21
Collaborative strategies to reduce tobacco exposure among low-income families Katie Marble, CHES Joan Orr, CHES Healthy Community Coalition
| Date post: | 03-Jan-2016 |
| Category: |
Documents |
| Upload: | cecil-burns |
| View: | 221 times |
| Download: | 2 times |
Collaborative strategies to reduce tobacco exposure among
low-income families
Katie Marble, CHES
Joan Orr, CHES
Healthy Community Coalition
Learning Objective
• You will be able to identify cost-effective strategies to reduce prenatal and secondhand smoke exposure in low-income families through multi-agency collaboration.
Service Area
• Population of service area: 40,000 • Classified as “very rural” with just 17.4
people per square mile.• Franklin County has lowest adult smoking
rate in Maine at 17% (Maine’s adult smoking rate is 23.5%)
(Maine BRFSS, Community Health Profile 2000)

Health Assets
• Healthy Community Coalition of the Franklin Community Health Network
• Healthy Maine Partnerships/Fund for Healthy Maine
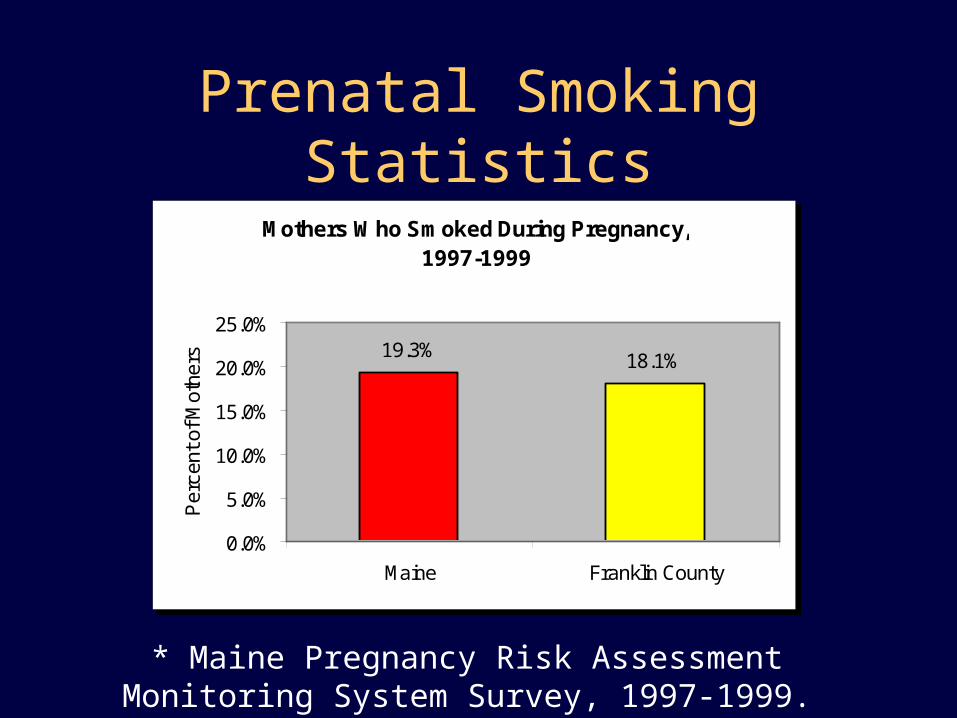
Prenatal Smoking Statistics
Mothers Who Smoked During Pregnancy, 1997-1999
19.3% 18.1%
0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
Maine Franklin County
Per
cent
of M
othe
rs
* Maine Pregnancy Risk Assessment Monitoring System Survey, 1997-1999.
Prenatal Smoking Statistics
• 25% return to smoking postpartum
• 66% of premature births in Franklin County were to women who smoked.
• Women who continue to smoke during pregnancy are almost exclusively low-income.– 90% have a household income of less than
24,000 (140% of poverty).* Maine Pregnancy Risk Assessment Monitoring System
Survey, 1997-1999.
