77
CHRONIC OBSTRUCTIVE CHRONIC OBSTRUCTIVE PULMONARY DISEASE PULMONARY DISEASE
| Date post: | 27-Dec-2015 |
| Category: |
Documents |
| Upload: | teresa-doyle |
| View: | 256 times |
| Download: | 13 times |
CHRONIC CHRONIC OBSTRUCTIVEOBSTRUCTIVE
PULMONARY DISEASE PULMONARY DISEASE
Chronic Obstructive Chronic Obstructive Pulmonary Disease Pulmonary Disease
(COPD)(COPD) Chronic Obstructive Airway disease Chronic Obstructive Airway disease
(COAD)(COAD)
DEFINITIONDEFINITION
COPD is a disease state characterized by COPD is a disease state characterized by increase in resistance to airflow due to partial or increase in resistance to airflow due to partial or complete obstruction of airway at any level from complete obstruction of airway at any level from the trachea to respiratory bronchiole. Changes the trachea to respiratory bronchiole. Changes are usually irreversible esp. in chronic bronchitis are usually irreversible esp. in chronic bronchitis and emphysema.and emphysema.
- Predominant symptom; Dyspnoea- Predominant symptom; Dyspnoea
- Predominant cause; Smoking- Predominant cause; Smoking
Pulmonary function testsPulmonary function tests show : show :
1-Increased pulmonary resistance1-Increased pulmonary resistance
2- Limitation of maximal expiratory 2- Limitation of maximal expiratory
flow rates (reduced FEV1).flow rates (reduced FEV1).
1.1. EMPHYSEMAEMPHYSEMA
2.2. CHRONIC BRONCHITISCHRONIC BRONCHITIS
3.3. ASTHMA ASTHMA
4.4. BRONCHIECTASISBRONCHIECTASIS
Emphysema.Emphysema.
--Abnormal permanent enlargement of the Abnormal permanent enlargement of the
distal air spaces due to destruction of the distal air spaces due to destruction of the
alveolar walls and loss of respiratory tissue.alveolar walls and loss of respiratory tissue.
-“Obstruction” is caused by lack of elastic -“Obstruction” is caused by lack of elastic
recoil. recoil.
Etiology:Etiology:
1-1- Most common cause is Most common cause is smokingsmoking: produces : produces
combination of emphysema and chronic inflammation combination of emphysema and chronic inflammation
2- 2- GeneticGenetic deficiency of alpha1 antitrypsin (Pi locus on deficiency of alpha1 antitrypsin (Pi locus on
chromosome 14) ; alpha-1-antitrypsin deficiency chromosome 14) ; alpha-1-antitrypsin deficiency
produces almost pure emphysemaproduces almost pure emphysema

Pathogenesis:Pathogenesis:
1- 1- Protease-antiprotease imbalanceProtease-antiprotease imbalance ::
. Alpha1 antitrypsin present in serum, tissue . Alpha1 antitrypsin present in serum, tissue fluids, macrophagesfluids, macrophages
. Inhibitor of proteases (esp. elastase secreted . Inhibitor of proteases (esp. elastase secreted by neutrophils by neutrophils
during inflammation)during inflammation)
.Stimulus--TNF,IL8--Increased neutrophils--Release of .Stimulus--TNF,IL8--Increased neutrophils--Release of
proteases(elastase,proteinase-3,cathepsin-G)--Elastic lung tissue proteases(elastase,proteinase-3,cathepsin-G)--Elastic lung tissue
destructiondestruction
Pathogenesis
2- Oxidant-antioxidant imbalance:
Smoking--Free O2 radicals--Deplete Antioxidant in lung (superoxide dismutase, glutathione)—Damage of lung tissue
Types of EmphysemaTypes of Emphysema
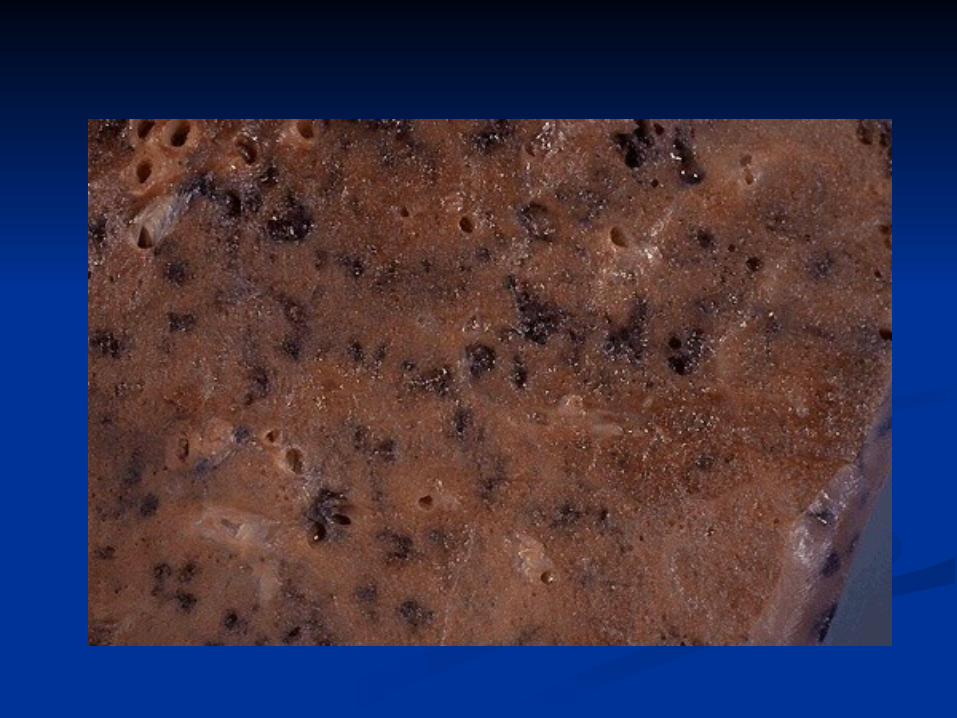
1-Centroacinar (Centrilobar) 1-Centroacinar (Centrilobar) EmphysemaEmphysema
-- -- Affects central (proximal) parts of the acini Affects central (proximal) parts of the acini
(respiratory bronchioles) but spares the distal (respiratory bronchioles) but spares the distal
alveoli.alveoli.
- More severe in upper lobes, especially apical - More severe in upper lobes, especially apical
segments segments
..

Causes:-Smoking-Coal dust

2-Panacinar (Panlobar) 2-Panacinar (Panlobar) EmphysemaEmphysema
-- -- Uniform enlargement of the acini in a lobule.Uniform enlargement of the acini in a lobule.
- May not necessarily involve entire lung- May not necessarily involve entire lung
- Predominantly lower lobes.- Predominantly lower lobes.
- - Alpha -1- antitrypsin deficiencyAlpha -1- antitrypsin deficiency is prototype. is prototype.
