21
USVI HEALTH CARE CLAIM 837 Companion Guide Version 0.1 February 6, 2013
USVI HEALTH CARE CLAIM 837 Companion Guide
Version 0.1
February 6, 2013

February 6, 2013 2 837 Companion Guide
Table of Contents
1.0 COMPANION GUIDE PURPOSE .............................................................................. 4
2.0 ATYPICAL PROVIDERS ........................................................................................... 4
3.0 CONTROL STRUCTURE DEFINITIONS .................................................................. 5
3.1 ISA - INTERCHANGE CONTROL HEADER SEGMENT ............................... 5
3.2 IEA - INTERCHANGE CONTROL TRAILER .................................................. 5
3.4 GE – FUNCTIONAL GROUP TRAILER ......................................................... 6
3.5 VALID DELIMITERS FOR USVI MEDICAID .................................................. 6
4.0 TRANSMISSION CONSTRAINTS ............................................................................. 6
5.0 COMPANION GUIDE FOR THE 837 PROFESSIONAL TRANSACTION ................ 7
6.0 COMPANION GUIDE FOR THE 837 INSTITUTIONAL TRANSACTION ............... 11
6.1 ADDITIONAL PROVIDER INFORMATION .................................................. 17
7.0 COMPANION GUIDE FOR THE 837 DENTAL TRANSACTION ............................ 18

February 6, 2013 3 837 Companion Guide
Record of change
DATE DESCRIPTION OF CHANGE ORIGINATOR
11/1/12 Created to reflect 5010 USVI EDI
2/6/13 QA Review M. Searcy
The Molina Healthcare Companion Guide for USVI Medicaid is subject to change prior to July 1, 2013 or at the instruction of the Department. Therefore, it is the responsibility of the trading partner to ensure that the latest version of this guide is used when designing\building NX12 5010 EDI transactions. The trading partner should frequently check for updates to the companion guide. Molina Healthcare accepts no liability for any costs that the trading partner may incur that arise from or are related to changes to the companion guide.

February 6, 2013 4 837 Companion Guide
1.0 COMPANION GUIDE PURPOSE
This companion guide document for the transaction type listed below further defines situational and required data elements that are used for processing claims for programs administered by U.S. Virgin Island Department of Human Services. This document is not the complete EDI transaction format specifications.
2.0 ATYPICAL PROVIDERS
This section is for Atypical Providers (performing non-health care services) who will be permitted to bill using their existing Medicaid ID numbers. The EDI formatting location of Billing, Referring, and Rendering Provider Information is dependent upon the situation being billed. Below are the circumstances and EDI billing locations of this information. Billing Provider Location This is used when the Billing Provider is a servicing provider only and/or if the Billing Provider is the same as the Pay-To Provider.
Loop Header Loop Reference Definition Values Billing Provider Tax Identification
