111
Council of Governors 10 April 2014,10:00 am Holiday Inn Express, Reedfield Place, Walton Summit PR5 8AA
Council of Governors 10 April 2014,10:00 am
Holiday Inn Express, Reedfield Place, Walton Summit
PR5 8AA

�

FORMAL COUNCIL OF GOVERNORS Meeting to be held at
Holiday Inn Express, Reedfield Place, Preston PR5 8AA
10:00am, Thursday 10 April 2014
A G E N D A
Item Number Item Presenting Time
CG 016/14 Welcome and opening comments Derek Brown 10:00
CG 017/14 Apologies and Declaration of Interests Derek Brown 10:05
CG 018/14 Minutes of the Council of Governor meeting held on 14 January 2014 Derek Brown 10:10
CG 019/14 Matters Arising and Action Tracker Updates Derek Brown 10:15
CG 020/14 Chair’s Report Derek Brown 10:20
CG 021/14
Thematic Reviews
• Trust Research & Development (presentation)
Heather Iles-Smith 10:25
Break 11:00
Formal Business of the Council
CG 022/14
CG 023/14
CG 024/14
CG 025/14
• Governance Handbook Review: Terms of Reference
• Governance Handbook Review: NED Recruitment
• Governor Training Programme 2014/15
• Annual Members Meeting 2014 Recommendation (verbal)
Diane Halsey Nigel Harrison Diane Halsey Lin Jones
11:20 11:25 11:30 11:40
CG 026/14
CG 027/14
CG 028/14
CG 029/14
Reports issued for information and assurance
• Chief Executive Assurance Report • Quarterly Workforce Report • Sub Committee Key Messages
• Sub-Committee’s Cycles of Business
Heather Tierney-Moore Craig Barratt Sub-Committee Chairs
Sub-Committee Chairs
12:00
-
12:10
12:20
CG 030/14 Any Other Business 12:30
CG 031/14
Date and Time of Next Meeting Chief Executive’s Briefing
Wednesday 14 May @ 10:00am, Ribby Hall Village
12:35

Informal CoG (with part Formal)
Wednesday 11 June @ 10:00am, Ribby Hall Village
Lunch Break 12:40
Governor Training & Development Programme:
• Emotional Intelligence Training Andy Hesketh (facilitator)
13:30
Close of Session

COUNCIL OF GOVERNORS Minutes of the meeting of the Council of Governors held on 14 January 2014 Present Derek Brown (Chair) Public Governors Alan Ravenscroft Brian Spencer Brian Taylor Bill Coulton Catherine Dobson David Jackson Linda Jones Hilary Whitworth John MacLeod Mike Marsden Mike Wedgeworth Tahir Khan Tom Lawman Appointed Governors David Jones Staff Governors Dr Graham Ash Andrew Kirkby Barbara Hummer Lynne Bax Linda Ravenscroft Paul Morris
In Attendance Peter Ballard, Non-Executive Director (SID) Naseem Malik, Non-Executive Director Diane Halsey, Company Secretary Craig Barratt, Director of Workforce, Innovation & Transformation Steve Winterson, Engagement Director Dee Roach, Director of Nursing Heather Tierney-Moore, CEO David Keddie, Stakeholder Engagement Director 1 x member of the public
CG001.14 WELCOME AND OPENING COMMENTS The Chair welcomed everyone to the meeting and confirmed that the meeting was quorate. Particular welcome was given to the new Governors, Bill Coulton and Lynne Bax. The newly appointed Director of Nursing gave a short introduction about her background. Naseem Malik, newly appointed Non-Executive Director also introduced herself and briefly described her experience and public sector background. The Chair reminded Governors of the need to complete a personal biography for the Trust internet page. A response to a Governor question was tabled for discussion in Any Other Business.
CG002.14 APOLOGIES FOR ABSENCE AND DECLARATIONS OF INTEREST Apologies had been received from Nigel Harrison and Steve Sansbury.
Unconfirmed

There were no declarations of interest.
CG003.14 MINUTES OF COUNCIL OF GOVERNOR MEETING HELD ON 29 OCTOBER 2013 Subject to one amendment the minutes of the last meeting held on 29th October 2013 were accepted as a true and accurate record. Minute CG 097.13 would be amended to reference the Executive Quality Committee instead of the Medical Advisory Committee.
CG004.14 MATTERS ARISING AND ACTION TRACKER UPDATES The Chair noted there were no outstanding actions on the tracker.
CG005.14 CHAIRS REPORT The Chair explained the purpose of the Chair’s Report in ensuring Governors remain updated about Non-Executive Director activity and provided additional details of developments since the report was written. It was noted that a Non-Executive Director had successfully participated in a conference to engage with GPs in Blackpool led by one of the Trusts Clinical Directors and an update would be brought to the CoG in due course.
CG006.14 CQC OUTCOMES AT WORDSWORTH The Chair provided background on the thematic review of the Wordsworth
Unit and introduced Mandy Thompson, Modern Matron for Clinical Business Unit 5. Mandy explained the purpose of the thematic review and described the Care Quality Commission (CQC) visit and subsequent report which initially highlighted minor concerns within the then Coniston ward. The Modern Matron discussed the details of the failings and issues with implementation of required processes and procedures which had been highlighted in the CQC report. It was noted that the Trust had identified the concerns raised together with some other concerns and had determined a comprehensive action plan which exceeded the requirements based on the CQC visit alone.
The Modern Matron explained the implications of the CQC report and made
particular note of the management decisions taken by the Trust in response to the issues raised, including closure of the specialist dementia ward and suspension of staff.
The Modern Matron gave a comprehensive overview of the 8-step
improvement plan which was developed and implemented over a 6 month period. Amongst the improvements made to clinical care processes saw the implementation of regular ward meetings and a robust clinical supervision programme to ensure high standards of care. She noted the full implementation of the Friends & Family Test across the unit and described a new patient & carer feedback group to ensure relatives are involved in the quality of service provision. The improvements made have been very well received amongst staff, doctors and patients and carers and the ward was re-named and re-opened as the Wordsworth Unit on 24th September 2013 with a new skill mix of staff to ensure the improvements continue to be embedded.
The Modern Matron explained some of the improvements made to the therapeutic care environment of the unit with input from a leading dementia specialist to redesign wards and communal areas. She noted that patients have benefited from new technology such as Skype to communicate with relatives and programmes designed to aide memory and recollection.
The Modern Matron gave an overview of the unit at present following all the
recent changes, noting that all wards comply with Quality SEEL and matrons have seen their time spent on the ward increase to 80-90% meaning care is monitored regularly. The positive outcome of the CQC re-visit was highlighted and acknowledgement given to the vast improvements made to the wards.
The Modern Matron outlined the aspirations for the future of Wordsworth and
summarised by noting the feelings and thoughts of the staff including increased morale, pride in the unit and in the care they provide.
Following a Governor query around teamwork within the unit, the Modern
Matron described the improvement to team dynamics and increase in morale. When prompted if this improvement to staff attitudes has positively affected patients, the Modern Matron noted that although patients remain acutely unwell when they enter the ward, assurance remains around the strong governance of care processes and procedures in place to support patients. The Chief Executive supported this view and praised the highly effective engagement of staff at the unit.
A query from a Governor regarding the extra funding and resource allocated
to Wordsworth generated a discussion around how the improvement plan was financed. The Chief Executive described the use of existing administrative staff resource to minimise impact upon clinical services and explained the necessary allocation of capital expenditure due to the challenging nature of the care environment. The Chief Executive emphasised the need for special measures to ensure Wordsworth would not only meet required standards but also to ensure the unit met the Trust’s aspiration of excellent inpatient dementia care.
A discussion followed around the involvement of carers and family in care
planning for dementia inpatients, and the impact when patients are moved back into the community. It was acknowledged that care provision in the community is shared across several organisations and continuity of care can be difficult to manage. The need to work closely with partners to ensure improvements can be made to quality of care planning was recognised and the Trust is seeing substantial progress between inpatient and community teams.
The Chief Executive agreed with a Governor request that staff learning from
the experiences at Wordsworth be utilised to ensure ongoing learning for the wider Trust. The importance of utilising the Family and Friends test for monitoring relative’s views was noted and assurance given that this is now
incorporated into the Wordsworth Team Information Board and discussed at each meeting.
A Governor acknowledged the positive reports from Wordsworth. The Chair thanked the Modern Matron on behalf of the Council. CG007.14 BI-ANNUAL ELECTION ACTIVITY The Company Secretary gave an overview of the governor election activity in
November 2013 and highlighted the statutory requirement to report the election turnout. She described the use of a new election partner, UK Engage and outlined the plan for recruitment to other governor vacancies in the near future. It was noted that raising profile of the governor is a key priority for recruiting to the Council and the importance of governor biographies in this process was emphasised.
A Governor noted the relatively low turnout figures during the election,
particularly the disappointing staff turnout figures. The Company Secretary explained that although turnout is low it is not untypical for Foundation Trusts. The high number of staff governor nominations was very encouraging and the focus for future elections will ensure we further develop the engagement of staff during elections.
CG008.14 CALENDAR OF MEETINGS & CYCLE OF BUSINESS 2014/15 The Company Secretary gave some background to the Cycle of Business
2014/15 and explained the content is drafted around discharge of statutory governor duties as well as thematic reviews to give greater understanding of the Trust. She highlighted the full regard given to Governor input whilst drafting the Cycle of Business and noted specific aspects of the Cycle which have been tailored to Governor requests, including the responsive agenda for thematic reviews which allows the Council free scope to request topics for review. The process for suggesting thematic reviews was outlined and Governors were encouraged to utilise informal CoG meetings to suggest and discuss possible topics. The accompanying CoG Calendar of Meetings 2014/15 was also provided for approval and would become effective from April 2014.
There were no questions and the Council accepted the Cycle of Business and Calendar of Meetings 2014/15.
CG009.14 REFORMAT OF PATIENT EXPERIENCE SUB-COMMITTEE The Company Secretary gave the background and rationale for instigating a
re-focus of business for the Patient Experience Oversight Group (PEOG), which was initiated by the previous PEOG Chair. The Council were required to ratify the decision to appoint David Jones as the new PEOG Chair to lead the implementation of the new Cycle of Business for the Committee. A current member of PEOG confirmed the group would continue to receive both quantitative, and qualitative data reports in order to discharge their responsibilities.