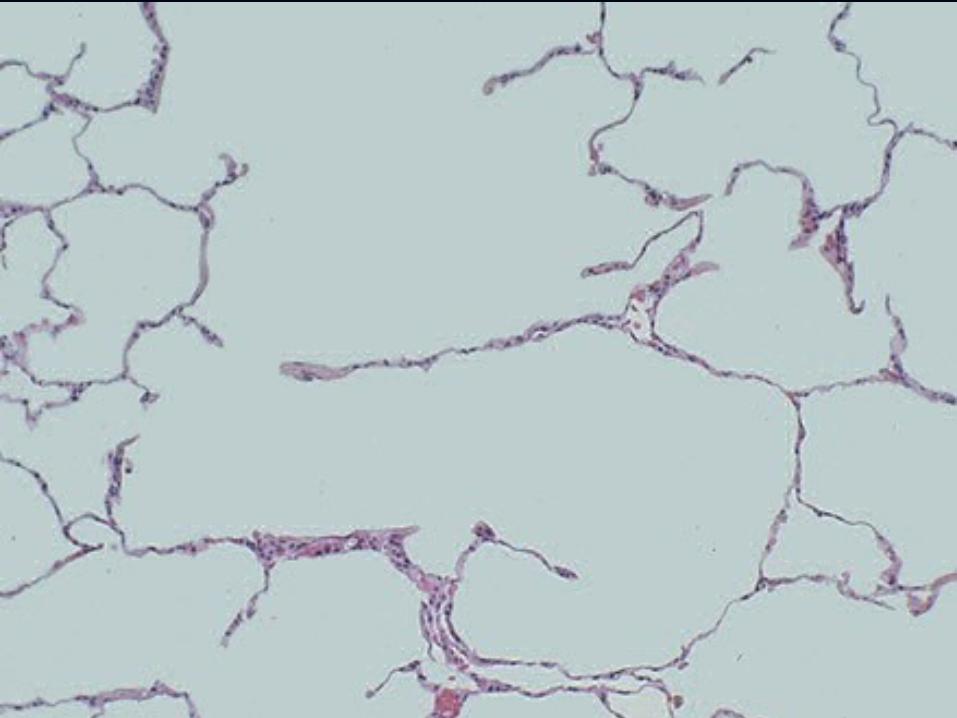
3-Paraseptal (Distal 3-Paraseptal (Distal Acinar) EmphysemaAcinar) Emphysema
-- -- Proximal acinus normal, distal part involvedProximal acinus normal, distal part involved
- Most prominent adjacent to pleura and along - Most prominent adjacent to pleura and along
the lobular connective tissue septa.the lobular connective tissue septa.
- Probably underlies - Probably underlies spontaneous spontaneous
pneumothoraxpneumothorax in young adults.in young adults.
4-Bullous Emphysema4-Bullous Emphysema
-- -- Any form of emphysema which produces Any form of emphysema which produces
large subpleural blebs or bullae (> 1cm).large subpleural blebs or bullae (> 1cm).
- Localized accentuation of any one of the - Localized accentuation of any one of the
type.type.

5-Interstitial Emphysema5-Interstitial Emphysema
Air penetration into the connective tissue Air penetration into the connective tissue
stroma of the :stroma of the :
- lung- lung
- mediastinum or- mediastinum or
- subcutaneous tissue. - subcutaneous tissue.
6-Compensatory 6-Compensatory “Emphysema”“Emphysema”
- - Dilatation of alveoli in response to loss of Dilatation of alveoli in response to loss of
lung substance elsewherelung substance elsewhere..
- - Actually hyperinflation since no Actually hyperinflation since no
destruction of septal walls.destruction of septal walls.
7-Senile “Emphysema”7-Senile “Emphysema”
- - Change in geometry of lung with larger Change in geometry of lung with larger
alveolar ducts and smaller alveoli.alveolar ducts and smaller alveoli.
- No loss of lung tissue; hence not really - No loss of lung tissue; hence not really
an emphysema.an emphysema.
Chronic BronchitisChronic Bronchitis
- - Clinical definitionClinical definition: persistent cough with : persistent cough with
sputum production for at least three months in at sputum production for at least three months in at