2010AA REF01 Reference Identification Qualifier
‘EI’ or ‘SY’
Billing Provider Tax Identification
2010AA REF02 Billing Provider Additional Identifier
Billing Provider Secondary Identification
2010BB REF01 Reference Identification Qualifier
‘G2’
Billing Provider Secondary Identification
2010BB REF02 Billing Provider Additional Identifier
Billing Medicaid Provider Number
Rendering Provider Name
2310B REF01 Reference Identification Qualifier
‘G2’
Rendering Provider Name
2310B REF02 Reference Identification
Rendering Medicaid Provider Number

February 6, 2013 5 837 Companion Guide
3.0 CONTROL STRUCTURE DEFINITIONS
3.1 ISA - INTERCHANGE CONTROL HEADER SEGMENT
Reference Definition Values ISA01 Authorization Information
Qualifier 00
ISA02 Authorization Information [space fill]
ISA03 Security Information Qualifier
00
ISA04 Security Information [space fill]
ISA05 Interchange ID Qualifier ZZ
ISA06 Interchange Sender ID Insert with the unique number found on your USVI Transaction Information Form.
ISA07 Interchange ID Qualifier ZZ
ISA08 Interchange Receiver ID VI_MMIS_4MOLINA
ISA09 Interchange Date The date format is YYMMDD
ISA10 Interchange Time The time format is HHMM
ISA11 Repetition Separator ^
ISA12 Interchange Control Version Number
00501
ISA13 Interchange Control Number
Must be identical to the interchange trailer IEA02 (defined by sending Trading Partner)
ISA14 Acknowledgment Request 1
ISA15 Usage Indicator T= Test Data P = Production Data
ISA16 Component Element Separator
:
3.2 IEA - INTERCHANGE CONTROL TRAILER
Reference Definition Values IEA01 Number of included
Functional Groups Count of included Functional Groups
IEA02 Interchange Control Number
Must be identical to the value in ISA13
February 6, 2013 6 837 Companion Guide
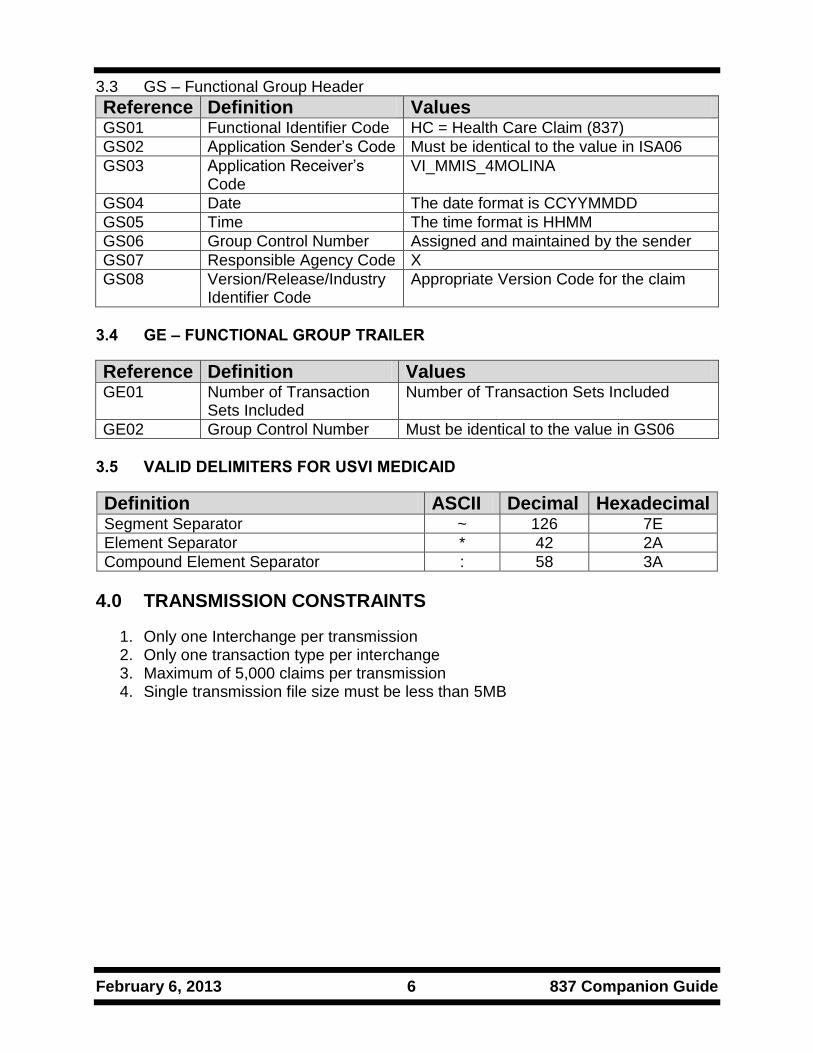
3.3 GS – Functional Group Header
Reference Definition Values GS01 Functional Identifier Code HC = Health Care Claim (837)
GS02 Application Sender’s Code Must be identical to the value in ISA06
GS03 Application Receiver’s Code
VI_MMIS_4MOLINA
GS04 Date The date format is CCYYMMDD
GS05 Time The time format is HHMM
GS06 Group Control Number Assigned and maintained by the sender
GS07 Responsible Agency Code X
GS08 Version/Release/Industry Identifier Code
Appropriate Version Code for the claim
3.4 GE – FUNCTIONAL GROUP TRAILER
Reference Definition Values GE01 Number of Transaction
Sets Included Number of Transaction Sets Included
GE02 Group Control Number Must be identical to the value in GS06
3.5 VALID DELIMITERS FOR USVI MEDICAID
Definition ASCII Decimal Hexadecimal Segment Separator ~ 126 7E
Element Separator * 42 2A
Compound Element Separator : 58 3A
4.0 TRANSMISSION CONSTRAINTS
1. Only one Interchange per transmission 2. Only one transaction type per interchange 3. Maximum of 5,000 claims per transmission 4. Single transmission file size must be less than 5MB
February 6, 2013 7 837 Companion Guide
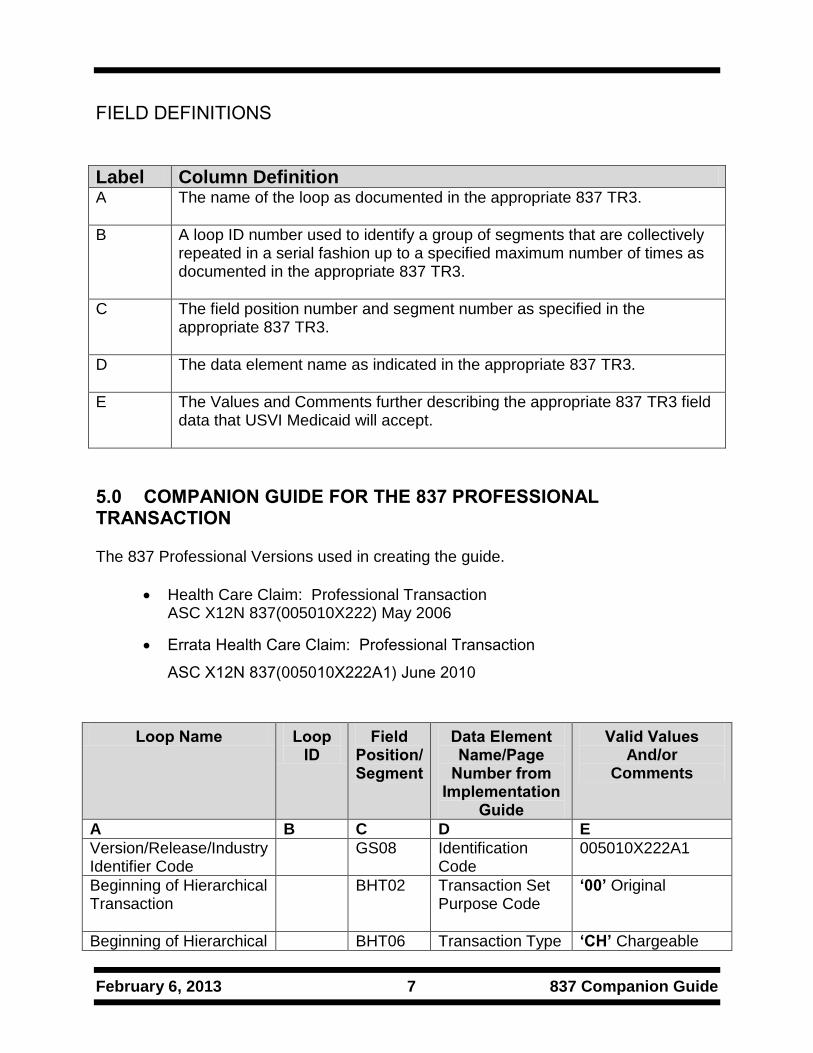
FIELD DEFINITIONS
Label Column Definition A The name of the loop as documented in the appropriate 837 TR3.
