79
Cáncer de ovario y BRCA Abriendo un nuevo camino Dra. Yolanda García Oncología Médica Parc Taulí Sabadell. Hospital Universitari Panticosa, 15 Mayo 2015
Cáncer de ovario y BRCA
Abriendo un nuevo camino Dra. Yolanda García
Oncología Médica
Parc Taulí Sabadell. Hospital Universitari
Panticosa, 15 Mayo 2015
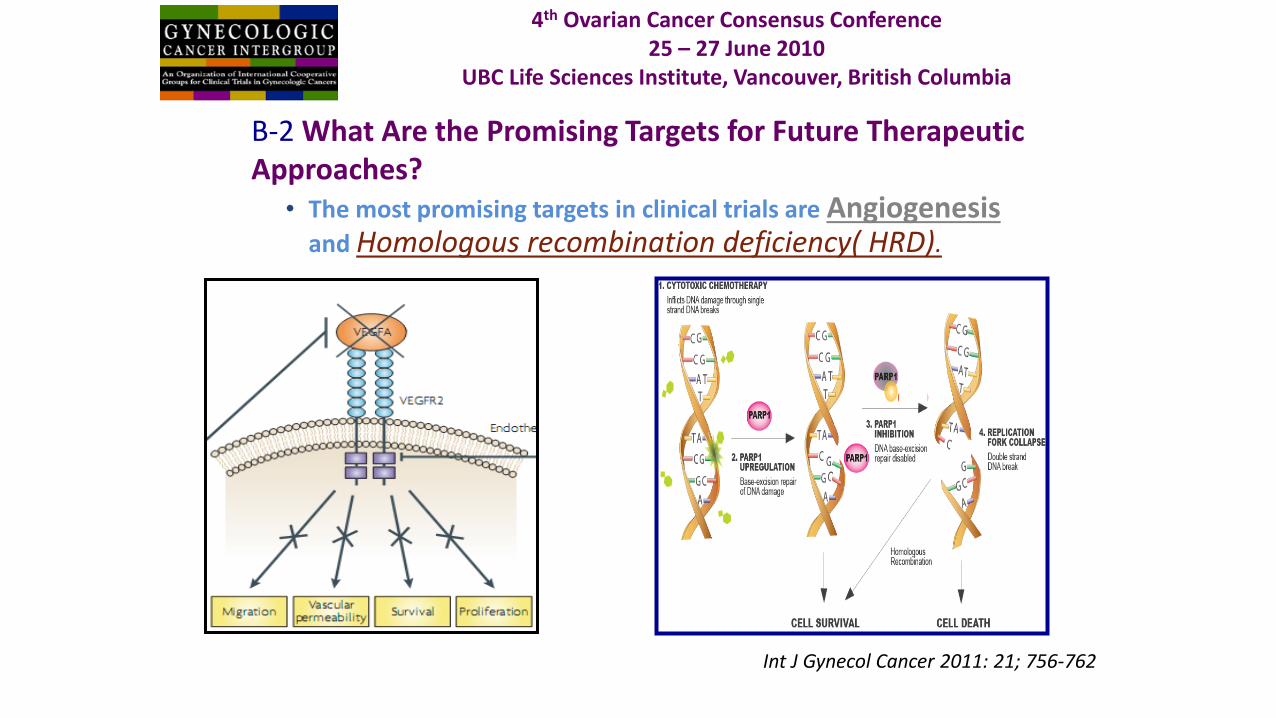
B-2 What Are the Promising Targets for Future Therapeutic Approaches?
• The most promising targets in clinical trials are Angiogenesis and Homologous recombination deficiency( HRD).
Int J Gynecol Cancer 2011: 21; 756-762
4th Ovarian Cancer Consensus Conference 25 – 27 June 2010
UBC Life Sciences Institute, Vancouver, British Columbia
BRCAness HDR
Letalidad sintética
Mecanismo de acción iparp
Iparp’s en cáncer de
ovario
Olaparib
Veliparib Niraparib Rucaparib
BMN 673
Logística
Guías
Futuro
BRCAness HDR
Letalidad sintética
Mecanismo de acción iparp
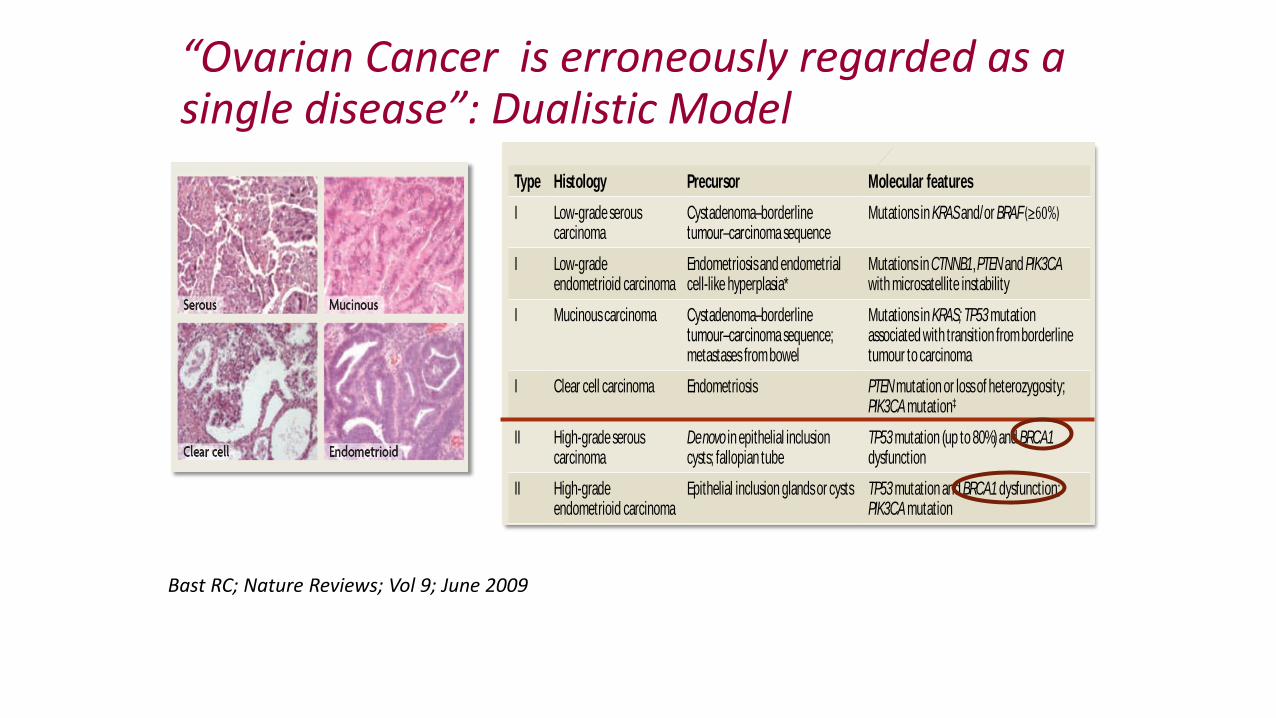
“Ovarian Cancer is erroneously regarded as a single disease”: Dualistic Model
apoptosis and induce angiogenesis. Nuclear localization
of activated phosphorylated STAT3 occurs in more than
70% of ovarian cancers and is associated with decreased
overall survival61. Activated STAT3 also translocates to
focal adhesion complexes and stimulates motility in
combination with SRC . In addition to antibodies against
IL-6 and inhibitors of JAK2 (REFS 62,63), new inhibitors
of STAT3 are being developed that might be used to tar-
get most ovarian cancers64.
Lysophosphatidic acid (LPA) is produced by the
phosphodiesterase autotoxin (ATX; also known as lyso-
phospholipase D). The G protein-linked LPA receptors
LPAR2 and LPAR3 are upregulated during the malignant
transformation of ovarian surface epithelial cells. LPAR3
responds to LPAs with unsaturated fatty acyl chains that
are produced by ovarian cancers. Interestingly, cyclic
phosphatidic acid blocks ATX, reducing LPA levels and
metastasis, but not the growth of primary cancers65. LPA-
neutralizing antibodies have been developed, and LPA
receptor inhibitors are being sought that might block the
proliferation of ovarian cancer cells66.
The NF-κB transcription factor is constitutively acti-
vated in more than half of ovarian cancers67,68 through
signalling initiated by several cytokines (IL-1 and TNFα)
and growth factors (EGF). Inactive NF-κB is complexed
with inhibitor of NFκB (IκB) and is generally activated
by the IκB kinase (IKK) complex, which contains two
kinase subunits (IKKα and IKKβ) and a regulatory
subunit (IKKγ)69. MEKK3 is one of several kinases that
can activate the IKK complex70,71 and is overexpressed
in >50% of ovarian cancers. The resultant activation of
NF-κB upregulates anti-apoptotic genes (for example,
CFLAR), antioxidant proteins (superoxide dismutase or
ferritin heavy chain), growth regulatory cytokines (IL-6
or growth regulated-α (GRO1)) and angiogenic factors
(IL-8)71. Selective inhibition of NF-κB has been difficult
to achieve, but gene therapy with adenoviral E1A reduces
NF-κB signalling and increases sensitivity to paclitaxel in
xenograft models, which has prompted a clinical trial at
the University of Texas M. D. Anderson Cancer Center of
liposomal E1A in combination with paclitaxel in patients
with intra-abdominal recurrence of ovarian cancer.
Tumour biologyProliferation. The fraction of cycling cells in different
ovarian cancers varies over a wide range from 1% to 79%
(REF. 72). Upregulation of cyclin D1 or E1, E2F1 or cyclin-
dependent kinases (CDK2), and downregulation of CDK
inhibitors (p16, p21 and p27) have been observed in a
fraction of ovarian cancers, and the levels of cyclins and
CDKs correlate with prognosis73,74. In addition to intrin-
sic deregulation of checkpoints in the cell cycle, a range of
autocrine and paracrine growth factors stimulate ovarian
cancer proliferation, including EGF, transforming growth
factor-α (TGFα), amphiregulin, heregulin, VEGFA, insu-
lin-like growth factor 1 (IGF1), IL-6 and LPA.
In normal ovarian surface epithelial cells, autocrine
growth inhibition is maintained by TGFβ75. In approxi-
mately 40% of ovarian cancers, expression of or respon-
siveness to TGFβ is lost. Although mutation of SMAD4
is sometimes observed, TGFβRI and TGFβRII receptors
are generally intact, as is Smad signalling downstream of
the receptors. Loss of growth inhibition and increased
invasiveness might relate to ecotropic viral integration
Box 3 | Molecular classif icat ion of epithelial ovarian cancers
PTEN α PIK3CA
KRAS BRAF CTNNB1 TP53
TP53
BRCA1 BRCA2
Type Histology Precursor Molecular features
I Low-grade serous carcinoma
Cystadenoma–borderline tumour–carcinoma sequence
Mutations in KRAS and/or BRAF
I Low-grade endometrioid carcinoma
Endometriosis and endometrial cell-like hyperplasia*
Mutations in CTNNB1, PTEN and PIK3CA with microsatellite instability
I Mucinous carcinoma Cystadenoma–borderline tumour–carcinoma sequence; metastases from bowel
Mutations in KRAS; TP53 mutation associated with transition from borderline tumour to carcinoma
I Clear cell carcinoma Endometriosis PTEN mutation or loss of heterozygosity; PIK3CA mutation‡
II High-grade serous carcinoma
De novo in epithelial inclusion cysts; fallopian tube
TP53 mutation (up to 80%) and BRCA1 dysfunction
II High-grade endometrioid carcinoma
Epithelial inclusion glands or cysts TP53 mutation and BRCA1 dysfunction; PIK3CA mutation
* Endometriosis and adjacent low-grade endometrioid carcinoma share common genetic events such as loss of heterozygosity at the same loci involving the same allele (for example, PTEN). By contrast, high-grade and poorly differentiated endometrioid carcinomas are similar to high-grade serous carcinomas. ‡ PIK3CA at 3q26 encodes the p110 catalytic subunit of PI3K19.
REVIEWS
422 | JUNE 2009 | VOLUM E 9 www.nature.com/reviews/cancer
Bast RC; Nature Reviews; Vol 9; June 2009
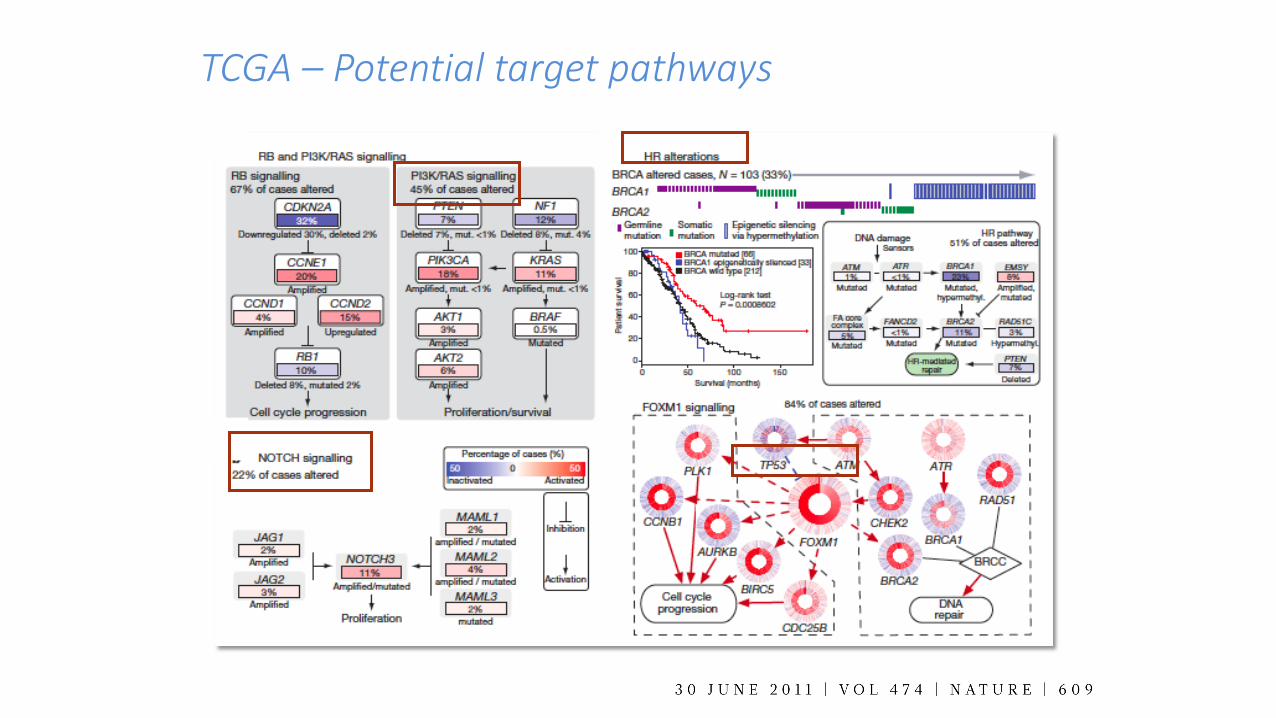
TCGA – Potential target pathways

