKie
20 22/3/21 06/21 NHS Charities Together Fund
Juliette Tait and Adele McKie to discuss spending of the £6k
July 21 Adele McKie Juliette Tait
21 22/3/21 06/21 NHS Charities Together Fund
Updated regarding spending of monies to come to the meeting – delivered in a multi-faceted way
July 21 Juliette Tait
Not yet due
Completed on time
In progress and on target
Incomplete and overdue
Committee Chair’s Report to the Board of Directors
CHARITABLE FUNDS COMMITTEE
Date of Board Meeting: 26 July 2021
Date of Committee Meeting: 5 July 2021
Committee Chair: Anthony Bell, Non-Executive Director (Committee Chair)
Date of Chair’s Report: 6 July 2021
Date of Next Committee Meeting: 6 December 2021
Key Developments Terms of Reference These were agreed and will be present to Board at the July meeting. Draft Charitable Accounts The committee was assured by the accounts presented and requested clarification on 2 presentational points. External scrutiny of the accounts is required where donated income received exceeds £25k. Quotes are currently being obtained to enable an appointment to be made. Independently examined accounts will come back to the December meeting prior to submission by 31 January 2022. Charitable Annual Report A draft report has been compiled which is currently with the Communications Team and will be brought to the December meeting. This is a requirement of the Charity Commission. Finance Report – 31 May 2021 Of the available funds £213k is fully committed and £60k uncommitted. The committee have requested further details on the Wigan charitable funds that will transfer. The committee requested further assurance around the legitimacy of some charitable bids and whether these should be routinely funded from NHS monies. Captain Tom Farewell Fund 120 bids were received asking for funding to support needs around wellbeing for staff and service users. A proforma has been developed to provide the appropriate level of governance. Communication to go out asap to all staff regarding number of bids received and to confirm success status; followed by individual letters to those who have submitted bids. It was agreed that this should be on 5th July as the NHS Birthday.
2
The committee was assured by the process and was very supportive pf the innovative and inclusive way this had been approached. Non-executive members are keen to see the outputs in person once service visits can be resumed. Charity Strategy An action plan to be developed and brought to the December meeting regarding heightening the awareness of the Charity for this to include 3 priority projects which money could be raised for and an engagement plan around these. Consideration also to be given around involving staff and services users in the process.
Any Risks
Identified and
Agreed Actions
None
Other Items for
the Board’s
Attention
None
TERMS OF REFERENCE
CHARITABLE FUNDS COMMITTEE
Constitution & Authority
The purpose of the Charitable Funds Committee, hereafter referred to as the Committee, is to ensure that the Trust Board properly discharges its responsibilities in relation to its role as Corporate Trustee of the Charitable Funds.
Overall Aim & Purpose • To ensure the effective management of Charitable Funds of the Trust
Scope & Duties Functions
• To oversee the effective management of the affairs of the Charitable Funds on behalf of the Trustees (Board of Directors)
• To apply all charitable funds in accordance with the NHS Act 2006, Charities Act 2011, Commissioner requirements and other sources of good practice.
• To ensure that decisions on the use or investment of such funds are, where applicable, restricted to the explicit condition or purpose of each donation, legacy or grant.
• To make decisions involving the use of charitable funds within the terms of the ‘Declaration of Trust’ and with regard to the ‘Trustee Act 2000’ and any subsequent legislation.
• To ensure that the Trust’s policies and procedures for charitable funds and investments are followed.
• To ensure that funding decisions are consistent with the Trust’s vision, values and objectives and that such decisions provide added value and benefit to service users and staff above those afforded by revenue.
• To, where necessary, appoint Investment Advisors and to monitor the performance of the charitable funds investment portfolio.
• To oversee and monitor the functions performed by the Director of Finance and IM&T and Chief Executive with regard to the investment, accounting and reporting on the use of charitable funds.
• To receive the Annual Accounts and Report of the Trust’s Charitable Funds for consideration and recommendation for final approval, or otherwise, to the Trust Board.
