37
CHRONIC MYELOID CHRONIC MYELOID LEUKAEMIALEUKAEMIA
Dr Rosline HassanDr Rosline HassanDepartment of HaematologyDepartment of HaematologySchool of Medical SciencesSchool of Medical SciencesUniversiti Sains MalaysiaUniversiti Sains Malaysia
Leukaemias Leukaemias What are LeukemiasWhat are Leukemias
– Neoplasm of white blood cell and its Neoplasm of white blood cell and its precursorprecursor
– Clonal proliferations and Clonal proliferations and accumulation of cells in marrow accumulation of cells in marrow
– Classify as Classify as Acute leukaemiasAcute leukaemias Chronic leukaemiasChronic leukaemias
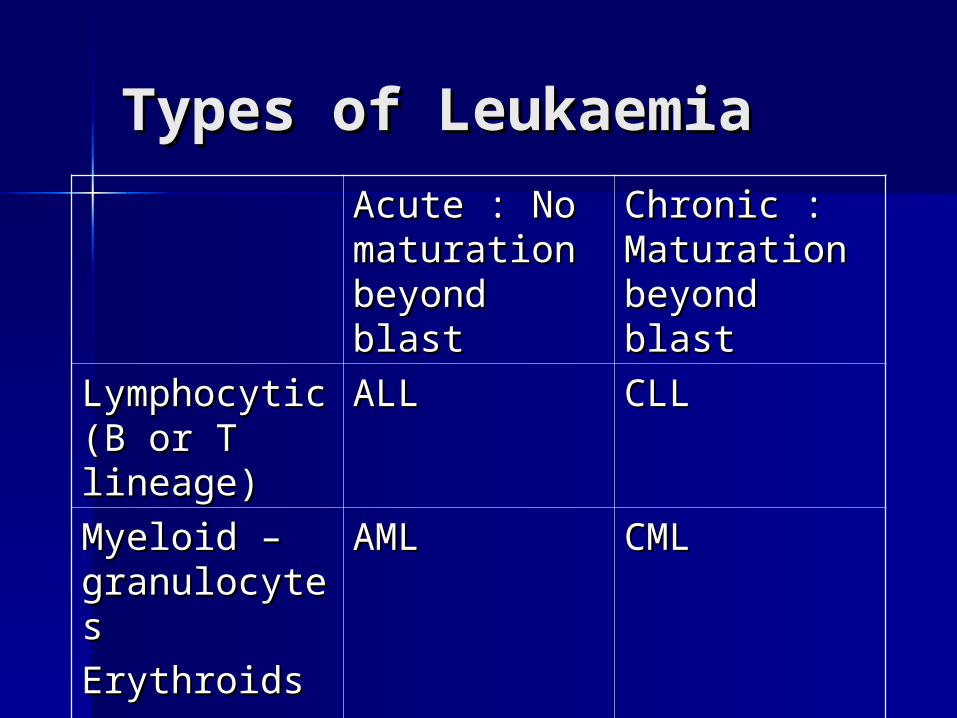
Types of LeukaemiaTypes of LeukaemiaAcute : No Acute : No maturation maturation beyond blastbeyond blast
Chronic : Chronic : Maturation Maturation beyond blastbeyond blast
Lymphocytic Lymphocytic (B or T (B or T lineage) lineage)
ALLALL CLLCLL
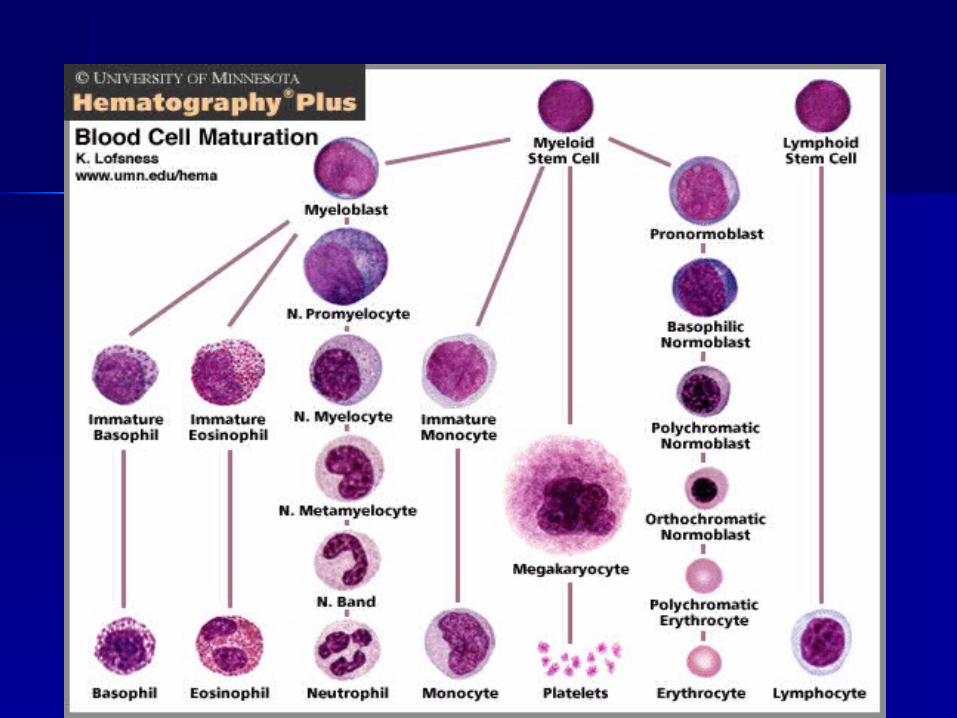
Myeloid – Myeloid – granulocytesgranulocytesErythroidsErythroidsMonocytesMonocytesPlatelets Platelets
AMLAML CMLCML

