70
Bones and Skeletal Tissue

Bones and Skeletal Tissue

6 2
Skeletal System
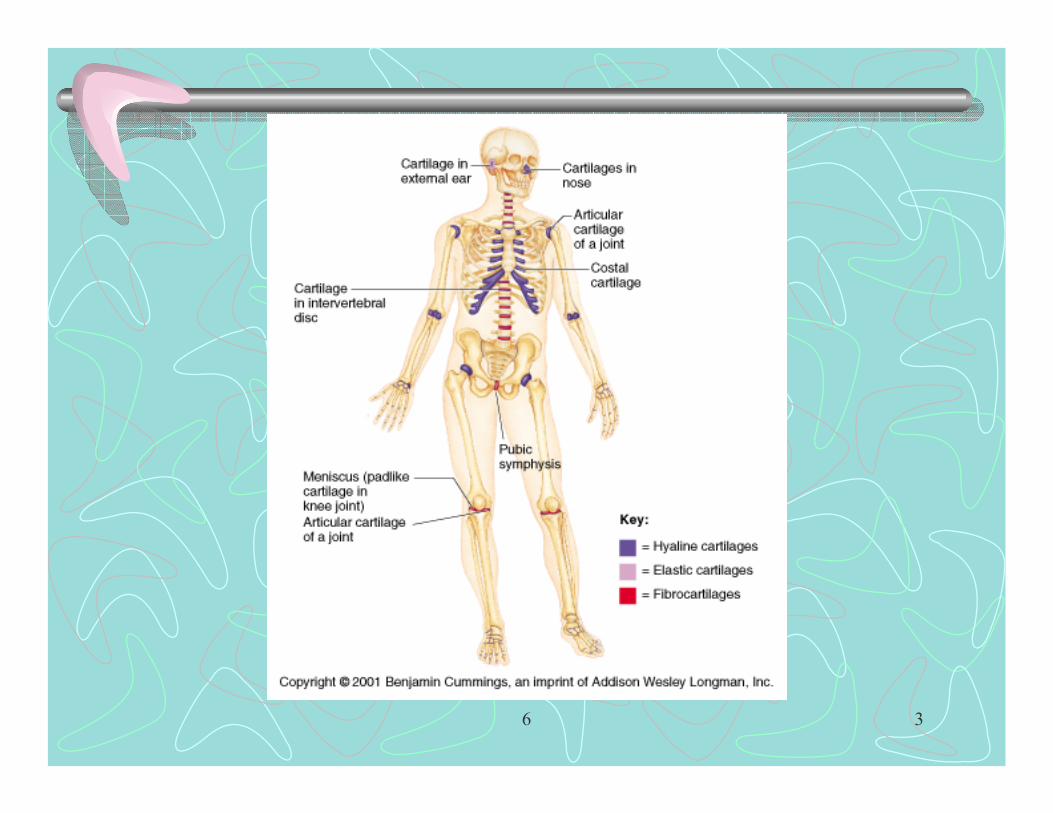
• Bones and Cartilages• Growth of cartilage:
– Appositional growth – growth from outside• Perichondrium chondroblasts secrete new matrix against
external face of cartilage– Interstitial growth – growth from inside
• Lacunae bound chondrocytes inside cartilage secrete new matrix
• Growth ceases when skeleton stops growing
6 3

6 4
6 5
Classification of bones• Axial vs. appendicular skeleton• 1 Long bones – significantly longer than wide
– All limb bones except patella, wrist & ankle bones– Diaphysis (shaft)– Two epiphyses (extremities) –proximal & distal
• Trabecular spaces filled with red bone marrow– Compact bone– Spongy bone (cancellous) – with trabeculae– Periosteum – 2 layers
• Fibrous layer – outer, dense irregular c.t. • Osteogenic layer – inner, osteoblasts & osteoclasts

6 6

6 7

6 8
Classification of bones• 1 Long bones – significantly longer than wide
– Medullary (bone marrow) cavity• Contains yellow bone marrow• Lined by trabeculae• Covered internally by endosteum – membrane containing
osteoblasts & osteoclasts – Articular cartilage – hyaline cartilage covers articular
surfaces– Epiphyseal line – between diaphysis & epiphysis
• Remnant of epiphyseal plate (hyaline cartilage) of growing bone– Nutrient foramen– Sharpey’s fibers

6 9
6 10
Classification of bones
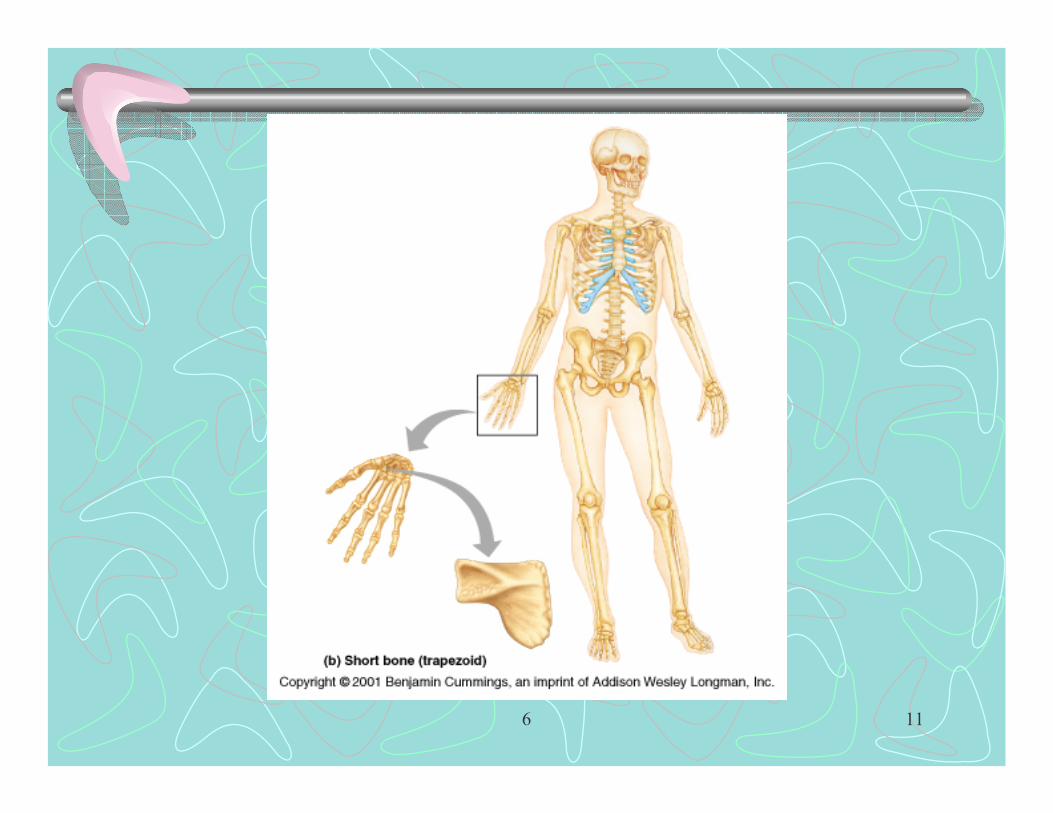
• 2 Short bones – length & width roughly equal– Wrist & ankle bones - ligament interconnections– No epiphysis, diaphysis or bone marrow cavity– Periosteum covering compact bone– Compact bone– Internal spongy bone with red bone marrow in
trabecular spaces
6 11

