Note: This copy is for your personal, non-commercial use only. To order presentation-ready copies for distribution to your colleagues or clients, contact us at www.rsna.org/rsnarights. 342 radiology.rsna.org n Radiology: Volume 254: Number 2—February 2010 REVIEWS AND COMMENTARY n STATE OF THE ART 1 From the Department of Radiology, Mayo Clinic, 200 First St SW, Rochester, MN 55905 (D.L.B., K.M.D.); and Depart- ment of Radiology, Brigham and Women’s Hospital and Harvard Medical School, Boston, Mass (F.C.L.). Received March 30, 2009; revision requested May 6; revision received June 9; accepted June 11; final version accepted June 15. Address correspondence to D.L.B. (e-mail: [email protected]) Q RSNA, 2010 Pelvic ultrasonography (US) remains the imaging modality most frequently used to detect and characterize adnexal masses. Although evaluation is often aimed at distinguishing benign from malignant masses, the majority of adnexal masses are benign. About 90% of adnexal masses can be adequately characterized with US alone. In this article, the important US features that should allow one to make a reasonably confident diagnosis in most cases will be dis- cussed. The role of follow-up US and alternative imaging modalities, along with the importance of careful reporting of adnexal masses, will also be reviewed. Douglas L. Brown, MD Kika M. Dudiak, MD Faye C. Laing, MD Adnexal Masses: US Characterization and Reporting 1
Transcript
Note: This copy is for your personal, non-commercial use only. To order presentation-ready copies for distribution to your colleagues or clients, contact us at www.rsna.org/rsnarights.
342 radiology.rsna.org n Radiology: Volume 254: Number 2—February 2010
REVI
EWS
AND
COM
MEN
TARY
n S
TATE
OF
THE
ART
1 From the Department of Radiology, Mayo Clinic, 200 First St SW, Rochester, MN 55905 (D.L.B., K.M.D.); and Depart-ment of Radiology, Brigham and Women’s Hospital and Harvard Medical School, Boston, Mass (F.C.L.). Received March 30, 2009; revision requested May 6; revision received June 9; accepted June 11; fi nal version accepted June 15. Address correspondence to D.L.B. (e-mail: [email protected] )
Q RSNA, 2010
Pelvic ultrasonography (US) remains the imaging modality most frequently used to detect and characterize adnexal masses. Although evaluation is often aimed at distinguishing benign from malignant masses, the majority of adnexal masses are benign. About 90% of adnexal masses can be adequately characterized with US alone. In this article, the important US features that should allow one to make a reasonably confi dent diagnosis in most cases will be dis-cussed. The role of follow-up US and alternative imaging modalities, along with the importance of careful reporting of adnexal masses, will also be reviewed.
Douglas L. Brown , MD Kika M. Dudiak , MD Faye C. Laing , MD
Adnexal Masses: US Characterization and Reporting 1
STATE OF THE ART: US Characterization of Adnexal Masses Brown et al
Radiology: Volume 254: Number 2—February 2010 n radiology.rsna.org 343
U ltrasonography (US) continues to be the primary imaging modality used to identify and characterize
adnexal masses ( 1 , 2 ). The collective ex-perience from numerous centers world-wide has provided a wealth of informa-tion that allows accurate characterization of about 90% of adnexal masses on the basis of their US features ( 3 ). Adequate characterization of an adnexal mass is important both to determine which pa-tients need surgery and to help defi ne the type of surgery and whether a surgi-cal subspecialist is needed ( 4 ).
Various approaches to characteriz-ing adnexal masses have been used, including subjective assessment, simple scoring systems, statistically derived scoring systems or probability predic-tors based on logistic regression analy-sis, and more complex mathematical models such as neural networks ( 5 ). Of these, the subjective approach, also called a pattern recognition approach, has been shown to be superior to other methods, with a sensitivity of 88%–100% and specifi city of 62%–96% for predicting malignancy ( 6 – 8 ). The high accuracy of the subjective approach was obtained in specialized centers with experienced imagers. The quality of US scans may not be as consistent in less specialized centers ( 7 ), although the knowledge and skill set needed to re-produce this degree of performance should be attainable by anyone who routinely performs gynecologic US ( 8 ).
Essentials
With few specifi c exceptions, a n
solid component is the most pre-dictive US feature for malignancy in a cystic ovarian mass.
The most common adnexal n
masses are benign and can usu-ally be reliably recognized on the basis of their typical US features.
The assumption that an adnexal n
mass arises from the ovary may lead to diagnostic errors.
The manner in which adnexal n
masses are described and reported may enhance or impede patient care.
When determining the risk of ma-lignancy for an adnexal mass, consider-ation should also be given to factors other than imaging fi ndings. These in-clude patient age, menopausal status, personal or family history of breast or ovarian cancer, and serum CA-125 level. CA-125 levels are less valuable in premenopausal women since many be-nign diseases will cause it to increase, though usually only to a mild degree.
In this article, we will focus on US features that are most useful to predict malignancy and will emphasize how these features differ from those of be-nign disease. Although many physicians are understandably concerned about the failure to detect an ovarian malignancy, it is important to realize that the major-ity of adnexal masses, particularly in premenopausal women, are benign ( 3 , 9 – 12 ). We will review the distinguish-ing US features that can be used to con-fi dently identify the majority of common benign masses. With this knowledge, we can avoid creating unnecessary concern for the patient or the referring physician while remaining vigilant for adnexal malignancy. Extraovarian masses, along with the role of follow-up US and alter-native imaging modalities, will also be discussed. Finally, we will examine the role and method of US reporting, dis-cussing potential problems that may lead to miscommunication and adversely af-fect patient care. Concomitantly, we will suggest alternative approaches to better convey this information. We will limit our discussion to adults. Masses due to ectopic pregnancy and adnexal torsion are beyond the scope of our discussion.
US Technique
While transabdominal US is helpful for larger masses or those located superi-orly or laterally in the pelvis, transvagi-nal US provides optimal visualization of most adnexal diseases. Real-time US observations contribute to improved characterization ( 13 ) and suggest value in recording video clips. Two-dimensional US remains the mainstay for pelvic US, though three-dimensional US is being used with increasing frequency. Little formal comparison of the two tech-
Published online before print
10.1148/radiol.09090552
Radiology 2010; 254:342–354
Authors stated no fi nancial relationship to disclose.
niques is currently available, but three-dimensional US has not been shown to be superior to two-dimensional US in characterizing adnexal masses ( 14 ). Three-dimensional US may have some value in determining the origin of an adnexal mass, however ( 15 ). Doppler US is useful in cases with an apparent solid area or septum and will be dis-cussed subsequently. Contrast material–enhanced US remains an investigational technique ( 14 ).
Features of Malignant Ovarian Neoplasms
Classifi cation of ovarian neoplasms is based on histologic features and typically includes the general categories of epi-thelial, germ cell, sex cord-stromal, and metastatic neoplasms ( 16 ). About 90% of primary ovarian malignancies arise in the epithelial group ( 11 ). Borderline tu-mors, also known as tumors of low ma-lignant potential, are a subgroup of epi-thelial cancers and have a more favorable prognosis. Most germ cell and sex cord-stromal neoplasms are benign, with a few uncommon malignant varieties in these groups. In general, US features that indi-cate malignancy include a solid compo-nent (particularly if there is visible fl ow in it at Doppler evaluation), thick septa, and ascites ( 17 ).
Solid Component US demonstration of a solid component within a cystic mass ( Fig 1 ) is the most important predictor of malignancy, and conversely, malignancy is very unlikely in the absence of a solid component ( 4 , 8 , 17 , 18 ). Terminology to describe the solid component varies and also includes papillary projection, excres-cence, vegetation, and nodule. The dis-tinction between wall irregularity and small papillary projections along the wall can be diffi cult. It has been suggested that small solid areas that protrude
STATE OF THE ART: US Characterization of Adnexal Masses Brown et al
344 radiology.rsna.org n Radiology: Volume 254: Number 2—February 2010
3 mm or more from the cyst wall be considered as papillary projections ( 8 , 19 ).
Though a solid component within a cystic mass is generally a reliable indi-cator of neoplasia ( 4 , 18 ), pitfalls can occasionally lead to diagnostic prob-lems. Solid components can be seen with benign, as well as borderline and malignant neoplasms ( 3 , 20 ). Papillary projections are known to occur in some serous and mucinous cystadenomas and cystadenofi bromas ( 8 ). Solid-appearing components may also be present in dermoids and hemorrhagic cysts, both common benign lesions that will be dis-cussed in more detail subsequently. With a dermoid ( Fig 2 ), the solid area is typically hyperechoic compared with the cyst wall and often has acoustic shadowing ( 17 ). In contrast, the mural nodule of other neoplasms usually has echogenicity similar to that of the cyst wall ( 4 ). Clot in a hemorrhagic cyst may occasionally mimic a solid nodule of a neoplasm. Clot, however, often has concave borders ( Fig 3 ) due to clot re-traction, while a true mural nodule has outwardly convex borders ( 4 , 21 ). Color or power Doppler US can be helpful in this distinction, with absent fl ow char-acteristic for clot and defi nite visible fl ow typical for neoplasm ( 4 ). Wall irregu-larities due to a collapsing cyst ( Fig 4 ) can simulate small solid nodules that
Figure 2: Mature cystic teratoma in a 31-year-old woman. Transvaginal US scan shows a complex ovar-ian cyst (long arrows) with low-level internal echoes and a markedly hyperechoic solid-appearing area (short arrow) with faint distal acoustic shadowing (S).
Figure 2
Figure 1: Serous cystadenocarcinoma of the ovary in a 38-year-old woman. Transvaginal color Doppler US scan demonstrates a complex ovarian cyst with septum and a solid nodule (arrow). There is fl ow within the solid nodule, typical of malignancy.
