42
Chronic HIV Infection Clinical Manifestations Opportunistic Infections O.I. Prophylaxis
| Date post: | 23-Dec-2015 |
| Category: |
Documents |
| Upload: | blanche-cunningham |
| View: | 226 times |
| Download: | 1 times |
Chronic HIV Infection
Clinical Manifestations
Opportunistic Infections
O.I. Prophylaxis

1
10
100
1,000
10,000
100,000
1,000,000
10,000,000
Pla
sma
HIV
RN
A
Plasma RNA Copies
CD4 Cells
4-8 Weeks Up to 12 Years 2-3 Years
CD
4 Cell C
ount
1,000
500
Intermediate Stage AIDS
Primary Infection
Sero-conversion
CD4 Count, Viral Load and Clinical Course

Common Clinical Manifestations of Chronic HIV Infection
• Constitutional Symptoms– fever– weight loss/wasting– fatigue
• Organ/System Specific– virtually all organ systems can be affected
• Consider HIV testing for unexplained syndromes

Wasting
By Salvatore Marra, from AIDS imaging http://members.xoom.it/Aidsimaging

By Salvatore Marra, from AIDS imaging http://members.xoom.it/Aidsimaging

http://hivinsite.ucsf.edu

By Salvatore Marra, from AIDS imaging http://members.xoom.it/Aidsimaging

By Salvatore Marra, from AIDS imaging http://members.xoom.it/Aidsimaging

By Salvatore Marra, from AIDS imaging http://members.xoom.it/Aidsimaging

By Salvatore Marra, from AIDS imaging http://members.xoom.it/Aidsimaging

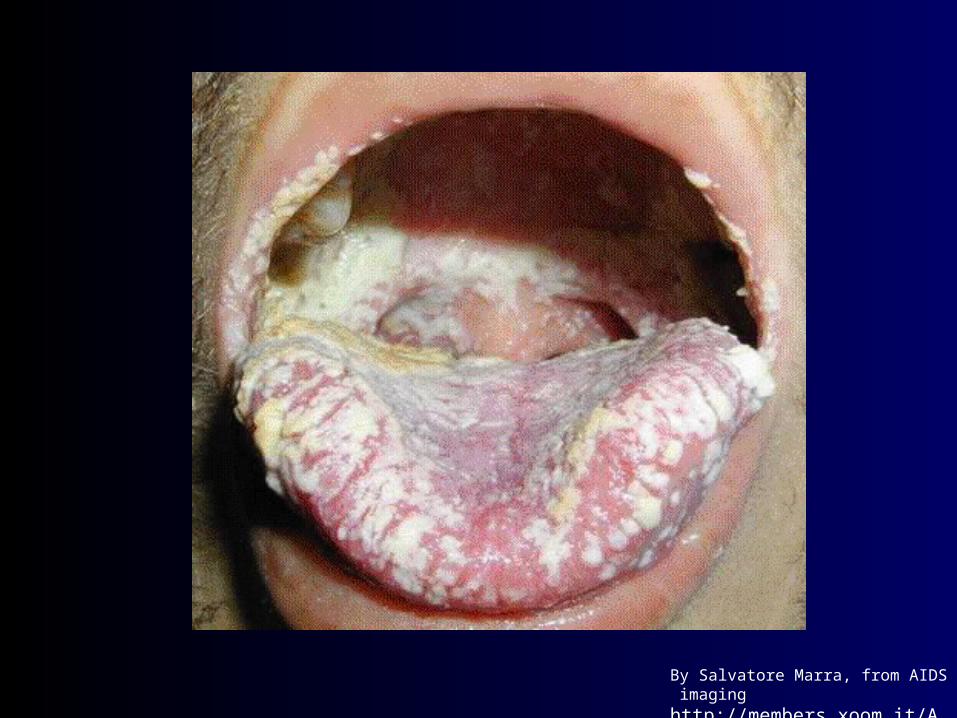
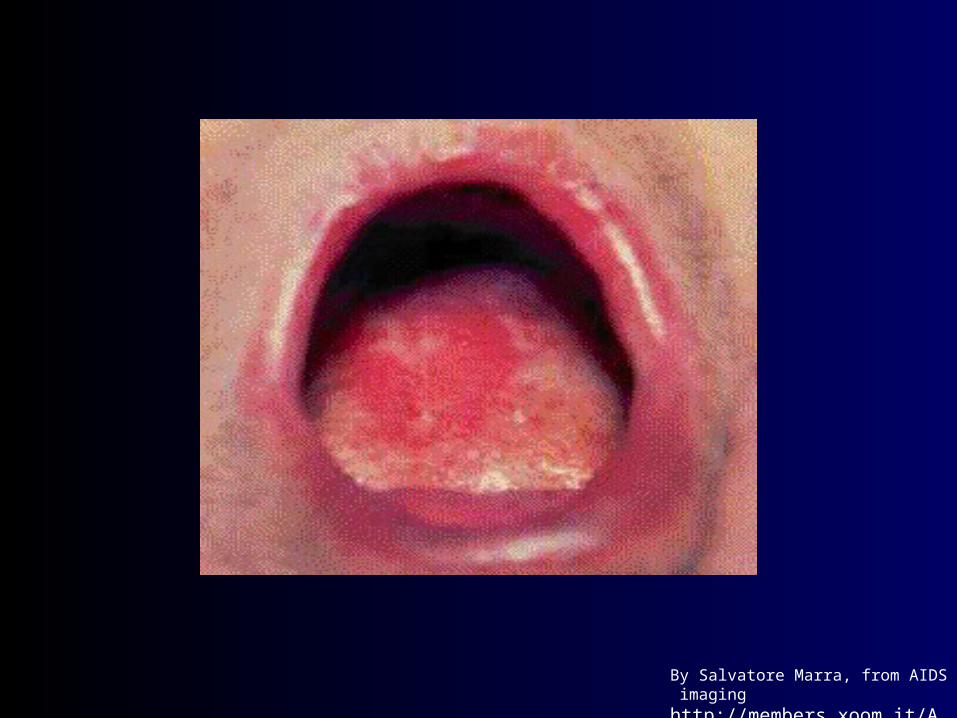
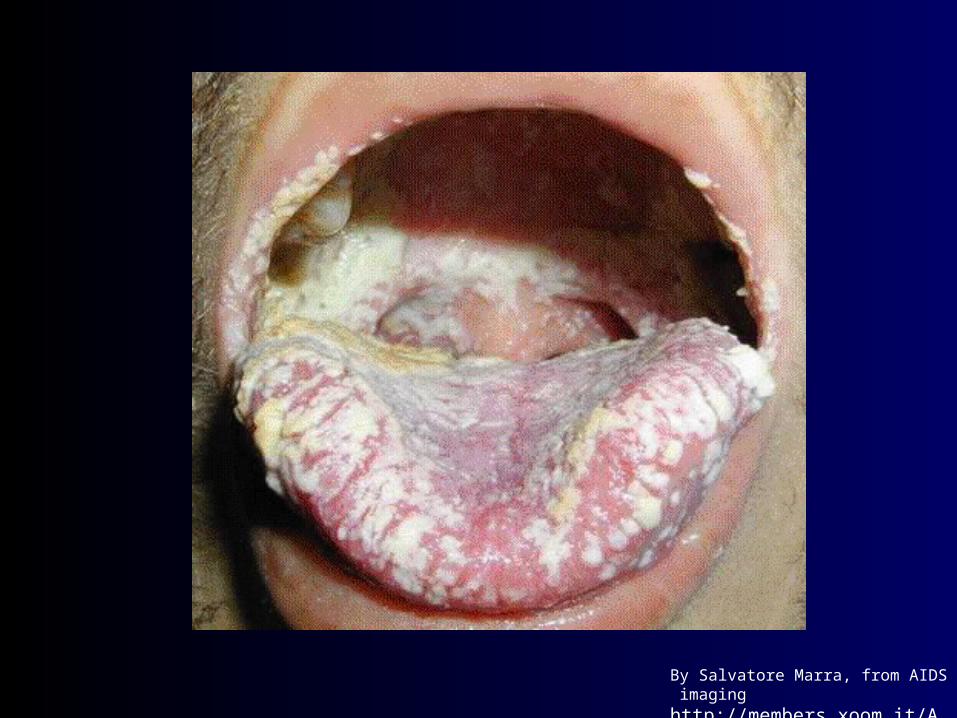
Oral Manifestations of HIV/AIDS

By Salvatore Marra, from AIDS imaging http://members.xoom.it/Aidsimaging

By Salvatore Marra, from AIDS imaging http://members.xoom.it/Aidsimaging
By Salvatore Marra, from AIDS imaging http://members.xoom.it/Aidsimaging
By Salvatore Marra, from AIDS imaging http://members.xoom.it/Aidsimaging