least two consecutive years.least two consecutive years.
- Can occur with or without evidence of airway - Can occur with or without evidence of airway
obstruction obstruction
- - SmokingSmoking is the most important cause. is the most important cause.
::
Basic Mechanism: Basic Mechanism: Hypersecretion of mucusHypersecretion of mucus HistologyHistology
-Increased numbers of goblet cells in small airways as -Increased numbers of goblet cells in small airways as
well as large airways.well as large airways.
-Increased size of submucosal glands in large airways -Increased size of submucosal glands in large airways
(Reid index: ratio of thickness of mucosal glands to (Reid index: ratio of thickness of mucosal glands to
thickness of wall between epithelium and cartilage)thickness of wall between epithelium and cartilage)
-Peribronchiolar chronic inflammation.-Peribronchiolar chronic inflammation.

BronchiectasisBronchiectasis
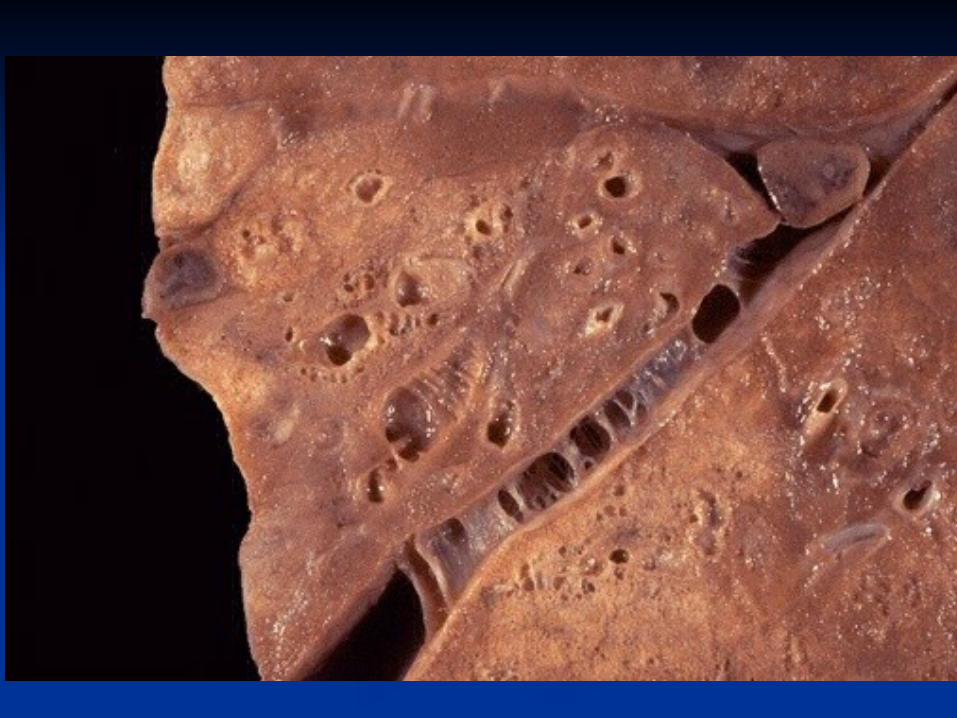
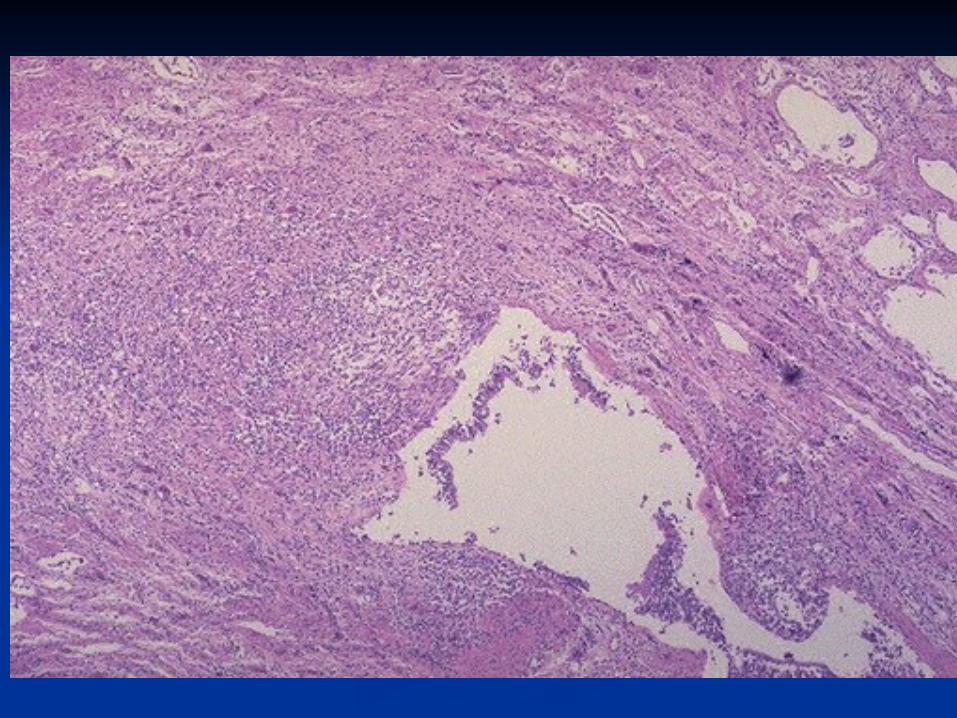
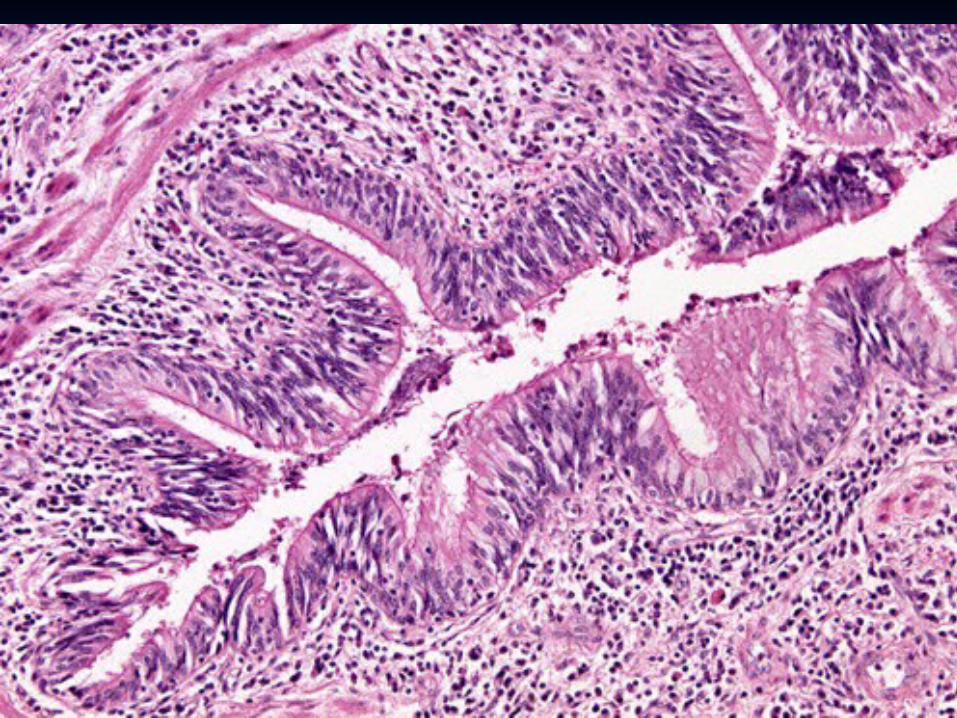
- - Permanent abnormal dilation of bronchi and Permanent abnormal dilation of bronchi and
bronchioles, bronchioles,
- Usually associated with chronic necrotizing - Usually associated with chronic necrotizing
inflammation inflammation
- Patients have fever, cough, foul–smelling sputum.- Patients have fever, cough, foul–smelling sputum.
- More common in left lung, lower lobes.- More common in left lung, lower lobes.


Causes:Causes:
Obstruction (tumor, mucus) Obstruction (tumor, mucus)
CongenitalCongenital
Intralobar sequestration Intralobar sequestration
Cystic fibrosisCystic fibrosis
Immotile cilia syndrome Immotile cilia syndrome
Necrotizing pneumoniaNecrotizing pneumonia
Kartaganer’s SyndromeKartaganer’s Syndrome

AsthmaAsthma
- - Increased responsiveness of Increased responsiveness of
tracheobronchial tree to various stimuli, tracheobronchial tree to various stimuli,
