

Introduction:
My name is Frank Nicolosi, thank you very much for inviting me today.(Feb. 25, 2008)
In Today’s lecture of Mental Capacity/Competency I would like to approach this in the way that we all can learn from each other. Since this group is relatively small, I think we can leave the floor open to questions, comments, insights to go along with my actual presentation. I believe this will help keep the flow going well and be the most enjoyable way to tackle this very interesting and challenging topic.
Ok, now I have my ‘lecture handouts’. I refer to them as such, as I would like your to follow my talk with these notes. These notes are the abbreviated version, but the entire ‘lecture notes’ can be found on my website: www.illinoismediationlaw.com . (Go to my website, look under lecture and you will find the entire lecture notes available). Please feel free to scribble any notes on them, as the handouts of course are yours to keep and it is my hope that you can use these in the future as good references for ‘Mental Competency’ issues. (the handouts follow my lecture, but also listed are my references and other information that I feel can be very helpful to all of us in the future.
First of all an over view of what we will cover:
I. Brief IntroductionII. Mental Competency for Lawyers/JudgesIII. Mental Competency for Physicians and Health Care WorkersIV. Summary
I. Introduction:As we all know Mental Competency, or ‘Mental Incompetency’ is a very hot topic in both law and medicine. Lawyers can be faced sometimes often with having to make decisions on a client’s competency. Such areas including wills, estates, guardianships are just some of these areas.Judges also can at times be faced with deciding a plaintiff’s or a defendant’s ‘mental competency’.
1
As a physician, health care worker we are often also faced with problems of ‘is this patient mentally competent to live alone, take care of him or her self, take his/her own medicines, etc. Also, such decisions as , can this person competently decide on if a procedure should be done, or can he/she decide what plan of treatment would be suitable for them and would they be able to follow such plan?
Ok, now to the ‘legal aspect’ of competency:
II. Legal CompetencyWhen preparing this lecture/dialogue, I felt that it would be very helpful to at least ‘touch base’ on some principles that I thought are crucial to ‘legal mental competency’. Although, again my focus is medical competency, as attorneys it is my hope that you will be able to gather and keep some ‘Take Home Points’ that can be used in your every day and not so every days of your practice.
First of all, since legal competency issues can cover many areas of law, (if not technically all areas), as some have been mentioned above, I would like to direct our energies first on: Guardianships. Guardianships, as we know, a Guardianship is needed when a person is unable to make and communicate responsible decisions regarding his personal care or finances due to a mental, physical or developmental disability.
The extent to which a guardian is allowed to make decisions for a ward is determined by the court based on a thorough clinical evaluation and report.
Two basic types of guardianship are "person guardianship" and "estate guardianship ". (as we know….) “guardian of the person" is appointed by the court when a disabled individual cannot make or communicate responsible decisions regarding his personal care. This guardian will make decisions about medical treatment, residential placement, social services and other needs.
2
The court appoints a "guardian of the estate" when a disabled person is unable to make or communicate responsible decisions regarding the management of his estate or finances. The guardian will, subject to court supervision, make decisions about the ward's funds and the safeguarding of the ward's income or other assets.
Excellent Handbook (Must Get) :
ASSESSMENT of Older AdultsWITH DIMINISHED CAPACITY:
http://www.abanet.org/aging/publications/publicationslistorder.shtml#capacity
A Handbook for LawyersAssessment of Older Adults with Diminished Capacity: A Handbook for Lawyers
------American Bar Association Commission on Law and Aging and American Psychological Association. With the coming demographic avalanche as the Boomers reach their 60s and the over-80 population swells, lawyers face a growing challenge: older clients with problems in decision-making capacity. While most older adults will not have impaired capacity, some will. Obvious dementias impair decision-making capacity-but what about older adults with an early stage of dementia or with mild central nervous system damage? Such clients may have subtle decisional problems and questionable judgments troubling to a lawyer. Assessment of Older Adults with Diminished Capacity: A Handbook for Lawyers offers ideas for effective practices and makes suggestions for attorneys who wish to balance the competing goals of autonomy and protection as they confront the difficult challenges of working with older adults with diminished capacity. 80 pp. 2005. ISBN 1-59031-497-2/ Product Code: 4280025. $25. L
Judicial Determination of Capacity of Older Adults in Guardianship Proceedings
-------American Bar Association Commission on Law and Aging, American Psychological Association, and National College of Probate Judges. This book contains practical tools to equip a wide audience of judges to conduct
3

any form of guardianship proceeding more effectively, improve communication with healthcare professionals, creatively use less-restrictive alternatives and limited guardianships, and accommodate disabilities of older adults in ways that will enhance capacity. Specifically, the handbook 1) outlines the “six pillars of capacity assessment,” essential to a full and accurate assessment of capacity; and 2) gives a practical explanation of the “five key steps in judicial determination of capacity.” The handbook provides a layered information approach that enables you to go as far as you need to on any aspect of capacity assessment. Links to expanded information, work sheets, model forms, and fact sheets are available at no charge on the Web site of the ABA Commission on Law and Aging at http://www.abanet.org/aging/. 41 pp. 2006. ISBN 978-1-59031-764-8/Product Code: 4280026. $25. J.
From The Handbook of Lawyers:
1. What are legal standards of diminished
capacity?
2. What are clinical models of capacity?
3. What signs of diminished capacity should a
lawyer be observing?
4. Capacity Worksheet for Lawyers (pp. 23 - 26)
This capacity worksheet helps you identify andorganize:
1. Observational signs of diminished capacity.2. Mitigating factors affecting capacity.3.Transaction-specific elements of legal capacity.4. Task-specific factors in evaluating capacity.5. Preliminary conclusions about client capacity.6. What mitigating factors should a lawyer take into account?
7. Should a lawyer use formal clinical assessmentinstruments? (Ch. IV, pp. 21 - 22). It is generallynot appropriate for lawyers to use formal clinical
4