TCGA – Potential target pathways
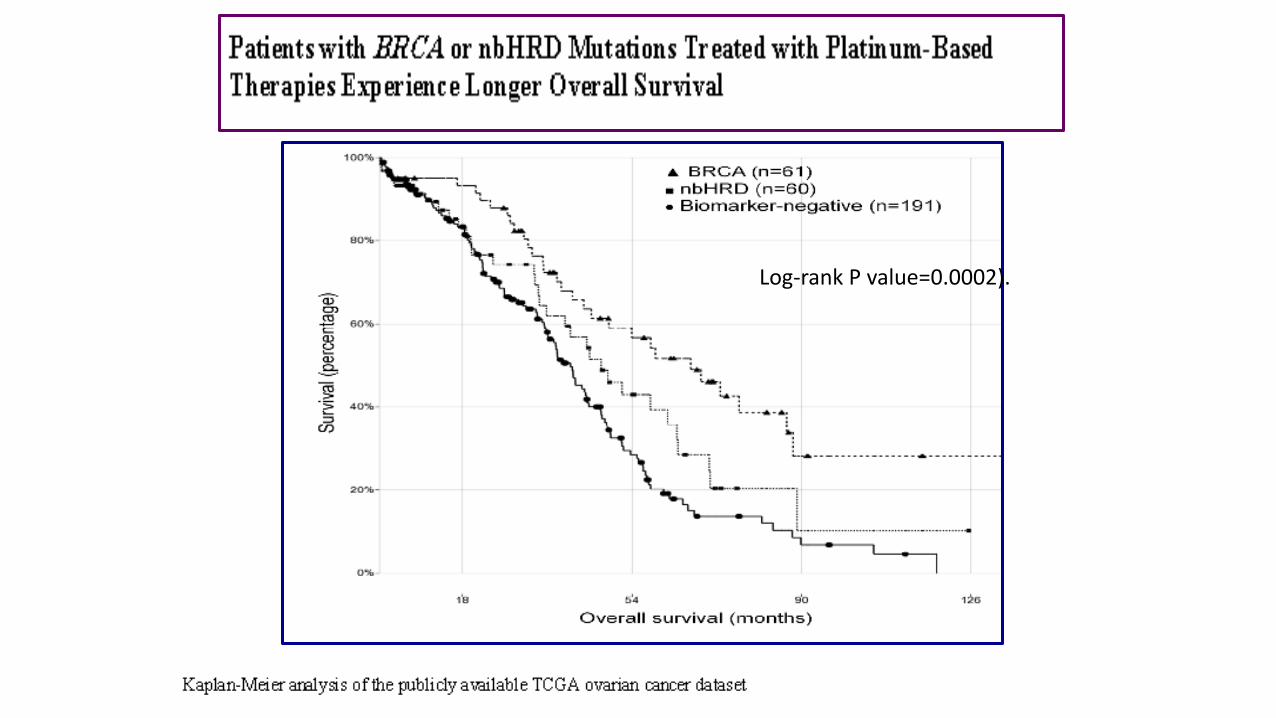
Log-rank P value=0.0002).
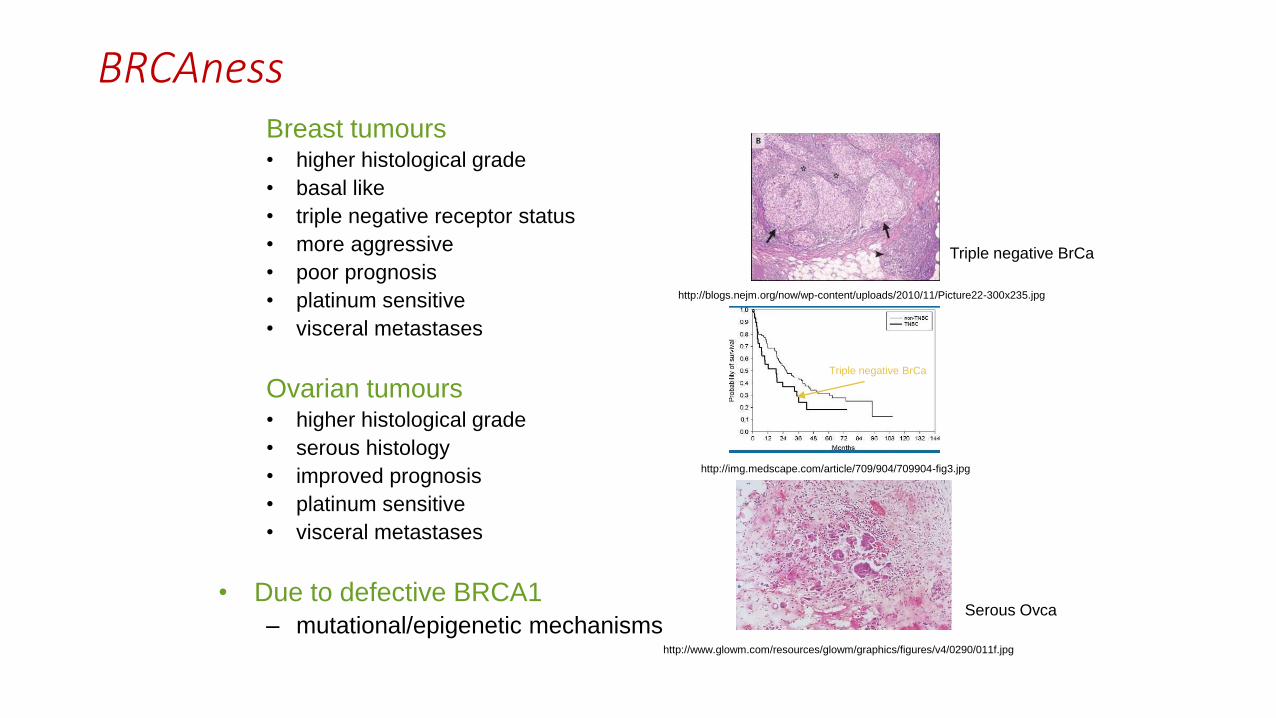
Breast tumours • higher histological grade
• basal like
• triple negative receptor status
• more aggressive
• poor prognosis
• platinum sensitive
• visceral metastases
Ovarian tumours • higher histological grade
• serous histology
• improved prognosis
• platinum sensitive
• visceral metastases
• Due to defective BRCA1
– mutational/epigenetic mechanisms
http://img.medscape.com/article/709/904/709904-fig3.jpg
http://blogs.nejm.org/now/wp-content/uploads/2010/11/Picture22-300x235.jpg
http://www.glowm.com/resources/glowm/graphics/figures/v4/0290/011f.jpg
Triple negative BrCa
Triple negative BrCa
Serous Ovca
BRCAness
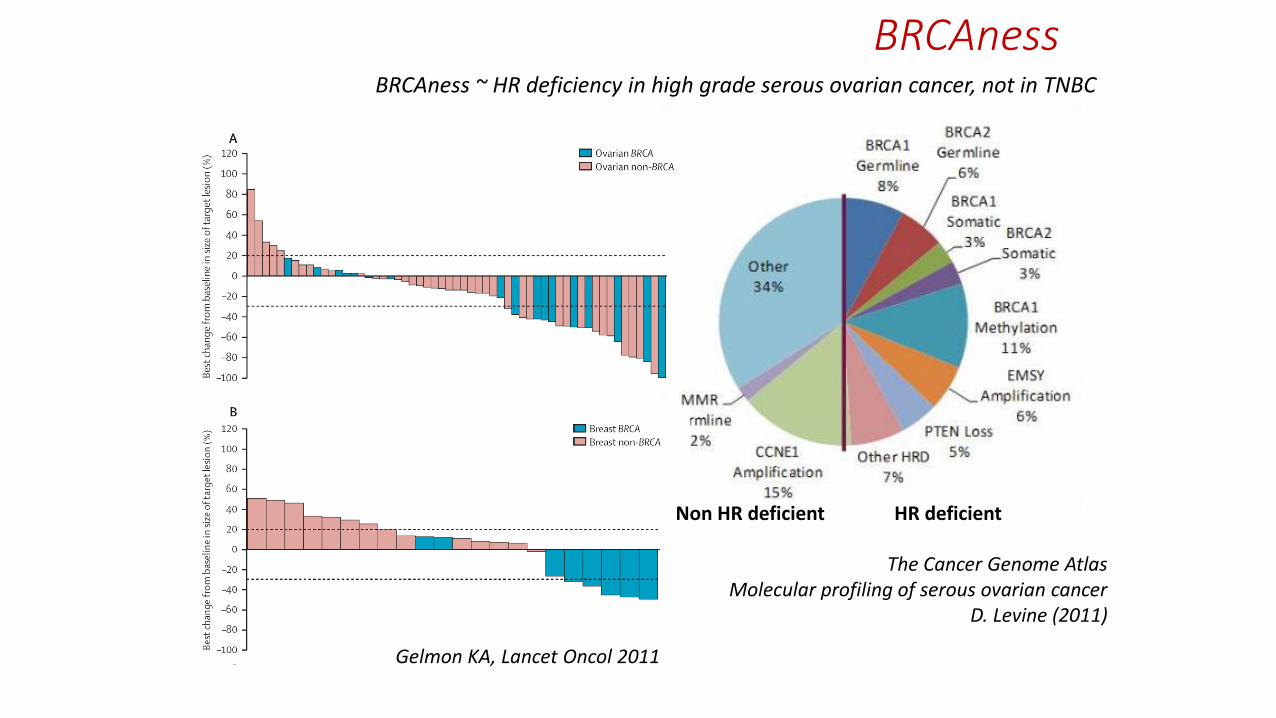
BRCAness BRCAness ~ HR deficiency in high grade serous ovarian cancer, not in TNBC
The Cancer Genome Atlas Molecular profiling of serous ovarian cancer
D. Levine (2011)
Gelmon KA, Lancet Oncol 2011
Non HR deficient HR deficient
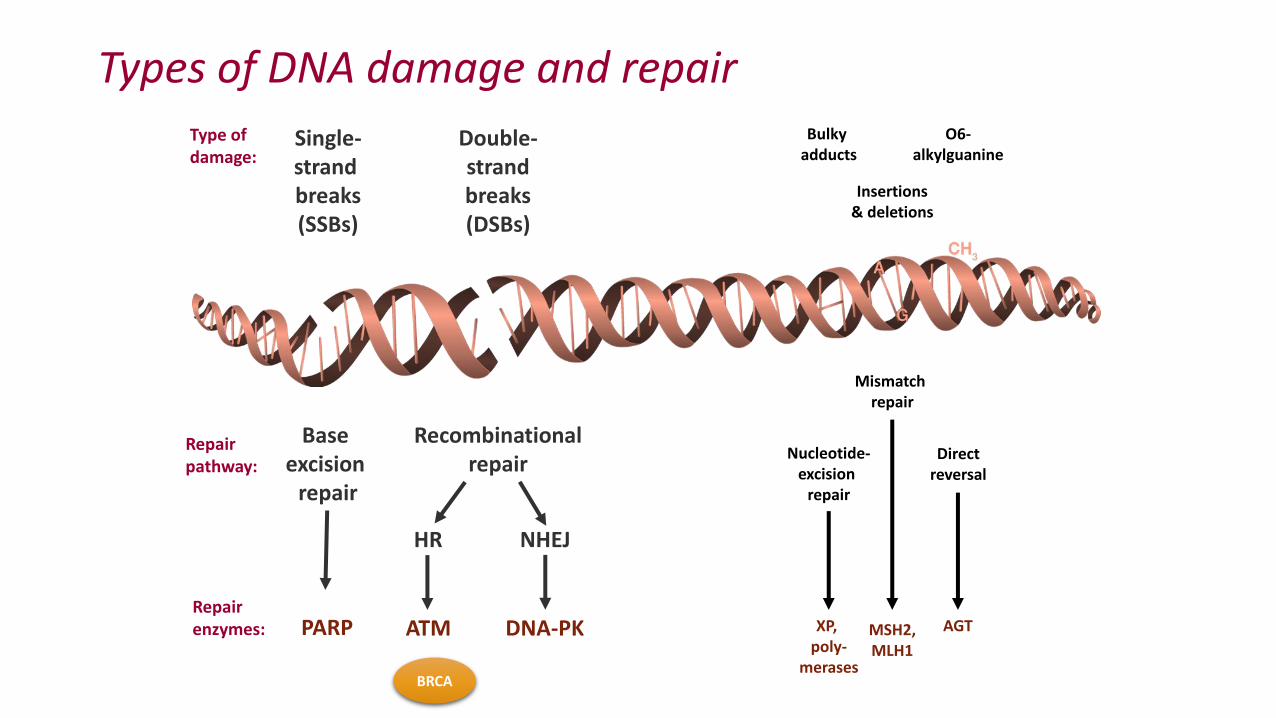
Base excision
repair
Type of damage:
Bulky adducts
Insertions & deletions
O6- alkylguanine
Repair pathway:
Nucleotide- excision
repair
Mismatch repair
Direct reversal
Repair enzymes:
Double- strand breaks (DSBs)
Single- strand breaks (SSBs)
PARP
Recombinational repair
ATM DNA-PK
HR NHEJ
XP, poly-
merases
MSH2, MLH1
AGT
Types of DNA damage and repair
BRCA
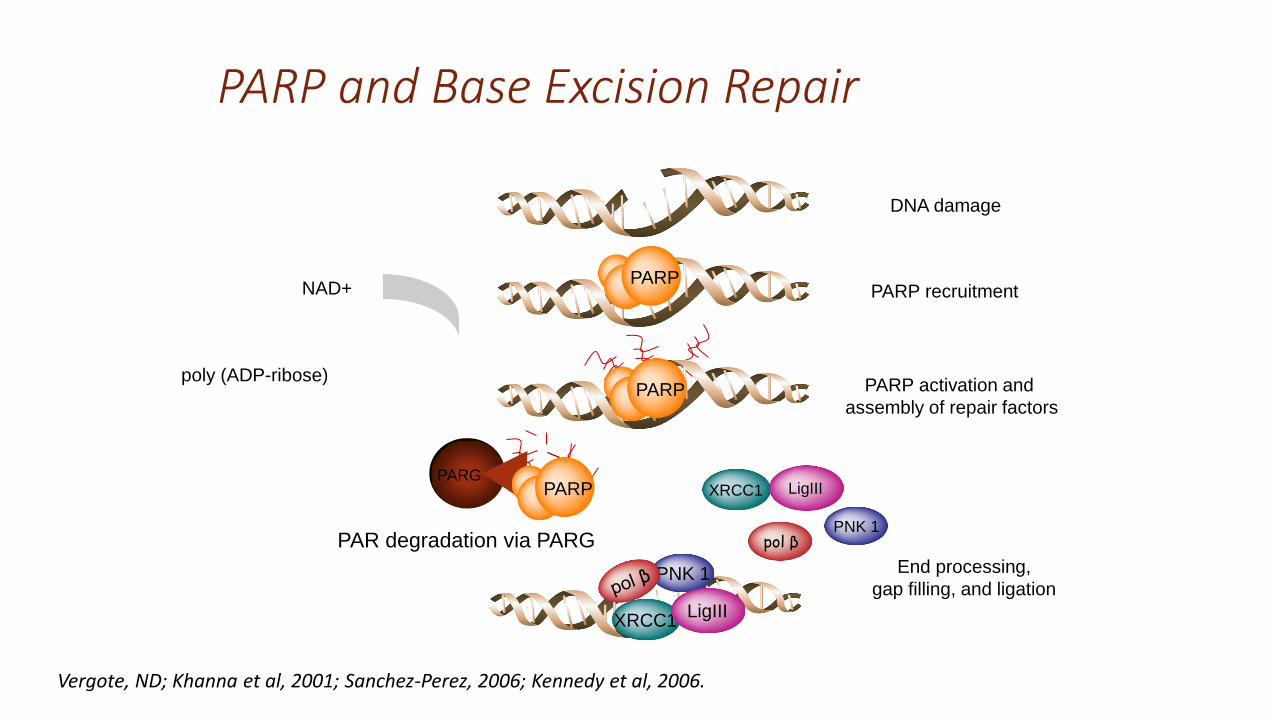
PARP recruitment PARP
DNA damage
PARP activation and
assembly of repair factors
NAD+
poly (ADP-ribose) PARP
PAR degradation via PARG
PARG
PARP
End processing,
gap filling, and ligation PNK 1
XRCC1 LigIII
pol β
XRCC1 LigIII
PNK 1
Vergote, ND; Khanna et al, 2001; Sanchez-Perez, 2006; Kennedy et al, 2006.
PARP and Base Excision Repair

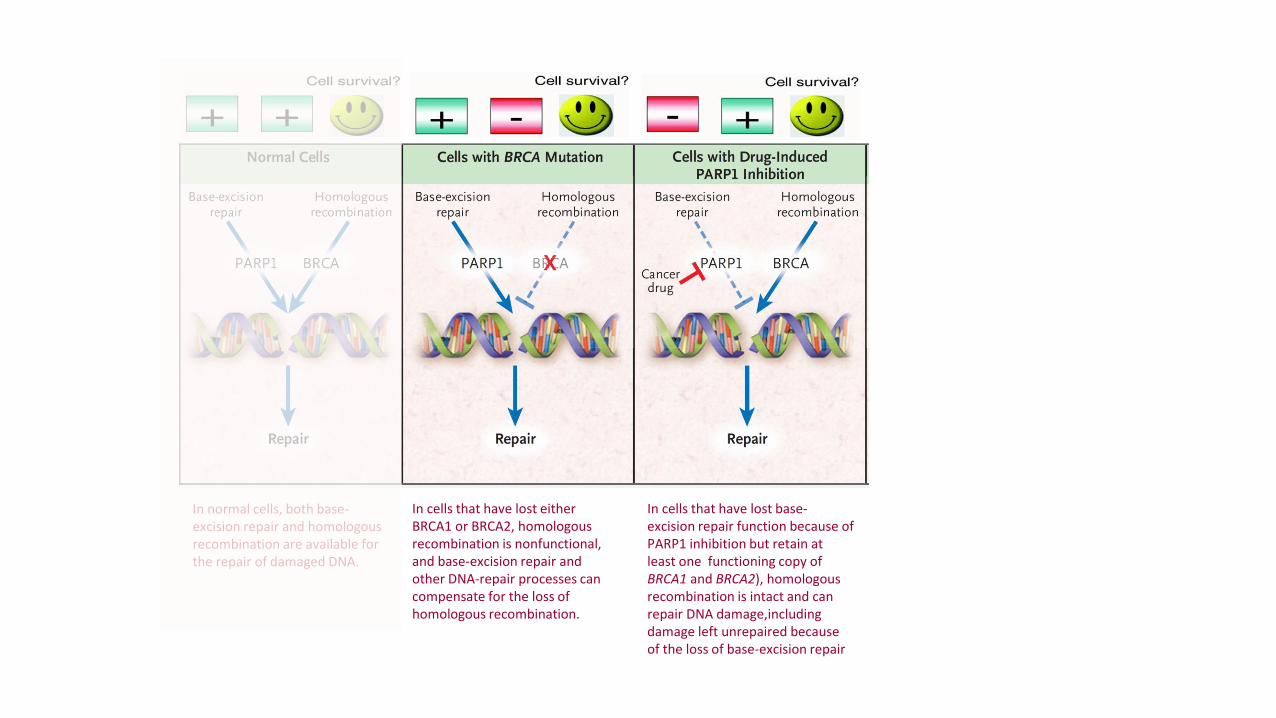
In normal cells, both base-excision repair and homologous recombination are available for the repair of damaged DNA.
In normal cells, both base-excision repair and homologous recombination are available for the repair of damaged DNA.
In cells that have lost either BRCA1 or BRCA2, homologous recombination is nonfunctional, and base-excision repair and other DNA-repair processes can compensate for the loss of homologous recombination.
In cells that have lost base-excision repair function because of PARP1 inhibition but retain at least one functioning copy of BRCA1 and BRCA2), homologous recombination is intact and can repair DNA damage,including damage left unrepaired because of the loss of base-excision repair

In the cancer cells of mutation carriers, all BRCA1 or BRCA2 function is absent, and when PARP1 is inhibited, cancer cells are unable to repair DNA damage by homologous recombination or base-excision repair, and cell death results.
In normal cells, both base-excision repair and homologous recombination are available for the repair of damaged DNA.
In cells that have lost either BRCA1 or BRCA2, homologous recombination is nonfunctional, and base-excision repair and other DNA-repair processes can compensate for the loss of homologous recombination.
In cells that have lost base-excision repair function because of PARP1 inhibition but retain at least one functioning copy of BRCA1 and BRCA2), homologous recombination is intact and can repair DNA damage,including damage left unrepaired because of the loss of base-excision repair