6 12
6 13
Classification of bones
• 3 Flat bones – 2 parallel plates of compact bone (inner & outer tables)– Internal layer of spongy bone (diploe) contains red bone
marrow– Calvarium, ribs, sternum
• 4 Irregular bones – match none of preceding categories– Vertebrae, ethmoid, sphenoid and os coxae bones– Spongy bone inside with red bone marrow

6 14
6 15

6 16
Functions of bones
• Supports body and provides form• Movement - used as levers to move body & its
parts• Protection of internal organs• Storage of minerals – Ca++, PO4
---
• Hemopoiesis (hematopoiesis) – blood cell formation –red bone marrow
6 17
Misc.
• Sesamoid bones – type of short bone formed within a tendon– Sesame seed shape– Patella
• Hemopoiesis in adult long bones:– Yellow bone marrow extends well into epiphyses
therefore, mainly carried out in heads of humerus & femur
6 18

6 19
Chemical Composition of Bone• Organic components:
– Of osteocytes, osteoblasts, osteoclasts –2%– Osteoid – an organic 1/3 of matrix
• Ground substance (proteoglycans & glycoproteins)• Collagenous fibers• Contribute flexibility & high tensile strength
• Inorganic components –2/3 of matrix– Hydroxyapatite – Ca10(PO4)6(OH)2 (a mineral)
• Crystals also incorporate CaCO3 & Na, Mg, F ions– Deposited around collagenous fibers
• Resists compression, but brittle

6 20

6 21
Bone Development
• Osteogenesis – process of bone tissue development
• Ossification – process of replacing other tissues with bone