Figure 1
may be misconstrued for malignancy ( 4 ). Awareness of this pitfall and follow-up US to confi rm resolution should eluci-date its benign etiology. Endometri-omas may contain a small solid area in 4%–20% of cases ( Fig 5 ), and these can simulate the mural nodule of malig-nant neoplasm ( 22 , 23 ). While this most likely is due to clot or endometrial tis-sue, Doppler US can sometimes depict fl ow when the solid area is endometrial tissue, and the reliability of Doppler US in this setting is unclear ( 24 , 25 ).
The completely solid adnexal mass is another potential problem. Most com-
monly, such a mass is due to a peduncu-lated uterine leiomyoma or an ovarian fi broma ( 26 ). The defi nition of a solid mass in some studies, however, allows for up to a 20% cystic component and such masses have been found to be as-sociated with malignancy ( 19 , 27 , 28 ). We suspect that malignancies in pre-dominately solid masses usually occur in those masses that still have some cystic component. The majority of epi-thelial ovarian malignancies have a cystic component and are rarely com-pletely solid ( 27 , 28 ). There are sporadic
Figure 3: Hemorrhagic cyst with a clot in a 40-year-old woman. Sagittal transvaginal color Doppler US scan shows a complex cystic mass within the periph-ery of the ovary. The seemingly solid area within the cystic mass has concave margins (arrows) and no demonstrable fl ow, both typical features of a clot.
Figure 3
Figure 4: Collapsing ovarian cyst in a 34-year-old woman. Sagittal transvaginal US scan shows the walls of the ovarian cyst, which are slightly irregular (arrows) due to collapse of the cyst as it involutes.
Figure 4
Figure 5: Endometrioma in a 46-year-old woman. Transverse transvaginal US scan reveals a complex ovarian cyst with homogeneous internal echoes. It contains a small solid-appearing area (arrow). Color Doppler US (not shown) did not demonstrate fl ow in the solid area.
Figure 5
STATE OF THE ART: US Characterization of Adnexal Masses Brown et al
Radiology: Volume 254: Number 2—February 2010 n radiology.rsna.org 345
exceptions, but the majority of com-pletely (ie, 100%) solid, solitary adnexal masses are benign in our experience, and other authors have a similar opin-ion ( 8 , 29 ). Ovarian malignancies that are most likely to manifest as solid or nearly completely solid masses include metastases, lymphoma, neoplasms of the sex cord-stromal group, and other rare malignancies such as malignant teratomas or dysgerminomas ( 11 , 30 ). In particular, when the patient has a malignancy with a propensity to metas-tasize to the ovaries, the presence of bilateral solid masses should raise con-cern for metastases ( 31 ). Breast and gastrointestinal tract carcinomas are the most common neoplasms to metas-tasize to the ovary. Given the above considerations, most truly solid adnexal masses that cannot be confi dently at-tributed to pedunculated uterine leio-myomas are removed surgically ( 29 ).
Septa Septa in a cystic ovarian mass ( Fig 6 ) are strong evidence of a neoplasm ( 4 ) and are more likely to indicate malig-nancy if they are greater than 2–3 mm in thickness or have detectable fl ow on Doppler US scans ( 17 ). A cystic ovarian mass with septa (particularly when thin) but without a solid component is likely to be a benign neoplasm, though
occasionally may be malignant when there are a very large number of septa ( 8 ). A cystic mass with multiple, smooth, thin septa and no nodularity is sugges-tive of a mucinous cystadenoma ( 8 ).
There are also a few pitfalls related to septa. Fibrin strands within a hem-orrhagic cyst should not be miscon-strued for true septa. Fibrin strands ( Fig 7 ) are typically very thin weak re-fl ectors, are numerous, and do not tra-verse the entire cyst ( 4 ). In contrast, true septa are usually thicker, less nu-merous, and extend in continuity course across the cyst ( 4 ). Another pitfall may occur when the juxtaposed walls be-tween two or more adjacent simple cysts ( Fig 8 ) mimic a septum ( 4 ). Follow-up US is often helpful to differentiate this from a septated cystic mass.
Ascites Ascites, an indirect indicator of malig-nancy, occurs with peritoneal tumor spread ( 17 ). Ascites may allow perito-neal implants to be seen. Although a small amount of fl uid in the cul-de-sac is normal in premenopausal women, an increased risk of malignancy has been reported if it measures more than 15 mm in anteroposterior dimension ( 28 ). The signifi cance of ascites should be in-terpreted in light of the patient’s pre-sentation and any preexisting illness,
such as cirrhosis. Meigs syndrome is the occurrence of ascites and pleural ef-fusion in association with a benign ovar-ian tumor, most frequently an ovarian fi broma. It is uncommon, however, oc-curring in about 1% of fi bromas ( 32 , 33 ). Ascites alone may also occur with fi bro-mas ( 33 ). The ascites in these cases has the potential to be mistaken for evi-dence of malignancy. Echogenic ascitic fl uid may occur with malignancy, but it may also occur with benign disease such as hemoperitoneum from a rup-tured cyst or ectopic pregnancy.
Other US Features Several other features of lesser clinical utility have been associated with malig-nancy. These include mass size, wall thickness, and Doppler US characteris-tics. Larger masses are often consid-ered more suspicious for malignancy; however, malignancy is more reliably predicted on the basis of morphologic features than size ( 31 ). A thickened cyst wall has been described as a fea-ture of malignancy, but its usefulness is limited since this feature can be seen in many benign lesions.
Spectral Doppler US does not yield any substantial improvement over gray-scale US for predicting malignancy ( 34 – 36 ). There is a general trend toward lower pulsatility index, lower resistive
Figure 6: Serous cystadenocarcinoma of the ovary in a 60-year-old woman. Transvaginal US scan shows a complex ovarian cyst (calipers) with several thick septa (arrows) and solid areas. Color Doppler US scan (not shown) revealed fl ow in the septa and solid areas.
Figure 6
Figure 7: Hemorrhagic cyst in a 30-year-old woman. Sagittal transvaginal US scan demonstrates a complex ovarian cyst with internal echoes. There is a reticular or fi shnet pattern to the internal echoes due to fi brin strands (arrows). Note how the fi brin strands are thin and do not extend completely across the cyst, in contrast to the true septa of a neoplasm in Figure 6.
Figure 7
Figure 8: Adjacent cysts simulating a septated cystic mass in a 38-year-old woman. Transvaginal US scan shows several adjacent ovarian cysts where the intervening ovarian stroma (arrows) simulates septa within a larger cystic mass. Color Doppler US scan (not shown) revealed fl ow within the interven-ing tissue. A 1-month follow-up US scan (not shown) showed complete resolution.
Figure 8
STATE OF THE ART: US Characterization of Adnexal Masses Brown et al
346 radiology.rsna.org n Radiology: Volume 254: Number 2—February 2010
index, and higher velocity in malignant neoplasms as opposed to benign neo-plasms. However, because of the substan-tial overlap of these spectral Doppler pa-rameters in benign and malignant lesions, they have little to no role in the charac-terization of adnexal masses ( 8 , 37 ).
Color Doppler US is best utilized in a qualitative mode to look for fl ow within a solid component or septum ( 38 ) ( Fig 1 ). If distinct vessels can be seen with color or power Doppler US, then fl ow is present. However, if only a few scattered pixels of color are displayed, it may be diffi cult to know if this is true fl ow or an artifact from noise. Spectral Doppler US should be performed in this instance to determine if blood fl ow is really present. The presence of fl ow increases concern for malignancy, though many benign neoplasms will also have detectable fl ow. If there is no detectable fl ow in a solid-appearing area, particu-larly in a premenopausal woman, one should consider the possibility of blood clot rather than a true solid component. Power Doppler US may be superior to conventional color Doppler US for iden-tifying malignancy, with slightly higher sensitivity but similar specifi city ( 14 ). Three-dimensional power Doppler US examinations, either for evaluating ves-sel morphology or obtaining new indexes that attempt to quantify fl ow, are still considered investigational ( 14 ).
Benign Ovarian Masses That Can Usually Be Predicted at US
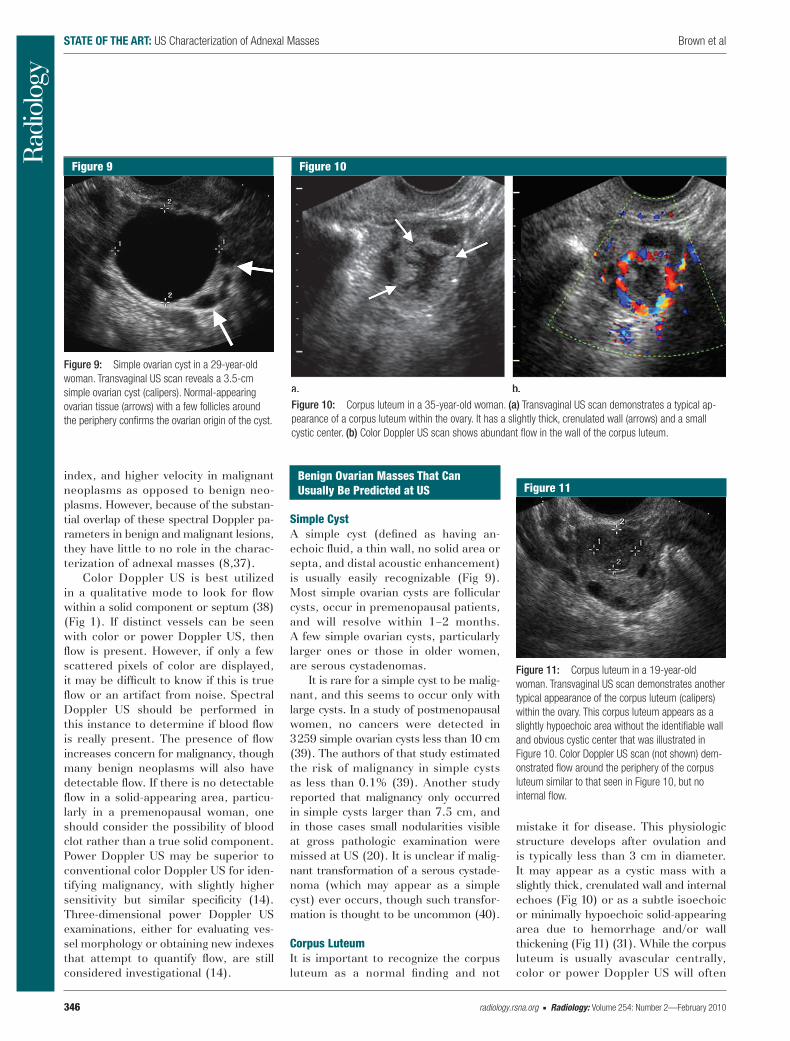
Simple Cyst A simple cyst (defi ned as having an-echoic fl uid, a thin wall, no solid area or septa, and distal acoustic enhancement) is usually easily recognizable ( Fig 9 ). Most simple ovarian cysts are follicular cysts, occur in premenopausal patients, and will resolve within 1–2 months. A few simple ovarian cysts, particularly larger ones or those in older women, are serous cystadenomas.