assessment instruments such as the Mini-MentalStatus Examination (MMSE), as they are not trainedin using and interpreting these tests, the information yielded is limited, and the results may be misleading.
Unavoidable capacity determinations:
1. Does the client have the capacity to contractfor my services?2. Does the client have the capacity to completethe legal transaction?
Lawyers need a conceptually sound andconsistent process for answering these questions.
***Lawyers need to be familiar with three facets ofdiminished capacity:
1. Standards of capacity for specific legaltransactions.2. Approaches to capacity in state guardianshipand conservatorship laws.3. Ethical guidelines for assessing client capacity.
Another source to at look at:
Science, common sense, and the determination of mental capacity.By Frolik, LawrencePsychology, Public Policy, and Law. Vol 5(1), Mar 1999, 41-58.AbstractIn 1993, when the Supreme Court decided Daubert and created the modern standard for the admissibility of scientific evidence, it almost certainly did not consider its possible effect on evidentiary hearings in probate courts even though such courts routinely admit expert testimony in will contests and guardianship hearings. Probate courts also admit
5
testimony of lay witnesses who express their opinion as to the mental capacity of the individual in question. Yet both expert and lay witnesses are only "fact bringers" and not "fact interpreters" because the ultimate question of capacity is legal, not factual. Because the determination of legal capacity is made by the judge or jury, the role of experts in capacity trials is not fundamentally different than that of lay persons. The limited role of the expert suggests that probate courts should allow great latitude in the admission of expert testimony because the fact finders must ultimately rely on their own amorphous sense of "legal capacity." (PsycINFO Database Record (c) 2008 APA, all rights reserved)
(I would be happy to e-mail this above full article to anyone who e-mails me)
III. Mental Competency for Physicians and Health Care Workers
Several of many good Articles on Mental Capacity:
Competency Evaluations Start With Five Senses: Ken Hausman, Psychiatric News, May 16, 2003
http://pn.psychiatryonline.org/cgi/content/full/38/10/34
A forensic psychiatrist who is often called on to conduct mental competency evaluations of elderly individuals advises colleagues on the dos and don’ts of such assessments. Carla Rodgers, M.D.
Rodgers urges psychiatrists who conduct competency evaluations to rely on their senses of sight, smell, touch, and hearing to fill in a substantial number of the competency evaluation blanks.
She also advised psychiatrists to pay attention to an evaluee’s facial expression, grooming such as nail care, and clothing. Clothing that is disheveled or rife with food stains could be signs of a loss of mental competence
As for hearing, she urged psychiatrist evaluators to listen for wheezing and hoarseness and, though it may seem basic, whether the person can hear what the psychiatrist is saying, which includes "checking to make sure hearing aids are actually turned on."
6

Rodgers also urged psychiatrist evaluators to obtain as much collateral data as possible. These should come from the evaluee’s medical charts and laboratory reports, hospital and nursing-home staff or other caregivers, family members, the attending physician, and other consultants.
Throughout a competency evaluation the psychiatrist should keep in mind the specific type of competency at issue.
If, for example, competency to make a will is being assessed, key issues evaluators need to assess center on whether the elderly person knows who his or her natural heirs are and the nature and extent of the estate involved.
Evaluating a person’s competence to make medical decisions, in contrast, requires that the individual know what is wrong with him or her and who is doing the treating, as well as understand the proposed treatment in general terms and the risks and benefits of that treatment compared with receiving no treatment, Rodgers explained.
And do not overlook an exploration of the family’s motives in requesting a competency evaluation, she cautioned. Do family members have reason for wanting their oddly behaving relative to be declared incompetent?
capacity." (PsycINFO Database Record (c) 2008 APA, all rights reserved)
UPtoDate website:
http://www.uptodate.com
Evaluation of cognitive impairment and dementia
Authors Marie-Florence Shadlen, MDEric B Larson, MD, MPH
Section Editors Steven T DeKosky, MD, FAANKenneth E Schmader, MD
7

INTRODUCTION — Dementia is a disorder that is
characterized by impairment of memory and at least
one other cognitive domain (aphasia, apraxia,
agnosia, executive function). These must represent a
decline from previous level of function and be severe
enough to interfere with daily function and
independence [1].
Alzheimer disease (AD) is the most common form of
dementia in the elderly, accounting for 60 to 80 percent of
cases, and it is estimated to affect more than 4 million
Americans [2-5].
DEFINITION OF DEMENTIA — Although a number of
definitions exist for dementia, the DSM-IV definition is
widely accepted and includes the following [1]:
Evidence from the history and mental status
examination that indicates major impairment in
learning and memory as well as at least one of the
following:
- Impairment in handling complex tasks
- Impairment in reasoning ability
- Impaired spatial ability and orientation
- Impaired language
The cognitive symptoms must significantly interfere
with the individual's work performance, usual social
activities, or relationships with other people
8
This must represent a significant decline from a
previous level of functioning
The disturbances are of insidious onset and are
progressive, based on evidence from the history or
serial mental-status examinations
The disturbances are not occurring exclusively during
the course of delirium
The disturbances are not better accounted for by a
major psychiatric diagnosis
The disturbances are not better accounted for by a
systemic disease or another brain disease
In a practice guideline published by the American Academy
of Neurology (AAN), the DSM-IIIR definition of dementia
(identical to the DSM-IV definition) was reported to have
good to very good reliability and was recommended for
routine use [8].
IDENTIFICATION OF DEMENTIA — Detecting dementia
is a problem in routine, day-to-day medical practice
[9]. One study found that the diagnosis was missed in 21
percent of demented or delirious patients on a general
medical ward, while 20 percent of nondemented patients
were misjudged as demented [10]. Nonetheless, the clinical
9