B A loop ID number used to identify a group of segments that are collectively repeated in a serial fashion up to a specified maximum number of times as documented in the appropriate 837 TR3.
C The field position number and segment number as specified in the appropriate 837 TR3.
D The data element name as indicated in the appropriate 837 TR3.
E The Values and Comments further describing the appropriate 837 TR3 field data that USVI Medicaid will accept.
5.0 COMPANION GUIDE FOR THE 837 PROFESSIONAL TRANSACTION
The 837 Professional Versions used in creating the guide.
Health Care Claim: Professional Transaction ASC X12N 837(005010X222) May 2006
Errata Health Care Claim: Professional Transaction
ASC X12N 837(005010X222A1) June 2010
Loop Name Loop ID
Field Position/ Segment
Data Element Name/Page
Number from Implementation
Guide
Valid Values And/or
Comments
A B C D E
Version/Release/Industry Identifier Code
GS08 Identification Code
005010X222A1
Beginning of Hierarchical Transaction
BHT02
Transaction Set Purpose Code
‘00’ Original
Beginning of Hierarchical BHT06 Transaction Type ‘CH’ Chargeable

February 6, 2013 8 837 Companion Guide
Loop Name Loop ID
Field Position/ Segment
Data Element Name/Page
Number from Implementation
Guide
Valid Values And/or
Comments
A B C D E
Transaction Code
Submitter Name 1000A NM109 Identification Code
Insert with the unique number found on your USVI Transaction Information Form.
Submitter Contact Information
1000A PER03 Communication Number Qualifier
‘TE’ Telephone Minimum requirement, PER 05 –PER08 may also be sent.
Receiver Name 1000B NM103 Name Last or Organization Name
VI_MMIS_4MOLINA
Receiver Name 1000B NM109 Identification Code
VI_MMIS_4MOLINA
Billing Provider Name
2010AA NM108 Identification Code Qualifier
‘XX’ National Provider ID. Atypical Providers refer to Atypical Section.
Billing Provider Name
2010AA NM109 Identification Code
Billing Provider National Provider ID. Usage changed to situational.
Billing Provider Address 2010AA N403 Postal Code
Billing Provider Zip Code must be the full 9 digits
Subscriber Hierarchical Level
2000B HL04 Hierarchical Child Code
‘0’ No subordinate HL Segment in the Hierarchical Structure
Subscriber Information 2000B SBR09 Claim Filing Indicator Code
MC
Subscriber Name 2010BA NM102 Entity Type Qualifier
‘1’ Person
Subscriber Name 2010BA NM108 Identification Code Qualifier
‘MI’ Member Identification Number
Subscriber Name 2010BA NM109 Identification Code
USVI Medicaid 10 digit Recipient

February 6, 2013 9 837 Companion Guide
Loop Name Loop ID
Field Position/ Segment
Data Element Name/Page
Number from Implementation
Guide
Valid Values And/or
Comments
A B C D E
Number
Payer Name 2010BB NM103 Name Last or Organization Name
VI_MMIS_4MOLINA
Payer Name 2010BB NM108 Identification Code Qualifier
‘PI’ Payer Identification
Payer Name 2010BB NM109 Identification Code
VI_MMIS_4MOLINA
Claim Information 2300 CLM01 Claim Submitter’s Patient Account / Identifier Number
Patient Control Number
Claim Information 2300 CLM06 Yes/No Condition or Response Code
‘Y’ Yes
Claim Information 2300 CLM08 Yes/No Condition or Response Code
‘Y’ Yes
Health Care Diagnosis Code
2300 HI01-2 Industry Code Diagnosis Code
Required on all claims. Transportation claims use 799.0 when unknown.