The Council approved the appointment of David Jones as Chair of PEOG. CG010.14 CHIEF EXECUTIVE ASSURANCE REPORT The Chief Executive introduced her report and highlighted the positive
reduction in out of area bed placements despite continuing pressure on mental health beds. She noted a large scale transformation project, sponsored by the Medical Director, was underway within the Trust to review and redesign the whole of the mental health urgent care pathway. The project was expected to last for 12 months and an update would be brought back to the Council in due course.
Referring to the assurance report, a Governor queried the interpretation of
the narrative text. The Chief Executive clarified the need for more precision when reporting figures and this would be fed back for future reports.
A Governor raised a query around Lancashire Care Trust’s bank and agency
spend. The Director of Workforce, Transformation & Innovation explained that although the usage level of agency staff is currently higher than desired, the use of bank staff isn’t an inherently bad thing as it allows flexibility within the workforce. A discussion followed around ensuring continuing quality of care and lower agency spends. The Director of Workforce, Innovation & Transformation offered to conduct a deeper review for the next Workforce report and the Chair requested a thematic review be scheduled focussed on HR functions.
The discussion continued around use of qualified and unqualified bank and agency staff. The Chief Executive confirmed that whilst the use of agency staff does not represent a risk in general administrative areas, use in clinical areas can pose a quality risk and she confirmed that the Director of Nursing was undertaking a piece of work aimed at eliminating agency staff in these areas. Following a Governor query the term Wellness Presence was defined by the Director of Workforce, Innovation & Transformation. A Non-Executive Director requested that future Quarterly Workforce Reports also include a breakdown of diversity. Governors agreed the new format of the report is much improved and Governors suggested minor areas of alteration for future reports.
Following a query from a governor the procedure for recruitment of bank and agency staff was outlined, it was emphasised that the Trust have robust temporary staffing procedures to ensure existing staff who register with an agency are not re-employed by the Trust at premium cost. A Governor referred back to the bed occupancy figures within the Chief Executive Assurance Report and a discussion followed around the constant review and evaluation of the provision of mental health beds.

CG011.14 QUARTERLY WORKFORCE REPORT This report was covered in CG010.14. There were no further questions. CG012.14 MEMBERSHIP & STAKEHOLDER ENGAGEMENT UPDATE The Stakeholder Engagement Manager introduced himself and his report
into the membership strategy and stakeholder engagement update. He gave an overview of the membership strategy and its purpose, the importance of having regular reviews of strategy implementation and discussed key drivers such as diversity of membership, profile of the Trust as well as cost effectiveness.
The delivery mechanisms of member engagement were outlined with details
given of the most recent public engagement event on Long Term Conditions, which was jointly hosted by Lancashire Care, Lancashire County Council, Lancashire Teaching Hospitals, Healthwatch Lancashire and both Chorley & South Ribble and Greater Preston CCGs. The Stakeholder Engagement Manager discussed the strategic intentions for stakeholder engagement in more detail, in particular he highlighted that the engagement is clinically led, co-owned and managed in an integrated way.
He summarised by describing the role of Governors within the Trusts engagement activity. He reminded the Council of the forthcoming engagement workshops designed specifically for Governors to inform and equip them with additional knowledge of the Trust prior to participating in external engagement.
CG013.14 SUB COMMITTEE KEY MESSAGES No items were raised in relation to this item. The CoG accepted the Key
Messages reports. CG014.14 ANY OTHER BUSINESS
The Chair referenced the tabled response to a Governor question around waiting times for mental health services and offered the Governor opportunity to contextualise his question for the benefit of other Governors. The Chief Executive provided a detailed overview of the Executive investigations into waiting times across the health sector and explained in particular how the Board needs to be confident that Trust waiting times are acceptable and being managed in accordance with demand. A discussion followed around the involvement and engagement of third sector parties in establishing a mechanism for the Trust to engage more widely with the voluntary sector with a view to providing a wider offer of complementary services to client groups as appropriate. A discussion was had around accessing crisis resolution and home treatment teams out of hours and in particular the impact for families and patients. It was noted that the current delivery of crisis services is matched to demand and makes the most efficient use of resources that are available. There was a recognition that increased signposting of out of hours care was needed but that the pressure which builds in the system has to be addressed.