6 22
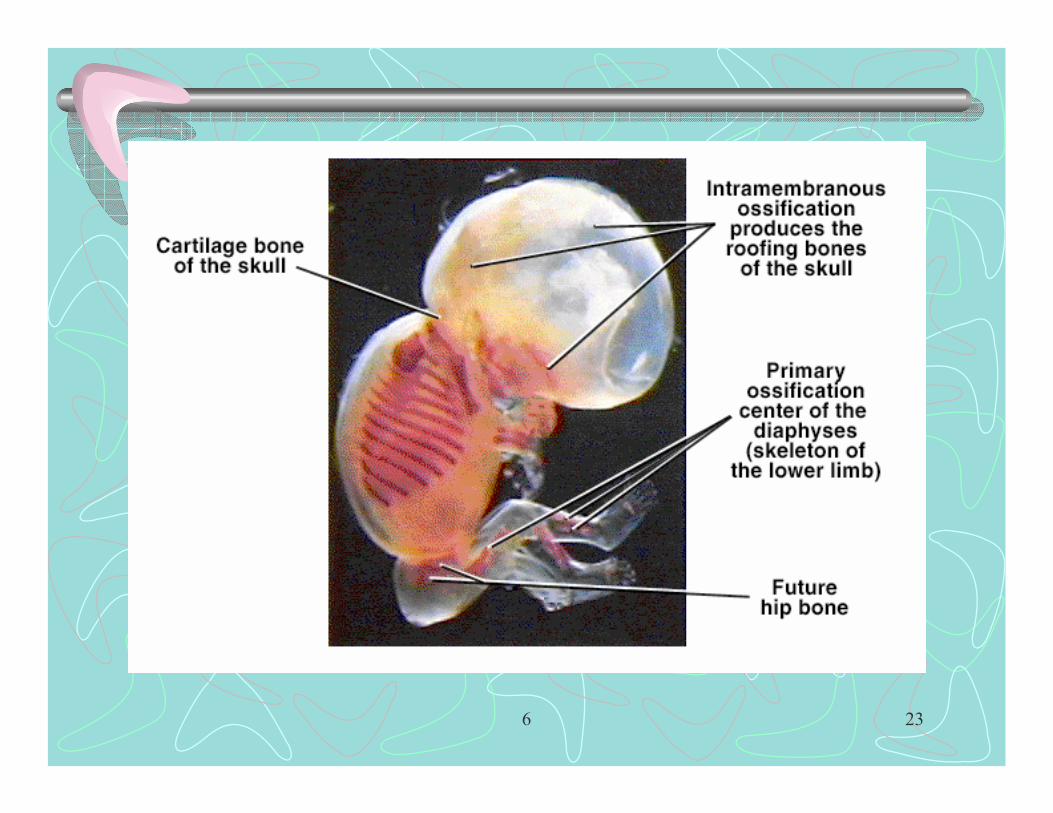
Formation of Bony Skeleton
• Before 8 weeks, embryo skeleton composed of fibrous membranes and cartilage
• At about 8 weeks ossification begins– Intramembranous ossification – from fibrous
tissue called mesenchyme– Endochondral ossification – from hyaline cartilage
6 23
6 24
6 25
Intramembranous Ossification
• Most bones of skull & clavicle, all are flat bones• Mesenchymal tissue – a fibrous embryonic c. t.
containing mesenchyme cells is the starting tissue
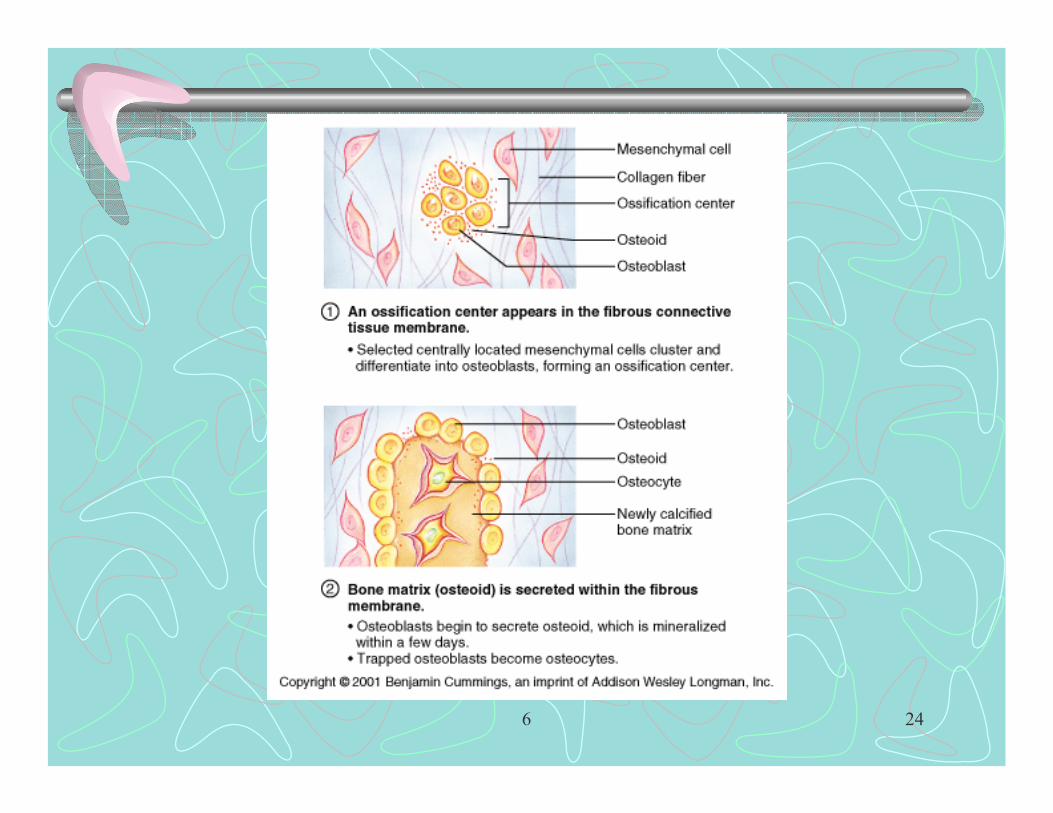
• Four Steps:– 1 An ossification center appears in mesenchyme
• Mesenchyme cells cluster and differentiate into osteoblast cells

6 26

6 27
Intramembranous Ossification
– 2 Osteoid, a bone matrix, is secreted into surrounding mesenchyme by osteoblasts
• Osteoid is mineralized within few days• Trapped osteoblast become osteocytes
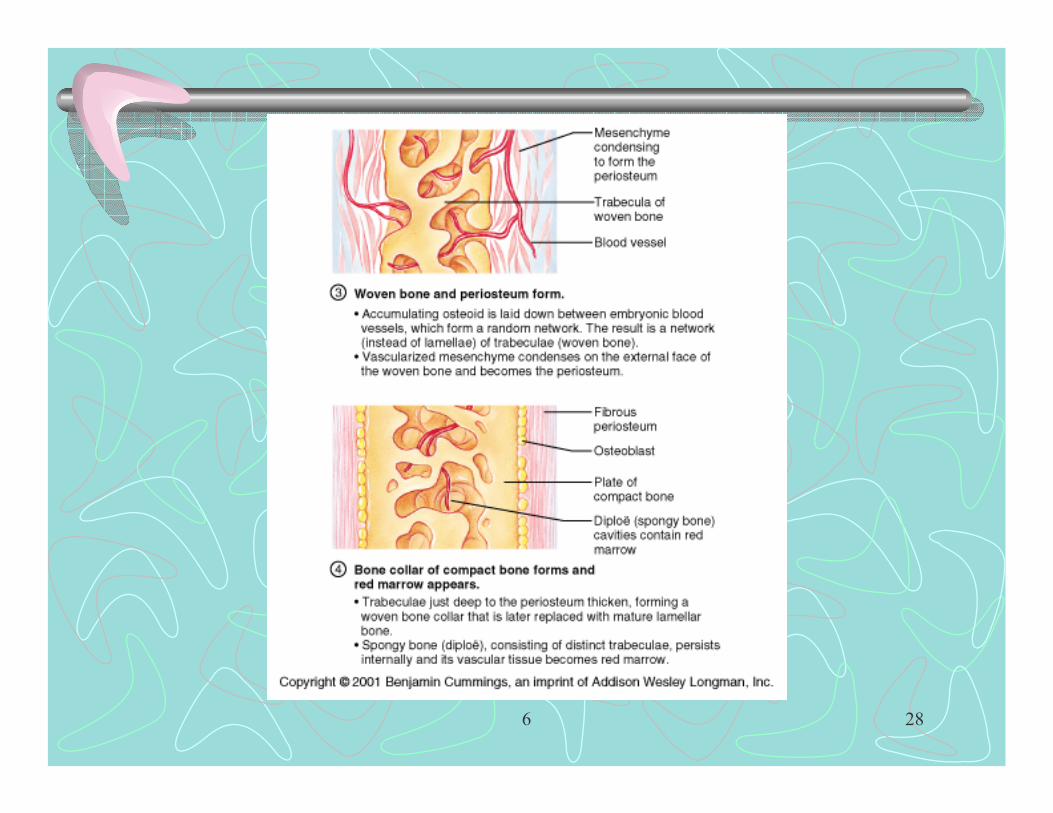
– 3 Woven bone & periosteum form• Osteoid is laid down between embryonic blood vessels
forming a random network of trabeculae (woven bone)• Vascularized mesenchyme condenses on external face of
woven bone forming the periosteum
6 28