Referring Provider Name 2310A NM108 Identification Code Qualifier
‘XX’ National Provider ID
Referring Provider Name 2310A NM109 Identification Code
Referring Provider National Provider ID
Rendering Provider Name
2310B NM108 Identification Code Qualifier
‘XX’ National Provider ID
Rendering Provider Name
2310B NM109 Identification Code
Rendering Provider National Provider ID
Rendering Provider Name
2310B PRV01 Provider Code
‘PE’ Performing
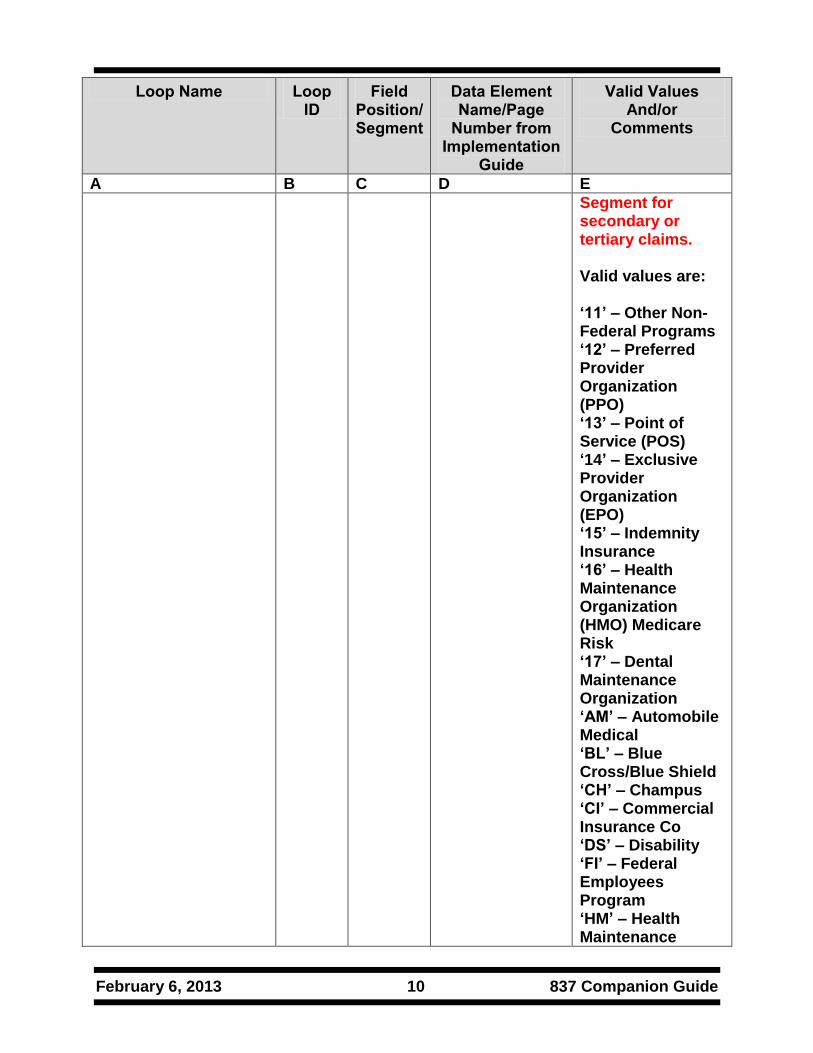
SBR-Other Subscriber Information
2320 SBR09 Claim Filing Indicator Code
Please ensure to use the correct indicator code(s) when billing VI Medicaid as a secondary or tertiary payer. Do not send ‘MC’ in this Position/
February 6, 2013 10 837 Companion Guide
Loop Name Loop ID
Field Position/ Segment
Data Element Name/Page
Number from Implementation
Guide
Valid Values And/or
Comments
A B C D E
Segment for secondary or tertiary claims. Valid values are: ‘11’ – Other Non-Federal Programs ‘12’ – Preferred Provider Organization (PPO) ‘13’ – Point of Service (POS) ‘14’ – Exclusive Provider Organization (EPO) ‘15’ – Indemnity Insurance ‘16’ – Health Maintenance Organization (HMO) Medicare Risk ‘17’ – Dental Maintenance Organization ‘AM’ – Automobile Medical ‘BL’ – Blue Cross/Blue Shield ‘CH’ – Champus ‘CI’ – Commercial Insurance Co ‘DS’ – Disability ‘FI’ – Federal Employees Program ‘HM’ – Health Maintenance
February 6, 2013 11 837 Companion Guide
Loop Name Loop ID
Field Position/ Segment
Data Element Name/Page
Number from Implementation
Guide
Valid Values And/or
Comments
A B C D E
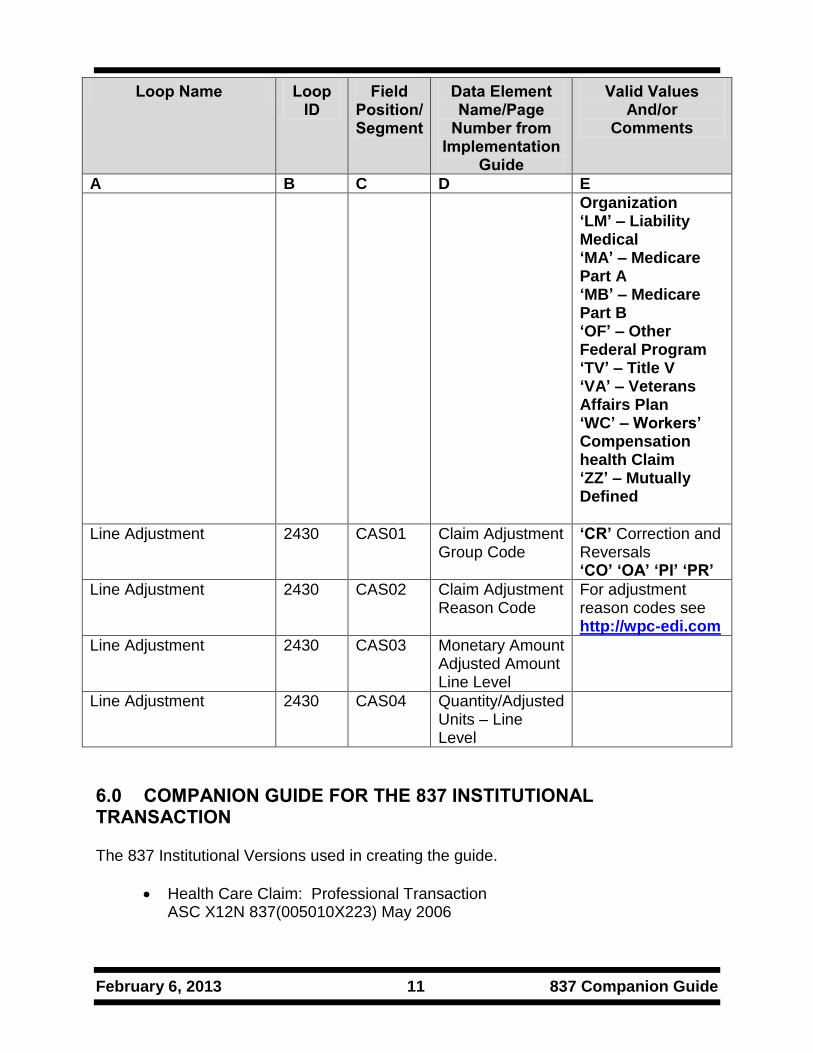
Organization ‘LM’ – Liability Medical ‘MA’ – Medicare Part A ‘MB’ – Medicare Part B ‘OF’ – Other Federal Program ‘TV’ – Title V ‘VA’ – Veterans Affairs Plan ‘WC’ – Workers’ Compensation health Claim ‘ZZ’ – Mutually Defined
Line Adjustment 2430 CAS01 Claim Adjustment Group Code
‘CR’ Correction and Reversals ‘CO’ ‘OA’ ‘PI’ ‘PR’
Line Adjustment 2430 CAS02 Claim Adjustment Reason Code
For adjustment reason codes see http://wpc-edi.com
Line Adjustment 2430 CAS03 Monetary Amount Adjusted Amount Line Level
Line Adjustment 2430 CAS04 Quantity/Adjusted Units – Line Level
6.0 COMPANION GUIDE FOR THE 837 INSTITUTIONAL TRANSACTION
The 837 Institutional Versions used in creating the guide.
