Comparison of Dexis CariVu And Bitewing Radiography In Detecting Interproximal Caries In Permanent Teeth BY Ann Mast B.S., B.A., University of North Carolina, Chapel Hill, NC, 2010 D.D.S., University of North Carolina, Chapel Hill, NC, 2014 THESIS Submitted as partial fulfillment of the requirements for the degree of Master of Science in Oral Sciences in the Graduate College of the University of Illinois at Chicago, 2019 Chicago, Illinois Defense Committee Dr. Sahar Alrayyes, DDS, MS, Department of Pediatric Dentistry, Chair and Advisor Dr. Satish Alapati, BDS, MS, PhD, Department of Endodontics Dr. Evelina Kratunova, MDS, MFD, D.Ch.Dent, FFD, Department of Pediatric Dentistry
Transcript
Comparison of Dexis CariVu And Bitewing Radiography In Detecting Interproximal
Caries In Permanent Teeth
BY
Ann Mast B.S., B.A., University of North Carolina, Chapel Hill, NC, 2010
D.D.S., University of North Carolina, Chapel Hill, NC, 2014
THESIS
Submitted as partial fulfillment of the requirements for the degree of Master of Science in Oral Sciences
in the Graduate College of the University of Illinois at Chicago, 2019
Chicago, Illinois
Defense Committee
Dr. Sahar Alrayyes, DDS, MS, Department of Pediatric Dentistry, Chair and Advisor Dr. Satish Alapati, BDS, MS, PhD, Department of Endodontics Dr. Evelina Kratunova, MDS, MFD, D.Ch.Dent, FFD, Department of Pediatric Dentistry
ii
ACKNOWLEDGEMENTS
I would like to thank my primary mentor, Dr. Alrayyes for her tireless effort and dedication
in making this project possible. She was there through all the roadblocks including complete
change of research project topic, obtaining new IRB approval, and seeing this project through to
completion. There were many sleepless nights where Dr. Alrayyes spent working on editing
proposals, protocols, and reviewing images and editing my drafts so that this project could be
completed on time and deadlines could be met. I also want to thank Dr. Alrayyes for her support
and faith in me to complete this project. I also would like to thank Dr. Alapati for his
encouragement and keeping me motivated throughout this entire process. His expertise was a great
contribution to the design of this study. I would like to thank Dr. Kratunova for her optimism and
positivity as well as her contribution as an expert on this project and providing valuable feedback.
Thank you Dr. Koerber for your help on the data analysis and helping me make sense of my data.
I would like to thank my mom and my sister Bonni for their emotional support throughout
this entire process. Thank you for always putting things into perspective and makes me feel like
that no matter what, things will always work out. Lastly, I would like to thank Charlie always
being there by my side through this whole process.
AMM
iii
TABLE OF CONTENTS
iv
TABLE OF CONTENTS (continued)
v
LIST OF TABLES
TABLE PAGE
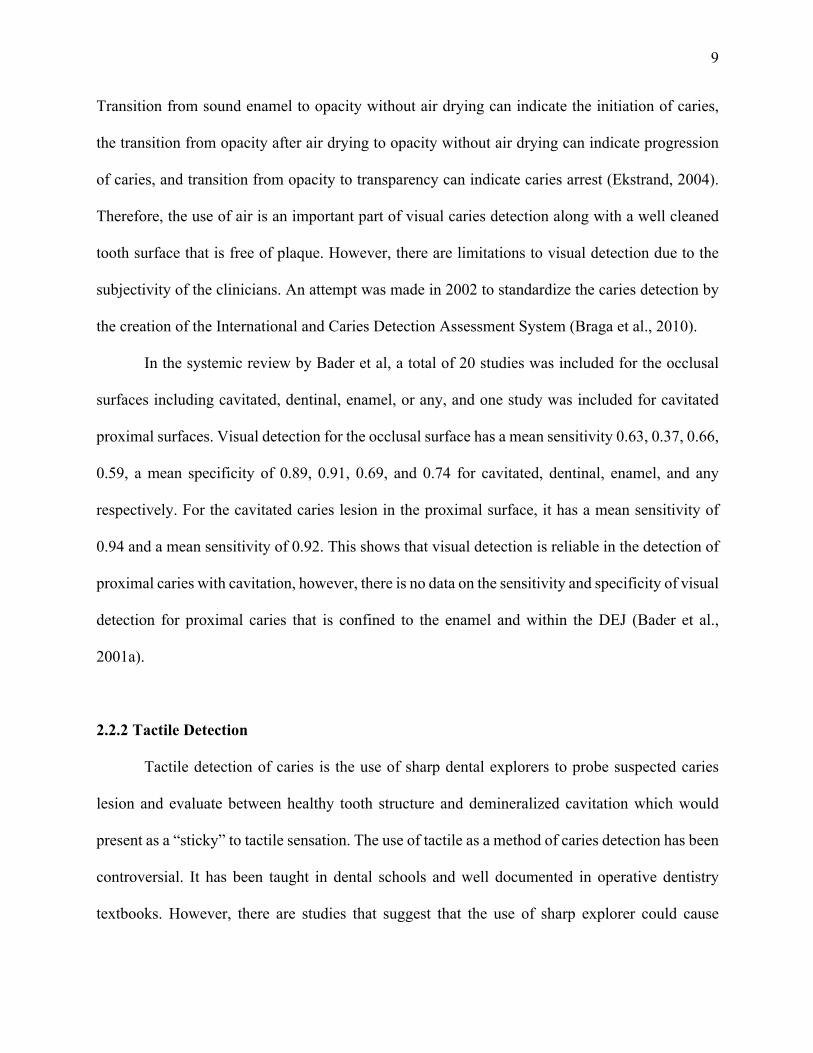