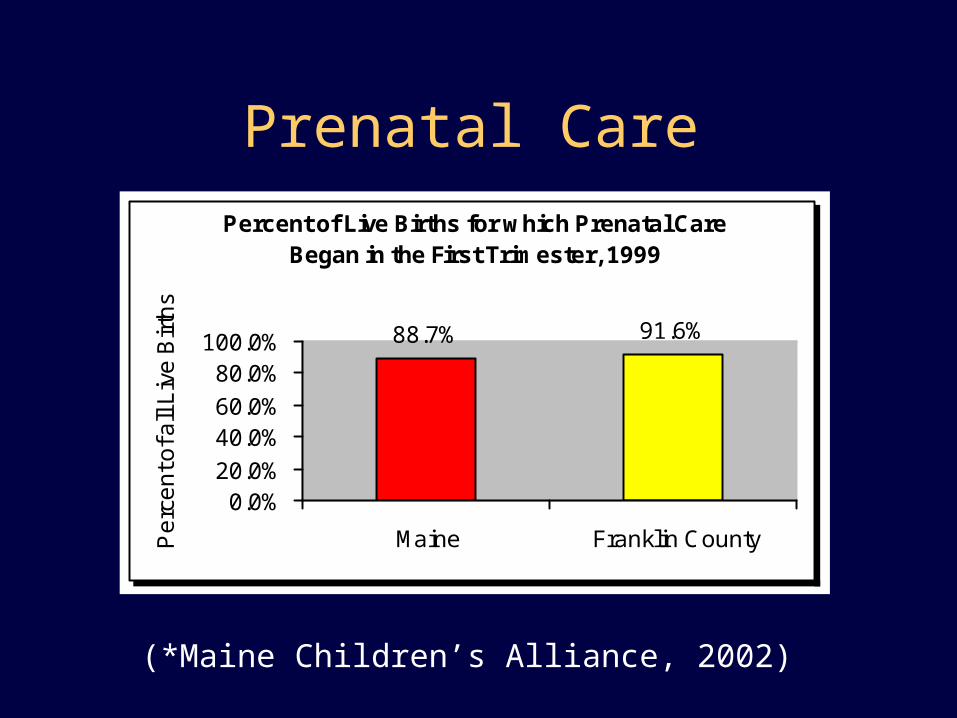
Prenatal Care
Percent of Live Births for which Prenatal Care Began in the First Trimester, 1999
88.7% 91.6%
0.0%20.0%
40.0%60.0%
80.0%100.0%
Maine Franklin CountyPe
rce
nt o
f all
Liv
e B
irth
s
(*Maine Children’s Alliance, 2002)
Tobacco-Free Franklin Families
• 3 year pilot program funded by the American Legacy Foundation Priority Population Grant.
• Goals to:– Reduce prenatal smoking– Reduce postpartum relapse– Reduce the # of children 0-5 exposed to ETS– Build a system of effective tobacco-use
reduction services for low-income families
Strategies
• Reach the maximum number of women with American Legacy Grant
• Have women repeatedly exposed to cessation messages
• Collaborate with Prenatal Care Providers & Agencies already reaching low-income women
• Target stress management
Founding Partners
• Pine Tree Women’s Care
• WIC
• Head Start
• Growing Healthy Families
• Franklin Childcare
Costs
• Trainings
• Meeting Support
• Resources Materials
• Incentives
Savings• Agencies provide outreach through out the
county (over 1697.81 square miles -1 1/2 times the size of Rhode Island), saving transportation costs or having to establish multiple sites
• Reach over 5000 families of 6194 families with a household income under $25,000 (more than our program could reach working alone:)
• Sustainable Strategy
Implementation
• Trained agency staff in the 5 A’s of intervention, nicotine addiction & the “stage of change” model.
• Established meetings to plan how intervention would take place in each agency.
• Each agency provides a different level of intervention. Home Visitors provide more in-depth intervention. Prenatal Care Providers at least a five minute intervention.
Implementation
• The intervention is guided by process evaluation, Tobacco Flow Chart.
• Assistance includes prenatal program Every Mother’s Wish, Maine Tobacco Helpline, Stress workshops
• Media campaign
• Established workgroup meetings and site visits to problem solve.
*Clarifying Success*• Important to let healthcare providers there are
many types of success within smoking cessation counseling.– Moving someone from one stage of change to another.
– Making an impact by mentioning tobacco
– Delayed reaction of participants
– Getting tobacco smoke outdoors
– Reducing the number of cigarettes smoked/day
– Someone quits smoking
Preliminary Results• This year over 72 health and social service
providers have had in-depth training in the 5 A’s of intervention. (42 more than year one goal)
• The calls to the Maine Tobacco Helpline from Franklin County were double the number expected from Jan.-Mar. 2003
• Tobacco status addressed as a vital sign with 100% of patients at Pine Tree Women’s Care.
Preliminary Results
• 81% of all women who smoke were provided with the 5 A’s of intervention at prenatal care offices
• 30 women completed Every Mother’s Wish Program in year one (out of 110)
• Additional agencies are requesting training on the 5 A’s of tobacco intervention
Lessons Learned:• Partners are the key to a successful program
• Clearly define the role of both your agency and the partner agency
• Identify the roles of people within each partner agency
• Identify a champion at each site
• Create a bonding experience for that site
• Never Underestimate the power of incentives (aka. Food)
More Lessons Learned
• Bring the programs/training to the audience not the audience to the program (especially in rural areas).
• Listen, Listen, Listen, Listen, Act, & the Listen Again.
• REMAIN FLEXIBLE

Thank-you
Contact us at:
Healthy Community Coalition
207-645-3136
Check our web site: http://www.FCHN.org/HCC