It is rare for a simple cyst to be malig-nant, and this seems to occur only with large cysts. In a study of postmenopausal women, no cancers were detected in 3 259 simple ovarian cysts less than 10 cm ( 39 ). The authors of that study estimated the risk of malignancy in simple cysts as less than 0.1% ( 39 ). Another study reported that malignancy only occurred in simple cysts larger than 7.5 cm, and in those cases small nodularities visible at gross pathologic examination were missed at US ( 20 ). It is unclear if malig-nant transformation of a serous cystade-noma (which may appear as a simple cyst) ever occurs, though such transfor-mation is thought to be uncommon ( 40 ).
Corpus Luteum It is important to recognize the corpus luteum as a normal fi nding and not
mistake it for disease. This physiologic structure develops after ovulation and is typically less than 3 cm in diameter. It may appear as a cystic mass with a slightly thick, crenulated wall and internal echoes ( Fig 10 ) or as a subtle isoechoic or minimally hypoechoic solid-appearing area due to hemorrhage and/or wall thickening ( Fig 11 ) ( 31 ). While the corpus luteum is usually avascular centrally, color or power Doppler US will often
Figure 9: Simple ovarian cyst in a 29-year-old woman. Transvaginal US scan reveals a 3.5-cm simple ovarian cyst (calipers). Normal-appearing ovarian tissue (arrows) with a few follicles around the periphery confi rms the ovarian origin of the cyst.
Figure 9
Figure 10: Corpus luteum in a 35-year-old woman. (a) Transvaginal US scan demonstrates a typical ap-pearance of a corpus luteum within the ovary. It has a slightly thick, crenulated wall (arrows) and a small cystic center. (b) Color Doppler US scan shows abundant fl ow in the wall of the corpus luteum.
Figure 10
Figure 11: Corpus luteum in a 19-year-old woman. Transvaginal US scan demonstrates another typical appearance of the corpus luteum (calipers) within the ovary. This corpus luteum appears as a slightly hypoechoic area without the identifi able wall and obvious cystic center that was illustrated in Figure 10. Color Doppler US scan (not shown) dem-onstrated fl ow around the periphery of the corpus luteum similar to that seen in Figure 10, but no internal fl ow.
Figure 11
STATE OF THE ART: US Characterization of Adnexal Masses Brown et al
Radiology: Volume 254: Number 2—February 2010 n radiology.rsna.org 347
depict hypervascularity around its periphery, sometimes referred to as a “ring of fi re” ( Fig 10 ). While the US fea-tures of the corpus luteum have been described ( 41 – 43 ) and are reasonable based on its physiology, the reliability of US features to distinguish a corpus luteum from other lesions has not been established. Given the common occur-rence of corpora lutea, however, when they have one of the typical features de-scribed above, we do not feel that US follow-up is needed. If one is uncer-tain whether the area in question is a corpus luteum, then follow-up US is reasonable.
Hemorrhagic Cyst Hemorrhagic ovarian cysts are likely caused by bleeding into a corpus luteum. The majority have typical US features that allow a confi dent diagnosis to be made ( 21 ). A reticular pattern of inter-nal echoes due to fi brin strands ( Fig 7 ) is a strong predictor of a hemorrhagic cyst. This pattern has also been referred to as having a fi shnet, lacy, cobweb, or spiderweb appearance. The distinction of true septa from fi brin strands was discussed earlier. While a clot may oc-casionally simulate a solid nodule, it is usually recognizable by its concave outer margin and/or absence of detectable fl ow at color or power Doppler US ( Fig 3 ). Follow-up US scans are useful if one is not confi dent. Blood clot can some-
times be recognized on a gray-scale US scan by its jellylike movement when pressure is applied with the transducer ( 8 ). A fl uid level occasionally occurs in a hemorrhagic cyst ( 44 ).
If imaged acutely, before fi brin strands or a retracting clot develops, a hemorrhagic cyst can be partly or com-pletely fi lled with heterogeneous echoes ( Fig 12 ) that may simulate a solid mass ( 31 , 44 ). One should consider this possibility in a younger woman with an ovarian mass that contains a seemingly solid heterogeneous component that lacks internal fl ow at Doppler US.
Endometrioma Endometriomas ( Fig 13 ) typically ap-pear as complex cysts, either unilocular or multilocular, that have a ground glass appearance due to diffuse, homoge-neous, low to medium level internal echoes ( 8 ). Similar diffuse internal echoes may sometimes occur in other lesions such as hemorrhagic cysts, dermoids, and some ovarian carcinomas ( 4 ). Thus, one should carefully evaluate for any other features such as a solid component that would suggest a differ-ent diagnosis. An endometrioma is very likely when there are diffuse internal echoes in a cystic mass lacking other US features ( 22 ). It is unclear whether lack of acoustic streaming (movement of fl uid due to energy transfer from the ultrasound wave) following insonation
with Doppler US is a predictive feature of endometriomas ( 45 ).
Additional features reported with endometriomas include echogenic foci in the wall and small solid areas along the wall, as discussed previously ( 22 , 25 ). Not surprisingly, the occasional small solid area may confound US interpretation, making it diffi cult to distinguish endo-metriomas from neoplasms. A small per-centage (probably , 15%) of endometri-omas have less typical US features such as anechoic fl uid, a fl uid-fl uid level, het-erogeneity, or calcifi cation ( 22 , 25 , 46 – 48 ). Endometriomas may occasionally simu-late a solid mass, especially when they are chronic ( 46 , 49 , 50 ). Rarely, endo-metroid or clear cell carcinoma may develop within an endometrioma; this is more likely in women older than 45 years of age and in endometriomas larger than 9 cm ( 51 ).
Mature Cystic Teratoma Mature cystic teratomas, often referred to as dermoids or dermoid cysts, are usu-ally easily recognized at US ( 8 ). A hyper-echoic area ( Fig 2 ) is a highly predictive feature of a dermoid, particularly when it is associated with distal acoustic shadow-ing ( 52 , 53 ). This hyperechoic area is not usually as intensely echogenic as
Figure 12: Subacute hemorrhagic cyst in a 37-year-old woman. Color Doppler transvaginal US scan shows a complex ovarian cyst with a seemingly solid area due to a clot (C). This could be mistaken for the solid area of a neoplasm. No fl ow was evident within the solid-appearing area and the cyst resolved at follow-up US 2 months later.
Figure 12
Figure 13: Endometrioma in a 36-year-old woman. Transvaginal US scan reveals a complex ovarian cyst (between arrows) with homogeneous internal echoes. As opposed to Figure 5, this is the more typical appearance of an endometrioma, with no solid nodule present.
Figure 13
Figure 14: Mature cystic teratoma in a 48-year-old woman. Transvaginal US scan demonstrates a complex cystic ovarian mass (calipers). A portion of the mass consists of fl uid with hyperechoic lines and dots (arrows) and has been termed dermoid mesh. The mass contains a hyperechoic solid-ap-pearing area (*), also typical of a teratoma.
Figure 14
STATE OF THE ART: US Characterization of Adnexal Masses Brown et al
348 radiology.rsna.org n Radiology: Volume 254: Number 2—February 2010
calcifi cation, but it is hyperechoic rela-tive to adjacent soft tissues. Hyperechoic lines and dots, sometimes called the der-moid mesh ( Fig 14 ), are also very pre-dictive ( 52 , 53 ). Less common but also chara cteristic are a fl uid-fl uid level with the more echogenic fl uid located in a nondependent position ( 54 ) and fl oating globules ( 55 ). The demonstration of any two or more of the above features in a mass is particularly predictive of a der-moid ( 53 ). Calcifi cation, often due to bone or a tooth, occurs in some der-moids, but cannot be used alone as de-fi nitive evidence of a dermoid since other neoplasms can also calcify. Rarely, a der-moid will have none of these characteris-tic US features ( 8 ).
