Ambo University College of Medicine and Health Sciences Department of Medicine C2 Pediatrics Seminar presentation on: The management of coma By: Hayelom Michael Habtamu Mokonen Hailemariam Bekele Moderator: Dr. Kissu Ambo,Ethiopia
Transcript
Ambo UniversityCollege of Medicine and Health
SciencesDepartment of Medicine
C2 PediatricsSeminar presentation on:The management of comaBy:
Hayelom MichaelHabtamu MokonenHailemariam Bekele
Moderator: Dr. Kissu
Ambo,Ethiopia
Outline• Objective• Introduction• Coma mimicking states• Cause • Pathophysiology• clinical features• Approach to comatose patient• Management of coma
Objective• To define coma and similar clinical
conditions.
• To describe the etiologies of coma
• To describe the pathophysiologic mechanism of coma in terms of the underlying anatomic and physiologic alterations.
• To explain the approach to a comatose patient.
• To explain the management of comatose patient
Introduction
• Consciousness is arousal, in which one is able to interact with the environment, and awareness, with the ability to know "what is going on.
• Is the product of two closely related cerebral functions:– Wakefulness i.e. arousal, alertness.– Content i.e. awareness of self and the env’t.
Cont….
• Coma is a state of unrousable, unconsciousnes without any psychologically understandable response to external stimuli or inner need.
• It is among the most common and striking problems in general medicine.
• There is a continuum of the states of consciousness, coma being the most severe.
Level of consciousness
• Reflects awareness and response to the environment:
• Alert - Appearance of wakefulness, awareness of the self and environment
• Lethargy :mild reduction in alertness -tends to drift of to sleep when not stimulated -when aroused has appropriate response• Obtundation - moderate reduction in alertness.
- It requires touch or voice to maintain arousal. -When aroused is in confusional state. -Usually constant stimulation is required
• Stupor: Deep sleep, patient can be aroused only by vigorous and repetitive stimulation.
-Returns to deep sleep when not continually stimulated.
• Coma: -Sleep like appearance and behaviorally
unresponsive to all external stimuli (Unarousable unresponsiveness, eyes closed)
Coma mimicking states
– Minimally conscious state(MCS)
– Persistently vegetative state(PVS)
– Locked in syndrome(LIS)
– Psychogenic unresponsiveness
– Brain death
• Differentiating coma from related states:
1.purpose full response to stimuli?
2.Brain stem reflex?
3.Sleep wake cycle?
4.EEG?
Minimally conscious state(MCS)
• The patient has rudimentary vocal or motor behaviors, often spontaneous, but some in response to touch, visual stimuli, or command.
• Cardiac arrest with cerebral hypoperfusion and head injuries are the most common causes.
Persistently vegetative state(PVS)
• Signifies an awake but nonresponsive state in a patient who has emerged from coma.
• The vegetative state is characterized by loss of all cognitive functions & the un awareness self &surroundings.
• Reflex & vegetative function, including sleep wake cycles.
• These individuals have spontaneous eye opening with out concurrent awareness.
• Diagnosis criteria for Vegetative state include:
-The absence of awareness self&environment
and inability to interact with others.
-The absence of sustained or reproducible voluntary behavioral responses.
-lack of language comprehension
-Suffiently preserved hypothalamus & brain stem function to maintain life.
NB. The PVS requires that condition has continued for at least 1 month.
Few, if any, meaningful responses to the external and internal environment—in essence, an "awake coma."
• Indicates extensive damage in both cerebral hemispheres, usually 2° to ischemic injury
Locked in syndrome
• An awake patient has no means of producing speech or volitional movement but retains voluntary vertical eye movements and lid elevation, thus allowing the patient to signal with a clear mind.
• The pupils are normally reactive. • The usual cause is an infarction or
hemorrhage of the ventral pons that transects all descending motor (corticospinal and corticobulbar) pathways
Psychogenic unresponsiveness
• Also termed 'pseudocoma‘, this describes a patients who appear to be unconscious and in coma but who are not.