SYNTHETIC LETHALITY
“Situation when a mutation in one of two gens individually has no effect but combining the mutations leads to cell death”.
T Dobzhansky, Genetics 1946
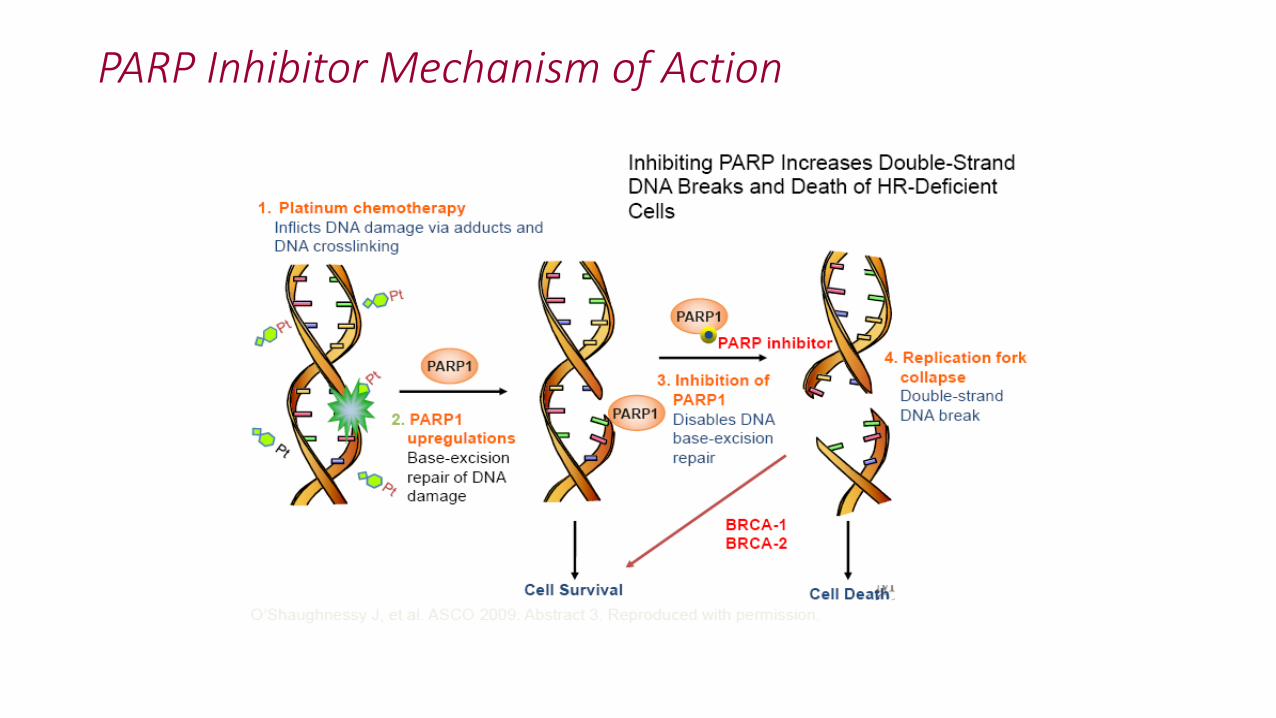
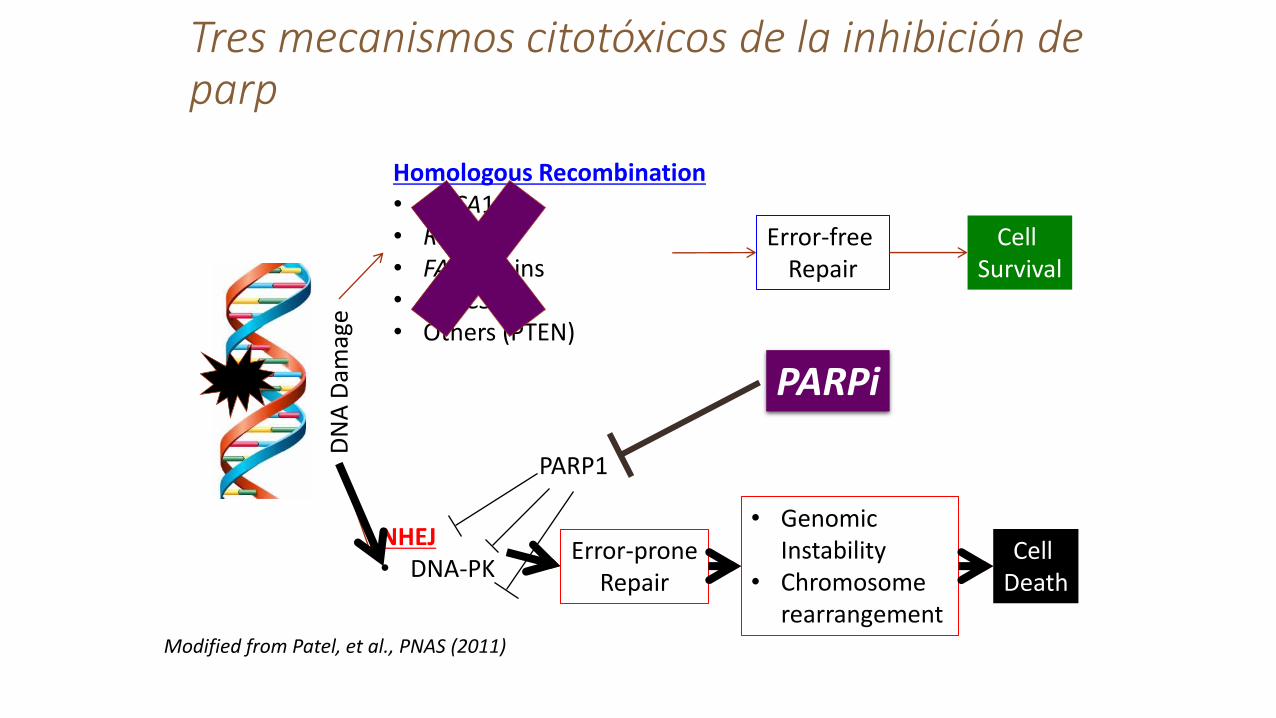
PARP Inhibitor Mechanism of Action
PARP Inhibitor Mechanism of Action
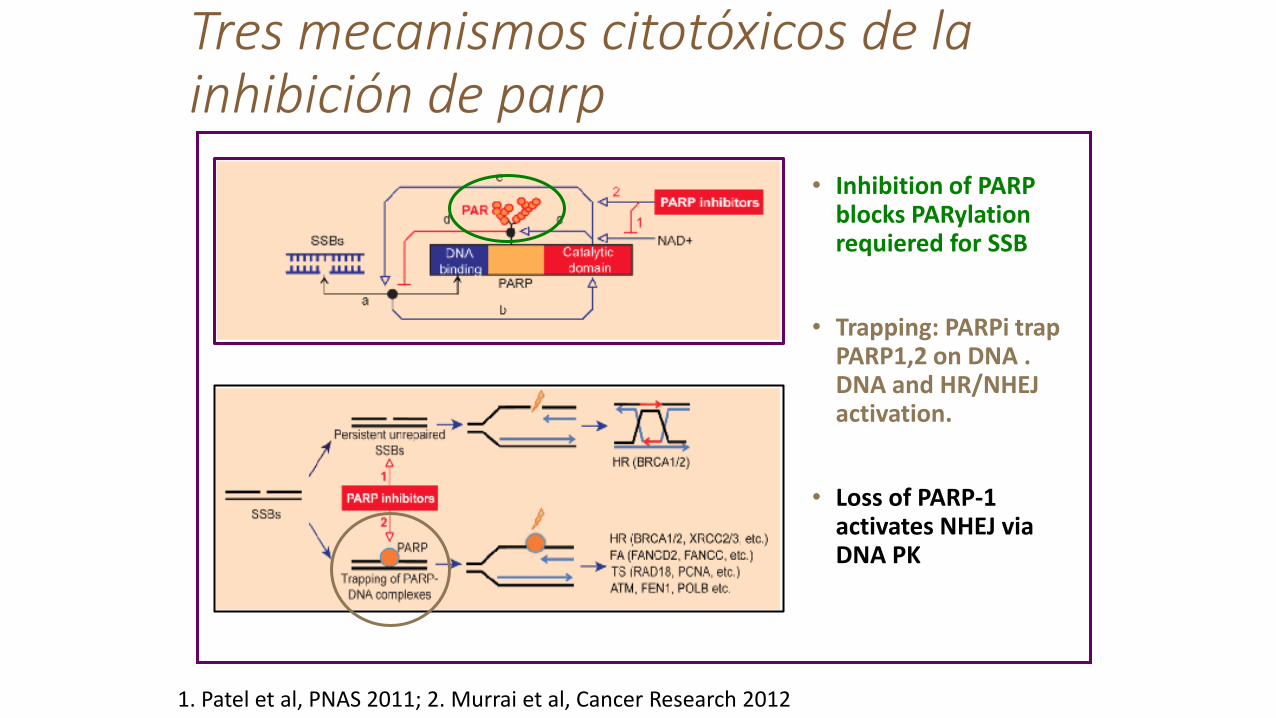
• Inhibition of PARP blocks PARylation requiered for SSB
• Trapping: PARPi trap PARP1,2 on DNA . DNA and HR/NHEJ activation.
• Loss of PARP-1 activates NHEJ via DNA PK
1. Patel et al, PNAS 2011; 2. Murrai et al, Cancer Research 2012
Tres mecanismos citotóxicos de la inhibición de parp
Tres mecanismos citotóxicos de la inhibición de parp
Homologous Recombination • BRCA1/2 • Rad51 • FA proteins • XRCC3 • Others (PTEN)
Error-free Repair
Cell Survival
NHEJ • DNA-PK
Error-prone Repair
Cell Death
• Genomic Instability
• Chromosome rearrangement
DN
A D
amag
e
PARP1
Modified from Patel, et al., PNAS (2011)
PARPi