By Salvatore Marra, from AIDS imaging http://members.xoom.it/Aidsimaging

By Salvatore Marra, from AIDS imaging http://members.xoom.it/Aidsimaging

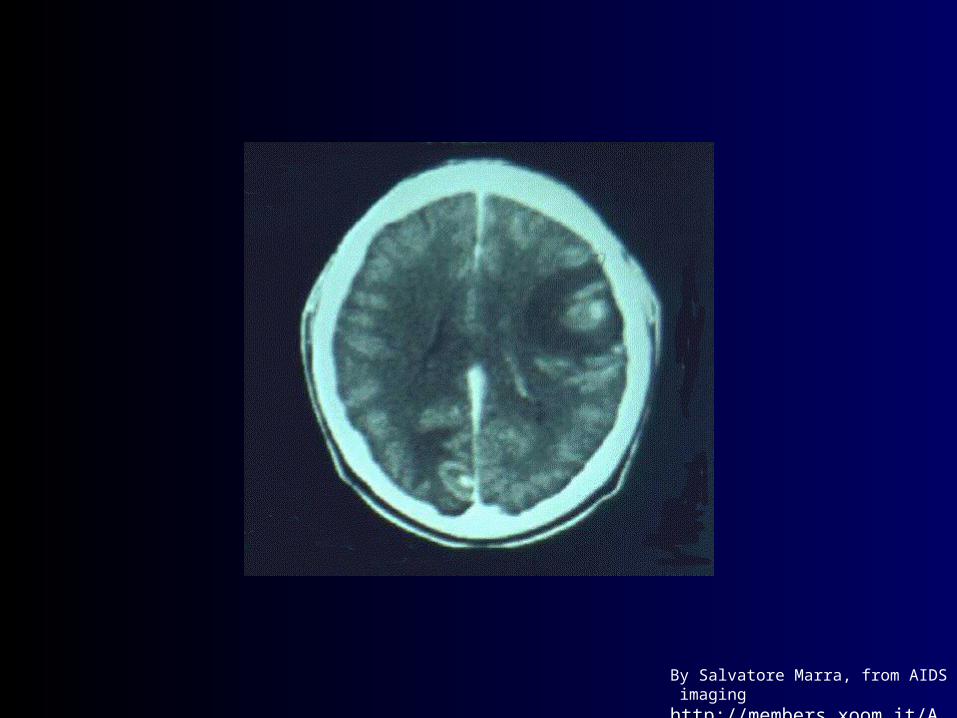
CNS Lesions

By Salvatore Marra, from AIDS imaging http://members.xoom.it/Aidsimaging

By Salvatore Marra, from AIDS imaging http://members.xoom.it/Aidsimaging
By Salvatore Marra, from AIDS imaging http://members.xoom.it/Aidsimaging
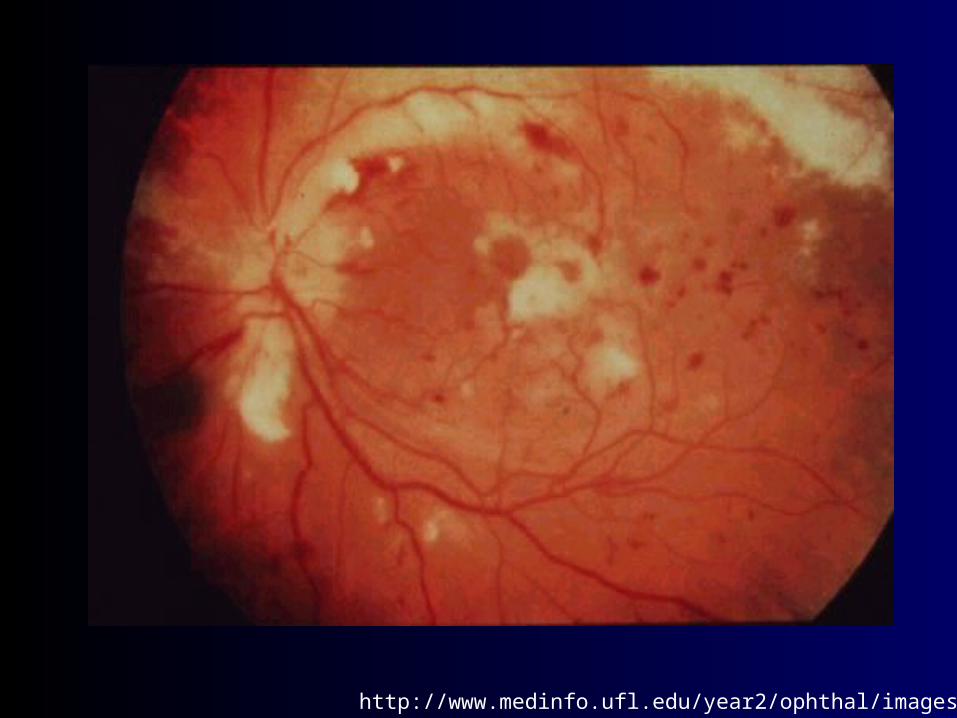
http://www.medinfo.ufl.edu/year2/ophthal/images/35.jpg
By Salvatore Marra, from AIDS imaging http://members.xoom.it/Aidsimaging
By Salvatore Marra, from AIDS imaging http://members.xoom.it/Aidsimaging