CG015.14 DATE AND TIME OF NEXT MEETING Chief Executive Briefing, Wednesday 19 February 2014
Informal Council of Governors, 18 March 2014

�
Meeting Date
Agenda Item
Number
Action Required By When Responsible For Action
Comments Status Minute Ref
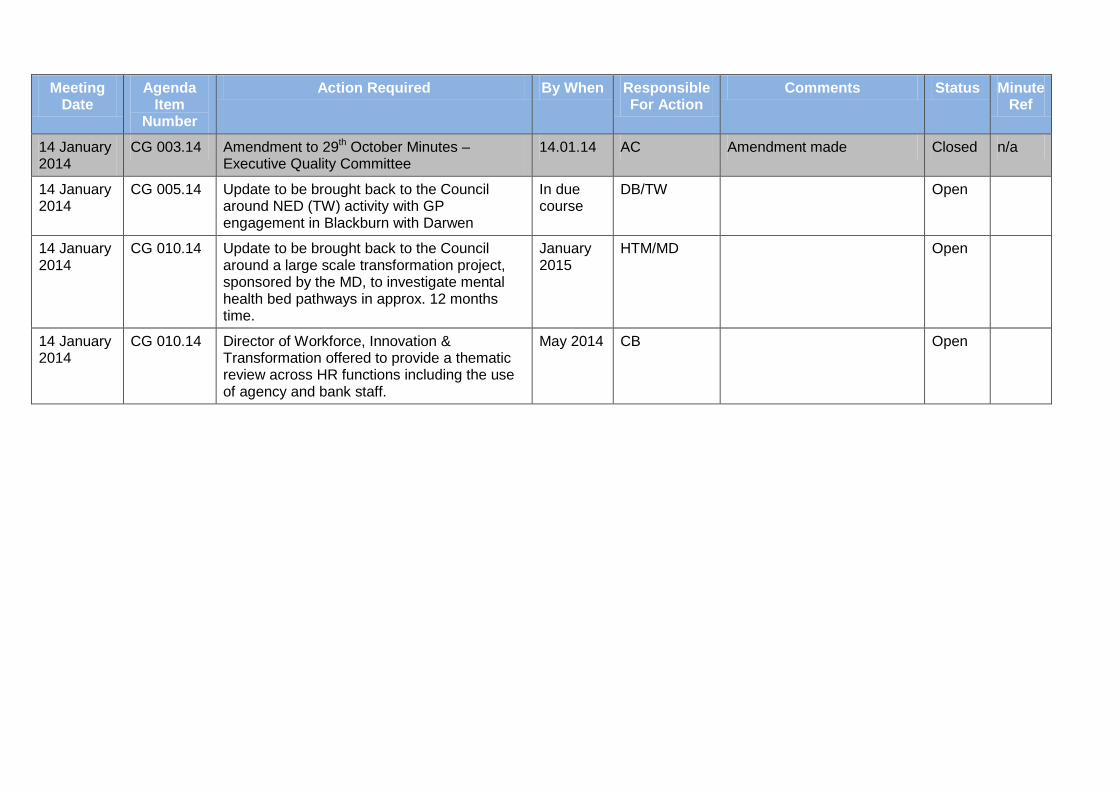
14 January 2014
CG 003.14 Amendment to 29th October Minutes – Executive Quality Committee
14.01.14 AC Amendment made Closed n/a
14 January 2014
CG 005.14 Update to be brought back to the Council around NED (TW) activity with GP engagement in Blackburn with Darwen
In due course
DB/TW Open
14 January 2014
CG 010.14 Update to be brought back to the Council around a large scale transformation project, sponsored by the MD, to investigate mental health bed pathways in approx. 12 months time.
January 2015
HTM/MD Open
14 January 2014
CG 010.14 Director of Workforce, Innovation & Transformation offered to provide a thematic review across HR functions including the use of agency and bank staff.
May 2014 CB Open

�

AGENDA NUMBER: CG 020/14
COUNCIL OF GOVERNORS – 10 April 2014 Chairs Report
FOIA STATUS: No Exemption
PAPER TITLE: Chairs Report
PURPOSE: The purpose of this report is to provide Governors with an update of the Non-Executive Directors activities
ACTION RECOMMENDED:
Noting
PAPER PREPARED BY: Jo Alker, Assistant Company Secretary
1.0 MONITOR CODE OF GOVERNANCE
In December 2013, Monitor re-issued the NHS Foundation Trust Code of Governance. The revised code originally applied from 1 April 2014 but has been brought forward to 1 January 2014 and will be reflected in this year’s Annual Report. The changes include a more prescriptive approach to how the Code is discharged and more granulation around reporting. It is not anticipated that we will have any difficultly with compliance other than in relation to the exceptional term of office for the Trust Chair and the Chair of Audit Committee. This will be fully disclosed and explained.
2.0 HOLDING THE NON-EXECUTIVE DIRECTORS TO ACCOUNT
In addition to the usual Board business, NEDs have been involved in their areas of special interest during the period from January to March: Teresa Whittaker has met with various LCFT employees, Internal and External Audit on a number of occasions. Teresa has attended Health Informatics Committee and a Complaints Panel. Chris Heginbotham chaired the Mental Health Act Committee and attended a meeting in preparation for that Committee. Chris acted as a panel member on an Appeal Hearing. Gwynne Furlong attended the Red Rose Corporate Services Board meeting and participated in a Complaints Panel. Gwynne acted as a panel member on interviews for the Red Rose Corporate Services Director, attended the Executive Property Strategy Committee, undertook a Good Practice visit and met with Executives on various topics. Peter Ballard acted as a panel member on an Appeal Hearing, attended a Healthwatch event and a Good Practice visit. Naseem Malik has attended service visits and undertook introductory meetings along with Louise Dickinson. All Non-Executive Directors have met with Andrew Harrison as part of the Board Evaluation exercise and attended a Board to Board with Chorley and South Ribble and Great Preston CCG.

AGENDA NUMBER: CG 020/14
COUNCIL OF GOVERNORS – 10 April 2014 Chairs Report
3.0 BOARD EVALUATION
It is now mandatory for Foundation Trusts Boards to review their effectiveness every three years and Monitor has issued a governance framework that outlines the approach that should be taken. I have commissioned an external independent company to undertake this review and a number of Governors have already been involved in a working group and provided feedback. Once the outcome of the review is available, I will circulate to Governors.
4.0 TRAINING Following the informal session on ‘Holding Non-Executive Directors to Account’ that took place on 26 June, feedback was collated and a ‘You Said, We Did’ action plan was produced and presented to Governors on 24 July 2013. Governors will be kept up to date on an ongoing basis as actions are implemented and closed off via this report. An updated version of the ‘You Said, We Did’ action plan detailing the action already taken is attached as Appendix One.
�

Lancashire Care NHS Foundation Trust
Council of Governors Action Plan “You Said, We Did” An overview of current provisions and future plans in response to Council of Governors discussions around Holding NEDs to Account

Council of Governors Informal Session – “You Said, We Did”
BACKGROUND
The Council of Governors undertook an informal discussion with a selection of Non-Executive Directors at the CoG meeting in June 2013. The initial purpose of this informal discussion was to raise awareness of the new statutory duty for Governors brought in by the Health and Social Care Act 2012; to hold the Non-Executive Directors, individually and collectively to account for the performance of the Board of Directors and to facilitate meaningful discussions around how Governors can expect to discharge these new responsibilities. Governors appoint NEDs to provide leadership, strategic direction and independent scrutiny and so Governors have to ensure they receive relevant assurances from NEDs and hold them to account for the performance of the organisation and the Board.
A number of Non-Execs took part in the session to provide knowledge and expertise to the conversations, especially around the specific areas of NED involvement and how Governors can hold NEDs to account in practice.
The outcomes of the discussions were collated and an action plan has been produced to reflect the top 4 themes emerging from the discussions along with some specific comments arising from Governor discussions. Accompanying these themes and comments are details of the current provisions already in place to address some suggestions as well as action points for any areas that require further investigation and development.
The top 4 themes arising from discussions were:
• Statutory duties of Governors & discharge of responsibilities• Non-Executive Directors – holding to account• Governor Development• Information Streams and data
�

