Introduction: My name is Frank Nicolosi, thank you very much for inviting me today.(Feb. 25, 2008) In Today’s lecture of Mental Capacity/Competency I would like to approach this in the way that we all can learn from each other. Since this group is relatively small, I think we can leave the floor open to questions, comments, insights to go along with my actual presentation. I believe this will help keep the flow going well and be the most enjoyable way to tackle this very interesting and challenging topic. Ok, now I have my ‘lecture handouts’. I refer to them as such, as I would like your to follow my talk with these notes. These notes are the abbreviated version, but the entire ‘lecture notes’ can be found on my website: www.illinoismediationlaw.com . (Go to my website, look under lecture and you will find the entire lecture notes available). Please feel free to scribble any notes on them, as the handouts of course are yours to keep and it is my hope that you can use these in the future as good references for ‘Mental Competency’ issues. (the handouts follow my lecture, but also listed are my references and other information that I feel can be very helpful to all of us in the future. First of all an over view of what we will cover: 1
Transcript
Introduction:
My name is Frank Nicolosi, thank you very much for inviting me today.(Feb. 25, 2008)
In Today’s lecture of Mental Capacity/Competency I would like to approach this in the way that we all can learn from each other. Since this group is relatively small, I think we can leave the floor open to questions, comments, insights to go along with my actual presentation. I believe this will help keep the flow going well and be the most enjoyable way to tackle this very interesting and challenging topic.
Ok, now I have my ‘lecture handouts’. I refer to them as such, as I would like your to follow my talk with these notes. These notes are the abbreviated version, but the entire ‘lecture notes’ can be found on my website: www.illinoismediationlaw.com . (Go to my website, look under lecture and you will find the entire lecture notes available). Please feel free to scribble any notes on them, as the handouts of course are yours to keep and it is my hope that you can use these in the future as good references for ‘Mental Competency’ issues. (the handouts follow my lecture, but also listed are my references and other information that I feel can be very helpful to all of us in the future.
First of all an over view of what we will cover:
I. Brief IntroductionII. Mental Competency for Lawyers/JudgesIII. Mental Competency for Physicians and Health Care WorkersIV. Summary
I. Introduction:As we all know Mental Competency, or ‘Mental Incompetency’ is a very hot topic in both law and medicine. Lawyers can be faced sometimes often with having to make decisions on a client’s competency. Such areas including wills, estates, guardianships are just some of these areas.Judges also can at times be faced with deciding a plaintiff’s or a defendant’s ‘mental competency’.
As a physician, health care worker we are often also faced with problems of ‘is this patient mentally competent to live alone, take care of him or her self, take his/her own medicines, etc. Also, such decisions as , can this person competently decide on if a procedure should be done, or can he/she decide what plan of treatment would be suitable for them and would they be able to follow such plan?
Ok, now to the ‘legal aspect’ of competency:
II. Legal CompetencyWhen preparing this lecture/dialogue, I felt that it would be very helpful to at least ‘touch base’ on some principles that I thought are crucial to ‘legal mental competency’. Although, again my focus is medical competency, as attorneys it is my hope that you will be able to gather and keep some ‘Take Home Points’ that can be used in your every day and not so every days of your practice.
First of all, since legal competency issues can cover many areas of law, (if not technically all areas), as some have been mentioned above, I would like to direct our energies first on: Guardianships. Guardianships, as we know, a Guardianship is needed when a person is unable to make and communicate responsible decisions regarding his personal care or finances due to a mental, physical or developmental disability.
The extent to which a guardian is allowed to make decisions for a ward is determined by the court based on a thorough clinical evaluation and report.
Two basic types of guardianship are "person guardianship" and "estate guardianship ". (as we know….) “guardian of the person" is appointed by the court when a disabled individual cannot make or communicate responsible decisions regarding his personal care. This guardian will make decisions about medical treatment, residential placement, social services and other needs.
2
The court appoints a "guardian of the estate" when a disabled person is unable to make or communicate responsible decisions regarding the management of his estate or finances. The guardian will, subject to court supervision, make decisions about the ward's funds and the safeguarding of the ward's income or other assets.