Iparp’s en cáncer de
ovario
Veliparib Niraparib Rucaparib
BMN 673
Olaparib
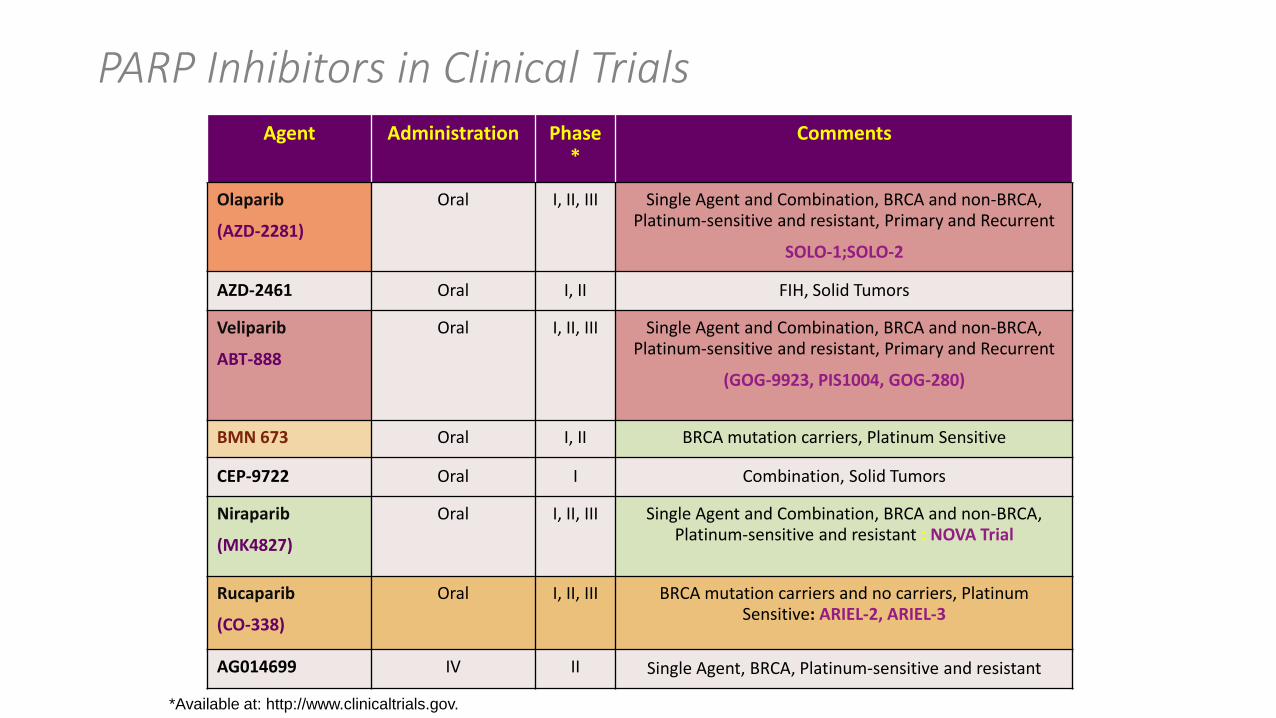
Agent Administration Phase*
Comments
Olaparib
(AZD-2281)
Oral I, II, III Single Agent and Combination, BRCA and non-BRCA, Platinum-sensitive and resistant, Primary and Recurrent
SOLO-1;SOLO-2
AZD-2461 Oral I, II FIH, Solid Tumors
Veliparib
ABT-888
Oral I, II, III Single Agent and Combination, BRCA and non-BRCA, Platinum-sensitive and resistant, Primary and Recurrent
(GOG-9923, PIS1004, GOG-280)
BMN 673 Oral I, II BRCA mutation carriers, Platinum Sensitive
CEP-9722 Oral I Combination, Solid Tumors
Niraparib
(MK4827)
Oral I, II, III Single Agent and Combination, BRCA and non-BRCA, Platinum-sensitive and resistant : NOVA Trial
Rucaparib
(CO-338)
Oral I, II, III BRCA mutation carriers and no carriers, Platinum Sensitive: ARIEL-2, ARIEL-3
AG014699 IV II Single Agent, BRCA, Platinum-sensitive and resistant
*Available at: http://www.clinicaltrials.gov.
PARP Inhibitors in Clinical Trials
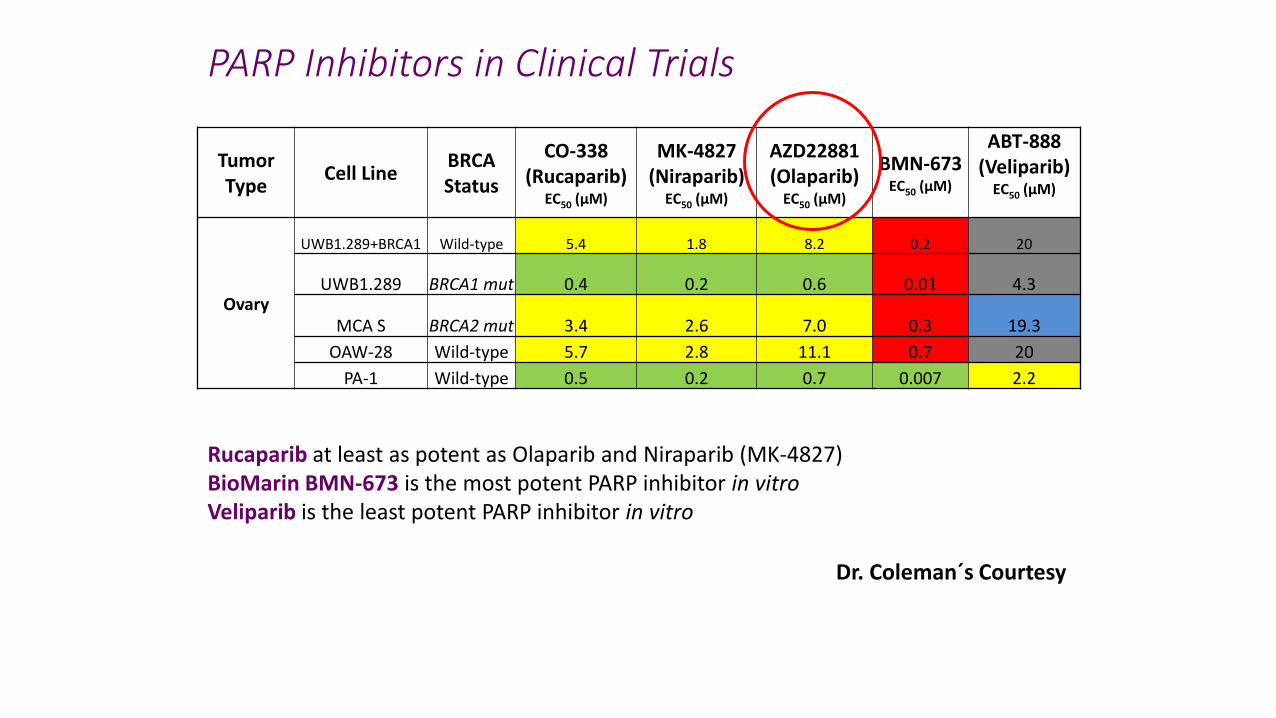
Tumor Type
Cell Line BRCA Status
CO-338 (Rucaparib)
EC50 (µM)
MK-4827 (Niraparib)
EC50 (µM)
AZD22881 (Olaparib)
EC50 (µM)
BMN-673 EC50 (µM)
ABT-888 (Veliparib)
EC50 (µM)
Ovary
UWB1.289+BRCA1 Wild-type 5.4 1.8 8.2 0.2 20
UWB1.289 BRCA1 mut 0.4 0.2 0.6 0.01 4.3
MCA S BRCA2 mut 3.4 2.6 7.0 0.3 19.3
OAW-28 Wild-type 5.7 2.8 11.1 0.7 20
PA-1 Wild-type 0.5 0.2 0.7 0.007 2.2
Rucaparib at least as potent as Olaparib and Niraparib (MK-4827) BioMarin BMN-673 is the most potent PARP inhibitor in vitro Veliparib is the least potent PARP inhibitor in vitro
PARP Inhibitors in Clinical Trials
Dr. Coleman´s Courtesy
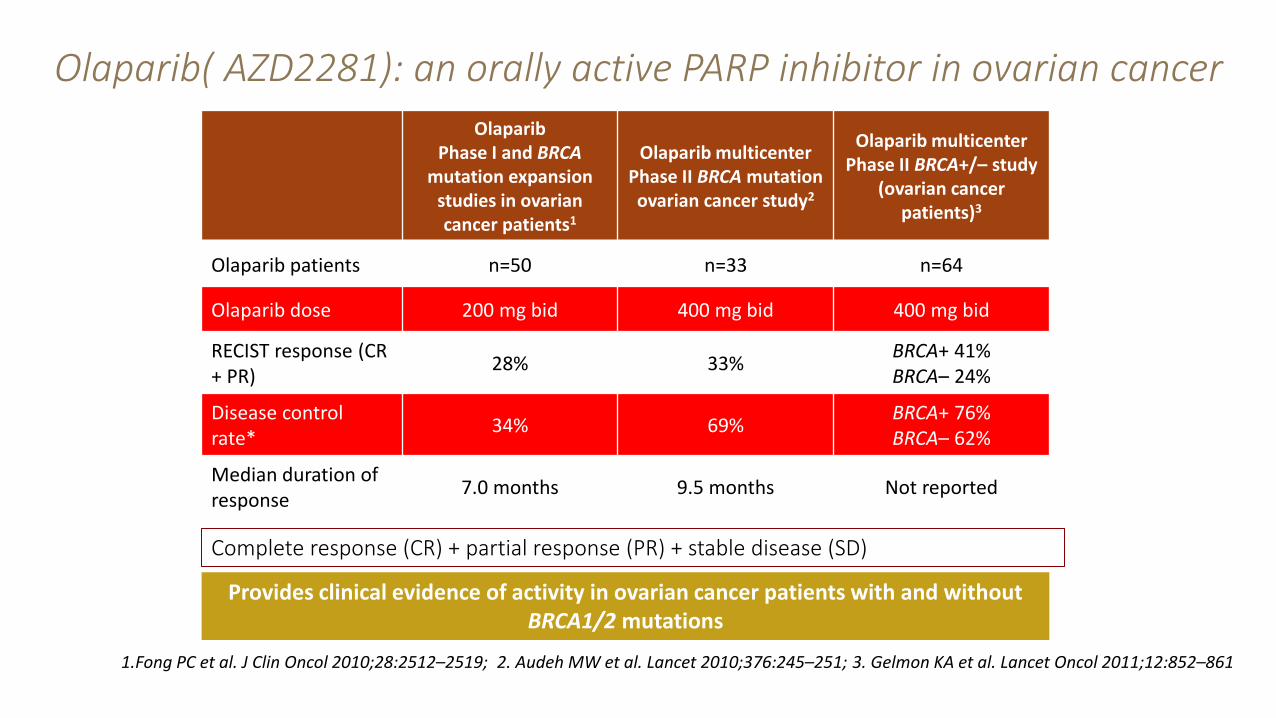
Olaparib Phase I and BRCA
mutation expansion studies in ovarian cancer patients1
Olaparib multicenter Phase II BRCA mutation ovarian cancer study2
Olaparib multicenter Phase II BRCA+/– study
(ovarian cancer patients)3
Olaparib patients n=50 n=33 n=64
Olaparib dose 200 mg bid 400 mg bid 400 mg bid
RECIST response (CR + PR)
28% 33% BRCA+ 41% BRCA– 24%
Disease control rate*
34% 69% BRCA+ 76% BRCA– 62%
Median duration of response
7.0 months 9.5 months Not reported
Complete response (CR) + partial response (PR) + stable disease (SD)
1.Fong PC et al. J Clin Oncol 2010;28:2512–2519; 2. Audeh MW et al. Lancet 2010;376:245–251; 3. Gelmon KA et al. Lancet Oncol 2011;12:852–861
Provides clinical evidence of activity in ovarian cancer patients with and without BRCA1/2 mutations
Olaparib( AZD2281): an orally active PARP inhibitor in ovarian cancer
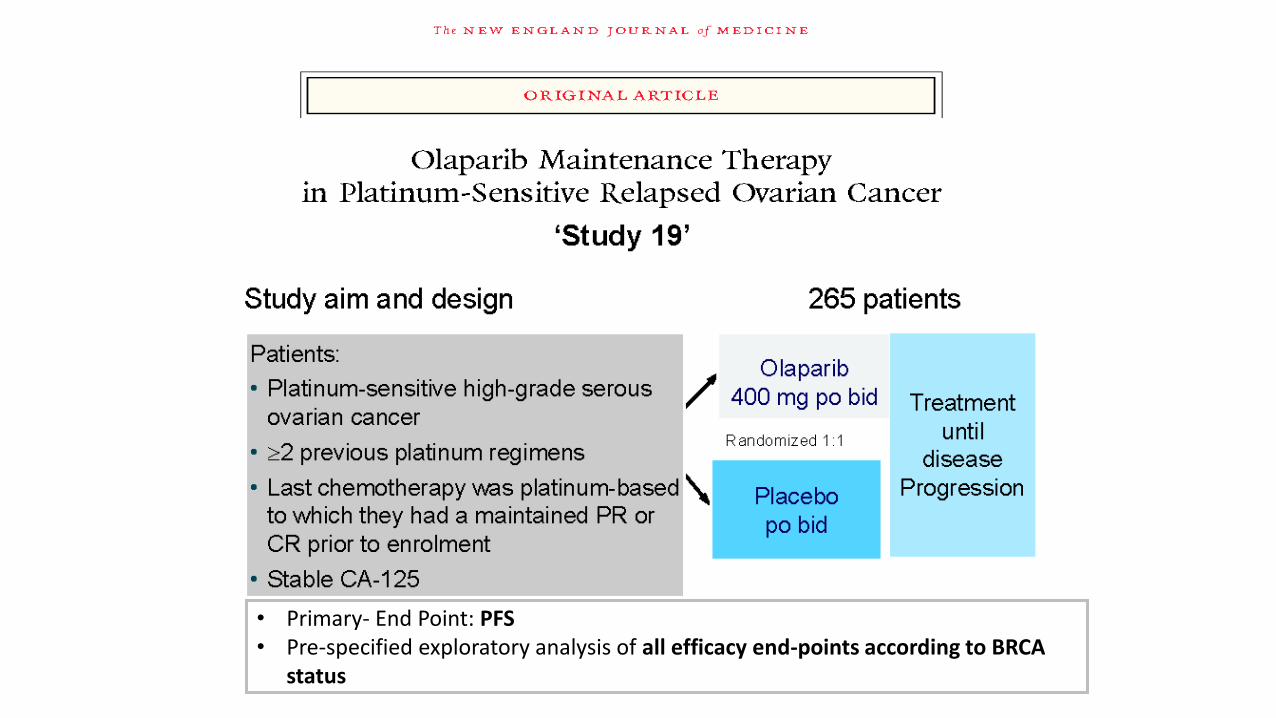
• Primary- End Point: PFS • Pre-specified exploratory analysis of all efficacy end-points according to BRCA
status
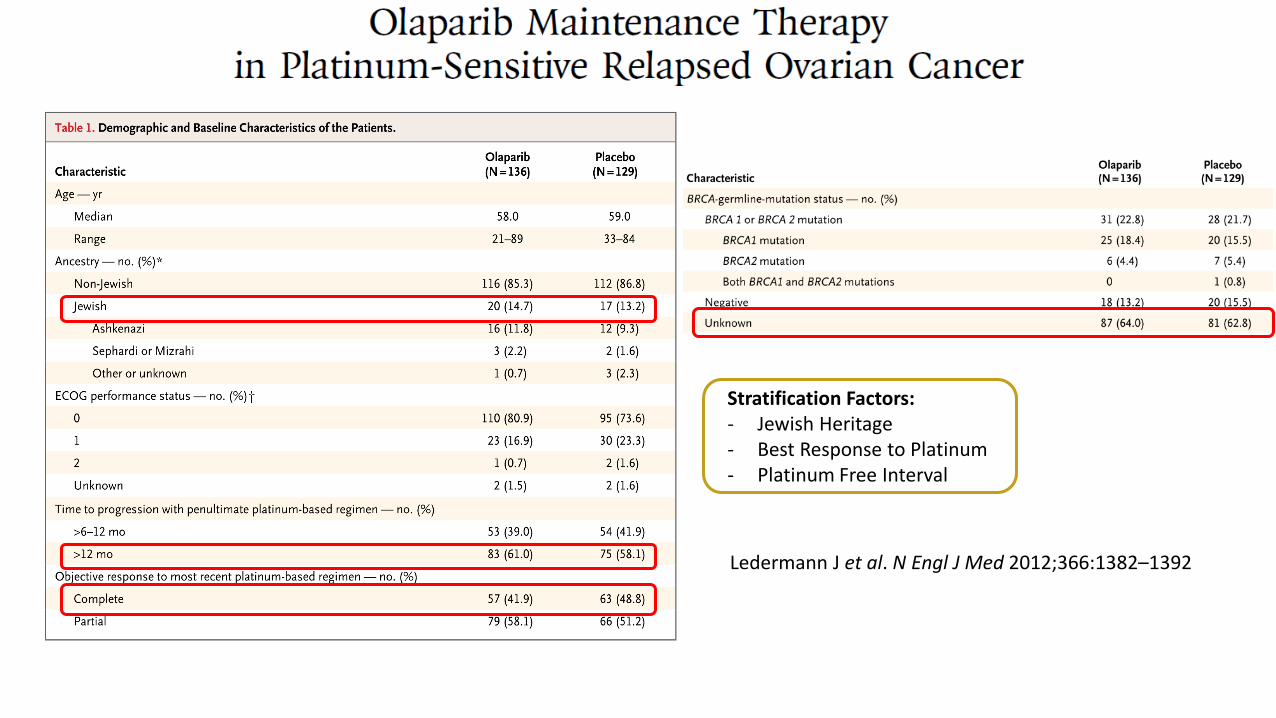
Ledermann J et al. N Engl J Med 2012;366:1382–1392
Stratification Factors: - Jewish Heritage - Best Response to Platinum - Platinum Free Interval
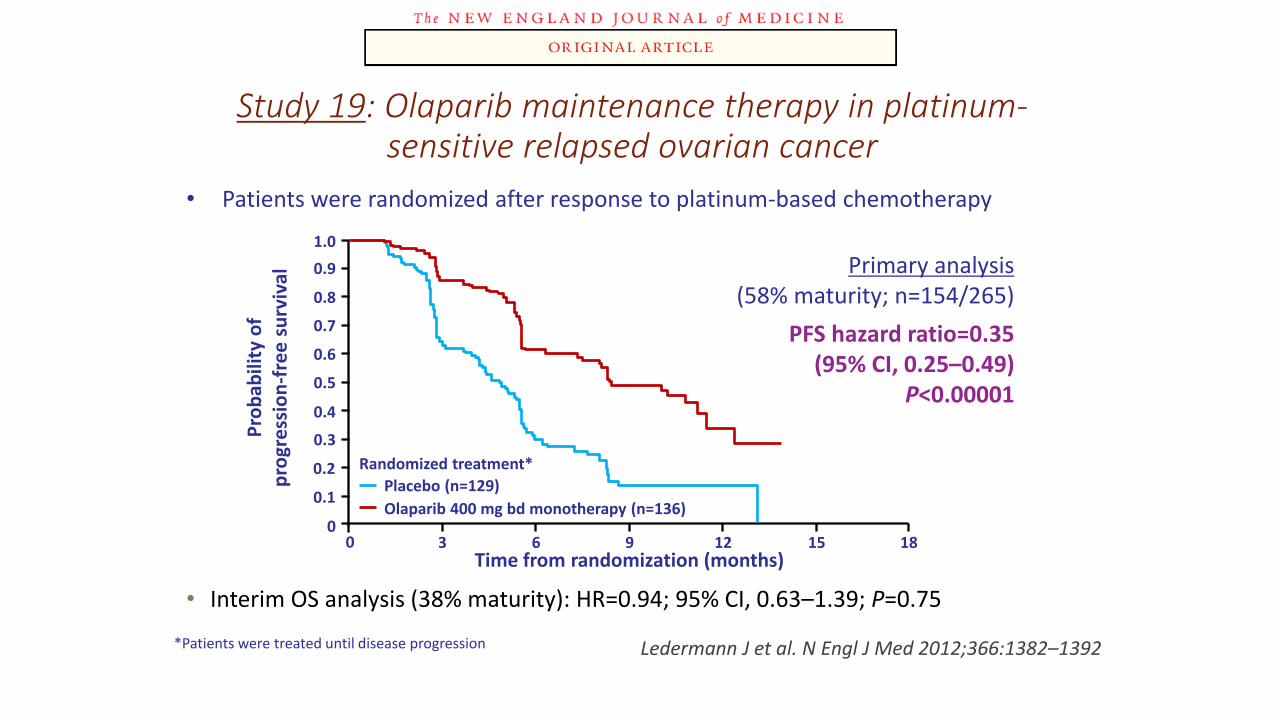
• Interim OS analysis (38% maturity): HR=0.94; 95% CI, 0.63–1.39; P=0.75
0
0.6
0.8
0.9
0
0.1
0.2
0.3
0.4
0.5
0.7
1.0
3 6 9 12 15 18
Pro
bab
ility
of
p
rogr
ess
ion
-fre
e s
urv
ival
Time from randomization (months)
Primary analysis (58% maturity; n=154/265)
PFS hazard ratio=0.35 (95% CI, 0.25–0.49)
P<0.00001
Randomized treatment*
Placebo (n=129)
Olaparib 400 mg bd monotherapy (n=136)
Study 19: Olaparib maintenance therapy in platinum-sensitive relapsed ovarian cancer
Ledermann J et al. N Engl J Med 2012;366:1382–1392 *Patients were treated until disease progression
• Patients were randomized after response to platinum-based chemotherapy
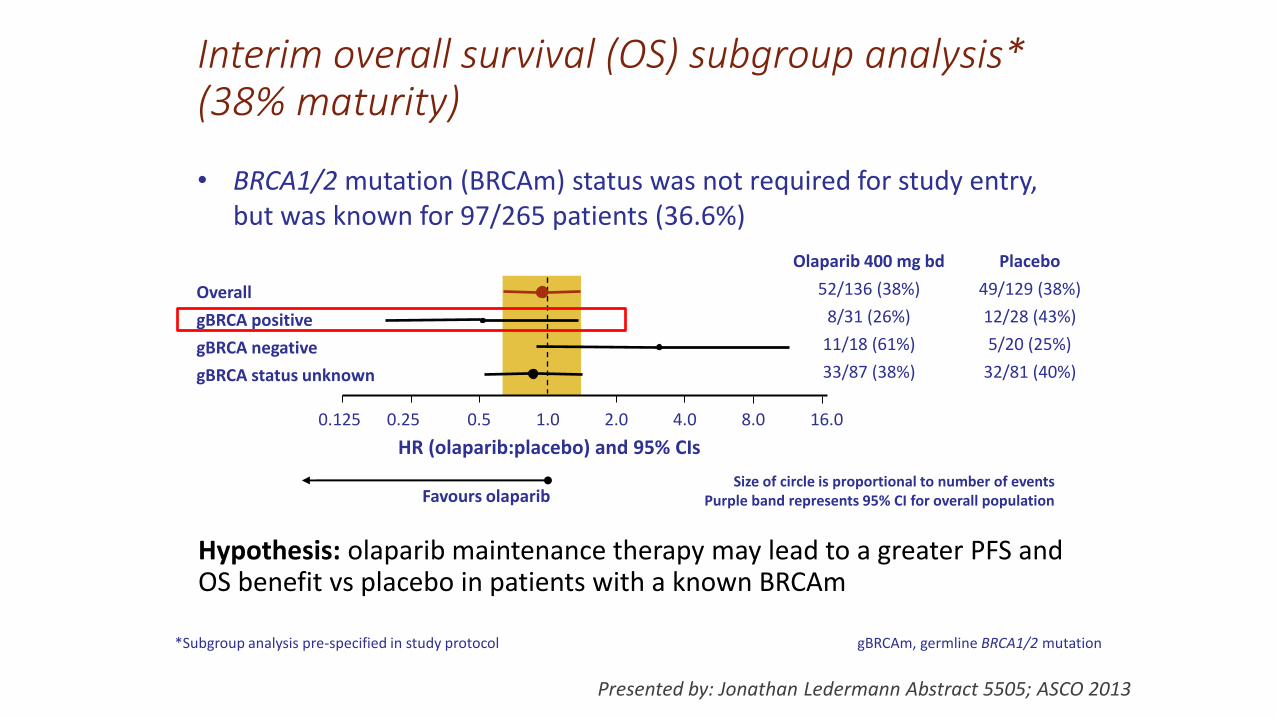
Interim overall survival (OS) subgroup analysis* (38% maturity)
Hypothesis: olaparib maintenance therapy may lead to a greater PFS and OS benefit vs placebo in patients with a known BRCAm
HR (olaparib:placebo) and 95% CIs
Favours olaparib
• BRCA1/2 mutation (BRCAm) status was not required for study entry, but was known for 97/265 patients (36.6%)
Size of circle is proportional to number of events Purple band represents 95% CI for overall population
Overall
gBRCA positive
gBRCA negative
gBRCA status unknown
Olaparib 400 mg bd
52/136 (38%)
8/31 (26%)
11/18 (61%)
33/87 (38%)
Placebo
49/129 (38%)
12/28 (43%)
5/20 (25%)
32/81 (40%)
0.125 0.25 0.5 1.0 2.0 4.0 8.0 16.0
*Subgroup analysis pre-specified in study protocol gBRCAm, germline BRCA1/2 mutation
Presented by: Jonathan Ledermann Abstract 5505; ASCO 2013
Methods: BRCAm testing
• Germline BRCAm (gBRCAm) status was determined retrospectively in an additional 121 patients (218 in total)
‒ The diagnostic assay (Myriad Genetics) used blood samples collected before randomization from consenting patients
• Since patients without an inherited gBRCAm can develop somatic mutations, tumour BRCAm (tBRCAm) status was also determined in 209/265 patients
‒ Archival tumour samples were analyzed by Foundation Medicine
Presented by: Jonathan Ledermann Abstract 5505; ASCO 2013
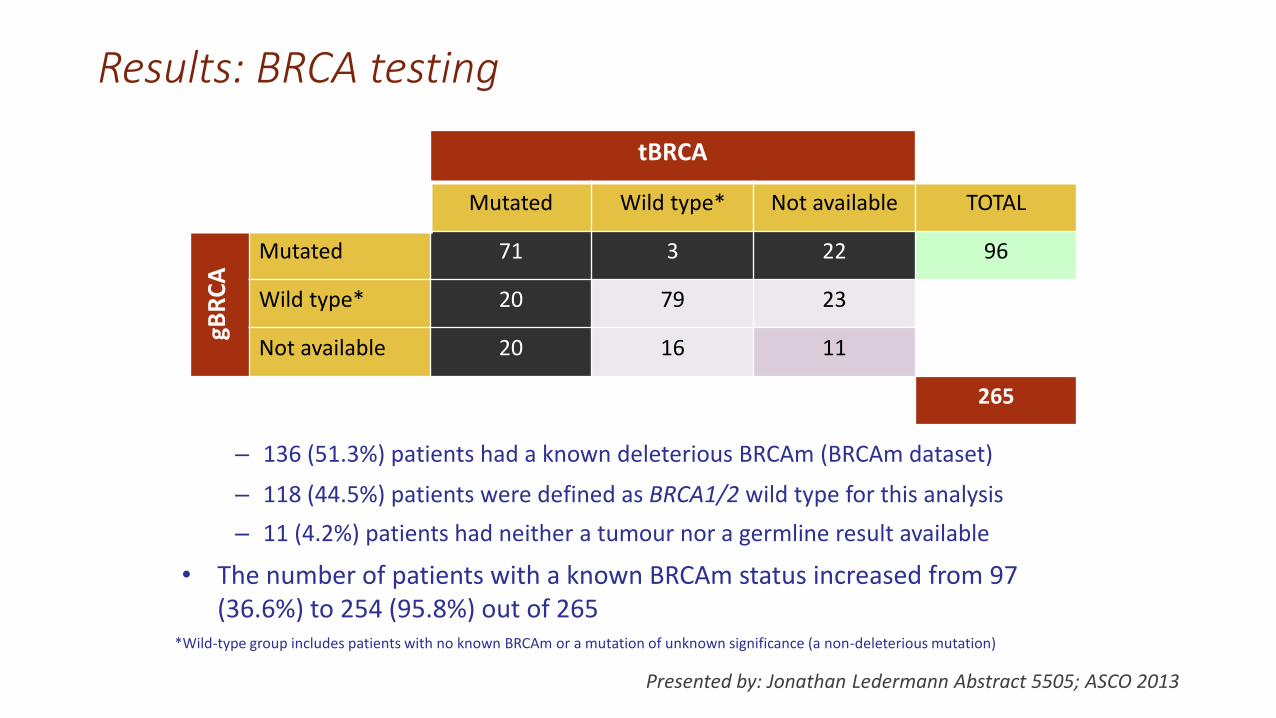
Results: BRCA testing
tBRCA
Mutated Wild type* Not available TOTAL gB
RC
A Mutated 71 3 22 96
Wild type* 20 79 23
Not available 20 16 11
265
*Wild-type group includes patients with no known BRCAm or a mutation of unknown significance (a non-deleterious mutation)
• The number of patients with a known BRCAm status increased from 97 (36.6%) to 254 (95.8%) out of 265
– 11 (4.2%) patients had neither a tumour nor a germline result available
– 118 (44.5%) patients were defined as BRCA1/2 wild type for this analysis
– 136 (51.3%) patients had a known deleterious BRCAm (BRCAm dataset)
Presented by: Jonathan Ledermann Abstract 5505; ASCO 2013
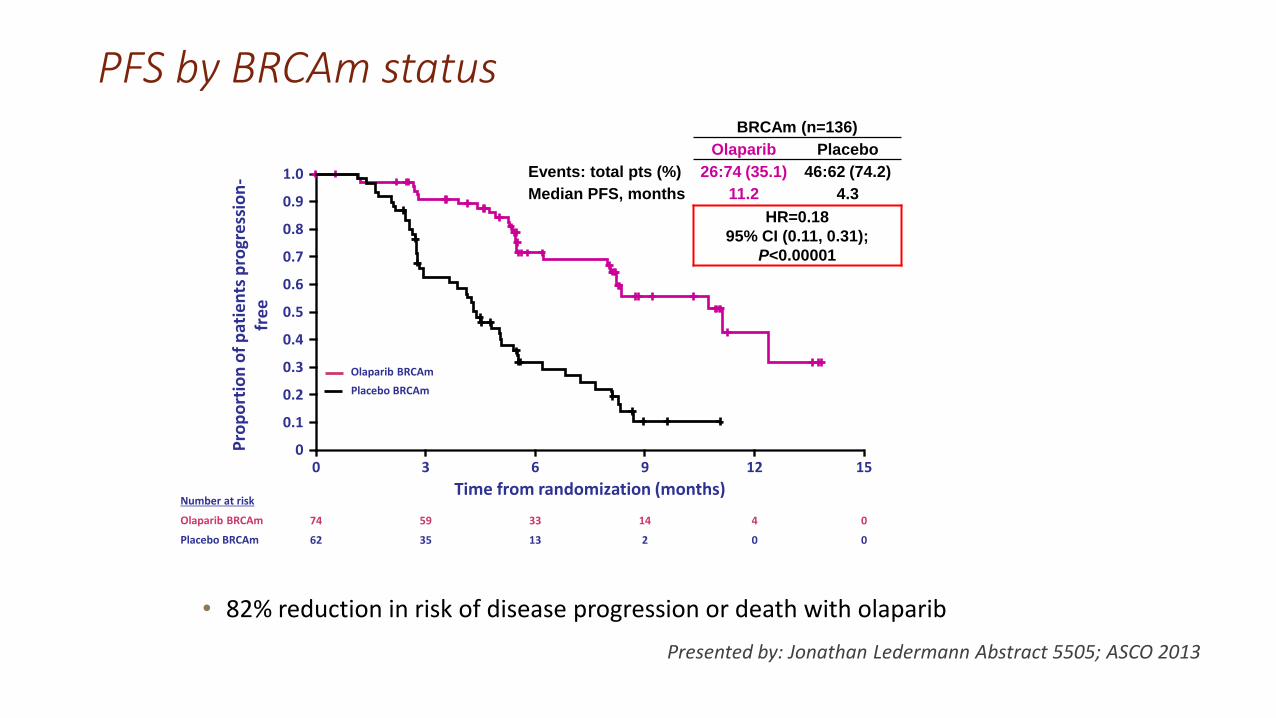
BRCAm (n=136)
Olaparib Placebo
Events: total pts (%) 26:74 (35.1) 46:62 (74.2)
Median PFS, months 11.2 4.3
HR=0.18
95% CI (0.11, 0.31);
P<0.00001
PFS by BRCAm status
0
Time from randomization (months)
0
1.0
Pro
po
rtio
n o
f p
atie
nts
pro
gre
ssio
n-
fre
e
3 6 9 12 15
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
• 82% reduction in risk of disease progression or death with olaparib
Olaparib BRCAm
Placebo BRCAm
Number at risk
Olaparib BRCAm
Placebo BRCAm
74 59 33 14 4 0
62 35 13 2 0 0
Presented by: Jonathan Ledermann Abstract 5505; ASCO 2013
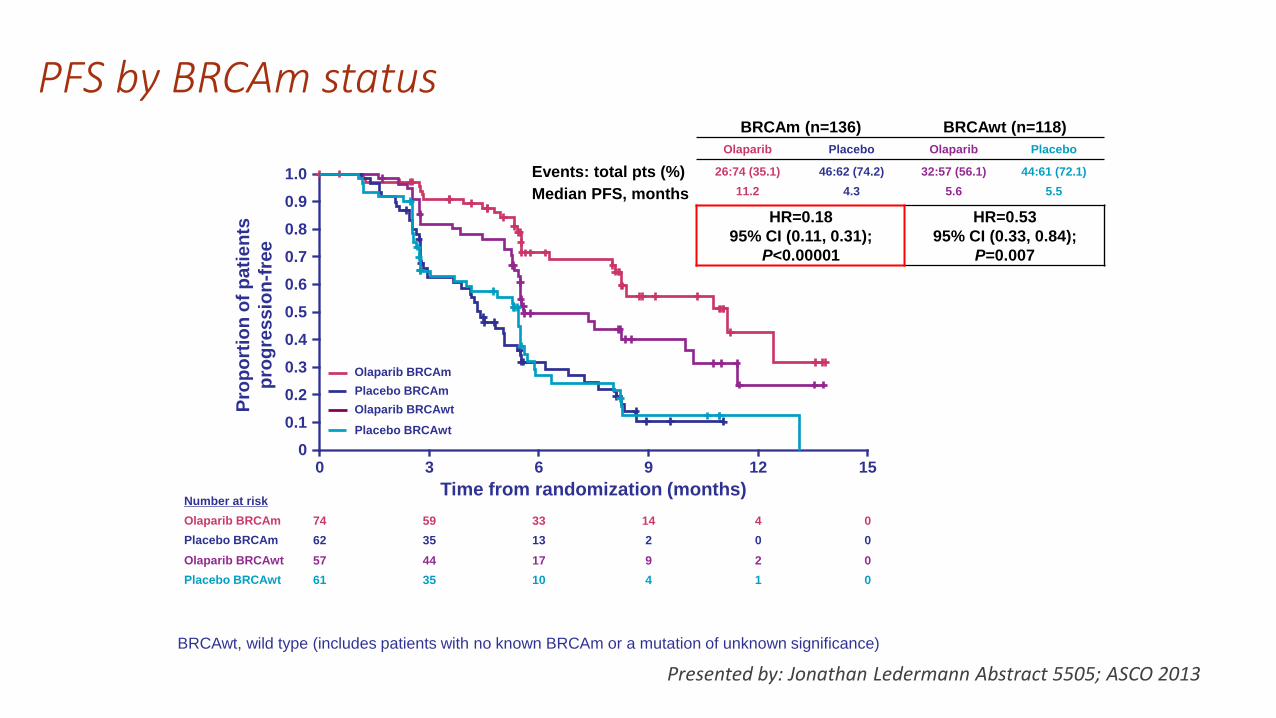
PFS by BRCAm status
0
Time from randomization (months)
0
1.0
Pro
po
rtio
n o
f p
ati
en
ts
pro
gre
ss
ion
-fre
e
3 6 9 12 15
Olaparib BRCAm
Olaparib BRCAwt
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
BRCAm (n=136) BRCAwt (n=118)
Olaparib Placebo Olaparib Placebo
Events: total pts (%) 26:74 (35.1) 46:62 (74.2) 32:57 (56.1) 44:61 (72.1)
Median PFS, months 11.2 4.3 5.6 5.5
HR=0.18
95% CI (0.11, 0.31);
P<0.00001
HR=0.53
95% CI (0.33, 0.84);
P=0.007
Placebo BRCAm
Placebo BRCAwt
Number at risk
Olaparib BRCAm
Olaparib BRCAwt
Placebo BRCAm
Placebo BRCAwt
74 59 33 14 4 0
57 44 17 9 2 0
62 35 13 2 0 0
61 35 10 4 1 0
BRCAwt, wild type (includes patients with no known BRCAm or a mutation of unknown significance)
Presented by: Jonathan Ledermann Abstract 5505; ASCO 2013
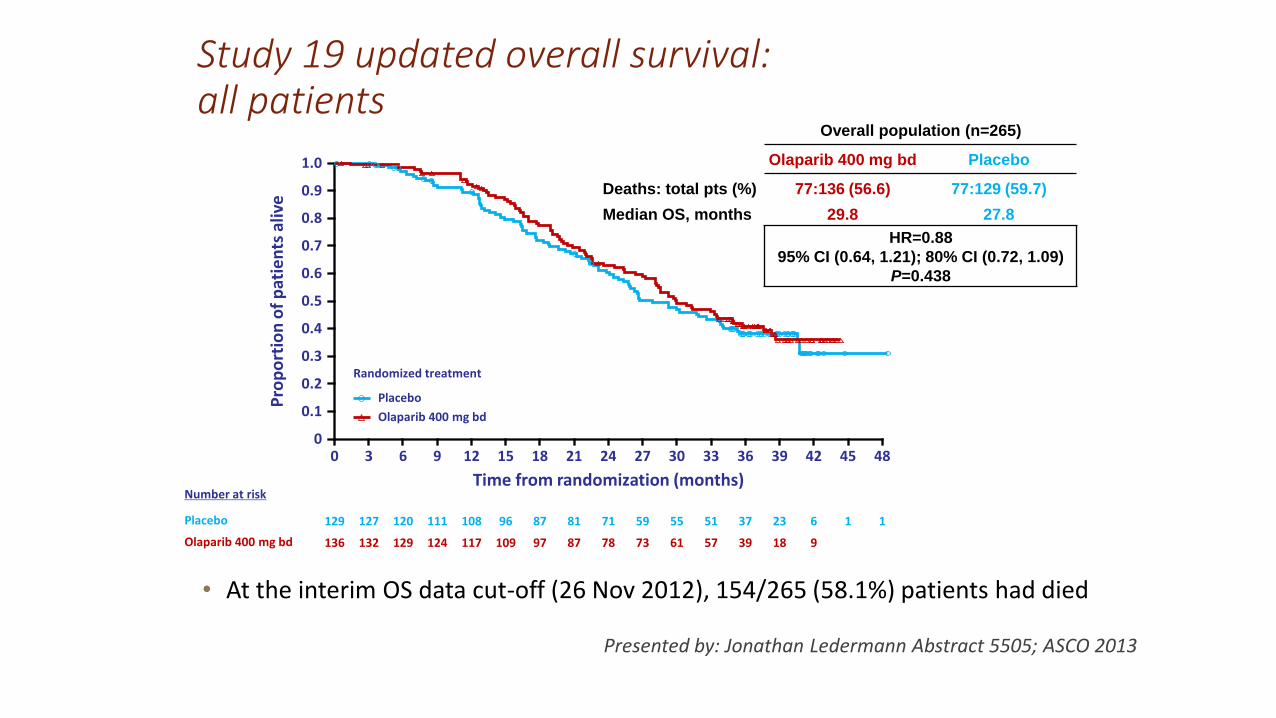
Study 19 updated overall survival: all patients
Presented by: Jonathan Ledermann Abstract 5505; ASCO 2013
0
Time from randomization (months)
0 48
1.0
Pro
po
rtio
n o
f p
atie
nts
aliv
e
3 6 9 12 15 18 21 24 27 30 33 36 39 42 45
Number at risk
129 1 127 120 111 108 96 87 81 71 59 55 51 37 23 6 1 Placebo
136 132 129 124 117 109 97 87 78 73 61 57 39 18 9 Olaparib 400 mg bd
Randomized treatment
Placebo
Olaparib 400 mg bd
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
Overall population (n=265)
Olaparib 400 mg bd Placebo
Deaths: total pts (%) 77:136 (56.6) 77:129 (59.7)
Median OS, months 29.8 27.8
HR=0.88
95% CI (0.64, 1.21); 80% CI (0.72, 1.09)
P=0.438
• At the interim OS data cut-off (26 Nov 2012), 154/265 (58.1%) patients had died
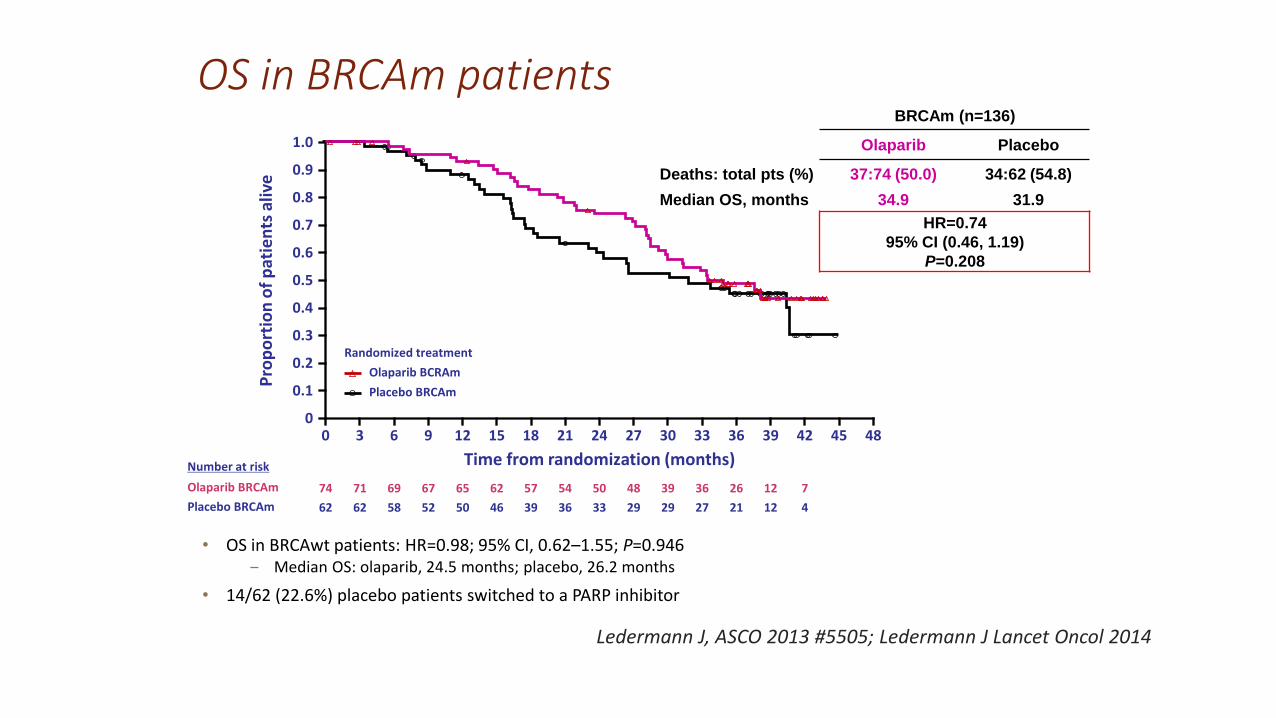
OS in BRCAm patients
0
Time from randomization (months)
0 48
1.0
Pro
po
rtio
n o
f p
atie
nts
aliv
e
3 6 9 12 15 18 21 24 27 30 33 36 39 42 45
Number at risk
62 62 58 52 50 46 39 36 33 29 29 27 21 12 4 Placebo BRCAm
74 71 69 67 65 62 57 54 50 48 39 36 26 12 7 Olaparib BRCAm
Randomized treatment
Placebo BRCAm
Olaparib BCRAm
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
BRCAm (n=136)
Olaparib Placebo
Deaths: total pts (%) 37:74 (50.0) 34:62 (54.8)
Median OS, months 34.9 31.9
HR=0.74
95% CI (0.46, 1.19)
P=0.208
• OS in BRCAwt patients: HR=0.98; 95% CI, 0.62–1.55; P=0.946 ‒ Median OS: olaparib, 24.5 months; placebo, 26.2 months
• 14/62 (22.6%) placebo patients switched to a PARP inhibitor
Ledermann J, ASCO 2013 #5505; Ledermann J Lancet Oncol 2014
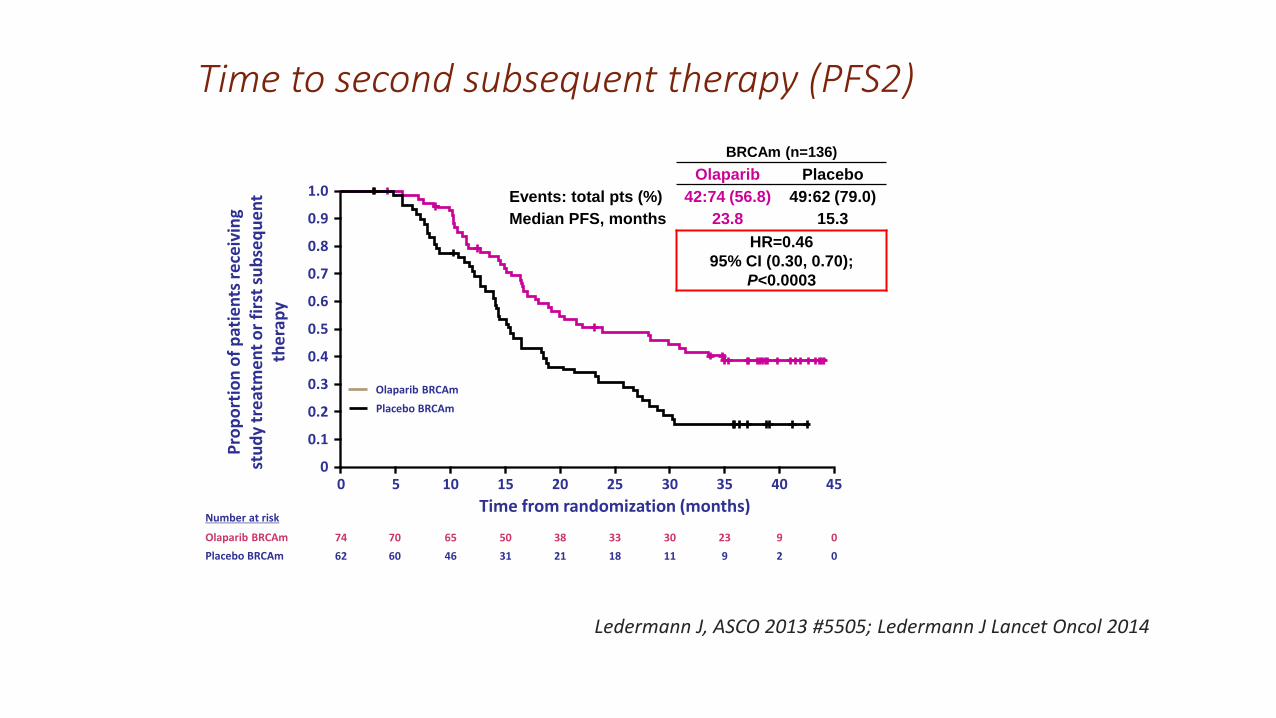
Time to second subsequent therapy (PFS2)
0
Time from randomization (months)
0
1.0
Pro
po
rtio
n o
f p
atie
nts
re
ceiv
ing
stu
dy
tre
atm
en
t o
r fi
rst
sub
seq
ue
nt
the
rap
y
10 20 30 40
Olaparib BRCAm
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
Placebo BRCAm
Number at risk
Olaparib BRCAm
Placebo BRCAm
74
62
5 15 25 35 45
70
60
65
46
50
31
38
21
33
18
30
11
23
9
9
2
0
0
BRCAm (n=136)
Olaparib Placebo
Events: total pts (%) 42:74 (56.8) 49:62 (79.0)
Median PFS, months 23.8 15.3
HR=0.46
95% CI (0.30, 0.70);
P<0.0003
Ledermann J, ASCO 2013 #5505; Ledermann J Lancet Oncol 2014
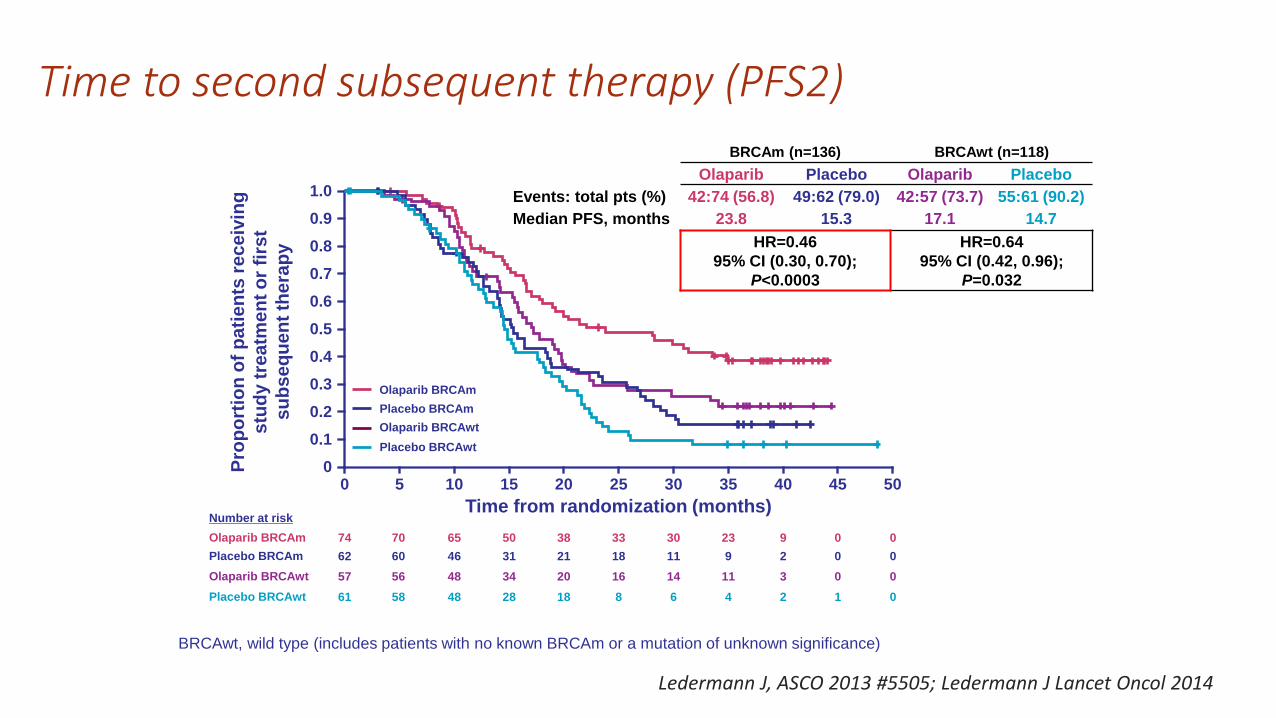
Time to second subsequent therapy (PFS2)
0
Time from randomization (months)
0
1.0
Pro
po
rtio
n o
f p
ati
en
ts r
ec
eiv
ing
stu
dy t
rea
tme
nt
or
firs
t
su
bs
eq
ue
nt
the
rap
y
10 20 30 40 50
Olaparib BRCAm
Olaparib BRCAwt
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
Placebo BRCAm
Placebo BRCAwt
Number at risk
Olaparib BRCAm
Olaparib BRCAwt
Placebo BRCAm
Placebo BRCAwt
74
57
62
61
5 15 25 35 45
70
56
60
58
65
48
46
48
50
34
31
28
38
20
21
18
33
16
18
8
30
14
11
6
23
11
9
4
9
3
2
2
0
0
0
1
0
0
0
0
BRCAm (n=136) BRCAwt (n=118)
Olaparib Placebo Olaparib Placebo
Events: total pts (%) 42:74 (56.8) 49:62 (79.0) 42:57 (73.7) 55:61 (90.2)
Median PFS, months 23.8 15.3 17.1 14.7
HR=0.46
95% CI (0.30, 0.70);
P<0.0003
HR=0.64
95% CI (0.42, 0.96);
P=0.032
BRCAwt, wild type (includes patients with no known BRCAm or a mutation of unknown significance)
Ledermann J, ASCO 2013 #5505; Ledermann J Lancet Oncol 2014
Duration of treatment and tolerability
• As of 23 May 2013, 26 patients remain on study treatment (olaparib, n=23; placebo, n=3)
• 33/136 patients (24%) have received >3 years of olaparib treatment, of whom 22 had a known BRCAm
• Olaparib tolerability was similar in patients with a BRCAm and the overall population
‒ The most common AEs in patients with a BRCAm were low-grade nausea (73%) and fatigue (54%)
Ledermann J, ASCO 2013 #5505; Ledermann J Lancet Oncol 2014
Conclusions
• Olaparib maintenance therapy led to the greatest clinical benefit, compared with placebo, in patients with a BRCAm
‒ PFS median improvement of 6.9 months; HR=0.18 (95% CI, 0.11–0.31)
‒ PFS2 median improvement of 8.5 months; HR=0.46 (95% CI, 0.30–0.70)
‒ OS median improvement of 3.0 months; HR=0.74 (95% CI, 0.46–1.19)
• No significant OS benefit was observed in the overall patient population
‒ The final OS analysis will be performed at ~85% maturity (after ~222 deaths)
• As a result of these compelling data, Phase III confirmatory trials in patients with a BRCA mutation had been completed. Results pending.
Ledermann J, ASCO 2013 #5505; Ledermann J Lancet Oncol 2014
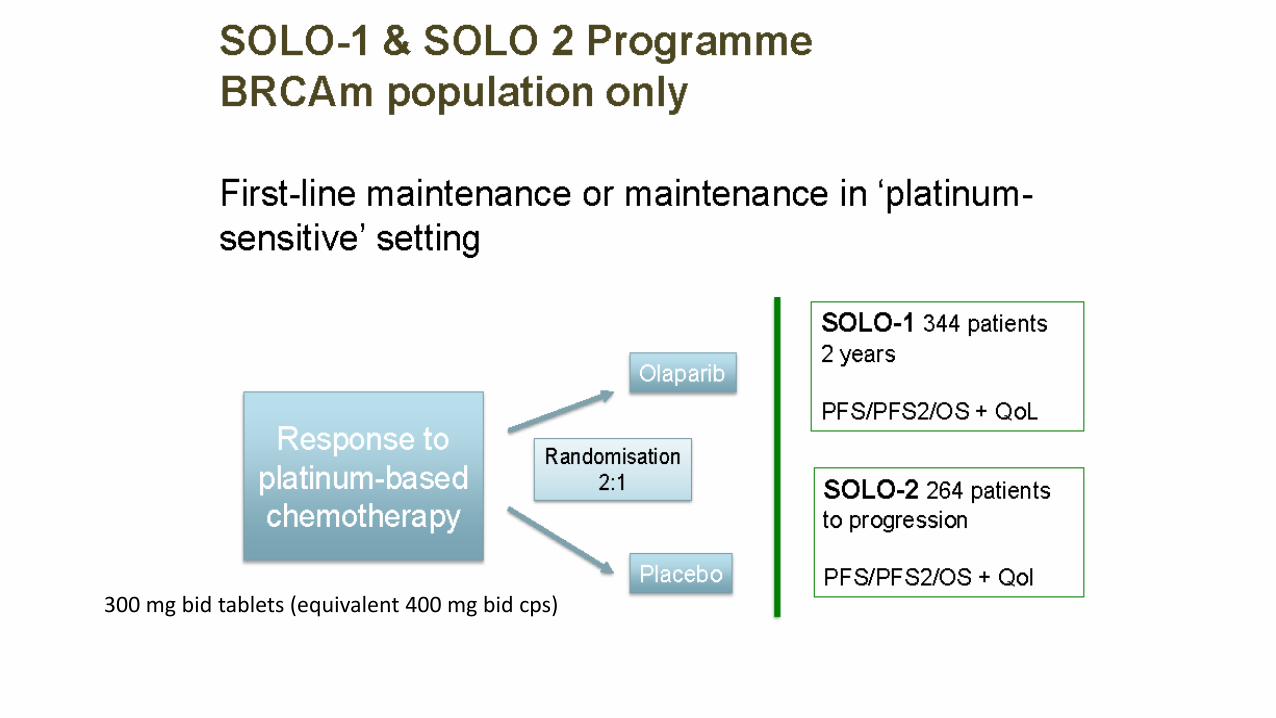
300 mg bid tablets (equivalent 400 mg bid cps)