6 29
Intramembranous Ossification• 4 Bone collar of compact bone forms and red marrow
appears– Trabeculae deep to periosteum thicken, forming a woven bone
collar» This is later replaced by lamellar bone
– Red marrow forms in vascularized diploe region

6 30

6 31
Endochondral Ossification
• All bones from base of skull down except clavicle• Begins in 2nd month of development• Uses hyaline cartilage as a model• Hyaline cartilage broken down as ossification
proceeds

6 32

6 33
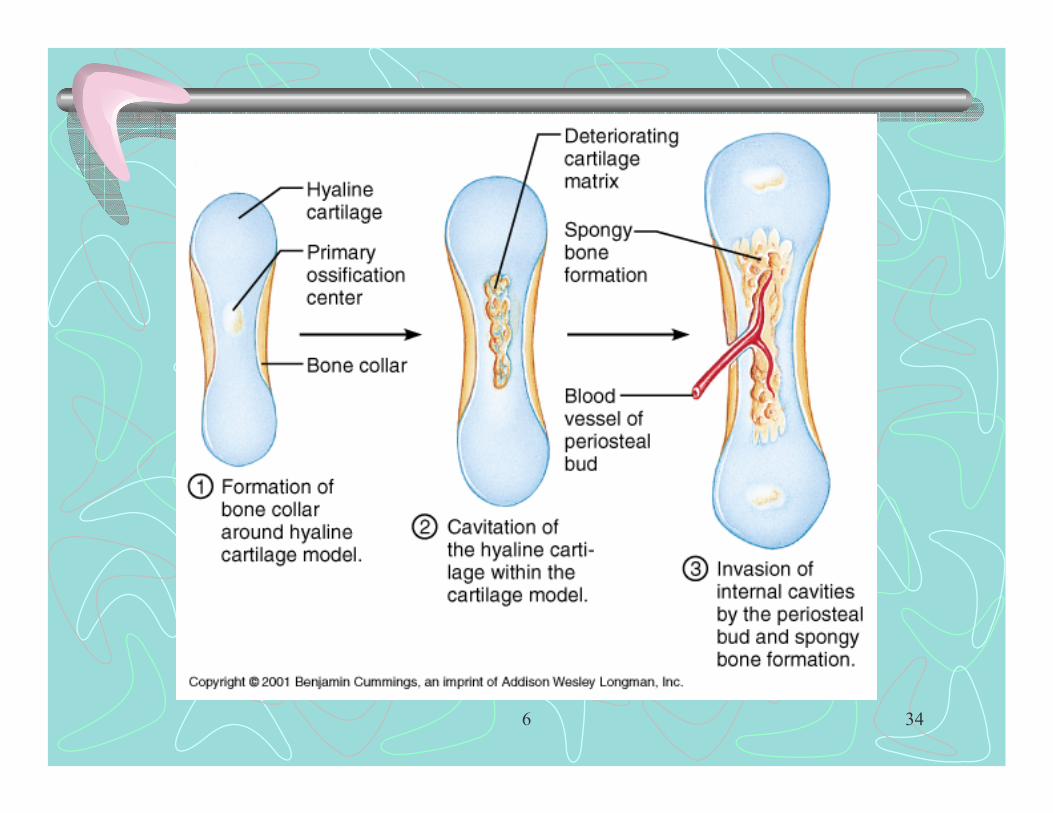
Steps in Endochondral Ossification
• 1 A bone collar forms around the diaphysis of hyaline cartilage model– Perichondrium converted by infiltration of blood
vessels to periosteum (change in differentiation of mensenchyme cells)
– Osteoblast secrete osteoid against outer surface of cartilage
6 34
6 35
Steps in Endochondral Ossification
• 2 Cartilage in center of diaphysis calcifies, forming 1o center of ossification and then cavitates– Chondrocytes hypertrophy (enlarge)– Hyaline cartilage becomes calcified cartilage
• Inadequate diffusion of nutrients chondrocytes die• Matrix deteriorates forms cavities
– Elsewhere cartilage is healthy & grows cartilage model elongates

6 36

6 37
Steps in Endochondral Ossification
• 3 Periosteal bud invades internal cavities and spongy bone forms– Periosteal bud composed of nutrient artery & vein,
lymphatics, nerve fibers, red marrow elements, osteoblasts & osteoclasts
• Osteoclasts erode calcified cartilage matrix• Osteoblasts secrete osteoid around remaining
fragments of calcified cartilage earliest spongy bone

