Damage Control in the Damage Control in the Surgical Patient Surgical Patient Christine S. Cocanour, MD, FACS, FCCM Christine S. Cocanour, MD, FACS, FCCM Professor of Surgery Professor of Surgery Division of Trauma and Emergency Surgery Division of Trauma and Emergency Surgery UC Davis Medical Center UC Davis Medical Center
Transcript
Damage Control in the Damage Control in the Surgical PatientSurgical Patient
Christine S. Cocanour, MD, FACS, FCCMChristine S. Cocanour, MD, FACS, FCCMProfessor of SurgeryProfessor of Surgery
Division of Trauma and Emergency SurgeryDivision of Trauma and Emergency SurgeryUC Davis Medical CenterUC Davis Medical Center
Damage ControlDamage Control
Used in the Merchant Marine, maritime industry Used in the Merchant Marine, maritime industry and navies since the 1950s to describe the and navies since the 1950s to describe the emergency control of situations that may hazard emergency control of situations that may hazard the sinking of a ship.the sinking of a ship.US Navy defines it as “the capacity of a ship to absorb damage and maintain mission integrity”
Damage ControlDamage Control
USS Cole 12 October 2000
Aden, Yemen
Damage ControlDamage Control
Damage ControlDamage Controlin the Surgical Patientin the Surgical Patient
Control hemorrhage and contaminationControl hemorrhage and contamination
Definitive injury management and closureDefinitive injury management and closure
Evolution of Damage ControlEvolution of Damage Controlin the Surgical Patientin the Surgical Patient
1908 Pringle: compression and hepatic packing 1908 Pringle: compression and hepatic packing for portal venous hemorrhagefor portal venous hemorrhage
Ann Surg 1908; 48:541
Evolution of Damage ControlEvolution of Damage Controlin the Surgical Patientin the Surgical Patient
1913 Halsted: 1913 Halsted: guttaguttaperchapercha sheets to prevent sheets to prevent granulation tissue from granulation tissue from growing into gauze growing into gauze packingpacking
Evolution of Damage ControlEvolution of Damage Controlin the Surgical Patientin the Surgical Patient
After WWII through the Viet Nam War era:After WWII through the Viet Nam War era:Packing fell into disfavor with reports of Packing fell into disfavor with reports of necrosis, sepsis and hemorrhage. necrosis, sepsis and hemorrhage. Newer surgical techniques were thought to be Newer surgical techniques were thought to be betterbetter
Evolution of Damage ControlEvolution of Damage Controlin the Surgical Patientin the Surgical Patient
1963: 1963: ShaftanShaftan, et al: faster and better , et al: faster and better resuscitation and better treatment of wounds to resuscitation and better treatment of wounds to limit liver mortalitylimit liver mortality
CAPPELLETTI, R R, GLIEDMAN, M L, & CAPPELLETTI, R R, GLIEDMAN, M L, & SHAFTAN, G W. (1963). Injuries of the liver: a SHAFTAN, G W. (1963). Injuries of the liver: a review of 111 cases. review of 111 cases. J Trauma;J Trauma; 3:633:63
Evolution of Damage ControlEvolution of Damage Controlin the Surgical Patientin the Surgical Patient
1979 1979 CalneCalne, et al: liver hemorrhage temporarily , et al: liver hemorrhage temporarily controlled with gauze packing enabling safe controlled with gauze packing enabling safe transfer and definitive management at a more transfer and definitive management at a more appropriate institutionappropriate institution
Evolution of Damage ControlEvolution of Damage Controlin the Surgical Patientin the Surgical Patient
1976 Lucas, CE and 1976 Lucas, CE and LedgerwoodLedgerwood, AM, AMProspective evaluation of Prospective evaluation of hemostatichemostatic techniques techniques for liver injuries for liver injuries J TraumaJ Trauma 16:44216:442
Evolution of Damage ControlEvolution of Damage Controlin the Surgical Patientin the Surgical Patient
1981 Feliciano DV, Mattox KL, Jordan, GL 1981 Feliciano DV, Mattox KL, Jordan, GL JrJr““IntraIntra--abdominal packing for control of hepatic abdominal packing for control of hepatic hemorrhage: a reappraisalhemorrhage: a reappraisal””
90% survival rate in 10 patients with 90% survival rate in 10 patients with perihepaticperihepaticpackingpacking“…“…intraintra--abdominal packing for control of abdominal packing for control of exsanguinatingexsanguinating hepatic hemorrhage appears to be a hepatic hemorrhage appears to be a lifesaving maneuver in highly selected patients in whom lifesaving maneuver in highly selected patients in whom coagulopathiescoagulopathies, hypothermia, and acidosis, hypothermia, and acidosis make make further surgical efforts likely to increase hemorrhage.further surgical efforts likely to increase hemorrhage.””
