29
Chapter 13 Disorders of the Pancreas Lecture 13 The Nature of Disease Pathology for the Health Professions Thomas H. McConnell
| Date post: | 01-Jan-2016 |
| Category: |
Documents |
| Upload: | osborne-jacobs |
| View: | 236 times |
| Download: | 0 times |

Chapter 13
Disorders of the Pancreas
Lecture 13
The Nature of DiseasePathology for the Health Professions
Thomas H. McConnell

Overview of Today’s Lecture
– Review of normal pancreatic anatomy & physiology
– Pancreatitis
– Diabetes mellitus
– Pancreatic neoplasms
Figure from: McConnell, The Nature of Disease, 2nd ed., LWW, 2014
Figure from: Huether & McCance, Understanding
Pathology, 5th ed., Elsevier, 2012
From: Pathophysiology: A Clinical Approach, Braun & Anderson, Lippincott, 2011

• The exocrine pancreas excretes digestive juice into the intestine.– Protease secreted as inactive enzyme (zymogen)
– Lipase and amylase secreted as active enzyme
• The endocrine pancreas excretes hormones into blood.– Alpha cells: glucagon. Functional opposite of insulin,
stimulates liver glycogen >> glucose. Raises blood glucose
– Beta cells: insulin. Opens cell membrane to glucose. Lowers blood glucose
– Delta cells: somatostatin. Inhibits glycogen formation and insulin secretion. Raises blood glucose
– PP cells: pancreatic polypeptide, acts on stomach to stimulate juices and slow intestinal motility
Normal Pancreatic Physiology

4
Pancreas
Exocrine (digestive) and endocrine (metabolic) functions
Completes digestion of proteins that was started in the stomach

5
Pancreatic Juice
• pancreatic amylase – splits glycogen into disaccharides
• pancreatic lipases – break down triglycerides
• pancreatic nucleases – digest nucleic acids
• bicarbonate ions – make pancreatic juice alkaline (pH = 8) and neutralize acid coming from stomach
• Pancreatic proteolytic enzymes…

6
Pancreatic Proteolytic Enzymes
Pancreas
ProelastaseProcarboxypeptidaseChymotrypsinogen
Trypsinogen Trypsin
Enteropeptidase (Enterokinase)
(brush border of sm. intestine)
ElastaseCarboxypeptidaseChymotrypsin
ProteinsDipeptides, tripeptides, amino acids
(Proenzymes, Zymogens)
Purpose of proteolytic enzymes is continued breakdown of proteins that began in the stomach
(Active enzymes)

7
Regulation of Pancreatic Secretions
• acidic chyme stimulates release of secretin
• secretin stimulates release of watery pancreatic juice with bicarbonate and phosphate (= buffers; to pH)
CCK and parasympathetic NS stimulate production and secretion of pancreatic enzymes and zymogens

Anatomic detail of the pancreas
Figure from: McConnell, The Nature of Disease, 2nd ed., LWW, 2014

Glucose, glycogen, insulin, and glucagon metabolism
Figure from: McConnell, The Nature of Disease, 2nd ed., LWW, 2014
The endocrine function of the pancreas

Pancreatitis
• Extremely serious disease
• Escape of pancreatic enzymes– Normally very small amount– Stasis increases likelihood that enzymes will cause
inflammation• Damage parenchyma of pancreas
• Damage to blood vessels, nerves
• Damage causes more pancreatic enzymes to be released
• Can be – Acute : Reversible inflammation of the pancreas– Chronic: Irreversible destruction and scarring

Acute Pancreatitis• Known associated conditions
– Alcohol abuse (67% of cases)
– Gallstones (50% of cases)
– Unknown etiology (10%)
– Other causes • Mnemonic phrase: Get Smashed – SG p171)
• Initial lesions• Edema, congestion, acute inflammation
• Congestion (stasis) causes autodigestion of pancreas
• May result in hemorrhagic pancreatitis (severe)
• Complication after resolution– Fibrous walling off of inflammation
– Cysts: pseudocysts (no epithelial lining; not true cyst)