leading to paroxysmal airway constrictionleading to paroxysmal airway constriction
- Unremitting attacks (status asthmaticus) - Unremitting attacks (status asthmaticus)
can be fatal.can be fatal.
Etiology :Etiology :
1- Extrinsic Factors (atopic, allergic); most 1- Extrinsic Factors (atopic, allergic); most
commoncommon
2- Intrinsic Factors (idiosyncratic); now 2- Intrinsic Factors (idiosyncratic); now
recognize mixed.recognize mixed.
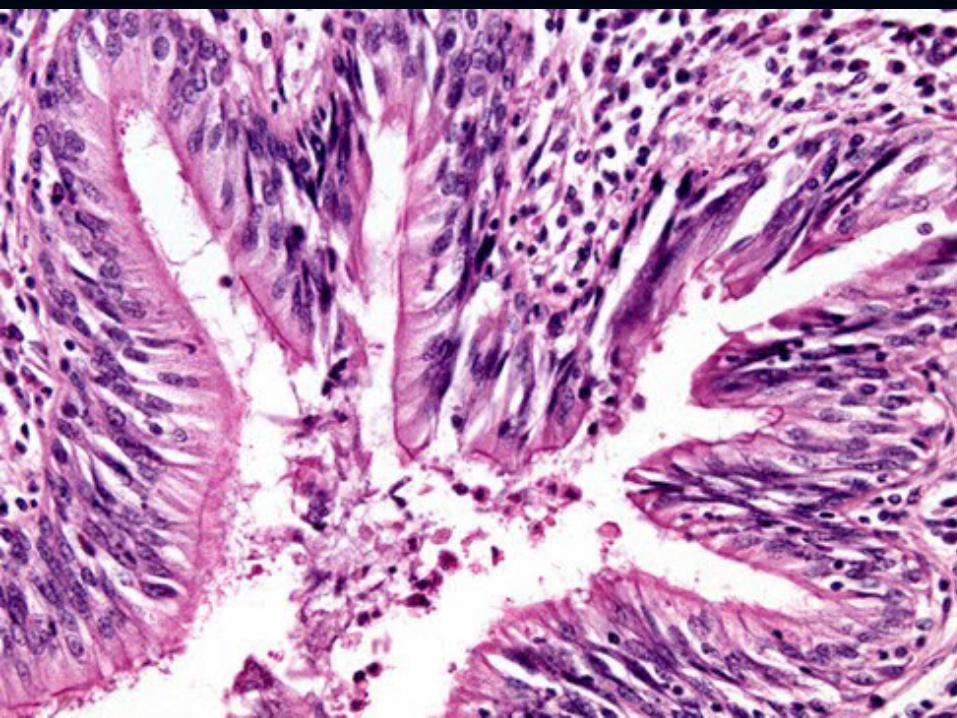
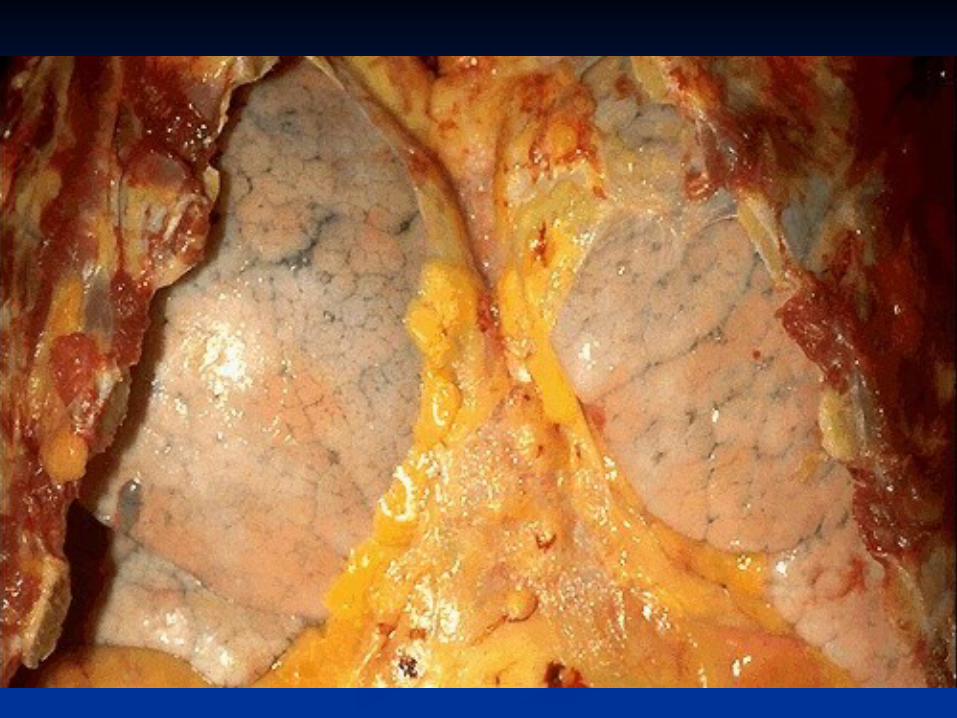
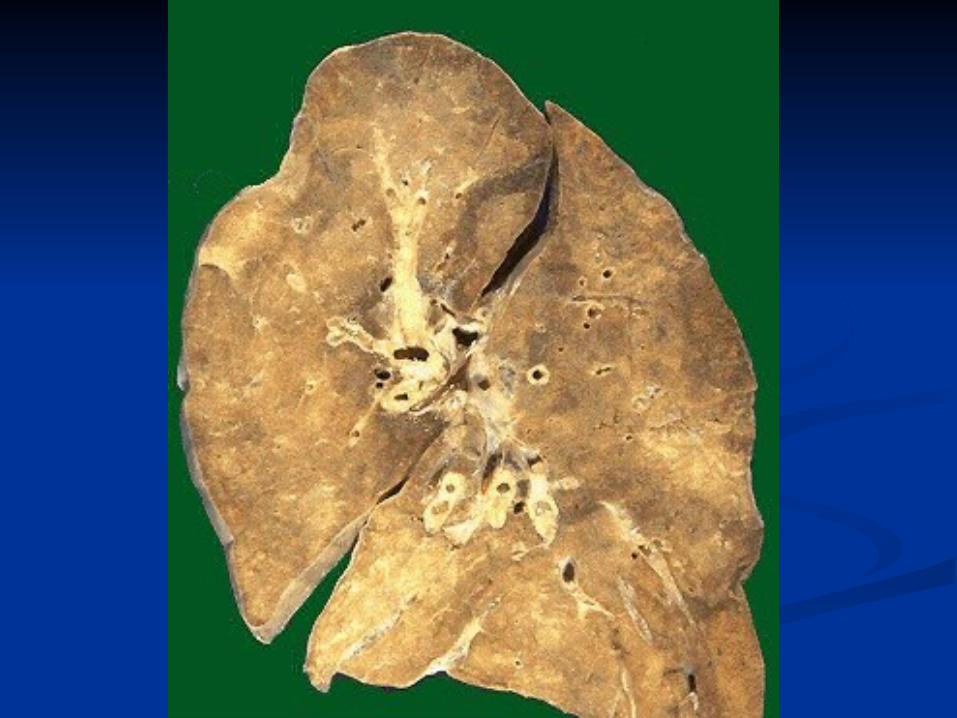
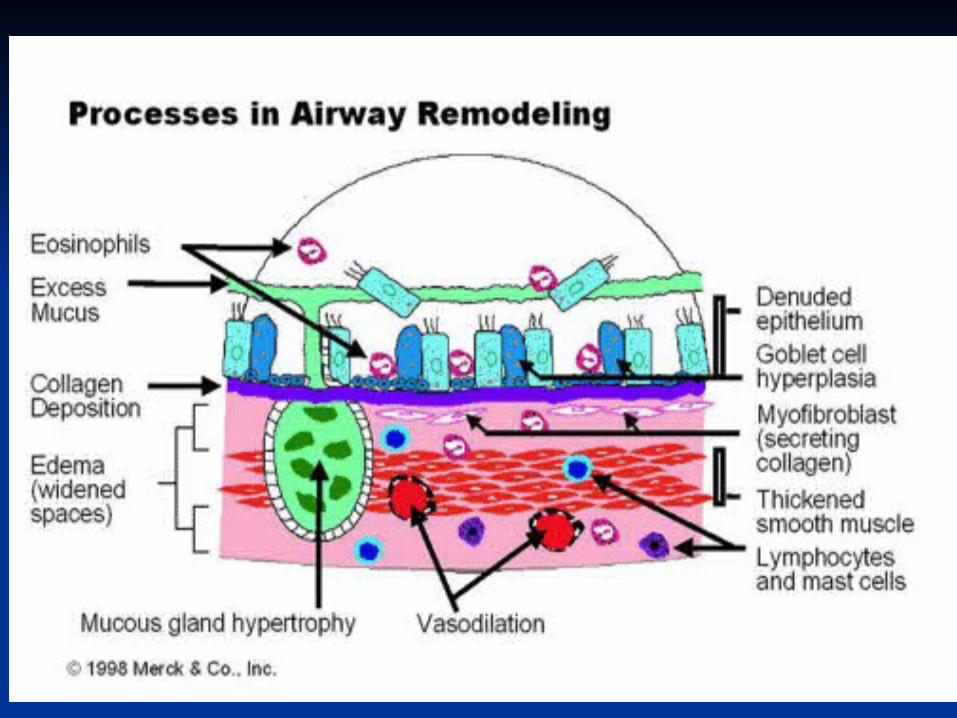
Basic MechanismBasic Mechanism
- Bronchial plugging by thick mucous plugs - Bronchial plugging by thick mucous plugs
containing eosinophils, whorls of shed epithelium containing eosinophils, whorls of shed epithelium
(Curschmann’s spirals), and Charcot – Leyden (Curschmann’s spirals), and Charcot – Leyden
crystals (Eosinophil membrane protein); crystals (Eosinophil membrane protein);
- Distal air- spaces become over distended.- Distal air- spaces become over distended.


Histology:Histology:
-Thick basement membrane-Thick basement membrane
-Edema and infiltration of the bronchial walls by -Edema and infiltration of the bronchial walls by
inflammatory cells with prominence of inflammatory cells with prominence of
eosinophils, eosinophils,
- Hypertrophy of bronchial wall muscle.- Hypertrophy of bronchial wall muscle.
Therapeutic agentsTherapeutic agents are aimed at increasing are aimed at increasing
cAMP levels either by :cAMP levels either by :
- increasing production (ß-agonists, e.g - increasing production (ß-agonists, e.g
epinephrine) orepinephrine) or
- decreasing degradation (Methyl xanthines, e.g - decreasing degradation (Methyl xanthines, e.g
theophylline). theophylline).
- Cromolyn sodium prevents mast cell - Cromolyn sodium prevents mast cell
degranulation. degranulation.