Evolution of Damage ControlEvolution of Damage Controlin the Surgical Patientin the Surgical Patient
1983 Stone, et al: 1983 Stone, et al: coagulopathycoagulopathy contributed to contributed to poor outcomes. Proposed truncation of poor outcomes. Proposed truncation of laparotomylaparotomy, reversal of , reversal of coagulopathycoagulopathy and then and then return to the OR for definitive surgical repairreturn to the OR for definitive surgical repair
Ann Surg. 1983 May; 197(5): 532
Evolution of Damage ControlEvolution of Damage Controlin the Surgical Patientin the Surgical Patient
Evolution of Damage ControlEvolution of Damage Controlin the Surgical Patientin the Surgical Patient
Burch, et al 1992Burch, et al 1992
Ann Surg. 1992 May; 215(5): 476
Evolution of Damage ControlEvolution of Damage Controlin the Surgical Patientin the Surgical Patient
1993 1993 RotondoRotondo and the U Penn group coined and the U Penn group coined ““damage control damage control laparotomylaparotomy””
20 year review: mortality 52%, morbidity 40%20 year review: mortality 52%, morbidity 40%
Damage ControlDamage Controlin the Surgical Patientin the Surgical Patient
Trauma, general surgery, vascular Trauma, general surgery, vascular surgery, surgery, orthoorthoEvolved to combat lethal triad and Evolved to combat lethal triad and abort the abort the ‘‘bloody, vicious cyclebloody, vicious cycle’’
The Lethal TriadThe Lethal Triad
HYPOTHERMIAHYPOTHERMIA
ACIDOSISACIDOSIS COAGULOPATHYCOAGULOPATHY
Active Hemorrhage
IatrogenicFactors
Cellular Shock
Tissue Injury
ContactActivation
Clotting Factor Deficiencies
Coagulopathy
Acidosis
Hypothermia
Massive Transfusion
Pre-ExistingDiseases
“THE BLOODY VICIOUS CYCLE”
Kashuk JL, Moore EE, Millikan JS, Moore JBJ Trauma 1982; 22:672-279
Damage ControlDamage Controlin the Surgical Patientin the Surgical Patient
Communication essential between resuscitation Communication essential between resuscitation team and ED, IR, OR, ICU, blood bank, team and ED, IR, OR, ICU, blood bank, laboratory and pharmacylaboratory and pharmacyDamage control patient is at or near the point of Damage control patient is at or near the point of physiologic exhaustionphysiologic exhaustion
Damage ControlDamage Controlin the Surgical Patientin the Surgical Patient
Recognition of who needs itRecognition of who needs itShockShockCoagulopathyCoagulopathyHypothermia (temperature Hypothermia (temperature << 3535ººC)C)Massive transfusion or resuscitationMassive transfusion or resuscitation
>> 10 units of 10 units of PRBCsPRBCsAcidosis (pH < 7.3 or worsening base deficit)Acidosis (pH < 7.3 or worsening base deficit)Definitive repair would require prolonged operative time Definitive repair would require prolonged operative time or extensive surgical procedures (> 90 minutes)or extensive surgical procedures (> 90 minutes)Surgeon Surgeon ‘‘gestaltgestalt’’
Damage ControlDamage Controlin the Surgical Patientin the Surgical Patient
Make the decision early!Make the decision early!