Introduction- CMLIntroduction- CML Clonal malignant myeloproliferative Clonal malignant myeloproliferative
disorder characterized by increased disorder characterized by increased proliferation of the granulocytic cell line proliferation of the granulocytic cell line without the loss of their capacity to without the loss of their capacity to differentiate differentiate
Results in increases in myeloid cells, Results in increases in myeloid cells, erythroid cells and platelets in peripheral erythroid cells and platelets in peripheral blood and marked myeloid hyperplasia in blood and marked myeloid hyperplasia in the bone marrow the bone marrow
Originate in a single abnormal Originate in a single abnormal haemopoietic stem cellhaemopoietic stem cell
Introduction- CMLIntroduction- CML Incidence :1 per 100,000 (UK)Incidence :1 per 100,000 (UK) Accounts for 7-15% of all Accounts for 7-15% of all
leukaemia in adultsleukaemia in adults Median age : 53 yearsMedian age : 53 years All age groups, including children, All age groups, including children,
can be affectedcan be affected

Introduction- CMLIntroduction- CML EtiologyEtiology
– Not clearNot clear– Little evidence of genetic factors Little evidence of genetic factors
linked to the diseaselinked to the disease– Increased incidence Increased incidence
Survivors of the atomic disasters at Survivors of the atomic disasters at Nagasaki & HiroshimaNagasaki & Hiroshima
Post radiation therapyPost radiation therapy