diagnosis of dementia is reasonably accurate for those with
experience in the evaluation of this disorder (show table 1)
[11].
Table I
Sensitivity and specificity of diagnostic tests for dementia
Diagnostic test Sensitivity, percent
Specificity, percent
Mini-Mental State Exam*
87 82
Short Portable Mental Status Questionnaire* Any dementia 82 92 Mild dementia 55 96 NINCDS criteria 92 65DSM-IV criteria 76 80Clinical judgment 85 82
Diagnosis of dementia.Diagnosis of Alzheimer disease.
*Most patients with dementia do not present with a
complaint of memory loss; it is often a spouse or other
informant who brings the problem to the physician's
attention. Self-reported memory loss does not appear to
10
correlate with the subsequent development of dementia,
while informant-reported memory loss is a much better
predictor of the current presence and future development of
dementia [12,13]. Nevertheless, family members are often
delayed in recognizing the signs of dementia, many of which
are inaccurately ascribed to "aging."
The normal cognitive decline associated with aging consists
primarily of mild changes in memory and the rate of
information processing, which are not progressive and do
not affect daily function. In a study of 161 community-
dwelling, cognitively normal individuals ages 62 to 100
years, learning or acquisition performance declined
uniformly with increasing age [14]. In contrast, delayed
recall or forgetting remained relatively stable. Similarly, a
second report found that aging was associated with a decline
in the acquisition and early retrieval of new information but
not in memory retention [15].
Patients with dementia may have difficulty with one
or more of the following [16]:
Learning and retaining new information (eg, trouble
remembering events)
Handling complex tasks (eg, balancing a checkbook)
Reasoning (eg, unable to cope with unexpected events)
Spatial ability and orientation (eg, getting lost in
familiar places)
Language (eg, word finding)
Behavior
11
Patients and informants are often uncertain about the onset
of symptoms since the appearance of dementia is insidious.
The physician can usually date the onset of dementia by
identifying when the patient stopped driving or managing
finances. Useful questions for the patient and informant are,
"When did you first notice the memory loss?" and "How has
the memory loss progressed since then?"
The diagnosis of dementia must be distinguished
from delirium and depression (show table 2) [17].
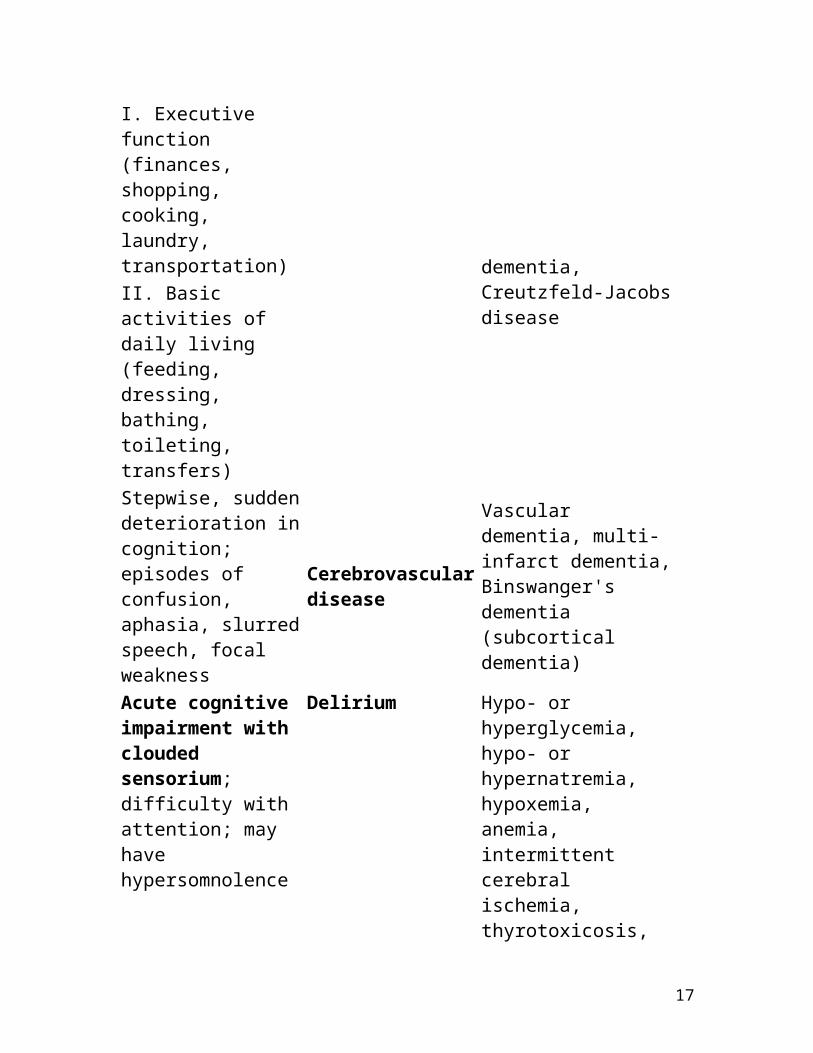
Table 2
Differential diagnosis of memory loss Symptom Usual cause Examples Gradual onset of short-term memory loss and functional impairment in more than one domain:
Dementia
Alzheimer disease, Parkinson dementia, Lewy body dementia, Pick's disease, alcohol-related dementia, Creutzfeld-Jacobs disease
I. Executive function (finances, shopping, cooking, laundry, transportation) II. Basic activities of daily living (feeding, dressing, bathing, toileting, transfers) Stepwise, sudden deterioration in cognition; episodes of confusion,
Cerebrovascular disease
Vascular dementia, multi-infarct dementia, Binswanger's
12
aphasia, slurred speech, focal weakness
dementia (subcortical dementia)
Acute cognitive impairment with clouded sensorium; difficulty with attention; may have hypersomnolence
Delirium
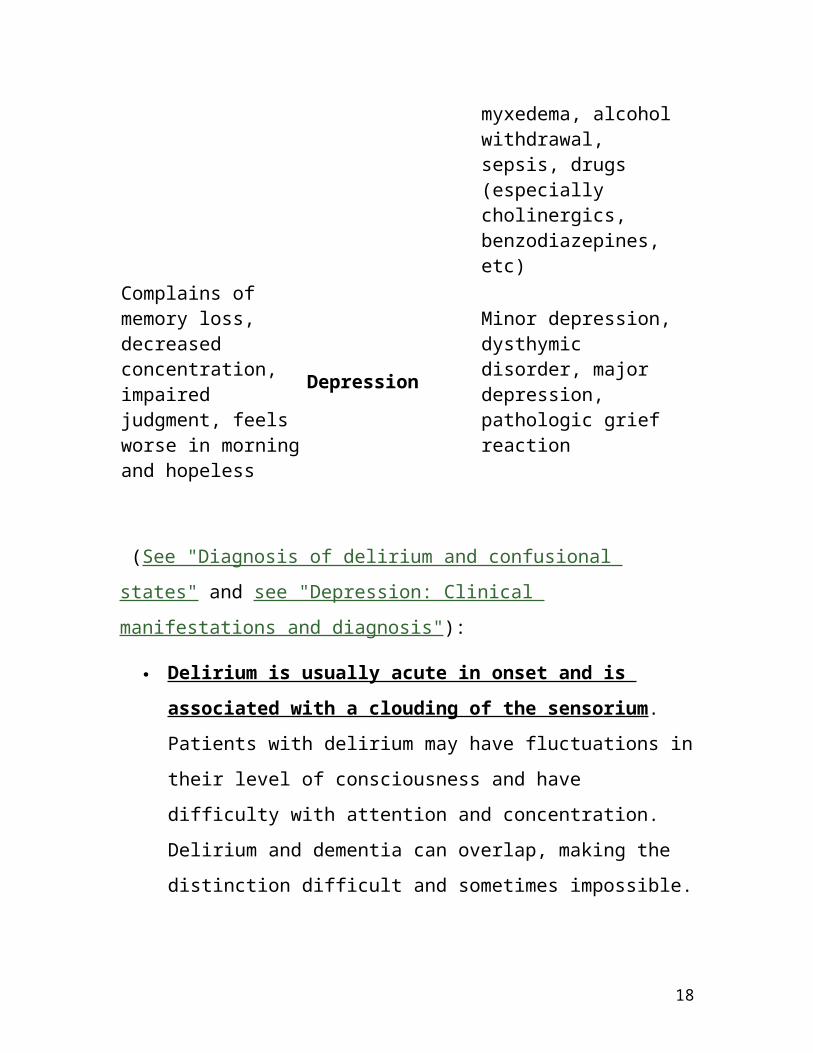
Hypo- or hyperglycemia, hypo- or hypernatremia, hypoxemia, anemia, intermittent cerebral ischemia, thyrotoxicosis, myxedema, alcohol withdrawal, sepsis, drugs (especially cholinergics, benzodiazepines, etc)
Complains of memory loss, decreased concentration, impaired judgment, feels worse in morning and hopeless
Depression
Minor depression, dysthymic disorder, major depression, pathologic grief reaction
(See "Diagnosis of delirium and confusional states" and see
"Depression: Clinical manifestations and diagnosis"):
Delirium is usually acute in onset and is
associated with a clouding of the sensorium.
Patients with delirium may have fluctuations in their
level of consciousness and have difficulty with attention
and concentration. Delirium and dementia can overlap,
13

