54
Complications of Neonatal Surgical Cases: NEC and Birth Defects Dr. Phillip Pan, MD Neonatologist Bellevue Woman’s Center, a service of Ellis Medicine Albany Medical Center
| Date post: | 15-Dec-2015 |
| Category: |
Documents |
| Upload: | linda-waitt |
| View: | 213 times |
| Download: | 0 times |
Complications of Neonatal Surgical Cases:
NEC and Birth Defects
Dr. Phillip Pan, MDNeonatologist
Bellevue Woman’s Center, a service of Ellis MedicineAlbany Medical Center

Complications of Neonatal Surgical Cases: Objectives
• Necrotizing Enterocolitis
• Birth Defects• Tracheoesophageal Fistula• Myelomeningocele• Abdominal wall defects (gastroschisis,
omphalocele)• Hydrocephalus (congenital, post-hemorrhagic)
• Gastrostomy tube
Necrotizing Enterocolitis
• Characterized by injury to the intestines with variable degrees of intestinal ischemia, usually including the terminal ileum
• Gas develops within the muscular and submucosal layers and may be seen as pneumatosis intestinalis
• When full-thickness necrosis occurs, perforation and peritonitis develop

Characteristics
• 1-5% of all NICU admissions
• usually onset between 3rd - 10th day of life
• no association between sex, race, season or socioeconomic status
• predominantly affects premature infants, but about 10% of those affected are term infants
• mortality is between 30-40%
Theories
• Variable theories – infection, inflammation, ischemia/reperfusion injury
• Probably multifactorial and requires interaction of immaturity, previous gastrointestinal ischemia, enteral feeding and bacterial invasion
• Contradicting the theory is NEC occurs in infants• with no identifiable risk factors, • who were never fed enterally, and• among otherwise healthy full-term infants
Bell Clinical Staging
• Stage I – Suspected NEC• Temp instability, apnea, gastric residuals,
abdominal distension. No radiographic abnormalities
• NPO, antibiotics for 2-3 days pending culture
• Stage II – Definite NEC• Also includes absent bowel sounds,
abdominal tenderness• Ileus, pneumatosis (see photo)• NPO, antibiotics x14 days

Copyright ©2001 American Academy of Pediatrics
Dimmitt, R. A. et al. Neoreviews 2001;2:110-e117
A plain anteroposterior radiograph demonstrating pneumatosis

Bell Clinical StagingStage III – Advanced NEC
• hemodynamic instability, DIC, neutropenia, metabolic acidosis, respiratory compromise
• generalized peritonitis, marked tenderness and distension of abdomen
• antibiotics, inotropes, assisted ventilation
• Includes bowel perforation, pneuomoperitoneum

Copyright ©2001 American Academy of Pediatrics
Dimmitt, R. A. et al. Neoreviews 2001;2:110-e117
An anteroposterior radiograph showing extensive pneumatosis and free air

Surgical Management
• Indications include pneumoperitoneum, persistent metabolic acidosis, rapidly worsening pulmonary status and unremitting neutropenia or thrombocytopenia
• Emergently a peritoneal drain may be placed
• Staged exploratory laporatomies to identify ischemic, perforated, and necrotic bowel

Complications
• stricture formation occurs in 25-35% of survivors• “silent” strictures may be identified by barium
enema• late-onset intestinal obstruction following
medical and/or surgical management includes adhesions, scarring and short bowel syndrome
• neurodevelopmental delays occur in 50% of survivors
• most serious intestinal complication is short bowel syndrome (25%)
Short Bowel Syndrome
• NEC is the leading cause of SBS• other causes include congenital malformations
• More than 50% of small bowel must be removed before substantial malabsorption occurs• normal lengths - 150 cm at 28 weeks vs 250 cm at
term• an important determinant of future function is
presence of ileocecal valve• 20 cm is minimal length sufficient to allow
dependence on TPN
• following ileocolic anastomasis, painless rectal bleeding or melena from anastomotic ulcers can occur years after NEC surgery