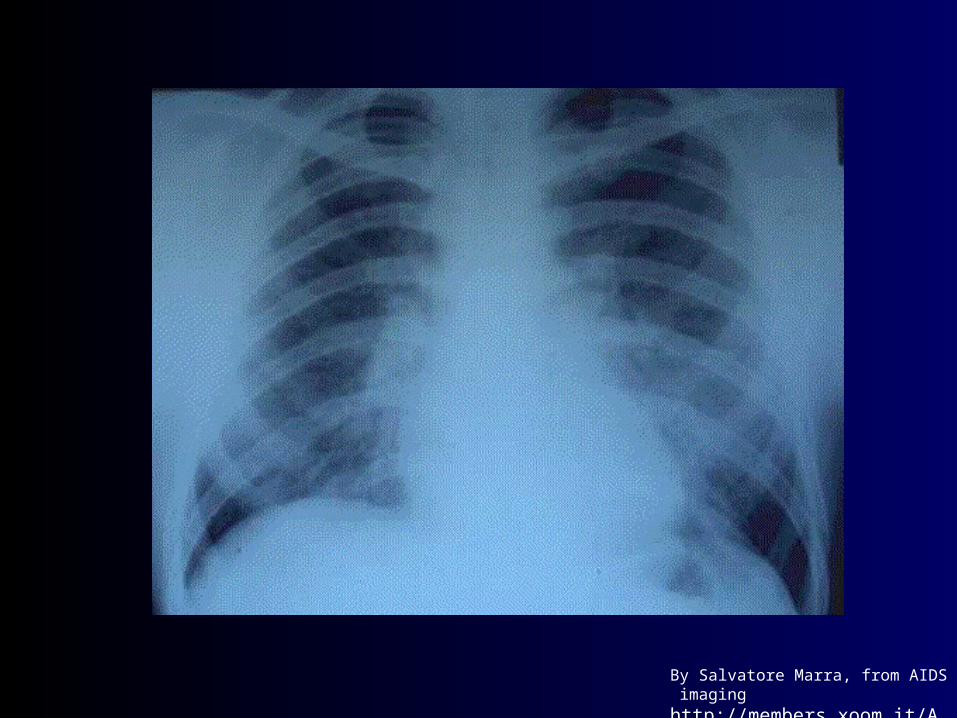
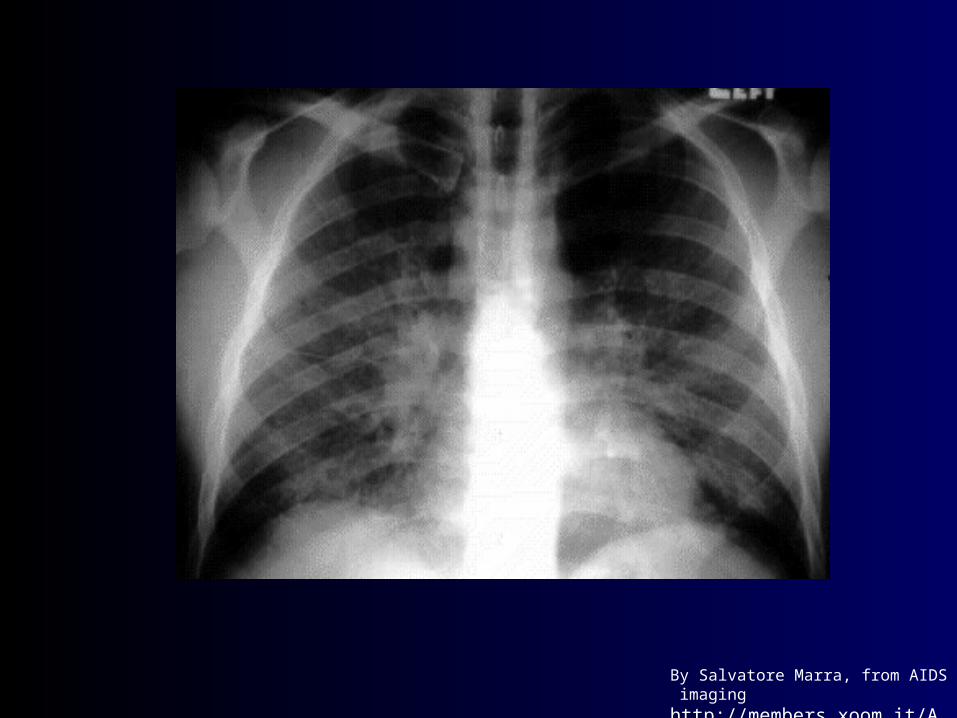
Prophylaxis against Opportunistic Infections
• Pneumocystis carinii pneumonia (PCP)
• Toxoplasmosis gondii