making the distinction difficult and sometimes
impossible.
Patients with depression are more likely to
complain about memory loss than those with
dementia; the latter are frequently brought to
physicians by their families, while depressed
patients often present by themselves. Patients
with depression may have signs of psychomotor
slowing and produce a poor effort on testing, while
those with dementia often try hard but respond with
incorrect answers. Depression and dementia may occur
in the same patient.
The US Preventive Services Task Force has concluded that
there is insufficient evidence to recommend for or against
routine screening for dementia in older adults [18,19]. The
USPSTF clinical practice guideline for screening for dementia,
as well as other USPSTF guidelines, can be accessed through
the website for the Agency for Healthcare Research and
Quality at www.ahrq.gov/clinic/uspstfix.htm.
Mild cognitive impairment — Mild cognitive impairment
(MCI) is generally defined by the presence of memory
difficulty and objective memory impairment but preserved
ability to function in daily life. Patients with MCI appear to be
14

at increased risk of dementia. This topic is discussed
separately. (See "Mild cognitive impairment").
Dementia syndromes — The major dementia
syndromes include [20-22]: (see "Dementia
syndromes")
Alzheimer disease (AD)
Dementia with Lewy bodies (DLB)
Frontotemporal dementia (FTD)
Vascular (multi-infarct) dementia (VaD)
Parkinson disease with dementia (PDD)
Less common disorders such as progressive supranuclear
palsy (PSP) can also be associated with dementia. Non-
neurodegenerative dementias may be reversible, if the
underlying cause can be identified and adequately treated
[23].
Most elderly patients with chronic dementia have AD
(approximately 60 to 80 percent). The vascular
dementias account for 10 to 20 percent, and PD for 5
percent. The prevalence of VaD is relatively high in blacks,
hypertensive persons, and patients with diabetes; some of
the reversible dementias (eg, metabolic dementias) tend to
occur in younger individuals. DLB may be as prevalent as
VaD in older cohorts of patients [24]. FTD is much less
common than AD, VaD, or DLB.
15