Prognosis
• prognosis of patients with short bowel syndrome is guarded
• infants are followed by the primary physician, pediatric gastroenterologist and surgeon
• Some of these complications may be present at discharge from the NICU, and some require continued surveillance
• Poor growth is a frequent outcome
• Dumping syndrome is observed in infants with ostomies or severe diarrhea during GI infections
• Dumping syndrome may cause rapid dehydration and electrolyte imbalance
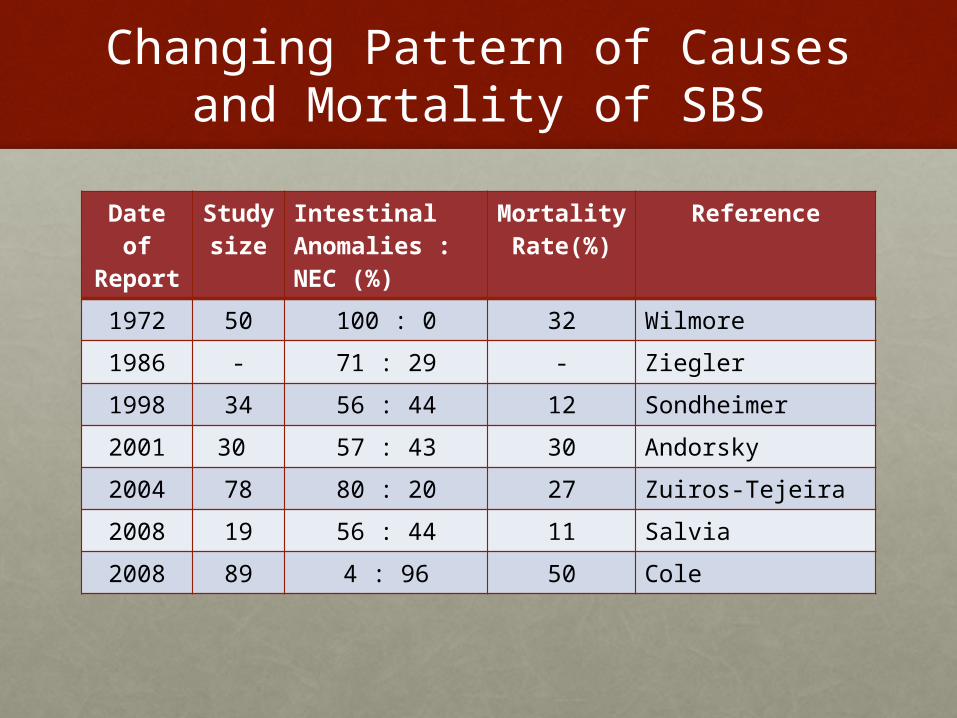
Changing Pattern of Causes and Mortality of SBS
Date of Report
Study size
Intestinal Anomalies : NEC (%)
Mortality Rate(%)
Reference
1972 50 100 : 0 32 Wilmore
1986 - 71 : 29 - Ziegler
1998 34 56 : 44 12 Sondheimer
2001 30 57 : 43 30 Andorsky
2004 78 80 : 20 27 Zuiros-Tejeira
2008 19 56 : 44 11 Salvia
2008 89 4 : 96 50 Cole
Bowel and Liver transplantation
• Boston Children’s Hospital
• Children Hospital of Philadelphia
• New York city
• 105.09 liver transplantation - for 1 year following the date of transplantation

TPN-related cholestasis
• Characterized by direct hyperbilirubinemia, hepatomegaly and increased serum transaminases
• Risk factor includes prolonged enteral fasting
• Treatment includes enteral nutrition, increasing bile acid production (actigall, phenobarbitol) and stopping TPN

Gastrostomy tube
• Anatomic, neurologic and developmental disorders
• Memorable cases• Congenital myotonic dystrophy• Pierre Robin sequence• Tracheo-esophageal fistula• Severe bronchopulmonary dysplasia
• 105.10 - Need for supplemental daily enteral feeding via a g-tube for children < 3 years