• Oculovestibular testing, will reveal the presence of nystagmus and indicate that the patient has an intact brainstem and cortex.
Brain death
• This is a state of cessation of cerebral function with preservation of cardiac activity and maintenance of somatic function by artificial means.
• It is equivalent to death. • Brain death Criteria: (1) widespread cortical destruction that is reflected by
deep coma and unresponsiveness to all forms of stimulation;
(2) global brainstem damage demonstrated by absent pupillary light reaction and by the loss of oculovestibular and corneal reflexes;
(3) destruction of the medulla, manifested by complete apnea.
Cause
• A more practiced &clinically relevant categorization of CNS insults sever enough to cause coma involves the categorization of as:
• Almost all instances of diminished alertness can be traced to:
widespread abnormalities of the cerebral hemispheres
reduced activity of a special thalamocortical alerting system termed the reticular activating system (RAS).
• The proper functioning of this system, its ascending projections to the cortex, and the cortex itself are required to maintain alertness and coherence of thought.
Cont…
• The ascending RAS, from the lower border of the pons to the ventromedial thalamus
• The cells of origin of this system occupy a paramedian area in the brainstem
Cont…• It follows that the principal causes of coma
are:
(1) lesions that damage the RAS in the upper midbrain or its projections
(2) destruction of large portions of both cerebral hemispheres
(3) suppression of reticulocerebral function by drugs, toxins, or metabolic derangements such as hypoglycemia, anoxia, uremia, and hepatic failure
Coma Due to Cerebral Mass Lesions
• Herniation is the principal mechanism
A) Uncal (most common)
B) central
C) transfalcial
D) foraminal
Coma Due to Metabolic Disorders
Interruption of the delivery of energy substrates (e.g., hypoxia, ischemia, hypoglycemia)
Alteration of neuronal excitability (drug and alcohol intoxication, anesthesia, and epilepsy)
• Unlike hypoxia-ischemia, which causes neuronal destruction, most metabolic disorders such as hypoglycemia,hyponatremia,hyperosmolarity, hypercapnia, hypercalcemia, and hepatic and renal failure : - impaired energy supplies,
-changes in ion fluxes across neuronal membranes, and
-neurotransmitter abnormalities.
Toxic (Including Drug–Induced) Coma
• Many drugs and toxins are capable of: depression of nervous system function. producing coma by affecting both the
brainstem nuclei, including the RAS, and the cerebral cortex.
• The combination of cortical and brainstem signs, which occurs in certain drug overdoses, may lead to an incorrect diagnosis of structural brainstem disease.
• Overdose of medications that have atropinic actions produces signs such as dilated pupils, tachycardia, and dry skin; opiate overdose produces pinpoint pupils <1 mm in diameter.
Coma Due to infection
• The most common causes include: Pyogenic menigitis ,TB meninigitis, Cerebral malaria,HIV, encephiltis,
• Widespread structural cerebral damage→ a metabolic disorder of the cortex.
• Hypoxia-ischemia is perhaps the most known →hypoperfusion and oxygen deprivation of the brain.
• Similar bihemispheral damage is produced by disorders that occlude small blood vessels throughout the brain
• Diffuse white matter damage from inflammatory demyelinating diseases causes a similar syndrome of coma.
Clinical features• Sleeplike state from which the patient cannot
be aroused.
• Eyes are closed and remain closed in the face of vigorous stimulation.
• Do not speak.
• Do not arouse to verbal,tactileor noxious stimuli • Motor activity is absent or abnormal and
reflexive rather than purposeful or defensive.
• as opposed to state of transient unconsciousness such as syncope& concussioncoma must last ≥1 hr.
Approach to a patient in Coma
Coma is a medical emergency whose evaluation requires a rapid, comprehensive, and systematic approach.
Early identification of the underlying cause of coma can be crucial for patient management and prognosis.