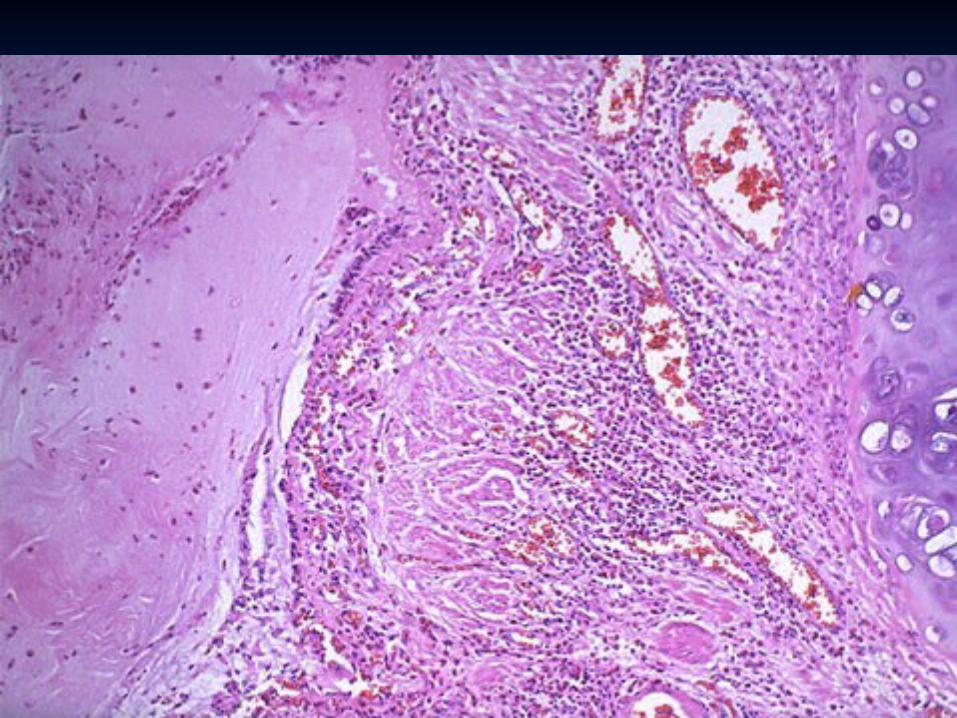
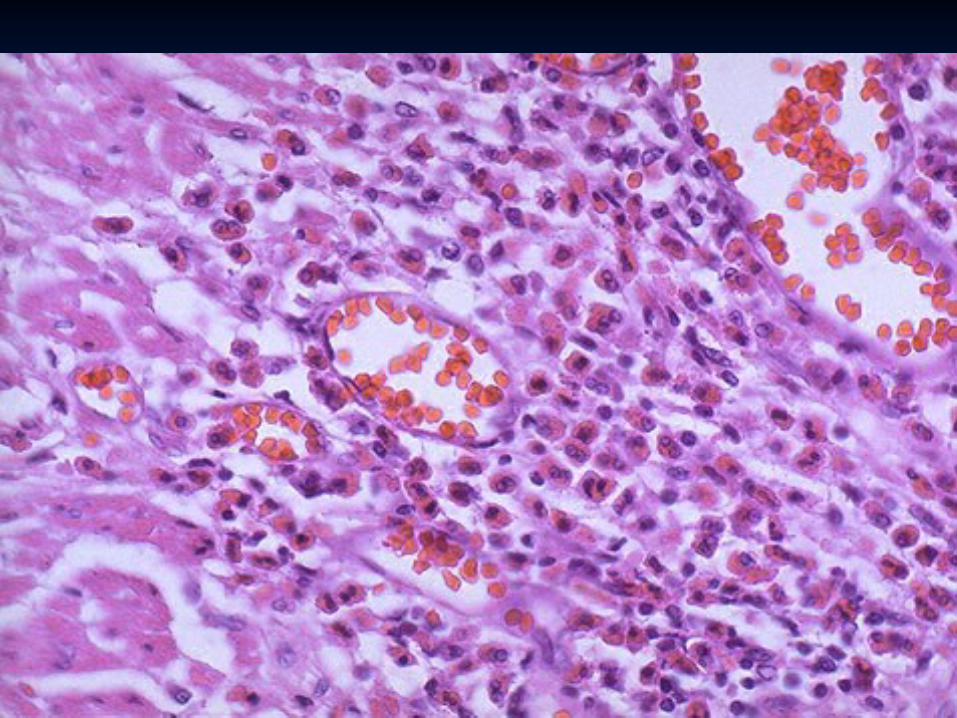
Allergic Allergic Bronchopulmonary Bronchopulmonary
Aspergillosis Aspergillosis
Occur in chronic asthmatics; hypersensitivity to non – Occur in chronic asthmatics; hypersensitivity to non –
invasive Aspergillus.invasive Aspergillus.
Bronchocentric granulomatous inflammation, mucus Bronchocentric granulomatous inflammation, mucus
impaction of bronchi, eosinophilic pneumoniaimpaction of bronchi, eosinophilic pneumonia..
Distinctive promixal bronchiectasis (?Pathgnomonic)Distinctive promixal bronchiectasis (?Pathgnomonic)
Burden of AsthmaBurden of Asthma
Prevalence increasing in developed countries Prevalence increasing in developed countries more than developing or underdeveloped more than developing or underdeveloped countries affecting 10 -15% of population.countries affecting 10 -15% of population.
The number of children with asthma has The number of children with asthma has increased six-fold in the last 25 yearsincreased six-fold in the last 25 years
Between 100 and 150 million people around Between 100 and 150 million people around the globe the globe
5.1 million people in the UK have asthma5.1 million people in the UK have asthma In South Asia (including Pakistan) rough In South Asia (including Pakistan) rough
estimates indicate a prevalence of between estimates indicate a prevalence of between 10% and 15% 10% and 15%
Burden of AsthmaBurden of Asthma
World-wide, the economic costs World-wide, the economic costs associated with asthma are estimated associated with asthma are estimated to exceed those of TB and HIV/AIDS to exceed those of TB and HIV/AIDS combined. combined.
In the United States, for example, In the United States, for example, annual asthma care costs (direct and annual asthma care costs (direct and indirect) exceed US$6 billion. indirect) exceed US$6 billion.
At present Britain spends about US$1.8 At present Britain spends about US$1.8 billion on health care for asthma and billion on health care for asthma and because of days lost through illness because of days lost through illness
Burden of AsthmaBurden of Asthma
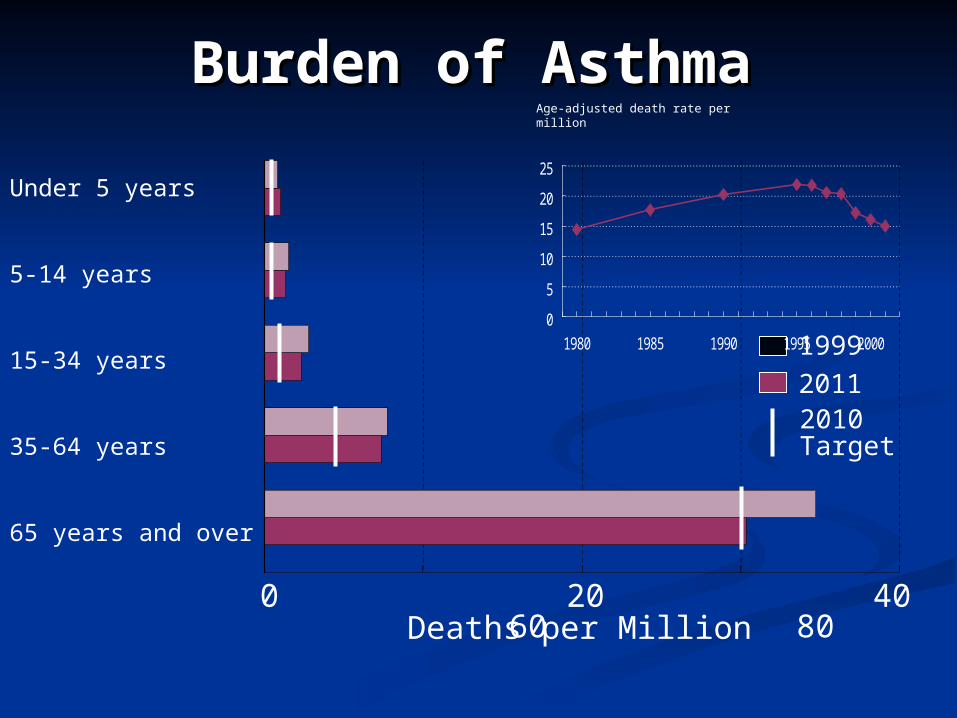
0 20 40 60 80 Deaths per Million
1999
20112010Target
0
5
10
15
20
25
1980 1985 1990 1995 2000
Age-adjusted death rate per million
Under 5 years
5-14 years
15-34 years
35-64 years
65 years and over
CLASSIFICATION OF CLASSIFICATION OF ASTHMAASTHMA
EXTRINSICEXTRINSICImplying a definite external causeImplying a definite external causeAtopic individualsAtopic individualsPositive skin prick testPositive skin prick testMore common More common Early onset in childhoodEarly onset in childhood INTRINSIC OR CRYPTOGENICINTRINSIC OR CRYPTOGENICLate onset (middle age)Late onset (middle age)