Gastrostomy tube
Mickey button
G-tube for GER
• some children who have antireflux surgery also benefit from a G-tube
• G-tube should be considered in children with neurologic impairment, poor gastric motility, or poor nutritional status
• In addition to facilitating postoperative feeding, it allows drainage or venting of the stomach

Birth Defects:outline
• Tracheoesophageal Fistula
• Myelomeningoceles
• Abdominal wall defects• Gastroschisis• Omphalocele
• Hydrocephalus• Congenital• Post-hemorrhagic

Birth Defects
• An abnormality of structure, function or metabolism that results in physical or mental disabilities or death
• 3% of all children (120,000 babies) are born with a serious structural defect
• The leading cause of death in the 1st year of life

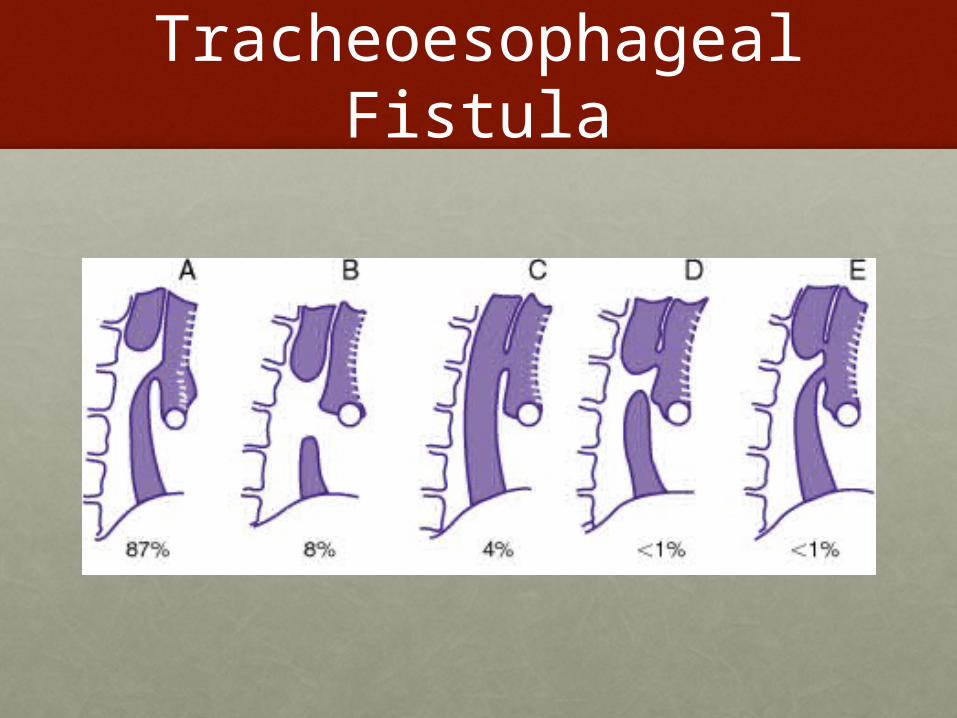
Tracheoesophageal Fistula


Surgical Repair of TEF
• Surgical repair depends on presence of esophageal atresia, gap between proximal and distal esophagus ends, degree of respiratory compromise
• Initial timing must consider aspiration of gastric contents into the lower lungs with urgent decompression and ligation of the distal TEF
• May involve gastric pull-up, colonic graft, gastrostomy tube
Complications
• Early – anastomotic leak, recurrent TEF and anastomotic strictures
• Late – GER, esophageal dysmotility and tracheomalacia
Outcome and Prognosis
• Statistics are constantly changing and improving
• Mortality ranges from 7-63% and 0-11% depending on classification technique and reporting statistics
• Fetuses with prenatal diagnoses of esophageal atresia have a worse prognosis with a mortality rate as high as 75% vs 21 % without esophageal atresia

Omphalocele vs gastroschisis
Omphalocele Gastroschisis
Pathogenesis Abnormality during body folding
Compromise of vascular supply
Etiology Sporadic. Increased assoc with genetic syndrome
Sporadic. Increased assoc with young mothers
Birth weight (< 5th %ile)
20% 77%
Mortality at 1 yr 40% 7.7%
PE AGA infant, enclosed sac, may include liver and other organs
SGA infant, exposed intestines.