Damage ControlDamage Controlin the Surgical Patientin the Surgical Patient
ComponentsComponents
1.1. Abbreviated surgery for rapid control of Abbreviated surgery for rapid control of hemorrhage and contaminationhemorrhage and contamination2.2. Resuscitation in the ICU with correction of Resuscitation in the ICU with correction of physiologic abnormalitiesphysiologic abnormalities3. Subsequent definitive repair and abdominal 3. Subsequent definitive repair and abdominal wall closurewall closure
Damage ControlDamage Controlin the Surgical Patientin the Surgical Patient
Abbreviated resuscitative surgeryAbbreviated resuscitative surgeryDo only necessary proceduresDo only necessary proceduresControl bleedingControl bleeding
LigationLigationShuntingShuntingPackingPacking
Excision/stapling of bowel to prevent further Excision/stapling of bowel to prevent further contaminationcontaminationLimit heat lossLimit heat lossChest/abdomen/extremity all potential candidatesChest/abdomen/extremity all potential candidates
Damage ControlDamage Controlin the Surgical Patientin the Surgical Patient
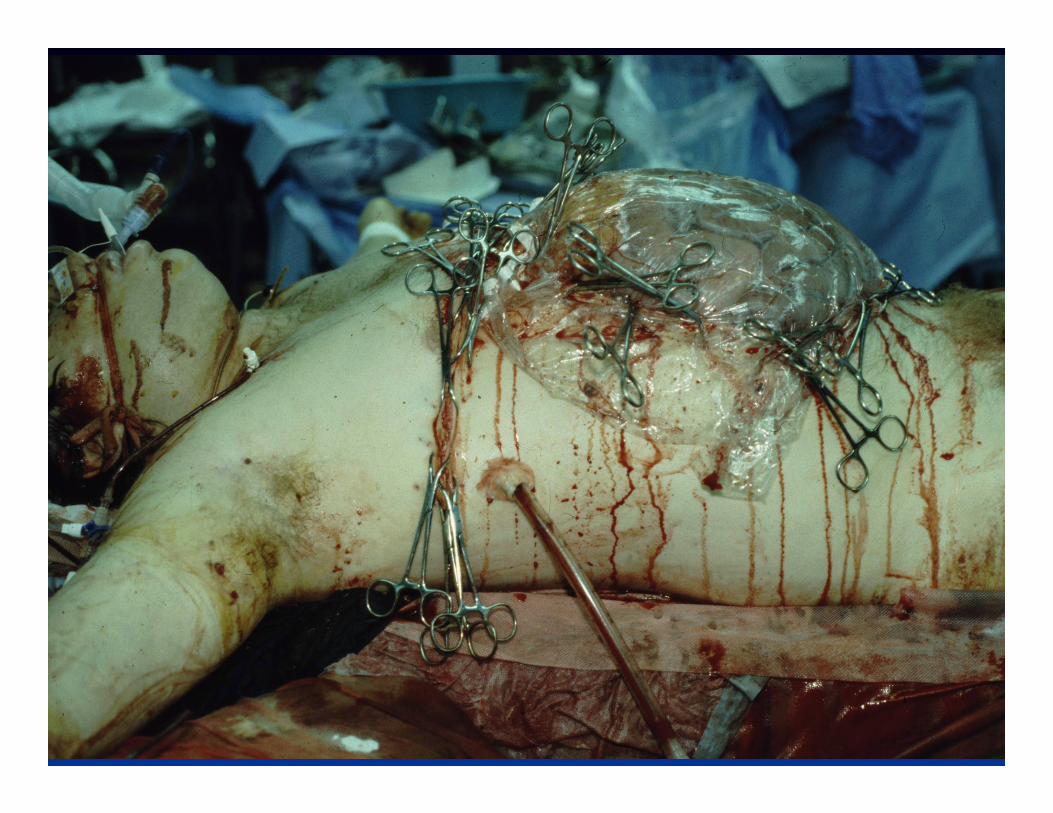
Temporary closure of the Temporary closure of the open abdominal defectopen abdominal defect
Vacuum Pack dressingVacuum Pack dressingInexpensiveInexpensivePerforated plastic sheet Perforated plastic sheet overlying boweloverlying bowelCovered with towels, Covered with towels, drains and adhesive drapedrains and adhesive drapeDrains placed to suction Drains placed to suction to control drainageto control drainage
ICU ResuscitationICU Resuscitation
Warm the patientWarm the patientCorrect the acidosisCorrect the acidosisCorrect the Correct the coagulopathycoagulopathy
HypothermiaHypothermia
--4.64.6°°C per hour even with warm IV fluid, C per hour even with warm IV fluid, gases and air convection blanketsgases and air convection blankets
Burch et al. Burch et al. SurgSurg ClinClin North Am North Am 1977; 77:7791977; 77:779
Mortality from 40% to 100% with core Mortality from 40% to 100% with core temp from 34temp from 34°°C to < 32C to < 32°°CC
JurkovichJurkovich et al. et al. J Trauma J Trauma 1987; 27:10191987; 27:1019
HypothermiaHypothermia
Cardiac Cardiac dysrhythmiasdysrhythmiasReduces cardiac outputReduces cardiac outputShifts the hemoglobin saturation curve to Shifts the hemoglobin saturation curve to the leftthe leftAffects clotting cascadeAffects clotting cascade