Alcohol-related dementia, medication side effects (eg,
antihistamine use), depression, and other central nervous
system illnesses are responsible for the remainder of the
chronic dementias.
Dementia frequently has more than one cause, particularly
as the condition progresses. In addition, medical illnesses
exacerbating poor cognition are common in patients with
dementia. The bedside evaluation combined with historical
information from a reliable informant provides most of the
information needed to ascertain the cause of dementia [17].
However, even with the addition of information from imaging
studies, clinical criteria for VaD have relatively poor
sensitivity [25].
DIAGNOSTIC APPROACH — The initial appointment in
a patient with suspected dementia should focus upon
the history. Preferably, family members are available to
give an adequate history of cognitive and behavioral
changes [21]. A drug history is particularly important; use of
drugs that impair cognition (eg, analgesics, anticholinergics,
psychotropic medications, and sedative-hypnotics) should be
sought.
A full dementia evaluation can probably not be
completed in a routine 30-minute visit; adequate time
should be arranged as a follow-up appointment. The initial
step at the follow-up visit is an assessment of cognitive
16
function. This should be followed by a complete physical
examination, including neurologic examination. The
subsequent work-up may include laboratory and imaging
studies (show algorithm 1) [26,27].
The DSM-IV criteria for the diagnosis of dementia are
shown in Table three (show table 3).
A full dementia evaluation can probably not be completed in
a routine 30-minute visit; adequate time should be arranged
as a follow-up appointment. The initial step at the follow-up
visit is an assessment of cognitive function. This should be
followed by a complete physical examination, including
neurologic examination. The subsequent work-up may
include laboratory and imaging studies (show algorithm 1)
[26,27]. The DSM-IV criteria for the diagnosis of dementia
are shown in Table three (show table 3).
Algorithm 1 :
Diagnosis of dementia
17
Adapted from Corey-Bloom, J, Thal, LJ, Galasko, D, et al, Neurology 1995; 45:211.
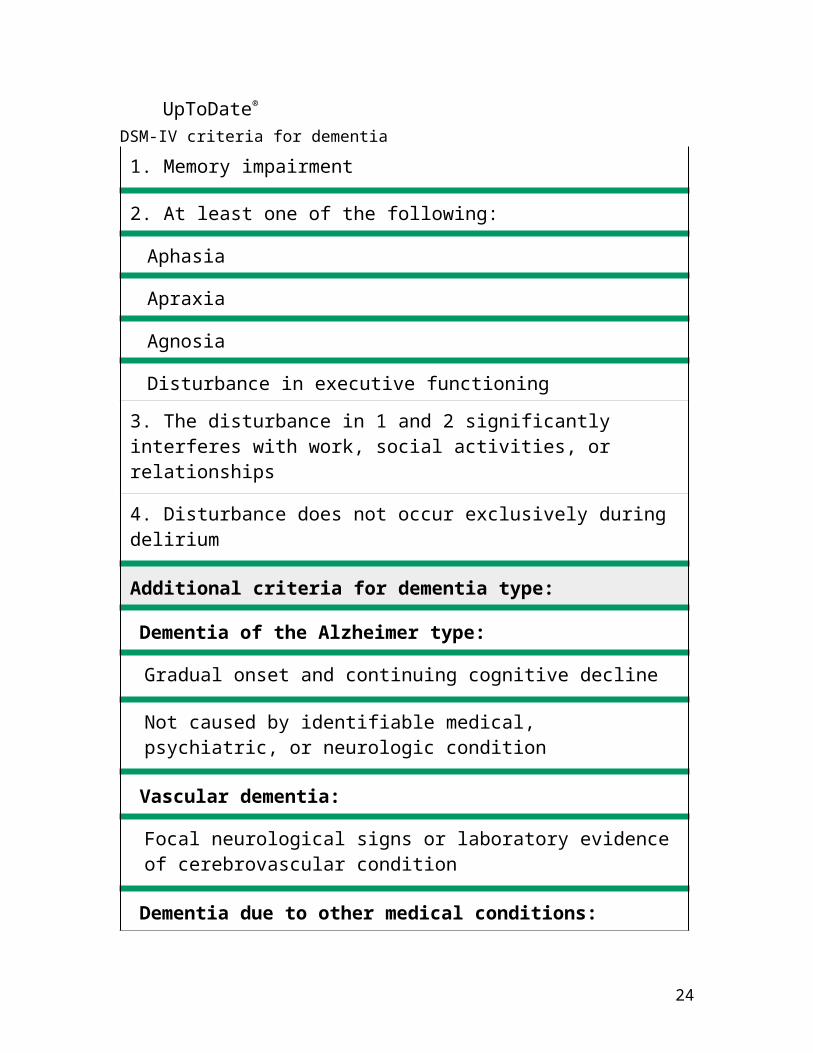
Table 3:
©2009 UpToDate®
DSM-IV criteria for dementia
1. Memory impairment
2. At least one of the following:
Aphasia
Apraxia
Agnosia
Disturbance in executive functioning
3. The disturbance in 1 and 2 significantly interferes with work, social activities, or relationships
18
4. Disturbance does not occur exclusively during delirium
Additional criteria for dementia type:
Dementia of the Alzheimer type:
Gradual onset and continuing cognitive decline
Not caused by identifiable medical, psychiatric, or neurologic condition
Vascular dementia:
Focal neurological signs or laboratory evidence of cerebrovascular condition
Dementia due to other medical conditions:
Evidence from history, physical exam, or laboratory findings of a specific medical condition causing cognitive deficits (HIV disease, head trauma, Parkinson disease, Huntington's chorea, Pick's disease, Creutzfeld-Jacob)
Adapted from American Psychiatric Association Diagnostic and Statistical Manual, 4th ed, APA Press, Washington DC, 1994.
Cognitive testing — Agreement between the history
and the mental status examination is strongly
suggestive of the diagnosis of dementia. When the
history suggests cognitive impairment but the mental status
examination is normal, possible explanations include mild
dementia, high intelligence or education, depression, or
rarely, misrepresentation on the part of the informants [28].
Conversely, when the mental status examination suggests
19