A. Immediate life supportB. Identification of causesC. Specific therapy
A. Immediate life support
Assessment and maintenance of vital function is the initial step
(ABC of life)
• Maintain the air ways patency and ensure adequate breathing
• Maintain circulation
B. Establishment of cause of coma:
is done by taking a careful history, doing rapid but through
physical examination and investigations.
Patient History
• It is often useful to obtain a history from witnesses, friends or
family members, and emergency medical technicians.
• The patient's personal effects: a Medical Alert bracelet or
necklace and/or a card in the wallet may contain a list of
illnesses and medications.
• Past medical history: looking for disease like diabetes,
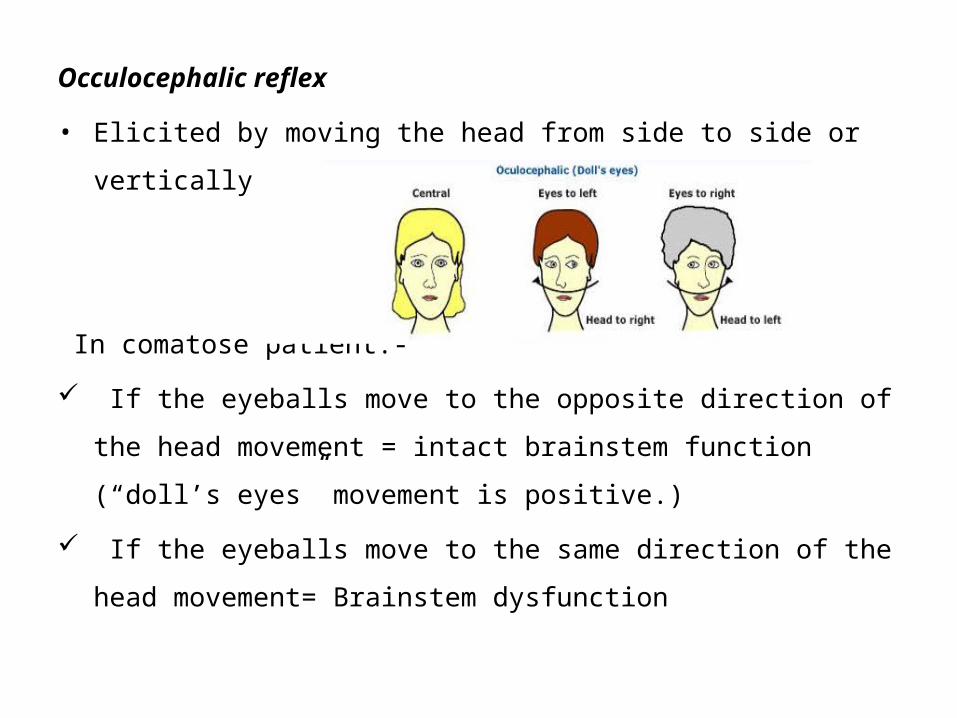
• Elicited by moving the head from side to side or vertically with eyes held
open.
In comatose patient:-
If the eyeballs move to the opposite direction of the head movement =
intact brainstem function (“doll’s eyes” movement is positive.)
If the eyeballs move to the same direction of the head movement=
Brainstem dysfunction
Caloric (occulovestibular) reflex
• This test is performed by irrigating the ear with ice (cold) to
stimulate the vestibular apparatus.
• In patients with intact brain stem the eyes move to the irrigated
ear.
c) Corneal reflex
The corneal reflex tests the sensory function of the
trigeminal nerve and the motor function of the
facial nerve.
• This test assesses the integrity of dorsal midbrain and
pontine.
• It is lost if the reflex connections between the fifth and the
seventh cranial nerves within the pons are damaged.
d) Respiration:
less localizing value in comparison to other brainstem signs.
• Shallow, slow, but regular breathing suggests metabolic or drug
depression.
• Cheyne-Stokes respiration signifies bihemispherical damage or metabolic
suppression, and commonly accompanies light coma.
• Kussmaul breathing usually implies metabolic acidosis but may also occur
with pontomesenephalic lesions and severe pneumonia.