Health Care Claim: Professional Transaction ASC X12N 837(005010X223) May 2006
February 6, 2013 12 837 Companion Guide
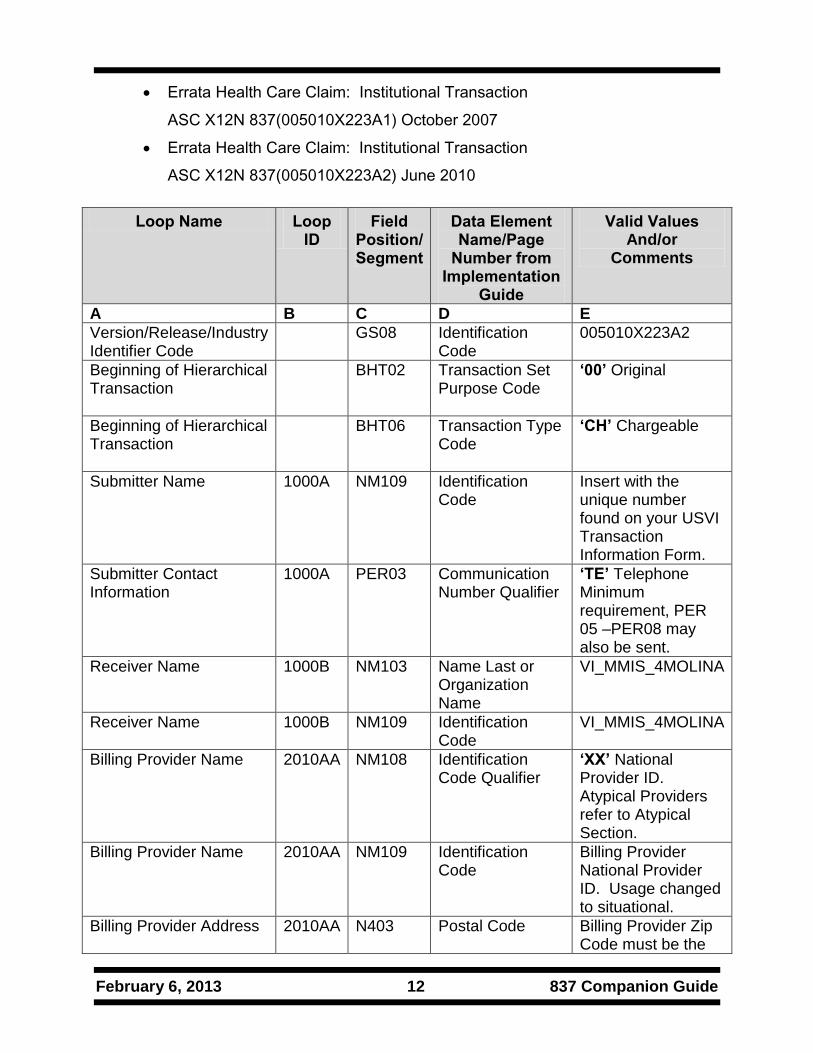
Errata Health Care Claim: Institutional Transaction
ASC X12N 837(005010X223A1) October 2007
Errata Health Care Claim: Institutional Transaction
ASC X12N 837(005010X223A2) June 2010
Loop Name Loop ID
Field Position/ Segment
Data Element Name/Page
Number from Implementation
Guide
Valid Values And/or
Comments
A B C D E
Version/Release/Industry Identifier Code
GS08 Identification Code
005010X223A2
Beginning of Hierarchical Transaction
BHT02
Transaction Set Purpose Code
‘00’ Original
Beginning of Hierarchical Transaction
BHT06
Transaction Type Code
‘CH’ Chargeable
Submitter Name 1000A NM109 Identification Code
Insert with the unique number found on your USVI Transaction Information Form.
Submitter Contact Information
1000A PER03 Communication Number Qualifier
‘TE’ Telephone Minimum requirement, PER 05 –PER08 may also be sent.
Receiver Name 1000B NM103 Name Last or Organization Name
VI_MMIS_4MOLINA
Receiver Name 1000B NM109 Identification Code
VI_MMIS_4MOLINA
Billing Provider Name
2010AA NM108 Identification Code Qualifier
‘XX’ National Provider ID. Atypical Providers refer to Atypical Section.
Billing Provider Name
2010AA NM109 Identification Code
Billing Provider National Provider ID. Usage changed to situational.