Etiology and Etiology and PathogenesisPathogenesis
AllergyAllergy Airway hyperresponsivenessAirway hyperresponsiveness Genetic factorsGenetic factors Asthma triggersAsthma triggers
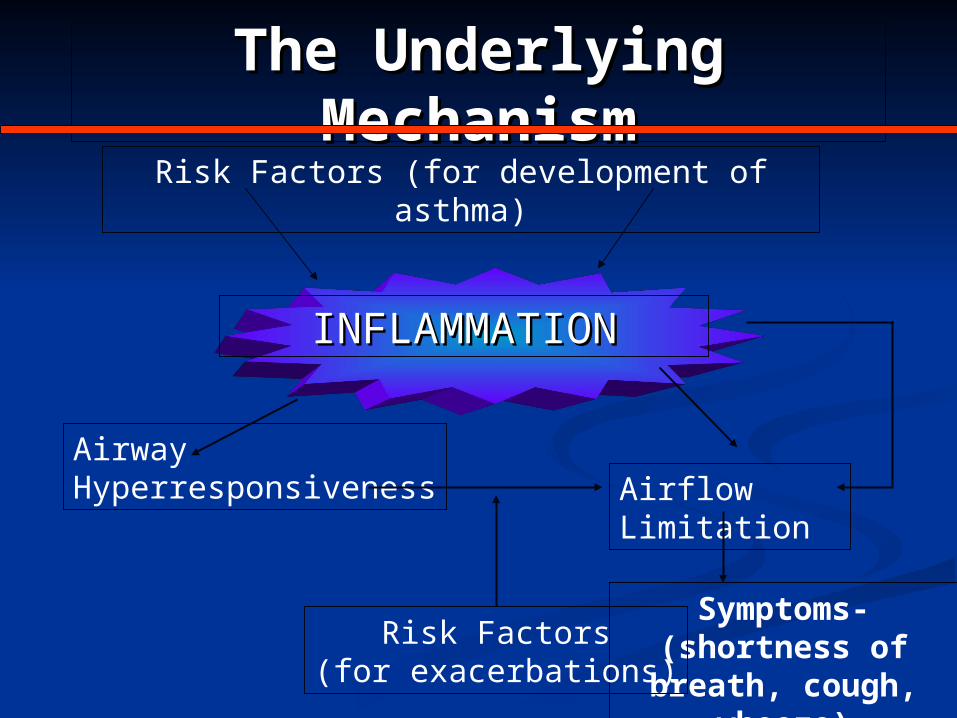
The Underlying MechanismThe Underlying Mechanism
INFLAMMATIONINFLAMMATION
Risk Factors (for development of asthma)
AirwayHyperresponsiveness Airflow
Limitation
Symptoms- (shortness of breath,
cough, wheeze)
Risk Factors(for exacerbations)
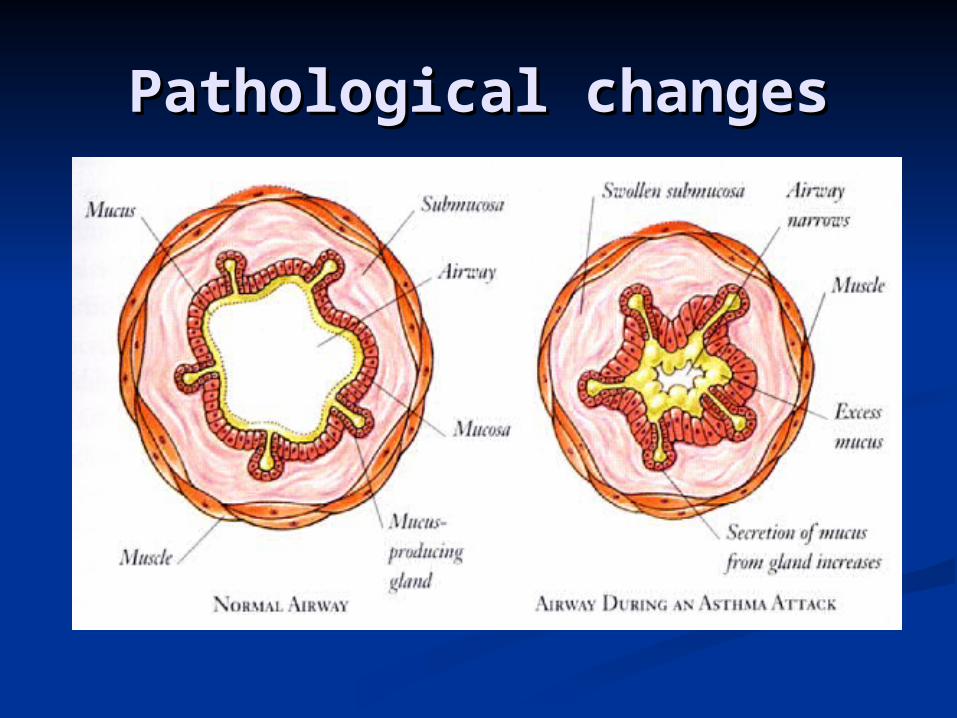
Pathological changesPathological changes
Genetic FactorsGenetic Factors
Candidate genes on chromosome Candidate genes on chromosome 5q31-335q31-33
(IL4 GENE CLUSTER)(IL4 GENE CLUSTER)
Responsible for production of Responsible for production of cytokines ,IL3,IL4 ,IL9 ,IL13, GM-cytokines ,IL3,IL4 ,IL9 ,IL13, GM-CSFCSF
Gene A
Gene B
Gene D
Gene E
Gene CAtopysusceptible
Asthmasusceptible
Asthma triggersAsthma triggers Indoor allergens Outdoor allergens Occupational
sensitizers Tobacco smoke Air Pollution Respiratory
Infections Parasitic infections
Socioeconomic factors Family size Diet and drugs Obesity Exercise Exercise Acid refluxAcid reflux
Burden of COPD
The global burden of COPD will increase enormously over the foreseeable future as the toll from tobacco use in developing countries becomes apparent.
In UK and USA COPD occurs in 18% male smokers14% female smokers6-7% those who have never smoked
Direct and Indirect Costs of COPD, (US $ Billions)
Direct Medical Cost: $18.0
Total Indirect Cost: $ 14.1
Mortality related IDC 7.3 Morbidity related IDC 6.8
Total Cost $32.1
Risk Factors for COPD
Host Factors Genes (e.g. alpha1-antitrypsin
deficiency) Hyperresponsiveness Lung growthExposure Tobacco smoke Occupational dusts and chemicals Infections Socioeconomic status
Pathogenesis of COPD
NOXIOUS AGENT(tobacco smoke, pollutants, occupational agent)
Genetic factors
Respiratory infection
Other
COPD
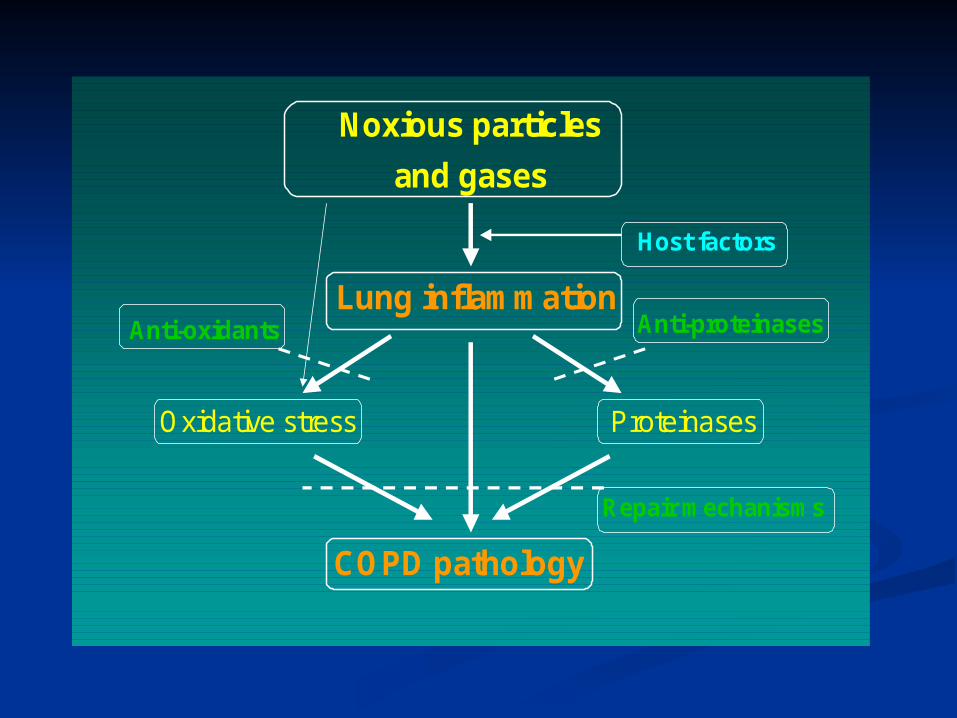
Noxious particles
and gases
Lung inflammation
Host factors
COPD pathology
ProteinasesOxidative stress
Anti-proteinasesAnti-oxidants
Repair mechanisms
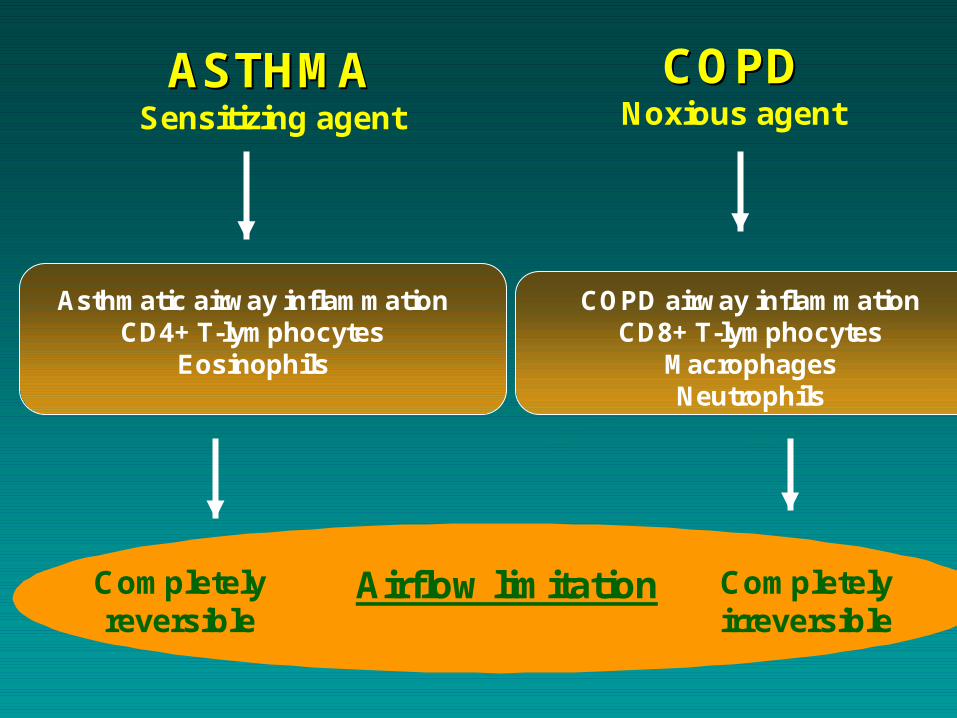
ASTHMAASTHMASensitizing agent
COPDCOPDNoxious agent
Asthmatic airway inflammationCD4+ T-lymphocytes
Eosinophils
COPD airway inflammationCD8+ T-lymphocytes
MacrophagesNeutrophils
Airflow limitationCompletelyreversible
Completelyirreversible
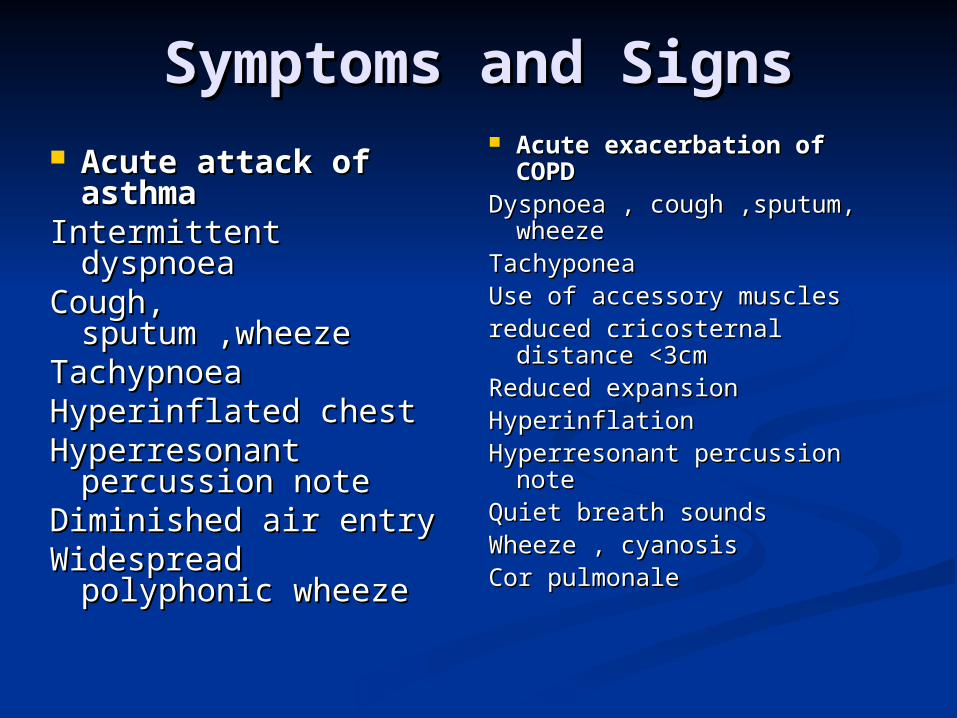
Symptoms and SignsSymptoms and Signs Acute attack of Acute attack of
asthmaasthmaIntermittent dyspnoeaIntermittent dyspnoeaCough, Cough,
sputum ,wheezesputum ,wheezeTachypnoeaTachypnoeaHyperinflated chestHyperinflated chestHyperresonant Hyperresonant
percussion notepercussion noteDiminished air entryDiminished air entryWidespread Widespread
polyphonic wheezepolyphonic wheeze