®
Olaparib y quimioterapia
Olaparib vs QT
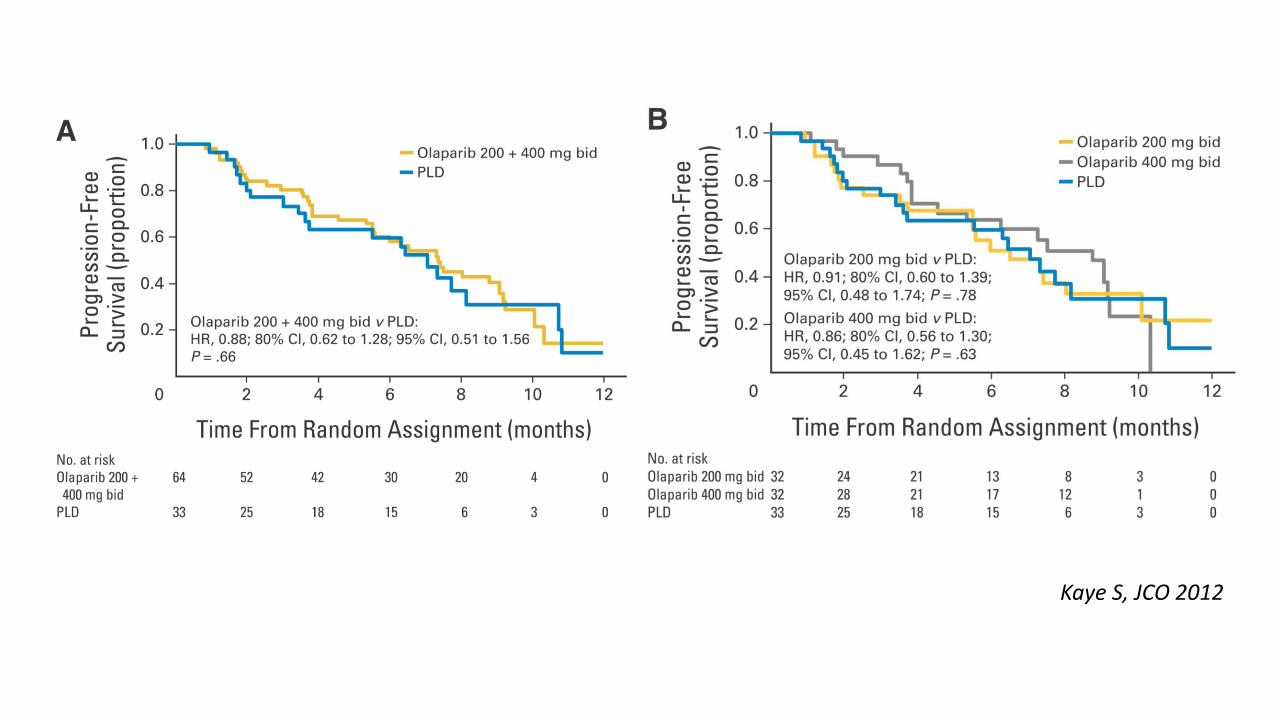
Kaye S, JCO 2012
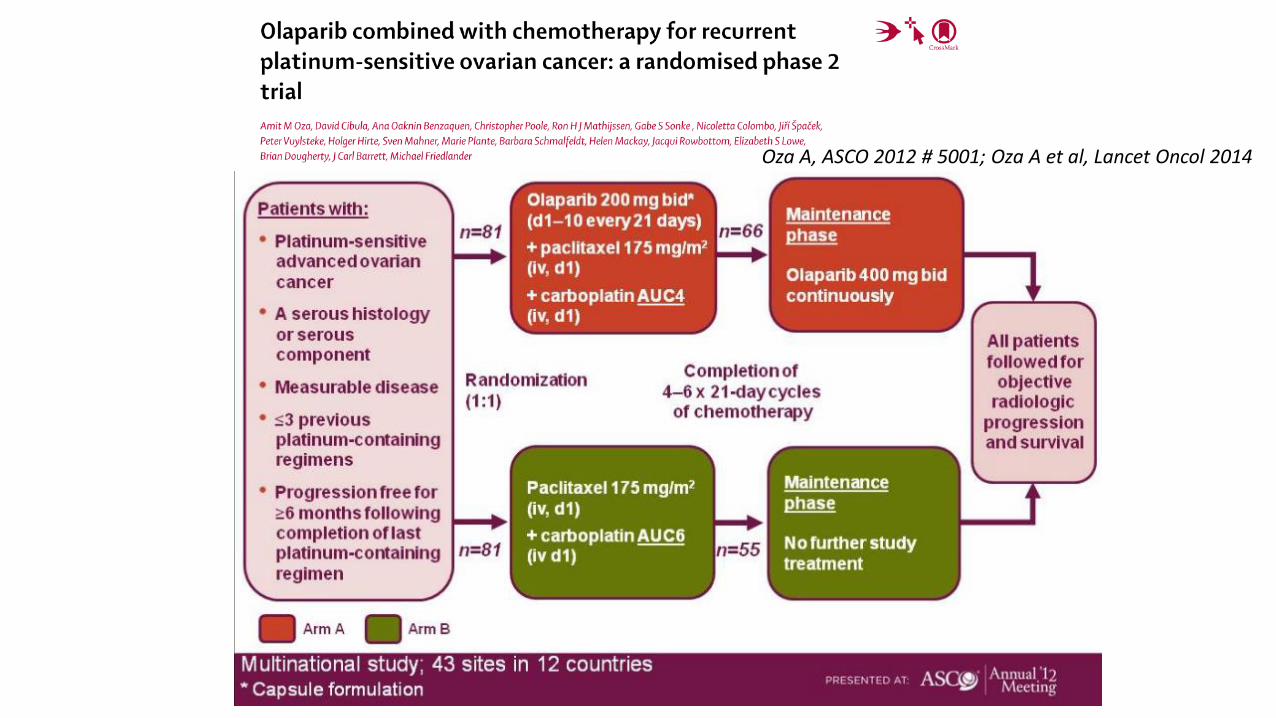
Oza A, ASCO 2012 # 5001; Oza A et al, Lancet Oncol 2014