cognitive impairment but the family and patient deny any
problems, possible explanations include an acute confusional
state, very low intelligence or education, or inadequate
recognition by the family [28]. Neuropsychological
assessment (psychometric testing) may be useful in difficult
situations; re-evaluation at a later time is often helpful.
Mini-Mental State Examination — The Mini-Mental
State Exam (MMSE) is the most widely used cognitive
test for dementia in US clinical practice [29,30]. The
examination takes approximately seven minutes to
complete. It tests a broad range of cognitive
functions including orientation, recall, attention,
calculation, language manipulation, and
constructional praxis.
The MMSE includes the following tasks [29]:
What is the date: (year)(season)(date)(day)(month) - 5
points
Where are we: (state)(county)(town)(hospital)(floor) - 5
points
Name three objects: Ask the patient all three after you
have said them. Give one point for each correct answer.
Then repeat them until he/she learns all three. Count
trials and record. The first repetition determines the
score, but if the patient cannot learn the words after six
trials then recall cannot be meaningfully tested.
Maximum score - 3 points.
20
Serial 7s, beginning with 100 and counting backward:
one point for each correct; stop after five answers.
Alternatively, spell WORLD backwards: one point for
each letter in correct order. Maximum score - 5 points.
Ask for the three objects repeated above: one point for
each correct. Maximum score - 3 points.
Show and ask patient to name a pencil and wrist watch
- 2 points.
Repeat the following, "No ifs, ands, or buts." Allow only
one trial - 1 point.
Follow a three stage command, "Take a paper in your
right hand, fold it in half, and put it on the floor." Score
one point for each task executed. Maximum score - 3
points.
On a blank piece of paper write "close your eyes;" ask
the patient to read and do what it says - 1 point.
Give the patient a blank piece of paper and ask him/her
to write a sentence. The sentence must contain a noun
and verb and be sensible - 1 point.
Ask the patient to copy a design (eg, intersecting
pentagons). All 10 angles must be present and two
must intersect - 1 point.
A total maximal score on the MMSE is 30 points. A score of
less than 24 points is suggestive of dementia or delirium.
21

Using a cutoff of 24 points, the MMSE had a sensitivity of 87
percent and a specificity of 82 percent in a large population
based sample (show table 1) [31]. However, the test is not
sensitive for mild dementia, and scores may be influenced
by age and education, as well as language, motor, and visual
impairments [32]. In one study, for example, the median
MMSE score was 29 for individuals with at least nine years of
schooling, 26 for those with five to eight years of schooling,
and 22 for those with four years of schooling or less [31].
The use of higher cutoff scores on the MMSE improves
sensitivity but lowers specificity. For research purposes,
some investigators use a cutoff score of 26 or 27 in
symptomatic populations in order to miss few true cases,
while lower cutoffs would be necessary in populations where
the expected prevalence is low [33]. Age-specific norms also
have been established [31]; some groups have developed
tools that incorporate age, gender, and education level
(show figure 1) [34,35].
The MMSE also has utility in assessing competency in
decision making. Studies suggest that high scores, ≥23, and
low scores, <19, can be highly predictive in discriminating
competency from incompetency. Intermediate scores
warrant more detailed competency evaluation [36,37].
The MMSE has limitations for assessing progressive cognitive
decline in individual patients over time. Changes of two
points or less are of uncertain clinical significance as they
22

may represent measurement error, regression to the mean,
or a practice effect [38].
Clinical Dementia Rating — The Clinical Dementia Rating
(CDR) was designed to assess severity of Alzheimers disease
in longitudinal studies and clinical trials [39]. This
assessment is also increasingly used in clinical decision
making as well, such as driving. (See "Safety and societal
issues related to dementia", section on Driving).
In a semi-structured interview with the patient and
caregiver, impairments in six domains (memory, orientation,
judgment and problem solving, community affairs, home and
hobbies, personal care) are assessed as none, questionable,
mild, moderate, and severe (0,0.5,1,2, and 3) [39]. A
caregiver who knows the patient well is necessary for an
accurate and valid assessment by the CDR. The global CDR
score is assigned based on performance in each domain,
placing particular weight on the memory score. A detailed
description of the CDR is available [39], and an algorithm for
scoring is available at www.biostat.wustl.edu/adrc/.
While time-consuming to administer, the test has established
validity and inter-rater reliability [40,41], and may be useful
in following disease progression over time.
Other brief cognitive assessments — Ideal tests for
mental status screening should be brief and have good
performance in populations with different cultural, linguistic,
and educational backgrounds.
23
Mini-Cog. The "Mini-Cog" test consists of a clock
drawing task (CDT) and an uncued recall of three
unrelated words [42]. The CDT is considered
normal if all numbers are present in the correct
sequence and the hands display the correct time
in a readable way. Scoring is based on a simple
decision tree with the following three rules:
Subjects recalling none of the words are classified as
demented
Subjects recalling all three words are classified as non-
demented
Subjects with intermediate (one to two) word recall are
classified based on the CDT (abnormal = demented;
normal = non-demented)
The advantages of the Mini-Cog include : high
sensitivity for predicting dementia status, short testing time
relative to the MMSE, ease of administration, and diagnostic
value not limited by the subject's education or language
[42].
Informant interview — A brief, eight-item
questionnaire for informants appears to be sensitive for
detecting dementia and cognitive impairment [44].
Informants are asked whether the patient has exhibited
any increase in the following deficits or behaviors:
- Problems with judgment
- Reduced interest in hobbies/activities
24