LeukaemogenesisLeukaemogenesis

LeukaemogenesisLeukaemogenesis Philadelphia Philadelphia
chromosome is an chromosome is an acquired cytogenetic acquired cytogenetic anomaly that is anomaly that is characterizes in all characterizes in all leukaemic cells in leukaemic cells in CMLCML
90-95% of CML pts 90-95% of CML pts have Ph chromosomehave Ph chromosome
Reciprocal Reciprocal translocation of translocation of chromosome 22 and chromosome 22 and chromosome 9chromosome 9
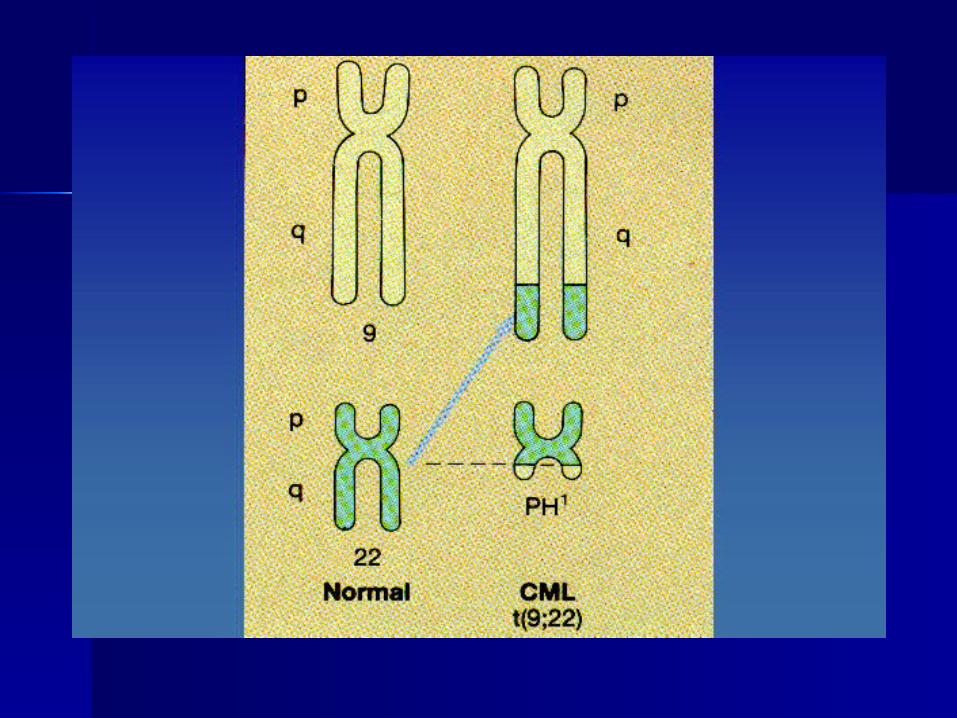
LeukaemogenesisLeukaemogenesis BCR (breakpoint cluster region)BCR (breakpoint cluster region) gene gene
on chromosome 22 fused to the on chromosome 22 fused to the ABL ABL (Ableson leukemia virus)(Ableson leukemia virus) gene on gene on chromosome 9chromosome 9
Ph chromosome is found on myeloid, Ph chromosome is found on myeloid, monocytic, erythroid, megakaryocytic, monocytic, erythroid, megakaryocytic, B-cells and sometimes T-cell proof B-cells and sometimes T-cell proof that CML derived from pluripotent that CML derived from pluripotent stem cellstem cell