Membership
Membership of the Committee will comprise of the following:
• Two Non-Executive Directors
• Director of Nursing and Governance
• Director of Finance and IM&T The Chair will have the deciding vote in the case of a tied decision. The Committee will be supported by:
• Associate Director of Finance
• Assistant Director of Finance – Financial Accounts and Systems Other attendees may be co-opted, with the prior consent of the Chair, as the agenda dictates/as required for specific items/input.
Page 2 of 3
Accountable for:
The Charitable Funds Committee is accountable to the Board.
Frequency of Meetings
Meetings will be held no less than three times a year. The Chair or an Executive member may request an additional meeting if they consider one to be necessary.
Quorum
Non-Executive Director to Chair the meeting and one Executive Director member to be present.
Agenda and Papers
An agenda for each meeting, together with relevant papers, will be forwarded to members to arrive 5 working days before the meeting. Any member wishing to include an item on the agenda should ensure this is with the secretary to the Committee 10 days before the meeting date and should be agreed with the Chair of the meeting. The meeting will be supported secretarially by the PA to the Director of Finance and IM&T. Dates of meetings will be set for a full year Unratified minutes and action log will be circulated to the membership.
Minutes Formal minutes will be taken at the meeting. They will be drafted no later than two weeks after the meeting has taken place. Minutes will be formally ratified by Committee members at the next Charitable Funds Committee and shared with Trust Board.
Record Keeping Agenda and Papers can be found in the following link: N:\The Curve\Corporate Affairs\CHARITABLE FUNDS COMMITTEE These can be accessed by the Executive PAs.
Monitoring At a minimum, an annual review of attendance and effectiveness will be undertaken in order to monitor compliance with the Terms of Reference. This will be the responsibility of the Chair.
Terms of Reference Review
It is the responsibility of the Chair to review the effectiveness of the Committee’s Terms of Reference.
Agreed date for the Review of the Terms of Reference
July 2022
Page 3 of 3
Chart of relationship to other Meetings
Revision Log:
Date Name Comments
1 July 2019 Janine Taylor New format Membership updated NHS Act 2006 Charities Act 2011
July 2019
Charitable Funds
Committee
GMMH
Board
1
Board of Directors – Part 1
TITLE OF REPORT: Audit Committee:
14.01 Minutes of the Meeting held 8 June 2021 (Ratified)
14.02 Committee Chair’s Assurance Report on the Meeting held 5 July 2021
DATE OF MEETING: Monday 26 July 2021
AGENDA ITEM: 14.01-14.02
PRESENTED BY: Andrea Harrison, Non-Executive Director and Audit Committee Chair
AUTHOR(S): Diana Paul, Executive PA
REPORT SUMMARY: The Board of Directors are asked to note the ratified minutes of the Audit
Committee meeting held on 8 June 2021 and the Committee Chair’s Assurance
Report on the meeting held on 5 July 2021.