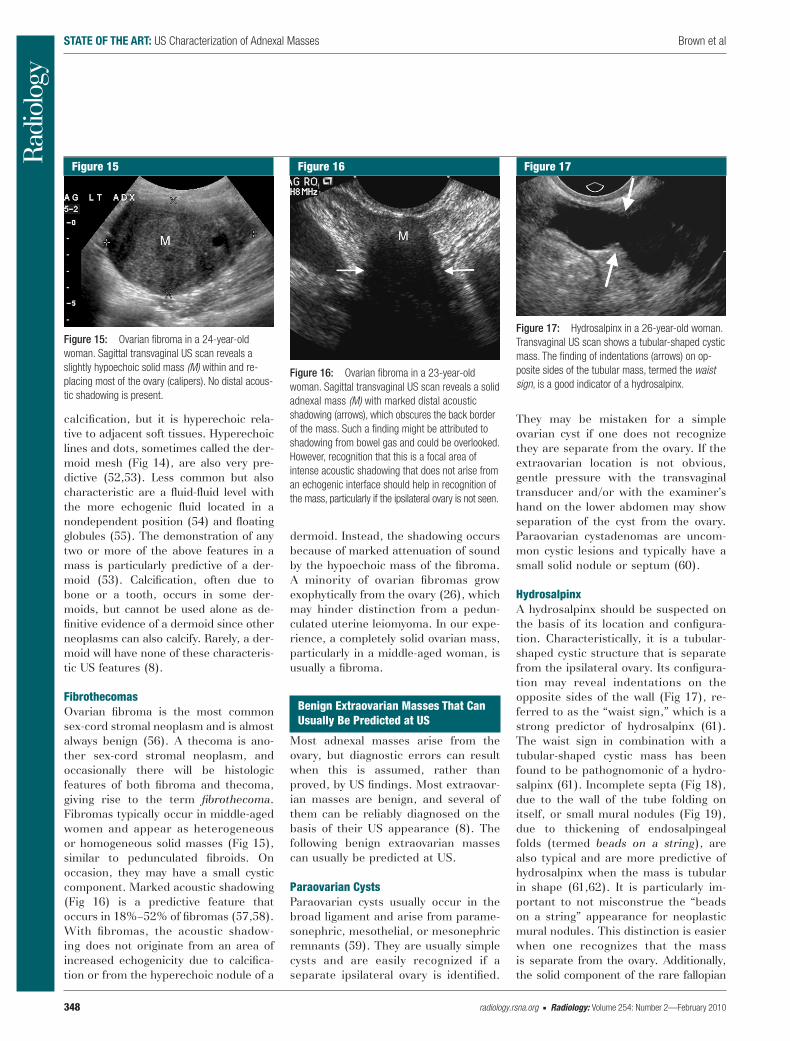
Fibrothecomas Ovarian fi broma is the most common sex-cord stromal neoplasm and is almost always benign ( 56 ). A thecoma is ano-ther sex-cord stromal neoplasm, and occasionally there will be histologic features of both fi broma and thecoma, giving rise to the term fi brothecoma . Fibromas typically occur in middle-aged women and appear as heterogeneous or homogeneous solid masses ( Fig 15 ), similar to pedunculated fi broids. On occasion, they may have a small cystic component. Marked acoustic shadowing ( Fig 16 ) is a predictive feature that occurs in 18%–52% of fi bromas ( 57 , 58 ). With fi bromas, the acoustic shadow-ing does not originate from an area of increased echogenicity due to calcifi ca-tion or from the hyperechoic nodule of a
dermoid. Instead, the shadowing occurs because of marked attenuation of sound by the hypoechoic mass of the fi broma. A minority of ovarian fi bromas grow exophytically from the ovary ( 26 ), which may hinder distinction from a pedun-culated uterine leiomyoma. In our expe-rience, a completely solid ovarian mass, particularly in a middle-aged woman, is usually a fi broma.
Benign Extraovarian Masses That Can Usually Be Predicted at US
Most adnexal masses arise from the ovary, but diagnostic errors can result when this is assumed, rather than proved, by US fi ndings. Most extraovar-ian masses are benign, and several of them can be reliably diagnosed on the basis of their US appearance ( 8 ). The following benign extraovarian masses can usually be predicted at US .
Paraovarian Cysts Paraovarian cysts usually occur in the broad ligament and arise from parame-sonephric, mesothelial, or mesonephric remnants ( 59 ). They are usually simple cysts and are easily recognized if a separate ipsilateral ovary is identifi ed.
They may be mistaken for a simple ovarian cyst if one does not recognize they are separate from the ovary. If the extraovarian location is not obvious, gentle pressure with the transvaginal transducer and/or with the examiner’s hand on the lower abdomen may show separation of the cyst from the ovary. Paraovarian cystadenomas are uncom-mon cystic lesions and typically have a small solid nodule or septum ( 60 ).
Hydrosalpinx A hydrosalpinx should be suspected on the basis of its location and confi gura-tion. Characteristically, it is a tubular-shaped cystic structure that is separate from the ipsilateral ovary. Its confi gura-tion may reveal indentations on the opposite sides of the wall ( Fig 17 ), re-ferred to as the “waist sign,” which is a strong predictor of hydrosalpinx ( 61 ). The waist sign in combination with a tubular-shaped cystic mass has been found to be pathognomonic of a hydro-salpinx ( 61 ). Incomplete septa ( Fig 18 ), due to the wall of the tube folding on itself, or small mural nodules ( Fig 19 ), due to thickening of endosalpingeal folds (termed beads on a string ), are also typical and are more predictive of hydrosalpinx when the mass is tubular in shape ( 61 , 62 ). It is particularly im-portant to not misconstrue the “beads on a string” appearance for neoplastic mural nodules. This distinction is easier when one recognizes that the mass is separate from the ovary. Additionally, the solid component of the rare fallopian
Figure 15: Ovarian fi broma in a 24-year-old woman. Sagittal transvaginal US scan reveals a slightly hypoechoic solid mass (M) within and re-placing most of the ovary (calipers). No distal acous-tic shadowing is present.
Figure 15
Figure 16: Ovarian fi broma in a 23-year-old woman. Sagittal transvaginal US scan reveals a solid adnexal mass (M) with marked distal acoustic shadowing (arrows), which obscures the back border of the mass. Such a fi nding might be attributed to shadowing from bowel gas and could be overlooked. However, recognition that this is a focal area of intense acoustic shadowing that does not arise from an echogenic interface should help in recognition of the mass, particularly if the ipsilateral ovary is not seen.
Figure 16
Figure 17: Hydrosalpinx in a 26-year-old woman. Transvaginal US scan shows a tubular-shaped cystic mass. The fi nding of indentations (arrows) on op-posite sides of the tubular mass, termed the waist sign , is a good indicator of a hydrosalpinx.
Figure 17
STATE OF THE ART: US Characterization of Adnexal Masses Brown et al
Radiology: Volume 254: Number 2—February 2010 n radiology.rsna.org 349
tube carcinoma is usually larger and less numerous than the multiple small nodules due to thickened endosalpin-geal folds.
Peritoneal Inclusion Cyst A peritoneal inclusion cyst is believed to occur in the presence of a functioning ovary and adhesions, with the latter usually due to prior pelvic surgery, en-dometriosis, or pelvic infl ammatory dis-ease. Peritoneal inclusion cysts ( Fig 20 ) typically appear as cystic masses with septa ( 63 , 64 ). The septa may be thick and contain detectable fl ow at color Doppler US. Peritoneal inclusion cysts
may be mistaken for ovarian neoplasms, but the key to their recognition is the demonstration of a normal ovary within or along the periphery of the cystic mass. Typically, the confi guration of a peritoneal inclusion cyst is passive and conform s to the contours of the adja-cent pelvic structures, but it may also have a spherical or ovoid shape ( 8 ).
Pedunculated Uterine Leiomyoma These are typically solid masses ( Fig 21 ) that may be mistaken for an ovarian fi broma if one does not identify a separate ipsilateral ovary. Color or power Dop-pler US demonstration of a vascular
pedicle connecting the mass to the uterus is good evidence of a peduncu-lated fi broid ( 65 , 66 ). Rarely, cystic de-generation can occur, leading to confu-sion with malignancy, particularly if the extraovarian location is not recognized.
Adnexal Masses That Are More Challenging to Predict at US
Less than 10% of adnexal masses are diffi cult to characterize at US ( 3 ). This may occur with a technically suboptimal examination, as a result of overlapping US features between some types of lesions, or with rare lesions.
Figure 18: Hydrosalpinx in a 46-year-old woman. Sagittal transvaginal US scan demonstrates a tubular-shaped cystic mass with several incomplete septa (arrows). Incomplete septa may occasionally be seen in other entities, but are typical of a hydros-alpinx when occurring in a tubular-shaped cystic mass. Real-time US is often helpful in demonstrating the tubular shape and showing how the walls of the folded fallopian tube appear as incomplete septa.
Figure 18
Figure 19: Hydrosalpinx in a 51-year-old woman. Transvaginal US scan shows a tubular-shaped cystic mass with a septum. Small nodules (arrows) in the mass are due to thickened endosalpingeal folds.
Figure 19
Figure 20: Peritoneal inclusion cyst in a 29-year-old woman. (a) Transverse transabdominal US scan shows a complex left adnexal cyst (arrows) with septa. A portion of the cyst conforms to the contour of the uterus (U) . (b) Transvaginal US scan reveals a normal ovary (arrows) at the periphery of the cyst.
Figure 20
Figure 21: Pedunculated uterine leiomyoma in a 43-year-old woman. (a) Coronal transvaginal US scan demonstrates a solid adnexal mass (M) adjacent to the left side of the uterus (U) . (b) Color Doppler US scan in the same plane shows connecting vessels (arrows) between the uterus and mass, helping to confi rm a pedunculated leiomyoma.
Figure 21
STATE OF THE ART: US Characterization of Adnexal Masses Brown et al
350 radiology.rsna.org n Radiology: Volume 254: Number 2—February 2010
Tubo-ovarian Abscess Because tubo-ovarian abscesses have various US appearances, they can be diffi cult to diagnose reliably on the ba-sis of US morphology ( 8 , 67 , 68 ). They can be unilocular or multilocular, vary with respect to their internal echoge-nicity, and may have solid-appearing areas ( 67 , 68 ). Patient history and clini-cal fi ndings consistent with pelvic in-fl ammatory disease are usually neces-sary to diagnose a tubo-ovarian abscess. If a component of the mass suggests a pyosalpinx (ie, echogenic fl uid within a hydrosalpinx) then a tubo-ovarian ab-scess should be considered, but this ap-pearance is uncommon ( 68 ). Cervical motion tenderness caused by the trans-vaginal transducer and pain when scan-ning directly over a dilated fallopian tube may increase confi dence in the diagnosis.
