25
Ch. 7 – Human Error in Health Care ETM 591 Adams, Duong, Lockwood, Meador September 23, 2010
| Date post: | 19-Dec-2015 |
| Category: |
Documents |
| View: | 213 times |
| Download: | 0 times |

Ch. 7 – Human Error in Health
Care
ETM 591Adams, Duong, Lockwood, Meador
September 23, 2010

04/18/23 2
Presentation Summary
• Introduction to Human Error in Health Care• Facts / Figures• Human Error in Medication• Human Error in Anesthesia• Human Error in Medical Devices• Human Error in Misc. Health Care Areas• Useful Guidelines to Prevent Occurrence of
Human Error• Scholarly Works on Human Error in Health Care• Conclusion
ETM 591 - Reliability and QA

Introduction to Human Error in Health Care
• History of human error in health care traced back to anesthetic death in 18481,2
• Studies regarding human error started to be conducted in 1950s and 1960s (main focus on anesthesia-related deaths)3,4
• 8th leading cause of death in U.S.• Annual total national cost of medical adverse
events is estimated to be $38 billion ($17 billion thought to be preventable)5
04/18/23 ETM 591 - Reliability and QA 3

Health Care Related Error – Facts/Figures
• Each year, more than 100,000 U.S. citizens die due to human error in the health care system5
• More than 50% of technical equipment problems linked to operator error9
• 7,391 people died due to medication errors (1993)7,10
• $7 billion – annual cost due to medication errors11
• Patient mistakenly give 120 cm^3 per minute of a powerful drug instead of 12 cm^3 per hour; patient died in New York City hospital (1990)19
04/18/23 ETM 591 - Reliability and QA 4

Human Error in Medication
• Medication Error – any preventable event that may lead to incorrect medication use or patient harm while the medication is in the control of a health care professional, consumer, or patient
• Types of Medications Errors:– Omission error– Incorrect dose error– Incorrect time error– Incorrect drug preparation error– Prescribing error– Unauthorized drug error– Incorrect dosage form error– Incorrect administration method error
04/18/23 ETM 591 - Reliability and QA 5

Human Error in Medication• Several Common Reasons:
– Poorly trained personnel– Illegible handwriting– Excessive Workload– Errors in labeling– Incorrect transcription
• Guidelines to Reduce Occurrence of Errors– Write legibly or use computer generated prescriptions– Don’t leave medication near patient’s bedside– Check patient’s I.D. bracelet before administering medication– Carry out dosage calculations on paper, not in head– Carefully check drug label three times– Avoid distractions when preparing medication for administration– Others
04/18/23 ETM 591 - Reliability and QA 6

Human Error in Medication
04/18/23 ETM 591 - Reliability and QA 7

Human Error in Anesthesia• Anesthesiology
– Element of Medicine to render patient insensitive to pain
• Defined in Two Ways– Mistake: linked an actual or probable adverse
out come– Slip: did not occur according to the plan
• Risk of Death– According to Canadian Medical Assoc. Journal,
(Anaesthesia in 1984, How safe is it?)• 1952-1984; decreased from 1 in 2,680 to approx
1 in 10,00004/18/23 ETM 591 - Reliability and QA 8

• Common Anesthesia Errors
04/18/23 ETM 591 - Reliability and QA 9
Human Error in Anesthesia
Common Anesthesia Errors
Premature extubation
Drug overdose
Syringe
Swap
Inadver-tent change in gas flow
Hypoventi-
lation (opera
tor error)
Wrong selecti
on airway
Mgtmethod
Loss of oxyge
n supply
Ampoule
swap
Breathing circuit disconnect
Breathing
circuit leak
Incorrect
blood transfused

• Methods to Prevent or Reduce Anesthetic Mishaps
Method I Method II
04/18/23 ETM 591 - Reliability and QA 10
Human Error in Anesthesia
Find out What Is going on
Collate all the Relevant information
Classify the problem errors and their contributing
factors
Develop preventative strategies
Implement strategies
Review strategies
Design and Organize workspace
Assure equipment performance to effective levels
Supervise and Train
Use appropriate monitoring instrumentation and vigilance
aids
Develop and closely follow all appropriate preparation and
inspection protocols
Act on incident reports in an effective manner
Recognize the limitation that influence individual
performance

Human Error in Medical Devices
• Human factors related problems encountered by novice and highly competent personnel– Cognitive, perceptual, and physical abilities by user
• Medical devices with High Incident of Human Errors
04/18/23 ETM 591 - Reliability and QA 11

