15
Ebola: FBO & community perspectives Nepal– why CCIH matters E Anne Peterson, MD,MPH Senior Vice-President Programs AmeriCares
| Date post: | 17-Aug-2015 |
| Category: |
Healthcare |
| Upload: | christian-connections-for-international-health |
| View: | 30 times |
| Download: | 2 times |

Ebola: FBO & community perspectives Nepal– why CCIH matters
E Anne Peterson, MD,MPH Senior Vice-President Programs AmeriCares
Community response to Ebola
Church in slums of Freetown Sierra Leone
Conducted a community and FBO assessment in Liberia and sierra Leone: Oct/Nov 2014
7/20/2015 2

Community response to Ebola
Cases surging in Liberia, traveling towards capital in Sierra Leone
·High media penetration to main messages but response was not as desired: still had late arrivals to ETU & secret burials
·High fatality rate, small difference in ETU survival and the messaging of the dangers > “why go to ETU? better to die at home with family”
7/20/2015 3
·“Don’t touch”: correct from infection control standpoint but not for a mother caring for children
·“come to ETU if you have these symptoms”: community correctly assessed that they were still most likely to have malaria, viral diarrhea… not Ebola. Why risk your child getting Ebola by going to ETU???
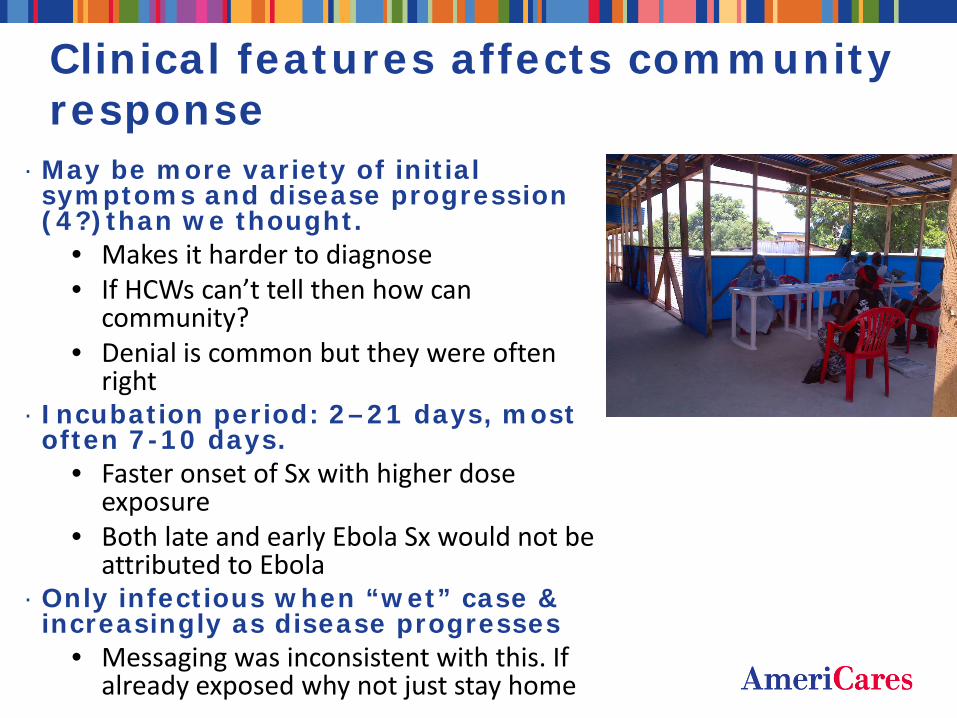
Clinical features affects community response
· May be more variety of initial symptoms and disease progression (4?)than we thought.
• Makes it harder to diagnose • If HCWs can’t tell then how can
community? • Denial is common but they were often
right · Incubation period: 2–21 days, most often 7-10 days.
• Faster onset of Sx with higher dose exposure
• Both late and early Ebola Sx would not be attributed to Ebola
· Only infectious when “wet” case & increasingly as disease progresses
• Messaging was inconsistent with this. If already exposed why not just stay home

Trust requires knowing their priorities: Massive indirect impacts of Ebola
1. Economic- first named concern, · Businesses closed, reduced income, · Travel restrictions · Increased price & decreased access
to food & goods, · Reduced from 2 to one meal per day
in slums with NO Ebola -yet 1. Health – non-Ebola excess mortality · Closed OPD & hospital · Diverted prevention programs · Reduced access · Could have been prevented
3. Education- schools closed 4. Girl & child protection: pregnancies, abuse…abandonment-
huge!
· Can’t wait for the end of Ebola – escalating quickly · Lots of people available for non-Ebola work
Assists in Ebola efforts by: · reducing competing diagnostic dilemmas · Rebuilding trust and resilience to deal with Ebola