LeukaemogenesisLeukaemogenesis Molecular consequence Molecular consequence
of the t(9;22) is the of the t(9;22) is the fusion protein BCR–ABL, fusion protein BCR–ABL, which has increased in which has increased in tyrosine kinase activitytyrosine kinase activity
BCR-ABL protein BCR-ABL protein transform hematopoietic transform hematopoietic cells so that their growth cells so that their growth and survival become and survival become independent of cytokinesindependent of cytokines
It protects hematopoietic It protects hematopoietic cells from programmed cells from programmed cell death (apoptosis) cell death (apoptosis)
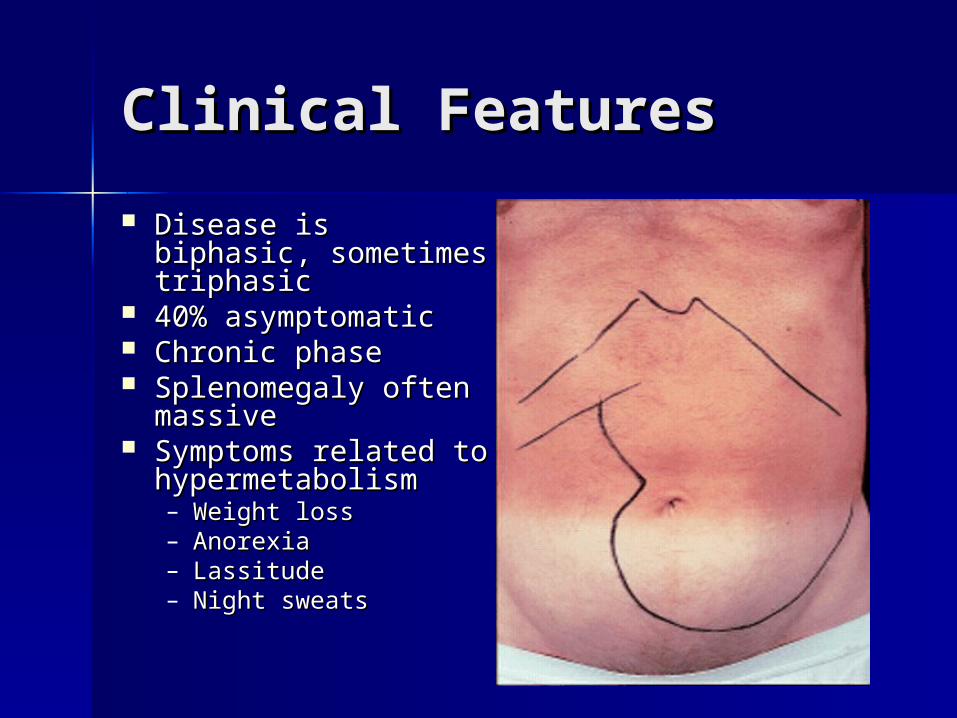
Clinical FeaturesClinical Features Disease is biphasic, Disease is biphasic,
sometimes triphasicsometimes triphasic 40% asymptomatic40% asymptomatic Chronic phaseChronic phase Splenomegaly often Splenomegaly often
massivemassive Symptoms related Symptoms related
to hypermetabolismto hypermetabolism– Weight lossWeight loss– AnorexiaAnorexia– LassitudeLassitude– Night sweatsNight sweats

Clinical FeaturesClinical Features Clinical features cont…Clinical features cont… Features of anaemiaFeatures of anaemia
– Pallor, dyspnoea, tachycardiaPallor, dyspnoea, tachycardia Abnormal platelet functionAbnormal platelet function
– Bruising, epistaxis, menorrhagiaBruising, epistaxis, menorrhagia Hyperleukocytosis Hyperleukocytosis
– thrombosisthrombosis– Increased purine breakdown : goutIncreased purine breakdown : gout– Visual disturbancesVisual disturbances– PriapismPriapism