I. PHYSICAL PRINCIPLES USED IN CARIES DETECTION METHODS…..
07
II DEFINING SENSITIVITY AND SPECIFICITY……………………………..
20
III. ACCURACY OF IMAGE SCORING FOR NO CARIES..………………..….
29
IV. ACCURACY OF IMAGE SCORING FOR INCIPIENT CARIES ……..........
29
V. ACCURACY OF IMAGE SCORING FOR CARIES REACHING DEJ……..
30
VI SENSITIVITY AND SPECIFICITY OF BITEWING RADIOGRAPHS COMPARED TO CARIVUTM IMAGES, GROUPED AS NO CARIES VERSUS ANY CARIES…………....……………………...………………….
31
VII. SENSITIVITY AND SPECIFICITY OF BITEWING RADIOGRAPHS COMPARED TO CARIVUTM IMAGES, GROUPED AS CARIES REACHING DEJ VS OTHER CATEGORIES..……………………………...
32
VIII. DISTRIBUTION OF SCORES CORRECT BY RATER STATUS………….. 37
vi
LIST OF FIGURES
FIGURE PAGE
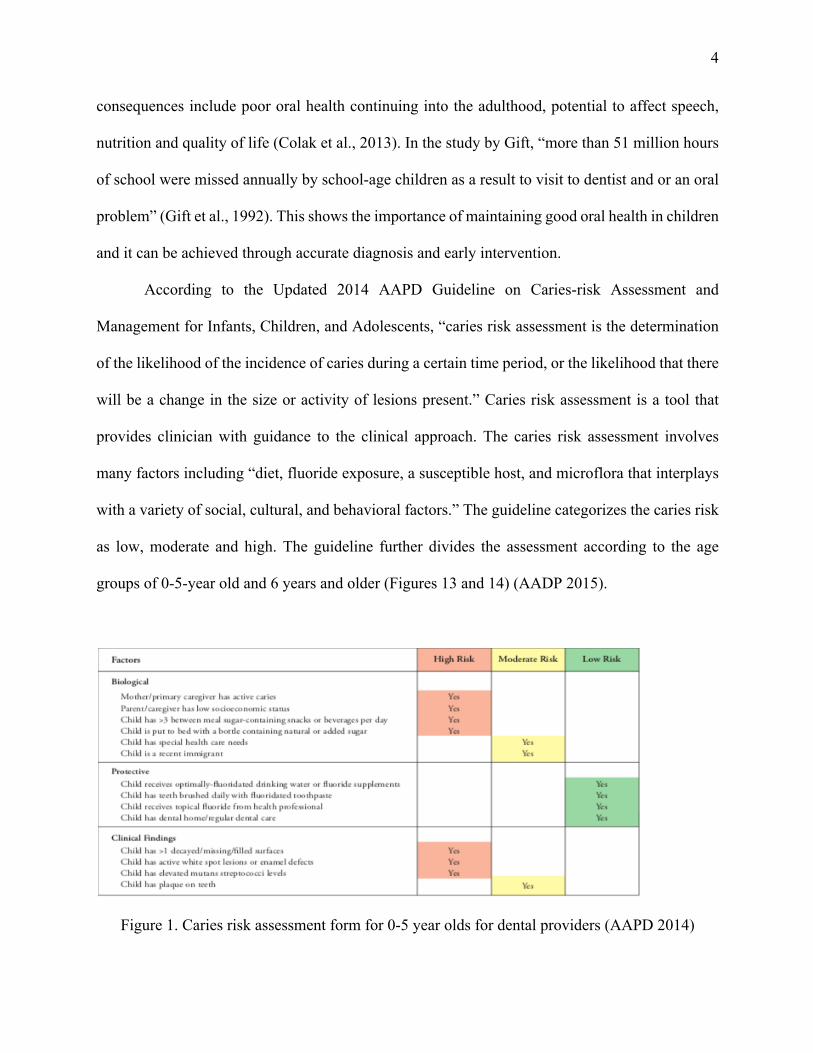
1. Caries risk assessment form for 0-5 year olds for dental providers……….. 4
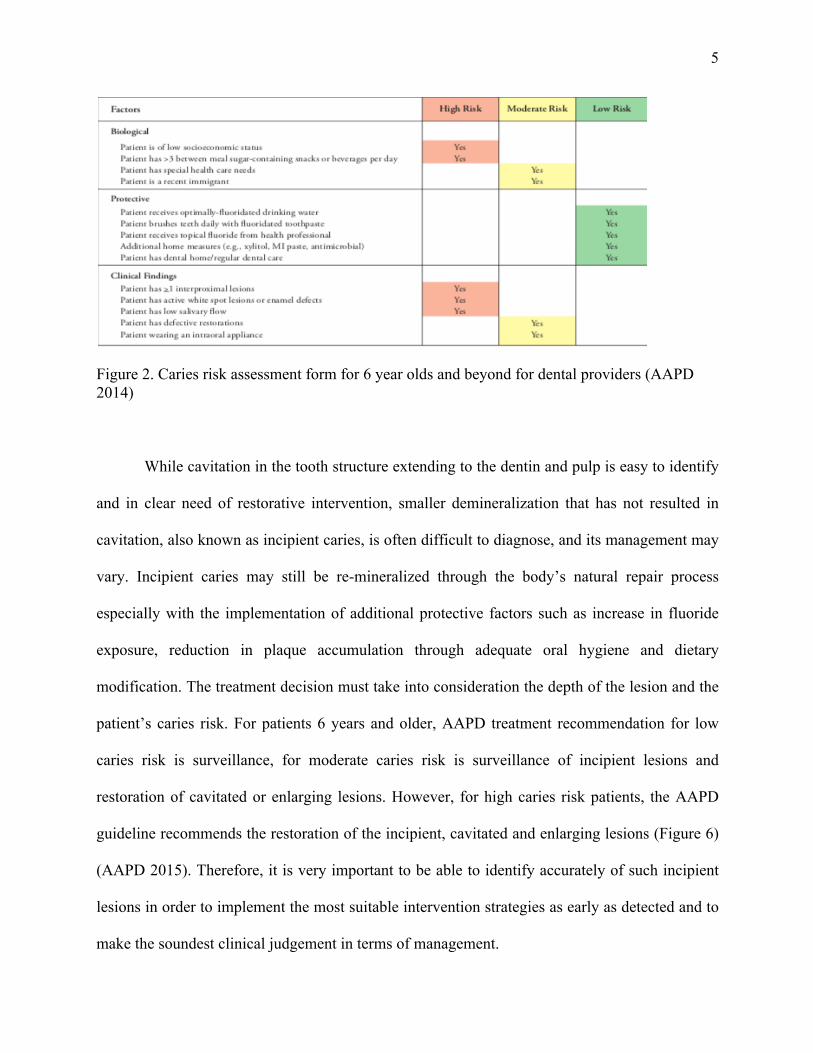
2. Caries risk assessment form for 6 year olds and beyond for dental providers…………………………………………………………………… 5
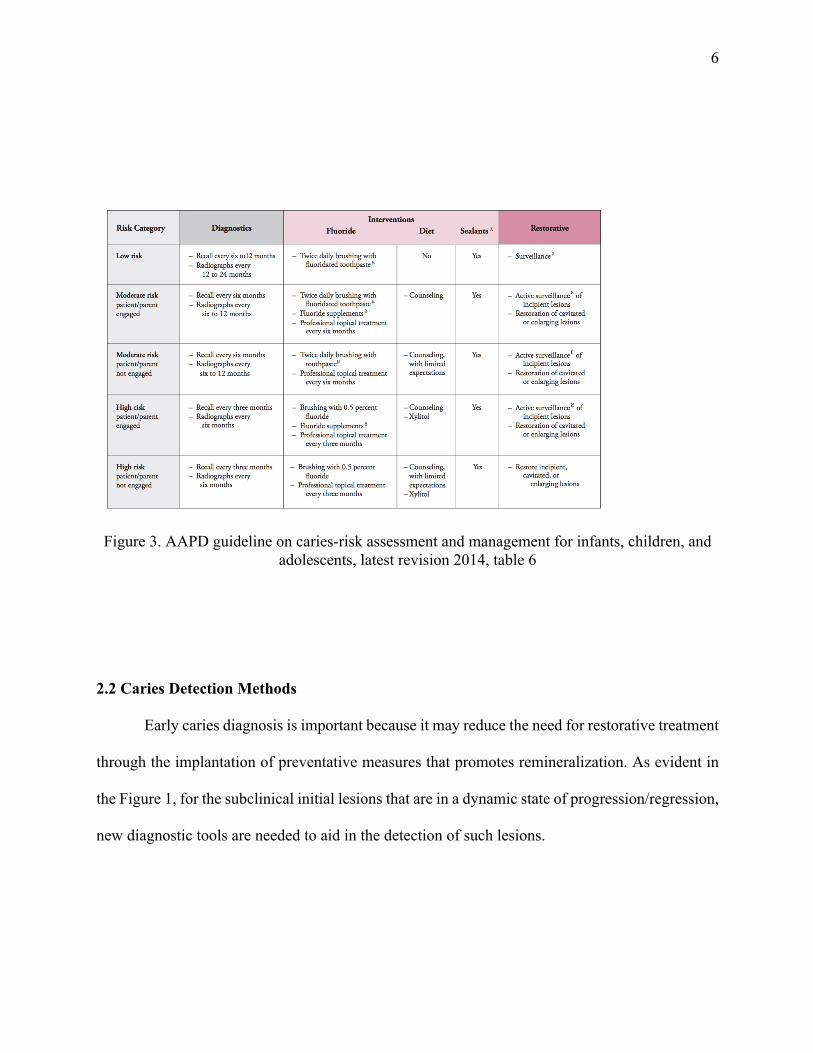
3. AAPD guideline on caries-risk assessment and management for infants, children, and adolescents …………………………...………………...… 6
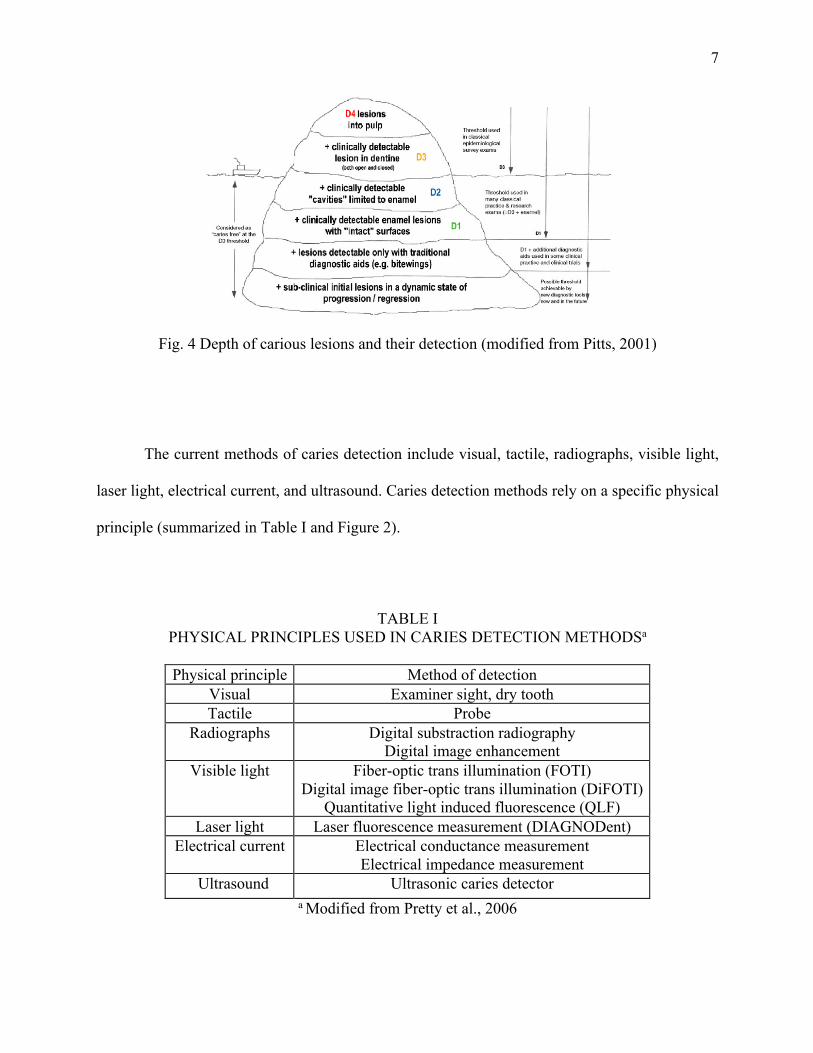
4. Depth of carious lesions and their detection …………...…………………..
7
5. Classification of common caries detection methods ………………..….… 8
In order to capture image, the DEXIS CariVuTM device is inserted intraorally and the tip of
the device is placed over the occlusal surfaces of the teeth. The rubber pieces on either side of the
camera are placed buccal and lingually of the teeth to stabilize the device (Figure 4). The device
is moved along the occlusal surfaces and over areas of interest. The images appear in real time on
a computer monitor, and when the area of interest is visualized, with a click of a button on the
device, the image is captured and stored within a software. Each teeth can be selected for which
17
the image correpsonds, and annotated as such. There is no emission from this device, and the
images are simply captured as they are visualized.
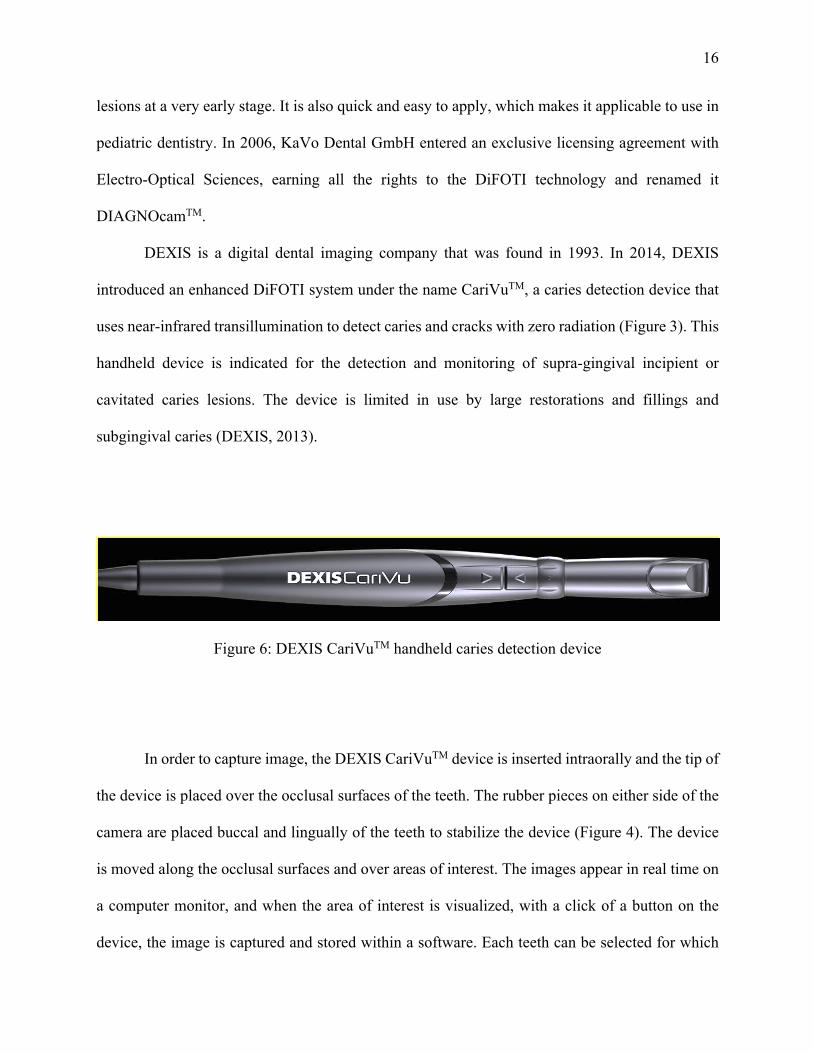
Figure 7: Tip of DEXIS CariVuTM device that is positioned over the tooth surface so that it hugs the tooth and the light shines on either side of the tooth.
The tooth structure allows the passage of light from the entry site to the device. Due to the
difference in porosity of healthy enamel and carious lesions, the light passing through the tooth
structure is reflected differently. While healthy tooth enamel reflects the light in full and appears
white, areas that block light transmission (such as carious lesions) show up clearly as well
delimited, dark areas. A digital camera then captures the image and makes it visible in real-time
on the computer screen (Figure 5).
18
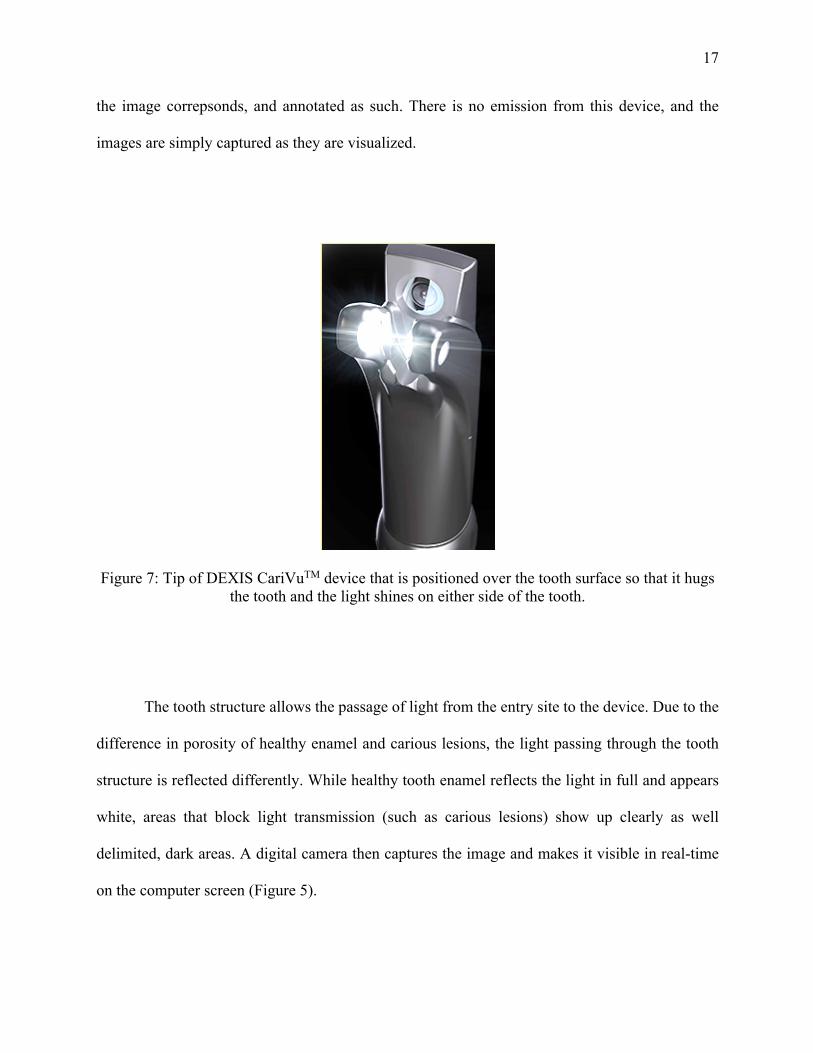
Figure 8: A depiction of a CariVuTM image (left) alongside a traditional bitewing image (right) of the same tooth surfaces (DEXIS, 2016).