6 38
6 39
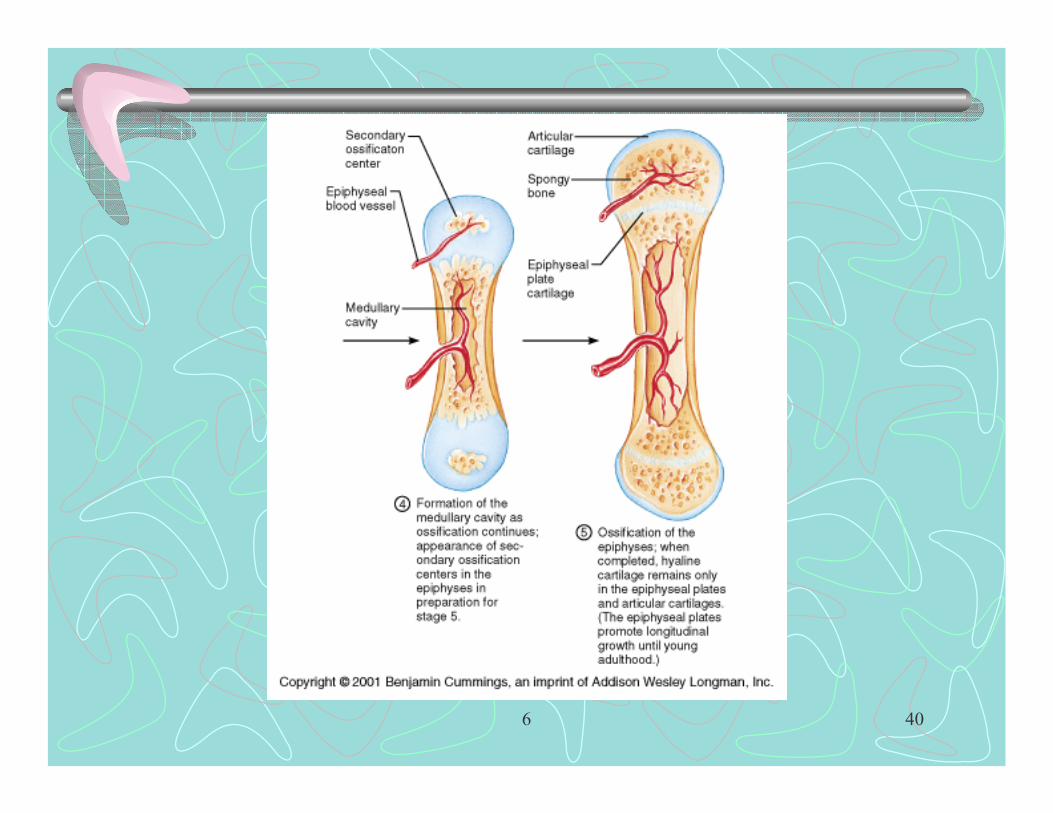
Steps in Endochondral Ossification
• 4 Diaphysis elongates & medullary cavity forms– 1o center elongates proximally & distally– At same time, osteoclast break down the newly formed
spongy bone medullary cavity– Throughout fetal period epiphyses consist of only rapidly
growing cartilage and model continues to elongate• Notice: on epiphyseal surfaces facing med.cav.
– Cartilage calcifying being eroded replaced by spicules
6 40

6 41
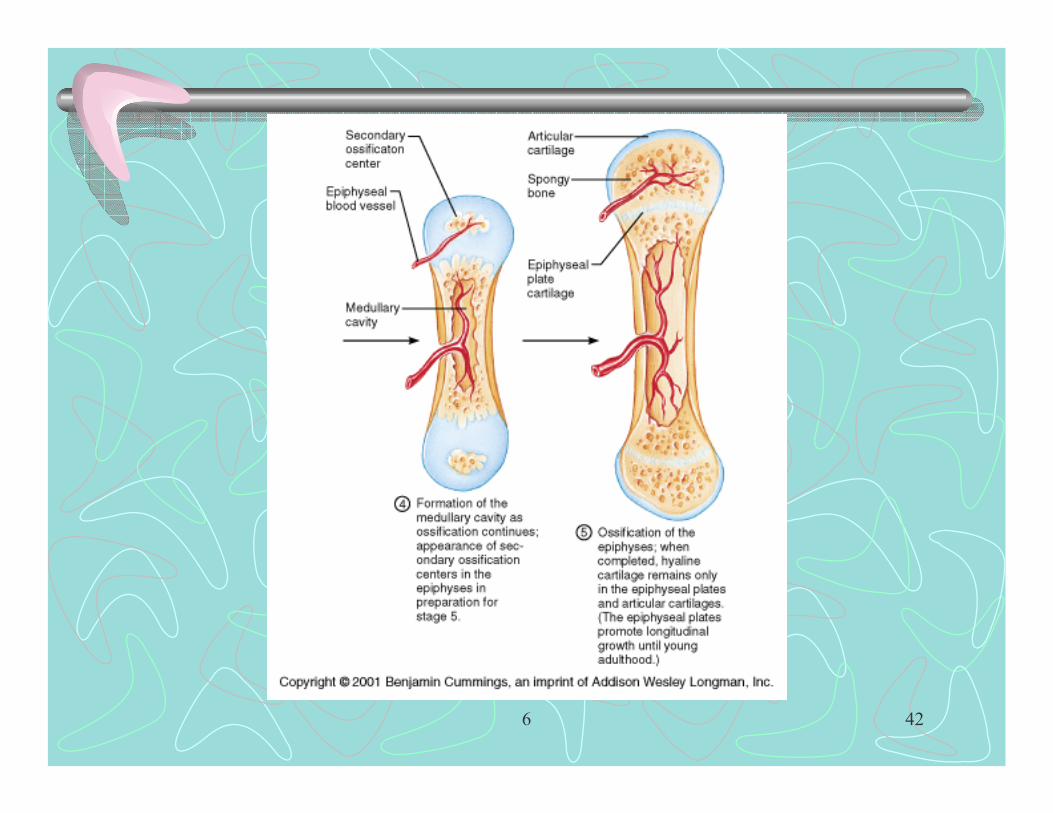
Steps in Endochondral Ossification• 5 The epiphyses ossify
– At birth most long bones are bony diaphysis surrounding remnants of spongy bone, a widening medullary cavity & 2 cartilagenous epiphyses
– Usually shortly after birth, 2o center of ossification appear• Cartilage in center of epiphysis calcifies then deteriorates creating
cavities that are invaded by new periosteal buds– Then changes as in 1o center occur, but with no medullary cavity
formed– When 2o ossification is complete the only cartilage remaining
is articular cartilage & epiphyseal plates (growth plates)
6 42