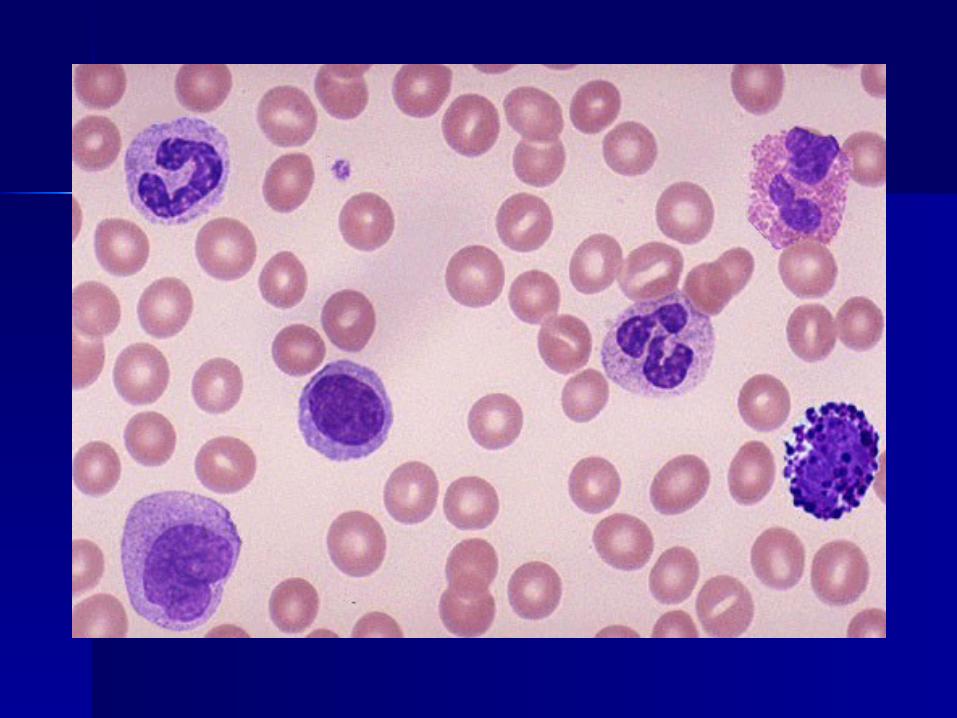
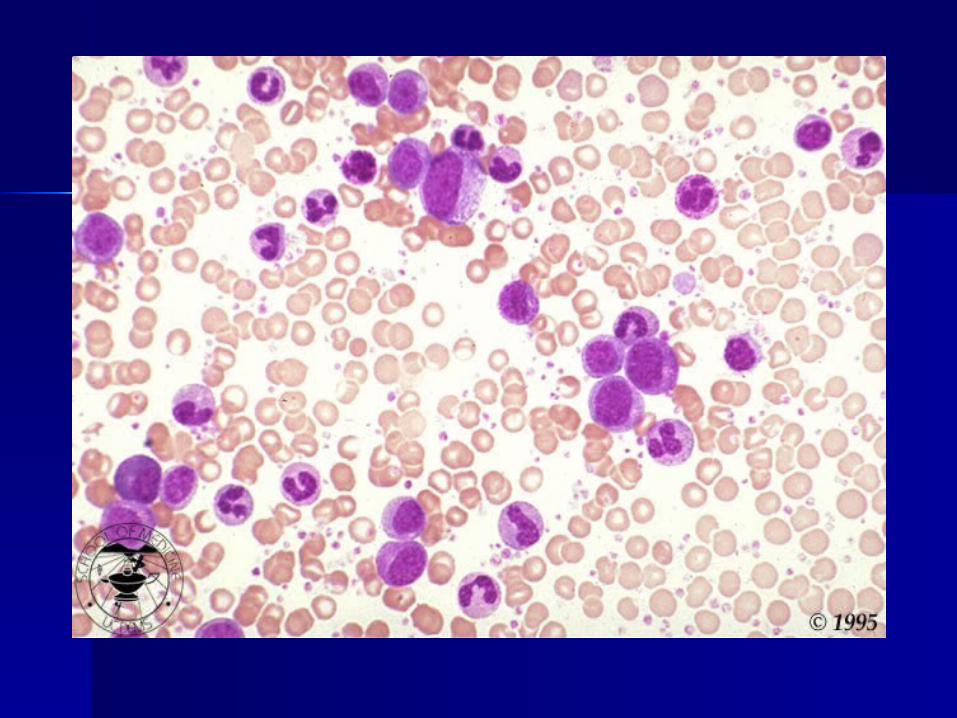
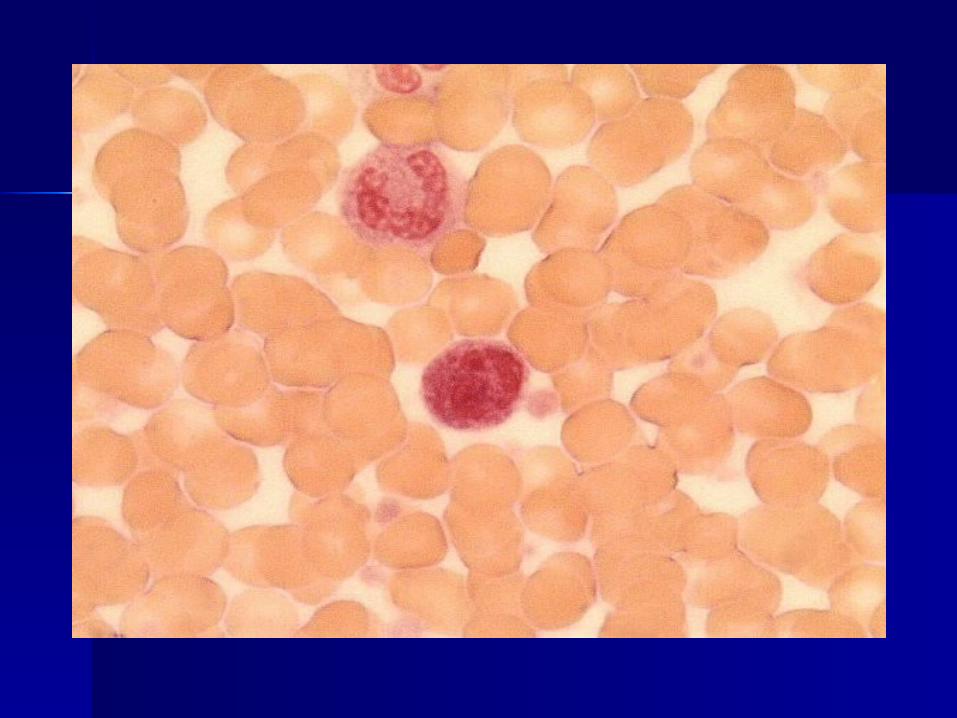
Lab featuresLab features Peripheral blood filmPeripheral blood film
– AnaemiaAnaemia– Leukocytosis (usu >25 x 10Leukocytosis (usu >25 x 1099/L, freq> /L, freq>
100 x 10100 x 1099/L/L– WBC differential shows granulocytes WBC differential shows granulocytes
in all stages of maturationin all stages of maturation– BasophiliaBasophilia– thrombocytosisthrombocytosis


