Health Policy, 7 (1987) 216-226 Elsevier 215 HPE 00144 Combining clinical budgets and DRGs for quality management* lden Wickings CASPE Research, King Edward’s Hospital Fund, London, U.K. Accepted 6 January 1987 Summary Global and clinical budgets are being introduced in the U.K. as elsewhere to con- trol health care costs. They are in fact showing effectiveness in terms of cost-con- trol. They do not, however, adequately address outcomes and quality of care. DRGs could be used as a tool for associating costs with outcome and quality measures. lf constructed carefully, the categorization through DRGs could give health system managers information about which prices for treatments can be reduced without af- fecting quality standards but can also provide a warning when lower prices begin to be associated with deterioration of outcomes. DRGs; Clinical budgets; U.K. Introduction How are we to maintain adequate standards in the quality of care, and even continue to improve standards, during a future of increasingly effective health pro- gramme cost constraints? The answers suggested in this paper are two: first, that both of the most pow- erful cost controls so far developed (by which I mean prospective treatment pric- ing and clinical budgeting) can be used as a basis for quality management; second, that because in future cost/outcome quality trade-offs can be analysed better, pre- cisely because of the lack of ambiguity in these two financial controls, this preci- sion presents us all with an opportunity that should not be missed. * Revised version of a paper presented at the 3rd Symposium on Health and Economics, Universitaire Instelling Antwerpen, Belgium, September 12-13, 1985. Address for correspondence: Iden Wickings, Ph.D., Deputy Secretary, King Edward’s Hospital Fund, 2 Palace Court, Bayswater. London W2 4HT, U.K. 0168-8510/87/$03.50 0 1987 Elsevier Science Publishers B.V. (Biomedical Division)
Transcript
Health Policy, 7 (1987) 216-226 Elsevier
215
HPE 00144
Combining clinical budgets and DRGs for quality management*
lden Wickings
CASPE Research, King Edward’s Hospital Fund, London, U.K.
Accepted 6 January 1987
Summary
Global and clinical budgets are being introduced in the U.K. as elsewhere to con- trol health care costs. They are in fact showing effectiveness in terms of cost-con- trol. They do not, however, adequately address outcomes and quality of care. DRGs could be used as a tool for associating costs with outcome and quality measures. lf constructed carefully, the categorization through DRGs could give health system managers information about which prices for treatments can be reduced without af- fecting quality standards but can also provide a warning when lower prices begin to be associated with deterioration of outcomes.
DRGs; Clinical budgets; U.K.
Introduction
How are we to maintain adequate standards in the quality of care, and even continue to improve standards, during a future of increasingly effective health pro- gramme cost constraints?
The answers suggested in this paper are two: first, that both of the most pow- erful cost controls so far developed (by which I mean prospective treatment pric- ing and clinical budgeting) can be used as a basis for quality management; second, that because in future cost/outcome quality trade-offs can be analysed better, pre- cisely because of the lack of ambiguity in these two financial controls, this preci- sion presents us all with an opportunity that should not be missed.
* Revised version of a paper presented at the 3rd Symposium on Health and Economics, Universitaire Instelling Antwerpen, Belgium, September 12-13, 1985.
Address for correspondence: Iden Wickings, Ph.D., Deputy Secretary, King Edward’s Hospital Fund, 2 Palace Court, Bayswater. London W2 4HT, U.K.