6 43
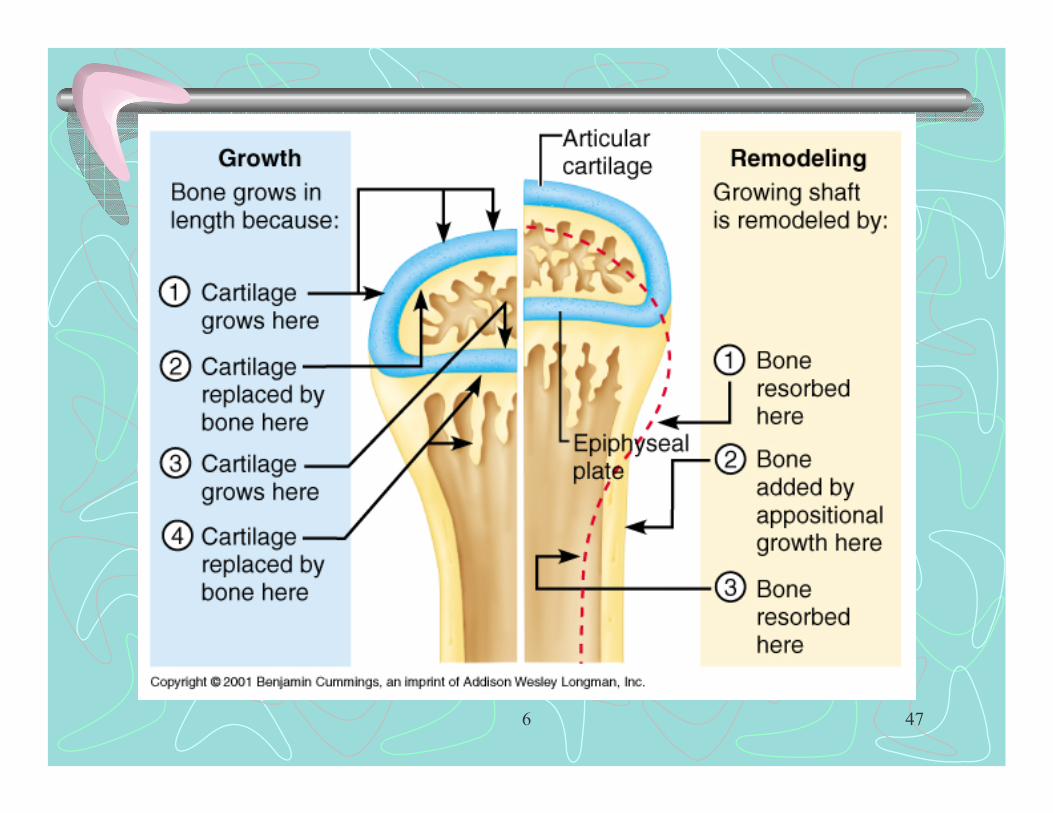
Growth in Length of Long Bones• Mimics events of endochondral ossification
– On epiphyseal side of epiphyseal plate cartilage is relatively inactive
– On shaft side of epiphyseal plate• Cartilage cells form a stack
– Growth Zone – cells undergo cell division– Transformation Zone – cells undergo hypertrophy, lacunae erode and
enlarge, matrix calcifies, cartilage cells die, matrix deteriorates leaving trabeculae
– Osteogenic Zone – invasion by marrow elements, further erosion by osteoclasts, osteoblast produce calcified osteoid
– During growth period epiphyseal plate is constant in thickness

6 44
6 45
Growth in Length of Long Bones
• Bone is constantly remodeled – both new bone formation & bone resorption
• Near end of growth in length – slowerchondroblast division, plate becomes thinner until replaced by bone
• Growth ceases with fusion of epi. and diaphyseal bone – synostosis– About 18 yrs. in female, 21 yrs. in male
6 46
Growth in Diameter of Long Bones
• By appositional growth– Osteoblast of periosteum secrete osteoid– Osteoclasts of endosteum remove bone, less than
new osteoblast activity however
6 47