Council of Governors Informal Session – “You Said, We Did”
Governor Comment “You Said” Current Provisions “We Do” Future Provisions “We Will” Updated in March 2014
1. Statutory Duties of Governors & Discharge of Responsibilities
“Be clear on roles of NEDs”
Remuneration/Nomination Committee receive the Role of the NEDs and Special Roles document
Circulate revised NED role descriptions and areas of interest out to wider Council
Non-Executive Director role descriptions circulated to all Governors on 05 November 2013
Remuneration/Nomination Committee involved in the recruitment process including role description of NEDs
NED Special Roles scheduled on the agenda for July Chief Executive Briefing
Scheduled onto the agenda and discussed
Governors have access to external guidance for background reading on NED roles and Governor roles e.g Monitor’s statutory duties for Governors
Electronic access to documents to be provided on CoG Zone area of website, redesign of webpage due Autumn 2013.
A working group to develop the CoG Zone have re-developed the site and it was re-launched February 2014
NEDs to give presentations of their roles and interests to the CoG.
All five of the existing Non-Executive Directors have now presented their Special Roles to the Governors.
“More work needed on CoG Cycle of Business to give the ‘bigger picture’”
Governor Handbook drives the formation of Cycle of Business and ensures discharge of responsibilities. Annual Plan drives the specific agenda items and themes are agreed by CoG
Schedule discussion on thematic reviews and priorities in October for setting next year’s Cycle of Business
Free agenda time has been scheduled into the CoG cycle of business for 2014/15 and it has been aligned to the cycle of business for the Board of Directors to ensure Governors receive timely performance and quality data
“Need for Governors to be at Board – everybody should have an opportunity to go to Board.”
All Governors were invited to put their name down to attend a formal Trust Board meeting and a schedule of attendance has been circulated. Governors also have the option of observing formal Trust Board but this needs to be pre-booked due to space limitations
Monthly CoG briefing disseminates outcomes from Board
Continue to promote this practice
The 2014/15 Trust Board meeting dates have been issued to Governors in February 2014 and included on the new Calendar of Meetings. Invites were extended to Governors and all of the places have now been booked. A reserve list is in operation for any governor cancellations to ensure places are distributed fairly.
“Potential of Governor learning and knowledge from attending Board”
Council of Governors Informal Session – “You Said, We Did”
Governor Comment “You Said” Current Provisions “We Do” Future Provisions “We Will” Updated in March 2014
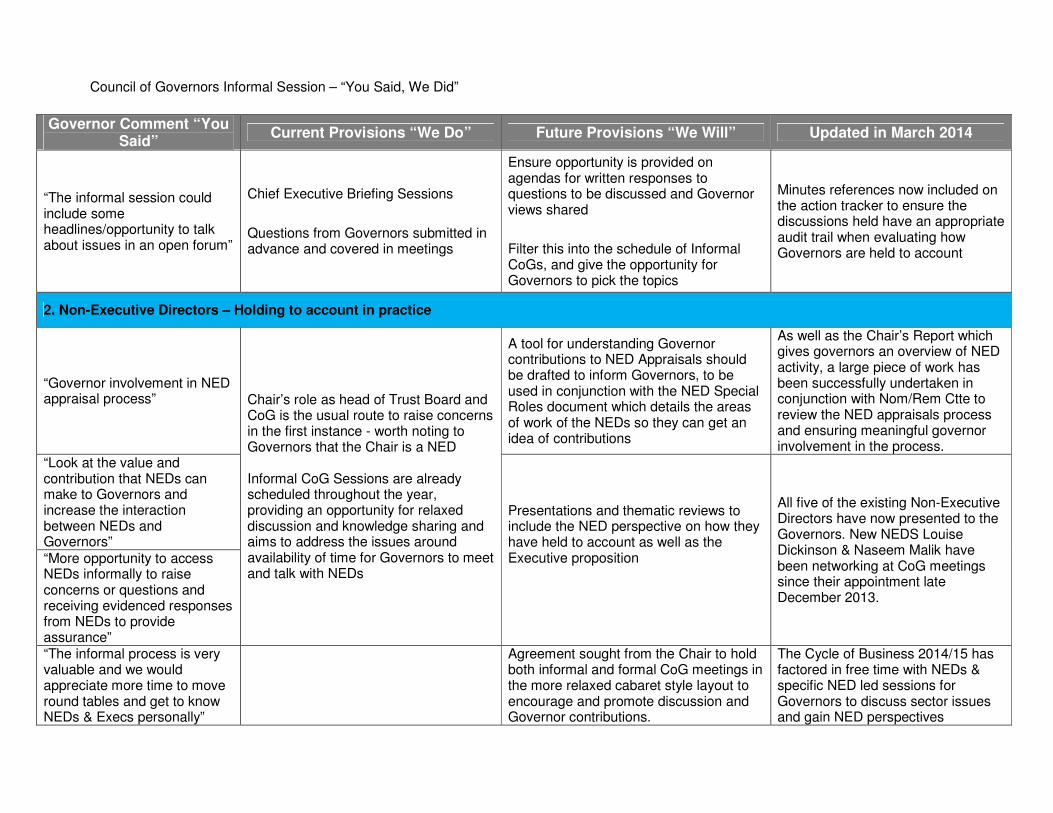
“The informal session could include some headlines/opportunity to talk about issues in an open forum”
Chief Executive Briefing Sessions
Questions from Governors submitted in advance and covered in meetings
Ensure opportunity is provided on agendas for written responses to questions to be discussed and Governor views shared
Filter this into the schedule of Informal CoGs, and give the opportunity for Governors to pick the topics
Minutes references now included on the action tracker to ensure the discussions held have an appropriate audit trail when evaluating how Governors are held to account
2. Non-Executive Directors – Holding to account in practice
“Governor involvement in NED appraisal process” Chair’s role as head of Trust Board and
CoG is the usual route to raise concerns in the first instance - worth noting to Governors that the Chair is a NED
Informal CoG Sessions are already scheduled throughout the year, providing an opportunity for relaxed discussion and knowledge sharing and aims to address the issues around availability of time for Governors to meet and talk with NEDs
A tool for understanding Governor contributions to NED Appraisals should be drafted to inform Governors, to be used in conjunction with the NED Special Roles document which details the areas of work of the NEDs so they can get an idea of contributions
As well as the Chair’s Report which gives governors an overview of NED activity, a large piece of work has been successfully undertaken in conjunction with Nom/Rem Ctte to review the NED appraisals process and ensuring meaningful governor involvement in the process.
“Look at the value and contribution that NEDs can make to Governors and increase the interaction between NEDs and Governors”
Presentations and thematic reviews to include the NED perspective on how they have held to account as well as the Executive proposition
All five of the existing Non-Executive Directors have now presented to the Governors. New NEDS Louise Dickinson & Naseem Malik have been networking at CoG meetings since their appointment late December 2013.
“More opportunity to access NEDs informally to raise concerns or questions and receiving evidenced responses from NEDs to provide assurance” “The informal process is very valuable and we would appreciate more time to move round tables and get to know NEDs & Execs personally”
Agreement sought from the Chair to hold both informal and formal CoG meetings in the more relaxed cabaret style layout to encourage and promote discussion and Governor contributions.
The Cycle of Business 2014/15 has factored in free time with NEDs & specific NED led sessions for Governors to discuss sector issues and gain NED perspectives

