51
Concussions: New Guidelines and What It Means In Today’s Athletic Environment Aaron Bott, MD Dave Schultz, MEd, ATC Sports Medicine Outreach Program Nebraska Sports Concussion Network
| Date post: | 11-Jan-2016 |
| Category: |
Documents |
| Upload: | laura-haynes |
| View: | 216 times |
| Download: | 0 times |

Concussions: New Guidelines and What It Means In Today’s Athletic Environment
Aaron Bott, MD
Dave Schultz, MEd, ATCSports Medicine Outreach Program
Nebraska Sports Concussion Network

The Concussion ProblemThe Concussion Problem
• Concussion injury reporting increasing dramatically.
• Substantial changes in concussion management guidelines in past 3-5 yrs.
• General void in education and awareness.• Disregard for seriousness of “minor” injuries.• Lack of consensus on management protocol by
healthcare professionals.

The Concussion ProblemThe Concussion Problem
• Athletes, knowingly & unknowingly, playing with symptoms, leave the brain vulnerable to long-term neurological impairment, serious and catastrophic injury, even death.


Nebraska Schools,Nebraska Schools, Serious & Catastrophic Head Injuries Serious & Catastrophic Head Injuries
Brent Cerny, Cedar Bluffs HS, FB 1995 Second-Impact Syndrome
Adrian Regier, Wheatland-Madrid HS, FB 1997 Second-Impact Syndrome
Nick Vorhees, Harvard HS, FB 1998 Subdural hematoma, decompression
Matt Hetrick, Coleridge HS, FB 2004 Subdural hematoma, hospitalized only
David Huebner, North Platte, FB 2004 Subdural hematoma, decompression
Brady Beran, Lincoln East, FB 2004 Subdural hematoma, decompression
Eric Lofton, Om. Northwest, FB, 2007 Subdural hematoma, decompression
Derek Ruth (12yo) Malcolm MS, FB 2008 Subdural hematoma, decompression
Shelton Dvorak, Pierce HS, FB Sept. 30, 2011


Concussion ScenariosConcussion Scenarios
• On-field Injuries (acute)• “Bell-Rung, Dinged”• “Dazed, Shaken Up, Rocked, Lit-Up”
• Injuries that are unknown and unreported • Injuries occurring outside team play
• MVA, playing on other teams, other mishaps
• Accumulative, sub-concussive injuries• Post-Concussion Syndrome (chronic)

Post-Concussion SyndromePost-Concussion Syndrome
• Chronic Headache (migraine)• Sensitivity to Light & Noise• Chronic Fatigue• Balance (vestibular) Problems• Behavioral Changes• Sleep Problems• Cognitive Deficits• Academic Difficulties

The Concussion ProblemThe Concussion Problem
• Growing evidence of causation for memory impairment, emotional instability, erratic behavior, depression, problems with impulse control, and early onset neuro-degenerative diseases.• Dementia• Chronic Traumatic Encephalopathy (CTE)
• Boxers, NFL football players

CTE
CTE, first reported in 1928 and originally referred to as “dementia pugilistica” because it was believed to only affect boxers, is a progressive neurodegenerative disease caused by repetitive trauma to the brain. The use of the terms Traumatic Encephalopathy and CTE were first used in the 1960s.
The disease is characterized by the build-up of a toxic protein called tau in the form of neurofibrillary tangles (NFTs) and neuropil threads (NTs) throughout the brain. The abnormal protein initially impairs the normal functioning of the brain and eventually kills brain cells.
Early on, CTE sufferers may display clinical symptoms such as memory impairment, emotional instability, erratic behavior, depression and problems with impulse control. However, CTE eventually progresses to full-blown dementia. Although similar to Alzheimer’s disease, CTE is an entirely distinct disease.