Uncommon Ovarian Neoplasms By virtue of their rarity, some ovarian neoplasms are diffi cult to diagnose at US or any other imaging modality. Sex cord-stromal tumors other than benign fi brothecomas are often low-grade ma-lignancies and fall into this category. Some can be suggested if accompanied by endocrine dysfunction. Granulosa cell tumors, which tend to be solid or multiloculated with solid components, may produce estrogen and cause endo-metrial disease ( 69 ). Sertoli-Leydig cell
tumors may produce androgens and cause virilization ( 70 ). These latter tu-mors can be subtle on US scans, as many are small solid tumors.
Within the germ cell group, variants of ovarian teratoma can be challenging to diagnose. Struma ovarii, a teratoma composed mostly of thyroid tissue, does not usually have the typical features of a teratoma at US or MR imaging and is only rarely associated with thyrotoxico-sis ( 3 , 71 ). These are rare and tend to develop in older women whose masses are larger than 6 cm ( 72 ). In contrast to their benign counterpart, malignant teratomas have more solid components with exophytic extension. Isoechoic branching structures within the mass have been suggested as a sign of malig-nancy ( 73 ). Because of their rarity, use of these features to diagnose a malig-nant teratoma is diffi cult to apply in daily practice. Other rare germ cell neo-plasms include dysgerminomas (which typically are solid masses occurring most frequently in adolescence and young adults), endodermal sinus tu-mors, choriocarcinomas, and embryonal carcinoma ( 74 ).
Uncommon Extraovarian Masses Several extraovarian masses occur too infrequently to discuss in detail. Tarlov cysts (also known as perineural cysts) should be considered when complex cystic masses with internal echoes are seen posteriorly, separate from the ovaries ( 75 ). An appendiceal mucocele typically appears as a complex cystic mass with internal echoes in the right lower abdomen or pelvis. Solid extrao-varian masses include neural tumors, lymphadenopathy, and the rudimentary horn of a unicornuate uterus. The post-operative nature of some cystic masses may suggest their diagnosis, such as he-matomas, lymphoceles, or seromas.
Fallopian tube carcinoma, a rare tu-mor, is considered within the spectrum of malignancies associated with BRCA1 and BRCA2 mutations ( 76 ). They are often diagnosed at surgery, having orig-inally been suspected to be an ovarian malignancy ( 76 ). A tubular-shaped mass with a large solid component sug-gests the diagnosis ( 77 , 78 ). This ap-
pearance should be contrasted with the multiple tiny nodules causing a “beads on a string” appearance that may occur with a hydrosalpinx. The appearance of fallopian tube carcinoma is variable, how-ever, and unfortunately it may appear as a completely solid mass, lacking US evidence of a tubular component ( 78 ).
Adnexal Masses in Pregnancy
A thorough discussion of adnexal masses in pregnancy is beyond the scope of this article, but the US approach and criteria are essentially the same as those used in a nonpregnant premenopausal woman ( 9 ). A more detailed discussion of adnexal masses in pregnancy is avail-able elsewhere ( 79 ).
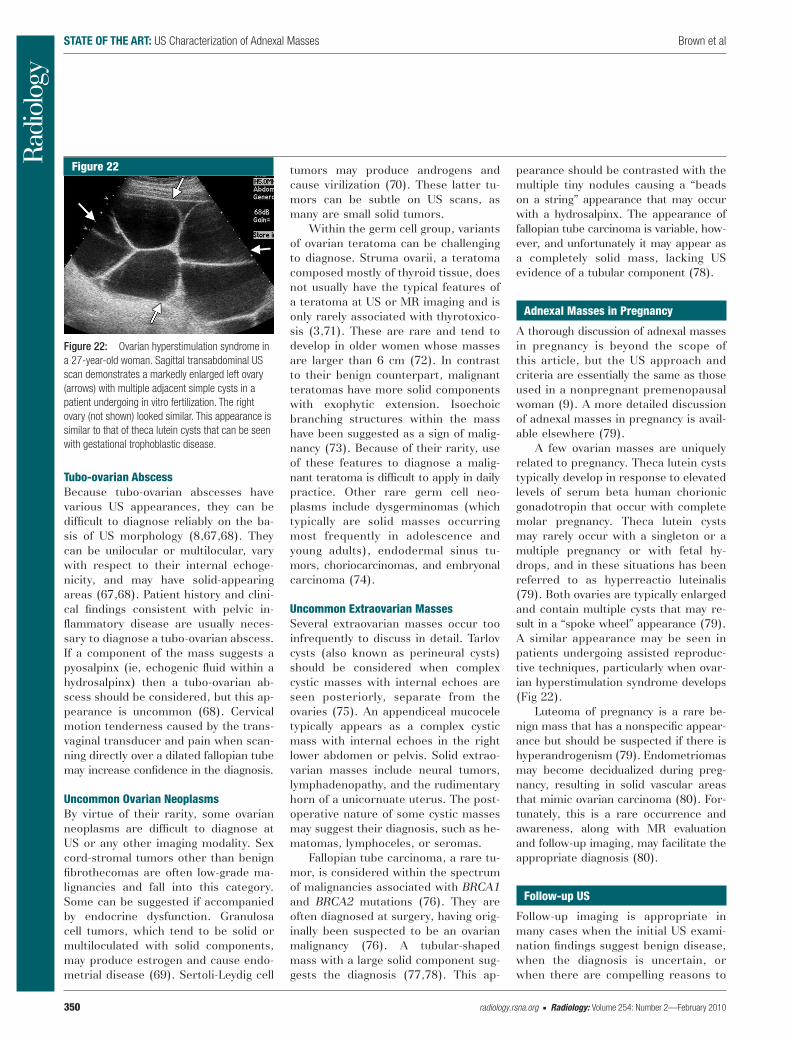
A few ovarian masses are uniquely related to pregnancy. Theca lutein cysts typically develop in response to elevated levels of serum beta human chorionic gonadotropin that occur with complete molar pregnancy. Theca lutein cysts may rarely occur with a singleton or a multiple pregnancy or with fetal hy-drops, and in these situations has been referred to as hyperreactio luteinalis ( 79 ). Both ovaries are typically enlarged and contain multiple cysts that may re-sult in a “spoke wheel” appearance ( 79 ). A similar appearance may be seen in patients undergoing assisted reproduc-tive techniques, particularly when ovar-ian hyperstimulation syndrome develops ( Fig 22 ).
Luteoma of pregnancy is a rare be-nign mass that has a nonspecifi c appear-ance but should be suspected if there is hyperandrogenism ( 79 ). Endometriomas may become decidualized during preg-nancy, resulting in solid vascular areas that mimic ovarian carcinoma ( 80 ). For-tunately, this is a rare occurrence and awareness, along with MR evaluation and follow-up imaging, may facilitate the appropriate diagnosis ( 80 ).
Follow-up US
Follow-up imaging is appropriate in many cases when the initial US exami-nation fi ndings suggest benign disease, when the diagnosis is uncertain, or when there are compelling reasons to
Figure 22: Ovarian hyperstimulation syndrome in a 27-year-old woman. Sagittal transabdominal US scan demonstrates a markedly enlarged left ovary (arrows) with multiple adjacent simple cysts in a patient undergoing in vitro fertilization. The right ovary (not shown) looked similar. This appearance is similar to that of theca lutein cysts that can be seen with gestational trophoblastic disease.
Figure 22
STATE OF THE ART: US Characterization of Adnexal Masses Brown et al
Radiology: Volume 254: Number 2—February 2010 n radiology.rsna.org 351
avoid surgery ( 9 ). In premenopausal women, many masses are functional cysts that will spontaneously resolve in several weeks. This often prompts a follow-up US about 6 weeks after the initial examination. Some of these studies may be unnecessary, although there is no consensus regarding which cysts do not need US follow-up. In an asymptomatic premenopausal woman, it has been suggested that a simple ovarian cyst smaller than about 4 cm may not need follow-up ( 4 , 81 ). Simi-larly, a classic-appearing hemorrhagic cyst probably does not need to be fol-lowed if the patient is, or becomes, asymptomatic ( 4 ).
Postmenopausal women with a sim-ple ovarian cyst less than 1 cm may be able to forego follow-up US ( 4 ). Post-menopausal women with a simple ovar-ian cyst greater than 1 cm, but less than 5 cm, can usually be followed with US ( 82 – 84 ), although optimum follow-up interval is uncertain. With short-interval follow-up, slow growth can occur with a benign neoplasm such as a serous cysta-denoma and may not be appreciated ( 4 ). Performance of US in about 6 months seems reasonable for the initial follow-up US examination ( 4 ), with fur-ther follow-up intervals adjusted on the basis of the degree of change. The Society of Radiologists in Ultrasound is sponsoring a consensus conference on the management of adnexal cysts that will address the issue of follow-up US for many adnexal cysts.
If the etiology of a mass is uncer-tain, but its appearance is not suspi-cious for malignancy, then follow-up US is also reasonable. For example, if a mass is likely a hemorrhagic cyst but also has atypical features, a follow-up US examination performed in 6 weeks is reasonable. This amount of time al-lows for resolution of most cysts and is at a different time of the menstrual cy-cle so that any new cyst will hopefully have a different appearance. Serial US examination may also be indicated to follow the course of a previously char-acterized benign lesion. This is com-monly performed in a patient with a dermoid, endometrioma, hydrosalpinx, or a peritoneal inclusion cyst. While
some persistent benign-appearing adn-exal masses may be removed due to potential torsion or rupture, recent evidence suggests that these complica-tions are less frequent than previously reported ( 4 , 85 ).