Excellent Handbook (Must Get) :
ASSESSMENT of Older AdultsWITH DIMINISHED CAPACITY:
A Handbook for LawyersAssessment of Older Adults with Diminished Capacity: A Handbook for Lawyers
------American Bar Association Commission on Law and Aging and American Psychological Association. With the coming demographic avalanche as the Boomers reach their 60s and the over-80 population swells, lawyers face a growing challenge: older clients with problems in decision-making capacity. While most older adults will not have impaired capacity, some will. Obvious dementias impair decision-making capacity-but what about older adults with an early stage of dementia or with mild central nervous system damage? Such clients may have subtle decisional problems and questionable judgments troubling to a lawyer. Assessment of Older Adults with Diminished Capacity: A Handbook for Lawyers offers ideas for effective practices and makes suggestions for attorneys who wish to balance the competing goals of autonomy and protection as they confront the difficult challenges of working with older adults with diminished capacity. 80 pp. 2005. ISBN 1-59031-497-2/ Product Code: 4280025. $25. L
Judicial Determination of Capacity of Older Adults in Guardianship Proceedings
-------American Bar Association Commission on Law and Aging, American Psychological Association, and National College of Probate Judges. This book contains practical tools to equip a wide audience of judges to conduct
any form of guardianship proceeding more effectively, improve communication with healthcare professionals, creatively use less-restrictive alternatives and limited guardianships, and accommodate disabilities of older adults in ways that will enhance capacity. Specifically, the handbook 1) outlines the “six pillars of capacity assessment,” essential to a full and accurate assessment of capacity; and 2) gives a practical explanation of the “five key steps in judicial determination of capacity.” The handbook provides a layered information approach that enables you to go as far as you need to on any aspect of capacity assessment. Links to expanded information, work sheets, model forms, and fact sheets are available at no charge on the Web site of the ABA Commission on Law and Aging at http://www.abanet.org/aging/. 41 pp. 2006. ISBN 978-1-59031-764-8/Product Code: 4280026. $25. J.
From The Handbook of Lawyers:
1. What are legal standards of diminished
capacity?
2. What are clinical models of capacity?
3. What signs of diminished capacity should a
lawyer be observing?
4. Capacity Worksheet for Lawyers (pp. 23 - 26)
This capacity worksheet helps you identify andorganize:
1. Observational signs of diminished capacity.2. Mitigating factors affecting capacity.3.Transaction-specific elements of legal capacity.4. Task-specific factors in evaluating capacity.5. Preliminary conclusions about client capacity.6. What mitigating factors should a lawyer take into account?
7. Should a lawyer use formal clinical assessmentinstruments? (Ch. IV, pp. 21 - 22). It is generallynot appropriate for lawyers to use formal clinical
assessment instruments such as the Mini-MentalStatus Examination (MMSE), as they are not trainedin using and interpreting these tests, the information yielded is limited, and the results may be misleading.
Unavoidable capacity determinations:
1. Does the client have the capacity to contractfor my services?2. Does the client have the capacity to completethe legal transaction?
Lawyers need a conceptually sound andconsistent process for answering these questions.
***Lawyers need to be familiar with three facets ofdiminished capacity:
1. Standards of capacity for specific legaltransactions.2. Approaches to capacity in state guardianshipand conservatorship laws.3. Ethical guidelines for assessing client capacity.
Another source to at look at:
Science, common sense, and the determination of mental capacity.By Frolik, LawrencePsychology, Public Policy, and Law. Vol 5(1), Mar 1999, 41-58.AbstractIn 1993, when the Supreme Court decided Daubert and created the modern standard for the admissibility of scientific evidence, it almost certainly did not consider its possible effect on evidentiary hearings in probate courts even though such courts routinely admit expert testimony in will contests and guardianship hearings. Probate courts also admit
5
testimony of lay witnesses who express their opinion as to the mental capacity of the individual in question. Yet both expert and lay witnesses are only "fact bringers" and not "fact interpreters" because the ultimate question of capacity is legal, not factual. Because the determination of legal capacity is made by the judge or jury, the role of experts in capacity trials is not fundamentally different than that of lay persons. The limited role of the expert suggests that probate courts should allow great latitude in the admission of expert testimony because the fact finders must ultimately rely on their own amorphous sense of "legal capacity." (PsycINFO Database Record (c) 2008 APA, all rights reserved)
(I would be happy to e-mail this above full article to anyone who e-mails me)
III. Mental Competency for Physicians and Health Care Workers
Several of many good Articles on Mental Capacity:
Competency Evaluations Start With Five Senses: Ken Hausman, Psychiatric News, May 16, 2003
A forensic psychiatrist who is often called on to conduct mental competency evaluations of elderly individuals advises colleagues on the dos and don’ts of such assessments. Carla Rodgers, M.D.