CTE

TAKE HOMETAKE HOME
Many head related catastrophes do not arise from the blow on the day of the catastrophe – but from an exacerbation of an earlier blow that did not heal.
Concussions not only result from a substantial blow or impact to the head, but also result from the accumulative affect of minor blows over time (hours/days/weeks), where such circumstances are much less apparent to the untrained and uniformed.

LB260 - Concussion Awareness ActLB260 - Concussion Awareness Act
• Interscholastic sports teams, and any youth sports organizations, 19yo and younger.
• 3 Primary Components:• EducationEducation, annual basis
• Coaches concussion training (online)• Athletes/Parents provided concussion information
• RemovalRemoval of athlete if “reasonably suspected” of having concussion.
• Written Clearance Written Clearance for RTP by appropriate licensed healthcare professional, and parent.

Appropriate Licensed Healthcare ProviderAppropriate Licensed Healthcare Provider
Physician: MD/DO, PA-C, APRNNeuropsychologistAthletic Trainer
• Or, qualified individual able to provide healthcare services where doing so falls within one’s scope of practice and state licensure, AND trained in the evaluation and management of traumatic brain injuries among a pediatric population.
LB260, July 2012
CONCUSSIONSCONCUSSIONSDefinitionA complex pathophysiological process affecting the brain, induced by traumatic biomechanical forces.
1. Direct blow to the head region; impulsive force transmitted to the head.
2. Rapid onset of short-lived neurological impairment that resolve spontaneously.
3. Acutely, symptoms largely reflect a functional disturbance, rather than structural injury.
4. Symptoms may or may not involve LOC, where resolution follows a sequential course, where some of which may be prolonged.
5. No abnormality in standard structural neuro-imaging studies.
Consensus Statement on Concussions in Sport: The 3rd International Conference on Concussion in Sport held in Zurich,
P McCrory, W Meeuwisse, K Johnston, J Dvorak, M Aubry, M Molloy & R Cantu, Br. J. Sports Med. 2009; 43;i76-i84, doi: 10.1136/bjsm.2009.058248

““Metabolically Metabolically for the brain, a for the brain, a concussion is concussion is like running a like running a marathon.”marathon.” Bleiberg, J. MD 2002

CONCUSSIONSCONCUSSIONS
Neurometabolic Cascade Indiscriminate release of
neurotransmitters Unchecked ionic fluxes
K+ efflux huge Ca+ influx
mitochondrial oxidation activates cell death
mechanisms
Neuronal depolarization Glucose metabolism
cellular energy crisis
cerebral blood flow
State ofState of
Post-Post-ConcussiveConcussive
VulnerabilityVulnerability

Second Impact Second Impact SyndromeSyndrome
• Condition is catastrophic; carries a 50% chance of death (mortality), and a 100% likelihood of permanent neurological impairment (morbidity).

Concussion Injury RatesConcussion Injury RatesPowell & Barber-Foss, 1999
• 3-6%3-6% of all athletic injuries occurring in contact and collision sports.
• 10%10% of athletes, on avg. (FB: 15-20%), in a contact or collision sport will sustain a concussion/season.
Concussion Case RateFootball: 63.4%Wrestling: 10.5%Soccer (G): 6.2%Soccer (B): 5.7%Basketball (G): 5.2%Basketball (B): 4.2%Softball: 2.1%Baseball: 1.2%F. Hockey (B): 1.1%Volleyball: 0.5%

Boden, BP, & Cantu, R. et al. . Catastrophic Head Injuries in Catastrophic Head Injuries in High School and College FootballHigh School and College Football. Am. J Sports Medicine, 2007, 35(7), 1075-1081.
• Nat’l Ctr. for Catastrophic Sports Injury Research• 13 academic yrs., 1989-2002
• 9494 catastrophic head injuries catastrophic head injuries• 75 subdural hematomas• 10 subdural hematomas & diffuse brain edema• 5 diffuse brain edema• 4 aneurysms or congenital A-V malformations
• 7.27.2 catastrophic head injuries per year

CONCUSSIONSCONCUSSIONSSymptoms
•Subtleties of “Symptoms” are not easily identifiable, but are at the core of proper concussion management.
•Greater concern for length of time symptoms are present, more so than which ones, or how many – but all 3 remain important to proper assessment & diagnosis of concussion.