Platelet dysfunction, endothelial abnormalities Platelet dysfunction, endothelial abnormalities and alterations in the and alterations in the fibrinolyticfibrinolytic systemsystemCoagulation assays inaccurate for hypothermic Coagulation assays inaccurate for hypothermic patientpatient< 35< 35°°C C →→ PT and PTT prolongedPT and PTT prolonged
Reed, et al Reed, et al Circ ShockCirc Shock 1990; 32:1411990; 32:141
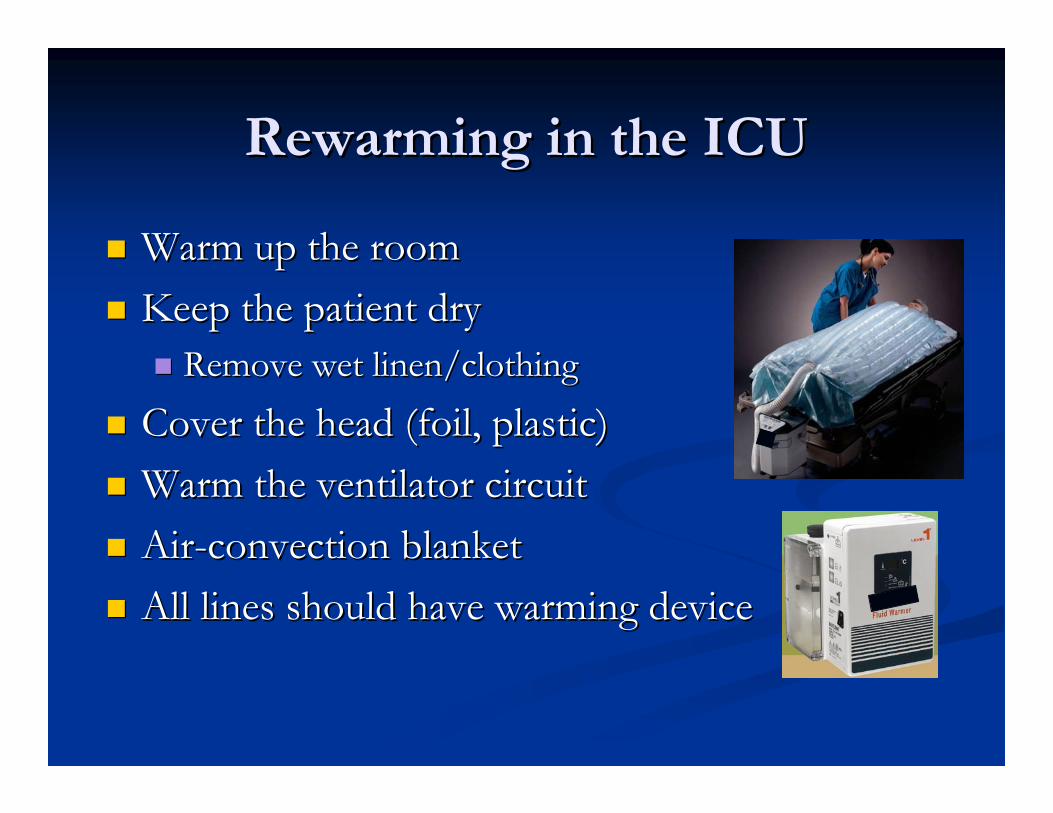
RewarmingRewarming in the ICUin the ICU
Warm up the roomWarm up the roomKeep the patient dryKeep the patient dry
Cover the head (foil, plastic)Cover the head (foil, plastic)Warm the ventilator circuitWarm the ventilator circuitAirAir--convection blanketconvection blanketAll lines should have warming device All lines should have warming device
RewarmingRewarming in the ICUin the ICU
If the temperature doesnIf the temperature doesn’’t respondt respondWarm pleural Warm pleural lavagelavage with NS via chest tubeswith NS via chest tubesContinuous AV warmingContinuous AV warmingGel pads simulate water Gel pads simulate water immersion connected to aimmersion connected to acontrol module control module
ResuscitationResuscitation
Access: Access: At least 2 large bore IVsAt least 2 large bore IVsCentral access Central access
Introducer sheathIntroducer sheath——make sure large enough to float make sure large enough to float PA catheter if neededPA catheter if neededPoiseuillePoiseuille’’ss LawLaw
Lines placed in ED or Lines placed in ED or OROR usually considered usually considered ““dirtydirty””, may keep for 24 hours, may keep for 24 hours
ResuscitationResuscitation
16 g 16 g IV tubingIV tubing 125 ml/min125 ml/minblood tubingblood tubing 193 ml/min193 ml/mintrauma tubingtrauma tubing 247 ml/min247 ml/min
DutkyDutky et al. Factors et al. Factors ffectingffecting rapid fluid resuscitation with large bore rapid fluid resuscitation with large bore introucerintroucer catheters. catheters. J TraumaJ Trauma 1989; 29:8561989; 29:856
ResuscitationResuscitation
AA--linelineUrinary bladder pressureUrinary bladder pressureBaseline fluid rate 125 cc/hr with boluses as Baseline fluid rate 125 cc/hr with boluses as necessarynecessaryPA catheterPA catheter
Older patientsOlder patientsLarge volume resuscitationLarge volume resuscitationBase deficit/lactic acidosis not improvingBase deficit/lactic acidosis not improving
May need to consider May need to consider inotropesinotropes------but only after but only after tank is fulltank is fullH/H, H/H, ChemChem profile including Caprofile including Ca++++, , PhosPhos, Mg, Mg++++, , lactic acid, INR, fibrinogen, platelet q 4 hourslactic acid, INR, fibrinogen, platelet q 4 hours
