32
Clinical Prediction Rules in Sports Medicine

Clinical Prediction Rules in Sports Medicine

Objectives
Define a clinical prediction rule Identify the three types of clinical prediction
rules Discuss the development of clinical prediction
rules Implement several clinical prediction rules for
one’s practice setting

What are Clinical Prediction Rules (CPRs)?
Evidence-based medicine Clinical decision making algorithm Increase sensitivity and specificity of clinical
exam Decrease use of unnecessary tests Decrease use of ineffective treatments
Glynn & Weisbach (2011)

Types of CPRs
Diagnostic Probability that a specific condition exists
Prognostic Likely outcome for patients with a specific
condition
Prescriptive Determine which patients will likely respond
favorably to a specific treatment or combination of treatments
Glynn & Weisbach (2011)

How are they developed?
4 levels of CPRs IV: rule has been developed and tested in a
specific population; predictor variables are selected
III: validation of the CPR in a patient sample; confirm predictor variables weren’t due to chance or errors within the study; new patients, new investigators
II: validated in a broad patient population I: demonstrated effectiveness in a varied
population on a large scale
Glynn & Weisbach (2011)
Development Example – NEXUS Protocol
Several studies defined 5 criteria that correlate with a low probability of c-spine injury after blunt trauma
Prospective study of more than 34,000 patients presenting to EDs after blunt trauma to validate findings
818 patients with positive imaging 8 of those 818 met NEXUS criteria and would not
be imaged based on CPR; only 2 were clinically significant findings
Hoffman et al. (2000)

Clinical Implications – NEXUS Protocol
False negative rate of 1 in 4000 12.6% reduction in c-spine radiographs Change in EMS protocols for spine boarding
Hoffman et al. (2000)

Diagnostic CPRs

Ottawa Ankle Rules (I)
Pain near the malleoli AND at least one of the following: Inability to bear weight immediately AND four steps in
the ED Tenderness anywhere along the distal 6 cm of either
malleoli
GET X-RAY
Leddy et al. (1998)

LE DVT - Wells Criteria (I)
Score Risk % Likelihood of DVT
0 points Low 6
1-2 points Medium 28
3 or more points
High 73
Riddle et al. (2005)

LE DVT (I) Predictor Variables Score Active cancer (treatment within last 6 months, current, or palliative)
1
Recent immobilization, paresis, paralysis 1 Major surgery in last month, or recently bedridden for at least 4 days
1
Local tenderness along path of deep vein 1 Edema of calf and thigh 1 Girth measure at 10cm distal to tibial tuberosity 3cm > contralateral measure
1
Pitting edema ipsilaterally 1 Superficial dilation of veins 1 Alternative diagnosis more or just as likely as DVT -2
Riddle et al. (2005)
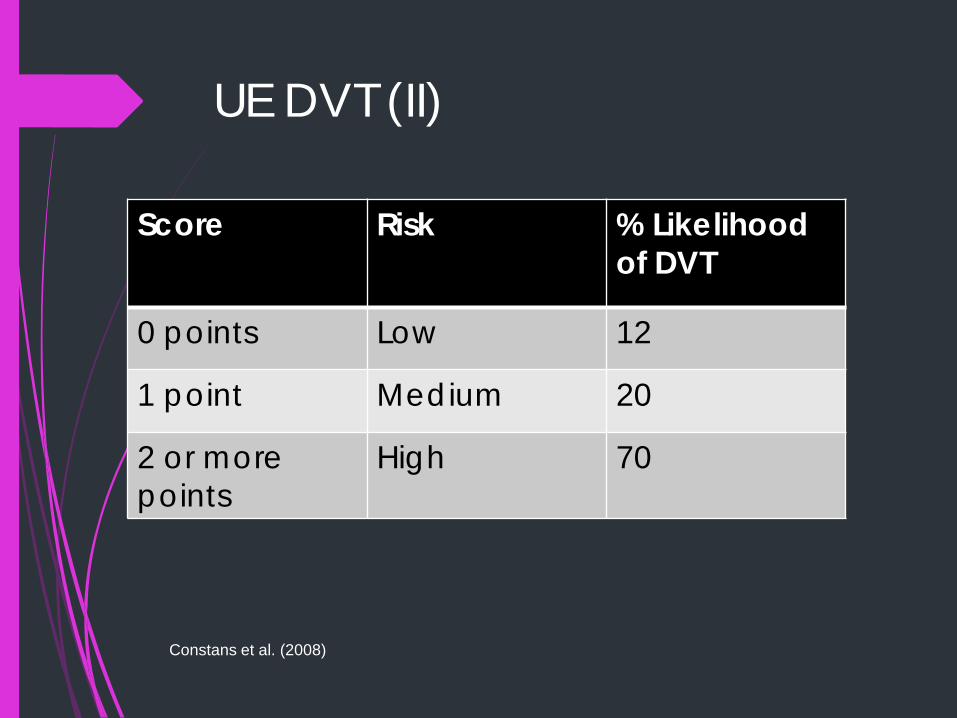
UE DVT (II)
Score Risk % Likelihood of DVT
0 points Low 12
1 point Medium 20
2 or more points
High 70
Constans et al. (2008)