Human Error in Medical Devices
• Human Errors causing user-interface design problems– Poorly designed labels, ambiguous displays, complex
installation/maintenance tasks, confusing operating instructions
• Medical Device-Associated Operator Errors
04/18/23 ETM 591 - Reliability and QA 12
Human Error in Medical Devices
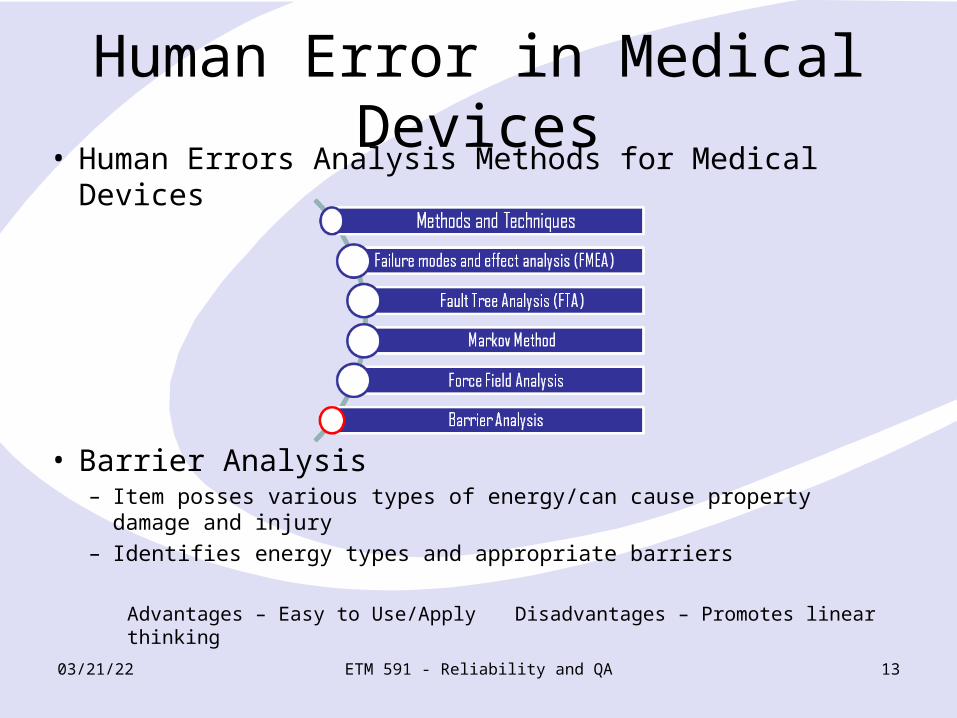
• Human Errors Analysis Methods for Medical Devices
• Barrier Analysis– Item posses various types of energy/can cause property damage
and injury– Identifies energy types and appropriate barriers
Advantages – Easy to Use/Apply Disadvantages – Promotes linear thinking
04/18/23 ETM 591 - Reliability and QA 13

Human Error in Miscellaneous Health Care Areas
• Emergency medicine • Intensive care units• Operating rooms• Radiotherapy• Image interpretation
04/18/23 ETM 591 - Reliability and QA 14
Human Error in Emergency Medicine
• 100 million emergency visits in U.S./year36
• Error result in substantial # of adverse events36
– Facts• 90% are preventable37, 38
• Missed diagnoses ~4.3% of 1,817 acute cardiac ischemia patients
incorrectly discharged39
• 8 – 11% disagreement in interpretation of radiographs between emergency radiologists & physicians40
04/18/23 ETM 591 - Reliability and QA 15

Reduce error by asking these questions39:
1. Ways to make errors more visible?2. Presence of pharmacologist?3. Usefulness of computerized clinical
information?4. Adjusting change-of-shift & lengths
of shifts?
04/18/23 ETM 591 - Reliability and QA 16

Human Error in Intensive Care Units (ICU)
• In 1960, 10% hospitals with › 200 beds in U.S. had ICU41, 42
• Currently more than 40,000 patients/day in ICU in U.S.
• Facts– From 1989-1999, most critical incidents due to staff
personnel errors43
– 66% of incidents in 7 ICU in 1 year were human errors44
– 554 human errors in a 6-bed ICU in 6-month45
• 45% by physicians45 • 55% by nursing staff45
04/18/23 ETM 591 - Reliability and QA 17

Important Identified Factors43
• Poor communication• Inadequate training & experience• Staff shortage• Night time
04/18/23 ETM 591 - Reliability and QA 18

10 Useful Guidelines to Prevent Occurrence of Human Error46
1. Simplify. Reducing # of process steps, nonessential procedures, equipment, & software; # of times an instruction is given, etc.
2. Redesign patient record for effectiveness. Currently too voluminous with buried important information
3. Stratify. Avoid over-standardization4. Make improvements in communication
patterns. Team members repeat orders to ensure instructions are clearly & correctly understood
04/18/23 ETM 591 - Reliability and QA 19

10 Useful Guidelines to Prevent Occurrence of Human Error46
5. Automate cautiously. Not over-automating because may prevent operators from judging true system state
6. Respect human shortcomings. Memory limitations, workload, stress, circadian rhythm, & time pressure in designing work systems & tasks
7. Standardize. Limit unneeded variety: supplies, drugs, equipment & rules. Procedure performed on regular basis reduce error
04/18/23 ETM 591 - Reliability and QA 20

10 Useful Guidelines to Prevent Occurrence of Human Error46
8. Use defaults effectively. Make correct action the easiest one. Default as standard order or rule that work well if nothing else intervenes
9. Use affordances. Designing features in items that automatically force proper use by providing clues to correct operation
10.Use sensible checklists. Developing & using checklists sensibly & effectively
04/18/23 ETM 591 - Reliability and QA 21