Council of Governors Informal Session – “You Said, We Did”
Governor Comment “You Said” Current Provisions “We Do” Future Provisions “We Will” Updated in March 2014
“Networking for Governors and NEDs – come prepared to share”
The outcomes of the informal session which took place in June suggested Governors were happy with the candour of the NEDs and felt they had come prepared to listen and engage
Informal meetings to include a networking opportunity for Governors, consideration to be given to how this can be facilitated to best effect.
Informal meetings will be about NED engagement.
Encouragement to be given to Governors to attend and contribute fully to CoG sessions.
The informal networking and NED led sessions which have been facilitated to date have been positively received by Governors and anecdotal feedback has shown Governors are appreciative of the additional input from NEDs over recent months.
“Possibilities to have conversations with NEDs – what’s going well, what’s not“
3. Governor Development
“Shadowing – attending CoG sub-committees to observe“
Governors can attend any committee to observe, by agreement with the Chair of the committee. For practical purposes around venues the visits need to be pre-planned
Governors continue to be able to attend sub-committees subject to agreement by the sub-ctte Chair.
“Don’t know what you don’t know – experience counts but learning all aspects of large organisation is difficult. Putting into context helps”
Invited to Membership Engagement events which provide insight as well as other engagement events
Governor Training Programme already in place which covers Audit, Finance, Equality and Diversity, Quality, Engagement & Membership as well as Emotional Intelligence Training
Attending Board meetings
Annual Planning process input from CoG.
Good Practice Visits
Not necessary to know all aspects of the
Continue to promote the importance of Governors attendance at training sessions.
Further NED Special Role sessions have been added to the meeting cycle including;
• Chris Heginbotham’s insight intohis role as Chair of the Mental Health Act Committee
• Gwynne Furlong discussing hisproperty background and involvement with the Trust Property Strategy
• Teresa Whittaker providing afollow up Audit master class
• Peter Ballard furthering the topic
All five of the existing Non-Executive Directors have now presented to the Governors.
The 2014/15 Trust Board meeting dates have been issued to Governors in February 2014 and included on the new Calendar of Meetings. Invites were extended to Governors and all of the places have now been booked. A reserve list is in operation for any governor cancellations to ensure places are distributed fairly
Governors have been involved in the annual planning process with a specific session facilitated by the
Council of Governors Informal Session – “You Said, We Did”
Governor Comment “You Said” Current Provisions “We Do” Future Provisions “We Will” Updated in March 2014
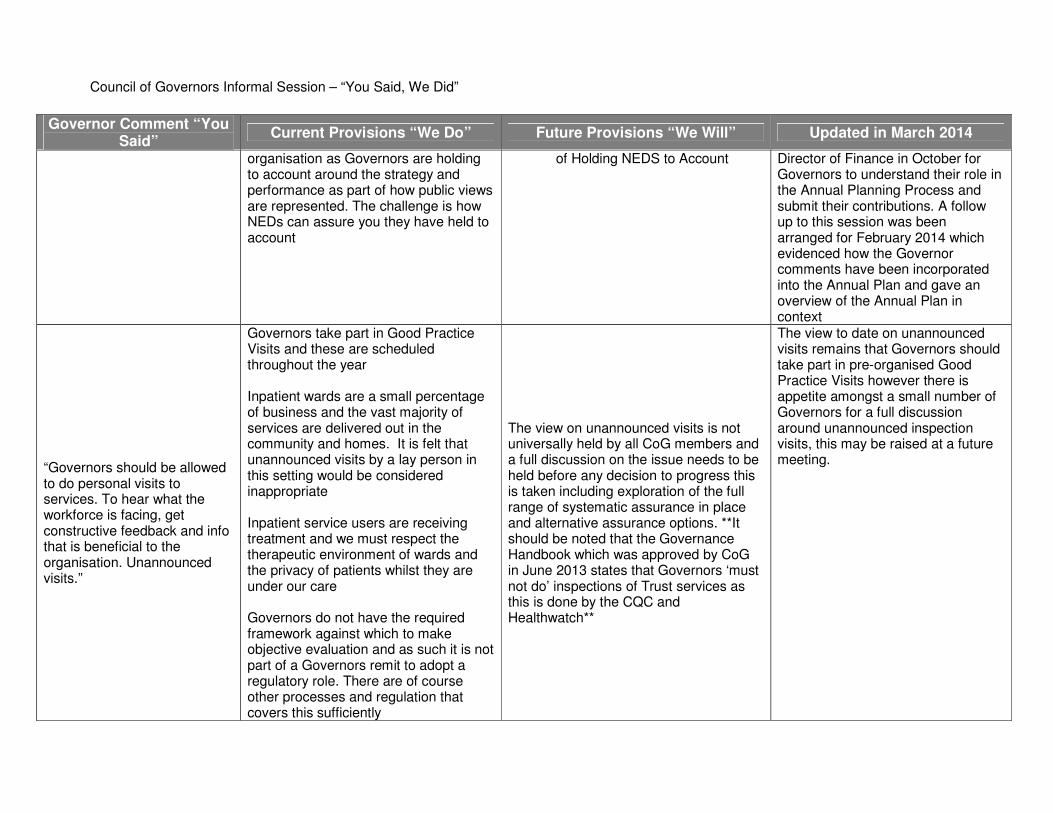
organisation as Governors are holding to account around the strategy and performance as part of how public views are represented. The challenge is how NEDs can assure you they have held to account
of Holding NEDS to Account Director of Finance in October for Governors to understand their role in the Annual Planning Process and submit their contributions. A follow up to this session was been arranged for February 2014 which evidenced how the Governor comments have been incorporated into the Annual Plan and gave an overview of the Annual Plan in context
“Governors should be allowed to do personal visits to services. To hear what the workforce is facing, get constructive feedback and info that is beneficial to the organisation. Unannounced visits.”
Governors take part in Good Practice Visits and these are scheduled throughout the year
Inpatient wards are a small percentage of business and the vast majority of services are delivered out in the community and homes. It is felt that unannounced visits by a lay person in this setting would be considered inappropriate
Inpatient service users are receiving treatment and we must respect the therapeutic environment of wards and the privacy of patients whilst they are under our care
Governors do not have the required framework against which to make objective evaluation and as such it is not part of a Governors remit to adopt a regulatory role. There are of course other processes and regulation that covers this sufficiently
The view on unannounced visits is not universally held by all CoG members and a full discussion on the issue needs to be held before any decision to progress this is taken including exploration of the full range of systematic assurance in place and alternative assurance options. **It should be noted that the Governance Handbook which was approved by CoG in June 2013 states that Governors ‘must not do’ inspections of Trust services as this is done by the CQC and Healthwatch**
The view to date on unannounced visits remains that Governors should take part in pre-organised Good Practice Visits however there is appetite amongst a small number of Governors for a full discussion around unannounced inspection visits, this may be raised at a future meeting.