• Mycobacterium Avium Complex (MAC)
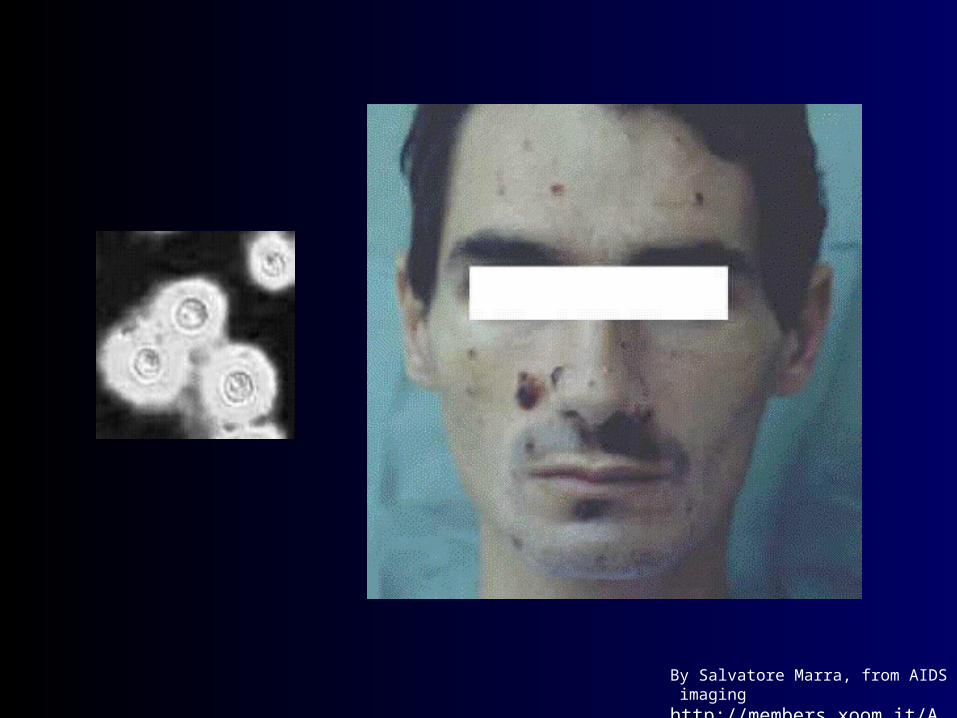
• Cryptococcal Meningitis
• CMV retinitis
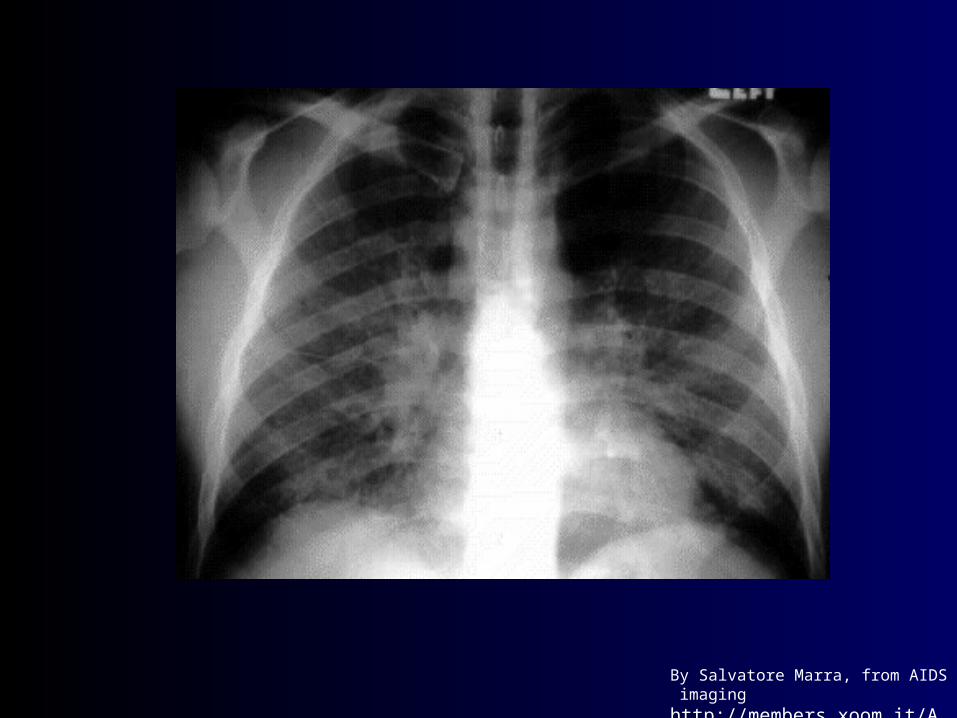
• Mycobacterium tuberculosis (TB)