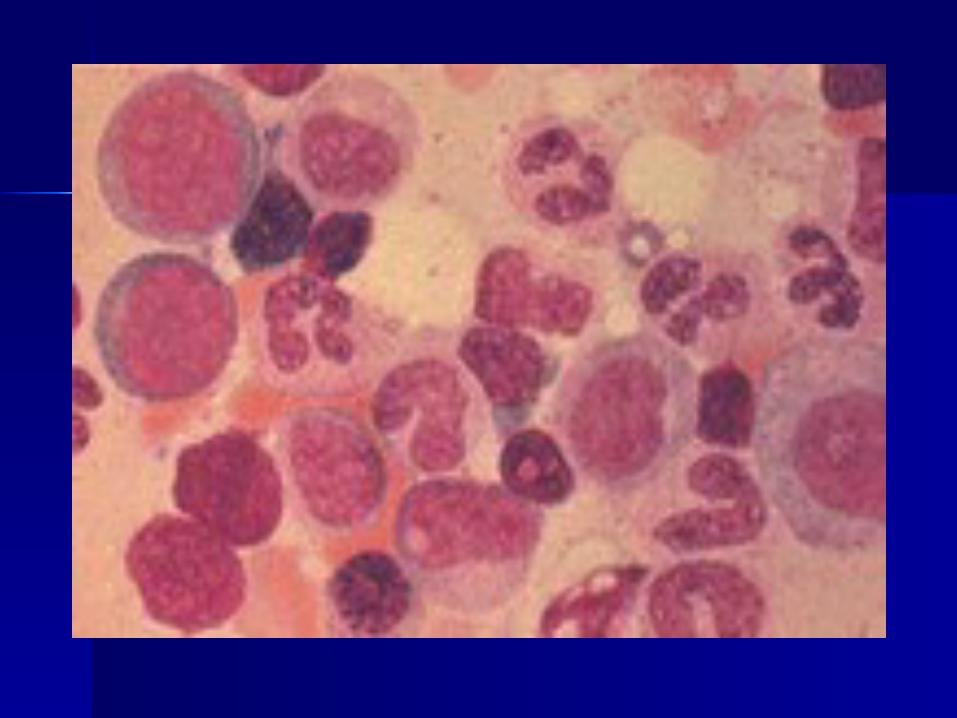
Lab featuresLab features Bone marrowBone marrow
– Hypercellular (reduced Hypercellular (reduced fat spaces)fat spaces)
– Myeloid:erythroid ratio Myeloid:erythroid ratio – 10:1 to 30:1 (N : 2:1)– 10:1 to 30:1 (N : 2:1)
– Myelocyte predominant Myelocyte predominant cell, blasts less 10%cell, blasts less 10%
– Megakaryocytes Megakaryocytes increased & dysplasticincreased & dysplastic
– Increase reticulin Increase reticulin fibrosis in 30-40%fibrosis in 30-40%

