World Vision: Moving forward from Apprehension to Acceptance, Appreciation, and Advocacy CCIH Conference June 28, 2015 Adrienne Allison, MA, MPA Senior Technical Advisor FP/RH World Vision 1
Transcript
World Vision: Moving forward from Apprehension to Acceptance, Appreciation, and Advocacy
2. Moving forward: from apprehension to acceptance, appreciation and advocacy for Healthy Timing and Spacing of Pregnancy (HTSP) 3. Results of integrating HTSP with MCHN programs
1. World Vision: Who we are
World Vision: • A Christian, humanitarian, development and advocacy
organization dedicated to working with children, families and their communities to help them reach their full potential by tackling the causes of poverty and injustice.
• One of the world’s largest child-focused non-governmental organizations that covers almost 100 countries, serving all people.
• WV’s goal – the sustained well-being of children within families and communities
1. World Vision: Who we are In 2006, the WV partnership adopted an updated “Policy on Reproductive Health” : • “WV’s reproductive health programs are based on biblical principles,
the best medical knowledge available, and good medical ethics. • WV employs established best practices for reproductive health. • WV holds the position that human life begins at conception. WV does
not provide, recommend nor support abortion nor methods of family planning that are determined to be abortive.
• WV respects the rights of parents to make their own decisions about family size and spacing without coercion.
• WV programs offer complete, accurate, unbiased, updated and comprehensive information disseminated in a caring, respectful, empowering, culturally and age-appropriate manner.”
1. World Vision: Who we are This partnership wide statement responded to three constituencies within World Vision: 1. Europe and offices in other developed countries supported the term
“reproductive health”. 2. Canada and the USA could not accept “reproductive health” because,
according to the 1994 International Conference on Population and Development, this includes the right to safe abortion .
3. WV US and partners in developing countries objected to “Family Planning” because it meant abortion, population or fertility control.
4. “FP” not resonate with youth who were not concerned with planning families, but with avoiding pregnancy.
How to move from apprehension to consensus within the World Vision Partnership?
2. Moving forward: acceptance, appreciation, advocacy • By 2007, WV agreed to the term “Birth Spacing”. • The USAID “Integrated Birth Spacing Project” enabled WV to integrate
Birth Spacing with MCHN programs in Haiti, India and Senegal, and called for capacity building for Birth Spacing within the WV partnership.
• Cautious acceptance for Birth Spacing grew as new data on the impact of timing and spacing on infant child and maternal mortality was published.
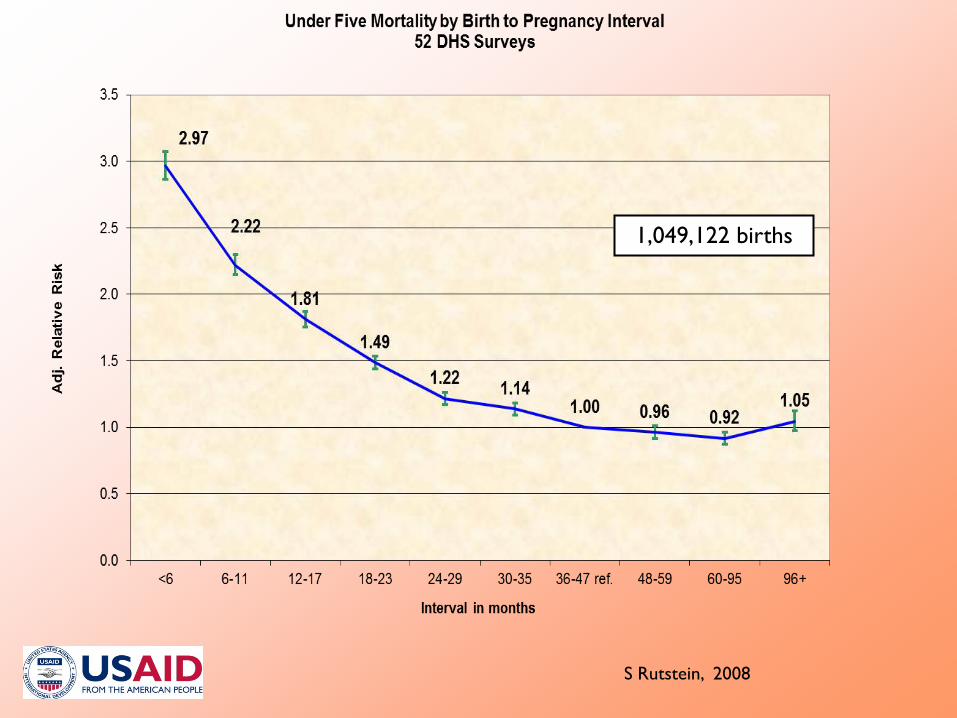
• The breakthrough came in 2008, with the publication of Rutstein’s analyses of 52 Demographic and Health Surveys of 1.12 million births in developing countries from 2000 to 2005.