Acute exacerbation of Acute exacerbation of COPDCOPD
Dyspnoea , cough ,sputum, Dyspnoea , cough ,sputum, wheezewheeze
TachyponeaTachyponeaUse of accessory musclesUse of accessory musclesreduced cricosternal distance reduced cricosternal distance
<3cm<3cmReduced expansionReduced expansionHyperinflationHyperinflationHyperresonant percussion Hyperresonant percussion
notenoteQuiet breath soundsQuiet breath soundsWheeze , cyanosisWheeze , cyanosisCor pulmonaleCor pulmonale
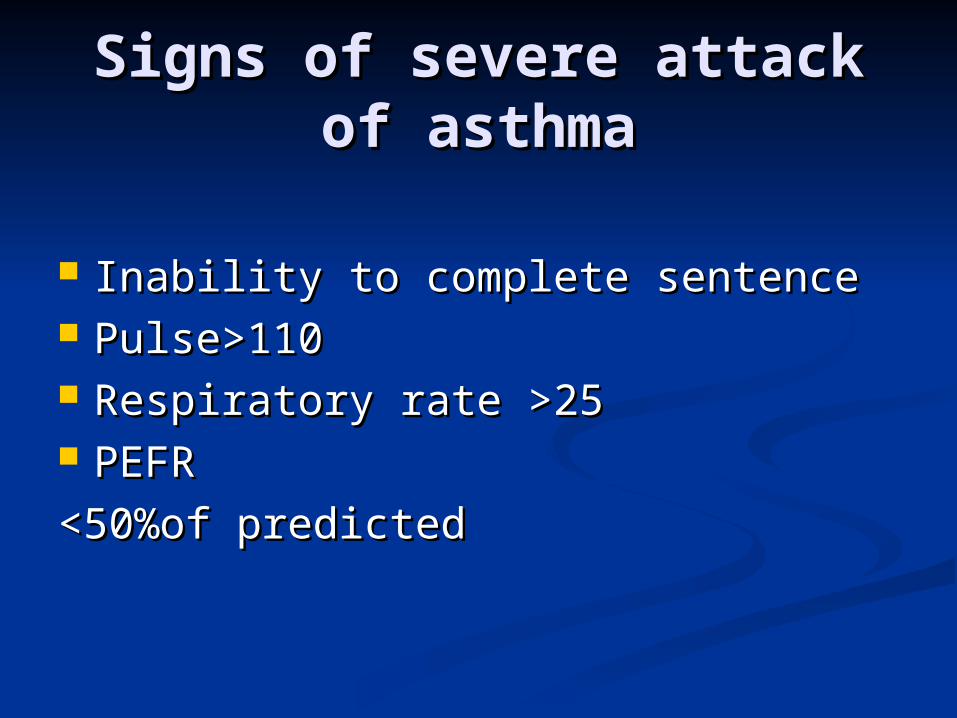
Signs of severe attack of Signs of severe attack of asthmaasthma
Inability to complete sentenceInability to complete sentence Pulse>110Pulse>110 Respiratory rate >25Respiratory rate >25 PEFRPEFR
<50%of predicted<50%of predicted
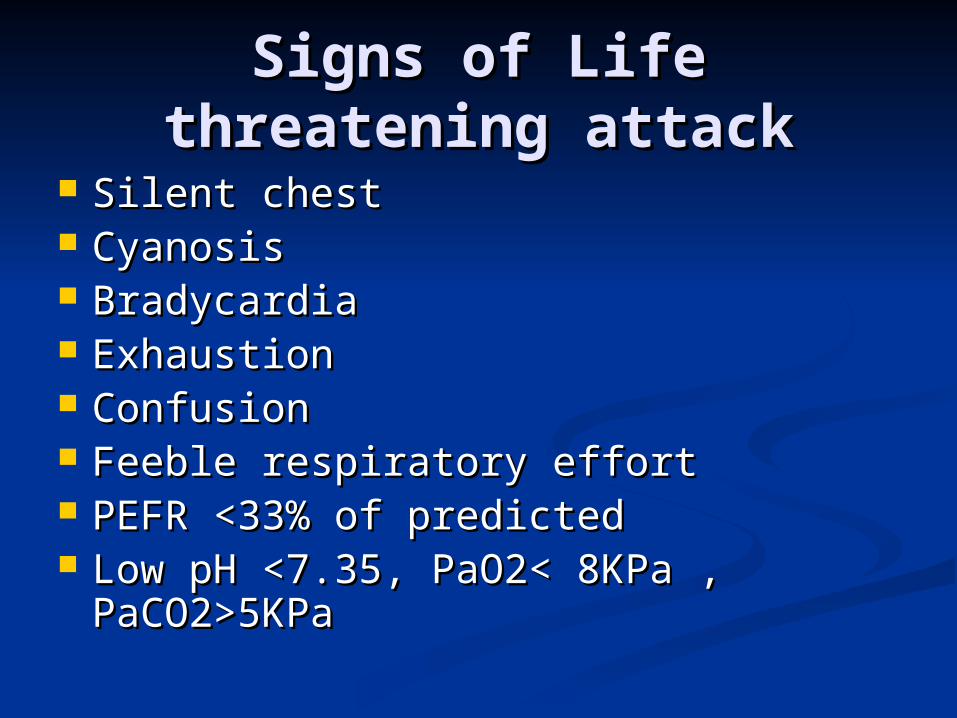
Signs of Life threatening Signs of Life threatening attackattack
Silent chest Silent chest CyanosisCyanosis BradycardiaBradycardia ExhaustionExhaustion ConfusionConfusion Feeble respiratory effortFeeble respiratory effort PEFR <33% of predictedPEFR <33% of predicted Low pH <7.35, PaO2< 8KPa , Low pH <7.35, PaO2< 8KPa ,
PaCO2>5KPaPaCO2>5KPa
Investigations for acute Investigations for acute attack of asthmaattack of asthma
Full Blood CountFull Blood Count Urine Complete and ElectrolytesUrine Complete and Electrolytes PEFR (pt may be too ill to perform it PEFR (pt may be too ill to perform it
well)well) Arterial Blood GasesArterial Blood Gases Pulse oximetryPulse oximetry ECG ECG CXRCXR
Investigations for Acute Investigations for Acute Exacerbation of COPDExacerbation of COPD
Full Blood CountFull Blood Count Urine Complete and ElectrolytesUrine Complete and Electrolytes PEFR (pt may be too ill to perform it well)PEFR (pt may be too ill to perform it well) Arterial Blood GasesArterial Blood Gases Pulse oximetryPulse oximetry ECG ECG CXRCXR Blood cultures (if Pyrexial)Blood cultures (if Pyrexial) Sputum for cultureSputum for culture
Differential DiagnosisDifferential Diagnosis
AsthmaAsthma COPDCOPD Pneumothorax Pneumothorax Pulmonary edemaPulmonary edema Upper respiratory tract obstructionUpper respiratory tract obstruction Pulmonary embolusPulmonary embolus AnaphylaxisAnaphylaxis
Management PlanManagement Plan
Immediate management to stabilize Immediate management to stabilize the patientthe patient
Long term management of diseaseLong term management of disease
Prevention of further attacksPrevention of further attacks
Immediate management of Immediate management of acute asthmatic attackacute asthmatic attack
B2 AgonistsB2 Agonists
Salbutamol 5mg or Terbutaline 10mg Salbutamol 5mg or Terbutaline 10mg nebulized with O2nebulized with O2
(se;tacchycardia,tremor,hypokalemia,ar(se;tacchycardia,tremor,hypokalemia,arrythmia)rythmia)
CorticosteroidsCorticosteroids