Pathogenesis of Acute Pancreatitis
Figures from: McConnell, The Nature of Disease, 2nd ed., LWW, 2014
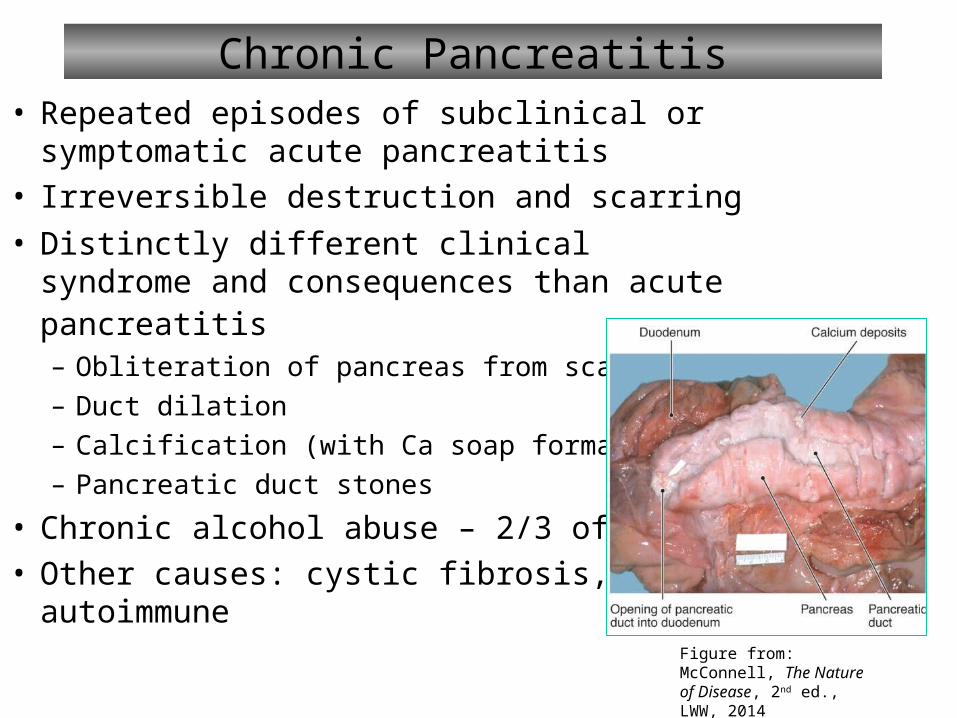
Chronic Pancreatitis• Repeated episodes of subclinical or
symptomatic acute pancreatitis• Irreversible destruction and scarring
• Distinctly different clinical syndrome and consequences than acute pancreatitis– Obliteration of pancreas from scar tissue
– Duct dilation
– Calcification (with Ca soap formation)
– Pancreatic duct stones
• Chronic alcohol abuse – 2/3 of cases• Other causes: cystic fibrosis,
autoimmune Figure from: McConnell, The Nature of Disease, 2nd ed., LWW, 2014

Chronic Pancreatitis
Figure from: McConnell, The Nature of Disease, 2nd ed., LWW, 2014

The Consequences of Pancreatitis
Figure from: McConnell, The Nature of Disease, 2nd ed., LWW, 2014

Diabetes Mellitus
• Disease causing hyperglycemia– Decreased insulin secretion (hyposecretion)– Decreased insulin action (resistance)
• Worldwide epidemic– 350 million people worldwide– 25 million in US alone– Over age 65, 27% are diabetic– Leading cause of morbidity and mortality
• Chronic renal failure
• Nontraumatic lower limb amputations
• Adult-onset blindness
• Major contributor to atherosclerosis

Criteria for Diagnosing Diabetes
Blood Glucose Level (mg/dl)
Euglycemia1 Pre-diabetes(glucose intolerant)
Diabetes
Fasting ≤ 100 100-125
≥ 126OR
3P’s + random ≥ 200
Peak (after OGTT)
≤ 140 140-100 ≥ 200
Hb A1c (%) < 6 5.7-6.4 ≥ 6.5
1 Normal fasting blood glucose range: 70 – 110 mg/dl

Type 1 Diabetes Mellitus• Genetic susceptibility and Environmental factors• Immunologically mediated destruction of beta cells
– Pancreatic atrophy and specific loss of beta cells; hyperglycemia when 80%-90% cells lost
– Macrophages, T- and B-lymphocytes, and natural killer cells are present
• Manifestations:– Hyperglycemia
– Polydipsia
– Polyuria
– Polyphagia
– Weight loss
– Fatigue
• Insulin, amylin, glucagon
Figure from: Huether & McCance,
Understanding Pathology, 5th ed., Elsevier,
2012