Recent history in the four main levels of decision taking
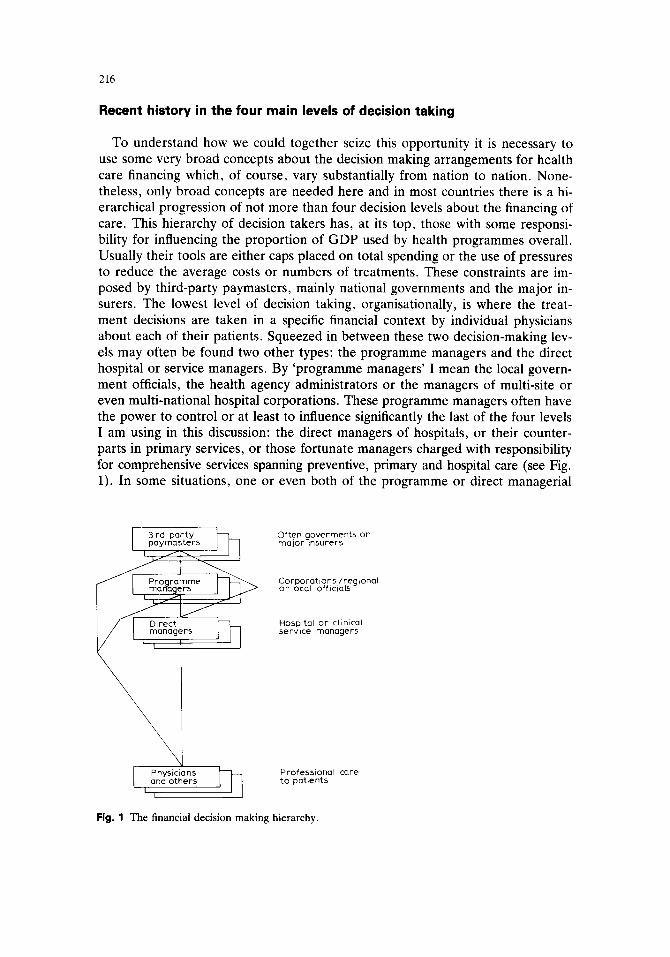
To understand how we could together seize this opportunity it is necessary to use some very broad concepts about the decision making arrangements for health care financing which, of course, vary substantially from nation to nation. None- theless, only broad concepts are needed here and in most countries there is a hi- erarchical progression of not more than four decision levels about the financing of care. This hierarchy of decision takers has, at its top, those with some responsi- bility for influencing the proportion of GDP used by health programmes overall. Usually their tools are either caps placed on total spending or the use of pressures to reduce the average costs or numbers of treatments. These constraints are im- posed by third-party paymasters, mainly national governments and the major in- surers. The lowest level of decision taking, organisationally, is where the treat- ment decisions are taken in a specific financial context by individual physicians about each of their patients. Squeezed in between these two decision-making lev- els may often be found two other types: the programme managers and the direct hospital or service managers. By ‘programme managers’ I mean the local govern- ment officials, the health agency administrators or the managers of multi-site or even multi-national hospital corporations. These programme managers often have the power to control or at least to influence significantly the last of the four levels I am using in this discussion: the direct managers of hospitals, or their counter- parts in primary services, or those fortunate managers charged with responsibility for comprehensive services spanning preventive, primary and hospital care (see Fig. 1). In some situations, one or even both of the programme or direct managerial
Often goverments or major ~nwrers
Corporatlons/reglonaI or local Off Iclals
and others Professional care to patents
Fig. 1 The financial decision making hierarchy.
217
levels may be absent, but this will not affect the broad principles of what is dis- cussed below.
Up until the last decade, the third-party paymasters’ regular attempts to limit spending were not very successful as one can see from the considerable growth in the proportion of the GDP that most countries spent during the sixties and sev- enties on health care. As an example of this growth, the OECD average for 20 countries, excluding Luxembourg, Portugal, Switzerland and Turkey, for the pe- riod 1960-1983 records a move in the percentage from 4.1 to 7.6 (1) But the third- party controls have slowly begun to be more successful, or certainly more pow- erful, as lessons have been learned. Iglehart, writing about the U.S.A. in 1986 noted: ‘Since 1981, reductions in Medicare expenditures (about 40 billion dollars) have totaled 12 percent of all federal budget reductions, although the program represents only 7 percent of federal outlays’. (2) In particular the use of Diagnosis Related Groups (DRGs) has had a dramatic impact. These various American con- trols have also had considerable influence on third-party paymasters in other coun- tries, who see themselves as facing the same challenge as those in the U.S.A. But there have been some significant differences in the responses to these challenges and we have seen the programme and hospital managers in several affluent coun- tries implementing some techniques of their own, such as the use of global, frame and clinical budgets, local tariffs, capitation limits, peer reviews and manpower, equipment and facility caps. One important development in the U.S.A., however, which may soon have a wider application, has been the emergence of HMO’s for which there are as yet few parallels elsewhere.