Rodgers urges psychiatrists who conduct competency evaluations to rely on their senses of sight, smell, touch, and hearing to fill in a substantial number of the competency evaluation blanks.
She also advised psychiatrists to pay attention to an evaluee’s facial expression, grooming such as nail care, and clothing. Clothing that is disheveled or rife with food stains could be signs of a loss of mental competence
As for hearing, she urged psychiatrist evaluators to listen for wheezing and hoarseness and, though it may seem basic, whether the person can hear what the psychiatrist is saying, which includes "checking to make sure hearing aids are actually turned on."
Rodgers also urged psychiatrist evaluators to obtain as much collateral data as possible. These should come from the evaluee’s medical charts and laboratory reports, hospital and nursing-home staff or other caregivers, family members, the attending physician, and other consultants.
Throughout a competency evaluation the psychiatrist should keep in mind the specific type of competency at issue.
If, for example, competency to make a will is being assessed, key issues evaluators need to assess center on whether the elderly person knows who his or her natural heirs are and the nature and extent of the estate involved.
Evaluating a person’s competence to make medical decisions, in contrast, requires that the individual know what is wrong with him or her and who is doing the treating, as well as understand the proposed treatment in general terms and the risks and benefits of that treatment compared with receiving no treatment, Rodgers explained.
And do not overlook an exploration of the family’s motives in requesting a competency evaluation, she cautioned. Do family members have reason for wanting their oddly behaving relative to be declared incompetent?
capacity." (PsycINFO Database Record (c) 2008 APA, all rights reserved)
UPtoDate website:
http://www.uptodate.com
Evaluation of cognitive impairment and dementia
Authors Marie-Florence Shadlen, MDEric B Larson, MD, MPH
Section Editors Steven T DeKosky, MD, FAANKenneth E Schmader, MD
Patients and informants are often uncertain about the onset
of symptoms since the appearance of dementia is insidious.
The physician can usually date the onset of dementia by
identifying when the patient stopped driving or managing
finances. Useful questions for the patient and informant are,
"When did you first notice the memory loss?" and "How has
the memory loss progressed since then?"
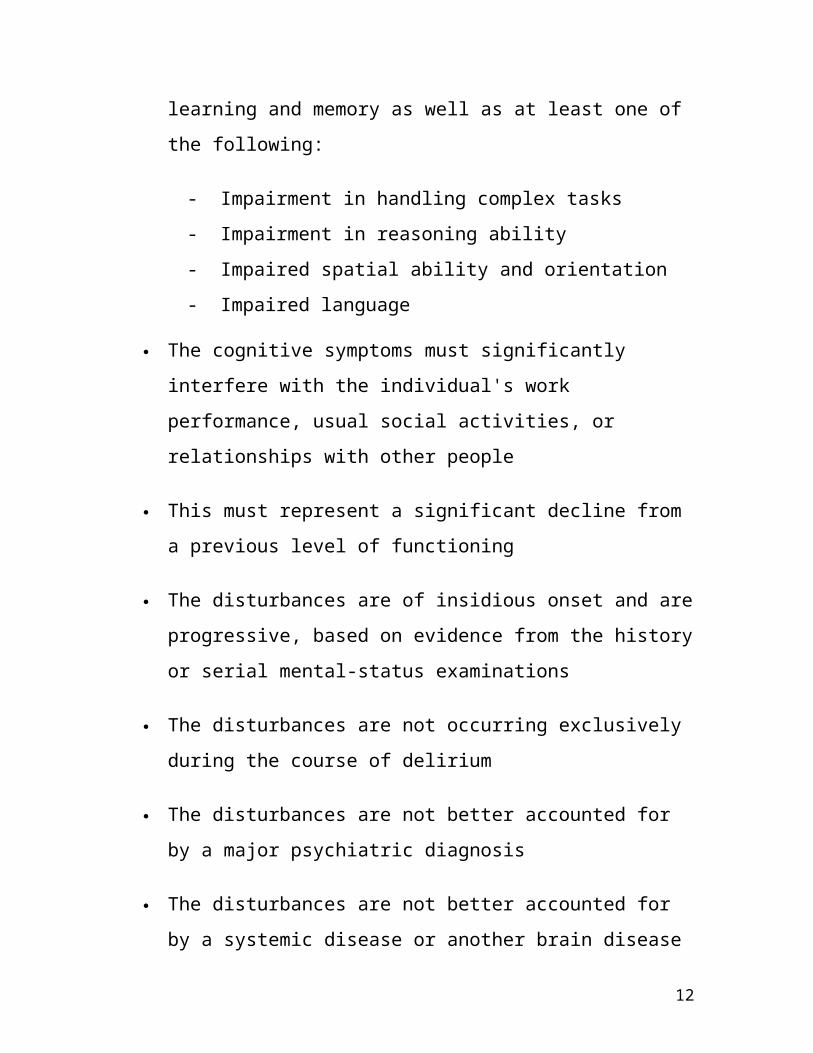
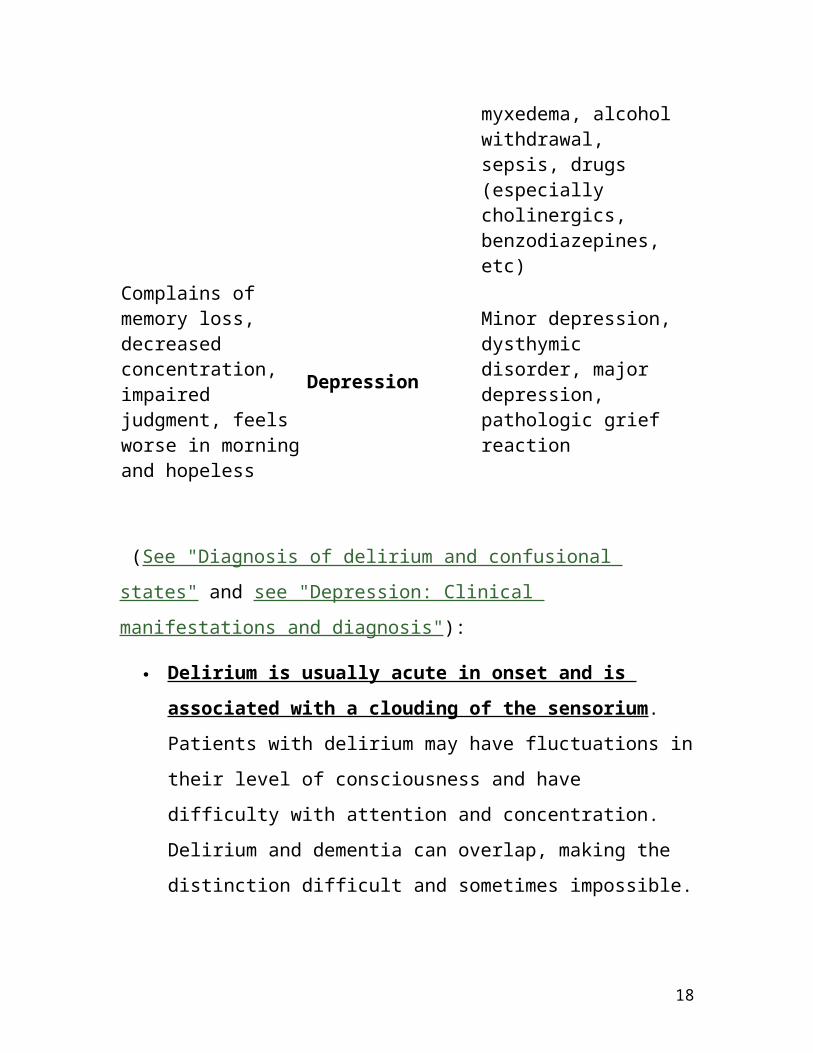
The diagnosis of dementia must be distinguished
from delirium and depression (show table 2) [17].