UE DVT (II)
Predictor Variables Score Presence of a device in a vein (catheter, port,) or pacemaker
1
Pitting edema 1 Local UE pain 1
Alternative diagnosis more or just as likely as DVT
-1
Constans et al. (2008)

PE – Wells Score (II)
Score Risk % Likelihood of DVT
< 2 points Low 3.6 2-6 points Medium 20.5 6 or more points
High 66.7
Calisir et al. (2009)

PE (II)
Predictor Variables Score s/s of DVT (LE edema and TTP of deep veins, at minimum)
3
No other diagnosis likely 3 HR >100 1.5
Surgery or immobilization within 4 weeks 1.5 Previous PE/DVT 1.5 Hemoptysis 1
Active cancer (treatment within last 6 months, current, or palliative)
1
Calisir et al. (2009)
Cervical Radiculopathy (IV)
Predictor variables: Ipsilateral cervical rotation < 60 ULTT A (+) Cervical distraction test (+) Spurling’s A (+)
Sidebent to ipsilateral side
Three or more present, moderate likelihood of the condition being present
Wainner et al. (2003)

Subacromial Impingement (IV)
Predictor variables Hawkins-Kennedy (+) Painful arc Pain or weakness with ER strength testing
(elbow at side)
All three predictor variables present is a strong indicator for diagnosis
Park et al. (2005)

Full-Thickness RCT (IV)
Predictor variables Painful arc Pain or weakness with ER strength testing
(elbow at side) Drop arm (+)
All three predictor variables present is a strong indicator for diagnosis
Park et al. (2005)
SI Joint Pain (IV)
Predictor variables SI compression (+) SI distraction (+) Femoral shear (+) Sacral provocation (+) Gaenslen’s test (+) R Gaenslen’s test (+) L
At least three predictor variables present is a moderate indicator for diagnosis
Laslett et al. (2005)

Prognostic CPRs

Recovery with LBP (III)
Predictor variables Initial p! < 8/10 p! less than 6 days No more than 1 previous episode of LBP
All three predictor variables present Study participants received mobilization
therapy (95% non-thrust) and Voltaren 95% better at 12 weeks
p! 0-1/10 for 1 week
Hancock et al. (2009)

Interventional CPRs

Cervical Traction for Mechanical Neck Pain (IV)
Predictor variables 55 years or older Shoulder abduction test (+) ULTT A (+) Peripheral symptoms with A/P glides of C4-C7 Neck distraction test (+)
Three or more predictor variables indicates a moderate likelihood that traction and exercise will produced a perceived benefit
Raney et al. (2009)

MWM and Exercise for Lateral Epicondylitis (IV)
Predictor variables Under 49 y.o. Pain-free grip > 25# (ipsilateral) Pain-free grip < 76# (contralateral)
At least two predictors indicates a shift in likelihood that the condition will improve with 3 weeks of MWM and rehabilitation
Vicenzino et al. (2009)
Lumbar Manipulation for LBP - Success (II)
Predictor variables Peripheral pain proximal to the knee Symptoms no longer than 16 days Hypomobile l-spine Hip IR >35 on either side Fear Avoidance Belief Questionnaire (work
subscale) <19 At least four predictor variables indicates a
large increase in likelihood that function will improve by 50% within 2 tx
Hancock et al. (2008)