CONCUSSIONSCONCUSSIONS
Hallmark Signs• Loss of
consciousness• Confusion• Disoriented• Unsteady

Severity Grading ScalesSeverity Grading Scales
Grade I Grade II Grade IIImild moderate severe
Colorado Medical No LOC No LOC LOC
Society Guidelines Confusion w/o PTA Confusion w/PTA
Cantu Grading System No LOC LOC <1min. LOC >1min.
PTA <30min. PTA >30min. - <24hrs. PTA >24hrs.
S/S <30min. S/S >30min. - <24hrs. S/S >1wk.
American Academy of No LOC No LOC Any LOC
Neurology Guidelines s/s abate <15 min. s/s >15 min.Transient confusion Transient confusion
Loss of Consciousness & Loss of Consciousness & Post-Traumatic AmnesiaPost-Traumatic Amnesia
• Grading Scales have not been data driven.
• Only 9% of concussions involve LOC
• Only 24% of concussions involve PTA• Retrograde v. Anterograde• Short-term memory, Memory recall• More persistent symptoms than those with
brief LOC.
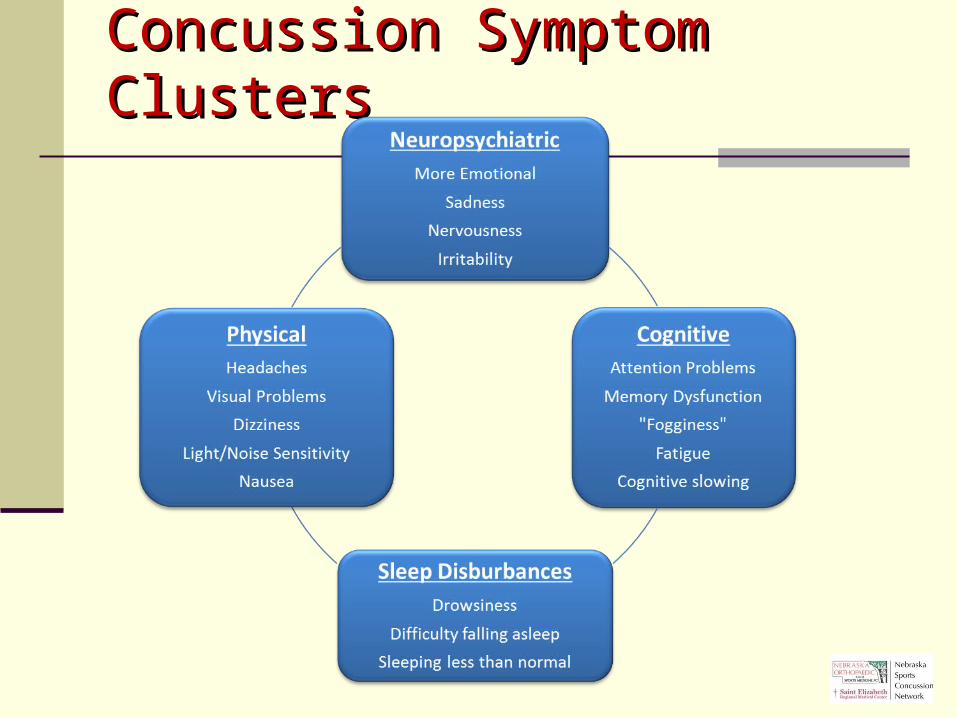
Concussion Symptom ClustersConcussion Symptom Clusters

CONCUSSIONSCONCUSSIONSSymptoms – Reported by Athlete [50%]
• Prior History (risk factor)
• Headache• Nausea• Balance Problem/
Dizziness• Fatigue• Drowsiness• Blurred vision
• Feeling like in a “fog”• Difficulty
concentrating• Difficulty
remembering• Sensitivity to light• Sensitivity to noise• Feeling slowed down