- Repeats questions, stories, or statements
- Trouble learning how to use a tool or appliance
- Forgetting the correct month or year
- Difficulty handling financial affairs (bill-paying, taxes)
- Difficulty remembering appointments
- Consistent problems with thinking and/or memory
Short portable mental status questionnaire. The
short portable mental status questionnaire is
another popular test of cognitive function [45]. It
can be performed in approximately five minutes.
This test contains items that test orientation, attention,
immediate recall, arithmetic, abstraction, construction,
information, and delayed (approximately three
minutes) recall. It is reasonably sensitive and specific
for the diagnosis of moderate to severe dementia, but
similar to the MMSE, it is relatively insensitive in cases
of mild dementia (show table 1).
Clock drawing. Asking the patient to draw a clock
with a specific time is a quick examination that
appears to correlate well with the MMSE score,
although it has not undergone as rigorous an evaluation
as the MMSE [46]. It is not a sensitive test for
identifying very mild dementia [47,48].
Neuropsychologic testing — Neuropsychologic testing
usually involves extensive evaluation of multiple
cognitive domains (eg, attention, orientation, executive
25
function, verbal memory, spatial memory, language,
calculations, mental flexibility and conceptualization).
In a 2001 parctice parameter, the AAN reviewed a number of
studies of neuropsychological testing for dementia; some
were well designed observational controlled studies [49-53],
and others were case series [54-56]. Most studies
demonstrated a relatively high sensitivity (range 80 to 98
percent) and specificity (from 44 to 98 percent) for detection
of dementia.
The AAN concluded that neuropsychologic batteries are
useful in identifying patients with dementia, particularly
when administered to those at higher risk by virtue of
memory impairment [49]. Neuropsychologic instruments
that emphasize memory function were considered most
useful. Five subtests (Animal naming, Modified Boston
Naming Test, MMSE, Constructional Praxis, and Word List
Memory) were identified to be a valid, reliable measure of
cognition in normal aging and AD. An aggregate total score
accurately differentiated normals from those with MCI and
AD [57]. However, it is important to recognize that scores
can also be influenced by education and age and apply only
to individuals whose primary language is English [58].
While different causes of dementia can preferentially affect
different cognitive domains, neuropsychologic testing has
limited utility for differentiating among causes of dementia
as there are substantial overlaps in test performance [ 59 ].
26
Follow-up testing may provide more helpful information than
a single study, particularly when results are equivocal, in
that evidence of decline can predict future decline [60]. (See
"Mild cognitive impairment", section on Neuropsychological
testing).
Physical examination — A thorough general physical
examination to rule out an atypical presentation of a
medical illness should be combined with a neurologic
examination. The latter should focus upon focal neurologic
deficits that may be consistent with prior strokes, signs of
Parkinson disease (PD) (eg, cogwheel rigidity and tremors),
gait, and eye movements. In comparison, patients with
Alzheimer disease (AD) generally have no motor deficits at
presentation. This examination, along with the medical and
neurologic history, will allow tailoring of laboratory tests.
Laboratory testing — The American Academy of
Neurology (AAN) recommends screening for B12
deficiency and hypothyroidism in patients with
dementia [8]. (See "Neurologic manifestations of
hypothyroidism" section on Screening for hypothyroidism in
cognitive impairment). There are no clear data to support or
refute ordering "routine" laboratory studies such as a
complete blood count, electrolytes, glucose, and renal and
liver function tests. Screening for neurosyphilis is not
recommended unless there is a high clinical suspicion.
The cost-effectiveness of obtaining multiple laboratory
studies in all patients is questioned because the yield is low
27