THIS REPORT SUPPORTS ACHIEVEMENT OF THE FOLLOWING STRATEGIC OBJECTIVES:
Objective 1 – Work with service users and carers to achieve their goals by delivering high quality care
Objective 2 – Create an outstanding place to work, ensuring staff feel valued and are supported to
reach their potential
Objective 3 – Continuously improve services for users through research, innovation and digital
technology
Objective 4 – Work in partnership with others to improve wellbeing and challenge stigma
Objective 5 – Be a sustainable, well-led organisation that delivers social value x
REPORT CONSIDERED AT THE FOLLOWING COMMITTEES/SUB-GROUPS:
Committee/Sub-Group: Date:
Audit Committee -
Quality Governance Committee -
Charitable Funds Committee -
Remuneration & Terms of Service Committee -
Council of Governors -
Executive Management Team -
2
LEGAL IMPLICATIONS: None identified
REGULATORY
IMPLICATIONS (CQC/NHSI):
None identified
THIS REPORT PROVIDES ASSURANCE AGAINST A RISK ON THE BOARD ASSURANCE FRAMEWORK (BAF):
No
If ‘yes’:
DATIX ID Strategic Objective Description (as per BAF)
PURPOSE OF REPORT – Please check all relevant boxes
Information
x Assurance x Approval/Decision
RECOMMENDATIONS: The Board of Directors are asked to review and note the following:
• Minutes of the Meeting held 8 June (Ratified)
• Committee Chair’s Assurance Report on the Meeting held 5 July 2021
RATIFIED
MINUTES OF THE AUDIT COMMITTEE MEETING
HELD 8 June 2021 AT 10.30AM VIA MICROSOFT TEAMS
Present:
Andrea Harrison - Non-Executive Director (Chair)
Anthony Bell - Non-Executive Director
Pauleen Lane - Non-Executive Director
In Attendance:
Rupert Nichols - Chair
Suzanne Robinson - Director of Finance & IM&T
Andrew Maloney - Director of HR/Deputy CEO
Janine Taylor - Associate Director of Finance
Colin Reid - Interim Company Secretary
Adele McKie - Assistant Director of Finance, Financial Services & Procurement
Kath Stott - Senior Manager, MIAA
Neil McQueen - Anti-Fraud Specialist, MIAA
Katie Scott - Senior Manager, KPMG
Diana Paul - Executive PA (Minutes)
No. Item Action
51/21 Welcome and Introductions
Andrea Harrison welcomed Kath Stott, Senior Manager, MIAA who will be
working with the Trust going forward.
52/21 Declaration of Interests
None were received.
Noted
53/21 Apologies for Absence
All Committee members were present.
Apologies for absence were received from:
• Neil Thwaite, Chief Executive
• Gill Green, Director of Nursing and Governance
Noted
54/21 Minutes of the Previous Meeting held 26 April 2021
The minutes of the previous meeting held on 26 April 2021 were agreed as a true
and correct record.
Approved
55/21 Matters Arising from the Previous Meeting
The Audit Committee noted the updates to the action log and that actions had
either been completed or were in progress.
Noted
56/21 Audit Committee Objectives
Andrea Harrison, Non-Executive Director informed the meeting the report sets
out the proposed objectives for the Audit Committee in 2021/22, these build on
Approved
Page 2 of 8
objectives agreed in previous years. She then went on to outline the detail within
the 4 proposed objectives for 2021/22.
The Committee noted the objectives and agreed they will be tracked and given
appropriate agenda time in future meetings.
The Committee approved the objectives.
57/21 Internal Audit Annual Report & Head of Internal Audit Opinion 202021
Kath Stott, Senior Manager, MIAA informed the meeting the Trust has been
awarded a Substantial level of assurance which means that there is a good
system of internal control designed to meet the organisation’s objectives and
that controls are generally being applied consistently’.
The Committee noted there had been no amendments to the report previously
presented at the last meeting and approved the report.
Noted and
Approved
58/21 External Audit Report – ISA 260 Audit Memorandum 2020/21
Katie Scott, Senior Manager, KPMG informed the meeting that the Trust had
received a positive report with two minor recommendations which are being
followed up.
Andrea Harrison, Non-Executive Director acknowledged that it is good to see a
clean report and asked for the Committee’s thanks to be passed on to the Finance
Team for enabling a good outcome of the audit.
Tony Bell. Non-Executive Director enquired as to the increase in audit fees. Katie
Scott explained this was due to the Value of Money scope and the additional work
required, also regarding the work around developing the Annual Report.
The Committee noted and approved the report.
Noted and
Approved
59/21 Audited Accounts for the Year Ended 31 March 2021 Adele McKie, Assistant Director of Finance informed the meeting that there had been 2 changes identified through internal checks since presenting in the last Audit Committee, these were outlined. Operating with the delegated authority of the Board of Directors, the Committee approved the Audited Accounts for 2020/21.
Approved
60/21 Annual Report 2020/21 Coin Reid, Interim Company Secretary informed the meeting that minor adjustments had been made to the report previously reviewed by the Audit Committee in April 2021 and Board of Directors in May 2021. Andrea Harrison, Non-Executive Director enquired as to the zero spend on the use of Consultants and what categories fall within the definition of the Accounting Manual. Adele McKie, Assistant Director of Finance agreed to share the definition within the Accountant Manual.