Management ofOpen Ventral Wall Defects
• Multidisciplinary teamwork
• Protect exposed bowel/mucosa• Prevent heat loss• Prevent insensible water loss• Prevent vascular compromise
• Nasogastric decompression
• Broad-spectrum antibiotic coverage
• Total parenteral nutrition
• Surgical correction

Gastroschisis

Compromised bowel

Omphalocele

Large with wharton jelly
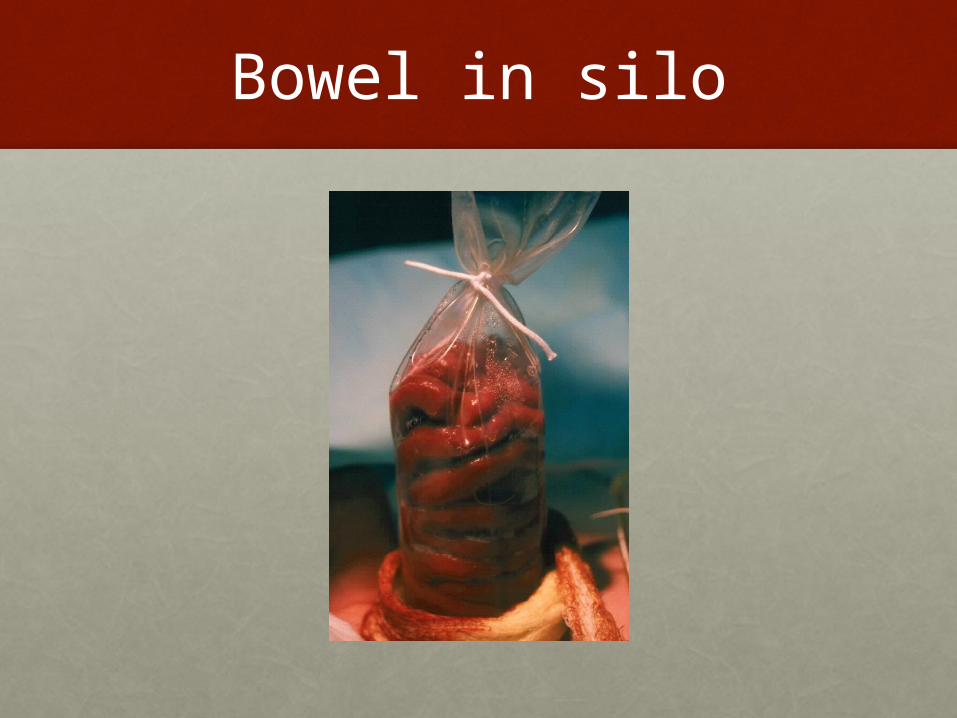
Bowel in silo


Neural Tube defects
• Neural tub defects affect about 3000 pregnancies each year in the US
• Risk may be reduced by taking at least 0.4 mg of vitamin B folic acid before and during early pregnancy
• The neural tube folds inward to form a tube by the 28th day after conception
• Includes spina bifida, anencephaly, encephalocele

Spina Bifida
• The most common NTD, affect 1500 babies each year in the US
• 3 classic forms• Occulta – mildest form with usually no
symptoms• Meningocele – rarest from with just cyst or fluid-
filled sac without spinal nerves• Myelomeningocele

Myelomeningocele
• both the membranes and nerve roots of the spinal cord are enclosed in cyst or fully exposed
• In spite of surgical repair, affect babies have some degree of leg paralysis, encoparesis and eneuresis