By Salvatore Marra, from AIDS imaging http://members.xoom.it/Aidsimaging
PCP - Primary Prophylaxis
• Initiate at CD4<200 or prior AIDS-defining illness
• Best: TMP-SMX– 1 DS qd, 1 SS qd, 1 DS qod or tiw– 1 DS qd also confers protection vs T. gondii and
common bacterial infections– consider desensitization if allergic reaction– up to 70% of patients can tolerate reinstitution of
therapy
By Salvatore Marra, from AIDS imaging http://members.xoom.it/Aidsimaging

Toxoplasmic Encephalitis Primary Prophylaxis
• Avoid contact with cat feces, raw or undercooked meat, esp. if IgG (-)
• Initiate primary prophylaxis at CD4<100
• Options include:– TMP-SMX– dapsone plus pyrimethamine/leucovorin– atovaquone plus pyrimethamine/leucovorin– pyrimethamine-sulfadiazine/leucovorin
MAC Primary Prophylaxis
• initiate at CD4<50; R/O dMAC first if symptomatic• options:
– clarithromycin 500mg po bid
– azithromycin 500mg po qd or 1200mg po qwk
– rifabutin 300mg po qd
• survival benefit shown for clarithromycin• multiple interactions between rifabutin and
antiretrovirals
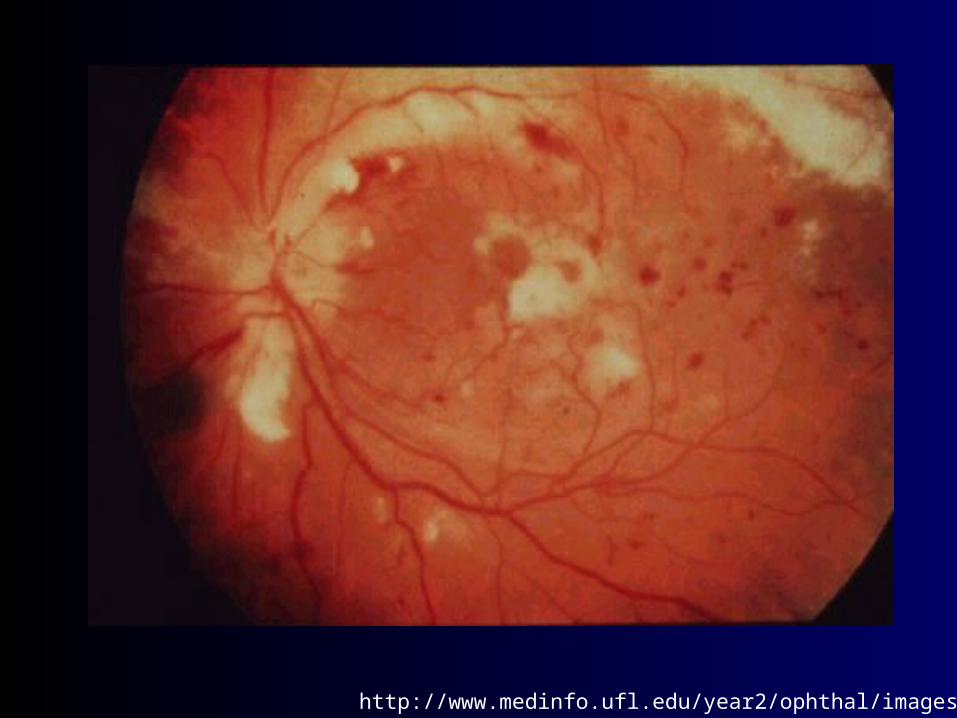
http://www.medinfo.ufl.edu/year2/ophthal/images/35.jpg
Cytomegalovirus Primary Prophylaxis
• Counseling and regular ophthalmological exams for patients with CD4<50
• CMV(-) blood for patients who are CMV(-) at baseline
By Salvatore Marra, from AIDS imaging http://members.xoom.it/Aidsimaging
Candidal Infections
• fluconazole can reduce risk of vaginal, oropharyngeal and esophageal infection
• however, generally not recommended:– potential for resistance, cost, possibility of drug
interactions
– low mortality associated with these infections
– acute treatment generally effective