Inevitably, these financially successful controls are beginning to pose a real risk that adequate quality standards for health care will be jeopardised at some time in the future. This threat to quality may neither present a widespread problem as yet, nor even be an imminent hazard for some countries, but it seems certain to become a substantial policy issue during the next decade.
Undoubtedly one of the most powerful of all the tools developed has been the use of DRGs and most international interest thus far has focussed on their cost- cutting potential. However, DRGs should not be seen as solely a method of con- trolling costs. Used imaginatively, and particularly if linked with clinical budgets, as I will suggest below, they could contribute to local, national and international analyses of cost/outcome/quality trade-offs. In turn these analyses could when ap- propriate lead to revisions of DRGs as a categorisation method, to the informed review of national or local financial tariffs, and to the quality-aware determination of specific clinical or programme budgets. Of course, there would need to be a genuine concern with cost and quality trade-offs within all the managerial levels I have identified and not merely the unthinking lip-service which is at present more customary. But such a concern could introduce a feed-back loop into the system which could powerfully influence all the principal actors, that is to say the third- party paymasters, the programme managers, the direct managers and the physi- cians. This new feed-back loop should use mainly statistical and epidemiological evidence but studies could be initiated upon the basis of concerns expressed by physicians. The feed-back should also encourage genuinely cost-effective behav-
218
Fig. 2 A language for health management? A stepped progression of symbiotic relationships.
iours at the level where treatment decisions are made. What would be required is shown schematically in Fig. 2.
In the immediately following sections I shall describe some of the controls that have often been introduced by the three broad levels of decision taking above the physicians that I am using in this discussion. I shall only give a few instances of the types of controls being used, because it is the general relationship between the controls and outcome quality which concerns me here. It will be seen in each case, however, that these resource constraints create dangers for those trying to main- tain or improve the quality of care: therefore although the controls may bring im- provements in efficiency they may hazard true effectiveness. In the final two sec- tions I will discuss how DRGs could be used as the basis for improved quality management in hospital care.
The third-patty paymasters
In relation to their health care responsibilities national and local governments, and the major commercial and public health insurers, are under great financial pressures in many countries. In the Northern hemisphere, and in the more devel- oped parts of the South, the pressures are frequently designed to control either the total level of national spending on health care or to reduce the taxation or insur- ance ‘prices’ charged, whether these are levied upon the individual citizen, or his employer, or on the work-force and industry more generally.
As a consequence of these forces third-party paymasters in virtually all coun- tries now ration health care by one means or another [3,4]. Sometimes the meth- ods used are price controls, or limits upon the types of treatment that may be of- fered. At other times, controls are placed upon the number of physicians who may practice, or the numbers of hospitals, or the authorised types of, and locations for,
219
new technology. There are also examples of financially poor citizens being ex- cluded from care - indeed this can be seen quite widely and not least in what is certainly one of the richest countries in the world [5].
To be effective all of these third-party controls need to be broadly acceptable to the public and indeed at times they have been actively encouraged by the com- munities served. In this area, the U.S.A. has again been in the forefront where changes in public opinion and consequential political actions are concerned. This rather surprising level of public support for controls on the cost of health care has probably been due to two factors. Firstly, the escalation in health care expenditure as a proportion of GDP has worried many observers. In the U.S.A., which has often led both public and political opinion in this area, the share of GDP grew from 5.3 to 10.8 percent between 1960 and 1983. This veritable explosion pro- duced some cynical and scare-mongering forecasts implying that, for instance, the whole of the U.S.A.‘s economy would be devoted to health care by some pre- dictable date. The rate of growth has varied internationally but the second factor has in no sense been peculiar to the U.S.A. Everywhere there have been occa- sional examples of inefficiency, extravagance or even financial greed within the health care industry. This has been the more shocking to communities in which there has been a history of charitable or religious involvement in health care. The results everywhere have been at least some limited public support for controls.