Lab featuresLab features Other lab features :Other lab features :
– NAP reducedNAP reduced– Serum B12 and transcobalamin Serum B12 and transcobalamin
increasedincreased– Serum uric acid increasedSerum uric acid increased– Lactate dehydrogenase increasedLactate dehydrogenase increased– Cytogenetic : Philadelphia Cytogenetic : Philadelphia
chromosomechromosome

Laboratory- summaryLaboratory- summary Lab investigation to confirm Lab investigation to confirm
diagnosisdiagnosis– Full blood pictureFull blood picture– Neutrophil alkaline phosphataseNeutrophil alkaline phosphatase– Bone marrow cytogeneticBone marrow cytogenetic
PhasesPhases Accelerated phaseAccelerated phase
– Median duration is 3.5 – 5 yrs before Median duration is 3.5 – 5 yrs before evolving to more aggressive phasesevolving to more aggressive phases
– Clinical featuresClinical features Increasing splenomegaly refractory to chemoIncreasing splenomegaly refractory to chemo Increasing chemotherapy requirementIncreasing chemotherapy requirement
– Lab featuresLab features Blasts>15% in bloodBlasts>15% in blood Blast & promyelocyte > 30% in bloodBlast & promyelocyte > 30% in blood Basophil 20% in bloodBasophil 20% in blood ThrombocytopeniaThrombocytopenia Cytogenetic: clonal evolutionCytogenetic: clonal evolution
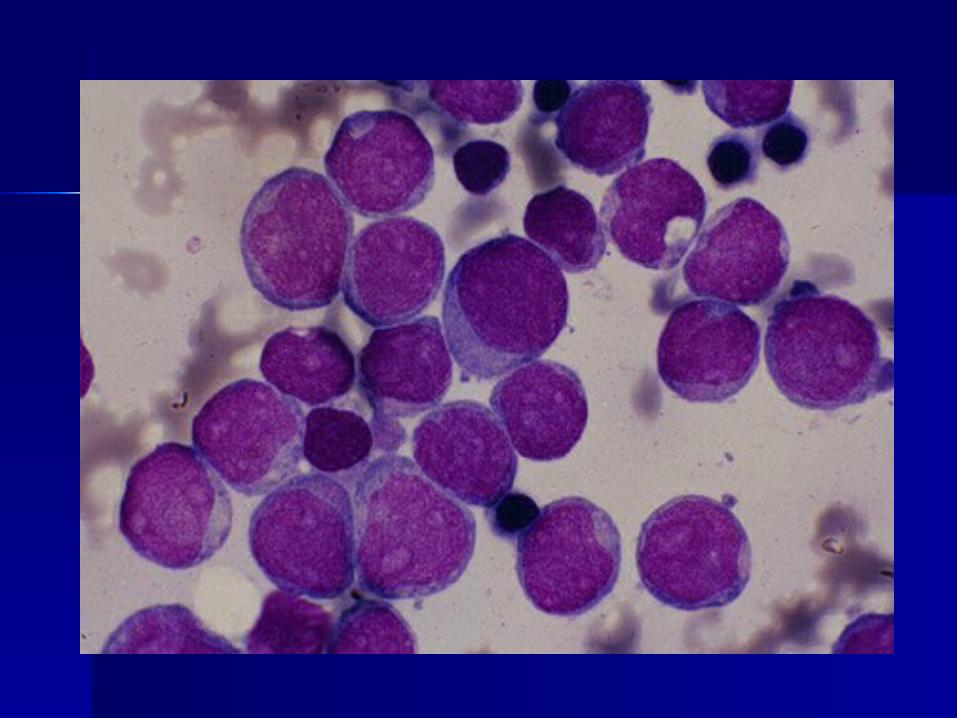
Phases Phases Blastic phase Blastic phase
– Resembles acute leukaemiaResembles acute leukaemia– Diagnosis requires > 30% blast in Diagnosis requires > 30% blast in
marrowmarrow– 2/3 transform to myeloid blastic phase 2/3 transform to myeloid blastic phase
and 1/3 to lymphoid blastic phaseand 1/3 to lymphoid blastic phase– Survival : 9 mos vs 3 mos (lym vs Survival : 9 mos vs 3 mos (lym vs
myeloid)myeloid)