• Agonal gasps are the result of lower brainstem (medullary)
damage and are recognized as the terminal respiratory
pattern of severe brain damage.
3. Motor function /response
Quadriparesis and flaccidity-suggest pontine or medullary damage.
Decorticate posturing: flexion of the elbows and the wrists with supination
of the arms, and extension of the legs, suggests severe bilateral or
unilateral hemispheric or diencephalic lesion (damage above the
midbrain.)
Decerebrate posturing (extension of elbows and the wrist with pronation of the
forearm and extension of the legs) indicates damage to the brainstem( midbrain or
pontine compromise )
Abnormal body movements – seizure, myoclonus may suggest the cause of the
coma is status epelepticus, uremia etc.
DIAGNOSTIC STUDIES
• Studies can be guided by HX and PE, but most patients presenting with coma of unknown etiology require laboratory testing and a neuroimaging study.
Laboratory Testing
• Patients presenting with altered consciousness should undergo a rapid bedside test for blood glucose and basic laboratory testing including:
• Serum electrolytes, calcium, magnesium, glucose
• Arterial blood gas • Liver function tests, ammonia • Complete blood count • Blood urea nitrogen, creatinine • Urine drug screen
• blood and urine tests
• Testing for fungi, rickettsia, mycobacteria, and parasites
• thyroid function tests
• cortisol levels/ carboxyhemoglobin, and coagulation studies
• Neuroimaging — CT is the best initial neuroimaging test. CT quickly detects hydrocephalus, herniation, and mass lesions due to infection, neoplasia, hemorrhage, and edema.
• When lumbar puncture is indicated, a CT is required in the comatose patient to rule out a mass lesion that might precipitate transtentorial herniation as a result of the procedure.
• MRI - provides greater structural detail and is more sensitive for early evidence of encephalitis, infarction, diffuse axonal injury from head injury, petechial hemorrhages, cerebral venous thrombosis, and demyelination.
• Lumbar puncture
• Electroencephalogram : coma of unknown etiology
• It is often the only means of recognizing non convulsive status epilepticus (NCSE), especially in patients who are paralyzed.
Treatment and Prognosis of Coma in Children
• TREATMENT — Early treatment of coma is generally supportive
• An important goal of early treatment is to limit brain injury.
• RX for dangerous etiologies (eg, hypoglycemia, increased ICP, bacterial meningitis) are often initiated empirically
• The primacy of ABCs applies to coma as to other medical emergencies.
Airway• attained by repositioning the child to open
the airway• Patients with GCS <8 are usually unable
to adequately protect their airway and should be intubated.
• If trauma is suspected, the cervical spine should be stabilized with a collar while securing the airway.
• Breathing — O2 saturation should be measured and supplemental O2 provided.
• Adequacy of ventilation should be assessed by examination and arterial blood gases.
• Moderate hyperventilation (target PaCO2 30 to 35 mm Hg) should only be initiated for patients with increased ICP.
• Extreme hyperventilation /aggressive hyperventilation (PaCO2 <30 mmHg) are only justified in patients with transtentorial herniation.
Circulation
Depressed level of consciousness may be an early indicator of poor end-organ perfusion in a patient with shock
Hypotension
• IV administration (NS or LR) and inotropes, if necessary, is essential to deliver oxygen and metabolic substrates to the brain and remove toxic metabolites.
Hypertensive encephalopathy
• The goal of therapy is to lower the DBP to 100 to 110 mmHg (or by a maximum of 25 percent) within two to six hours
• Hypertensive encephalopathy has an excellent prognosis for recovery if ischemia can be avoided
• Glucose — Glucose (2.5 mL/kg of 10 percent dextrose solution) should be administered even before test results are known. If hypoglycemia is revealed, then ongoing monitoring and treatment will be needed.
• Intracranial pressure — When increased ICP is suspected, emergent RX is recommended. Increased ICP is assumed when there is coma after head injury.