• Concurrently, we recognized that only pregnancies, not births can be spaced.
• Discarding “FP” and “Birth Spacing”, we renamed our approach “Healthy Timing and Spacing of Pregnancies”.
2. Moving to forward
• The WV partnership confirmed that HTSP directly “sustained the well-being of families and communities”, consistent with WV values.
• We gave webinars for WV’s global Health Team, participated in global and regional team meetings in Bangkok, Cypress, and Dakar and Mombasa, and lead workshops in Haiti, India and Senegal.
• We began to build a global group of champions, beginning with a very few.
• They in turn began to integrate HTSP within WV’s well-documented integrated strategy for MCHN.
0
0.5
1
1.5
2
2.5
3
3.5
4
<6 6 to 11 12 to 17 18 to 23 24 to 29 30 to 35 36 to 47 48 to 59
Mortality Risk
Birth-to-Pregnancy Interval (months)
InfantNeonatalEarly Neonatal
Birth to Pregnancy Intervals and Relative Risk of Neonatal and Infant Mortality
S Rutstein, 2008
1,049,122 births
S Rutstein, 2008
Percent of Children Alive and Not Undernourished by Duration of Preceding Birth to Conception Interval
HTSP messages on the risks of early pregnancy: • Pregnancy is the leading cause of death for teenage girls
globally • Girls age 15 to 19 are twice as likely to die in pregnancy
and childbirth as those age 20 – 24 • Girls less than 15 years old are 5 times more likely to die • Infants of teenage girls are almost twice as likely to die as
those born to mothers age 20 – 24. • Up to 40% of infants whose mothers’ die after childbirth
will likewise die before their first birthday. USAID, 2012
2. Moving forward – one photo, one statement
• Babies born less than 2 years apart are more than twice as likely to die before their first birthday, compared to babies born 3 to 4 years apart.
S. Rutstein, 2005
2. Moving forward – using evidence
WV MCHN programs consistently use 4 key messages: 1. Wait until age 18 before trying to become pregnant 2. Wait at least 6 months before trying for another
pregnancy after a miscarriage or abortion 3. Wait until your child is at least 2 years old before trying
for another pregnancy 4. Limit pregnancies to a mother’s healthiest ages, 18 to 34.
3. Results within World Vision • HTSP integrated within MCHN programs being implemented in 28
countries. • HTSP integrated with Life Skills training in Latin American, Middle
East and Eastern Europe. • HTSP messages integrated into the WV global Child Health Now
campaign, urging governments to MDG 4, 5 and 6; and within Sustainable Development Goals, to support universal access to MCHN services including HTSP.
• WV adopted began to support the use of Emergency Contraceptive Pills in 2011.
• WV includes HTSP in Global Policy Guidelines and Health technical guidelines.
Thank you!
3. Results • Using the term “HTSP” enabled WV to focus on healthy fertility to
save the lives of infants, children and their mothers. • Within communities, WV built new and lasting support for HTSP
among faith leaders and community influentials, (fathers, mothers and mothers-in-law) by discussing the health benefits of HTSP – a rationale that successfully replaced earlier foci on demographic or economic benefits of family planning.
• Burundi – CPR rose from an estimated 18% to 50% in
Rutegama • Haiti – CHWs deliver DMPA, and CPR rose from 12% to 18%
in Plateau Centrale and La Gonave • India – CPR increased from 44% to 77% in Hardoi, Uttar
Pradesh • Senegal – CPR rose from 12% to 17% in part of Fatick
District; imams supported HTSP in Friday prayers, and Catholic sisters promoted Standard Days Method, LAM, and referred to MOH for other methods.
3. Results – pilot projects produced strong results
Pregnant Women Children 0-24 months 1. Adequate diet 2. Iron/folate supplements 3. Tetanus toxoid
immunisation 4. Malaria prevention (IPT) 5. Healthy Timing and
Spacing of Pregnancies (HTSP)
6. De-worming 7. Access to antenatal and
postnatal care, skilled birth attendance, prevention of mother-to-child transmission of HIV
1. Appropriate breastfeeding 2. Essential Newborn Care 3. Hand washing 4. Appropriate complementary
feeding (6-24 months) 5. Adequate iron 6. Vitamin A supplementation 7. Oral Rehydration Therapy &
Zinc 8. Care seeking for fever 9. Full immunisation for age 10. Malaria prevention 11. De-worming (+12 months)
3. Results – Global MCHN Strategy includes HTSP
Support from political and relligious leaders for HTSP to save llives