Noted and
Approved
Adele McKie
Page 3 of 8
Suzanne Robinson, Director of Finance & IM&T, Colin Reid and Adele McKie to pick up outside of the meeting regarding list of Consultants used by the Trust. The meeting agreed for a report on Consultants to come to a future meeting. Anthony Bell, Non-Executive Director enquired as to whether other Trust have similar interpretations of the definition. Katie Scott, Senior Manager, KPMG acknowledged that she was happy with the consistency across Trusts in what is required to be submitted. Andrew Maloney, Director of HR/Deputy CEO thanked Colin Reid for picking up developing the Annual Report with a short turn-around timescale. Operating with the delegated authority of the Board of Directors, the Committee approved the final Annual Report 2020/21 for submission to NHS England and NHS Improvement by the deadline of 15 June 2021, Colin Reid confirmed that he would facilitate the Chair and Chief Executive’s signatures of the Annual Report and Accounts and also the laying of the report before Parliament date to be confirmed.
Adele McKie
61/21 Management Representation Letter Suzanne Robinson, Director of Finance & IM&T advised the Committee that the content seen within the Annual Report and Accounts was in line with that seen by the Board throughout the 2020/21 financial year. She also outlined the opinions which the letter provides. The Committee noted and approved the Management Representation Letter for signature by the Director of Finance & IM&T.
Approved
62/21
Anti-Fraud Annual Report 2020/21 Neil McQueen, Anti-Fraud Specialist introduced the annual report, which is a combination of those previously seen by the Committee throughout the year. He also expressed his thanks to Adele McKie, Assistant Director of Finance in her role as Fraud Champion. Neil also confirmed to the meeting that there were 2 successful prosecutions obtained within the year. The Committee noted the report.
Noted
63/21 Payable & Receivable Balances Adele McKie, Assistant Director of Finance stated for the reporting period 1 April 2021 – 31 April 2021, there were 2 payable balances and 1 receivable balance. Adele McKie stated that the 2 payable balances under investigation had been accrued at year end. In terms of exiting procedures for properties, Adele acknowledged that work is being done in this area around communication and ensuring appropriate letters are in place to clarify any outstanding financial obligations. The Committee noted the report.
Noted
64/21 Investment Performance
Noted
Page 4 of 8
Adele McKie, Assistant Director of Finance reported the Trust’s cash investment performance until 30 April 2021 stands at £2.29. Interest is currently not being earned on the Trust’s Government Banking account due to a 0% interest rate. The Committee agreed to suspend reporting on the Trust Investment Performance until interest rates change. The Committee noted the report.
65/21 Losses and Special Payments The Committee noted the payments made from 1 April 2021 to 30 April 2021.
Noted
66/21 Disposal of Tangible Assets
The Committee noted no items were disposed of during the reporting period 1
April 2021 – 31 April 2021.
Noted
67/21 SFI Compliance Report – Waivers and Retrospective Orders
Adele McKie, Assistant Director reported the number of waivers and
retrospective orders raised from 1 April 2021 to 30 April 2021.
Adele agreed to look at items badged as ‘continuity of service’ to ascertain if a
best value exercise had been undertaken and include in the next report.
Suzanne Robinson also informed the meeting that the Procurement Strategy is
being refreshed and updated, this will be brought back to a future meeting.
The Committee noted the report.
Noted
Adele McKie
Adele McKie
68/21 Any Other Business
Rupert Nichols, Chair, acknowledged that the end of year audit had been a
complex process and praised how well it had been handled. He also
acknowledged the excellent working relationships the Finance department has
had with KPMG and MIAA. He thanked all involved on behalf of the Trust Board.
98 8/6/21 60/21 Annual Report 20/21 Adele McKie to share the definition of consultants
July 21 5/7/21 Adele McKie
Page 6 of 8
No Meeting Minute
No.
Item Action Agreed
Timescale
Forecast
Completion
Update Owner Status
within the DHSC Group Accountant Manuel.