Billing Provider Address 2010AA N403 Postal Code
Billing Provider Zip Code must be the

February 6, 2013 13 837 Companion Guide
Loop Name Loop ID
Field Position/ Segment
Data Element Name/Page
Number from Implementation
Guide
Valid Values And/or
Comments
A B C D E
full 9 digits
Subscriber Hierarchical Level
2000B HL04 Hierarchical Child Code
‘0’ No subordinate HL Segment in the Hierarchical Structure
Subscriber Information 2000B SBR09 Claim Filing Indicator Code
MC
Subscriber Name 2010BA NM102 Entity Type Qualifier
‘1’ Person
Subscriber Name 2010BA NM108 Identification Code Qualifier
‘MI’ Member Identification Number
Subscriber Name 2010BA NM109 Identification Code
USVI Medicaid 10 digit Recipient Number
Payer Name 2010BB NM103 Name Last or Organization Name
VI_MMIS_4MOLINA
Payer Name 2010BB NM108 Identification Code Qualifier
‘PI’ Payer Identification
Payer Name 2010BB NM109 Identification Code
VI_MMIS_4MOLINA
Claim Information 2300 CLM01 Claim Submitter’s Patient Account / Identifier Number
Patient Control Number
Claim Information 2300 CLM06 Yes/No Condition or Response Code
‘Y’ Yes
Claim Information 2300 CLM08 Yes/No Condition or Response Code
‘Y’ Yes
Discharge Hour 2300 DTP01 Date Time Period Discharge Hour
‘096’
Claim Information 2300 DTP02 Date Time Period Format Qualifier
‘TM’
Admission Date/Hour 2300 DTP01 Date Time Qualifier
‘435’
Admission Date/Hour 2300 DTP02 Date Time Period Format Qualifier
‘D8’ or ‘DT’
Admission Date/Hour 2300 DTP03 Date Time Period
Institutional Claim Code 2300 CL101 Admission Type

February 6, 2013 14 837 Companion Guide
Loop Name Loop ID
Field Position/ Segment
Data Element Name/Page
Number from Implementation
Guide
Valid Values And/or
Comments
A B C D E
Code
Institutional Claim Code 2300 CL102 Admission Source Code
Institutional Claim Code 2300 CL103 Patient Status Code
Prior Authorization or Referral Number
2300 REF01 Reference Identification Qualifier
‘G1’ Prior Authorization Number
Prior Authorization or Referral Number
2300 REF02 Reference Identification Prior Authorization Number
Assigned Prior Authorization Number
Other Diagnosis Code 2300 HI01-2 Industry Code Diagnosis Code
Use appropriate Reference
Principal Procedure Information
2300 HI01-1 Code List Qualifier Code
‘BF’ International Classification of Diseases Clinical Modification (ICD-9-CM)
Principal Procedure Information
2300 HI01-2 Industry Code Principal Procedure Code
Principal Procedure Code
Other Procedure Information
2300 HI01-1 Code List Qualifier Code
‘BQ’ International Classification of Diseases Clinical Modification (ICD-9-CM) Procedure
Other Procedure Information
2300 HI01-2 Industry Code Procedure Code
Other Procedure Code
Other Procedure Information
2300 HI01-4 Date Time Period Procedure Date
Attending Physician Name
2310A NM108 Identification Code Qualifier
‘XX’ National Provider ID
Attending Physician Name
2310A NM109 Identification Code
Attending Physician National Provider ID
Attending Physician Name
2310A PRV01 Provider Code ‘AT’ Attending
Attending Physician Name
2310A PRV02 Reference Identification Qualifier
‘PXC’ Health Care Provider Taxonomy Code
February 6, 2013 15 837 Companion Guide
Loop Name Loop ID
Field Position/ Segment
Data Element Name/Page
Number from Implementation
Guide