In a literature review, 14 articles were found that are relevant to the use of near infrared
light transillumination and the DiFOTI technology as a method for detection of occlusal and
interproximal caries. Of the 14 studies, 11 were in vivo studies and 3 were in vitro studies, 12
studies examined the DIAGNOcamTM and 2 specifically studied the effectiveness of the DEXIS
CariVuTM. All 14 studies have found that the near infrared light transillumination method
performed the same or better when compared to traditional bitewing radiograph and could be an
used as an adjunct or as an alternative to traditional bitewing radiograph.
An in vitro study examined the accuracy of DEXIS CariVuTM in the detection of non-
cavitated interproximal lesions. Thirty human extracted premolars ranging from sound
19
interproximal surface to caries lesions extending into the outer one third of the dentin were
included in this study. The study showed that when compared to traditional bitewing radiographs,
DEXIS CariVuTM device performed the same in terms of accuracy, and demonstrated that it was
superior in terms of repeatability. The study supported that the DEXIS CariVuTM can be used as
an alternative to traditional bitewing radiograph for the detection of interproximal caries
(Abogazalah, 2017). A clinical study examined the effectiveness of DEXIS CariVuTM in the
diagnosis of interproximal caries lesions in thirty human subjects. The inter-reliability between
three examiners was evaluated. The study found that the caries depth classification between the
DEXIS CariVuTM and bitewing radiographs were strongly correlated (Berg, 2018a).
Even though there is literature supporting the use of near infrared transillumination as an
alternative or adjunct to traditional bitewing radiograph in the detection of interproximal lesion,
there is a lack of literature that specifically examines the DEXIS CariVuTM, and even more
specifically in the detection of caries that is confined to the DEJ. More so, there is a lack of
literature for in vivo studies that utilizes a gold standard instead of just examining the correlation
between two devices. More studies will need to be completed to close this gap in the knowledge
to determine if DEXIS CariVuTM is a reliable and accurate method for non-cavitated interproximal
caries diagnosis. This could potentially close the gap in the diagnosis of non-cavitated
interproximal caries where diagnostic bitewing radiographs are unattainable.
2.3 Sensitivity, Specificity, and Other Measures of Accuracy
Diagnostic accuracy is the degree of agreement between a reference test and the diagnostic
test being studied (van Stralen, 2009). In healthcare, the “gold standard” refers to the most accurate
test available to date where other tests are compared to determine whether it is a method that could
20
be used. Four different measures are often combined to determine the accuracy of the test, which
are sensitivity, specificity, positive predicative value, and negative predicative value.
Sensitivity is the ability to show a positive result for all those with the target condition. It
is the proportion of all with the target condition and have a positive result to those who indeed
have the target condition. However, in addition to having a high sensitivity, a good diagnostic test
should also be able to discern those without the target condition. Specificity is the ability to express
the negative result for all those without the target condition. It is the proportion of all without the
target condition and a negative test result of all those who indeed are negative for the target
condition (van Stralen, 2009).
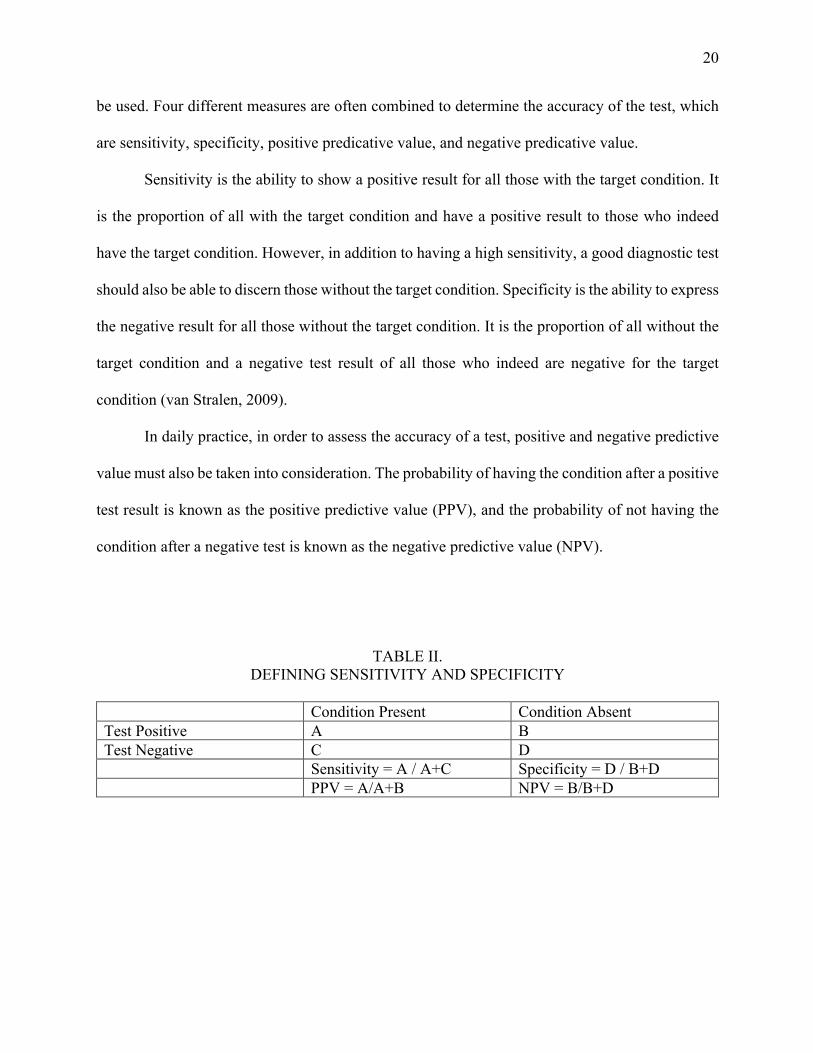
In daily practice, in order to assess the accuracy of a test, positive and negative predictive
value must also be taken into consideration. The probability of having the condition after a positive
test result is known as the positive predictive value (PPV), and the probability of not having the
condition after a negative test is known as the negative predictive value (NPV).
TABLE II. DEFINING SENSITIVITY AND SPECIFICITY
Condition Present Condition Absent Test Positive A B Test Negative C D Sensitivity = A / A+C Specificity = D / B+D PPV = A/A+B NPV = B/B+D
21
III. METHODOLOGY
3.1 Image Collection
Approval of the study was obtained from the University of Illinois at Chicago Institutional
Review Board (Appendix A).
DEXIS CariVuTM is a technology that has been adopted for caries detection in the UIC
Pediatric Dental Clinic. Young patients were assessed first clinically and, where deemed necessary
as per the recommendations of the American Academy of Pediatric Dentistry, 2014 updated
Guideline, standard bite-wing radiography was utilized for comprehensive evaluation of the
interproximal surfaces. Furthermore, these patients were examined with DEXIS CariVuTM device.
The radiographic and DEXIS CariVuTM images produced were stored in the patient’s electronic
health record (Axium) used in the UIC Pediatric Dental Clinic.
For the purposes of this study, the PI identified, by a search in Axium, a maximum of 100
patients that have had both bite-wing x-rays and DEXIS CariVuTM images documented. The report
generated from the search included the personal patient dental record number (in Axium) for
patients aged 6-16 years old, who have bitewing radiographs and CariVuTM images. The search
were based on the patients’ age and the billing codes of the bitewing radiograph and CariVuTM
images. The PI reviewed the charts and only healthy children aged 6-16 years old with mixed and
permanent dentition were included. This means that the patients will have a combination of
primary (baby) teeth and permanent (adult) teeth, or only permanent (adult) teeth in their mouths.
Images were only included if both the bitewing and CariVuTM image of the same tooth was
considered diagnostic by the PI. If there was an overlap between surfaces, poor illumination, or
otherwise non-diagnostic images, then the image pair was excluded from the study.
22
Each patient chart has the potential to generate a maximum of 24 images to utilize in the
questionnaire. There are potentially 24 interproximal posterior surfaces in the mouth of a full
mixed-dentition or permanent dentition patient as shown in the image (Figure 7).
Figure. 9: Depiction of the 24 interproximal tooth surfaces that can be generated from one permanent dentition patient.
All images were exported from DEXIS and stored in a Microsoft PowerPoint file. Patient
identifiers were not included with the images, but the images were labeled so that the pairs could
be matched later. In order to avoid repetitive collection of patient data, each included subject
received a study number. A key with all the coded data including the subjects study numbers and
the corresponding personal patient dental record number (in Axium) were kept in a separate
encrypted file in the password protected computer. The document containing the key was
23
destroyed at the end of the study following the official policy of the Department of Pediatric
Dentistry for disposing of confidential information.
3.2 Image Compilation
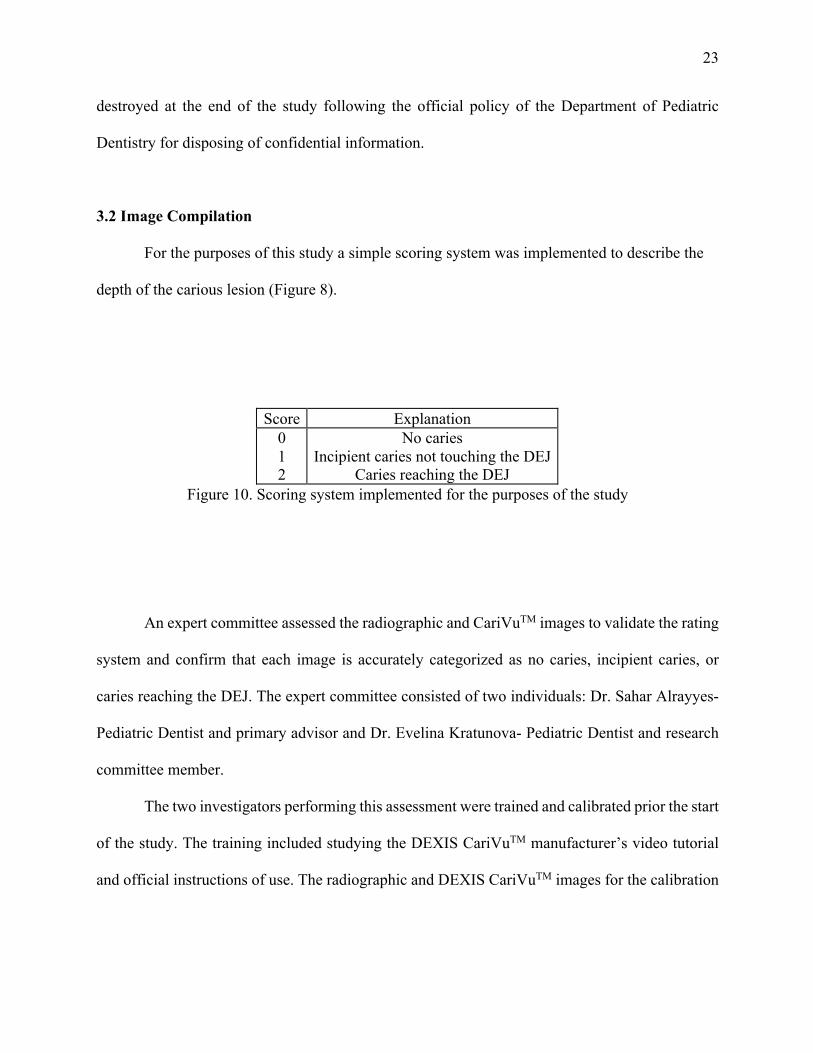
For the purposes of this study a simple scoring system was implemented to describe the
depth of the carious lesion (Figure 8).
Score Explanation
0 1 2
No caries Incipient caries not touching the DEJ
Caries reaching the DEJ Figure 10. Scoring system implemented for the purposes of the study
An expert committee assessed the radiographic and CariVuTM images to validate the rating
system and confirm that each image is accurately categorized as no caries, incipient caries, or
caries reaching the DEJ. The expert committee consisted of two individuals: Dr. Sahar Alrayyes-
Pediatric Dentist and primary advisor and Dr. Evelina Kratunova- Pediatric Dentist and research
committee member.
The two investigators performing this assessment were trained and calibrated prior the start
of the study. The training included studying the DEXIS CariVuTM manufacturer’s video tutorial
and official instructions of use. The radiographic and DEXIS CariVuTM images for the calibration
24
were compiled by the PI. The examiners assessed all 363 radiographic and corresponding
CariVuTM images collected in the study.
Each of the two experts scored both the bitewing and CariVuTM images. They scored
the images independently from one another. They gave separate bitewing and CariVuTM scores;
these scores did not have to match. They scored each image according to the designated system
(Figure 8) or chose to exclude the image altogether if they deemed it non-diagnostic.