ResuscitationResuscitation
Endpoints of ResuscitationEndpoints of ResuscitationReRe--establish endestablish end--organ perfusionorgan perfusionAdequate urinary outputAdequate urinary outputHematocritHematocrit > 20% (value depends upon age/> 20% (value depends upon age/sxsx))Keep > 30 if still bleeding!Keep > 30 if still bleeding!
Restoration of vital signsRestoration of vital signsNormal mixed venous oxygenationNormal mixed venous oxygenationNormal or high cardiac outputNormal or high cardiac output
Clearance of lactic acidosis/base deficitClearance of lactic acidosis/base deficitNormalize pHNormalize pH------preferably without NaHCOpreferably without NaHCO33 or or THAMTHAM
ResuscitationResuscitation
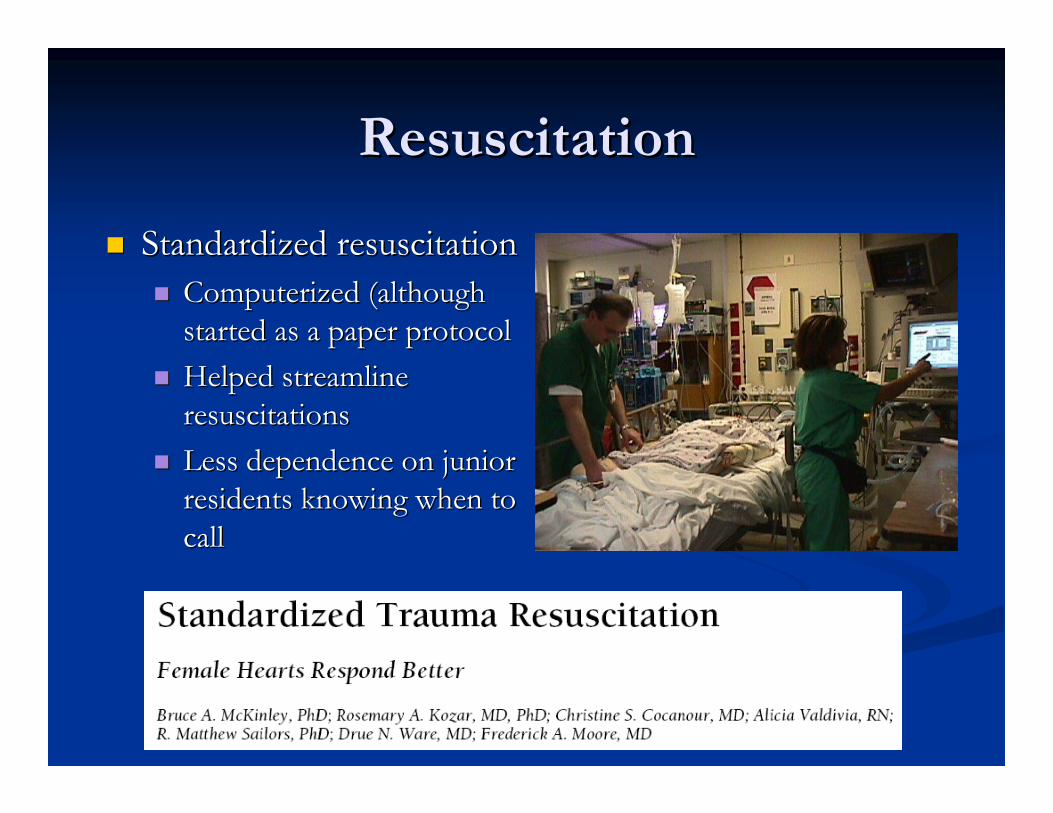
Standardized resuscitationStandardized resuscitationComputerized (although Computerized (although started as a paper protocolstarted as a paper protocolHelped streamline Helped streamline resuscitationsresuscitationsLess dependence on junior Less dependence on junior residents knowing when to residents knowing when to callcall
DO2I goal
1) Hb (PRBC; Hb > 10 )2) volume (LR; PCWP >15 )
3) Optimize CI - PCWP(Starling curve)
4) low dose Inotropes5) vasopressor
Yes No
Yes
No
Met inclusion criteria
On ICU admission:art, PA, NG tonometer catheters
baseline ABG, Hb, lactate
24 hours?24 hours?
Echocardiographystop resuscitationstandard ICU carestop resuscitationstandard ICU care
lactate, BD, PrCO2bladder pressureQ 4h (reassess sooner if abnormal)
Monitor:
Q 4h (reassess sooner if abnormal)
ResuscitationResuscitation
Intravascular volume restoration best Intravascular volume restoration best accomplished using FFP in a 1:1 ratio with accomplished using FFP in a 1:1 ratio with PRBCsPRBCsCrystalloid use is more limitedCrystalloid use is more limited
Massive TransfusionMassive Transfusion
Massive TransfusionMassive Transfusion
Massive transfusion Massive transfusion >> 10 units in first 24 hrs 10 units in first 24 hrs More than one blood volume in first 12 hrsMore than one blood volume in first 12 hrs
Traditional transfusion regimen: 6 units of Traditional transfusion regimen: 6 units of PRBCsPRBCs, then start FFP, then start FFPHirshbergHirshberg et al: computer model suggested that et al: computer model suggested that FFP:PRBC is 2:3FFP:PRBC is 2:3FFP:PRBC of 1:1 is associated with decreased FFP:PRBC of 1:1 is associated with decreased mortality and decreased transfusion mortality and decreased transfusion requirementsrequirements