Council of Governors Informal Session – “You Said, We Did”
Governor Comment “You Said” Current Provisions “We Do” Future Provisions “We Will” Updated in March 2014
In terms of workforce issues, staff wishing to express views have support from Staff Governors and Staff Side Reps as well as the Raising Concerns Policy
“Some Governors feel underutilised. They want to do things and in some cases they have experience and knowledge that is not being used to its full potential”
Explore the options for Governors assessment of interests and skills, and evaluate how Governors could link in with NED areas of interest and introduce ‘critical friends’
Consideration was given to skill sets of Governors and these have been utilised when allocating sub-committee membership for 2014/15. Expressions of interests for Chairing meetings are always welcomed from Governors to enable them to utilise their professional skills and provide potential to be involved in the sub-committees chairs group.
“Acceptance that Governors can’t know everything as there is so much to take in. However it feels that a better view overall in general terms is possible. Mentoring is supportive of this end to a point and needs to be on the right subject”
Review the scope for mentoring when the Guided Conversation is reviewed. Explore the possibility of peer review and an informal mentoring network.
Amendments to the Guided Conversation process have been made following feedback received from previous participants. The management of this tool and process will be taken over by the Company Secretary team in due course which will allow scope to broaden the process into a mentoring relationship between new and current governors
4. Information Streams & Data
“Access to a channel that Governor concerns can be fed into around services, service users, processes etc.”
Governors are able to raise issues informally at any time outside of meetings and they are free to raise concerns within meetings too
The Raising Concerns Policy also applies for Governors and are formally recorded
No update to report, the existing channels for raising concerns remain unchanged.
Council of Governors Informal Session – “You Said, We Did”
Governor Comment “You Said” Current Provisions “We Do” Future Provisions “We Will” Updated in March 2014
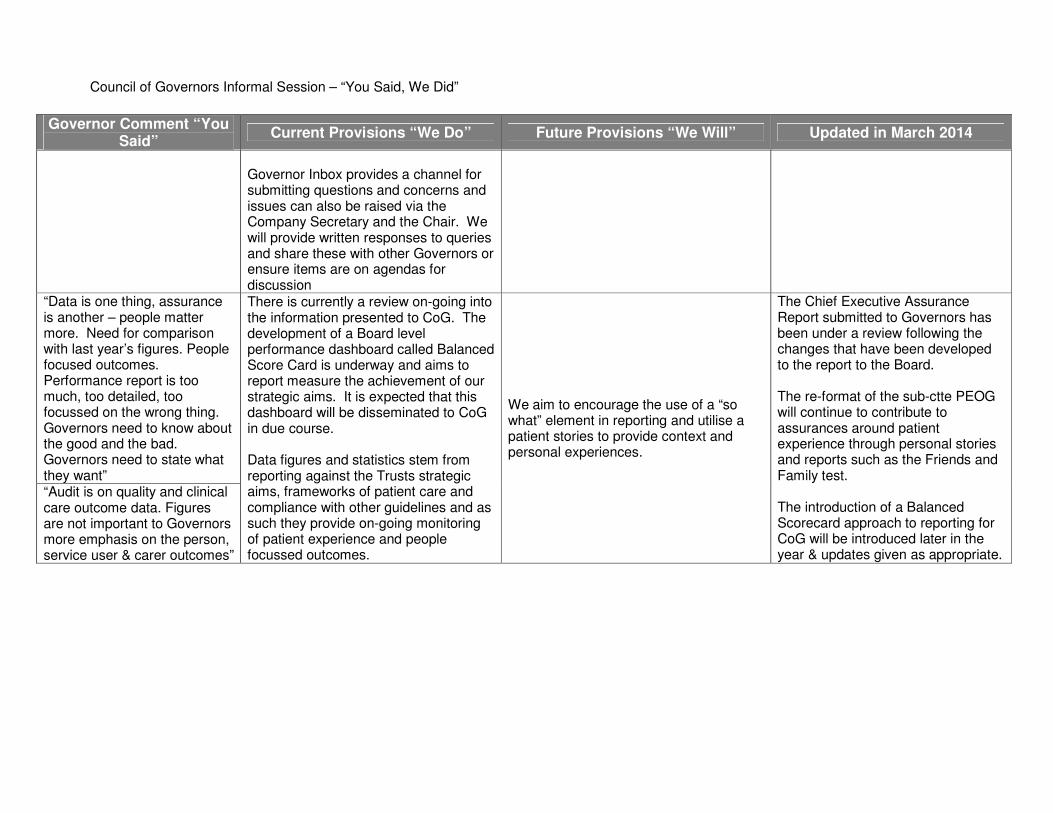
Governor Inbox provides a channel for submitting questions and concerns and issues can also be raised via the Company Secretary and the Chair. We will provide written responses to queries and share these with other Governors or ensure items are on agendas for discussion
“Data is one thing, assurance is another – people matter more. Need for comparison with last year’s figures. People focused outcomes. Performance report is too much, too detailed, too focussed on the wrong thing. Governors need to know about the good and the bad. Governors need to state what they want”
There is currently a review on-going into the information presented to CoG. The development of a Board level performance dashboard called Balanced Score Card is underway and aims to report measure the achievement of our strategic aims. It is expected that this dashboard will be disseminated to CoG in due course.
Data figures and statistics stem from reporting against the Trusts strategic aims, frameworks of patient care and compliance with other guidelines and as such they provide on-going monitoring of patient experience and people focussed outcomes.
We aim to encourage the use of a “so what” element in reporting and utilise a patient stories to provide context and personal experiences.
The Chief Executive Assurance Report submitted to Governors has been under a review following the changes that have been developed to the report to the Board.
The re-format of the sub-ctte PEOG will continue to contribute to assurances around patient experience through personal stories and reports such as the Friends and Family test.
The introduction of a Balanced Scorecard approach to reporting for CoG will be introduced later in the year & updates given as appropriate.
“Audit is on quality and clinical care outcome data. Figures are not important to Governors more emphasis on the person, service user & carer outcomes”
�

AGENDA NUMBER: CG 022/14
COUNCIL OF GOVERNORS – 10 April 2014 CoG & Sub Committee Terms of Reference
FOIA STATUS: No Exemption
PAPER TITLE: Council & Sub-Committee Terms of Reference Review
PURPOSE: The purpose of this report is to provide Governors with the updated Terms of Reference for CoG and its Sub-Committees.
ACTION RECOMMENDED:
Decision
PAPER PREPARED BY: Ashley Christian, Governor Project Support Officer
1.0 BACKGROUND Terms of Reference (ToR) are a document which outlines the purpose and structure of a meeting or committee. It clearly sets out details such as the membership of a meeting, the accepted quoracy levels and also the expected business of the group.
It is good practice to review Terms of Reference annually or when significant changes are made to the meeting or committee.
2.0 REASON FOR REVIEW The Terms of Reference for Council of Governors and two of its four sub-committees have undergone the following minor changes;
• Alterations to the mid-year reporting cycles – ToR now accurately reflect theexpected number of meetings and subsequent committee business
• Alterations to governor membership of committees – ToR set out aminimum number of governor members per committee
• Reduction in overall numbers of governors – quoracy levels have beenamended to reflect the reduction in governor numbers arising out of theEffectiveness Review of CoG.
The updated Terms of Reference have been attached as Appendices A –C, with changes highlighted in red.
The Nomination/Remuneration and Patient Experience Oversight Group Terms of Reference are not subject to this review but are attached as Appendix D & E for information.
3.0 COUNCIL OF GOVERNOR ACTION Governors are required to approve the minor changes to the Terms of Reference.

COUNCIL OF GOVERNORS
TERMS OF REFERENCE
1. AUTHORITYThe Council of Governors is accountable to the membership of Lancashire Care Foundation Trust and is regulated by Monitor as part of the governance arrangements of a Foundation Trust.
2. PURPOSEThe Council of Governors have a distinct role in providing representative and comprehensive governance arrangements in accordance with the Act. The responsibilities of the Governors are set out in the Constitution and in sector guidance published by Monitor. The Council of Governors of Lancashire Care Foundation Trust has developed a framework document which sets out how those duties and responsibilities will be discharged. These terms of reference should be read in conjunction with these source documents.
3. FUNCTIONSThe Council of Governors has the following specific responsibilities:
ESTABLISH • Nominations & Remuneration Committee of the Council of Governors• Such other committees of the Council of Governors as required from time to time• Task and finish working groups as necessary
APPROVE • the policies and procedures for the appointment of the Chair of the Board of
Directors and non-executive directors of the Trust Board on the recommendationof the CoG’s Nominations & Remuneration Committee
• the policies and procedures for the annual appraisal of the Chair of the Board ofDirectors and non-executive directors of the Trust Board on the recommendationof the CoG’s Nominations & Remuneration Committee
• the procedure for the resolution of disputes and concerns between the TrustBoard and the Council of Governors
• procedures leading to the removal of the Chair of the Board of Directors or a non-executive director where necessary
• the appointment or removal of a Chair of the Board on the recommendation of theCoG’s Nominations & Remuneration Committee
• the appointment or removal of a non-executive director on the recommendation ofthe CoG’s Nominations Committee
• changes to the existing levels of remuneration, allowances and other terms ofoffice for the Chair of the Board and other non-executive directors on therecommendation of the CoG’s Remuneration Committee
• the appointment of a proposed candidate as Chief Executive on therecommendation of the Trust Board of Directors
• the criteria for appointing, re-appointing or removing the Auditor• the appointment or re-appointment and the terms of engagement of the Auditor on
the recommendation of the Trust Board Audit Committee• subject to the approval of Monitor, amendments to the Constitution