Symptom ChecklistSymptom Checklist
(Graded Symptom Scale)(Graded Symptom Scale)
Player Name: ________________________________________________________
Date of Injury: ________________ Date of Exam: ______________________
absent Mild moderate severe 0 1 2 3 4 5 6 Score
Headache
Nausea
Balance problems/Dizziness
Fatigue
Drowsiness
Feel like "in a fog"
Difficulty concentrating
Difficulty remembering
Sensitivity to light
Sensitivity to noise
Blurred vision
Feeling slowed down
Total: Other symptoms evident since injury?:
Randolph, C, Millis, S., Barr, WB, McCrea, M, Guskiewicz, KM, Hammeke, TA & Kelly, JP. Concussion Symptom Inventory: An Empirically Derived Scale for Monitoring Resolution of Symptoms Following Sports-Related Concussion. Arch. Clin. Neuropsych, 24 (2009) 219-229.
Concussion Symptom Inventory (CSI)

Sideline Assessment ProcedureSideline Assessment Procedure
• Sideline Assessment Protocol• Assess for Signs & Symptoms• Check Orientation• Check Memory; Memory Recall• Check Concentration• Check Balance
• Athlete is disqualified with any abnormality or deficiency (positive finding)
• Direct to appropriate licensed healthcare provider

Balance Error Scoring System (BESS)Balance Error Scoring System (BESS)
• Errors:• Opened eyes• Stepped, fell, stumbled• Removed hands off hip• Moved hip 30º, flex/abd.• Lifted toes/heels• Remained out of
position >5 sec.• Errors tabulated for all 6
tests.

CONCUSSIONSCONCUSSIONS
No universal agreement on Grading Scales or Management Protocol.
Unanimous agreement that an athlete with post-concussion symptoms does not return to play contact/collision sports.

Know who you’re dealing withKnow who you’re dealing with
Type A - Warrior “…they’ll have to drag me off the field
before I stop playing – I’M FINE!!!”
Type B – Drama Queen “My mom and dad made me go out. I hate
playing… I’m looking for a way out… make it look like I have a concussion”.

Symptomatic 7 days 10 days
Concussed Athlete #1
Concussed Athlete #2
Concussed Athlete #3
Concussed Athlete #4
Concussed Athlete #5
Concussed Athlete #6
Concussed Athlete #7
Concussed Athlete #8
Concussed Athlete #9
Concussed Athlete #10
75% asymptomatic within 7 days
92% asymptomatic within 10 days
Symptom ResolutionSymptom Resolution

Symptoms vs. Neurocognitive FunctionSymptoms vs. Neurocognitive Function
• Management & Return to Play (RTP) decisions placing greater emphasis on brain function and the value of Neurocognitive Testing.
• Generally, Symptoms tend to resolve before Neurocognitive Brain Function.

(Neuro)Cognitive Function(Neuro)Cognitive Function
• Concentration• Memory
• Short-term• Delayed Recall
• Reaction Time• Attention Span• Processing Speed
Neurocognitive TestingNeurocognitive Testing
• Computerized application (on-line)• Evaluation of multiple aspects of brain function:
• Memory, Attention, Processing Speed, Reaction Time, Concentration
• “Snapshot” of brain function.• Pre-Injury v. Post-Injury Test Comparison• Valid, objective, more consistent, safer
concussion management and RTP decisions.
Baseline Testing• Preseason testing under normal conditions
prior to injury.• Testing conducted online in computer labs at
schools by school staff.• Testing completed in ~25 minutes; multiple
users to be tested at same time.• Baseline data saved on secure server and
accessed if an athlete sustains a head injury requiring post-injury testing.
Neurocognitive TestingNeurocognitive Testing