Alternative Imaging Modalities
To further evaluate an adnexal mass, additional imaging studies may be rec-ommended. Since MR imaging per-forms well for characterizing adnexal masses ( 86 , 87 ), it is the modality most frequently used to further evaluate adn-exal masses deemed indeterminate at US ( 10 , 88 ). The problem with this ap-proach is a lack of what defi nes a mass as indeterminate at US. Fortunately, when one applies the previously de-scribed US criteria to characterize adnexal masses, the number of truly US- indeterminate examination fi ndings is small. Furthermore, once a thorough US examination has been performed, additional imaging with other modali-ties is often of limited value ( 9 ). MR imaging is most benefi cial when a mass is very large, is located superiorly or laterally in the pelvis, has atypical US features, or is of unclear origin ( 4 , 9 , 89 , 90 ).
CT may be able to characterize adnexal masses as benign or malignant ( 91 ), but it has little role in the routine detection or characterization of adnexal masses. CT cannot usually be as spe-cifi c as to the type of benign mass in the manner that US can. Given the numer-ous advantages inherent to US, includ-ing wide availability, large collective ex-perience with this modality, lower cost, and lack of ionizing radiation, CT should generally be reserved to evaluate for spread of ovarian malignancy ( 9 ). While CT can demonstrate fat in dermoids, if there is no macroscopic fat in the mass, CT usually contributes little further in-formation for characterization. We pre-fer MR in this context if the diagnosis is unclear at US, since it cannot only dem-onstrate fat, but has the capacity to identify blood products within an endo-metrioma or hemorrhagic cyst, masses that are occasionally confused for a dermoid at US ( 53 ). CT may have utility
in selected cases of suspected tubo-ovarian abscess, since it is superior to US for revealing contiguous infl amma-tory changes and involvement of adja-cent organs ( 67 ).
Positron emission tomography (PET) may provide some information as to the etiology of a mass ( 92 , 93 ); however, current data do not support the use of PET scanning in the preoperative char-acterization of adnexal masses ( 9 ). PET or PET/CT scans may be useful in se-lected cases where recurrent cancer is suspected.
Reporting of the US Examination
The importance of communicating US fi ndings in a clearly worded, succinct report cannot be overstated. Reports that provide a clear description of the fi ndings and a most likely diagnosis, or a short list of most likely diagnoses, contribute to proper care of the patient. Inappropriate reporting may lead to un-warranted concern by the patient and referring clinician and could lead to un-necessary additional tests or surgery. This issue has been well discussed ( 94 ), and it is important that radiologists re-main aware of these problems and take responsibility for solving them. In our opinion, problems that relate to report-ing involve four areas that we will dis-cuss below. A reporting method similar to the Breast Imaging Reporting and Data System classifi cation used for breast masses has been suggested for adnexal masses ( 95 ) and could poten-tially improve communication of US re-sults, but there is no agreement yet on such an approach.
Use of the Term Cyst In any organ other than the ovary, an identifi able cyst indicates an abnormality, albeit usually benign. The premeno-pausal ovary is unique, however, in that small simple cysts, that is, follicles, are part of its normal structure. Thus, use of the term cyst with respect to the ovary has the potential to be misunder-stood, since “cyst” tends to connote disease ( 94 ). Of the several small folli-cles normally present, the dominant fol-licle will generally enlarge to a diameter
STATE OF THE ART: US Characterization of Adnexal Masses Brown et al
352 radiology.rsna.org n Radiology: Volume 254: Number 2—February 2010
of 20–25 mm before ovulation occurs. Therefore, a simple cyst less than about 25 mm is usually a normal follicle in a premenopausal woman, particularly when visible at mid cycle. Thus, it seems more precise and less likely to be mis-understood if one refrains from using the term cyst in any form to describe normal follicles, but rather just states that the ovary is “normal” or refers to them as “follicles” ( 4 , 94 ). Even reports of “multiple follicles” or “several small follicles” can be misinterpreted if the referring physician wonders about in-creased numbers of follicles in regard to polycystic ovary syndrome. Report-ing the ovary as “normal” seems to be the clearest wording.
Similarly, when there are typical features of a corpus luteum, also a nor-mal part of the ovary, the ovary should be reported either as “normal” or as containing a “corpus luteum.” The term corpus luteum cyst to describe this small normal fi nding should usually be avoided, since the word “cyst” typically implies disease ( 94 ). Occasionally, the corpus luteum may enlarge more than is typical and at some point addition of the word “cyst” or use of a term such as hemorrhagic corpus luteum cyst may be suitable ( 94 ), although the size where this is distinction is most appropriate is unclear.
Incomplete or Vague Description of the Mass The description of an adnexal mass will also be problematic if the report only states the presence of a “complex cystic adnexal mass.” Since many benign and most malignant masses are complex, additional descriptive adjectives and synthesis to include a likely diagnosis are necessary to avoid an incomplete and vague report that could be misun-derstood by the referring clinician. We do not object to the word “complex” as long as further descriptors are provided regarding the features that produce the complex appearance. We realize that approaches to reporting vary, with radi-ologists and other imagers being more or less detailed in their description, as is the norm in their practice. Nevertheless, with rare exception, there should at least be
an assessment of the fi ndings that re-sults in a conclusion regarding the most likely diagnosis or a short list of the most likely diagnoses. Patients some-times seek a second opinion in another locale, and accurate description and syn-thesis are even more important in this situation.
Frequent Suggestion of Malignancy as a Diagnosis Reports that frequently state ovarian cancer cannot be excluded or those that frequently include ovarian cancer in the differential diagnosis may also contrib-ute to improper patient care. Before the US examination is performed, the referring clinician is well aware of the long differential diagnosis of an adnexal mass, which includes ovarian cancer ( 94 ). Since most adnexal masses are benign and have defi ning characteristic features that can be identifi ed on the US scan, the role of US is to substantially narrow the list of diagnostic possibili-ties. Certainly, consideration of ovarian cancer is appropriate in some cases, but when all adnexal masses are taken into account, ovarian malignancy is relatively uncommon and should only be reported when neoplastic features are visible.
Frequent Recommendation of Alternative Imaging Modalities Alternative imaging may be appropriate in a small number of cases, as discussed previously. However, if the radiologist frequently recommends additional imag-ing studies, it is unlikely that all of the information from the US examination is being considered. Furthermore, when follow-up imaging is needed, a repeat US examination often suffi ces. Frequent recommendation of other diagnostic im-aging modalities contributes to unneces-sary imaging and additional costs and may place the referring clinician in a dif-fi cult situation if he or she does not con-cur that further imaging is warranted.
Summary
The overwhelming majority of adnexal masses are benign and most can be rec-ognized on the basis of characteristic US features. Malignancy, while infre-
quent, is likewise usually identifi able by a different set of distinguishing US features. Accordingly, in most cases the report should refl ect a reasonably confi -dent diagnosis of a benign or malignant entity. Clear communication of the US results will assist in proper patient care and should include a suffi cient descrip-tion and/or conclusion regarding the most likely diagnosis. In less defi nitive cases, unambiguous reporting will still aid in appropriate patient care. Follow-ing this approach will maximize the po-tential of US to correctly characterize a mass and should allow the majority of women to either have no follow-up at all or undergo a follow-up US when appro-priate. It should also assist in determin-ing the minority of women who need alternative imaging or surgery and help reduce unnecessary imaging and un-warranted clinical concern.
References 1 . American College of Radiology . ACR Appro-
priateness Criteria 2008: clinically suspected adnexal mass . American College of Radiology Web site. Available at http :// www . acr . org / SecondaryMainMenuCategories/quality_safety/app_criteria/pdf/ExpertPanelonWomensImaging/SuspectedAdnexalMasses-Doc11.aspx . Accessed November 9, 2009 .
2 . Liu J , Xu Y , Wang J . Ultrasonography, com-puted tomography and magnetic resonance imaging for diagnosis of ovarian carcinoma . Eur J Radiol 2007 ; 62 : 328 – 334 .
3 . Valentin L , Ameye L , Jurkovic D , et al . Which extrauterine pelvic masses are diffi -cult to correctly classify as benign or malig-nant on the basis of ultrasound fi ndings and is there a way of making a correct diagnosis? Ultrasound Obstet Gynecol 2006 ; 27 : 438 – 444 .
4 . Patel MD . Practical approach to the adnexal mass . Radiol Clin North Am 2006 ; 44 : 879 – 899 .
5 . Geomini P , Kruitwagen R , Bremer GL , Cnossen J , Mol BW . The accuracy of risk scores in predicting ovarian malignancy: a systematic review . Obstet Gynecol 2009 ; 113 : 384 – 394 .
6 . Timmerman D , Schwarzler P , Collins WP , et al . Subjective assessment of adnexal masses with the use of ultrasonography: an analysis of interobserver variability and experience . Ultrasound Obstet Gynecol 1999 ; 13 : 11 – 16 .
7 . Van Calster B , Timmerman D , Bourne T , et al . Discrimination between benign and malignant adnexal masses by specialist ultra-sound examination versus serum CA-125 . J Natl Cancer Inst 2007 ; 99 : 1706 – 1714 .
STATE OF THE ART: US Characterization of Adnexal Masses Brown et al
Radiology: Volume 254: Number 2—February 2010 n radiology.rsna.org 353
8 . Valentin L . Use of morphology to character-ize and manage common adnexal masses . Best Pract Res Clin Obstet Gynaecol 2004 ; 18 : 71 – 89 .
9 . American College of Obstetricians and Gynecologists . ACOG Practice Bulletin. Man-agement of adnexal masses . Obstet Gynecol 2007 ; 110 : 201 – 214 .
10 . Kinkel K , Lu Y , Mehdizade A , Pelte MF , Hricak H . Indeterminate ovarian mass at US: incremental value of second imaging test for characterization–meta-analysis and Bayesian analysis . Radiology 2005 ; 236 : 85 – 94 .