Oza A, ASCO 2012 # 5001
Iparp’s en cáncer de
ovario
Olaparib
Veliparib Niraparib Rucaparib
BMN 673
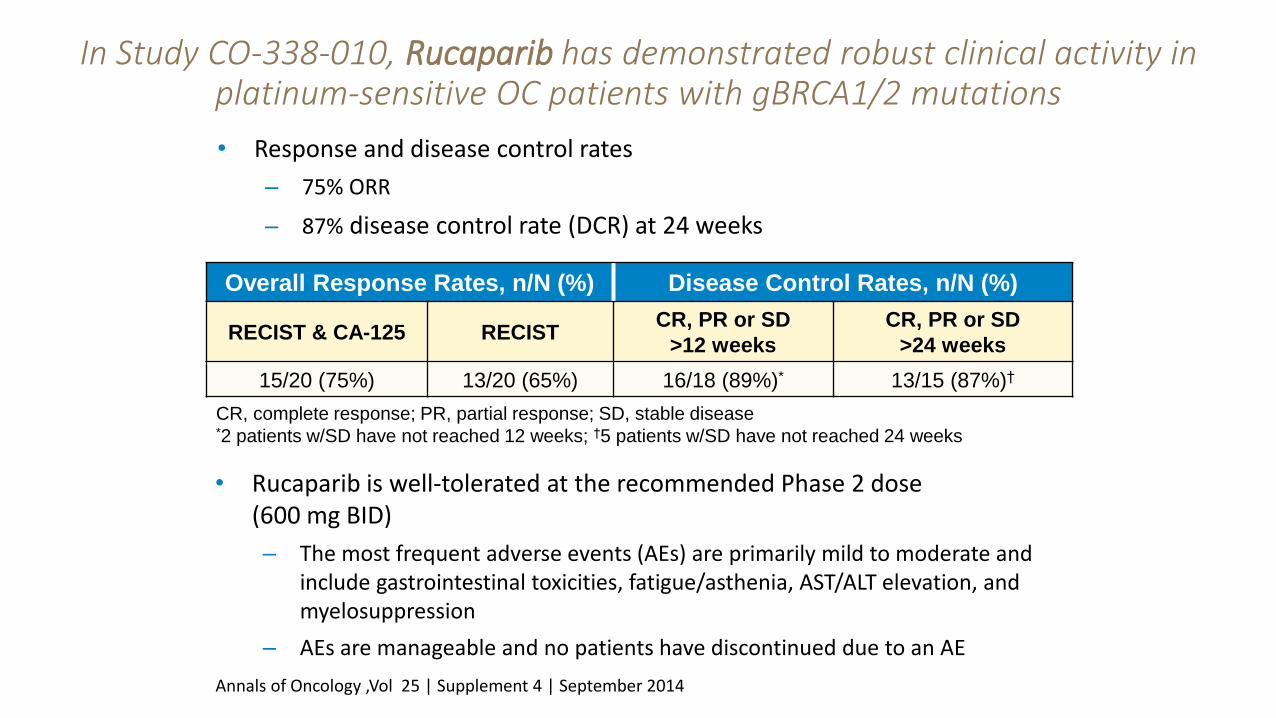
In Study CO-338-010, rucaparib has demonstrated robust clinical activity in platinum-sensitive OC patients with gBRCA1/2 mutations
48 | Confidential
Overall Response Rates, n/N (%) Disease Control Rates, n/N (%)
RECIST & CA-125 RECIST CR, PR or SD
>12 weeks
CR, PR or SD
>24 weeks
15/20 (75%) 13/20 (65%) 16/18 (89%)* 13/15 (87%)†
CR, complete response; PR, partial response; SD, stable disease
*2 patients w/SD have not reached 12 weeks; †5 patients w/SD have not reached 24 weeks
• Response and disease control rates
– 75% ORR
– 87% disease control rate (DCR) at 24 weeks
• Rucaparib is well-tolerated at the recommended Phase 2 dose (600 mg BID)
– The most frequent adverse events (AEs) are primarily mild to moderate and include gastrointestinal toxicities, fatigue/asthenia, AST/ALT elevation, and myelosuppression
– AEs are manageable and no patients have discontinued due to an AE
Annals of Oncology ,Vol 25 | Supplement 4 | September 2014
In Study CO-338-010, Rucaparib has demonstrated robust clinical activity in platinum-sensitive OC patients with gBRCA1/2 mutations
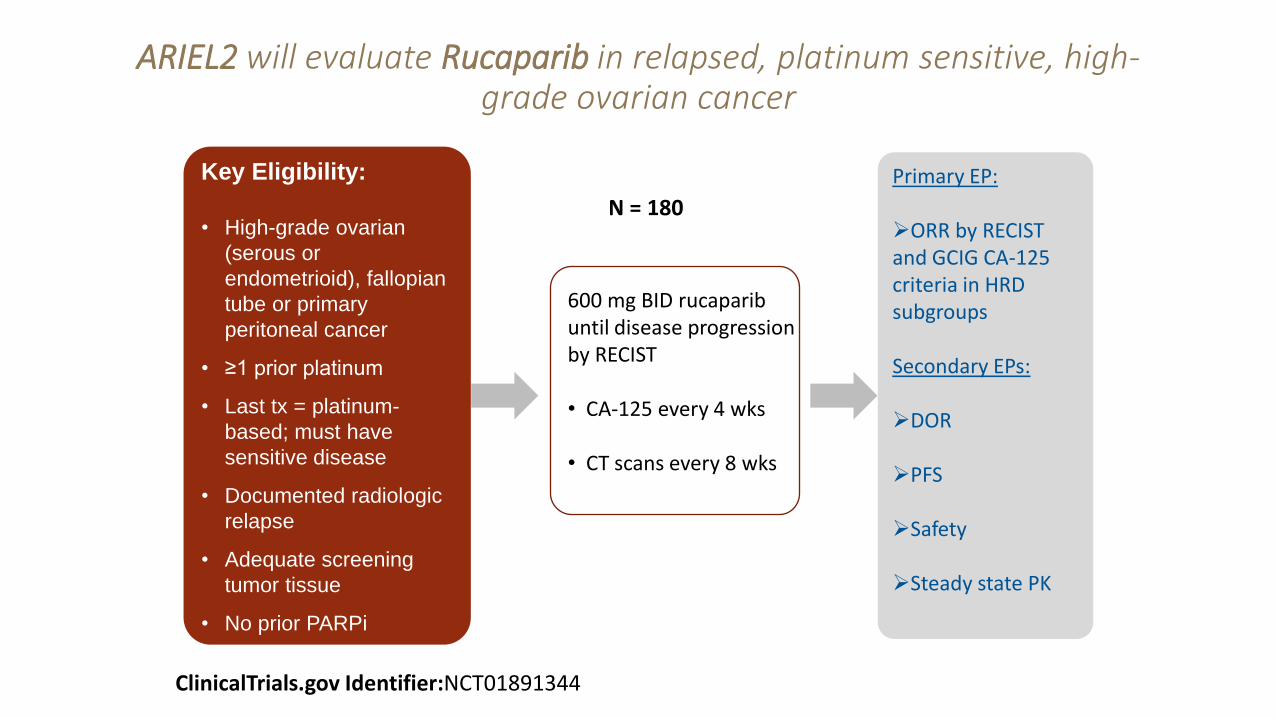
ARIEL2 will evaluate Rucaparib in relapsed, platinum sensitive, high-grade ovarian cancer
Key Eligibility:
• High-grade ovarian
(serous or
endometrioid), fallopian
tube or primary
peritoneal cancer
• ≥1 prior platinum
• Last tx = platinum-
based; must have
sensitive disease
• Documented radiologic
relapse
• Adequate screening
tumor tissue
• No prior PARPi
N = 180
Primary EP: ORR by RECIST and GCIG CA-125 criteria in HRD subgroups Secondary EPs: DOR
PFS
Safety
Steady state PK
600 mg BID rucaparib until disease progression by RECIST
• CA-125 every 4 wks
• CT scans every 8 wks
49 | Confidential ClinicalTrials.gov Identifier:NCT01891344
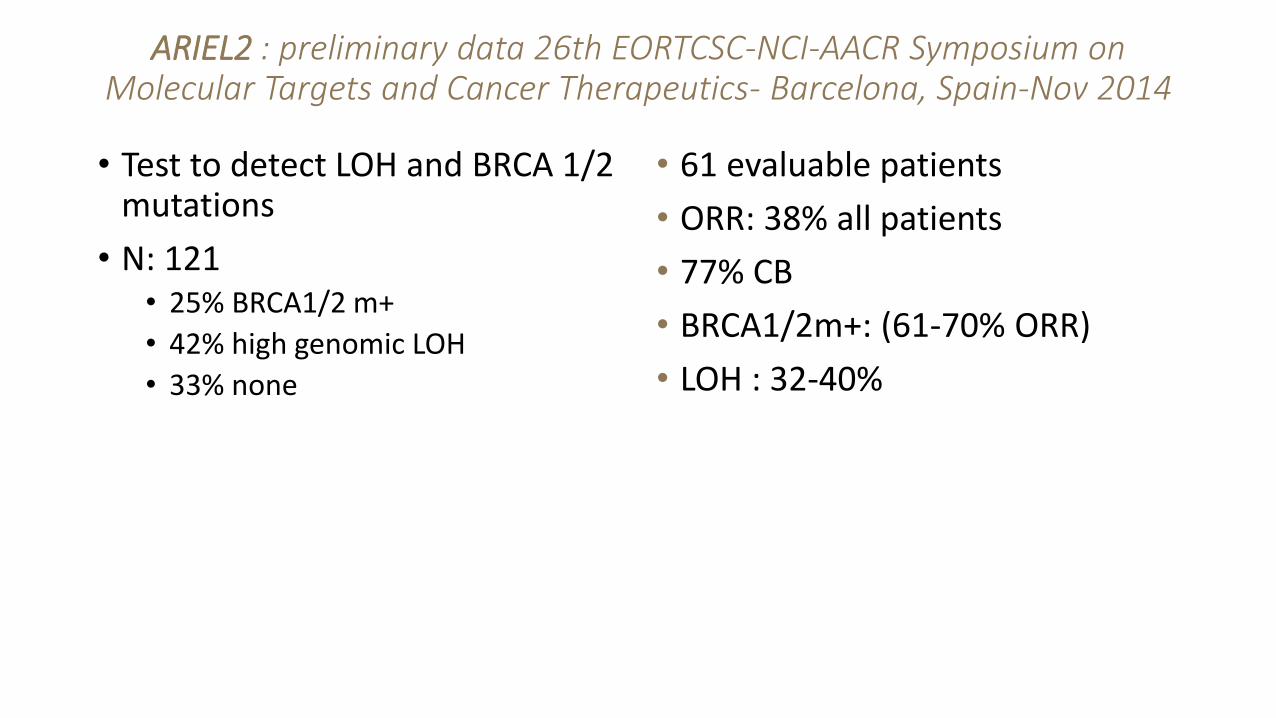
ARIEL2 : preliminary data 26th EORTCSC-NCI-AACR Symposium on Molecular Targets and Cancer Therapeutics- Barcelona, Spain-Nov 2014
• Test to detect LOH and BRCA 1/2 mutations
• N: 121 • 25% BRCA1/2 m+
• 42% high genomic LOH
• 33% none
• 61 evaluable patients
• ORR: 38% all patients
• 77% CB
• BRCA1/2m+: (61-70% ORR)
• LOH : 32-40%
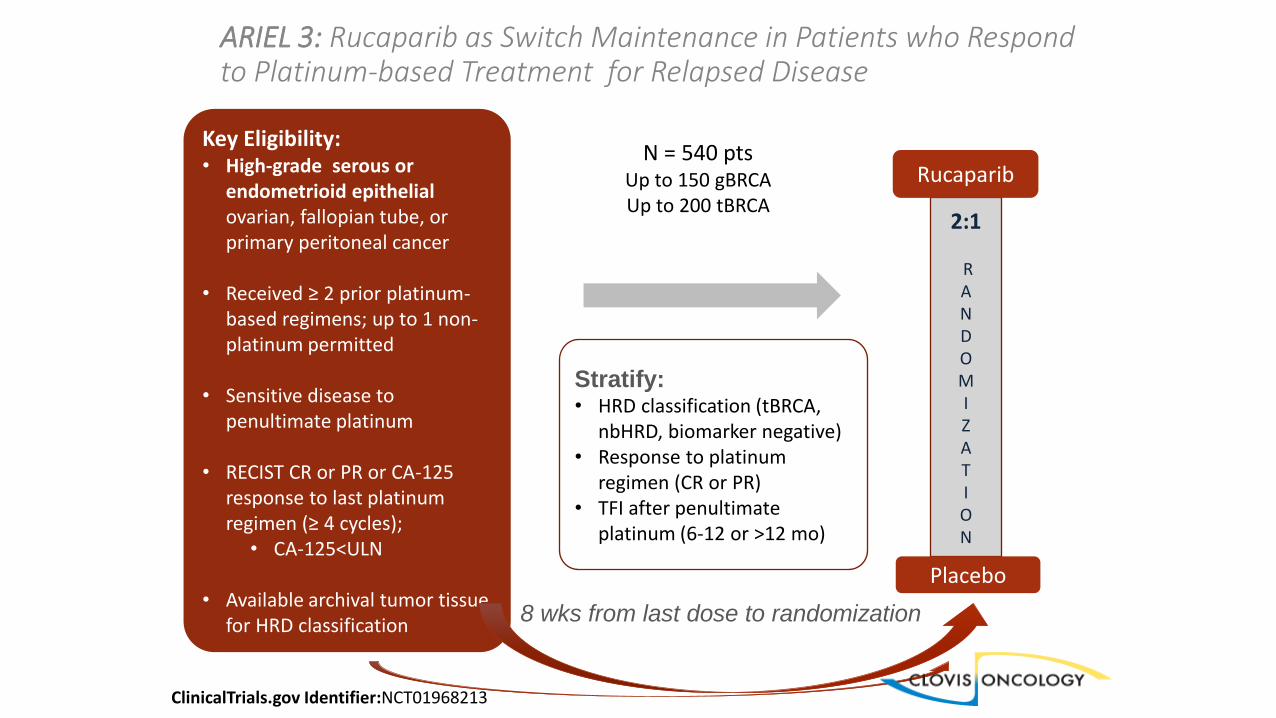
ARIEL 3: Rucaparib as Switch Maintenance in Patients who Respond to Platinum-based Treatment for Relapsed Disease
ClinicalTrials.gov Identifier:NCT01968213
Key Eligibility: • High-grade serous or
endometrioid epithelial ovarian, fallopian tube, or primary peritoneal cancer
• Received ≥ 2 prior platinum-based regimens; up to 1 non-platinum permitted
• Sensitive disease to penultimate platinum
• RECIST CR or PR or CA-125 response to last platinum regimen (≥ 4 cycles);
• CA-125<ULN
• Available archival tumor tissue for HRD classification
N = 540 pts Up to 150 gBRCA Up to 200 tBRCA
Stratify: • HRD classification (tBRCA,
nbHRD, biomarker negative) • Response to platinum
regimen (CR or PR) • TFI after penultimate
platinum (6-12 or >12 mo)
8 wks from last dose to randomization
2:1
R A N D O M I Z A T I O N
Rucaparib
Placebo
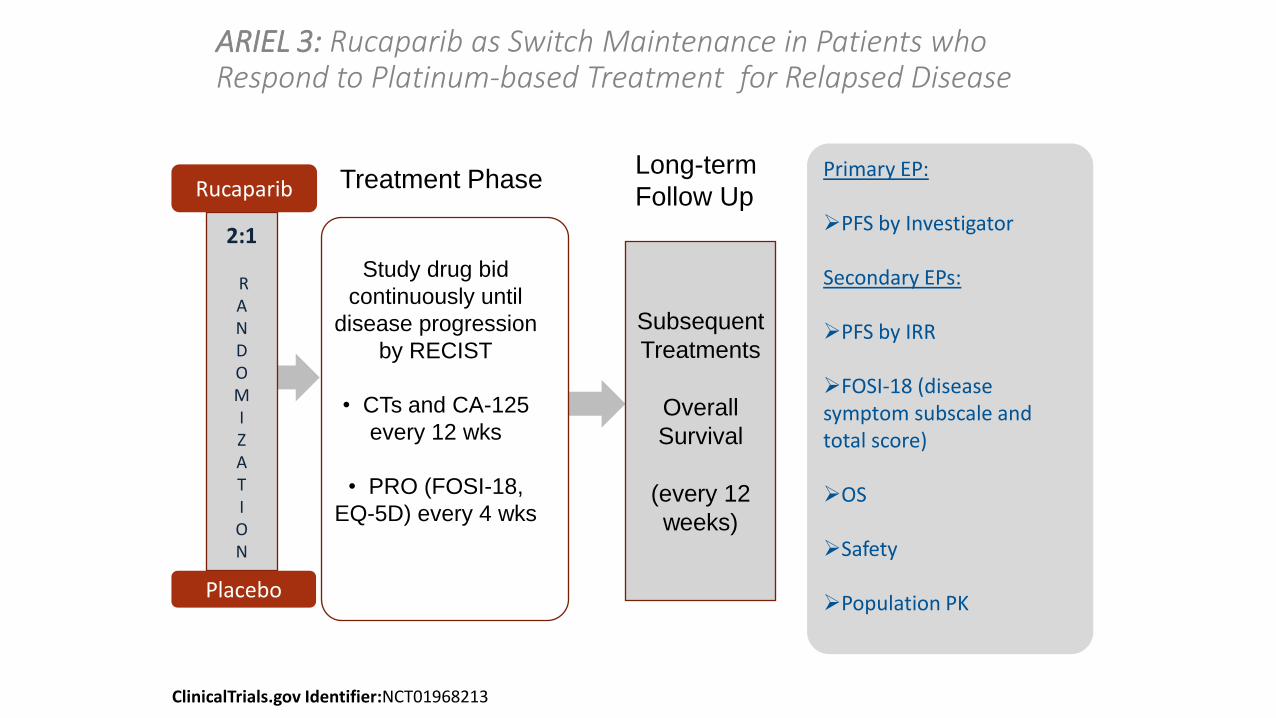
ARIEL 3: Rucaparib as Switch Maintenance in Patients who Respond to Platinum-based Treatment for Relapsed Disease
Study drug bid
continuously until
disease progression
by RECIST
• CTs and CA-125
every 12 wks
• PRO (FOSI-18,
EQ-5D) every 4 wks
Primary EP: PFS by Investigator Secondary EPs: PFS by IRR
FOSI-18 (disease symptom subscale and total score)
OS
Safety
Population PK
Subsequent
Treatments
Overall
Survival
(every 12
weeks)
Treatment Phase Long-term
Follow Up
2:1
R A N D O M I Z A T I O N
Rucaparib
Placebo
ClinicalTrials.gov Identifier:NCT01968213
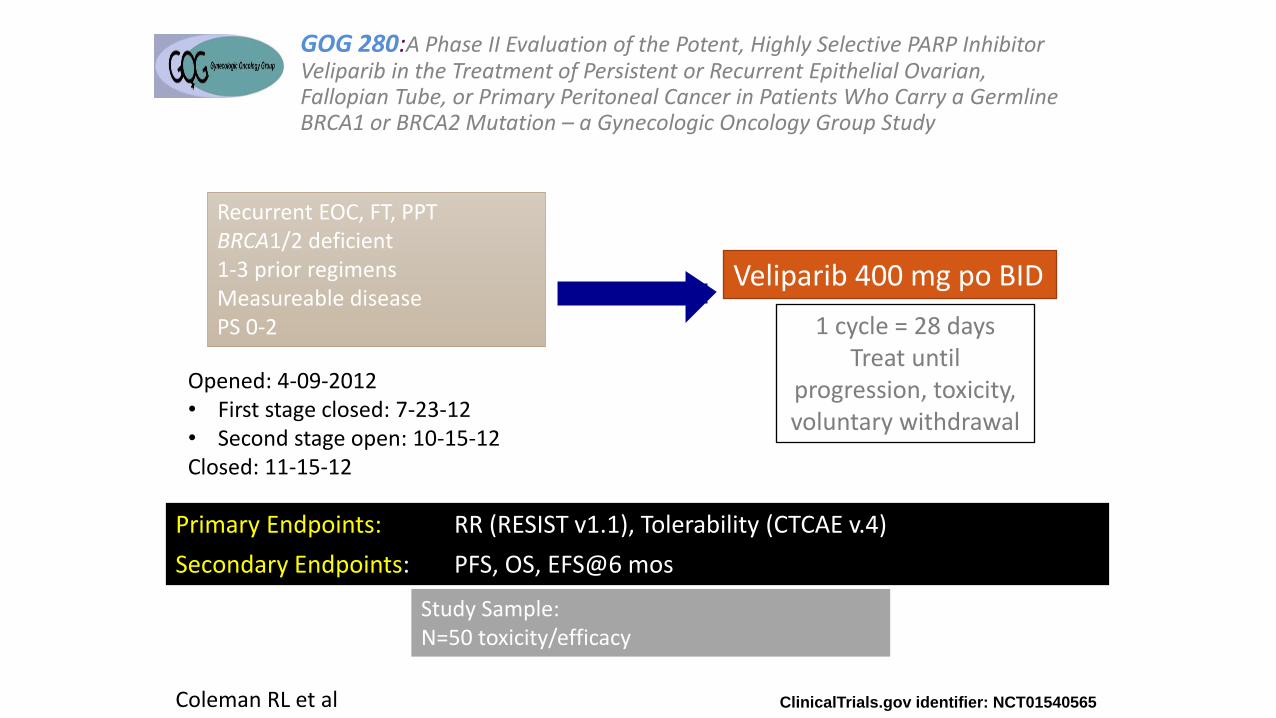
GOG 280:A Phase II Evaluation of the Potent, Highly Selective PARP Inhibitor Veliparib in the Treatment of Persistent or Recurrent Epithelial Ovarian, Fallopian Tube, or Primary Peritoneal Cancer in Patients Who Carry a Germline BRCA1 or BRCA2 Mutation – a Gynecologic Oncology Group Study
1 cycle = 28 days Treat until
progression, toxicity, voluntary withdrawal
ClinicalTrials.gov identifier: NCT01540565
Recurrent EOC, FT, PPT BRCA1/2 deficient 1-3 prior regimens Measureable disease PS 0-2
Veliparib 400 mg po BID
Primary Endpoints: RR (RESIST v1.1), Tolerability (CTCAE v.4)
Secondary Endpoints: PFS, OS, EFS@6 mos
Opened: 4-09-2012 • First stage closed: 7-23-12 • Second stage open: 10-15-12 Closed: 11-15-12
Study Sample: N=50 toxicity/efficacy
Coleman RL et al