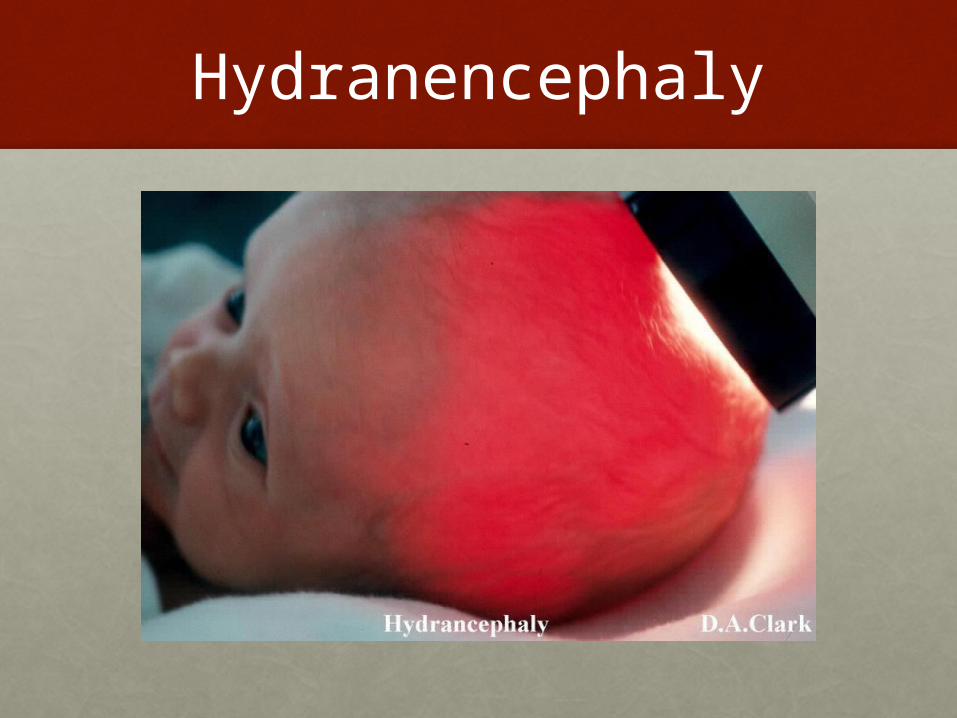
Hydranencephaly

Classic Dandy-Walker variant
Melissa A. Parisia and William B. Dobyns. Human malformations of the midbrain and hindbrain: review and proposed classification scheme. Molecular Genetics and Metabolism. 80 (2003): 36–53.

Dandy-Walker Variants
Incidence of IVH
• 34 - 49% LBW infants in 1970’s
• 20 - 29% LBW infants in 1980’s
• Incidence correlates with degree of prematurity
• Survival rates of smallest infants continue to increase