Valid Values And/or
Comments
A B C D E
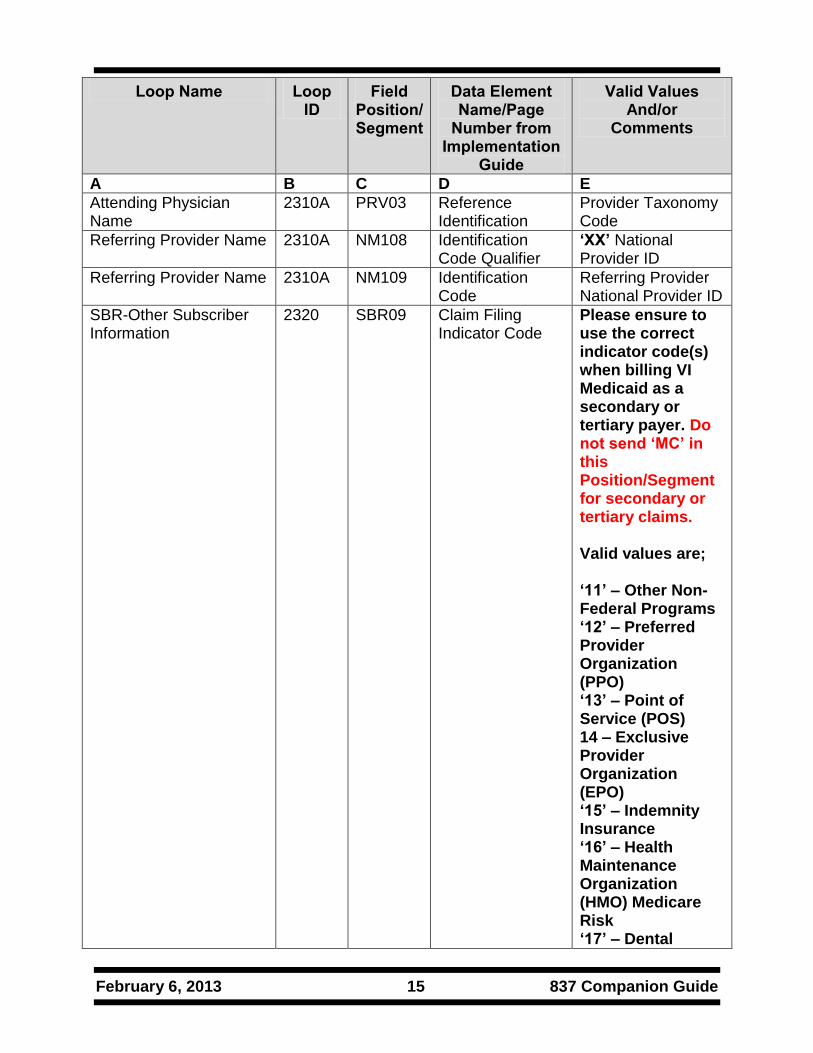
Attending Physician Name
2310A PRV03 Reference Identification
Provider Taxonomy Code
Referring Provider Name 2310A NM108 Identification Code Qualifier
‘XX’ National Provider ID
Referring Provider Name 2310A NM109 Identification Code
Referring Provider National Provider ID
SBR-Other Subscriber Information
2320 SBR09 Claim Filing Indicator Code
Please ensure to use the correct indicator code(s) when billing VI Medicaid as a secondary or tertiary payer. Do not send ‘MC’ in this Position/Segment for secondary or tertiary claims. Valid values are; ‘11’ – Other Non-Federal Programs ‘12’ – Preferred Provider Organization (PPO) ‘13’ – Point of Service (POS) 14 – Exclusive Provider Organization (EPO) ‘15’ – Indemnity Insurance ‘16’ – Health Maintenance Organization (HMO) Medicare Risk ‘17’ – Dental
February 6, 2013 16 837 Companion Guide
Loop Name Loop ID
Field Position/ Segment
Data Element Name/Page
Number from Implementation
Guide
Valid Values And/or
Comments
A B C D E
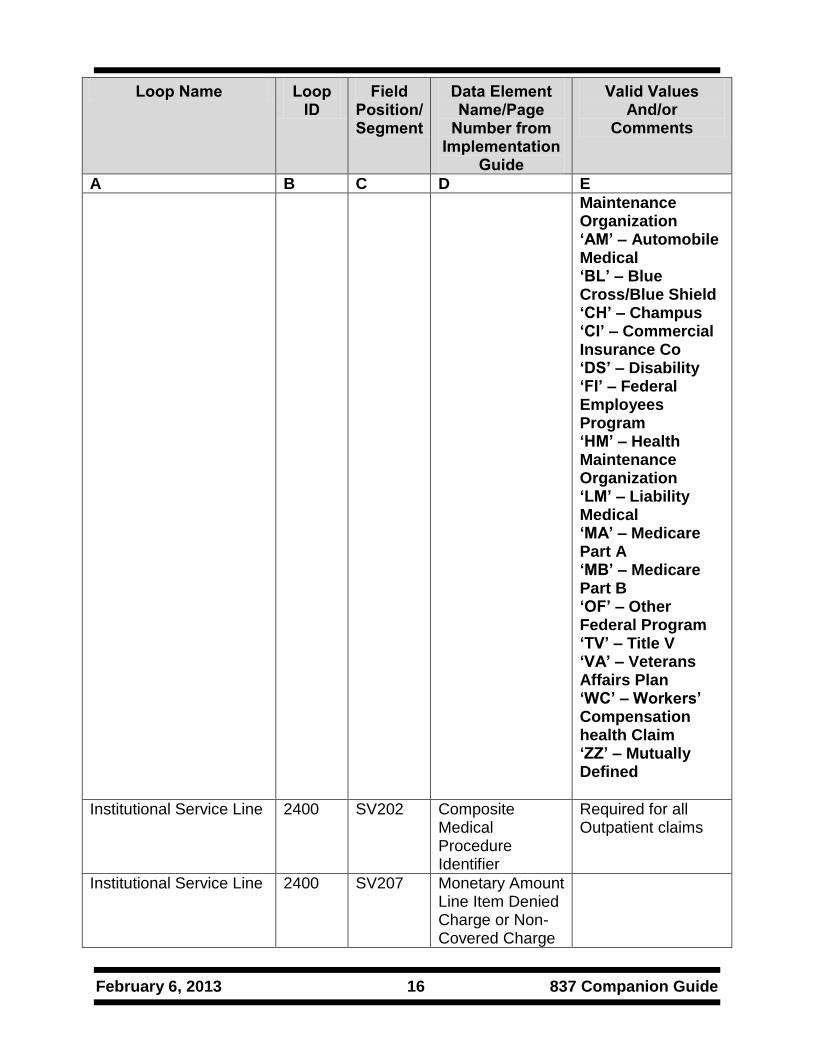
Maintenance Organization ‘AM’ – Automobile Medical ‘BL’ – Blue Cross/Blue Shield ‘CH’ – Champus ‘CI’ – Commercial Insurance Co ‘DS’ – Disability ‘FI’ – Federal Employees Program ‘HM’ – Health Maintenance Organization ‘LM’ – Liability Medical ‘MA’ – Medicare Part A ‘MB’ – Medicare Part B ‘OF’ – Other Federal Program ‘TV’ – Title V ‘VA’ – Veterans Affairs Plan ‘WC’ – Workers’ Compensation health Claim ‘ZZ’ – Mutually Defined
Institutional Service Line 2400 SV202 Composite Medical Procedure Identifier
Required for all Outpatient claims
Institutional Service Line 2400 SV207 Monetary Amount Line Item Denied Charge or Non-Covered Charge

February 6, 2013 17 837 Companion Guide
Loop Name Loop ID
Field Position/ Segment
Data Element Name/Page
Number from Implementation
Guide
Valid Values And/or
Comments
A B C D E
Amount
Line Adjustment 2430 CAS01 Claim Adjustment Group Code
‘CR’ Correction and Reversals ‘CO’ ‘OA’ ‘PI’ ‘PR’
Line Adjustment 2430 CAS02 Claim Adjustment Reason Code
For adjustment reason codes see http://wpc-edi.com
Line Adjustment 2430 CAS03 Monetary Amount Adjusted Amount Line Level
Line Adjustment 2430 CAS04 Quantity/Adjusted Units – Line Level
6.1 ADDITIONAL PROVIDER INFORMATION
Attending Physician NPI Location Required when the claim being billed is for an Inpatient Bill Type. VI Medicaid does not require the use of NPI when billing the Attending Physician number. Therefore the NPI “OR” Legacy ID may be submitted when billing the Attending Physician ID. Loop 2310A
Loop Name Loop ID Field Position/ Segment
Data Element Name/Page Number from
Implementation Guide
Valid Values And/or
Comments
Attending Physician Name
2310A NM108 Identification Code Qualifier ‘XX’ National Provider ID
Attending Physician Name
2310A NM109 Identification Code Attending Physician National Provider ID
Or

February 6, 2013 18 837 Companion Guide
Loop Name Loop ID Field Position/ Segment
Data Element Name/Page Number from
Implementation Guide
Valid Values And/or
Comments
Attending Physician Secondary Identification
2310A
REF01 Reference Identification Qualifier
‘G2’ Medicaid Provider Number
Attending Physician Secondary ID
2310A REF02 Reference Identification