Images were only included in the final questionnaire if the bitewing score for both expert
raters was the same. After excluding all non-matching bitewing scores and excluding all images
deemed non-diagnostic by the experts, 90 image pairs were agreed upon and included. All included
images were of permanent posterior teeth which included molars and premolars. Of these 90
images, the expert committee rated 30 as no caries, 30 as incipient caries not touching the DEJ,
and 30 as caries reaching the DEJ and into dentin. These categories will henceforth be referred to
as no caries, incipient caries, and caries reaching the DEJ.
The paired bitewing and CariVuTM images were separated into two image sets: bitewing
and CariVuTM. Each of these image sets was independently randomized using the randomization
tool on Microsoft Excel to generate a set of randomized numbers 1-90. Based on this
randomization, the image sets were manually re-ordered. An image file was created with the
composition of the 90 randomized bitewing and CariVuTM images. A questionnaire is created and
is included in Appendix B. The image file was then were exported as a PDF file and uploaded on
an Apple Ipad belonging to UIC Department of Pediatric Dentistry to be used in this study.
25
3.3 Choice of Gold Standard
For the purposes of this study, radiographs were selected as the gold standard for caries
diagnosis. The expert committee generated ratings for all of the radiographic images and these
ratings were then deemed to be the “correct” diagnosis.
3.4 Subject Enrollment
Pediatric dental patients at UIC College of Dentistry with both bitewing radiograph and
DEXIS CariVuTM images of the same tooth surfaces stored in the electronic dental health record
system Axium were identified by the PI, through a search on Axium for the treatment code
associated with bitewing radiographs and DEXIS CariVuTM images. There was no direct contact
with the subjects for enrollment.
All pediatric dental residents and faculty members at the UIC Department of Pediatric
Dentistry, were invited to participate as subjects in the study and to serve as raters. Raters were
recruited verbally. No advertising was utilized. Raters were asked to participate by completing the
questionnaire. Participants were informed that the questionnaire would take up to 30 minutes to
complete and were given the option to opt out and not complete the questionnaire, or to decide not
to participate after they had begun completing the questionnaire. The participating subjects were
not aware of which patients the images were taken from and were not aware of how the CariVuTM
and radiographic images matched. The PI and the two faculty committee members were excluded.
A 20 minute tutorial session was conducted by the PI to standardize the interpretation of the
CariVuTM images.
The questionnaire included a cover letter (Appendix C), which contained the elements of
informed consent. Participating subjects were given a sample of different CariVuTM images which
26
were taken from the DEXIS CariVuTM user manual (Appendix D). They were permitted to
reference this chart as they rated the images. Raters were informed that there were a total of 180
randomized images composed of both bitewing and CariVuTM images. The PI answered questions
about image orientation or which surface was meant to be scored. Beyond this, the PI did not
provide any information to the raters during the ratings. The raters reviewed the images on the
same device, the Apple Ipad with the uploaded PDF file, and recorded their findings in the
questionnaire. (Appendix E) The PI then recorded the ratings into a Microsoft Excel workbook.
The PI answered questions about image orientation or which surface was meant to be scored.
Beyond this, the PI did not provide any information to the raters during the ratings.
3.5 Statistical Analysis
IBM SPSS Statistical Analysis and Reporting program will be utilized to analyze the data
from this study. Each data set will involve a caries rating (yes/ incipient/ no) for a radiograph and
a corresponding caries rating (yes/ incipient/ no) for a CariVuTM image. Although the images will
not be paired on the questionnaire, they are related samples and will be paired for data analysis.
27
IV. RESULTS
4.1 Number of Raters and Response Rate
The data collection took place at the UIC Department of Dentistry between the dates of
February 20th, 2019 and March 13th, 2019. Participating subjects completed the questionnaire in
one setting and within 30 minutes.
All pediatric dentists and pediatric dental residents of the UIC Department of Pediatric
Dentistry were asked to participate in the study. This consisted of nine first year residents, seven
second year residents, two third year residents, and eight faculty members. One resident, the
principle investigator, and two faculty members, the expert committee, were excluded from
participating due to their involvement in compiling the images. There were therefore 26
individuals eligible for participation. All 26 individuals completed the questionnaire.
4.2 Demographics
The only demographic information collected was the status of the raters categorized either
as a first year resident, second year resident, third year resident and faculty member. The
participating subjects were asked to indicate their status on the questionnaire. Nine raters were first
year residents, seven raters were second year resident, two raters were third year resident, and eight
raters were faculty member.
4.3 Determination of observations for data analysis
A total of 180 images were determines eligible to be included in the study, 90 bitewings
radiographs and 90 CariVuTM images. Each image was rated once, where each rating was
computed as an independent observation. The sensitivity and specificity were calculated based on
28
the subject’s ratings and compared to the rating of the accurate rating of the corresponding
radiograph’s image, the gold standard. However, during processing of the data, it was discovered
that a single bitewing image was shown and rated twice, and the corresponding CariVuTM image
was also shown and rated twice. All corresponding ratings for the 4 images were excluded in the
data analysis for this study. This resulted in a total of 176 images, 88 bitewing and 88 CariVuTM
images, to be included in this study. There was a total of 26 raters, resulting in a total of 4576
observations. This included the bitewing and CariVuTM image for 30 caries reaching the DEJ, 29
incipient caries, and 29 no caries sites.
4.4 Accuracy of Image Scoring by Image Type