• subject to changes to the Constitution, amendments to the policy on thecomposition of the Council of Governors, including the representation of keypartner organisations through appointed governor roles
• amendments to the policy on the composition of the non-executive directors onthe recommendation of the Chair of the Board
• the removal from office of a Governor on the recommendation of the Chair of theBoard
• the allocation of members of the CoG’s as representatives on the Quality Cabinetand other relevant executive groups as required.
• the allocation of members to sub committees of the CoG’s• the Membership Engagement Strategy
CONTRIBUTE • to the development of strategic direction providing feedback to the Board of
Directors as appropriate in relation to proposed objectives• to the development of the Annual Plan, acting as critical friend to the Board of
Directors and providing input to into relevant aspects as directed• to the development of the annual report and the processes that underpin the
statements made in the report (e.g. Quality Account/ Standards for Better HealthDeclaration/Code of Governance compliance etc.)
• to the development of stakeholder, including member, understanding of the workof the Trust by seeking out opportunities to deliver the key messages about theTrusts vision and performance to the relevant member constituencies andstakeholder organisations who appoint governors and by acting as ambassadorsin order to raise the profile of the Trust work with the public, other stakeholdersand key influencers
• to the development of the Trusts understanding of user/carer experience byparticipating in programmes and activities designed to evaluate such experience.
• to the development of good working relationships between the Board of Directorsand the CoG’s by meeting regularly with the Board of Directors to establishappropriate channels of communication and a forum for constructive challenge
• by obtaining first-hand knowledge, through opportunities agreed with the ChiefExecutive, of services and environments such as PEAT Good Practice Visitsinspections/Quality Reviews/local activities and events, etc in order to providefeedback to the Board of Directors
• by promoting membership of the Foundation Trust and actively seekingopportunities to recruit members
• to the delivery of the Membership Strategy by participating in the progression ofaction plans underpinning the strategy on the recommendation of the Membership& Governance Committee
• by each governor attending at least two communication events per year plannedto facilitate contact between members and Governors and by ensuring thatopportunities exist to encourage public access to and accountability of Governorsacross all communities and constituencies
• by feeding back outcomes of discussions with members/public/users/carers inrelation to key concerns, good practice and apparent trends
• by co-operating with the Board of Directors, pursuing any requests as ‘criticalfriend’
• by actively seeking out the views of stakeholders and acting as a conduit forinformation to the trust reporting emerging trends (positive and negative) asappropriate
•
RECEIVE ASSURANCE AND HOLD THE BOARD OF DIRECTORS TO ACCOUNT • By receiving the Annual Report of the Audit Committee on the work, fees and
performance of the Auditor • By receiving the Annual Report and Accounts (including Quality Account) and the
report of the Auditor, including a presentation from the board on the financial highlights and key messages
• By receiving the Annual Plan• By monitoring progress against the key milestones in the strategic and annual
plans• By receiving a quarterly report of the Board of Directors on the performance of the
Trust against identified key financial, operational, quality and regulatorycompliance indicators and stated objectives
• By agreeing and keeping under review a schedule of assurance reports to beprovided periodically by the Board of Directors to the CoG’s
• By receiving the Trusts declaration on Standards for Better Health and the reportof the CoG’s Standards Assurance Committee in support of the declaration
• By receiving information about important sector or strategic issues together withthe Board of directors response
• by receiving a stakeholder impact map identifying the risk profile of all majorstakeholders of the Trust
• by receiving quarterly Key Messages reports from the Chairs of the CoG’s subcommittees outlining how their remit has been discharged and highlighting andareas of concern or particular interest
EVALUATE • the effectiveness and efficiency of the CoG’s in the successful discharge of their
responsibilities and achievement of objectives
4. MEETINGSIt is expected that the Council of Governors shall meet formally four times a year. A further four informal meetings are held at which the Council extends an open invitation to Members of the Trust Board to attend the meeting. Two additional meetings per year will be Chief Executive Briefings.
5. MEMBERSHIP AND ATTENDANCEThe determination of the composition of the membership of the Council of Governors is set out in section 9 of the Trust Constitution. The Chair of the Board is the Chair of the Council of Governors.
The Meeting shall be quorate provided that the majority of Governors present are Public Governors.
6. REVIEWThe Council will review its own terms of reference on an annual basis to ensure that it continues to operate effectively.
7. CONDUCT OF COMMITTEE MEETINGSThe Committee shall be supported by the Council of Governors/Membership Support Officer, who will agree the agenda with the Chair, produce all necessary papers, minute meetings, keep a record of matters arising and issues to be carried forward and generally provide support to the Chair and Members of the Committee.
COUNCIL OF GOVERNORS
MEMBERSHIP AND GOVERNANCE COMMITTEE
TERMS OF REFERENCE
1. AUTHORITYThe Committee has delegated authority to act in accordance with these Terms of Reference.
2. PURPOSEThe Membership & Governance Committee (‘the Committee’) is a formal sub-committee of the Council of Governors.
The Committee shall have Terms of Reference and shall seek assurance on behalf of the Council of Governors that seek assurance on behalf of the Council of Governors that the membership of the Trust remains representative of the service users and public served by the Trust and that the Membership Engagement Strategy is being effectively delivered by the Trust. The Committee shall also support the effectiveness and governance of the Council of Governors, making recommendations to the Council of Governors where appropriate.
3. FUNCTIONSThe Committee will:
• Recommend thea Membership Strategy to the Council of Governors for approval• Monitor the effectiveness of the Membership Strategy in sustaining a representative,
stable and engaged membership base• Make recommendations to the Council of Governors when membership should be
denied to individual applicants• Consider the format of the Annual Members’ Meeting and Member Conferences to
ensure they are as relevant as possible and recommend to the Council of Governorsfor approval
• Monitor Governor compliance with the Code of Conduct and Stewardship Code andrecommend corrective action to Council of Governors when issues arise
• Conduct an Annual Review of Council of Governors effectiveness and developproposals for improvements to the Council of Governors
• Oversee the development and training of Governors• Act as the main forum for discussion of issues relating to the Trust’s Constitution as it
relates to the Governors and make recommendations to the Council of Governors
4. MEETINGSIt is expected that the Committee will meet a minimum of 46 times a year in order to fulfil the remit. The work of the Committee will be supported by the Head of Company Secretary Service and Stakeholder Engagement Manager who will progress aspects of the work, as agreed by the Committee, between meetings.
5. MEMBERSHIP AND ATTENDANCEThe membership of the Committee shall consist of a minimum of 78 Governors.
The Committee Meeting shall be quorate provided that 4 members including the Chair and at least 2 Public Governors are present.
6. AGENDAThe agenda will include the following:
• Membership Strategy Updates• Panel Survey Reports• Membership Conferences/Events
The agenda and supporting papers will be sent out to committee members 5 working days prior to the committee, unless authorised by the Chair for exceptional circumstances
7. REPORTING MECHANISMSThe Committee will report to the Council of Governors via the Key Messages document.
8. REVIEWThe Chair and Deputy Chair of the Committee are appointed by the Sub-Committee Chair’s GroupCouncil of Governors and are reviewed on an annual basis. The Chair will be responsible for reporting the recommendations of the Committee to the Council of Governors and preparing a statement and Annual Report in due course.
9. RELATIONSHIPSThe Committee will support the work of the Council of Governors in discharging its statutory duties.
10. CONDUCT OF COMMITTEE MEETINGSThe Committee shall be supported by the Council of Governors/Membership Support OfficerCompany Secretary Service, who will agree the agenda with the Chair, produce all necessary papers, minute meetings, keep a record of matters arising and issues to be carried forward and generally provide support to the Chair and Members of the Committee.
COUNCIL OF GOVERNORS
STANDARDS & ASSURANCE COMMITTEE
TERMS OF REFERENCE
1. AUTHORITYThe Committee has delegated authority to act in accordance with these Terms of Reference.
2. PURPOSEThe Standards & Assurance Committee (“the Committee”) is a formal sub-committee of the Council of Governors.
The Committee shall have Terms of Reference and shall seek assurance on behalf of the Council of Governors that appropriate standards of healthcare are being met by the Trust.
3. FUNCTIONSThe Committee will:
• Review the Trust process for complying with the Care Quality Commission• Identify the nature of the information needs of the Governors in order to effectively
discharge the identified actions, including contextual information about standardsfrom responsible leads
• Explore the sources of assurance that the Council of Governors can draw on to verifyperformance across the whole range of relevant activity
• On the basis of identified risk, undertake a schedule of work aimed at providing highlevel independent verification of the reported outcomes of compliance with standards,and in particular in relation to;-- The identification of good practice examples as well as problems or areas for
improvement - Examples, facts, documentation or anecdotal evidence to back up the points that
the committee wants to highlight
4. MEETINGSIt is expected that the Committee will meet a minimum of 46 times a year in order to fulfil the remit. The work of the Committee will be supported by the Associate Director: Quality & Patient Experience and Head of Quality Improvement & ExperienceProgramme Lead: Clinical Safety and Effectiveness and the Head of Governance who will progress aspects of the work, as agreed by the Committee, between meetings.
5. MEMBERSHIP AND ATTENDANCEThe membership of the Committee shall consist of a minimum of 7 Governors including the Chair.
The Committee Meeting shall be quorate proved that at least 4 members including the Chair and at least 2 Public Governors are present.
6. AGENDAThe agenda will include the following:
• Quality Account