Phase II Veliparib: Results
Characteristic Response No Response Total (N) %
Platinum Resistant 6 24 30 20%
Platinum Sensitive 7 13 20 35%
Total N 13 37 50 26%
Fis
her’s
Exact P
= 0
.33
Characteristic Response No Response Total (N) %
BRCA1 10 29 39 26%
BRCA2 3 8 11 27%
Total N 13 37 50 26%
Fis
her’s
Exact P
= 1
.0

Niraparib: NOVA TESARO- ENGOT-OV16
• PFS endpoint primario • Ongoing, pendiente valoración de test predictivo de respuesta en
HRD, Myriad diagnostics presentado en Barcelona 2014
Iparp inhibitors and safety
Olaparib y antiangiogénicos

Presented By Joyce Liu at 2014 ASCO Annual Meeting
Liu J et al, Lancet Oncology 2014
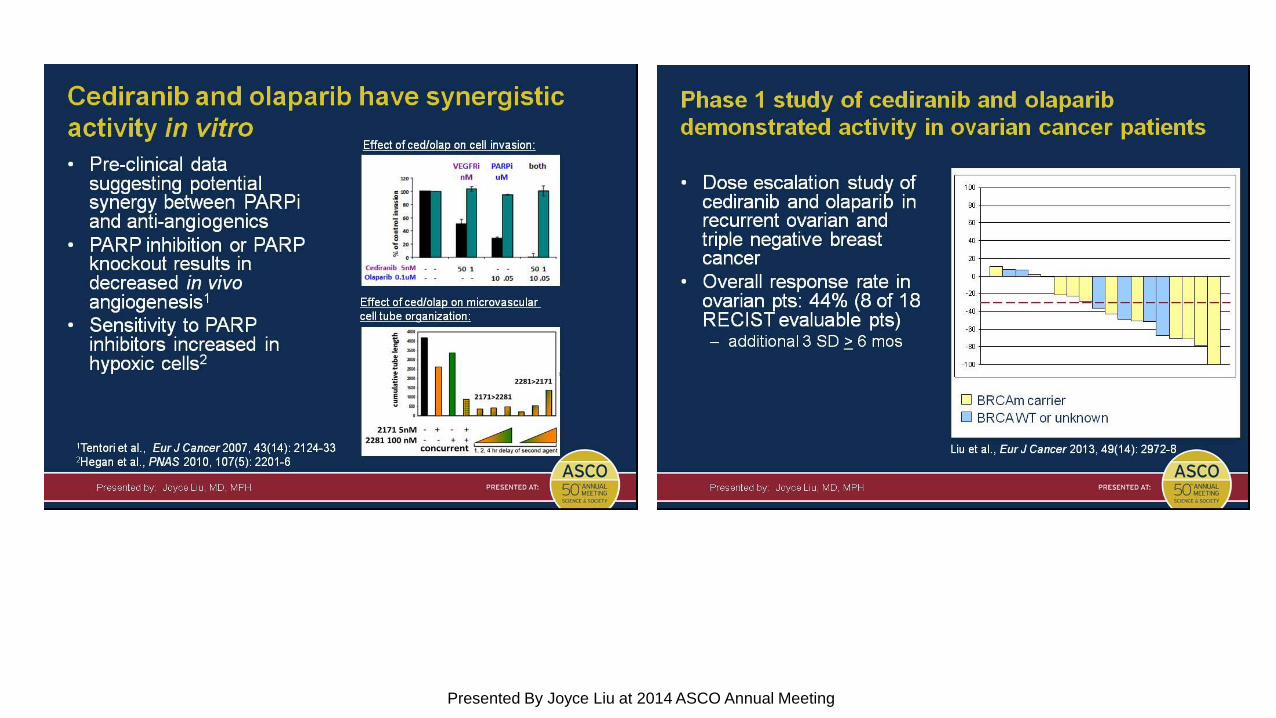
Cediranib and olaparib have synergistic activity in vitro
Presented By Joyce Liu at 2014 ASCO Annual Meeting
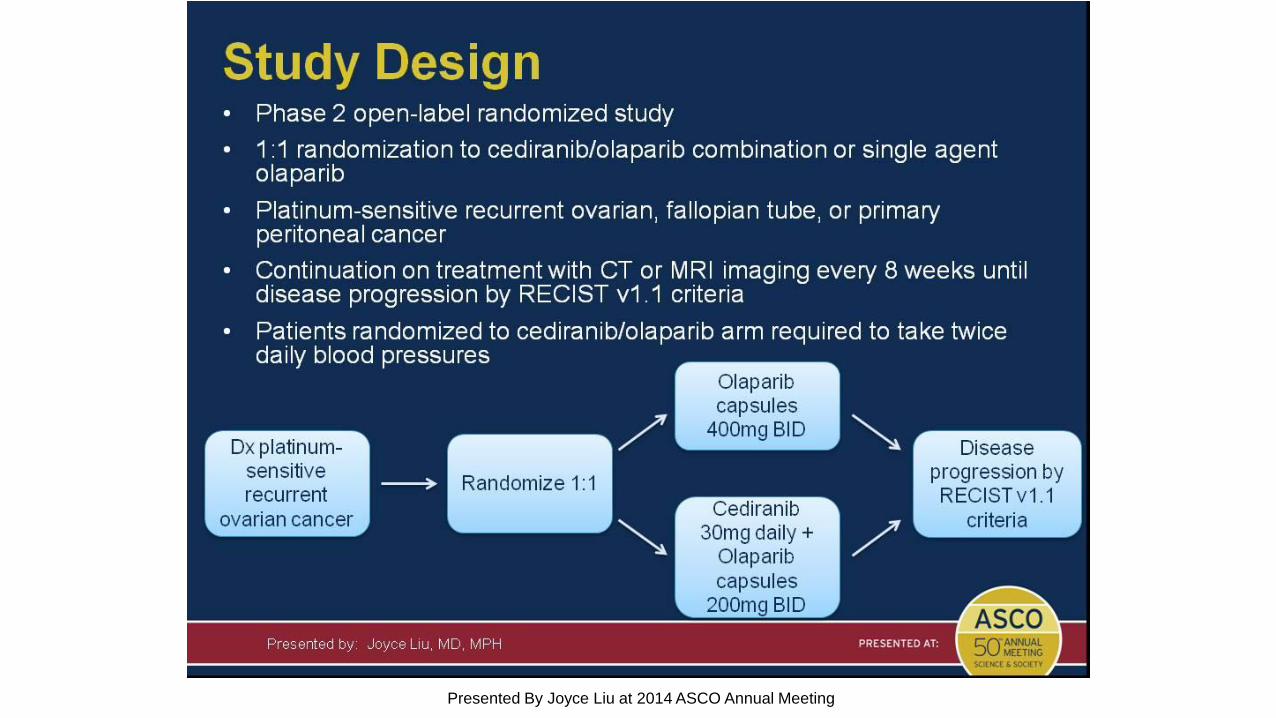
Study Design
Presented By Joyce Liu at 2014 ASCO Annual Meeting
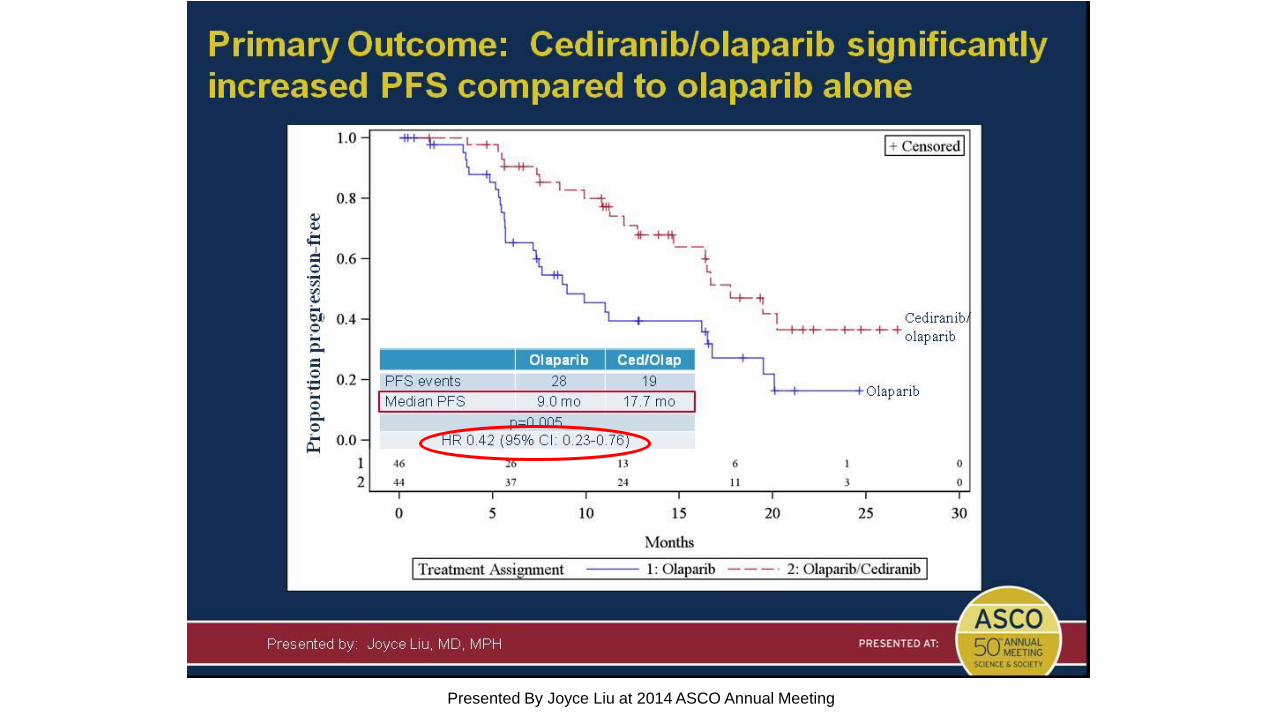
Primary Outcome: Cediranib/olaparib significantly increased PFS compared to olaparib alone
Presented By Joyce Liu at 2014 ASCO Annual Meeting