The accuracy of each image was determined by comparing each individual rating to the
correct diagnosis as determined by the expert committee using the bitewing image as the gold
standard. This was categorized into no caries, incipient caries, and caries reaching the DEJ and
examined by the image type either as bitewing radiograph or CariVuTM image. This study included
29 image pair as no caries, 29 image pair as incipient caries, and 30 image pair as caries reaching
the DEJ. Each image set included 2 images, one bitewing and one CariVuTM image. There was a
total of 26 raters, yielding a total of 754 image pair observations of no caries, 754 image pair
observations of incipient caries, and 780 image pair observations of caries reaching the DEJ. This
yielded a total of 4578 observations. The results of the percentage accurate is as shown in table III,
IV and V. The results are also represented graphically in figure 9.
29
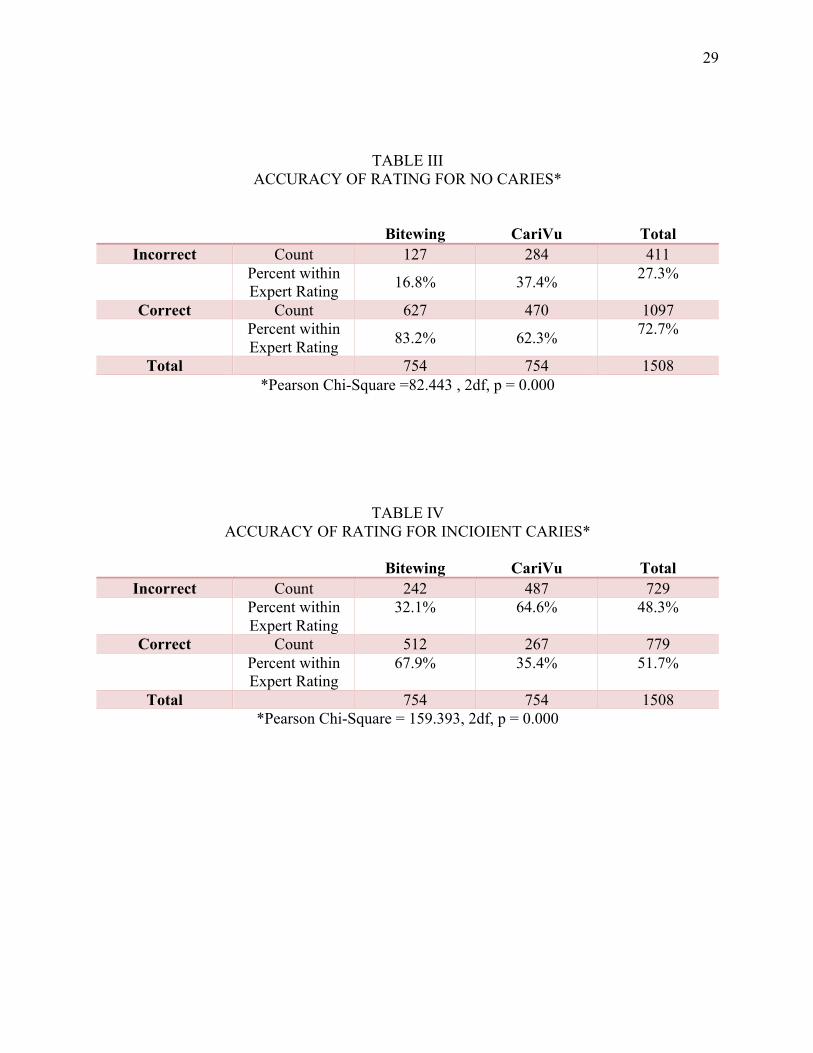
TABLE III
ACCURACY OF RATING FOR NO CARIES*
Bitewing CariVu Total Incorrect Count 127 284 411
Percent within Expert Rating 16.8% 37.4% 27.3%
Correct Count 627 470 1097 Percent within
Expert Rating 83.2% 62.3% 72.7%
Total 754 754 1508 *Pearson Chi-Square =82.443 , 2df, p = 0.000
TABLE IV ACCURACY OF RATING FOR INCIOIENT CARIES*
Bitewing CariVu Total
Incorrect Count 242 487 729 Percent within
Expert Rating 32.1% 64.6% 48.3%
Correct Count 512 267 779 Percent within
Expert Rating 67.9% 35.4% 51.7%
Total 754 754 1508 *Pearson Chi-Square = 159.393, 2df, p = 0.000
30
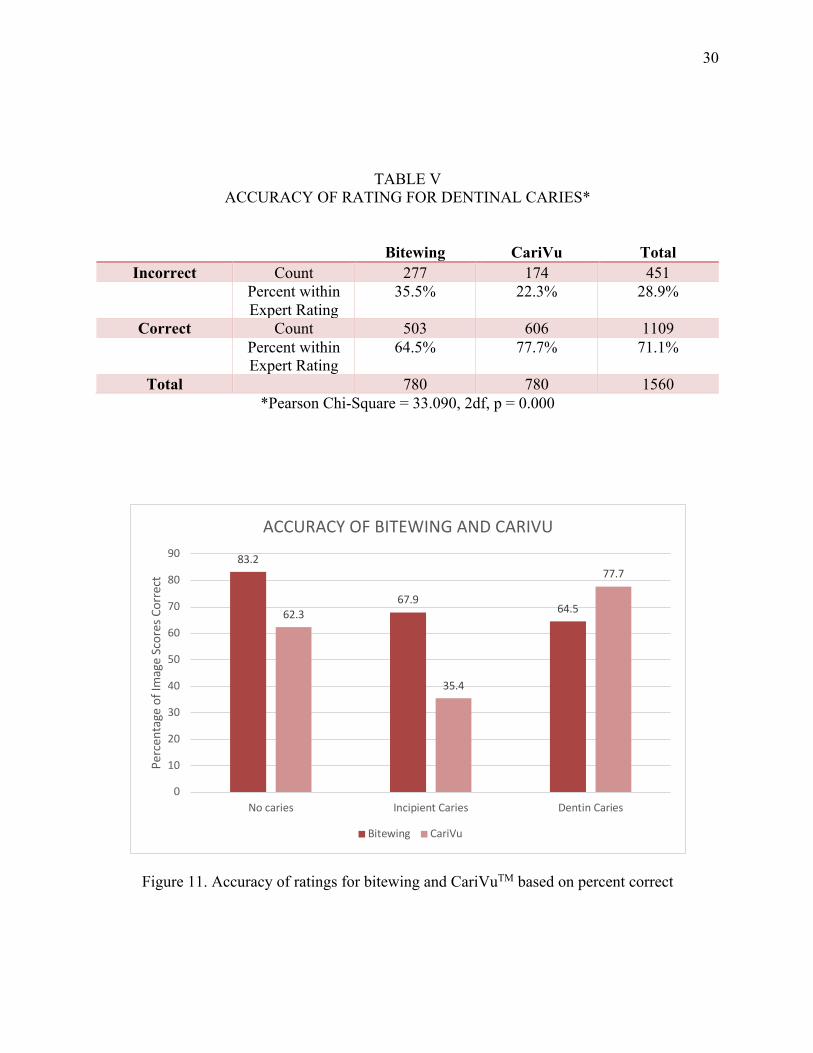
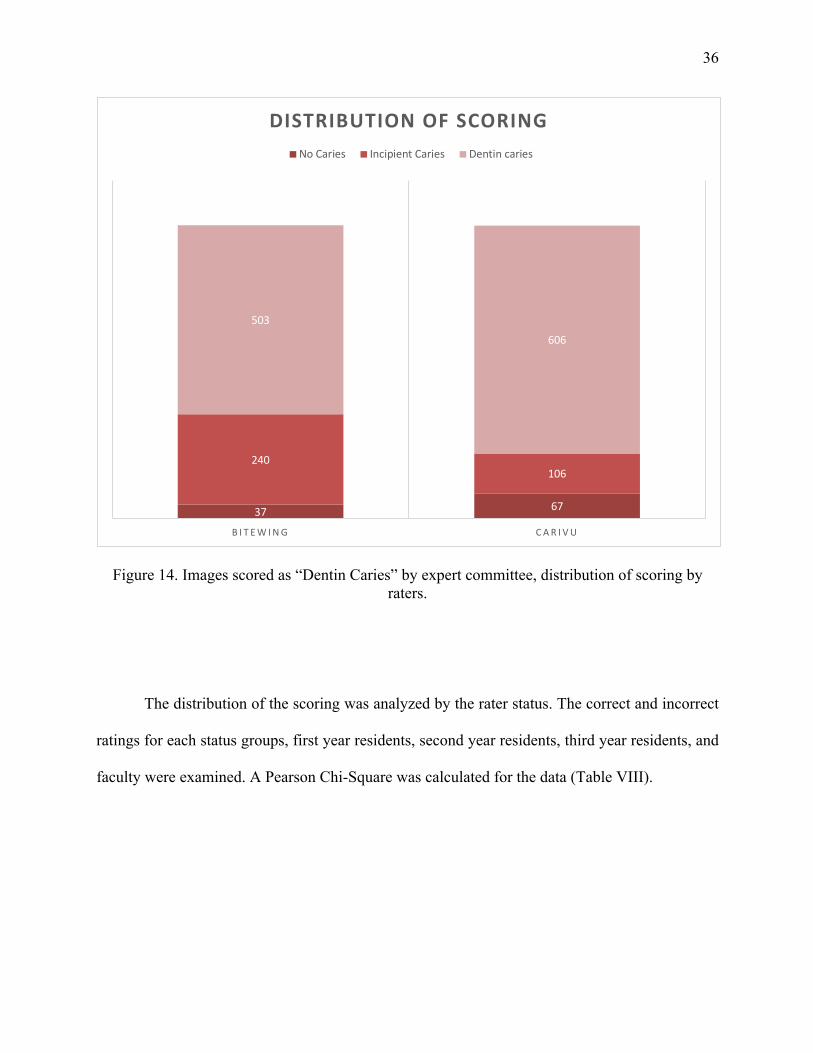
TABLE V ACCURACY OF RATING FOR DENTINAL CARIES*
Bitewing CariVu Total Incorrect Count 277 174 451
Percent within Expert Rating
35.5% 22.3% 28.9%
Correct Count 503 606 1109 Percent within
Expert Rating 64.5% 77.7% 71.1%
Total 780 780 1560 *Pearson Chi-Square = 33.090, 2df, p = 0.000
Figure 11. Accuracy of ratings for bitewing and CariVuTM based on percent correct
83.2
67.964.562.3
35.4
77.7
0
10
20
30
40
50
60
70
80
90
No caries Incipient Caries Dentin Caries
Perc
enta
ge o
f Im
age
Scor
es C
orre
ct
ACCURACY OF BITEWING AND CARIVU
Bitewing CariVu
31
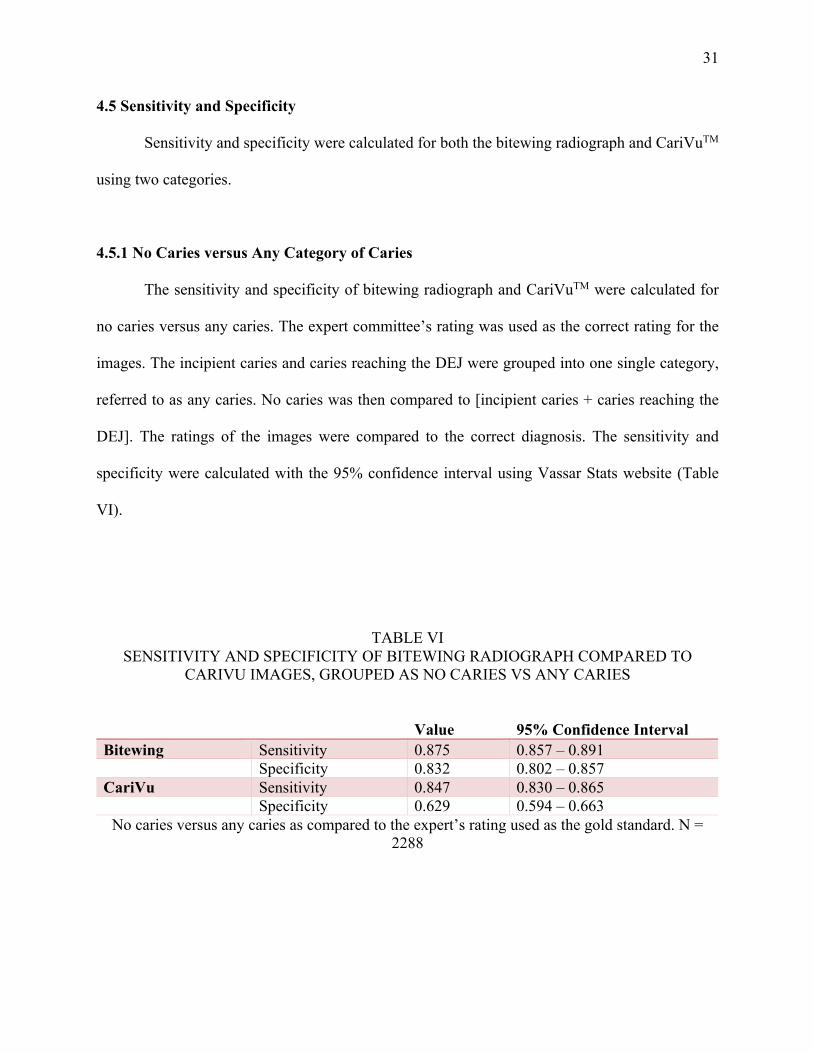
4.5 Sensitivity and Specificity
Sensitivity and specificity were calculated for both the bitewing radiograph and CariVuTM
using two categories.
4.5.1 No Caries versus Any Category of Caries
The sensitivity and specificity of bitewing radiograph and CariVuTM were calculated for
no caries versus any caries. The expert committee’s rating was used as the correct rating for the
images. The incipient caries and caries reaching the DEJ were grouped into one single category,
referred to as any caries. No caries was then compared to [incipient caries + caries reaching the
DEJ]. The ratings of the images were compared to the correct diagnosis. The sensitivity and
specificity were calculated with the 95% confidence interval using Vassar Stats website (Table
VI).
TABLE VI SENSITIVITY AND SPECIFICITY OF BITEWING RADIOGRAPH COMPARED TO
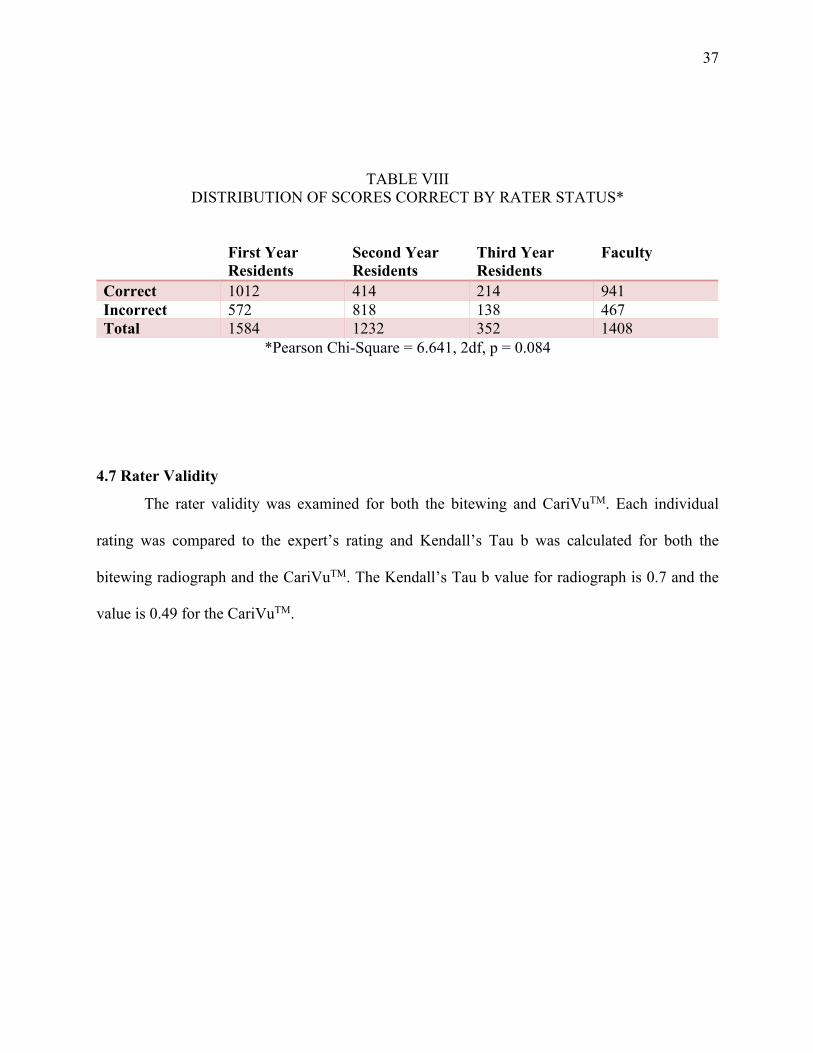
The rater validity was examined for both the bitewing and CariVuTM. Each individual
rating was compared to the expert’s rating and Kendall’s Tau b was calculated for both the
bitewing radiograph and the CariVuTM. The Kendall’s Tau b value for radiograph is 0.7 and the
value is 0.49 for the CariVuTM.
38
V. DISCUSSION
5.1 Strengths and Limitations of the Study
5.1.1The Choice of Gold Standard
The choice of gold standard in this study is the “correct” diagnosis determined by an expert
committee based on the bitewing radiographs. One limitation of this study is that this does not
truly reflect the caries status of the tooth, but rather what is deemed correct on the bitewing
radiographs by the expert committee. By using this as the gold standard, it is implying that the
bitewing radiograph has a 100% accuracy in determining the caries status, which we know it is not
the case. However, there are many other studies that have used similar designs and used bitewing
as the gold standard which shows that this is an acceptable methodology (Litzenburger 2018,
Bizhang 2016, Lara-Capi 2017).
Another concern would be the error introduced by the expert committee in their diagnosis
of caries as it appears on the bitewing radiographs. However, the images of the bitewing were
scored independently of the other committee member. Both members are highly qualified in their
professional experience which minimizes the chance of error in the diagnosis of caries. Only the
images that received the same diagnosis from both experts were included in this study, and this
further decreases the chance of error.
Other studies for the DiFOTI system have either utilized different gold standards or did not
include the use of a gold standards. In the study by Kunisch et al, the choice of gold standard is
the clinical determination of the depth by preparing the tooth and visualizing the lesions. The gold
standard of clinical verification was also used in the study by Ozkan et al in the examination of the
DIAGNOcamTM. Another study that examined the DEXIS CariVuTM and bitewing radiograph,
39
there is a lack of gold standard, and instead a correlation was examined for the two methods (Berg,
2018b).
The expert committee must agree on the diagnosis of the caries, and any non-diagnostic
radiographs such as those with overlaps and the ones with questionable quality were excluded.
Therefore, radiographs chosen to be included in this study were automatically preselected for its
clarity and diagnostic quality. This could introduce a limitation in this study because these images
do not reflect of those that are normally seen in the clinical setting. This could introduce bias for
the accuracy of the bitewing radiograph and its sensitivity and specificity. One way to eliminate
this bias is to include all bitewings in this study, however, this would mean that the bitewings could
not be used as a gold standard.
5.1.2 Lesions Included in This Study
The lesions included in this study are non-cavitated interproximal caries lesions in
permanent teeth. This is a strength in this study due the exclusion of cavitated lesions.
Traditionally, caries would appear as a dark area on the CariVuTM image. However, when there is
cavitation, sometimes depending on the placement of the CariVuTM device, the lesion could appear
transparent and lighter in color, which could be interpreted as no caries or incipient caries. By
excluding the cavitated lesions, the misrepresentation is eliminated.