Hydrocortisone 200 mg iv or Hydrocortisone 200 mg iv or Prednisolone 30 mg oral (both if very Prednisolone 30 mg oral (both if very ill)ill)
Immediate management of Immediate management of acute asthmatic attackacute asthmatic attack
Additional management in Life Additional management in Life threatening attackthreatening attack
Nebulize with Anti cholinergics Nebulize with Anti cholinergics (Ipratropium 0.5 mg add to B2agonist)(Ipratropium 0.5 mg add to B2agonist)
Aminophylline Aminophylline
250 mg (5mg/kg) I/V over 20 mins250 mg (5mg/kg) I/V over 20 mins I/V B2 agonistsI/V B2 agonists
Salbutamol or Terbutaline 0.25mg over 10 Salbutamol or Terbutaline 0.25mg over 10 minsmins
Effects of Corticosteroids in Effects of Corticosteroids in Acute Asthma Acute Asthma
Systemic Systemic CorticosteroidsCorticosteroids
Anti-inflammatoryAnti-inflammatory Late improvement in Late improvement in
outcomes (> 6 hrs)outcomes (> 6 hrs) Corticosteroids Corticosteroids
induce induce transcriptional transcriptional effects synthesis of effects synthesis of new proteinsnew proteins
Inhaled CorticosteroidsInhaled Corticosteroids TopicalTopical Early improvement in Early improvement in
outcomes (< 3 h)outcomes (< 3 h) Corticosteroids up-Corticosteroids up-
regulating regulating postsynaptic postsynaptic adrenergic receptors adrenergic receptors airway mucosa, airway mucosa, vasoconstriction vasoconstriction decrease airway decrease airway mucosal blood flow, mucosal blood flow, mucosal mucosal decongestiondecongestion
Complications Complications
Respiratory failureRespiratory failureType I continuous O2 Type I continuous O2 Type II controlled O2Type II controlled O2 Intubation and ventilation Intubation and ventilation Cor pulmonaleCor pulmonale Pneumothorax (ruptured bulla …Pneumothorax (ruptured bulla …
bullous lung disease, Indication of bullous lung disease, Indication of surgery)surgery)
Chest infection (pneumonia)Chest infection (pneumonia) PolycythemiaPolycythemia
ComplicationsComplications
Respiratory failureRespiratory failure Treatment options;Treatment options; Noninvasive Positive Pressure VentilationNoninvasive Positive Pressure Ventilation
IntubationIntubation
Sedatives and Neuromuscular BlockersSedatives and Neuromuscular Blockers
PREVENTIONPREVENTION
Elimination of risk factorsElimination of risk factors Patient education and informationPatient education and information Advice on not missing the doseAdvice on not missing the dose Proper management planProper management plan Addition of mast cell stabilizers like Addition of mast cell stabilizers like
sodium cromoglycate and nedocromil sodium cromoglycate and nedocromil and leukotriene antagonists e.g; and leukotriene antagonists e.g; montelukast and zafirlukast to montelukast and zafirlukast to traditional therapytraditional therapy


