• Early interventions to reduce ICP include treating fever, elevating the head of the bed to 30 degrees above horizontal, moderate hyperventilation (target PaCO2 30 to 35 mmHg) and administering mannitol(0.25 to 1 g/kg IV). Neurosurgery should be consulted.
• Seizures — If seizures have occurred, phenytoin or fosphenytoin(15 to 20 mg/kg phenytoin equivalent IV) should be administered.
• Non convulsive status epilepticus should be considered as a diagnosis even when there are no obvious seizure movements.
• If non convulsive seizures are suspected and an electroencephalogram (EEG) is not available, a therapeutic trial of phenytoin or lorazepam (1 to 2 mg IV) is reasonable.
• Infection — Empiric antibiotic and antiviral therapy are recommended
• If bacterial meningitis (eg, ceftriaxone100 mg/kg per day in one or two divided doses, maximum dose 4 g per day, plus vancomycin 60 mg/kg per day in four divided doses)
• Viral encephalitis ( acyclovir 30 to 60 mg/kg per day, in
three divided doses) are among the suspected entities. • Blood cultures should be obtained prior to starting
antibiotics but initiation of therapy should NOT await LP. • Therapy should be continued until these conditions have
been excluded
• Temperature control — Hyperthermia (>38.5 degrees C).
• Fever should be lowered with antipyretics and/or cooling blankets immediately. Shivering, which can contribute to elevated ICP, should be avoided.
• Hypothermia to 32 to 36 degrees has been suggested as a therapy for refractory increased ICP in children with traumatic brain injury - currently not recommended
• May be appropriate for children with o out-of-hospital arrest o persistent coma o ventricular fibrillation or o pulseless ventricular tachycardia
• Acid-base and electrolyte imbalance —resuscitation of patients with cardiovascular compromise should use isotonic solutions only (NS or RL).
• Antidotes — use is recommended only in the setting of known or strongly suspected drug overdose.
• Naloxone(0.1 mg/kg IV in patients up to 20 kg or ≤5 years; maximum 2 mg) - possible opiate ingestion.
• Flumazenil - benzodiazepine overdose, but will render benzodiazepines ineffective in the event of a seizure, so it should also be used with caution.
• Agitation — sedation - should be administered only when the benefits of relieving agitation outweigh the need for close neurologic monitoring by exam.
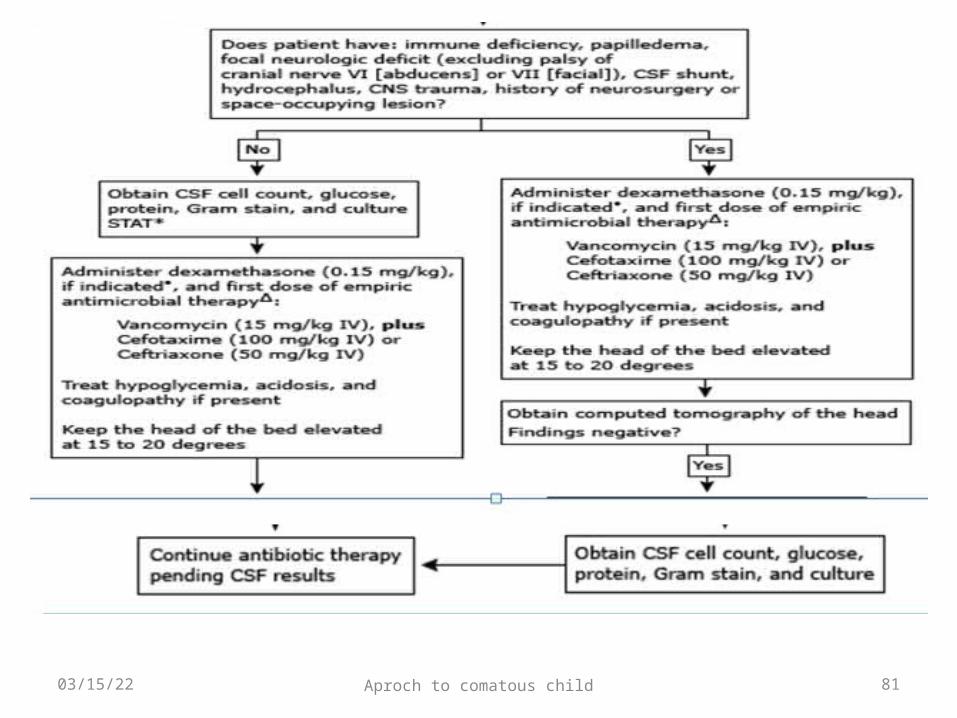
Management algorithm for infants (≥1 month) and children with suspected
bacterial meningitis
04/17/23 Aproch to comatous child 80
04/17/23 Aproch to comatous child 81
Tb meningitis
04/17/23 Aproch to comatous child 82
• Chemotherapy should be initiated with RHZS in an initial phase for 2 months and RH should be continued for 7 to 10 months in the continuation phase.