6 48
Hormone Regulation of Bone Growth During Youth
• Epiphyseal activity during infancy & childhood:– Growth hormone(HGH) from anterior pituitary
• Gigantism – hypersecretion, dwarfism - hyposecretion– Thyroid hormones(T3 & T4) –modulate activity of
HGH – for proper proportions• Dwarfism - hyposecretion
• At puberty, sex hormones promote growth spurtand masculinization or feminization of skeleton– Later they induce synostosis
6 49
Factors affecting bone development:
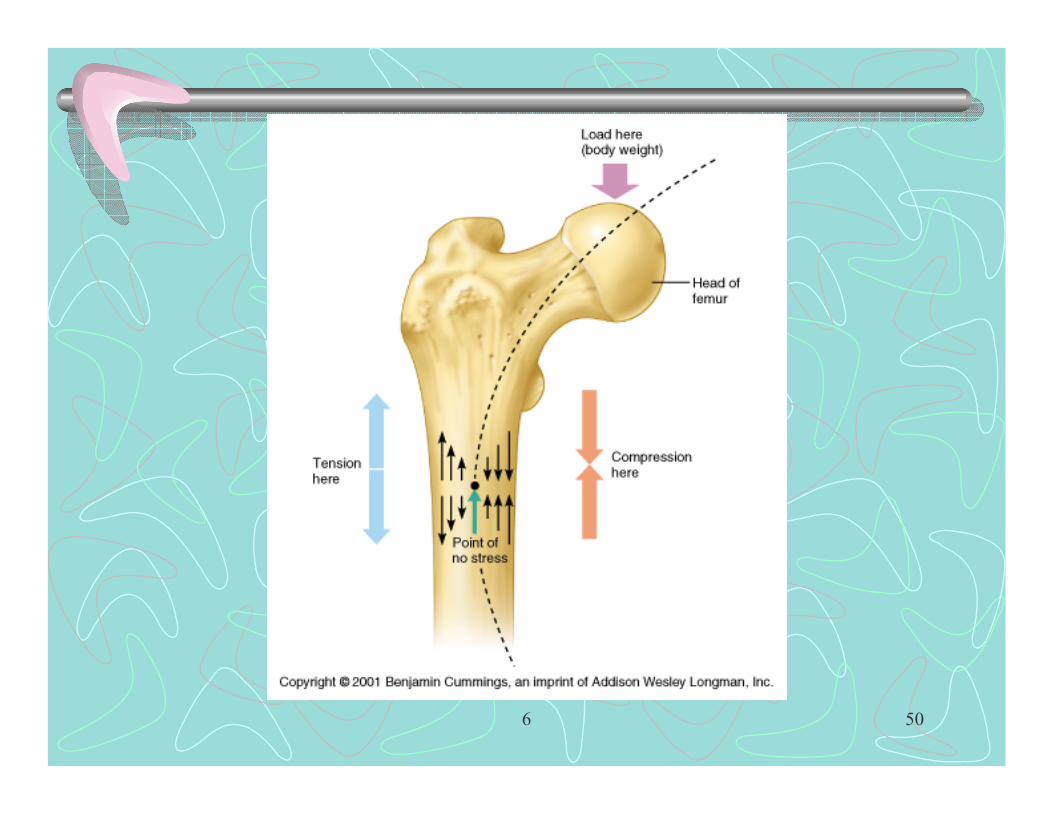
• Mechanical stress:• Wolff’s law – bone grows in response to forces
placed on it (compression vs. tension)– Thickest where bending stress is greatest– Gravitational (supporting weight) & muscle pull– Increased stress minute electrical field
attract osteoblasts increased bone formation– Decreased stress Ca++ resorption
6 50
6 51
Factors affecting bone development:
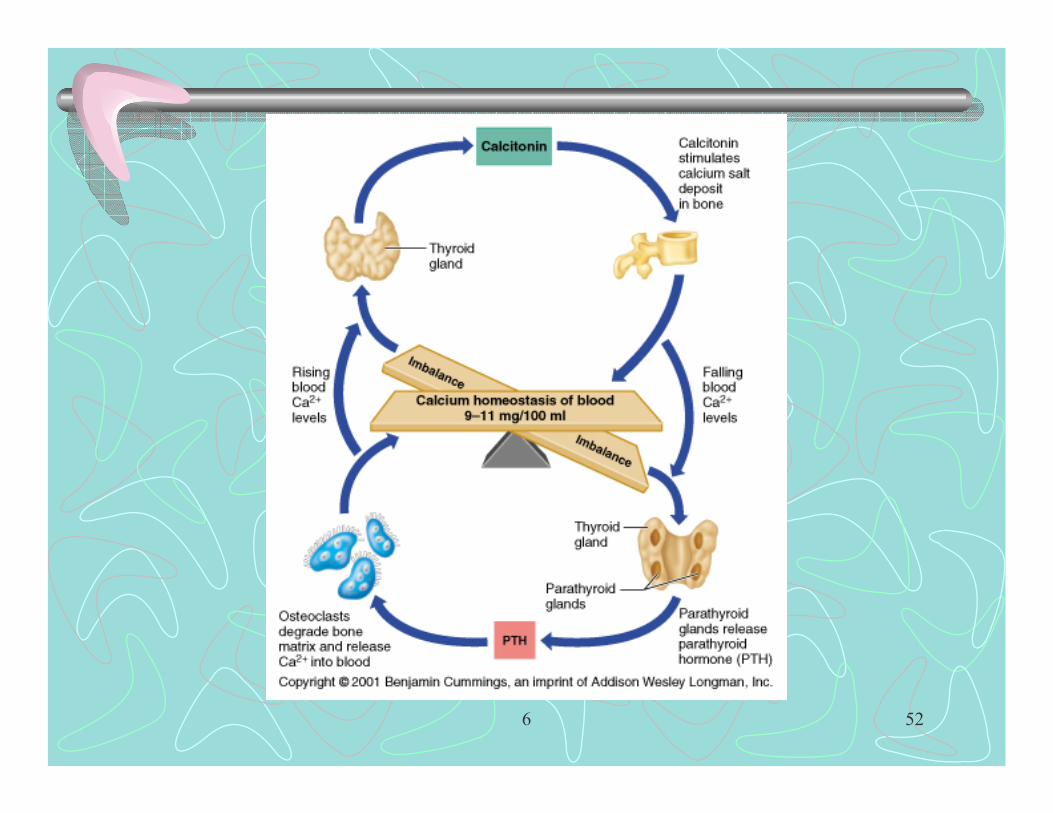
• Increased parathormone from parathyroid glands – increases osteoclast activity
• Increased calcitonin from thyroid gland decreases osteoclast activity
Ca++ of bone Ca++ of blood
Ca++ excretion Ca++ excretion parathormone
calcitonin
6 52
6 53
Factors affecting bone development:
• Nutritional:– Vitamin D – required for kidney production of
calcitriol (Increased absorption of Ca++ from intestinal lumen)
– Vitamin C – for collagen synthesis– Vitamin A – for balance between Ca++ deposit in &
removal from bone– Healthy diet rich in protein