Medicaid Provider Number
7.0 COMPANION GUIDE FOR THE 837 DENTAL TRANSACTION
The 837 Institutional Versions used in creating the guide.
Health Care Claim: Dental Transaction ASC X12N 837(005010X224) May 2006
Errata Health Care Claim: Dental Transaction ASC X12N 837(005010X224A1) October 2007
Errata Health Care Claim: Dental Transaction ASC X12N 837(005010X224A2) June 2010
Loop Name Loop ID Field Position/ Segment
Data Element Name/Page Number from Implementation Guide
Valid Values And/or Comments
A B C D E
Version/Release/Industry Identifier Code
GS08 Identification Code
005010X224A2
Subscriber Hierarchical Level
2000B HL04 Hierarchical Level
‘0’ No subordinate HL Segment in the Hierarchical Structure
Subscriber Hierarchical Level
2000B SBR09 Claim Filing Indicator Code
“MC” Medicaid
Subscriber Name
2010BA NM102 Entity Type Qualifier
“1” Person
Subscriber Name
2010BA NM108 Identification Code Qualifier
“MI” Member Identification Number

February 6, 2013 19 837 Companion Guide
Loop Name Loop ID Field Position/ Segment
Data Element Name/Page Number from Implementation Guide
Valid Values And/or Comments
Subscriber Name
2010BA NM109 Identification Code
USVI Medicaid 10 digit Recipient Number
Payer Name 2010BB NM103 Name Last or Organization Name
VI_MMIS_4MOLINA
Payer Name 2010BB NM108 Identification Code Qualifier
“PI” Payer Identification
Payer Name 2010BB NM109 Identification Code
VI_MMIS_4MOLINA
Claim Information
2300 CLM01 Claim Submitter’s Patient Account
Patient Control Number
Claim Information
2300 CLM11-1 Related Causes Code
“AA” – Auto Accident “OA” – Other Accident
Claim Information
2300 CLM12 Special Program Code
“01‟ EPSDT
Referral Identification
2300 REF01 Reference Identification Qualifier
“G3” Prior Authorization Number
Referral Identification
2300 REF02 Reference Identification Referral Number
Assigned Prior Authorization Number
SBR-Other Subscriber Information
2320 SBR09 Claim Filing Indicator Code
Please ensure to use the correct indicator code(s) when billing VI Medicaid as a secondary or tertiary payer. Do not send ‘MC’ in this

February 6, 2013 20 837 Companion Guide
Loop Name Loop ID Field Position/ Segment
Data Element Name/Page Number from Implementation Guide
Valid Values And/or Comments
Position/Segment for secondary or tertiary claims. Valid values are; ‘11’ – Other Non-Federal Programs ‘12’ – Preferred Provider Organization (PPO) ‘13’ – Point of Service (POS) 14 – Exclusive Provider Organization (EPO) ‘15’ – Indemnity Insurance ‘16’ – Health Maintenance Organization (HMO) Medicare Risk ‘17’ – Dental Maintenance Organization ‘AM’ – Automobile Medical ‘BL’ – Blue Cross/Blue Shield ‘CH’ – Champus ‘CI’ – Commercial Insurance Co

February 6, 2013 21 837 Companion Guide
Loop Name Loop ID Field Position/ Segment
Data Element Name/Page Number from Implementation Guide
Valid Values And/or Comments
‘DS’ – Disability ‘FI’ – Federal Employees Program ‘HM’ – Health Maintenance Organization ‘LM’ – Liability Medical ‘MA’ – Medicare Part A ‘MB’ – Medicare Part B ‘OF’ – Other Federal Program ‘TV’ – Title V ‘VA’ – Veterans Affairs Plan ‘WC’ – Workers’ Compensation health Claim ‘ZZ’ – Mutually Defined
Other Subscriber
2320 AMT02 Monetary Amount Payer Paid Amount
Other Insurance paid Amount

