• Adjunctive corticosteroid therapy with dexamethasone is recommended for all patients. The recommended regimen is:
04/17/23 Aproch to comatous child 83
• Dexamethasone- a total dose of 8 mg/day for children weighing less than 25 kg and 12 mg/day for children weighing 25 kg or more.
• The initial dose is given for 3 weeks and then decreased gradually during the following 3 weeks.
• Prednisolone- a dose of 2-4mg/kg/day for children for 3 weeks, then tapered of gradually over the following three weeks.
Long term essentials
04/17/23 Aproch to comatous child 84
• Skin care
• Oral hygiene
• Eye care
• Fluids
• Calories
• Sphincters
PROGNOSIS
• The prognosis in coma is etiology specific. • Mass lesions at the fully developed midbrain stage
do poorly even after surgical evacuation. • Sedative drug induced coma has a good
prognosis with proper supportive care.• Coma with purulent meningitis doubles
unfavorable outcome or death. • In hepatic or other metabolic comas, the absence
of pupillary, oculovestibular, and corneal reflexes on admission is a grave prognostic sign.
04/17/23 Aproch to comatous child 86
• Brisk, small-amplitude, mainly vertical eye movements are predictive of a fatal outcome.
• In cardiac arrest patients without seizures, return of pupillary reactivity and purposeful motor movements within the first 72 hours is highly correlated with a favorable outcome.
• Bilateral absence of somatosensory evoked responses in the first week predicts death or a persistent vegetative state.
PX Factors
04/17/23 Aproch to comatous child 87
• GCS
• Age
• Clinical features
• EEG
• MRI
• Serum biomarkers
• GCS - is associated with prognosis in a number of conditions as TBI.
• In some cases, “Age” < 2 years is associated with worse px.
• Clinical features — the presence and severity of certain early complications has been linked to worse outcome
• EEG -a predictor of outcome in coma of certain etiologies.
• Sedative drugs cause EEG abnormalities and make interpretation difficult, particularly for prognosis.
• An isoelectric baseline or a burst suppression pattern during the first week after coma - 100 % specific for poor outcome
• Other EEG patterns associated with poor outcome(but have poor sensitivity and specificity)
o periodic epileptiform dischargeso nonreactive rhythms
MRI• Presence and extent of brain edema,
brainstem injury, and diffuse axonal injury -associated with poorer prognosis in patients with TBI.
• Serum biomarkers — Elevated neuron specific enolase (NSE) levels have been associated with poor outcome after HIE, TBI and other conditions (e.g., encephalitis, Reye's syndrome).



















































































![Final coma stimulation[1]](https://static.documents.pub/doc/80x56/577d2e971a28ab4e1eaf786f/final-coma-stimulation1.jpg)