In most developed countries it is reasonable to assume that several years will have to pass before these controls will bite too deeply into health care standards and outcomes. As with all other large industries there is much waste to be rede- ployed and efficiency can be enhanced almost endlessly. To support this assertion it can be noted that even in the United Kingdom, where health care expenditure levels and their relative growth have been much less than in many other countries, there is abundant evidence both of inefficiency and of unacceptably wide varia- tions in professional practice, as James Coles and I have pointed out previously [6]. After all no-one can justify 24-fold variations in X-ray use, or 4-fold variations in length of hospital stay, for comparable cases. But the effects of financial con- trols imposed at the highest managerial levels are somewhat unpredictable and the third-party paymasters are too far from the patient’s bedside for their judgements to be unimpeachable. It may therefore be prudent for us to prepare to defend health care standards against what may be arbitrary controls.
Let me give just two examples, the first from the U.K. Changes were introduced by the Government a short while ago under which many, but not all, patients have to pay for a higher proportion of the total costs of their dental care, despite being partly covered by the NHS. Not surprisingly, this has been attacked by the British Dental Journal, which can claim to speak for the whole dental profession, many of whose members admittedly have a pecuniary interest in this topic. But, whether or not speaking with true objectivity, the Journal has reported that there is now a trend towards a proportion of patients choosing to have their bad teeth extracted, because they have found this costs them less than having crowns and bridges fit- ted. In Britain, such choices would not have to be made by the poorest citizens, because they get free treatment, but such decisions do face low or average earn-
220
ers. Similarly, in the U.S.A., DRGs have had a major benificial influence in so far as improvements in efficiency are concerned; but we should not forget that DRGs are also alleged to have had some undersirable outcomes, at least according to the American Medical Association. For instance Dawson has claimed that a survey re- vealed that 66 percent of respondents held that quality had deteriorated and 85 percent reported that at least one DRG was inadequately reimbursed [2]. The same type of allegations have been made by Gardner [7]. It would be miraculous, of course, if such powerful changes had not produced some problems, but I have quoted these examples because they are early indicators of the types of risk that tighter cost controls inevitably create.
What is needed is a method of feed-back under which the third-party paymas- ters, and more importantly the public, can see when health care cost controls are genuinely beginning to damage standards of care, and then make better balanced judgements.
The programme managers
Earlier I used the term programme managers to include the local government officials, the health agency administrators for regions and the managers of large hospital chains of national or even international health care corporations. Histor- ically, the programme managers have been willing to accept and publicly justi? properly incurred costs or to approve plans and developments to meet actual or anticipated workload growths. Historically, the assumption has been made that any clinically sanctioned work has been needed medically by the patient. This led to post-hoc reimbursement of any costs incurred in patient care, unless they were in some manner outrageous. However, that position has been changing for some years. One of the tools now being used more widely in this connection is the global budget. Examples of these global, or frame, budgets can be seen in Scandinavia, Canada, U.S.A., Eire, The Netherlands, the United Kingdom and elsewhere. Their distinctive characteristics are firstly that, at least in the short term, the budget for the region, hospital, primary care service or whatever will not be adjusted auto- matically to reflect any increased numbers of treatments; secondly, the overall sum of money to be made available may be specified but (as distinct from line budgets) thereafter the direct hospital or even the service managers (who may well be phy- sicians) have discretion within that budgeted resource cap to decide upon the lo- cally preferred detailed expenditure pattern.