Candidal Infections for which prophylaxis may be warranted:
• recurrent esophageal candidiasis: fluconazole 100-200mg qd
• recurrent Candida vaginitis: weekly intravaginal clotrimazole tablets or lactobacillus gel capsules reduces frequency by approximately 50%1
1. Abstract 677, 7th Conference on Retroviruses and Opportunistic Infections, 2000.
By Salvatore Marra, from AIDS imaging http://members.xoom.it/Aidsimaging
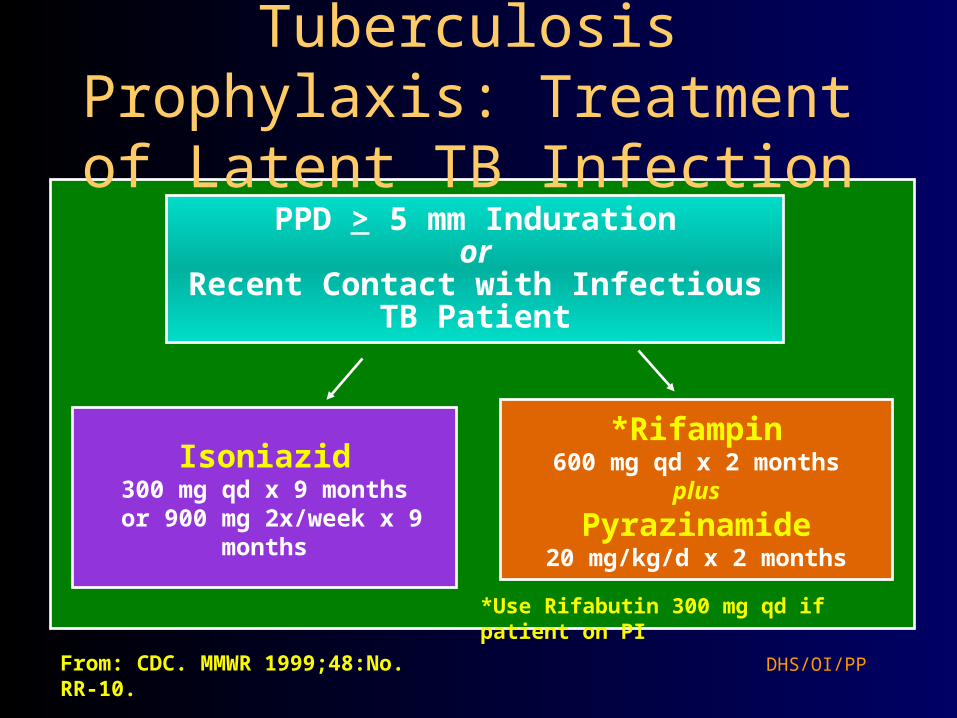
Tuberculosis Prophylaxis: Treatment of Latent TB Infection
DHS/OI/PP
Isoniazid300 mg qd x 9 months
or 900 mg 2x/week x 9 months
PPD > 5 mm Indurationor
Recent Contact with Infectious TB Patient
*Rifampin600 mg qd x 2 months
plus
Pyrazinamide20 mg/kg/d x 2 months
*Use Rifabutin 300 mg qd if patient on PI
From: CDC. MMWR 1999;48:No. RR-10.