6 54
Fractures (broken bones)
• Types:– Nondisplaced - bone ends retain normal position– Displaced – bone ends out of normal alignment– Complete – broken through vs. incomplete– Compound (open) – bone ends penetrate skin vs.
simple (closed)– Linear – parallel to long axis– Transverse – perpendicular to long axis
6 55
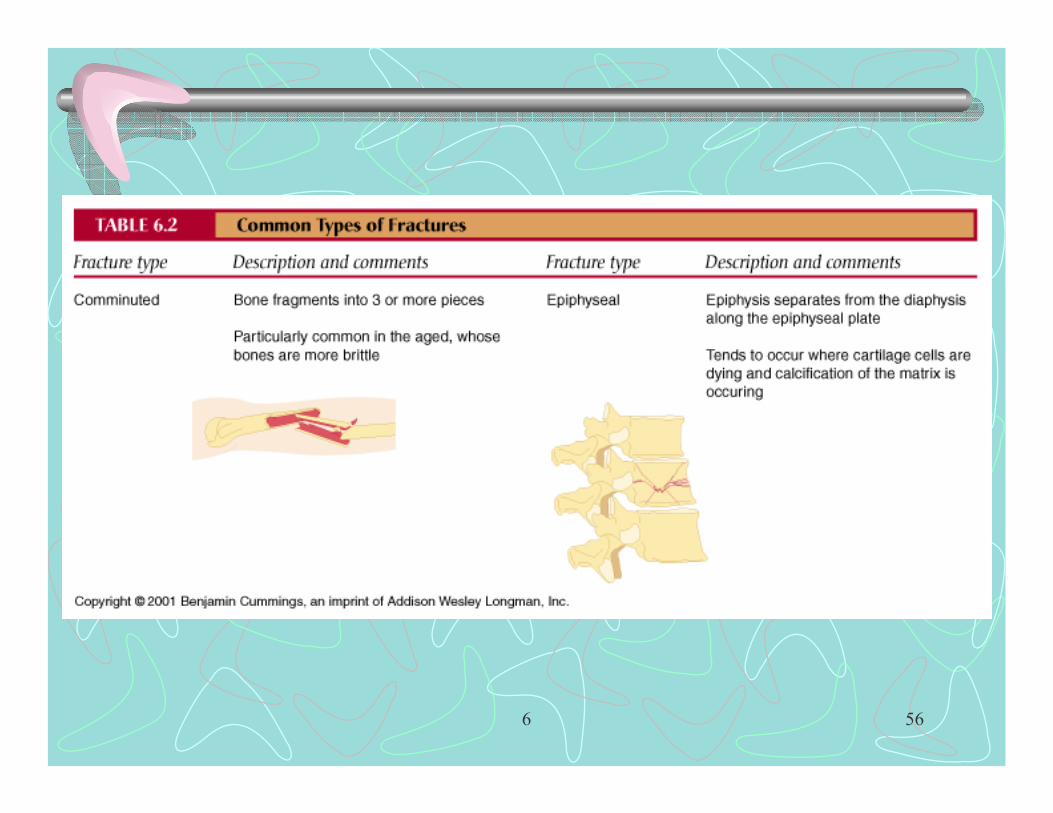
Fractures (broken bones)
• Types cont.’d:– Comminuted – 3 or more pieces at break site– Compression (impacted) – bone is crushed– Oblique – oblique angle across bone long axis– Spiral –– Depressed – broken region pushed inward, skull– Green-stick – break in convex surface, not all the
way through
6 56

6 57

6 58

6 59
Fractures (broken bones)
• Types cont.’d:– Colle’s – break at distal end of radius– Pott’s – malleoli of tibia & fibula, skiing accidents
• Displacement of talus, pinning• Treatments:
– Reduction - realignment of broken bone ends• Closed – bone ends coaxed into position by hands• Open – bone ends secured together surgically by pins or
wires

6 60
6 61
4 Stages in healing of bone fracture• 1 Hematoma formation – mass of clotted blood forms,
bone cells at site die, inflammation occurs• 2 Fibrocartilaginous callus formation –
– Granulation tissue forms –capillaries grow into hematoma, phagocytic cells invade & remove debris
• Fibroblasts & osteoblasts migrate into fracture site from periosteum & endosteum – begin reconstruction
– Fibroblasts produce collagenous fibers that span break, some differentiate into chondroblasts – secrete cart. Matrix
– Osteoblasts begin spongy bone formation, farthest from blood supply a cart. Bulge
• Note: internal & external callus

6 62
6 63
4 Stages in healing of bone fracture
• 3 Bony callus formation – Bone trabeculae begin to appear in fibrocartilaginous callus (3 to 4 wks. after injury continuing for 2-3 months)
• 4 Bone remodeling – last several months– Removal of excess material– Formation of compact bone
6 64
Rickets & Osteomalacia
• Deficiency of Vitamin D, demineralization & softening of bone– Rickets – in children, bowed-legs, knock-kneed,
rosary beads, pigeon breast– Osteomalacia – in adults
• Treatment: oral Ca & I.V. Vitamin D

6 65
Osteoporosis (“porous” bone)• Demineralization of bone (resorption exceeds bone
deposition)• Most common in postmenopausal women, in 50’s
– Estrogen deficiency – females– Androgen deficiency – males
• Other causes: immobilization, excess glucocorticoids, liver disease, osteoclast activating factor from some cancer cells, smoking ( reduces estrogen levels), hyperthyroidism, diabetes mellitus
6 66
Osteoporosis (“porous” bone)• Treatments & or prevention:
– Ca & Vit. D – Increased wt. Bearing– HRT hormone (estrogen) replacement therapy) – slows, but
does not reverse loss– Fosamax – depresses osteoclast activity –reverses
osteoporosis of spine– Evista – mimics estrogen without targeting uterus or breast– Soy protein – estrogenic compounds ( isoflavones &
genistein)– Fluoridated water

6 67
Misc.
• Paget’s Disease –excessive bone formation & breakdown (Pagetic bone)– High ratio of woven to compact bone– 3% of N.A. elderly, after age 40, distemper virus
• Electrical stimulation of fractures• Pulsed ultrasound treatments• Bone substitutes: Norian SRS

6 68
Bone development:
• Mesoderm mesenchymal tissue fibrous C.T. or cartilage (embryonic skeleton)
• Most long bones begin ossification by 8 wks.• Obvious 1o ossification centers by 12 wks.• At birth most long bones well ossified, except on
epiphyses• At 25 yrs. all bones completely ossified

6 69

6 70

