Joint Mobilization and Stretching for Lateral Ankle Sprain (IV)
Predictor variables Increased symptoms with standing Increased symptoms at end of day Navicular drop of at least 5 mm Hypomobile distal tib-fib
At least three predictor variables indicates a moderate likelihood of improvement within 2 tx
Whitman et al. (2009)
Bibliography Calisir, C., Yavas, U. S., Ozkan, I. R., Alatas, F., Cevik, A., Ergun, N., & Sahin, F. (2009). Performance of the Wells and Revised Geneva scores for predicting pulmonary embolism. Eur J Emerg Med, 16, 49-52.
Constans, J., Salmi, L. R., Sevestre-Pietri, M. A., Perusat, S., Nguon, M., Degeilh, M., … Bosson, J. L. (2008). A clinical prediction score for upper extremity deep venous thrombosis. Throm Haem, 99, 202- 207.
Glynn, P. E., & Weisbach, P. C. (2011). Clinical prediction rules. A physical therapy reference manual. Boston: Jones and Bartlett Publishers.
Hancock, M. J., Maher, C. G., Latimer, J., Herbert, R. D., & McAuley, J. H. (2009). Can rate of recovery be predicted in patients with acute low back pain? Development of a clinical prediction rule. Eur J Pain, 13, 51-55.

Bibliography Hancock, M. J., Maher, C. G., Latimer, J., Herbert, R. D., & McAuley, J. H. (2008). Independent evaluation of a clinical prediction rule for spinal manipulative therapy. A randomised controlled trial. Eur Spine J, 17, 936-943.
Hoffman, J. R., Mower, W. R., Wolfson, A. B., Todd, K. H., & Zucker, M. I. (2000). Validity of a set of clinical criteria to rule out injury to the cervical spine in patients with blunt trauma. NEJM, 343, 94- 99.
Laslett, M., Aprill, C. N., McDonald, B., & Young, S. B. (2005). Diagnosis of sacroiliac joint pain. Validity of individual provocation tests and composites of tests. J Man Ther, 10, 207- 218.
Leddy, J. J., Smolinski, R. J., Lawrence, J., Snyder, J. L., & Priore, R. L. (1998). Prospective evaluation of the Ottawa Ankle Rules in a university sports medicine center. AJSM, 26, 158-165.

Bibliography Park, H. B., Yokota, A., Gill, H. S., Rassi, G. E., & McFarland, E. G. (2005). Diagnostic accuracy of clinical tests for the different degrees of subacromial impingement syndrome. JBJS Am, 87-A, 1446-1455.
Raney, N. H., Petersen, E. J., Smith, T. A., Cowan, J. E., Rendeiro, D. G., Deyle, G. D. & Childs, J. D. (2009). Development of a clinical prediction rule to identify patients with neck pain likely to benefit from cervical traction and exercise. Eur Spine J, 18, 382- 391.
Riddle, D. L., Hoppener, M. R., Kraaijenhagen, R. A., Anderson, J., & Wells, P. S. (2005). Preliminary validation of clinical assessment for deep vein thrombosis in orthopaedic outpatients. Clin Orthop Rel Res, 432, 252-257.

Bibliography Vicenzino, B., Smith, D., Cleland, J., & Bisset, L. (2009). Development of a clinical prediction rule to identify initial responders to mobilisation with movement and exercise for lateral epicondylalgia. J Man Ther, 14, 550-554.
Wainner, R. S., Fritz, J. M., Irrgang, J. J., Boninger, M. L., Delitto, A., & Allison, S. (2003). Reliability and diagnostic accuracy of the clinical examination and patient self-report measures for cervical radiculopathy. Spine, 28, 52-62.
Whitman, J. M., Cleland, J. A., Mintken, P., Keirns, M., Bieniek, M. L., Albin, S. R., … McPoil, T. G. (2009). Predicting short-term response to thrust and nonthrust manipulation and exercise in patients post inversion ankle sprain. J Orthop Sports Phys Ther, 39, 188- 200.

THANK YOU!




![Arthroscopic Subacromial Decompression for Small and ...nosis of the subacromial impingement is usually clinical and based on the provocative clinical tests [8] -[10] , but occasionally](https://static.documents.pub/doc/80x56/60c199bcd9b91479387e740d/arthroscopic-subacromial-decompression-for-small-and-nosis-of-the-subacromial.jpg)