Dysfunction of the Pancreas
• Type 2 diabetes mellitus– Maturity-onset diabetes of youth (MODY)– Gestational diabetes mellitus (GDM)– Common form of diabetes mellitus type 2
• Initial insulin resistance
• Later loss of beta cells
• Diagnosis (fasting glucose, postprandial glucose, A1c)
• Manifestations (non-specific): fatigue, pruritus, recurrent infections, visual changes, or symptoms of neuropathy; often overweight, dyslipidemic, hyperinsulinemic, and hypertensive

Diabetes Types I/II Compared
Table from: McConnell, The Nature of Disease, 2nd ed., LWW, 2014

The Pathogenesis of Type I/II Diabetes
Figures from: McConnell, The Nature of Disease, 2nd ed., LWW, 2014

Acute Complications of Diabetes Mellitus
• Hypoglycemia• Diabetic ketoacidosis (Type I)• Hyperosmolar hyperglycemic non-ketotic syndrome
(HHNKS) (Type II)• Somogyi effect
– Hypoglycemia followed by rebound hyperglycemia
– Due to release of epinephrine, GH, corticosteroids
– Gluconeogenesis increases blood glucose
• Dawn phenomenon– Early morning rise in blood glucose
– Related to nocturnal release of GH

Chronic Complications of Diabetes Mellitus• Hyperglycemia and nonenzymatic glycosylation
– Normal reversible attachment of glucose becomes irreversible
– Blood vessel walls, interstitial tissue, cells
• Hyperglycemia and the polyol pathway– Insulin independent tissues (kidney, RBC, nerves, etc.)
• ↑ sorbitol, increasing osmotic pressure in cells
• Reduction in glutathione (antioxidant)
• Hyperglycemia and Protein kinase C (PKC) activation– Insulin resistance
– Proinflammatory cytokines
– Vascular endothelial proliferation
• Microvascular disease related to diabetes mellitus– Retinopathy
– Diabetic nephropathy
– Neuropathy
Mnemonic: SHAKE (see p. 173 in Study guide)

Metabolic Derangements/Complications in Diabetes
Figures from: McConnell, The Nature of Disease, 2nd ed., LWW, 2014

Diabetic Ketoacidosis
Figure from: Huether & McCance, Understanding Pathology, 5th ed., Elsevier, 2012

Treatment & Control of Diabetes Mellitus
• Three main levels of control– Diet and exercise
– Insulin replacement (Type I, Type II if needed)
– Oral hypoglycemic drugs
• Increase insulin secretion and/or production
• Decrease resistance to insulin
• Patient education is critically important• Food and the glycemic index
– Indicator of how fast a food is converted to glucose
– Glucose has an index of 100
– All other foods compared to this
• Hb A1c – useful confirmation of diagnosis

Glycemic Index and Glycemic Load
Glycemic index - compares the potential of foods containing the same amount of carbohydrate to raise blood glucose. However, the amount of carbohydrate consumed also affects blood glucose levels and insulin responses.
Glycemic Load - The glycemic load of a food is calculated by multiplying the glycemic index by the amount of carbohydrate in grams provided by a food and dividing the total by 100 (1). Dietary glycemic load is the sum of the glycemic loads for all foods consumed in the diet. The concept of glycemic load was developed by scientists to simultaneously describe the quality (glycemic index) and quantity of carbohydrate in a meal or diet.
From: http://lpi.oregonstate.edu/mic/food-beverages/glycemic-index-glycemic-load
From: http://nutritiondata.self.com/topics/glycemic-index

Pancreatic Neoplasms
• Pancreatic neoplasms can be– Cystic or Solid
– Benign or Malignant
– Endocrine or Exocrine
• Pancreatic carcinoma is common and lethal
• Cystic neoplasms are uncommon and usually benign
• Islet cell tumors are usually benign and functional
95% Exocrine duct adenocarcinoma

Pancreatic Carcinoma
Figures from: McConnell, The Nature of Disease, 2nd ed., LWW, 2014












![4679385 Blues [Mcconnell]](https://static.documents.pub/doc/80x56/577c7d2f1a28abe0549db5e8/4679385-blues-mcconnell.jpg)