Scholarly Works on Human Error in Health Care
• Reason, J. (2000). Human error: models and management. British Medical Journal, Retrieved from http://www.bmj.com/content/320/7237/768.full?ijkey=1181633917c8e870e42b6e210c8ca71ef69c325a&keytype2=tf_ipsecsha
• Cochrane,G. Toit, R. Mesurier, R. (2010). Management of refractive error. British Medical Journal, Retrieved from http://www.bmj.com/content/340/bmj.c1711.full?sid=87684ed7-3c41-49c6-a877-c493c7f2e435
• Cooper, J. Newbower, R. Long, C. McPeek, B. (2002). Preventable anesthesia mishaps: a study of human factors. Quality and Safety in Healthcare, Retrieved from http://qshc.bmj.com/content/11/3/277.abstract
• Leape, L. Woods, D. Hatlie, M. Kizer, K. Schroeder, S. Lundberg, G. (1998). Promoting patient safety by preventing medical error. The Journal of the American Medical Association, 280(16), Retrieved from http://jama.ama-assn.org/cgi/content/full/280/16/1444
04/18/23 ETM 591 - Reliability and QA 22

References• 1. Beecher, H.K. The First Anesthesia Death and Some Remarks Suggested by It on the Fields of
the Laboratory and the Clinic in the Appraisial of New Anesthetic Agents. Anesthesiology 2 (1941): 443-449.
• 2. Cooper, J.B., Newbower, R.S., Kitz, R.J. An Analysis of Major Errors and Equipment Failures in Anesthesia Management: Considerations for Prevention and Detection. Anesthesiology 60 (1984): 34-42.
• 3. Edwards, G., Morlon, H.J.V., Pask, E.A. Deaths Associated with Anesthesia: A report on 1,000 Cases. Anesthesia 11 (1956): 194-220.
• 4. Clifton, B.S., Hotten, W.I.T. Deaths Associated with Anesthesia. British Journal of Anesthesia 35 (1963): 250-259.
• 5. Kohn, L.T., Corrigan, J.M., Donaldson, M.S., eds. To Err Is Human: Building a Safer Health System. Washington, D.C: Institute of Medicine, National Academy of Medicine, National Academies Press, 1999.
• 7. Dhillon, B.S. Human Reliability and Error in Medical System. River Edge, NJ: World Scientific Publishing, 2003.
• 9. Dhillon, B.S. Medical Device Reliability and Associated Areas. Boca Raton, FL: CRC Press, 2000.
• 10. Phillips, D.P., Christenfeld, N., Glynn, L.M., Increase in U.S. Medication-Error Deaths Between 1983 and 1993. Lancet 351 (1998): 643-644.
• 11. Wechsler, J. Manufacturers Challenged to Reduce Medication Errors. Pharmaceutical Technology February (2000): 14-22.
• 19. Belkin, L. Human and Mechanical Failures Plague Medical Care. New York Times, March 31, 1992, B1, B6.
04/18/23 ETM 591 - Reliability and QA 23

References• 36. Kyriacou, D,N., Coben, J.H. Errors in Emergency Medicine: Research Strategies. Academic
Emergency Medicine 7 (2000): 1201-1203.• 37. Wears, R.L., Leape, L.L. Human Error in Emergency Medicine. Annals of Emergency
Medicine 34 (1999): 370-372.• 38. Bogner, M.S., ed. Human Error in Medicine. Hillsdale, NJ: Lawrence Erlbaum Associates,
1994.• 39. Pope, J.H., Aufderheide, T.P., Ruthazer, R., et al. Missed Diagnoses of Acute Cardiac
Ischemia in the Emergency Department. New England Journal of Medicine 342 (2000): 1163-1170.
• 40. Espinosa, J.A., Nolan, T.W. Reducing Errors Made by Emergency Physicians in Interpreting Radiographs: Longitudinal Study. British Medical Journal 320 (2000): 737-740.
• 41. Hospital Statistics: 1979 Edition. Chicago: American Hospital Association, 1979.• 42. Knaus, W.A., Wagner, D.P., Draper, E.A., et al. The Range of Intensive Care Services Today.
Journal of the American Medical Association 246 (1981): 2711-2716.• 43. Wright, D. Critical Incident Reporting in an Intensive Care Unit. Report, Western General
Hospital, Edinburgh, Scotland, UK, 1999.• 44. Beckmann, V., Baldwin, I., Hart, G.K., et al. The Australian Incident Monitoring Study in
Intensive Care (AIMS-ICU): An Analysis of the First Year of Reporting. Anaesthesia and Intensive Care 24 (1996): 320-329.
• 45. Donchin, Y., Gopher, D., Olin, M., et al. A Look Into the Nature and Causes of Human Error in Intensive Care Unit. Critical Care Medicine 23 (1995): 294-300.
• 46. Crane, M. How Good Doctors Can Avoid Bad Errors. Medical Economics April (1997): 36-43.
04/18/23 ETM 591 - Reliability and QA 24

Conclusion
• Questions / Comments / Discussions
04/18/23 ETM 591 - Reliability and QA 25

