An example of the dangers posed by these particular powerful financial con- trols, operating at the programme level, can be quoted from the United Kingdom. Here global budgets have been applied for some years to both regional and local health authorities. Often, the budgets have been determined in relation to a for- mula largely based on the population served and paying little heed to the treat- ments actually provided for that population. At a regional level, often serving populations of several millions, this system seems to have worked well in achieving greater equity in resource distribution. But the same may not be true where smaller populations are concerned. These budgets, particularly where they have been held
221
constant or been reduced in real terms, have led to a dramatic fall in the number of hospital beds. Particularly in central London, many thousands of beds have been closed. It is true that the speed of treatment has been correspondingly increased with the result that more patients have still been treated in fewer hospitals. But this has led to a growing pressure upon community-based services which may, in certain cases, cost more to provide [8,9].
There have been important but unanticipated consequences from the vigorous introduction of global budgets in the U.K. Previously hospital physicians regarded it as a sign of high quality work if they attracted patients from far and wide. Con- versely, the hospital specialist in any major centre who only had patients referred to him by general practitioners working in his immediate locality might suspect that his reputation was not of the highest. Although this was a very crude and unreli- able measure, hospital physicians often talked of the number of patients referred to them as an important quality indicator. The position has begun to change in the U.K. because global budgets will often encourage a reduction to, or limits on, the number of patients treated. They will certainly do so if the system promises mar- ginal increases to future global budgets which only seem to compensate poorly for the immediate costs of providing high-cost treatments today to patients referred from afar. Yet, crude and unreliable as this quality indicator might have been in the past, as yet we have nothing much better to put in its place, while the trend towards more local referral patterns in the London area continues.
Another area in which pressures from programme managers may, in many countries, jeopardise quality concerns the lengths of acute hospital stay. Once again, no commentator could justify the widespread variations seen within individual countries as well as internationally but there is no evidence that shorter treatments are always superior. Probably shorter stays will more often than not reflect more
20- ,,’ .’
,’ 10 6’ a /
0 10 20 30 40 50 60 70 80 90 100
Cumulative % bed-days
Fig. 3 DRG-150. Peripheral vascular disorders.
222
effective care. Harper showed this to be true in his own surgical practice in 1979 and the position is unlikely to have changed [lo]. Common sense also suggests that better care will improve the patient’s condition sooner in most diagnoses and thus allow earlier discharge. Nevertheless shorter stays will not always be beneficial and a feed-back loop is required to show nationally and at a local level, and on a con- tinual basis because circumstances change, when quality is at risk. By way of con- trast, Fig. 3 shows that in one English health authority with which I have worked those physicians who treated the most patients in a given DRG did so more effi- ciently than their colleagues. We have found the same thing with other specialties with different health authorities. Their greater efficiency may well be associated with better care. A cardiac surgeon working in England has similarly reported that mortality rates following surgery for ischaemic heart disease were lower in the busier units [ll] and other centres have produced similar results. So the issue is not that it is unreasonable for programme managers to push for reductions in the average length of stay, but that it is irresponsible for them to do so without a feed- back loop monitoring any effects on the quality of care.
The use of clinical budgets
The direct hospital and service managers have felt themselves to be increasingly pressurised either by economic factors generally or by some combination of global budgets or price controls like DRGs. In consequence they have themselves begun to introduce budgets for clinical services [12,13]. Sometimes these have been flex- ibly linked to the numbers or types of patients treated. Sometimes they have not, when they could be regarded as small scale examples of global budgets.