General ManagementGeneral Management Discussion with familyDiscussion with family
– The disease & diagnosisThe disease & diagnosis– Prognosis Prognosis – Choices of treatmentChoices of treatment
Cytotoxic drug vs bone marrow Cytotoxic drug vs bone marrow transplanttransplant
Side effectSide effect

CML - principles of CML - principles of treatmenttreatment Relieve symptoms of hyperleukocytosis, Relieve symptoms of hyperleukocytosis,
splenomegaly and thrombocytosissplenomegaly and thrombocytosis– HydrationHydration– Chemotherapy (bulsuphan, Hydoxyurea)Chemotherapy (bulsuphan, Hydoxyurea)
Control and prolong chronic phase Control and prolong chronic phase (non-curative)(non-curative)– alpha interferon+chemotherapyalpha interferon+chemotherapy– imatinib mesylate imatinib mesylate – chemotherapy (hydroxyurea)chemotherapy (hydroxyurea)

CML - principles of CML - principles of treatmenttreatment Treatment cont…Treatment cont… Eradicate malignant clone Eradicate malignant clone
(curative)(curative)– allogeneic transplantationallogeneic transplantation– alpha interferon ?alpha interferon ?– imatinib mesylate/STI 571 ?imatinib mesylate/STI 571 ?
(Thyrosine kinase inhibitor)(Thyrosine kinase inhibitor)
Chemotherapy Chemotherapy BusulphanBusulphan
– Alkylating agentAlkylating agent– Preferred in older pts (not candidate Preferred in older pts (not candidate
for transplant)for transplant)– Side effect :Side effect :
prolonged myelosuppressionprolonged myelosuppression Pulmonary fibrosisPulmonary fibrosis Skin pigmentationSkin pigmentation infertilityinfertility

ChemotherapyChemotherapy HydoxyuresHydoxyures
– Fewer side effectFewer side effect– Acts by inhibiting the enzyme Acts by inhibiting the enzyme
ribonucleotide reductaseribonucleotide reductase Haematological remissions obtain in Haematological remissions obtain in
80% for both drugs 80% for both drugs However disease progression not However disease progression not
altered and persistence of Ph altered and persistence of Ph chromosome containing clonechromosome containing clone

ChemotherapyChemotherapy Recombinant human Recombinant human α- α- InterferonInterferon
– Prolong chronic phase and increase Prolong chronic phase and increase survivalsurvival
– Haematogical and cytogenetic remissionHaematogical and cytogenetic remission– Side effect Side effect
Flu like symptomsFlu like symptoms Fever and chillsFever and chills AnorexiaAnorexia DepressionDepression


CML - prognosisCML - prognosis Median survivalMedian survival 3.5 yrs (range 3.5 yrs (range
2-8 yrs)2-8 yrs) Interferon + chemotherapy :6 Interferon + chemotherapy :6
years years Transplant :Transplant : 5+ years5+ years imatinib mesylate ?imatinib mesylate ?
Thank youThank you

