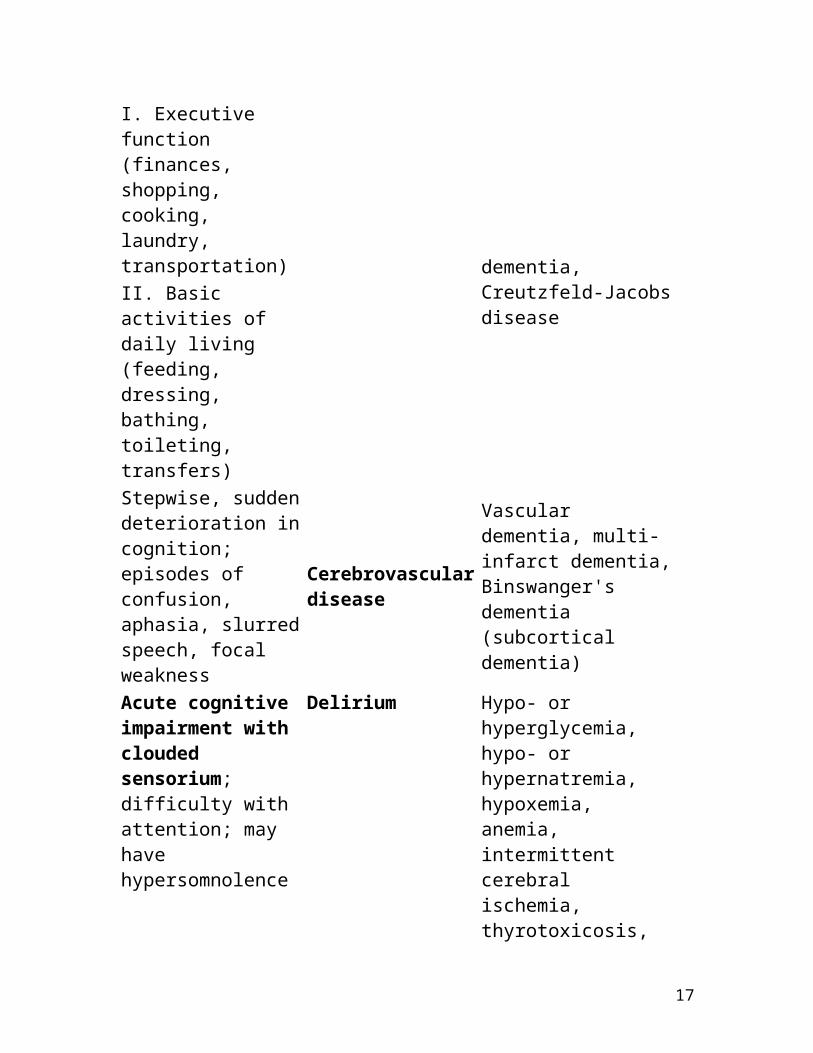
Table 2
Differential diagnosis of memory loss Symptom Usual cause Examples Gradual onset of short-term memory loss and functional impairment in more than one domain:
I. Executive function (finances, shopping, cooking, laundry, transportation) II. Basic activities of daily living (feeding, dressing, bathing, toileting, transfers) Stepwise, sudden deterioration in cognition; episodes of confusion,
3. The disturbance in 1 and 2 significantly interferes with work, social activities, or relationships
18
4. Disturbance does not occur exclusively during delirium
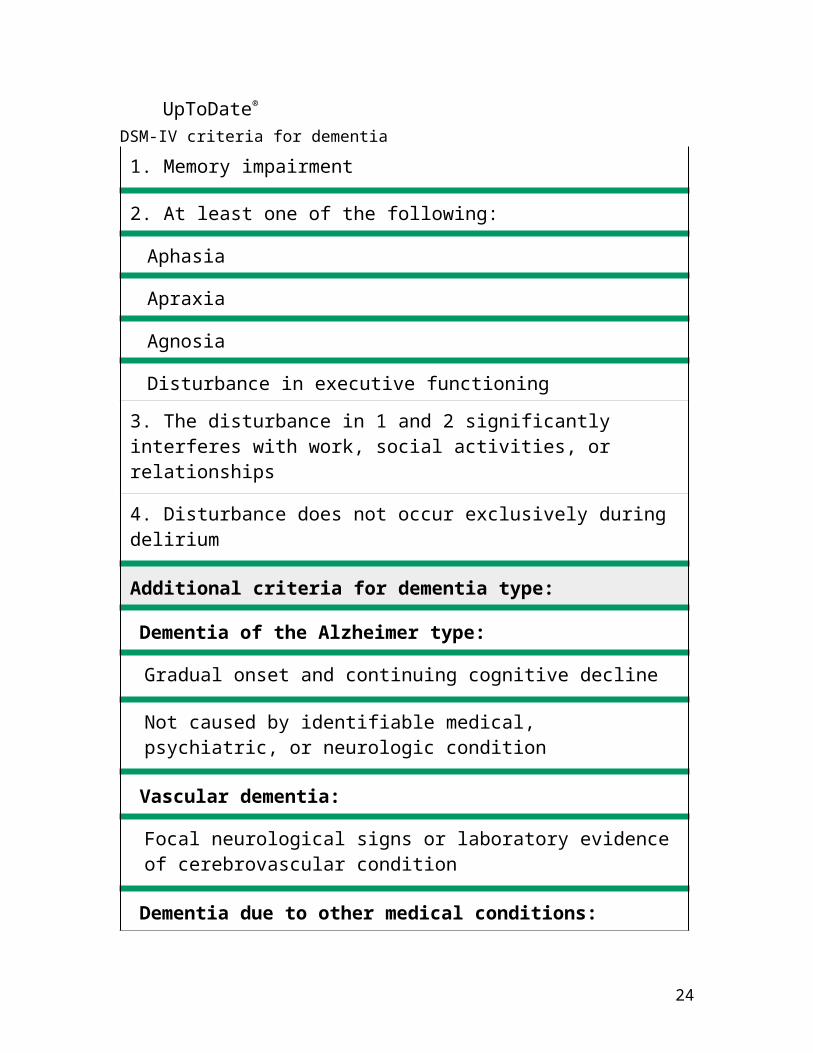
Additional criteria for dementia type:
Dementia of the Alzheimer type:
Gradual onset and continuing cognitive decline
Not caused by identifiable medical, psychiatric, or neurologic condition
Vascular dementia:
Focal neurological signs or laboratory evidence of cerebrovascular condition
Dementia due to other medical conditions:
Evidence from history, physical exam, or laboratory findings of a specific medical condition causing cognitive deficits (HIV disease, head trauma, Parkinson disease, Huntington's chorea, Pick's disease, Creutzfeld-Jacob)
Adapted from American Psychiatric Association Diagnostic and Statistical Manual, 4th ed, APA Press, Washington DC, 1994.
Cognitive testing — Agreement between the history
and the mental status examination is strongly
suggestive of the diagnosis of dementia. When the
history suggests cognitive impairment but the mental status
examination is normal, possible explanations include mild
dementia, high intelligence or education, depression, or
rarely, misrepresentation on the part of the informants [28].
Conversely, when the mental status examination suggests