Clinical budgets are introduced for various different purposes. One purpose is simply to gain more control over clinically initiated expenditures. Another, which is more relevant to the theme of this symposium, is to offer an incentive to phy- sicians to use resources better [14]. For instance, if the clinical budget is finite and the physician wants to introduce an improvement to his service then there is an incentive for the physician to search for and then abandon his least valued current practice. In this way he can afford his preferred improvement. There is good evi- dence now from many countries that clinical budgets do provide an incentive of this type, leading to more cost-efficient behaviour [15,16]. These clinical budgets are generally acceptable to physicians who value the opportunity to make resource switching choices in hard times [17]. It is now planned that budgets for clinical services will be used throughout the NHS although they will not invariably afford incentives to the physicians affected [18]. The British case for their adoption mainly relies upon the evidence that they improve physician efficiency and that physicians can be given more discretion about spending choices and not less. Whether ben- efits will follow from the use of imposed budgets that offer physicians no greater discretion over spending choices seems to me to be far from certain. But the phy- sicians can only be given more discretion if they stay within their allocated budg- ets. Any powerful budgeting system working at the level of the individual physi- cian, or physicians in small groups, may encourage efficiency (which I define as
223
cian, or physicians in small groups, may encourage efficiency (which I define as undertaking the preferred task for less cost) but it may not necessarily encourage effectiveness (which may be regarded as encouraging physicians’ behaviours that will have the maximum effect for any given cost upon the natural course of the illness or disease).
Once again, it is obvious that budgets for clinical services can be imposed by those I have called the direct managers and that the finances could easily be re- duced, over time, to the point at which there would be a real threat to the main- tenance or continuing improvement of standards of care. How could this threat be minimised or avoided?
Using DRGs to improve quality
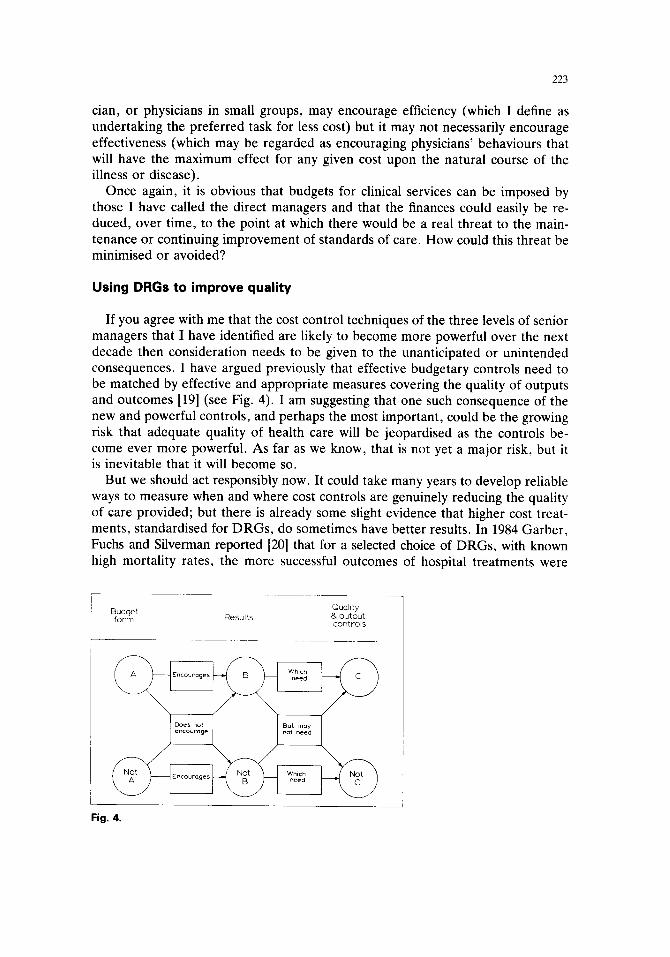
If you agree with me that the cost control techniques of the three levels of senior managers that I have identified are likely to become more powerful over the next decade then consideration needs to be given to the unanticipated or unintended consequences. I have argued previously that effective budgetary controls need to be matched by effective and appropriate measures covering the quality of outputs and outcomes [19] ( see Fig. 4). I am suggesting that one such consequence of the new and powerful controls, and perhaps the most important, could be the growing risk that adequate quality of health care will be jeopardised as the controls be- come ever more powerful. As far as we know, that is not yet a major risk, but it is inevitable that it will become so.