The DHSC GAM
defines consultancy as
:
“The provision to
management of
objective advice and
assistance relating to
strategy, structure,
management or
operations of an
organisation in pursuit
of its purposes and
objectives. Such
assistance will be
provided outside the
’business[1]as-usual’
environment when in-
house skills are not
available and will be of
no essential
consequence and
time-limited.
Consultancy may
include the
identification of
options with
Page 7 of 8
No Meeting Minute
No.
Item Action Agreed
Timescale
Forecast
Completion
Update Owner Status
recommendations, or
assistance with (but
not delivery of) the
implementation of
solutions”
99 8/6/21 60/21 Annual Report 20/21 Report on Consultants to come to a future meeting.
Tbc Adele McKie
100 8/6/21 67/21 SFI Compliance
Report – Waivers
and Retrospective
Orders
Adele agreed to look at
items badged as
continuity of service to
ascertain if a best value
exercise had been
undertaken and include in
the next report.
July 21 5/7/21
Further investigation
of the 3 waivers which
had been authorised
on the basis of
continuity of service
found that 2 of them
should in fact have
been recorded under
the sole supplier
heading as they
related to a recharge
of staff under the s75
agreement and the
sub contracting of a
CCG commissioned
service.
The third waiver
related to an order for
the second year of a 2
Adele McKie
Page 8 of 8
No Meeting Minute
No.
Item Action Agreed
Timescale
Forecast
Completion
Update Owner Status
year contract and
should have been
recorded.
101 8/6/21 67/21 SFI Compliance
Report – Waivers
and Retrospective
Orders
Procurement Strategy is
being refreshed and
updated, this will be
included within this report
and brought back to a
future meeting.
Tbc Suzanne
Robinson
102
Not yet due
Completed on time
In progress and on target
Incomplete and overdue
1
Chair’s Assurance Report to the Board of Directors
AUDIT COMMITTEE
The Committee has received the following assurances on behalf of the Board:
TOPIC AREA ISSUES DISCUSSED RISK ON BAF?
Substantial Assurance – The Committee has received assurances on behalf of the
Board as to the consistent application of controls in respect of the following matters:
Limited Assurance – The Committee considers that there are some gaps/weakness in controls in respect of the following matters, which are of sufficient concern to require escalation to the Board for information at this stage
Use of Agency • High risk recommendation re retrospective
agency bookings for vacancies
• High % of medical rates above framework
limit
Y
No Assurance –The Committee considers that there are significant gaps/weaknesses in controls in respect of the following matters, which are of sufficient concern to require escalation to the Board for discussion on immediate action:
- - -
4. Other Items for the Board’s Attention:
Internal Audit Progress Report Workforce Strategy review was agreed to be postponed to Q3 to allow the recently refreshed People Plan to embed within the organisation. The focus on the Estates audit on Statutory Compliance has been amended based on exec/non-exec feedback. Internal Follow Up Report Further section to be added to the report which documents the high/ medium outstanding actions, this will enable the Committee to be aware of them and access whether it requires key leads to be invited to the Committee to discuss.
Date of Board Meeting: 26 July 21
Date of Committee Meeting: 5 July 2021
Committee Chair: Andrea Harrison,
Non-Executive Director and Audit Committee Chair
Date of Assurance Report: 6 July 2021
Date of Next Committee Meeting: 21 September 2021
2
Technical Update The accounts have now been submitted. KMPG contract is due to expire. Suzanne Robinson, Director of Finance & IM&T will share a paper with audit committee members regarding the appointing of external auditors. Annual Quality Assurance & Quality Improvement Report The Committee acknowledged the work that has been undertaken. Gill Green, Director of Nursing & Governance also asked members for feedback regarding the report if further information is required to be included. Information Governance Update Noted the increase in high level IG incidents, reportable to the ICO. Chris Daly, Associate Medical Director is leading a Trust wide learning session on incidents on 16 July. The session will also draw attention to the importance of staff being compliant in their IG Training. The Committee has requested some benchmarking information to provider further assurance.