Consultation Services for Clinicians Caring for Patients with HIV/AIDS
• Northwest AETC– (206) 994-8773 pager, (206) 731-1058 VM
• University of Washington MEDCON– (800) 326-5300
• National HIV Telephone Consultation Service (Warmline)– (800) 933-3413
• National Clinicians’ Post-Exposure Prophylaxis Hotline (PEPline)– (888) HIV-4911
Extra slides
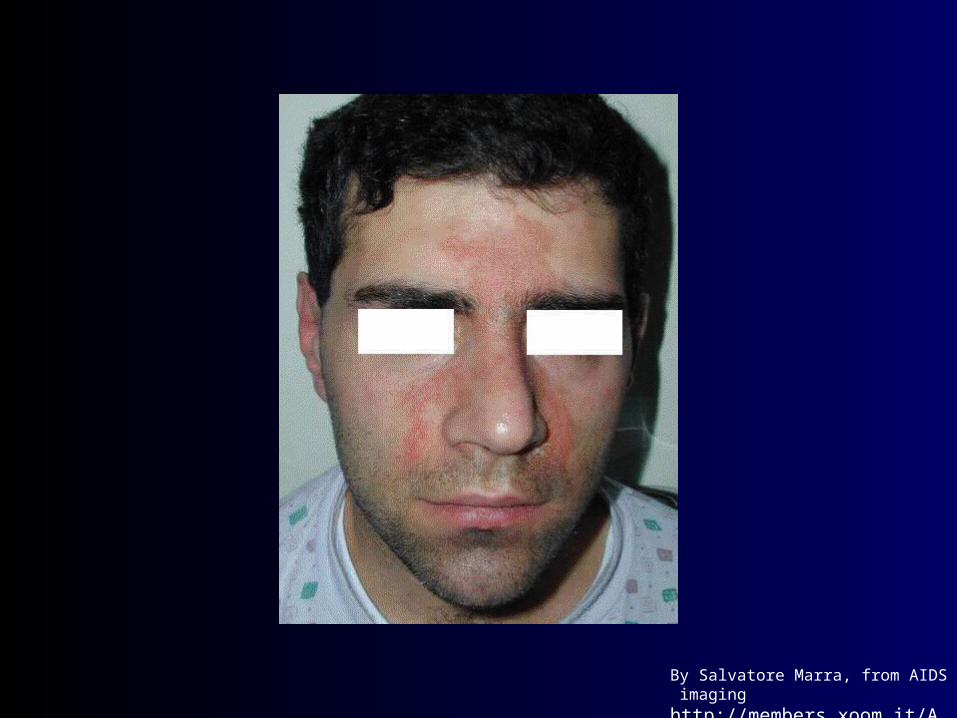
By Salvatore Marra, from AIDS imaging http://members.xoom.it/Aidsimaging
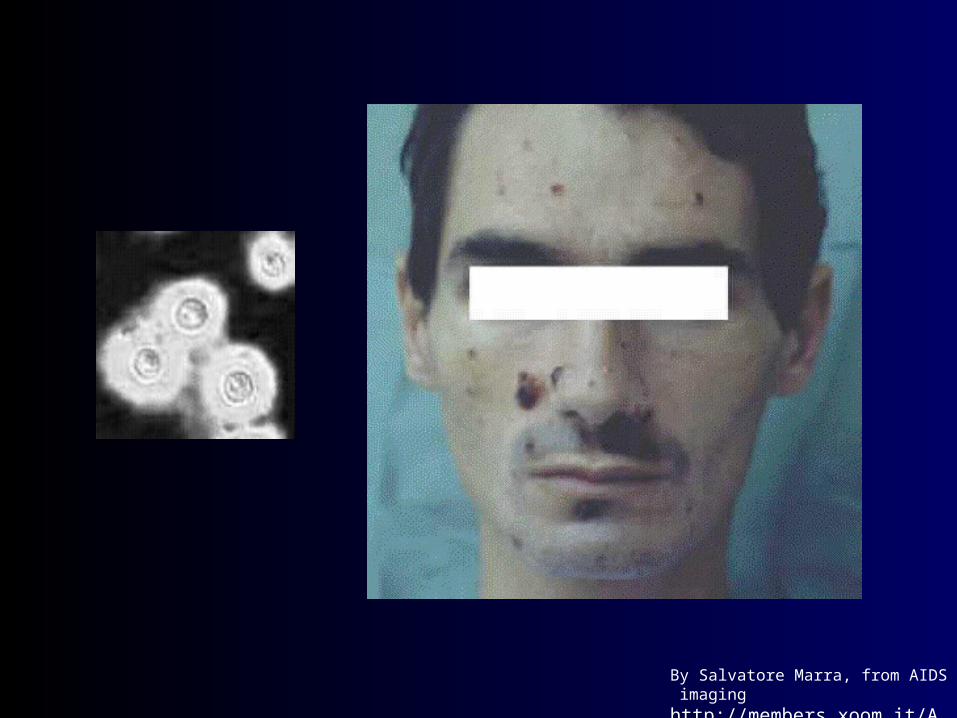
By Salvatore Marra, from AIDS imaging http://members.xoom.it/Aidsimaging
Primary Prophylaxis vs Cryptococcal Meningitis?
• Fluconazole provides limited protection
• resistance can develop
• Not routinely recommended

