Screening for B12 deficiency and hypothyroidism is
recommended for patients being evaluated for
dementia.
Screening for depression in patients with dementia is
recommended because depression is a common
treatable comorbidity that may also masquerade as
dementia.
Genetic testing for the apolipoprotein E epsilon 4 allele
is not currently recommended, nor is genetic testing for
other potential causes of dementia.
Structural neuroimaging with either a noncontrast head
CT or MRI is recommended in the routine initial
evaluation of all patients with dementia.
Use of UpToDate is subject to the Subscription and
License Agreement.
References:
1) www.uptodate.com
2) ASSESSMENT of Older Adults WITH DIMINISHED CAPACITY: (A Handbook for Lawyers) http://www.abanet.org/aging/publications/publicationslistorder.shtml#capacity
3) Science, common sense, and the determination of mental capacity. By Frolik, Lawrence Psychology, Public Policy, and Law. Vol 5(1), Mar 1999, 41-58.
(I can( e-mail) send this to anyone wanting the entire 18 page article)
4) American Psychiatric Association Diagnostic and Statistical Manual, 4th ed, APA Press, Washington DC, 1994 5)Jacobson: Psychiatric Secrets, 2nd ed. Second Edition
James L. Jacobson, MD Associate Professor, Department of Psychiatry, University of Vermont
Medical School, Burlington, Vermont Alan M. Jacobson, MD Professor, Department of Psychiatry, Harvard Medical School Senior Vice President, Strategic Initiatives, Joslin Diabetes Center, Boston, Massachusetts
6) Early Diagnosis of Dementia, American Family Physician.February 15, 2001 http://www.aafp.org/afp/AFPprinter/20010215/703.html?print=yes
7) Competency Evaluations Start With Five Senses: Ken Hausman, Psychiatric News, May 16, 2003