In the routine practice of diagnosing interproximal lesions, a practitioner would utilize a
combination of methods including visual, tactile, and radiograph. For the cavitated interproximal
lesions, they can be detected with visual and tactile in addition to radiograph due to the cavitation
extending to the occlusal, buccal and lingual surfaces. In those instances, it eliminates the need for
adjunct tools in its detection as it can be affirmed that the lesions do exist. In this study, the
selection of only non-cavitated lesions is a strength because it reflects the clinical scenario that an
40
adjunct is indicated in addition to bitewing radiographs. This is a strength of the study because the
lesions examined in this study are equivalent to those that are usually in question in a clinical
setting.
5.1.3 Inexperience of the Users
There are two different components of inexperience of the users; the inexperience in the
obtaining of the CariVuTM images and in the interpretation of the images. A short training was
provided to all the dental assistants as well as the residents at UIC Department of Pediatric
Dentistry. However, the assistants and residents still have less experience in obtaining the
CariVuTM images as compared to bitewing radiographs. The inexperience could result in decreased
quality of the CariVuTM images obtained. The residents and faculty surveyed in this study all have
had limited experience with the interpretation of the CariVuTM images. This could also result in
error in the interpretation of the CariVuTM images by the raters.
5.1.4 The View of the Images
The images were accessed on DEXI software. Each image was cropped to only show the
surface of interest, and the contrast and brightness were maximized by the PI. The images were
copied and compiled into a PDF file and downloaded on an Apple Ipad. The Ipad was given to the
raters individually to be rated independently. Since all the raters used the same device in rating of
the lesions, the images viewed were standardized which is a strength in this study.
The cropping of the image to only contain the surface of interest could cause visual effects
since the surface is at the edge of the image, and this could askew how the lesion appears. The
background on the PDF file is white, which is different from black background in the DEXIS
41
software. Normally when viewing the images on the DEXIS software, the brightness and contrast
could be adjusted as needed to best visualize the lesions. However, in this study, the images are
adjusted as to what the PI would deem to be the clearest. The raters could enlarge the images as
needed on the Ipad, however, they do not have the contrast and brightness tools as they to help
visualize the caries lesions. Also, the resolution of the images viewed on the Ipad may be different
from the computer screen used in the clinic.
5.2 Accuracy of Image Scoring by Image Type
There is a difference in the accuracy of the bitewing and CariVuTM images in this study. In
this study, the bitewing images are more accurate for the detection of no caries and incipient caries,
while the CariVuTM was more accurate in the detection of caries reaching the DEJ. This indicates
that the CariVuTM is more likely to pick up caries reaching the DEJ versus the no caries and
incipient caries, and that the CariVuTM is inferior to the bitewing in the detection of no caries and
incipient caries. However, as previously discussed, the bitewing radiographs were specifically
chosen for its quality in this study. Even though the bitewing is more accurate than the CariVuTM
in this study for the detection of no caries and incipient caries, the bitewing radiographs had an
advantage compared to the CariVuTM. Therefore, the accuracy of the CariVuTM as compared to
bitewing may actually be higher in routine clinical settings than what is concluded in this study
due to the bias in the pre-selection of the bitewing radiographs.
5.3 Sensitivity and Specificity
In this study, the bitewing images were rated first by the expert committee. Only those
bitewing radiographs with the ratings that was agreed upon by the committee were chosen to be
42
included in this study. In this case, instead of truly determining the sensitivity and specificity of
the bitewing and CariVuTM in caries detection, this study actually examined the sensitivity and
specificity of detecting the caries noted by the expert committee on the bitewing radiographs.
Sensitivity and specificity are used to measure the presence or absence of disease. This is
a comparison of a binomial ordinates of disease present, disease absent, test positive, and test
negative. For this study, the incipient caries poses as a third category and it must be taken into
consideration when determining the sensitivity and specificity of the bitewing radiograph and
CariVuTM device. Two questions were examined in this study: how valid is the CariVuTM at
detecting any caries, and how valid is the CariVuTM in only detecting caries reaching the DEJ. In
the first question, the incipient caries is considered as diseased and would require treatment
intervention such as implementation of preventative measures. In the second question, only the
caries reaching the DEJ is considered as diseased and would require restorative intervention.
The sensitivities for the bitewing radiograph are 0.88 and 0.644 for any caries and caries
reaching the DEJ respectively. In previous studies, it has been shown that the sensitivity ranges
from 0.14 – 0.66 for non-cavitated proximal caries (Bader et al, 2001, Gomez et al., Schwendicke
et al.). This could be due to the fact that these bitewing radiographs are used as the gold standard
in this study, and only the clear and high diagnostic quality images were included. This does not
reflect what may be routinely seen in the clinical setting. The specificities for the bitewing
radiograph in this study is 0.83 and 0.93 for any caries and caries reaching the DEJ. The reported
range of specificity is 0.55 – 0.95 (Bader et al., 2001d, Gomez et al., 2013d, Schwendicke et al.,
2015b). The specificities that we found in this study is within the range of other studies. This shows
that the bitewing radiographs used in this study was a reliable method for detecting caries and not
overly diagnose caries.
43
The sensitivity for CariVuTM was 0.68 and 0.78 for any caries and caries reaching the DEJ.
The sensitivity range for the CariVuTM for any caries overlaps with the sensitivity of the bitewing
for the same category. This shows that the CariVuTM is equally as accurate in detecting any caries.
However, the sensitivity of CariVuTM for caries reaching the DEJ is higher than that of bitewing
radiograph. This shows that the CariVuTM is more likely to detect caries reaching the DEJ than
bitewing radiograph. The specificity for CariVuTM is 0.63 and 0.69 for any caries and caries
reaching the DEJ. These specificity values are lower than that of bitewing for both categories. This
shows that the CariVuTM is more likely to produce false positives for any caries as well as for
caries reaching the DEJ. This means that the CariVuTM is more likely to over diagnose caries as
compared to bitewing radiographs.
5.4 Distribution of Scoring
The distribution of the scoring was assessed for all three image types. Computing the
distribution of scoring is critical and has clinical implications in uncovering whether the CariVuTM
device under or over diagnose the severity of dental caries. If the rater is more likely to rate the
lesion as more severely diseased, this would lead to over treatment of the lesion. The reverse is
true, if the rater is scoring the images as less severely diseased, then the device is under diagnosing
true lesions that may require intervention.
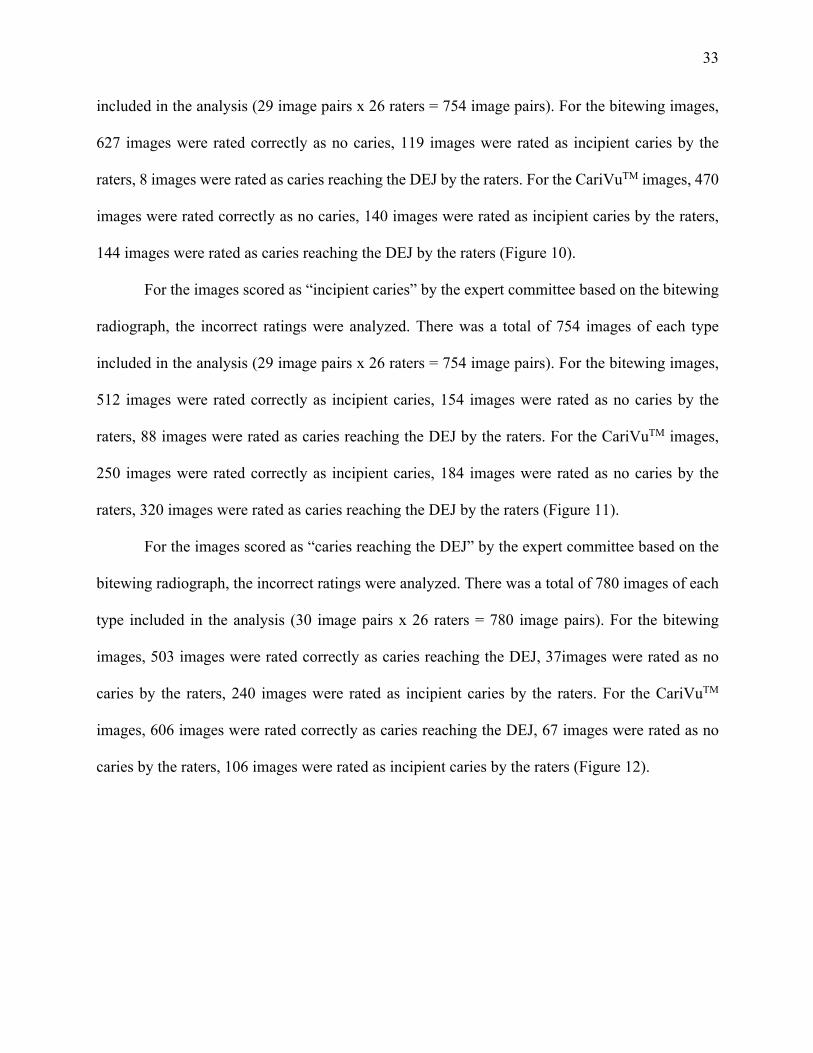
For the category of “no caries” as determined by the expert committee, the raters rated 16%
incorrectly as incipient caries and 1% incorrectly as caries reaching the DEJ. For the CariVuTM
images, the rater rated 19% incorrectly as incipient caries and 19% incorrectly as caries reaching
the DEJ. This is concerning because the CariVuTM ratings were scored as more diseased than the
bitewing radiographs which would lead to over diagnosis of the severity of the lesions.
44
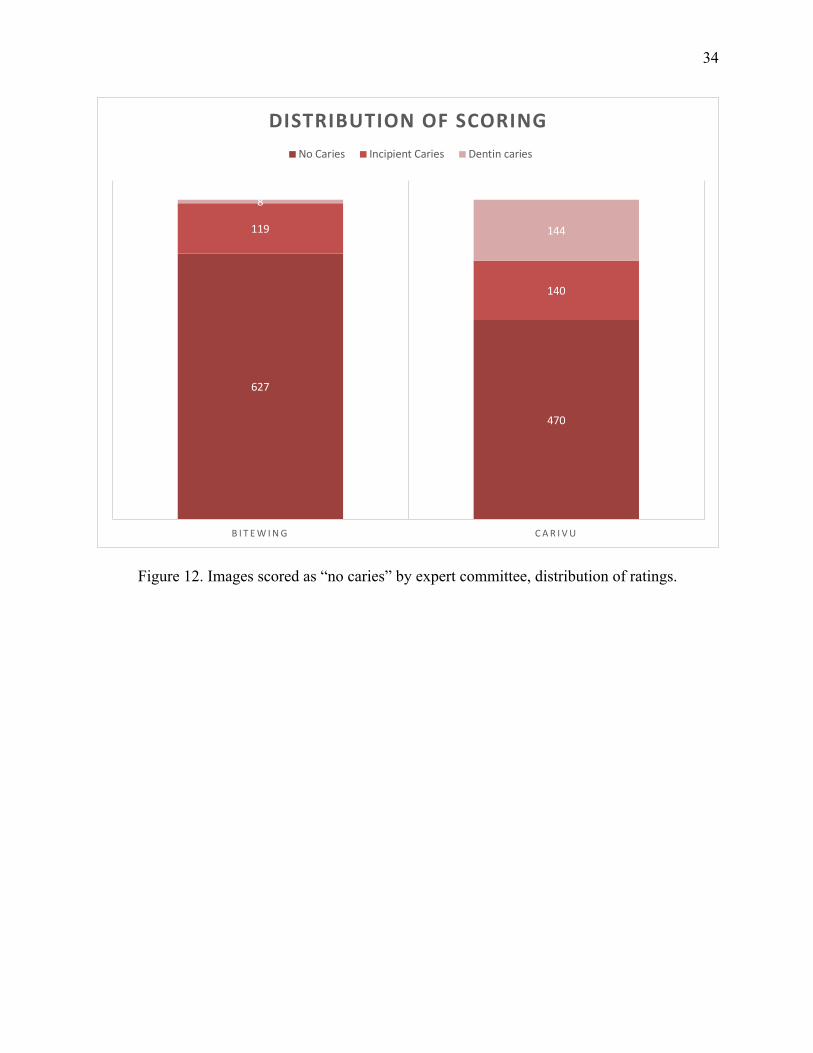
For the category of “incipient” as determined by the expert committee, the raters rated 20%
incorrectly as no caries and 12% incorrectly as caries reaching the DEJ. This shows that the ratings
bitewing radiograph is slightly towards less diseased when the “correct diagnosis” is incipient
caries. For the CariVuTM images, the rater rated 22% incorrectly as no caries and 42% incorrectly
as caries reaching the DEJ. Even though the CariVuTM has more rating of no caries than bitewing
radiograph, this is because there is a larger percentage of all incorrect for the CariVuTM than
bitewing radiograph. The 42% rating of the CariVuTM as caries reaching the DEJ is significant and
it further confirms that the CariVuTM would over diagnose the severity of disease and lead to over
treatment.