Factor Factor VIIaVIIaNo FDA indication for traumatic shockNo FDA indication for traumatic shockShould only be considered on a compassionate use Should only be considered on a compassionate use basis basis afterafter surgical bleeding controlled, aggressive surgical bleeding controlled, aggressive coagulation factor and platelet replacement has coagulation factor and platelet replacement has occurred and acidosis correctedoccurred and acidosis correctedThromboticThrombotic events in this patient population not well events in this patient population not well characterizedcharacterizedUse remains controversialUse remains controversialMore use of 1:1 PRBC to FFP, decreased use of Factor More use of 1:1 PRBC to FFP, decreased use of Factor VIIaVIIa
Metabolic AcidosisMetabolic Acidosis
HypoperfusionHypoperfusionShift from aerobic to anaerobic metabolism at the Shift from aerobic to anaerobic metabolism at the cellular level, cellular level, ieie cellular hypoxiacellular hypoxia
Lactic acidosisLactic acidosisAble to clear lactate within 24 hours = 100% Able to clear lactate within 24 hours = 100% survivalsurvival
Metabolic AcidosisMetabolic Acidosis
Usually corrects on its own once patient is warm Usually corrects on its own once patient is warm and volume resuscitatedand volume resuscitatedOO22 debt repaiddebt repaidAnaerobic Anaerobic →→ aerobic metabolismaerobic metabolismNeed for NaHCONeed for NaHCO33 rare butrare but……
If If cardiotoniccardiotonic agents needed, keep pH > 7.2agents needed, keep pH > 7.2Avoid use of Avoid use of bicarbbicarb and THAM as this eliminates and THAM as this eliminates the use of base deficit for monitoring resuscitationthe use of base deficit for monitoring resuscitation
VentilationVentilation
At risk for Acute Lung Injury (ALI)At risk for Acute Lung Injury (ALI)Direct Direct parenchymalparenchymal lung injurylung injuryShockShockMassive resuscitation volumesMassive resuscitation volumes
Continued hemorrhageContinued hemorrhageExpect H/H to decreaseExpect H/H to decrease
EquilibrationEquilibrationContinued non surgical losses especially if Continued non surgical losses especially if coagulopathycoagulopathy and and hypothermia are not yet correctedhypothermia are not yet corrected
> 2 units PRBC/hour x > 2 units PRBC/hour x 33 hourshoursEspecially in a warm, non Especially in a warm, non coagulopathiccoagulopathic patientpatient
PitfallsPitfalls