Ministry of Social Welfare, Gender and Children's Affairs/Partners
Sources: March 17, 2015 Summary Report on the Rapid Registration of Ebola Affected Children, Ministry of Social Welfare, Gender and Children's Affairs/Partners; March 18, 2015 Updated Case Counts from WHO SitReps
Sierra Leone: Ebola Case Counts, Mar 17, 2015 and Ebola-affected Children Counts, Mar 18, 2015
11779
18,225
02000400060008000
100001200014000160001800020000
total EBV cases total affected childrenTotal Affected Children
Total EBV Cases
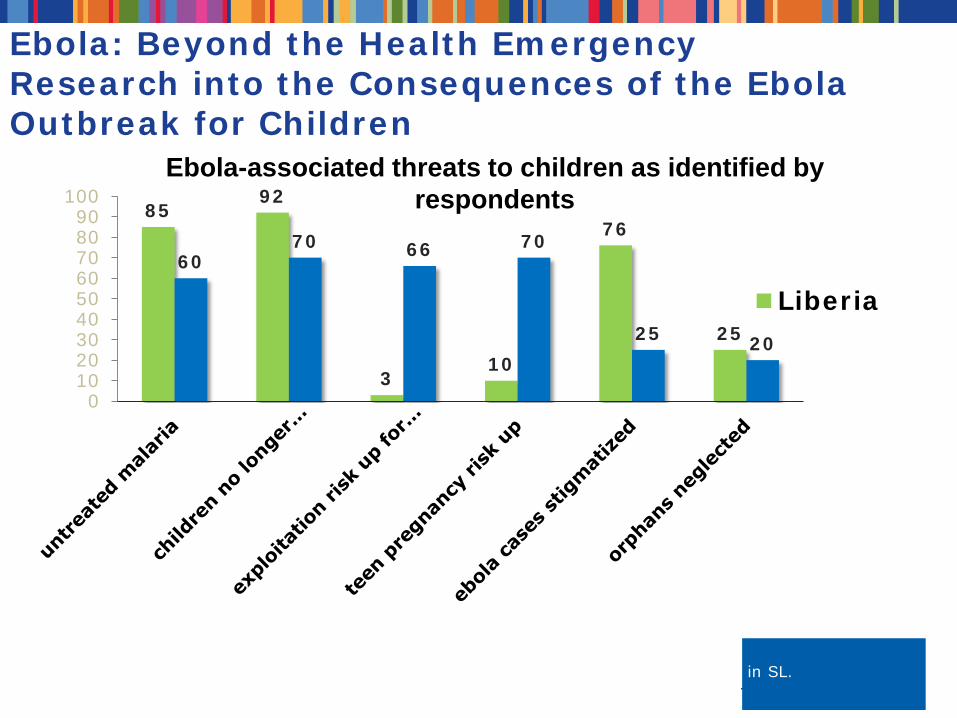
85 92
3 10
76
25
60 70 66 70
25 20
0102030405060708090
100
Liberia
Ebola-associated threats to children as identified by respondents
NOTE: Exploitation and teen pregnancy reported by adults in Liberia and child respondents in SL.
Ebola: Beyond the Health Emergency Research into the Consequences of the Ebola Outbreak for Children

“Social mobilization” – community empowerment & ownership
· Currently communities are treated as powerless victims. This leads to less than optimal responses: fatalism, blame, stigma, hopelessness
· Communities were passive – not part of the response • But they are the largest population and the ones who most care about the
impact of Ebola • Engaging them multiplies the respondents immeasurably • This was done with small pox • Requires:
o that they see that they CAN do something, o that it WILL make a difference o That responding will help with their other higher level needs. o (Ebola is less a pervasive threat than the economic impact and other
health impact)

Role of Faith-based organizations Engage earlier, enable them
·FBOs were responding: • Mixed but mostly in good ways • Information source was primarily public or
media sources • Most were disconnected from decision
making, organizational pillars so information and coherence to overall efforts was difficult
·Faith leaders are usually trusted leaders in their communities
• Armed with correct information and messages they can help disseminate fear, overcome mistrust of the government
• Voice of the community was also not at the decision tables and faith leaders can give voice to the community perspective
• They saw and voiced the indirect impacts early and are well positioned to respond 7/20/2015 9
First Lady of Sierra Leone
5 key areas of FBO Ebola response · Stop Ebola spread: burial, home protection, treat patients
· “Social mobilization” – community empowerment & ownership.
• Message from community perspective o Go so that you protect your family
• Communications: both ways • Daily updates: Ebun James-DeKam, General Secretary,Council of Churches in Sierra
Leone · Enhance role of faith leaders; training & empowerment
• Reduce bad messages • Enhance positive messages • Train in their faith language
· Kids, Survivors & families: address needs of those directly devastated • Fear of getting Ebola • Limitation of economics for absorbing abandoned kids • Double orphans • Destruction of Ebola homes • Trauma counseling
· Address massive indirect impacts of Ebola • Health 10 fold higher deaths than Ebola • Food • Vulnerabilities: sex, labor, total abandonment • Education 2.5 m kids out of school

· Example of a technical issue that usually disseminated out through health/technical channels & experts
· At Ebola centers: triage • Only Ebola patients > Ebola beds reduced overload of patients • Reduced transmission in ETUs
· At OPD & non-Ebola hospitals • Only non-Ebola patients here & HCWs can safely return to work • Patients can safely seek Rx for malaria etc • Massive reduction in excess mortality possible
· At community burials • Only Ebola patients require Ebola burial & houses decontamination • Faster care for family contacts • Less anger at burial teams & government, fewer secret burials
FBOs & church leaders are needed so community will understand, trust and act on all the benefits of upcoming availability of an Ebola RDT
Rapid diagnostic test: game changer

Nepal
12
AmeriCares Response
13

CCIH contribution
14
Take home thoughts · Correct messaging & better mobilization could have changed the trajectory
and size of the Ebola catastrophe
· FBOs provide essential services
· FBOs can work with governments to their mutual benefits – it just takes finding common ground and language
· Even in dilemmas that are very technical Faith leaders can help if empowered
· FBOs themselves are part of the body of Christ –can and should play a role in empowering the church
· Working with each other, we can multiply our impact · We still have the opportunity to avert some of the follow-on consequences of
Ebola.
· Rebuild Trust. Rebuild the health system
15
Thank You

