For the category of “caries reaching the DEJ” as determined by the expert committee, the
raters rated 5% incorrectly as no caries and 31% incorrectly as incipient caries. For the CariVuTM
images, the rater rated 9% incorrectly as incipient caries and 14% incorrectly as caries reaching
the DEJ. For the bitewing, the incorrect rating of incipient caries is greater than those that were
incorrectly rated as no caries, and there is more correlation in the error for the severity of the lesion.
Whereas, the difference between the incorrect rating of incipient caries and no caries for the
CariVuTM is smaller and the error is more inconsistent and random. This shows that the even when
rated incorrectly, the disease severity is still rated as closer to the true status of the disease as
detected by the bitewing radiograph than the CariVuTM. This also could imply that the bitewing
radiograph under-diagnosis the severity of the disease as compared to the CariVuTM.
We also examined the distribution of the scoring based on the status of the raters. There is
no significant difference between the 1st year residents, 2nd year residents, 3rd year residents, and
faculty. One might expect that the 1st year residents would have the least accurate ratings and the
faculty would have the most accurate ratings due the difference in clinical experience. This result
45
may be due to that all the rater status groups had the same amount of limited experience with the
CariVuTM device. Also, as previously discussed, the bitewing radiographs included in this study
have better diagnostic quality which eliminates the uncertainty in the diagnosis. The combination
of these two factors could be why there was no difference amongst the raters based on their status.
5.5 Rater Validity
The validity of the ratings were examined by measuring the Kendall’s Tau b value for the
bitewing radiograph and CariVuTM. This is answering the question, “how similar are the raters to
the expert?” This also helps in answering the question of validity of the bitewing radiograph and
CariVuTM. The Kendall Tau b value for bitewing is 0.70, and 0.49 for the CariVuTM. This shows
that the raters rating of the bitewing radiograph is more similar to the expert’s rating of caries than
the CariVuTM. This again shows that the CariVuTM overall is less valid than the bitewing
radiograph in detecting caries in this study.
5.6 Implications for Care
For the incipient caries in this study, the CariVuTM over diagnosed the severity of the
disease by 42%. This would have clinical implications in that it would lead to over diagnosis and
over treatment by the clinicians for the patients in low and moderate caries risk category. Unlike
bitewing radiographs, the CariVuTM device emits no radiation, therefore images could be taken
more frequently with no contraindications. The CariVuTM is also more accurate and more sensitive
in detecting caries reaching the DEJ than bitewing radiographs. For the patients in low and
moderate caries risk categories, the CariVuTM can be used as an adjunct in the monitoring of the
progression of the caries, especially as the caries progresses and approaches the DEJ.
46
For the patients that is deemed to be at high caries risk, the AAPD guideline recommends
the restoration of the incipient, cavitated and enlarging lesions. In this regard, the CariVuTM is a
suitable device for patients who are placed in the high caries risk category. Even though the
CariVuTM device would overly diagnose the severity of the lesion, however, the same treatment is
indicated for both the incipient caries and caries reaching the DEJ.
5.7 Future Studies
In this study, the choice of gold standard is bitewing radiographs rated by an expert
committee. In future studies, other choice of gold standard could be utilized such as histological
sections of the teeth, use of CBCT, or examination of prepared teeth to determine the extent of the
lesions. This could yield a true reference for the status of the caries in the tooth.
All young permanent posterior teeth were included in this study and was not distinguished
between the types of teeth. In a future study, it could examine only premolars or molars, or a
comparison of the different teeth types to see if there is any difference in the DEXIS CariVuTM in
the detection of caries.
In this study, the CariVuTM images were taken on patients who already have bitewing
radiographs and the CariVuTM was used as an adjunct tool to aid in the decision to whether treat
the lesions. The patients with the CariVuTM images in this study were relatively older and
cooperative for the bitewing radiographs. However, the pediatric patients may not always be able
to cooperate for the bitewing radiograph. A future study could examine the use of the DEXIS
CariVuTM from a behavioral perspective and determine whether the DEXIS CariVuTM device
would be more tolerated in by the pediatric dental patients than the bitewing radiographs.
47
The subjects in this study were the residents and faculty of the UIC Department of Pediatric
Dentistry. Even though the DEXIS CariVuTM is available to be used in the clinic, there is still a
limited utilization by the residents and faculty. The subjects have had fairly limited exposure and
use of the DEXIS CariVuTM in both taking and interpreting of the images as compared to bitewing
radiographs. A future study where practitioners with more exposure and experience with the
CariVuTM device could be studied to eliminate the factor of inadequate experience.
48
VI. CONCLUSIONS
1. There is a difference in the accuracy of caries detection between bitewing radiographs and
CariVuTM images, with the bitewing radiographs being more accurate for no caries and
incipient caries, and the DEXIS CariVuTM being more accurate for caries reaching the DEJ.
The greatest difference was for incipient caries.
2. CariVuTM is equally as sensitive in detecting if there is any caries as bitewing radiograph,
however there is more false positives than bitewing radiograph. CariVuTM is more sensitive
in detecting caries reaching the DEJ than bitewing radiographs but also with more false
positives.
3. There is difference in the rater validity between the CariVuTM and bitewing radiograph,
with the bitewing being more valid than the CariVuTM.
49
CITED LITERATURE
Abdelaziz, M., Krejci, I., Perneger, T., Feilzer, A., & Vazquez, L. (2018). Near infrared transillumination compared with radiography to detect and monitor proximal caries: A clinical retrospective study. Journal of Dentistry, 70, 40–45.
Abogazalah, N., & Ando, M. (2017). Alternative methods to visual and radiographic examinations for approximal caries detection. Journal of Oral Science, 59(3), 315–322.
Abogazalah, N., Eckert, G. J., & Ando, M. (2017). In vitro performance of near infrared light
transillumination at 780-nm and digital radiography for detection of non-cavitated approximal caries. Journal of Dentistry, 63, 44–50.
American Academy of Pediatric Dentistry Clinical Affairs Committee, American Board of
Pediatric Dentistry. Guideline on Caries-risk Assessment and Management for Infants, Children, and Adolescents, Revised 2014. Pediatric Dentistry, Reference Manual, May 2015; 37 (6) 132-139.
American Dental Association. The use of dental radiographs: Update and recommendations.
(2006). The Journal of the American Dental Association, 137(9), 1304–1312. Bader, J. D., Shugars, D. A., & Bonito, A. J. (2001). Systematic reviews of selected dental caries
diagnostic and management methods. Journal of Dental Education, 65(10), 960 LP-968.
Bader, J. D., &Shugars, D. A. N. A. (2004). A systematic review of the performance of a laser fluorescence device for detecting caries. The Journal of the American Dental Association, 135(10), 1413–1426.
Baltacioglu, I. H., & Orhan, K. (2017). Comparison of diagnostic methods for early
Oral Health, 17(1), 130. Berg SC, Stahl JM, Lien W, Slack CM, Vandewalle KS. A clinical study comparing digital
radiography and near‐infrared transillumination in caries detection. J Esthet Restor Dent. 2018;30:39–44.
Braga, M. M., Mendes, F. M., & Ekstrand, K. R. (2010). Detection activity assessment and diagnosis of dental caries lesions. Dental Clinics of North America, 54(3), 479–493.
Bizhang, M., Wollenweber, N., Singh-Hüsgen, P., Danesh, G., & Zimmer, S. (2016). Pen-type laser fluorescence device versus bitewing radiographs for caries detection on approximal surfaces. Head & Face Medicine, 12(1), 30.
Çolak H, Dülgergil ÇT, Dalli M, Hamidi MM. Early childhood caries update: A review of causes, diagnoses, and treatments. Journal of Natural Science, Biology, and Medicine. 2013;4(1):29-38.
50
“DEXIS CariVu,” DEXIS Digital X-ray & Imaging, CariVu, accessed December 2016, http://www.dexis.com/carivu.
DEXIS, LLC. DEXIS CariVu Operator Manual. Copyright 2013-2014. Dye BA, Thornton-Evans G, Li X, Iafolla TJ. Dental caries and sealant prevalence in children
and adolescents in the United States, 2011–2012. NCHS data brief, no 191. Hyattsville, MD: National Center for Health Statistics. 2015.
Ekstrand KR. (2004) Improving clinical visual detection--potential for caries clinical trials. J
Dent Res. 83 Spec No C: C67-71. Elhennawy, K., Askar, H., Jost-Brinkmann, P.-G., Reda, S., Al-Abdi, A., Paris, S., &
Schwendicke, F. (2018). In vitro performance of the DIAGNOcam for detecting proximal carious lesions adjacent to composite restorations. Journal of Dentistry, 72, 39–43.
Ellwood, R. P., & Côrtes, D. F. (2004). In vitro Assessment of Methods of Applying the Electrical Caries Monitor for the Detection of Occlusal Caries. Caries Research, 38(1), 45–53.
Featherstone, J. (2008), Dental caries: a dynamic disease process. Australian Dental Journal, 53:
286-291.
Gift HC, Reisine ST, Larach DC. The social impact of dental problems and visits. Am J Public Health. 1992; 82(12):1663–1668.
Gomez, J., Tellez, M., Pretty, I. A., Ellwood, R. P., & Ismail, A. I. (2013). Non-cavitated carious lesions detection methods: a systematic review. Community Dentistry and Oral Epidemiology, 41(1), 55–66.
Hamilton, J. C., & Stookey, G. (2005). Should a dental explorer be used to probe suspected carious lesions? The Journal of the American Dental Association, 136(11), 1526–1532.
Ko, H.-Y., Kang, S.-M., Kim, H. E., Kwon, H.-K., & Kim, B.-I. (2015). Validation of
quantitative light-induced fluorescence-digital (QLF-D) for the detection of approximal caries in vitro. Journal of Dentistry, 43(5), 568–575.
Kühnisch, J., Söchtig, F., Pitchika, V., Laubender, R., Neuhaus, K. W., Lussi, A., & Hickel, R.
(2016). In vivo validation of near-infrared light transillumination for interproximal dentin caries detection. Clinical Oral Investigations, 20(4), 821–829.
Campus, G. (2017). Digital transillumination in caries detection versus radiographic and clinical methods: an in-vivo study. Dento Maxillo Facial Radiology, 46(4), 20160417.
Lederer, A., Kunzelmann, K.-H., Heck, K., Hickel, R., & Litzenburger, F. (2019). In vitro
51
validation of near-infrared transillumination at 780 nm for the detection of caries on proximal surfaces. Clinical Oral Investigations.
Litzenburger, F., Heck, K., Pitchika, V., Neuhaus, K. W., Jost, F. N., Hickel, R., Kühnisch, J. (2018). Inter- and intraexaminer reliability of bitewing radiography and near-infrared light transillumination for proximal caries detection and assessment. Dentomaxillofacial Radiology, 47(3), 20170292.
Longbottom, C., & Huysmans, M.-C. D. N. J. M. (2004). Electrical Measurements for Use in Caries Clinical Trials. Journal of Dental Research, 83(1_suppl), 76–79.
Matalon, S., Feuerstein, O., & Kaffe, I. (2003). Diagnosis of approximal caries: Bite-wing
radiology versus the Ultrasound Caries Detector. An in vitro study. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontology, 95(5), 626–631.
Ozkan, G., & Guzel, K. G. U. (2017). Clinical evaluation of near-infrared light transillumination in approximal dentin caries detection. Lasers in Medical Science, 32(6), 1417–1422.
Pitts NB. (1996) The use of bitewing radiographs in the management of dental caries: scientific and practical considerations. Dentomaxilofac Radiol, 25(1):5-1
Pitts NB. Clinical diagnosis of dental caries: a European perspective. Journal of Dental Education 2001;65(10):972–8.
Schaefer, G., Pitchika, V., Litzenburger, F., Hickel, R., & Kühnisch, J. (2018). Evaluation of occlusal caries detection and assessment by visual inspection, digital bitewing radiography and near-infrared light transillumination. Clinical Oral Investigations, 22(7), 2431–2438.
Schwendicke, F., Tzschoppe, M., & Paris, S. (2015). Radiographic caries detection: A systematic review and meta-analysis. Journal of Dentistry, 43(8), 924–933.
Shi, X.-Q., Tranaeus, S., & Angmar-Månsson, B. (2001). Validation of DIAGNOdent for
quantification of smooth-surface caries: an in vitro study. Acta Odontologica Scandinavica, 59(2), 74–78.
Söchtig F, Hickel R, Kühnisch J. Caries detection and diagnostics with near-infrared light
transillumination: clinical experiences. Quintessence Int. 2014 Jun;45(6):531-8. Twetman, S., Axelsson, S., Dahlén, G., Espelid, I., Mejàre, I., Norlund, A., & Tranæus, S.