Continued hemorrhageContinued hemorrhageExpect H/H to decreaseExpect H/H to decrease
EquilibrationEquilibrationContinued non surgical losses especially if Continued non surgical losses especially if coagulopathycoagulopathy and and hypothermia are not yet correctedhypothermia are not yet corrected
> 2 units PRBC/hour x 2 hours> 2 units PRBC/hour x 2 hoursEspecially in a warm, non Especially in a warm, non coagulopathiccoagulopathic patientpatient
Vessels that were constricted and NOT Vessels that were constricted and NOT ligatedligated at time of Op at time of Op may begin bleeding as patient is warmed and resuscitatedmay begin bleeding as patient is warmed and resuscitated
RETURN TO THE OR (or IR)RETURN TO THE OR (or IR)
PitfallsPitfalls
Continued shockContinued shockMissed injuryMissed injuryFailed repair with leakageFailed repair with leakageInsufficient replacement of fluid from open Insufficient replacement of fluid from open abdomenabdomen
Urgent Urgent ReoperationReoperation
OR is best place to beOR is best place to beVent requirements too much for the ORVent requirements too much for the OR
Use bedside vent in the OR (if you can transport Use bedside vent in the OR (if you can transport on vent)on vent)Bring the OR to the ICU bedsideBring the OR to the ICU bedside
Not optimal if bleeding expectedNot optimal if bleeding expected
Complication of damage control Complication of damage control laparotomylaparotomyAbdominal packsAbdominal packsOngoing bleedingOngoing bleedingProgressive bowel edemaProgressive bowel edema
Failure of non operative management of solid Failure of non operative management of solid organ injuries organ injuries
Secondary ACSSecondary ACS
No abdominal injuriesNo abdominal injuriesSevere shock requiring massive Severe shock requiring massive resuscitationresuscitationPelvic fracturesPelvic fracturesBowel edema and Bowel edema and ascitesascites
Definitive RepairDefinitive Repair
When to return to the OR?When to return to the OR?When patients are warm, acidosis and When patients are warm, acidosis and coagulopathycoagulopathycorrectedcorrected3636--72 hours had reduced risk of 72 hours had reduced risk of rebleedingrebleeding for for patients with patients with perihepaticperihepatic packingpacking
Caruso, et al Caruso, et al Arch Arch SurgSurg 1999; 134:9621999; 134:962
Coincides with fluid mobilizationCoincides with fluid mobilization? Use of diuretics? Use of diuretics
Definitive RepairDefinitive Repair
Bowel injuries:Bowel injuries:Colostomy or Colostomy or anastomosisanastomosis??