Post-Injury Testing• If an athlete sustains a concussion, they are
tested again, 24-72 hrs. s/p injury, or upon being asymptomatic.
• Post-injury testing is conducted by a trained physician, Neuropsych., or school’s ATC.
• Post-injury test data are compared to pre-injury baseline data.
• Once post-injury test scores return to baseline (normal), athlete may RTP*.
Neurocognitive TestingNeurocognitive Testing
ImPACT Test™
ImPACT Test ModulesDemographic sectionSymptom Inventory
1)Word Discrimination2)Design Memory3)X’s & O’s with distractor task4)Symbol Matching5)Color Match6)Three-Letters with distractor task
Symptom Inventory, 2nd trial optional
Non-verbal Problem Solving
Reaction Time Visual & Verbal Memory Response Variability Attention Span Working Memory Sustained Attention Selective Attention


ImPACT Test™

• Symptom-Free at Rest• Symptom-free with Cognitive/Physical Exertion• Stepwise RTP Progression• Normal Neurocognitive Data
Return to Play CriteriaReturn to Play Criteria

Stepwise Return to Play ProgressionStepwise Return to Play Progression
1. Complete Rest while symptomatic• Physical & Cognitive Rest
2. Begin light, aerobic activity (15-20 min.)• Bike, Walk, Swim; no wt. lifting
3. Sport/Position conditioning drills (30-45 min.)
4. Non-Contact practice (physician authorization)
5. Full, unrestricted practice
6. Competition

[Days, Weeks, Months]
Timeline:
Asymptomatic Return to full participation
Injury SymptomaticRest: physical & cognitive RTP Progression
Post-Injury Test
Post-Injury Test (24-72 hrs.)
Baseline Test
Monitor for return of S/S during & after
exertion
Timeline for Return to PlayTimeline for Return to Play

Take HomeTake Home
• FAR/coach’s role is to “RECOGNIZE” “RECOGNIZE” potential for head injury.
• If any S/S are noted, FAR/coach removes athlete. “The End – period.” Out of coach’s or player’s hands.
• Coaches should never render their own decision for RTP involving a concussed athlete or one suspected of having a concussion, without written authorization from appropriate licensed healthcare professional.

Return to PlayReturn to Play
• Schools/Athletic Training Staff retain the responsibility to disqualify any athlete’s RTP in the presence of note from anyone that clears an athlete that remains symptomatic.
1. Symptom-Free, during exertion.
2. Neurocognitive Test scores return to normal.
3. Athlete completes RTP Progression before resuming play.

• Nebraska Orthopaedic & Sports Medicine, PC
• Saint Elizabeth Regional Medical Center
• Medical Director, Daniel Tomes, MD• 100+ Credentialed ImPACT Consultants
•Regional Sponsors & Medical Communities
•80+ High School Athletic Programs• 9,000+ tests since July 2010
Nebraska Sports Concussion NetworkNebraska Sports Concussion Network

ImPACT Demo TestImPACT Demo Test
www.impacttestonline.com/impactdemoCustomer ID: KJZB2X8FHG (case sensitive)

ResourcesResources
• Nebraska Sports Concussion Network• http://www.NebSportsConcussion.org/
• ImPACT Testing Services• http://www.impacttest.com/

In ReviewIn Review
• Recognize that a concussion has occurred.• If concussion occurred, stop participation,
refer to appropriate healthcare provider • Symptom resolution varies widely.• While symptomatic, remain at rest, both
physically and cognitively.• RTP timeframe can not be established in
earliest stages of recovery.• RTP occurs after all criteria have been met.

QuestionsQuestions
Patrick E. Clare, MDRonald O. Schwab, MD
Donald J. Walla, MDThomas. M. Heiser, MD
Daniel R. Ripa, MDDavid J. Clare, MD
James W. Gallentine, MDSteven J. Volin, MDJustin D. Harris, MD
Scott A. Swanson, MDDaniel B. Cullan II, MD
Aaron M. Bott, MDJoseph Mulka, MD

THANK YOUTHANK YOU

