11 . Koonings PP , Campbell K , Mishell DR , Grimes DA . Relative frequency of primary ovarian neoplasms: a 10-year review . Obstet Gynecol 1989 ; 74 : 921 – 926 .
12 . Moszynski R , Szpurek D , Smolen A , Sajdak S . Comparison of diagnostic usefulness of predictive models in preliminary differentia-tion of adnexal masses . Int J Gynecol Cancer 2006 ; 16 : 45 – 51 .
13 . Van Holsbeke C , Yazbek J , Holland TK , et al . Real-time ultrasound vs evaluation of static images in the preoperative assessment of adnexal masses . Ultrasound Obstet Gynecol 2008 ; 32 : 828 – 831 .
14 . Alcazar JL . New ultrasound-based technologies for predicting ovarian cancer in adnexal masses . Curr Womens Health Rev 2007 ; 3 : 89 – 94 .
15 . Benacerraf BR , Benson CB , Abuhamad AZ , et al . Three- and 4-dimensional ultrasound in obstetrics and gynecology: proceedings of the American Institute of Ultrasound in Medicine Consensus Conference . J Ultrasound Med 2005 ; 24 : 1587 – 1597 .
16 . Scully RE . Classifi cation of human ovarian tu-mors . Environ Health Perspect 1987 ; 73 : 15 – 24 .
17 . Brown DL , Doubilet PM , Miller FH , et al . Benign and malignant ovarian masses: selec-tion of the most discriminating gray-scale and Doppler sonographic features . Radiology 1998 ; 208 : 103 – 110 .
18 . Granberg S , Wikland M , Jansson I . Macro-scopic characterization of ovarian tumors and the relation to the histological diagnosis: criteria to be used for ultrasound evaluation . Gynecol Oncol 1989 ; 35 : 139 – 144 .
19 . Timmerman D , Valentin L , Bourne TH , Collins WP , Verrelst H , Vergote I . Terms, defi nitions and measurements to describe the sonographic features of adnexal tumors: a consensus opinion from the International Ovarian Tumor Analysis (IOTA) Group . Ul-trasound Obstet Gynecol 2000 ; 16 : 500 – 505 .
20 . Ekerhovd E , Wienerroith H , Staudach A , Granberg S . Preoperative assessment of uni-locular adnexal cysts by transvaginal ultrasonog-raphy: a comparison between ultrasonographic morphologic imaging and histopathologic diagnosis . Am J Obstet Gynecol 2001 ; 184 : 48 – 54 .
21 . Patel MD , Feldstein VA , Filly RA . The likeli-hood ratio of sonographic fi ndings for the
diagnosis of hemorrhagic ovarian cysts . J Ul-trasound Med 2005 ; 24 : 607 – 614, quiz 615 .
22 . Patel MD , Feldstein VA , Chen DC , Lipson SD , Filly RA . Endometriomas: diagnostic performance of ultrasound . Radiology 1999 ; 210 : 739 – 745 .
23 . Alcazar JL , Laparte C , Jurado M , Lopez-Garcia G . The role of transvaginal ultrasonog-raphy combined with color velocity imaging and pulsed Doppler in the diagnosis of endo-metrioma . Fertil Steril 1997 ; 67 : 487 – 491 .
24 . Guerriero S , Ajossa S , Mais V , Risalvato A , Lai MP , Melis GB . The diagnosis of endo-metriomas using colour Doppler energy im-aging . Hum Reprod 1998 ; 13 : 1691 – 1695 .
25 . Asch E , Levine D . Variations in appearance of endometriomas . J Ultrasound Med 2007 ; 26 : 993 – 1002 .
26 . Oh SN , Rha SE , Byun JY , et al . MRI features of ovarian fi bromas: emphasis on their re-lationship to the ovary . Clin Radiol 2008 ; 63 : 529 – 535 .
27 . Granberg S , Norstrom A , Wikland M . Tu-mors in the lower pelvis as imaged by vaginal sonography . Gynecol Oncol 1990 ; 37 : 224 – 229 .
28 . Timmerman D , Testa AC , Bourne T , et al . Simple ultrasound-based rules for the diag-nosis of ovarian cancer . Ultrasound Obstet Gynecol 2008 ; 31 : 681 – 690 .
29 . Barney SP , Muller CY , Bradshaw KD . Pelvic masses . Med Clin North Am 2008 ; 92 : 1143 – 1161, xi .
30 . Valentin L , Ameye L , Testa A , et al . Ultra-sound characteristics of different types of adnexal malignancies . Gynecol Oncol 2006 ; 102 : 41 – 48 .
31 . Brown DL . A practical approach to the ultra-sound characterization of adnexal masses . Ultrasound Q 2007 ; 23 : 87 – 105 .
32 . Chechia A , Attia L , Temime RB , Makhlouf T , Koubaa A . Incidence, clinical analysis, and management of ovarian fi bromas and fi broth-ecomas . Am J Obstet Gynecol 2008 ; 199 : 473.e1 – 473.e4 .
33 . Vijayaraghavan GR , Levine D . Case 109: Meigs syndrome . Radiology 2007 ; 242 : 940 – 944 .
34 . Stein SM , Laifer-Narin S , Johnson MB , et al . Differentiation of benign and malignant adn-exal masses: relative value of gray-scale, color Doppler, and spectral Doppler sonography . AJR Am J Roentgenol 1995 ; 164 : 381 – 386 .
35 . Buy JN , Ghossain MA , Hugol D , et al . Char-acterization of adnexal masses: combination of color Doppler and conventional sonogra-phy compared with spectral Doppler analysis alone and conventional sonography alone . AJR Am J Roentgenol 1996 ; 166 : 385 – 393 .
36 . Valentin L . Prospective cross-validation of Doppler ultrasound examination and gray-scale ultrasound imaging for discrimination of benign and malignant pelvic masses . Ultrasound Obstet Gynecol 1999 ; 14 : 273 – 283 .
37 . Kurtz AB , Tsimikas JV , Tempany CMC , et al . Diagnosis and staging of ovarian cancer: comparative values of Doppler and conven-tional US, CT, and MR imaging correlated with surgery and histopathologic analysis-report of the radiology diagnostic oncology group . Radiology 1999 ; 212 : 19 – 27 .
38 . Kinkel K , Hricak H , Lu Y , Tsuda K , Filly R . US charaterization of ovarian masses: a meta-analysis . Radiology 2000 ; 217 : 803 – 811 .
39 . Modesitt SC , Pavlik EJ , Ueland FR , DePriest PD , Kryscio RJ , van Nagell JR . Risk of malig-nancy in unilocular ovarian cystic tumors less than 10 centimeters in diameter . Obstet Gy-necol 2003 ; 102 : 594 – 599 .
40 . Cass I , Karlan BY . Ovarian and tubal can-cers . In: Gibbs RS , Karlan BY , Haney AF , Nygaard IE , eds. Danforth’s obstetrics and gynecology . 10th ed. Philadelphia, Pa : Wolt-ers Kluwer/Lippincott Williams & Wilkins , 2008 ; 1022 – 1060 .
41 . Baerwald AR , Adams GP , Pierson RA . Form and function of the corpus luteum during the human menstrual cycle . Ultrasound Obstet Gynecol 2005 ; 25 : 498 – 507 .
42 . Bourne TH , Hagstrom H , Hahlin M , et al . Ultrasound studies of vascular and morpho-logical changes in the human corpus luteum during the menstrual cycle . Fertil Steril 1996 ; 65 : 753 – 758 .
43 . Durfee SM , Frates MC . Sonographic spec-trum of the corpus luteum in early pregnancy: gray-scale, color, and pulsed Doppler ap-pearance . J Clin Ultrasound 1999 ; 27 : 55 – 59 .
44 . Jain KA . Sonographic spectrum of hemor-rhagic ovarian cysts . J Ultrasound Med 2002 ; 21 : 879 – 886 .
45 . Van Holsbeke C , Meuleman C , Timmerman D . Acoustic streaming in two endometri-omas: the exception to the rule? Ultrasound Obstet Gynecol 2006 ; 27 : 89 – 90 .
46 . Bhatt S , Kocakoc E , Dogra VS . Endometriosis: sonographic spectrum . Ultrasound Q 2006 ; 22 : 273 – 280 .
47 . Dogan MM , Ugur M , Soysal SK , Soysal ME , Ekici E , Gokmen O . Transvaginal sonographic diagnosis of ovarian endometrioma . Int J Gynaecol Obstet 1996 ; 52 : 145 – 149 .
48 . Pascual MA , Tresserra F , Lopez-Martin L , Ubeda A , Grases PJ , Dexeus S . Role of color Doppler ultrasonography in the diagnosis of endometriotic cyst . J Ultrasound Med 2000 ; 19 : 695 – 699 .
49 . Guerriero S , Mais V , Ajossa S , et al . The role of endovaginal ultrasound in differenti-ating endometriomas from other ovarian cysts . Clin Exp Obstet Gynecol 1995 ; 22 : 20 – 22 .
50 . Valentin L . Pattern recognition of pelvic masses by gray-scale ultrasound imaging: the contribution of Doppler ultrasound . Ultra-sound Obstet Gynecol 1999 ; 14 : 338 – 347 .
51 . Kobayashi H , Sumimoto K , Kitanaka T , et al . Ovarian endometrioma: risks factors of ovarian
STATE OF THE ART: US Characterization of Adnexal Masses Brown et al
354 radiology.rsna.org n Radiology: Volume 254: Number 2—February 2010
68 . Varras M , Polyzos D , Perouli E , Noti P , Pan-tazis I , Akrivis C . Tubo-ovarian abscesses: spectrum of sonographic fi ndings with surgi-cal and pathological correlations . Clin Exp Obstet Gynecol 2003 ; 30 : 117 – 121 .