(2013). Adjunct methods for caries detection: A systematic review of literature. Acta Odontologica Scandinavica, 71(3–4), 388–397.
52
van Stralen, K. J., Stel, V. S., Reitsma, J. B., Dekker, F. W., Zoccali, C., & Jager, K. J. (2009). Diagnostic methods I: sensitivity, specificity, and other measures of accuracy. Kidney International, 75(12), 1257–1263.
Young, D. A., Nový, B. B., Zeller, G. G., Hale, R., Hart, T. C., Truelove, E. L., Beltran- Aguilar,
E. (2015). The American Dental Association Caries Classification System for Clinical Practice: A report of the American Dental Association Council on Scientific Affairs. The Journal of the American Dental Association, 146(2), 79–86.
Yu JL, Tang RT, Feng L, Dong YM. (2017) Digital imaging fiber optic transillumination (DIFOTI) method for determining the depth of cavity. Beijing Da Xue Xue Bao Yi Xue Ban, 49(1):81-5. Chinese.
Zandoná, A. F., & Zero, D. T. (2006). Diagnostic tools for early caries detection. The Journal of
the American Dental Association, 137(12), 1675–1684. Zhou Q, Peng CF, Qin M. (2019) Near-infrared light transillumination for detection of incipient
proximal caries in primary molars. Beijing Da Xue Xue Bao Yi Xue Ban. 2, 51(1):59-64.
53
APPENDICES
APPENDIX A
Exemption Granted February 5, 2019 Ann Mast Pediatrics RE: Research Protocol # 2018-1605 “Comparison of DEXIS CariVuTM caries detection device to traditional bite wing radiography for diagnosis of interproximal caries in young permanent teeth” Funding Source/Sponsor: None Dear Ann Mast: Your Claim of Exemption was reviewed on February 5, 2019 and it was determined that your research meets the criteria for exemption. You may now begin your research. Performance Site: UIC Subject Population: a) Adult (18+ years) pediatric dental residents and faculty members at the UIC Department of Pediatric Dentistry b) De-identified medical records initially collected for clinical purposes Number of Subjects: a) 40 b) 100 The specific exemption categories under 45 CFR 46.101(b) are: 2 and 4 HIPAA Waiver: The Board determined that this research meets the regulatory requirements for waiver of authorization as permitted at 45CFR164.512(i)(1)(i)(A). Specifically, that the use or disclosure of protected health information (PHI) meets the waiver criteria under 45CFR164.512(i)(2)(ii); the research involves no more than a minimal risk to the privacy of the individuals; the research could not practicably be conducted without the waiver; and the research could not practicably be conducted without access to and use of the PHI. You are reminded that investigators whose research involving human subjects is determined to be exempt from the federal regulations for the protection of human subjects still have responsibilities for the ethical conduct of the research under state law and UIC policy. Please be aware of the following UIC policies and responsibilities for investigators:
54
APPENDIX A (continued) Amendments You are responsible for reporting any amendments to your research protocol that may affect the determination of the exemption and may result in your research no longer being eligible for the exemption that has been granted. Record Keeping You are responsible for maintaining a copy all research related records in a secure location in the event future verification is necessary, at a minimum these documents include: the research protocol, the claim of exemption application, all questionnaires, survey instruments, interview questions and/or data collection instruments associated with this research protocol, recruiting or advertising materials, any consent forms or information sheets given to subjects, or any other pertinent documents. Final Report When you have completed work on your research protocol, you should submit a final report to the Office for Protection of Research Subjects (OPRS). Please be sure to use your research protocol number (2018-1605) on any documents or correspondence with the IRB concerning your research protocol. We wish you the best as you conduct your research. If you have any questions or need further help, please contact the OPRS office at (312) 996-1711 or me at (312) 355-2908. Sincerely, Charles W. Hoehne, B.S., C.I.P. Assistant Director, IRB #7 Office for the Protection of Research Subjects
55
APPENDIX B Images 1-9
56
APPENDIX B (continued)
Images 10-18
57
APPENDIX B (continued)
Images 19-27
58
APPENDIX B (continued)
Images 28-36
59
APPENDIX B (continued)
Images 37-45
60
APPENDIX B (continued)
Images 46-54
61
APPENDIX B (continued)
Images 55-63
62
APPENDIX B (continued)
Images 64-72
63
APPENDIX B (continued)
Images 73-81
64
APPENDIX B (continued)
Images 82-90
65
APPENDIX B (continued)
Images 91-99
66
APPENDIX B (continued)
Images 100-108
67
APPENDIX B (continued)
Images 109-117
68
APPENDIX B (continued)
Images 118-126
69
APPENDIX B (continued)
Images 127-135
70
APPENDIX B (continued)
Images 136-144
71
APPENDIX B (continued)
Images 145-153
72
APPENDIX B (continued)
Images 154-162
73
APPENDIX B (continued)
Images 163-171
74
APPENDIX B (continued)
Images 172-180
75
APPENDIX C
Dear Prospective Participant, We are attempting to ascertain how different diagnostic images are viewed and interpreted by practitioners. This study is strictly voluntary, and you can withdraw at any time. Every effort will be made to keep your participation confidential. Your decision whether or not to participate will not impact your relationship with UIC or the Department and will not impact your standing. There will be no risks involved in completing the questionnaire. The questionnaire will take you no longer than 30 minutes to complete. You will see a series of images. Some of these are traditional bite wing images. Some of these are CariVuTM images which were captured from the occlusal view of the tooth. You will be asked to classify each image as:
0 - No Caries 1 - Incipient caries not touching the DEJ 2 - Caries touching the DEJ and into dentin
For questions, you may contact the Primary Investigator, Ann Mast, DDS, at [email protected]. If you have any questions about rights as a research subject, please contact the office of protection of research subjects of the University of Illinois at Chicago at (312) 996-1711.
76
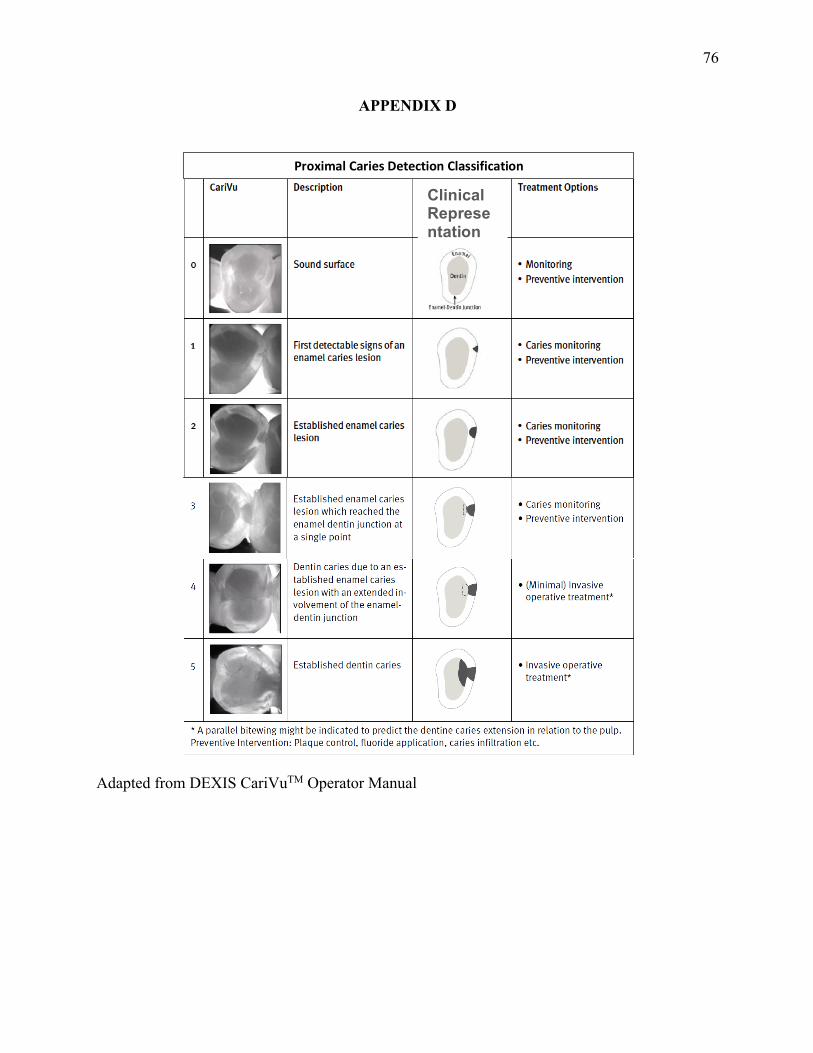
APPENDIX D
Adapted from DEXIS CariVuTM Operator Manual
Proximal Caries Detection Classification
Clinical Representation
77
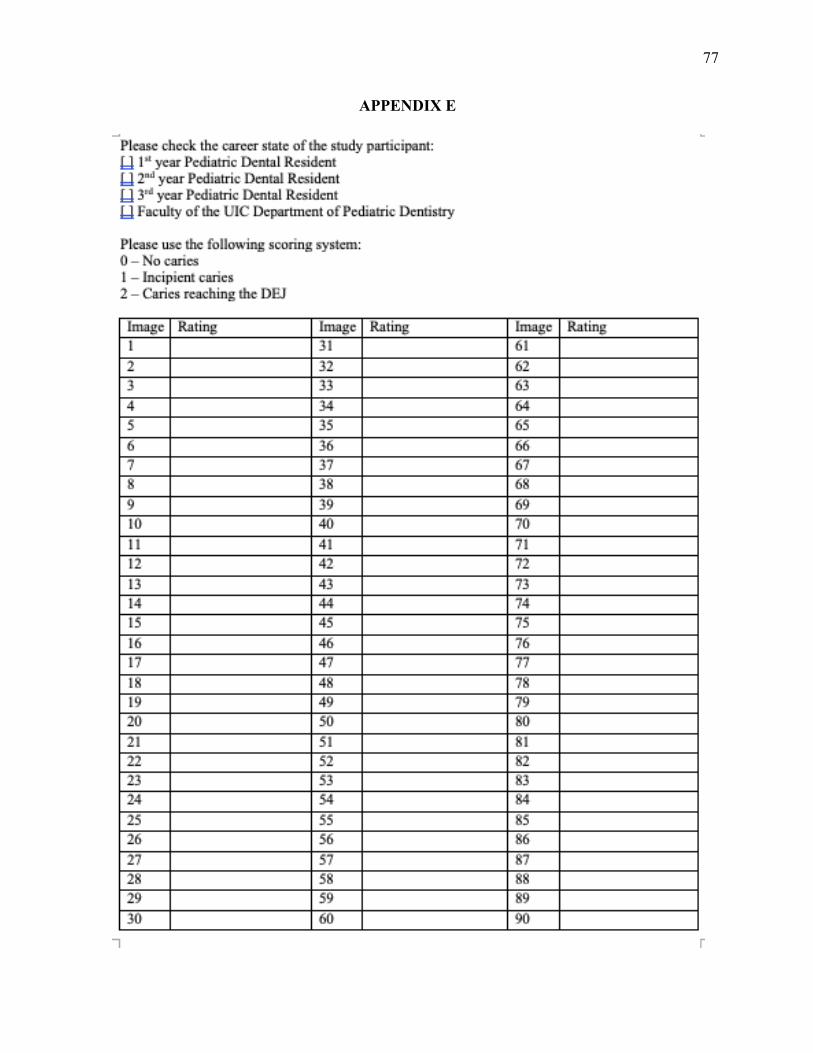
APPENDIX E
78
APPENDIX E (continued)
79
VITA
Ann Mast, DDS
PUBLICATIONS: Kennedy, S. A., Frazier, M. L., Steiniger, M., Mast, A. M., Marzluff, W. F., & Redinbo,
M. R. (2009). Crystal Structure of the HEAT Domain from the Pre-mRNA Processing Factor Symplekin. Journal of Molecular Biology, 392(1), 115–128.
EDUCATION: University of Illinois at Chicago, Chicago, Illinois 2017- 2019 Certificate in Pediatric Dentistry Master of Oral Sciences University of North Carolina, School of Dentistry, Chapel Hill, North
Carolina 2010 - 2014
Doctor of Dental Surgery University of North Carolina, Chapel Hill, North Carolina 2006 –2010 Bachelor of Science in Biology Bachelor of Arts in Asian Studies EMPLOYMENT: United States Air Force 2014 - 2017 General Dentist
Commissioned Officer – Captain LICENSURE: North Carolina State Dental License May, 2014 Illinois State Dental License July, 2017
PROFESSIONAL MEMBERSHIP: American Academy of Pediatric Dentistry 2017 - current Illinois Society of Pediatric Dentists