But we should act responsibly now. It could take many years to develop reliable ways to measure when and where cost controls are genuinely reducing the quality of care pr~ovided; but there is already some slight evidence that higher cost treat- ments, standardised for DRGs, do sometimes have better results. In 1984 Garber, Fuchs and Silverman reported [20] that for a selected choice of DRGs, with known high mortality rates, the more successful outcomes of hospital treatments were
Budget form Results
Quality B output controls
Fig. 4.
224
associated with higher cost treatment programmes. It must be said that, in their study, the benefits were not maintained for very many months after the patients’ discharge dates but the particular choice of DRGs may have explained this fully. However, at other times the less expensive treatments will be associated with the better care, just as Harper found (op tit). Sometimes, studies of associations be- tween resource use and outputs produce unanticipated results, as when Cochrane et al. found, in a review spanning 18 countries, that there was a positive associa- tion between a prevalence of physicians and mortality rates in the younger age groups [21]. The difficulty, at present, is that there is no consistent effort being made anywhere, to the best of my knowledge, to assess when reductions in the average costs of treating particular diagnoses are associated with worse results. But we cannot ignore this longer term risk and should now begin to establish appro- priate arrangements. A good beginning has been made at a broader level in this field already. For instance, Newhouse et al. have studied HMOs [22] and Holland et al. are analysing geographical variations in mortality from conditions amenable to medical intervention [23] but the whole array of routine patient care will have to be studied in due course.
The growing international use of DRGs and the various forms of clinical budg- eting provide a suitable opportunity for us. If efforts were made internationally to record the outcomes associated with particular DRGs then those outcomes could be related to the particular standard price and typical resource use for that treat- ment. The advantage of doing this within a framework of clinical budgets is that physicians will have the capacity to introduce developments in the treatment of one diagnostic group at the expense of changes in the treatments offered to patients in another DRG. They will only do this when the foregone expenditure is valued very little and will not significantly damage patient care. All of us would be able to learn from both changes if they are carefully validated.
Initially the societal pressures for more efficiency, to which I have already re- ferred, are likely to lead to a reduction in real cost terms of the reimbursements offered for each DRG. If the expected case mix to be treated helps to shape the clinical budget then we should expect that these budgets will often also reduce, or at least not increase. After all, to achieve an improvement in efficiency is a desir- able aim for us all. Only when lower prices begin to be associated with worsening outcomes would it be time to call a halt. However, I suspect that in most DRG reimbursement schedules considerable cost reductions could be achieved without sacrificing quality. This is because there is no reason to suggest that the average pattern of treatment is particularly efficient as yet.
I believe this to be the case not least because, in the U.K., we have found that considerably greater lengths of stay occur when physicians treat patients in a DRG that is seldom admitted to their service. This suggests that carefully referring pa- tients into the hands of the most appropriate physicians could itself, at least in some situations, reduce average costs for a particular DRG.
225
Conclusion
Controls on health care spending are at last becoming more effective. At pres- ent, such controls appear to be needed and to have wide public support. However, at some stage in the future such controls could begin to reduce outcome/quality standards and there is some slight evidence already available to support this as- sertion.
Clinical budgets and DRGs are tools that allow society to select the costs to be met for particular clinical services and diagnoses. Clinical budgets provide an in- centive for more efficient physician behaviour but do not address outcomes ade- quately. DRGs constrain physician choices and encourage efficiency; but they could also facilitate peer group comparisons within institutions, within countries and in- ternationally.
True effectiveness, however, requires that the expenditure options selected are those that will, on balance, most powerfully alter the patients’ conditions for the better. Using DRGs as a primary categorisation, with which outcomes and quality measures can be associated through research, could allow the necessary feed-back loop to be constructed. This could alert managers, at all the levels I have identified to an awareness that falling standards could follow, or are already following, cuts or other constraints that they may be imposing upon standard prices for treat- ments. However, constructing such a data base would also allow health system managers to continue to reduce standard prices up to the point that disbenefits be- gin to show. International comparisons will be crucial here. Moves towards im- proving efficiency could therefore be made with more, rather than less, confidence if this research was in progress. Providers have a long way to go in improving cost effective behaviour but it is now that we should be setting up advance warning sys- tems; we should not wait until it is too late.