Delayed Delayed anastomosesanastomoses were as safe as colostomywere as safe as colostomyMiller, et al Miller, et al Am Am SurgSurg 2007; 73:6062007; 73:606
Stapled Stapled vsvs handhand--sewn sewn anastomosisanastomosis??Controversial as to which is bestControversial as to which is bestSurgeon comfort with techniqueSurgeon comfort with techniquePresence of bowel edema?Presence of bowel edema?
Edematous bowel more prone to leakEdematous bowel more prone to leakWait for edema to resolve to do Wait for edema to resolve to do anastomosisanastomosis
ClosureClosure
Velcro Patch
ClosureClosure
Vacuum Closure
92% of patients closed in mean of 9.9 + 1.9 days
Garner, et al Am J Surg2001; 182:630
ClosureClosure
When the abdomen canWhen the abdomen can’’t be closedt be closedBowel becomes Bowel becomes ““stuckstuck””Multiple solutionsMultiple solutions
Permanent meshPermanent meshAbsorbable meshAbsorbable meshProsthetic patchesProsthetic patchesBioprostheticBioprosthetic patchespatchesSTSG directly on granulated bowelSTSG directly on granulated bowelComponent separation Component separation
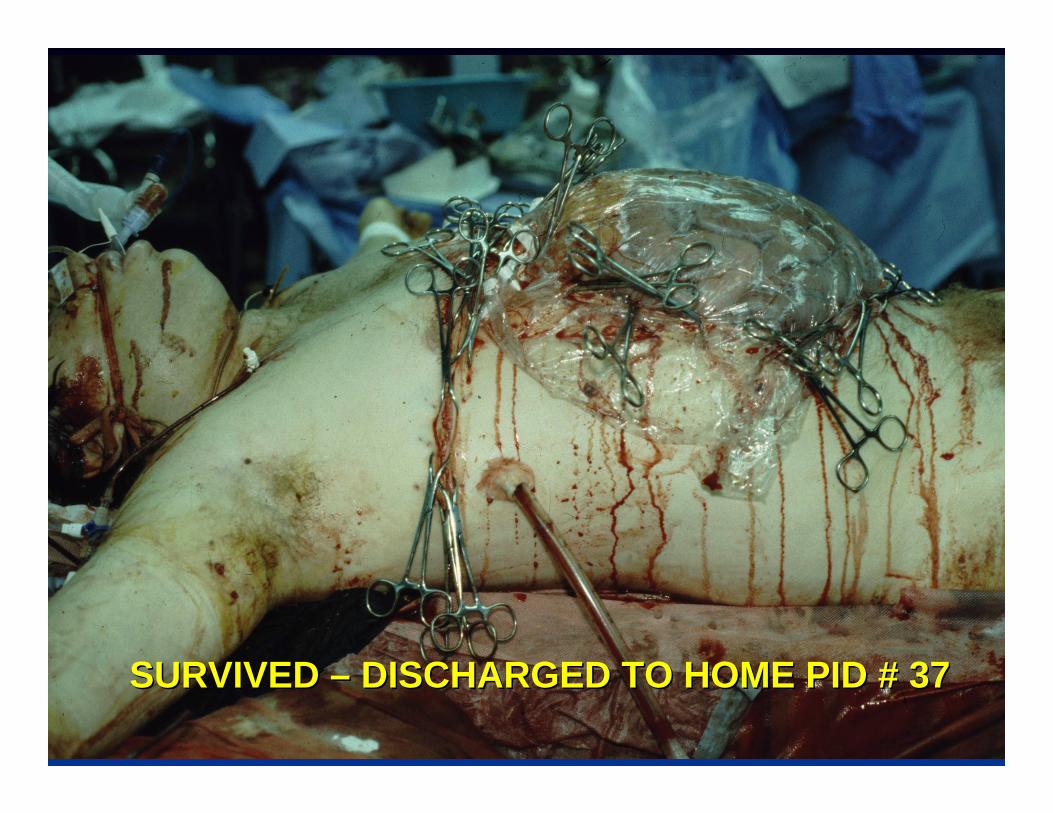
SURVIVED SURVIVED –– DISCHARGED TO HOME PID # 37DISCHARGED TO HOME PID # 37
““The art of medicine consists in amusing the patient The art of medicine consists in amusing the patient while nature cures the diseasewhile nature cures the disease””