Risk of IVH
• Risk is inversely proportional to gestational age
• 35% of infants with birth weights of 500-600 g have grade 3 or 4 IVH
• If posthemorrhagic ventricular dilatation occurs after intraventricular hemorrhage does, it is usually apparent on cranial ultrasonography within 2-3 weeks
• Infants who have had intracranial hemorrhage must always be monitored in neurodevelopmental follow-up clinics
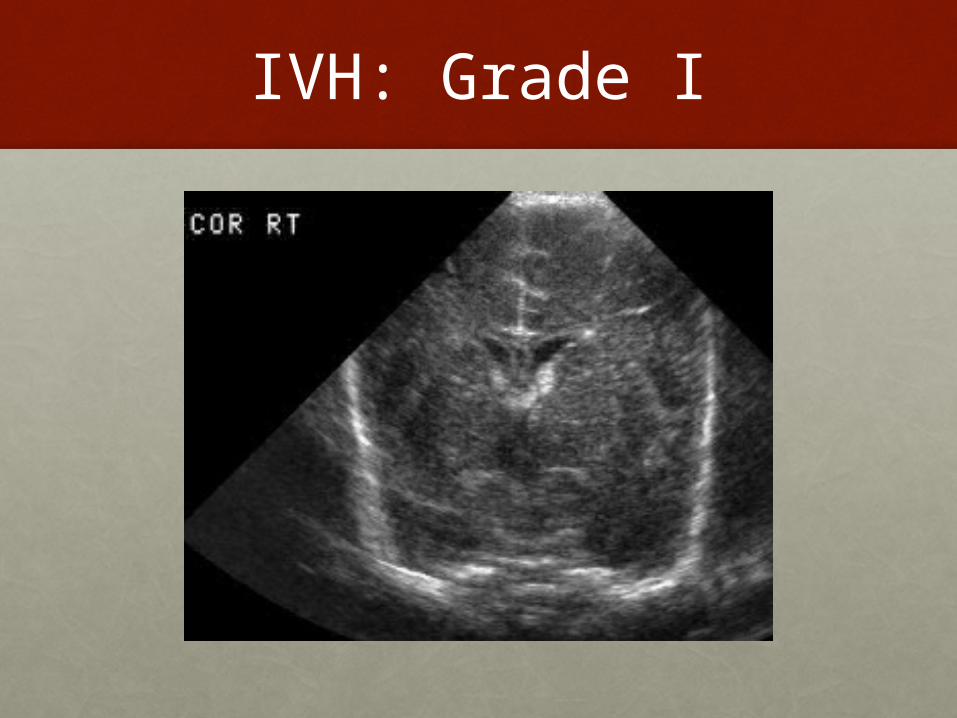
IVH: Grade I

IVH Pathology

IVH Pathology - Severe bleed

Outcomes for IVH
• ELBW preterm infants with grade I or II IVH may have poor neurodevelopmental outcomes
• Grade III or grade IV IVH is associated with the least favorable neurodevelopmental results• the degree of prematurity and the presence
of chorioamnionitis may also be major contributors to severe long-term disabilities
• IVH may lead to posthemorrhagic hydrocephalus

Post-hemorrhagic Ventricular Dilation
• 65% no progressive ventricular dilation• Majority of infants with slight/moderate IVH• Minority of infants with severe IVH
• 35% slowly progressive ventricular dilation• 65% spontaneous arrest within 4 weeks
with some or complete resolution• 30% continue to progress > 4 weeks, 1/3 of
these become rapid• 5% rapidly progress < 4 weeks

Outcomes forPHH/PVL
• parenchymal hemorrhage causes cerebral infarction and can lead to cerebral or cerebellar porencephaly
• Porencephaly and posthemorrhagic hydrocephalus are among the most devastating CNS events in premature infants.
• Cystic PVL• High risk for CP• Cognitive delays in children with severest lesions
on u/s and with spastic quadriplegia
Ventriculo-peritoneal shunt
• Although ventricular dilatation may be reversible, infants with severe ventricular enlargement are at high risk for neurodevelopmental handicap
• Rapidly progressive posthemorrhagic hydrocephalus may require permanent placement of a cerebrospinal fluid (CSF) shunt
• The long-term neurodevelopment of ELBW infants who require shunt insertion is very unfavorable compared with ELBW infants with intraventricular hemorrhage who do not have ventricular enlargement
• head circumference should be monitored for rapid or slow growth

Shunt Malfunction
• the NICU graduate with a VP shunt must be monitored for for shunt infections or malfunctions
• Malfunctions are typically due to an occlusion of the proximal or distal cannula with a subsequent increase in intracranial pressure
• Poor feeding, vomiting, irritability, lethargy, sleepiness, apnea, and seizures
• shunt infection and meningitis should be suspected with fever and malaise

PVL sequelae
• Other postnatal events leading to PVL include CSF infections or intraventricular hemorrhage, life-threatening apnea and bradycardia, and cardiorespiratory arrest
• The condition is otherwise identified on cranial sonograms as echogenic areas in the periventricular white matter. Injuries in these areas evolve into cysts
• PVL is highly associated with subsequent neurodevelopmental disabilities, particularly cerebral palsy
• Persistence of cysts is known to increase the risk of severe neuromotor abnormalities

