[63]. The prevalence of reversible dementia has fallen since
1972. In a 1994 study, this was less than one percent, and in
a 2006 community-based series, none of the 560 patients
with dementia screened had a treatable metabolic cause
[63,64]. Some tests can be tailored to patients with a
compatible history (eg, red blood cell folate in a patient with
ethanol dependence, or ionized serum calcium in a patient
with multiple myeloma, prostate cancer, or breast cancer).
Patients with an atypical syndrome, eg, rapidly progressive
dementia, may benefit from a more extensive evaluation
(show table 4) [65].
The value of genetic testing for AD in patients with
dementia is controversial. The apolipoprotein E
epsilon 4 allele has been considered for use as a
diagnostic test. As previously mentioned, however, many
patients who are homozygotes for this allele will not develop
AD [66]; thus, application of this test to large populations
would lead to the overdiagnosis of AD, a practice with
obvious potentially damaging consequences. For these
reasons, genetic testing for the apolipoprotein E epsilon 4
allele is not currently recommended [67], nor is genetic
testing for other potential causes of dementia [8].
While some studies suggest that increased levels of tau
protein and decreased levels of beta-amyloid protein ending
at amino acid 42 in cerebrospinal fluid or plasma may have
predictive value for AD in nondemented patients and in
patients with MCI, and may also distinguish AD from other
28
forms of dementia [68-77], a role for these measurements in
clinical practice has not been established [78-81].
Neuroimaging — The use of neuroimaging in patients with
dementia is controversial. A number of guidelines on the
clinical evaluation of dementia have been published, many
of which do not recommend imaging studies routinely, but
include clinical prediction rules to identify patients who
might have reversible causes of dementia that can be
diagnosed with imaging studies (eg, subdural hematoma,
normal pressure hydrocephalus, treatable cancer) [8,64,82-
88]. The prediction rules vary, including factors such as
young age (<60), focal signs, short duration of symptoms
(less than two years), among others. However, the
sensitivity and specificity of these prediction rules is low
[89]. The AAN recommends structural neuroimaging with
either a noncontrast head CT or MRI in the routine initial
evaluation of all patients with dementia [8].
MRI findings in AD include both generalized and focal
atrophy as well as white matter lesions [90]. In general,
these findings are nonspecific. course of the disease,
thereby guiding treatment decisions [91,96,97].
Demented patients with atherosclerotic risk factors may
harbor silent cerebrovascular disease. Neuroimaging in
these cases may lead to more aggressive management of
the patient's hypertension, diabetes, lipid disorders, and
smoking cessation, and may prompt one to prescribe aspirin.
29
A head CT scan is important for patients with acute onset of
cognitive impairment and rapid neurologic deterioration.
Neuroimaging is also indicated when there are historical
features or findings on physical examination suggestive of a
subdural hematoma, thrombotic stroke, or cerebral
hemorrhage, as well as in individuals with rapidly
progressive dementia [65].
AD and other neurodegenerative diseases can cause serious
alterations in brain metabolism, providing the rationale for
the use of positron emission tomography (PET) to assist in
the diagnosis of dementia. In one of the largest studies of
PET for this purpose to date, PET studies in 146 patients
presenting with cognitive symptoms of dementia were
sensitive indicators of the presence of AD and of
neurodegenerative disease in general [ 98 ]. A negative PET
scan indicated that pathologic progression of cognitive
impairment was unlikely to occur over the next three years.
The clinical application of PET scanning remains to be
determined [ 99 ].
Brain biopsy — Brain biopsy has a very limited role in the
diagnosis of dementia; the diagnostic yield is low, and the
test is invasive with a significant risk of serious
complications. Typically, it is reserved for younger patients
and those with atypical clinical presentations in which a
treatable cause of dementia (eg, inflammatory disorders
30
such as vasculitis or multiple sclerosis) is considered
plausible. in only 11 percent [106].
SUMMARY AND
RECOMMENDATIONS — Recommendations for the
evaluation of cognitive impairment and dementia are
derived from our clinical experience as well as from the
American Academy of Neurology (AAN) practice guidelines
[8,49].
The initial step in the evaluation of a patient with
suspected dementia should focus upon the history.
Family members or other informants who know the
patient well are invaluable resources for providing an
adequate history of cognitive and behavioral changes.
Adequate time should be arranged for a full assessment
of cognitive function, followed by a complete physical
examination, including neurologic examination.
The Mini-Mental State Exam is a useful screening test
for dementia; a score of less than 24 points is
suggestive of dementia or delirium.
Neuropsychologic testing batteries are useful in
identifying patients with dementia, particularly when
administered to those who may be at increased risk of
cognitive impairment.
31

Screening for B12 deficiency and hypothyroidism is
recommended for patients being evaluated for
dementia.
Screening for depression in patients with dementia is
recommended because depression is a common
treatable comorbidity that may also masquerade as
dementia.
Genetic testing for the apolipoprotein E epsilon 4 allele
is not currently recommended, nor is genetic testing for
other potential causes of dementia.
Structural neuroimaging with either a noncontrast head
CT or MRI is recommended in the routine initial
evaluation of all patients with dementia.
Use of UpToDate is subject to the Subscription and
License Agreement.
References:
1) www.uptodate.com
2) ASSESSMENT of Older Adults WITH DIMINISHED CAPACITY: (A Handbook for Lawyers) http://www.abanet.org/aging/publications/publicationslistorder.shtml#capacity
3) Science, common sense, and the determination of mental capacity. By Frolik, Lawrence Psychology, Public Policy, and Law. Vol 5(1), Mar 1999, 41-58.
32

(I can( e-mail) send this to anyone wanting the entire 18 page article)
4) American Psychiatric Association Diagnostic and Statistical Manual, 4th ed, APA Press, Washington DC, 1994 5)Jacobson: Psychiatric Secrets, 2nd ed. Second Edition
James L. Jacobson, MD Associate Professor, Department of Psychiatry, University of Vermont
Medical School, Burlington, Vermont Alan M. Jacobson, MD Professor, Department of Psychiatry, Harvard Medical School Senior Vice President, Strategic Initiatives, Joslin Diabetes Center, Boston, Massachusetts
6) Early Diagnosis of Dementia, American Family Physician.February 15, 2001 http://www.aafp.org/afp/AFPprinter/20010215/703.html?print=yes
7) Competency Evaluations Start With Five Senses: Ken Hausman, Psychiatric News, May 16, 2003
http://pn.psychiatryonline.org/cgi/content/full/38/10/34
8) Assessing Mental Capacity in Older Adults, APA online
Volume 35, No. 9 October 2004
http://www.apa.org/monitor/oct04/capacity.html
9) American Family Physician: Dementia What are the Common Signs? March 1,2003
10) Office of State Guardian Frequently Asked Questions, Illinois Guardianship and Advocacy Commision,
33

http://gac.state.il.us/osg/osgcont.html
11)Initial Evaluation of the Patient with Supected Dementia,
American Family Physician, May 1, 2005
http://www.aafp.org/afp/20050501/1745.html
12) Geldmacher DS, Whitehouse PJ. Evaluation of dementia. N Engl J Med 1996;335:330-336.
34