69 . Van Holsbeke C , Domali E , Holland TK , et al . Imaging of gynecological disease (3): clinical and ultrasound characteristics of granulosa cell tumors of the ovary . Ultra-sound Obstet Gynecol 2008 ; 31 : 450 – 456 .
70 . Demidov VN , Lipatenkova J , Vikhareva O , Van Holsbeke C , Timmerman D , Valentin L . Imaging of gynecological disease (2): clinical and ultrasound characteristics of Sertoli cell tumors, Sertoli-Leydig cell tumors and Ley-dig cell tumors . Ultrasound Obstet Gynecol 2008 ; 31 : 85 – 91 .
71 . Savelli L , Testa AC , Timmerman D , Paladini D , Ljungberg O , Valentin L . Imaging of gyneco-logical disease (4): clinical and ultrasound characteristics of struma ovarii . Ultrasound Obstet Gynecol 2008 ; 32 : 210 – 219 .
72 . Caspi B , Appelman Z , Rabinerson D , Zalel Y , Tulandi T , Shoham Z . The growth pattern of ovarian dermoid cysts: a prospective study in premenopausal and postmenopausal women . Fertil Steril 1997 ; 68 : 501 – 505 .
73 . Mlikotic A , McPhaul L , Hansen GC , Sinow RM . Signifi cance of the solid component in pre-dicting malignancy in ovarian cystic terato-mas . J Ultrasound Med 2001 ; 20 : 859 – 866 .
74 . Talerman A . Germ cell tumors of the ovary . In: Kurman RJ, ed. Blaustein’s pathology of the female genital tract . 5th ed. New York, NY : Springer-Verlag , 2002 ; 967 – 1033 .
75 . McClure MJ , Atri M , Haider MA , Murphy J . Perineural cysts presenting as complex cystic adnexal masses on transvaginal sonography . AJR Am J Roentgenol 2001 ; 177 : 1313 – 1318 .
76 . Pectasides D , Pectasides E , Economopoulos T . Fallopian tube carcinoma: a review . Oncolo-gist 2006 ; 11 : 902 – 912 .
77 . Kurjak A , Kupesic S , Jacobs I . Preoperative diagnosis of the primary fallopian tube carci-noma by three-dimensional static and power Doppler sonography . Ultrasound Obstet Gy-necol 2000 ; 15 : 246 – 251 .
78 . Patlas M , Rosen B , Chapman W , Wilson SR . Sonographic diagnosis of primary malignant tumors of the fallopian tube . Ultrasound Q 2004 ; 20 : 59 – 65 .
79 . Glanc P , Salem S , Farine D . Adnexal masses in the pregnant patient: a diagnostic and manage-ment challenge . Ultrasound Q 2008 ; 24 : 225 – 240 .
80 . Poder L , Coakley FV , Rabban JT , Goldstein RB , Aziz S , Chen LM . Decidualized endo-metrioma during pregnancy: recognizing an imaging mimic of ovarian malignancy . J Com-put Assist Tomogr 2008 ; 32 : 555 – 558 .
81 . Miller JC , Horowitz NS , Thrall JH , Lee SI . Evaluating adnexal lesions: which need follow-up? J Am Coll Radiol 2007 ; 4 : 725 – 729 .
82 . Levine D , Gosink BB , Wolf SI , Feldesman MR , Pretorius DH . Simple adnexal cysts: the natural history in postmenopausal women . Radiology 1992 ; 184 : 653 – 659 .
83 . Conway C , Zalud I , Dilena M , et al . Simple cyst in the postmenopausal patient: detec-tion and management . J Ultrasound Med 1998 ; 17 : 369 – 372 .
84 . Bailey CL , Ueland FR , Land GL , et al . The malignant potential of small cystic ovarian tumors in women over 50 years of age . Gyne-col Oncol 1998 ; 69 : 3 – 7 .
85 . Alcazar JL , Castillo G , Jurado M , Garcia GL . Is expectant management of sonographically benign adnexal cysts an option in selected asymptomatic premenopausal women? Hum Reprod 2005 ; 20 : 3231 – 3234 .
86 . Guerra A , Cunha TM , Felix A . Magnetic resonance evaluation of adnexal masses . Acta Radiol 2008 ; 49 : 700 – 709 .
87 . Sohaib SA , Sahdev A , Van Trappen P , Jacobs IJ , Reznek RH . Characterization of adnexal mass lesions on MR imaging . AJR Am J Roentgenol 2003 ; 180 : 1297 – 1304 .
88 . Adusumilli S , Hussain HK , Caoili EM , et al . MRI of sonographically indeterminate adn-exal masses . AJR Am J Roentgenol 2006 ; 187 : 732 – 740 .
89 . Chang SD , Cooperberg PL , Wong AD , Llewellyn PA , Bilbey JH . Limited-sequence magnetic resonance imaging in the evaluation of the ultrasonographically indeterminate pel-vic mass . Can Assoc Radiol J 2004 ; 55 : 87 – 95 .
90 . Levine D . Solving the problem pelvic ultra-sound with magnetic resonance imaging . Ul-trasound Q 2006 ; 22 : 159 – 168 .
91 . Zhang J , Mironov S , Hricak H , et al . Charac-terization of adnexal masses using feature analysis at contrast-enhanced helical com-puted tomography . J Comput Assist Tomogr 2008 ; 32 : 533 – 540 .
92 . Yamamoto Y , Oguri H , Yamada R , Maeda N , Kohsaki S , Fukaya T . Preoperative evaluation of pelvic masses with combined 18 F-fl uoro-deoxyglucose positron emission tomography and computed tomography . Int J Gynaecol Obstet 2008 ; 102 : 124 – 127 .
93 . Castellucci P , Perrone AM , Picchio M , et al . Diagnostic accuracy of 18F-FDG PET/CT in characterizing ovarian lesions and staging ovar-ian cancer: correlation with transvaginal ultra-sonography, computed tomography, and histol-ogy . Nucl Med Commun 2007 ; 28 : 589 – 595 .
94 . Timor-Tritsch IE , Goldstein SR . The com-plexity of a “complex mass” and the simplic-ity of a “simple cyst” . J Ultrasound Med 2005 ; 24 : 255 – 258 .
95 . Amor F , Vaccaro H , Alcazar JL , Leon M , Craig JM , Martinez J . Gynecologic imaging reporting and data system: a new proposal for classifying adnexal masses on the basis of sonographic fi ndings . J Ultrasound Med 2009 ; 28 : 285 – 291 .
cancer development . Eur J Obstet Gynecol Reprod Biol 2008 ; 138 : 187 – 193 .
52 . Caspi B , Appelman Z , Rabinerson D , Elcha-lal U , Zalel Y , Katz Z . Pathognomonic echo patterns of benign cystic teratomas of the ovary: classifi cation, incidence and accuracy rate of sonographic diagnosis . Ultrasound Obstet Gynecol 1996 ; 7 : 275 – 279 .
53 . Patel MD , Feldstein VA , Lipson SD , Chen DC , Filly RA . Cystic teratomas of the ovary: diagnostic value of sonography . AJR Am J Roentgenol 1998 ; 171 : 1061 – 1065 .
54 . Kim HC , Kim SH , Lee HJ , Shin SJ , Hwang SI , Choi YH . Fluid-fl uid levels in ovarian tera-tomas . Abdom Imaging 2002 ; 27 : 100 – 105 .
55 . Saba L , Guerriero S , Sulcis R , Virgilio B , Melis G , Mallarini G. Mature and immature ovarian teratomas: CT, US and MR imaging characteristics . Eur J Radiol 2008 Sep 19. [Epub ahead of print]
56 . Young RH , Scully RE . Sex cord-stromal, ste-roid cell, and other ovarian tumors with en-docrine, paraendocrine, and paraneoplastic manifestations . In: Kurman RJ, ed. Blaustein’s pathology of the female genital tract . 5th ed. New York, NY : Springer-Verlag , 2002 ; 905 – 966 .
57 . Conte M , Guariglia L , Panici PB , et al . Ovar-ian fi brothecoma: sonographic and histologic fi ndings . Gynecol Obstet Invest 1991 ; 32 : 51 – 54 .
58 . Bazot M , Ghossain MA , Buy JN , et al . Fi-brothecomas of the ovary: CT and US fi ndings . J Comput Assist Tomogr 1993 ; 17 : 754 – 759 .
59 . Kim JS , Woo SK , Suh SJ , Morettin LB . Sonographic diagnosis of paraovarian cysts: value of detecting a separate ipsilateral ovary . AJR Am J Roentgenol 1995 ; 164 : 1441 – 1444 .
60 . Korbin CD , Brown DL , Welch WR . Parao-varian cystadenomas and cystadenofi bromas: sonographic characteristics in 14 cases . Ra-diology 1998 ; 208 : 459 – 462 .
61 . Patel MD , Acord DL , Young SW . Likelihood ratio of sonographic fi ndings in discriminating hydrosalpinx from other adnexal masses . AJR Am J Roentgenol 2006 ; 186 : 1033 – 1038 .
63 . Guerriero S , Ajossa S , Mais V , Angiolucci M , Paoletti AM , Melis GB . Role of transvaginal sonography in the diagnosis of peritoneal in-clusion cysts . J Ultrasound Med 2004 ; 23 : 1193 – 1200 .
64 . Jain KA . Imaging of peritoneal inclusion cysts . AJR Am J Roentgenol 2000 ; 174 : 1559 – 1563 .
65 . Kim SH , Sim JS , Seong CK . Interface vessels on color/power Doppler US and MRI: a clue to differentiate subserosal uterine myomas from extrauterine tumors . J Comput Assist Tomogr 2001 ; 25 : 36 – 42 .
66 . Madan R . The bridging vascular sign . Radiol-ogy 2006 ; 238 : 371 – 372 .