Secondary Outcome: Cediranib/olaparib significantly increased overall response rate (ORR) compared to olaparib alone
Presented By Joyce Liu at 2014 ASCO Annual Meeting
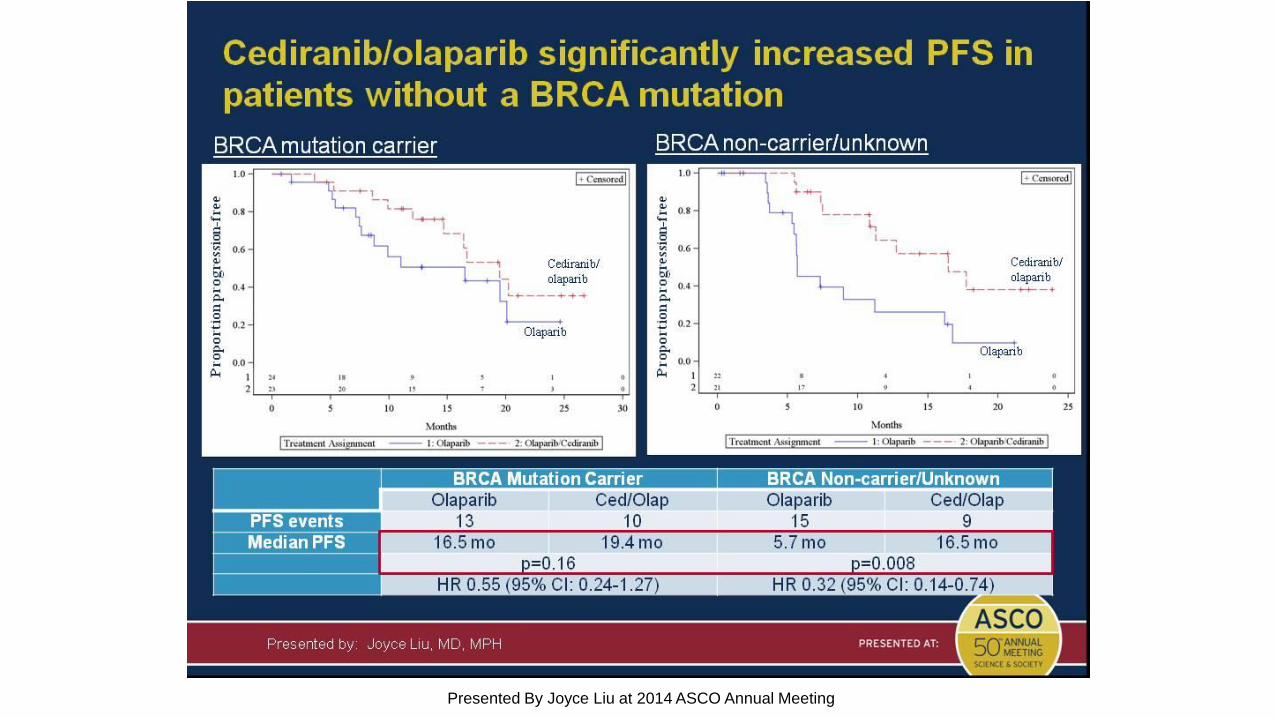
Cediranib/olaparib significantly increased PFS in patients without a BRCA mutation
Presented By Joyce Liu at 2014 ASCO Annual Meeting
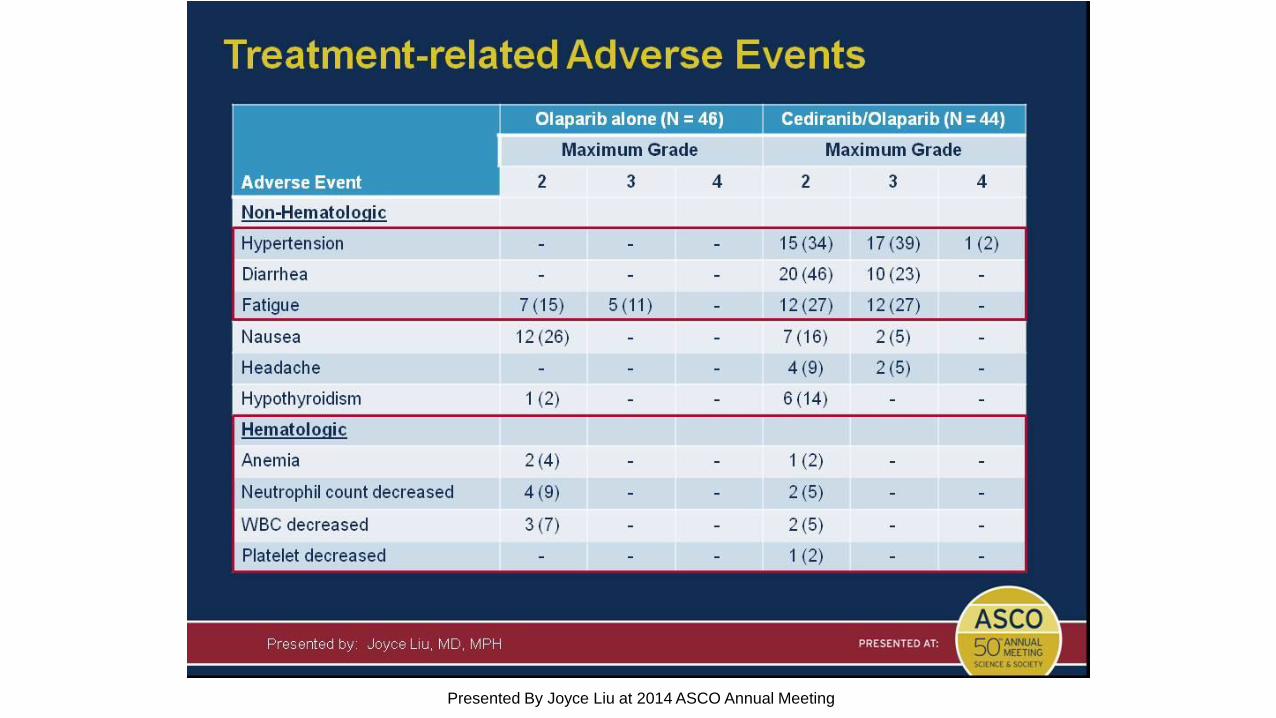
Treatment-related Adverse Events
Presented By Joyce Liu at 2014 ASCO Annual Meeting

Estudio PAOLA: olaparib + bevacizumab
Logística
Guías
Futuro
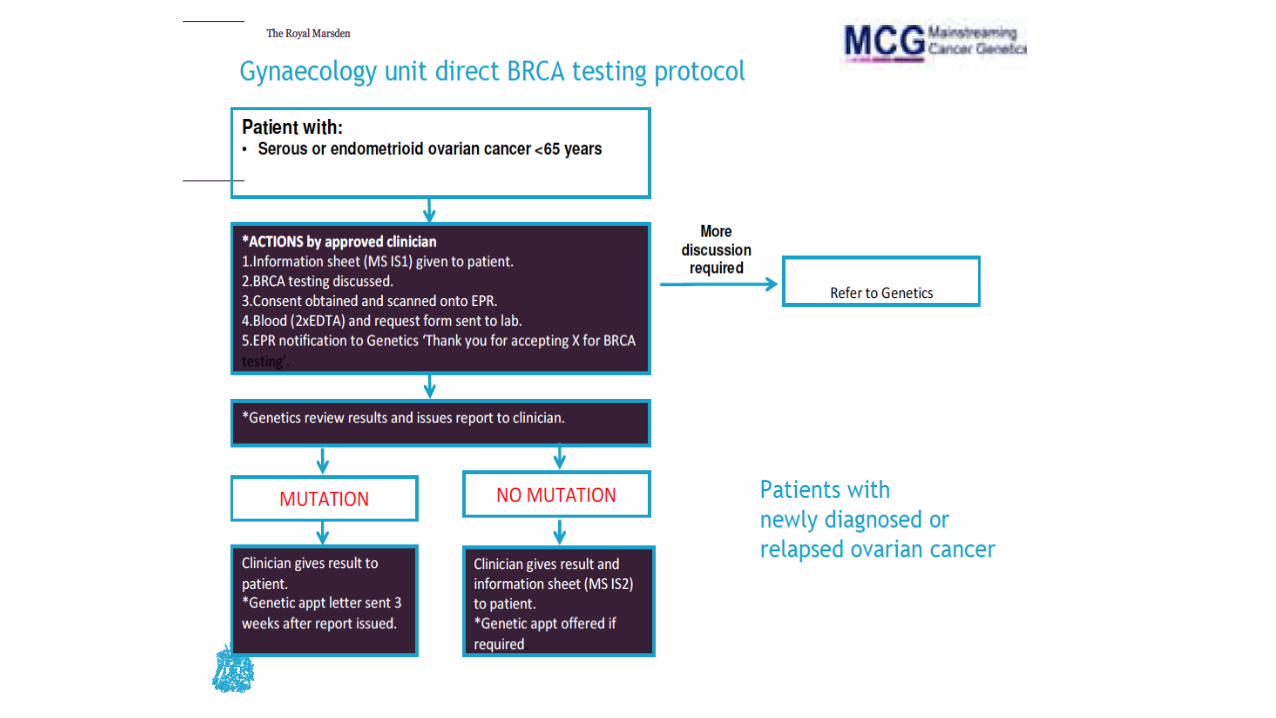

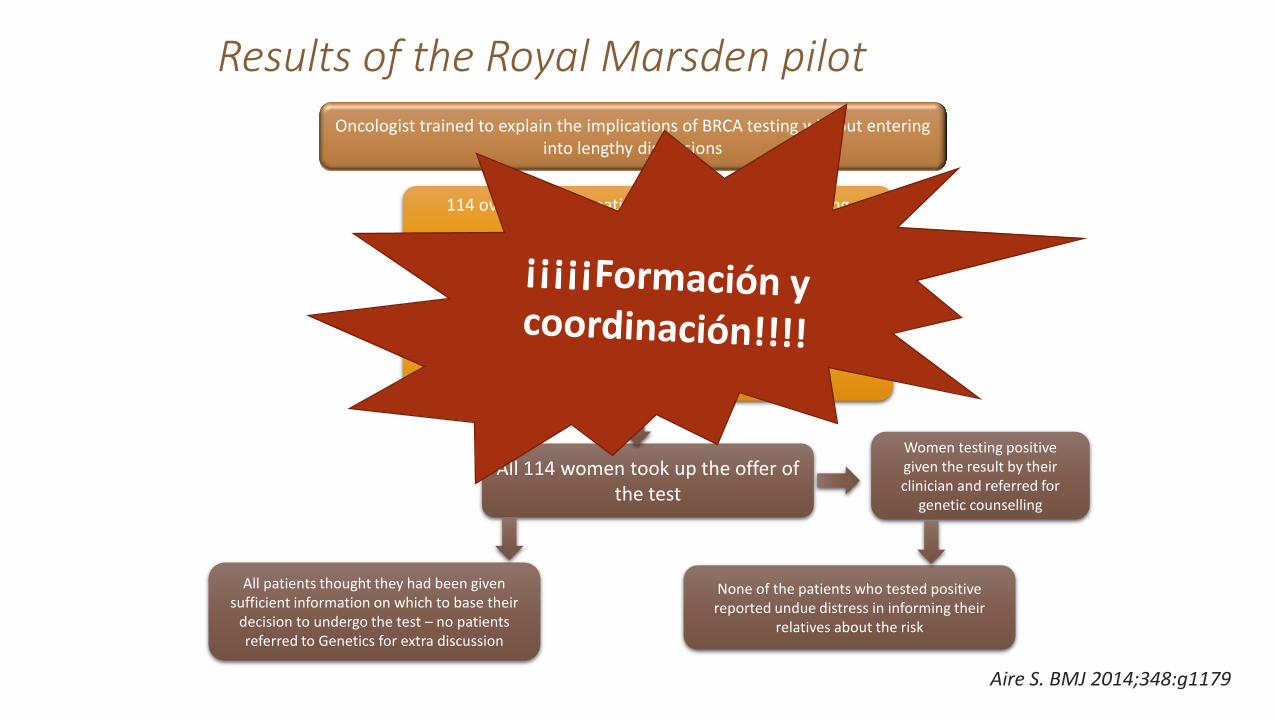
Results of the Royal Marsden pilot
114 ovarian cancer patients selected for BRCA testing (regardless of BRCA risk) –
from July to December 2013
Oncologist trained to explain the implications of BRCA testing without entering into lengthy discussions
Oncologists explained the test and secured patients’ consent, usually during the first consultation
All 114 women took up the offer of the test
All patients thought they had been given sufficient information on which to base their
decision to undergo the test – no patients referred to Genetics for extra discussion
None of the patients who tested positive reported undue distress in informing their
relatives about the risk
Women testing positive given the result by their clinician and
referred for genetic counselling
Aire S. BMJ 2014;348:g1179
Results of the Royal Marsden pilot
114 ovarian cancer patients selected for BRCA testing (regardless of BRCA risk) –
from July to December 2013
Oncologist trained to explain the implications of BRCA testing without entering into lengthy discussions
Oncologists explained the test and secured patients’ consent, usually during the first consultation
All 114 women took up the offer of the test
All patients thought they had been given sufficient information on which to base their
decision to undergo the test – no patients referred to Genetics for extra discussion
None of the patients who tested positive reported undue distress in informing their
relatives about the risk
Women testing positive given the result by their clinician and referred for
genetic counselling
Aire S. BMJ 2014;348:g1179
Logística
Guías
Futuro

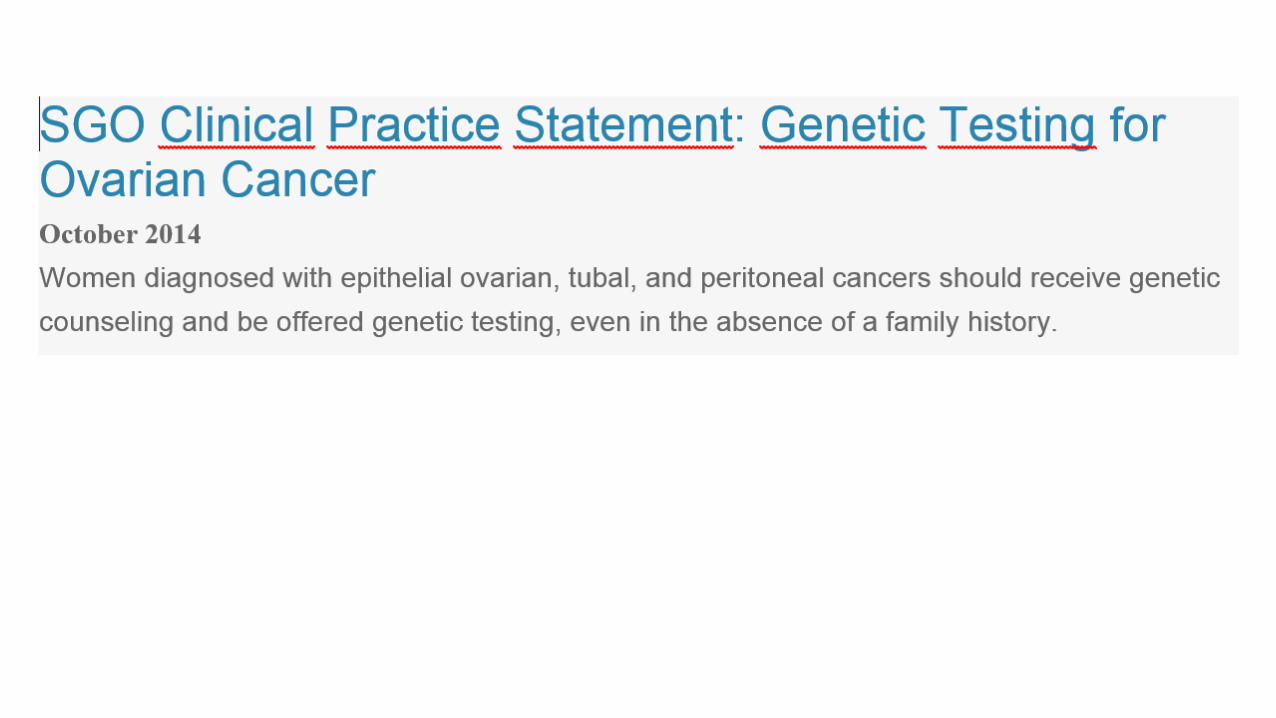
BRCA and high grade epitelial ovarian cancer: Who should be tested?
Logística
Guías
Futuro

Cuestiones por resolver….
• Administración: monoterapia vs combinación
• Biomarcadores de HRD ‒ gBRCA mut BIOMARCADOR ESTABLECIDO BENEFICIO IPARP ‒ ARIEL 2 LOH + BRCAm+ ‒ Mutaciones somáticas BRCA
• ¿Cuándo realizar tests genéticos?
• ¿Quién y cómo?
• Mecanismos de resistencia Iparp y respuesta a QT posterior
• ¿Adyuvancia/Quimioprevención en pacientes con mutación germinal?

Conclusiones
• Los inhibidores de PARP marcan un nuevo hito en el tratamiento del cáncer de ovario
‒ Olaparib indicación en mantenimiento tras recaida sensible a platinos y mutación BRCA
• Beneficio claro en pacientes con déficit de recombinación homóloga
‒ Mutación germinal BRCA biomarcador establecido
GRACIAS POR LA ATENCIÓN [email protected]

