References
1 OECDIODCE, Measuring Health Care 196C-1983, Paris, 1985, p. 12. 2 Iglehart, J.K., ‘Early experience with prospective payment of hospitals’ New England Journal of
Medicine, 314 (1986) 1460-1464. 3 Schwarz W.B., and Aaron, H.J., Special Report, Rationing Hospital Care: Lessons from Britain.
New England Journal of Medicine, 311 (1984) 52-56. 4 Jonsson B., The Costs of Health Care: Trends and Determining Factors, Scandinavian Journal of
Social Medicine, Suppl. 28 (1981). 5 Lune. N., Ward, N.B., Shapiro, M.F. and Brook, R.H. Termination from Medi-Cal. Does it affect
health? New England Journal of Medicine, 311 (1984) 480-484. 6 Wickings, I. and Coles, J. The ethical imperative of clinical budgeting, NuffielcUYork Portfolios No.
10, Nuffield Provincial Hospitals Trust, London, 1985. 7 Gardner, B.. The impact of DRGs on surgical practice, Surgery, Gynaecology and Obstetrics, 159
(1984) 75-76. 8 Wright, K. and Haycos, A., Costs of Alternative Forms of NHS care for mentally handicapped per-
sons, Discussion Paper No. 7, University of York, 1985. 9 Vinten. G., Study into the costing of Community Health Services, Medway H.D., Kent, England,
1981. 10 Harper. D.R., Disease cost in a surgical ward, British Medical Journal i (1979) 647-649.
226
11 English, T., The UK Cardiac Surgical Register. CASPE Seminar Report: Output Measurement and Costs, CASPE Research, London, 1983.
12 Heyssel, R.M., Gaintner, J.R., Kues, I.W., Jones, A.A. and Lipstein, S.H., Decentralised man- agement in a teaching hospital, New England Journal of Medicine, 310 (1984) 1477-1480.
13 Wickings, I., Coles, J.M., Flux, R. and Howard, L., Review of clinical budgeting and costing ex- periments, British Medical Journal, i (1983) 575-578.
14 Wickings, I., Incentives, Budgets and Planning Agreements for Clinical Teams, In Hospital Costing and the Clinician, Harrogate Seminar Reports, DHSS, London, 1978, pp. 23-26.
15 Walker, J.S., A year’s experience of functional budgeting in a clinical department, Anaesthesia, 36 (1981) 316318.
16 Bally, Y.. Clinical budgeting in the NHS, or going Dutch (Swedish French), Health Economics Re- search Unit, University of Aberdeen, 1982, pp. 20, 22, 38.
17 Anonymous, If I was forced to cut British Medical Journal, ii (1979) 905-906. 985-986. 1057-1058, 1203-1204, 1276-1277, 1351-1352, 1570-1571.
18 Griffiths, R. et al., NHS Management Inquiry, DHSS, London, 1983. 19 Wickings, I., Is there a general theory for health care budgeting? Effective Health Care, V. 2 (1984)
51-56. 20 Garber, A.M., Fuchs. V.R. and Silverman J.F., Case Mix, Costs and Outcomes, New England
Journal of Medicine, 310 (1984) 1231-1237. 21 Cochrane, A.L., St. Leger, A.S. and Moore, F., Health service input and mortality output in de-
veloped countries, J. Epid. and Comm. Health, 32 (1978) 200-205. 22 Newhouse, Joseph P. et al., Comparison of health outcomes at a Health Maintenance Organisation
with those of Fee-For-Service care, The Lancet, i (1986) 1017-1022. 23 Holland, W. W, et al., Geographical variation in mortality from conditions amenable to medical in-
tervention in England and Wales, The Lancet, i (1983) 691-696.