• Good Practice Visit Reports• Quality SEEL Reports
The agenda and supporting papers will be sent out to committee members 5 working days prior to the committee, unless authorised by the Chair for exceptional circumstances
7. REPORTING MECHANISMSThe Committee will report to the Council of Governors via the Key Messages document.
8. REVIEWThe Chair and Deputy Chair of the meeting are appointed by the Council of Governors and are reviewed on an annual basis. The Chair will be responsible for reporting the recommendations of the Committee to the Council of Governors and preparing a statement and Annual Report in due course.
9. RELATIONSHIPSThe Committee will support the work of the Council of Governors in discharging its statutory duties.
10. CONDUCT OF COMMITTEE MEETINGSThe Committee shall be supported by the Company Secretary ServiceCouncil of Governors/Membership Support Officer, who will agree the agenda with the Chair produce all necessary papers, minute meetings, keep a record of matters arising and issues to be carried forward and generally provide support to the Chair and Members of the Committee.

COUNCIL OF GOVERNORS
JOINT NOMINATIONS & REMUNERATION COMMITTEE
TERMS OF REFERENCE
1. AUTHORITYThe Committee is accountable to the Council of Governors and has delegated authority to act in accordance with these Terms of Reference.
2. PURPOSEA Joint Remuneration and Nominations Committee (the Committee) is to be established as a formal committee of the Council of Governors.
The Committee will make recommendations for ratification to the Council of Governors, for the appointment, removal and remuneration, allowances and other terms of office of the Chairman and Non-Executive Directors of the Trust.
3. FUNCTIONSThe Committee will:
• Recommend to the Council of Governors a clear and transparent policy andprocedure for identification and nomination of suitable candidates for the role of Chairof the Board of Directors and other Non-Executive Directors.
• In line with the agreed policy and procedures identify a short list of appointablecandidates and a preferred candidate to fill a vacancy for the post of Chair of theBoard of Directors or Non-Executive Director.
• Provide assurance to the Council of Governors on the process followed in theidentification of appointable candidates and recommendation of a preferred candidatefor appointment to the office of Chair of the Board of Directors or Non-ExecutiveDirector as appropriate.
• If requested by the Council of Governors, investigate and consult widely on thecircumstances leading to a vote of no confidence in the Chair of the Board ofDirectors and produce a full report to the Council of Governors convened for thepurpose of considering the removal of the Chair.
• Recommend and on an annual basis review the level of remuneration andallowances for the Chair and Non-Executive Directors to the Council of Governors.
• Recommend and on an annual basis review the terms and conditions of office of theChair and Non-Executive Directors in accordance with the policy agreed by theCouncil of Governors.
• Recommend and periodically review the procedure for the appraisal of the Chair ofthe Board of Directors and Non-Executive Directors.
4. MEETINGSThe Committee will meet at least annually and then as required to fulfil its responsibilities, as determined by the chairman. Papers will be issued to members at least 7 days prior to the meeting.

5. MEMBERSHIP AND ATTENDANCEAn Appointed Governor will be the Chair of the Committee and the Deputy Chair will be the Chair of the Trust Board.
The Chair of the Committee will be reviewed on an annual basis.
The Chair will be responsible for reporting the recommendations of the Committee to the Council of Governors and preparing a statement and Annual Report in due course
The membership of the Committee shall consist of 4 Public Governors, 1 Staff Governor, 1 Appointed Governor who is the Chair of the Committee and the Chair of the Trust Board.
The Committee Meeting shall be quorate proved that at least 4 members including the Chair and at least 2 Public Governors are present.
6. AGENDAThe agenda and supporting papers will be sent out to committee members 7 days prior to the committee, unless authorised by the Chair for exceptional circumstances
7. REPORTING MECHANISMSThe Chair of the Committee will report on the proceedings of each meeting to the next meeting of the Council of Governors.
The Committee will produce an Annual Report of its activity to the Council of Governors in accordance with the Schedule of Reports outlining how the Committee has discharged its duties under these Terms of Reference.
The Committee will produce an annual Remuneration Committee Report for inclusion in the Trusts Annual Report in the prescribed form.
8. REVIEWThe Chair of the meeting is appointed by the Council of Governors and is reviewed on an annual basis. The Chair will be responsible for reporting the recommendations of the Committee to the Council of Governors and preparing a statement and Annual Report in due course.
9. RELATIONSHIPSThe committee will support the work of the Council of Governors in discharging its statutory duties.
10. CONDUCT OF COMMITTEE MEETINGSThe Committee shall be supported by the Company Secretary who will agree the agenda with the Chair produce all necessary papers, minute meetings, keep a record of matters arising and issues to be carried forward.

PATIENT EXPERIENCE & OVERSIGHT COMMITTEE
TERMS OF REFERENCE
1. AUTHORITYThe Committee has delegated authority to act in accordance with these Termsof Reference.
2. PURPOSEThe Patient Experience & Oversight Group (‘the Committee’) is a formal sub-committee of the Council of Governors.
The Committee shall have Terms of Reference and shall seek assurance onbehalf of the Council of Governors that the duty to engage with the public,including service users and carers, and learn from the patient experience,thereby continuously improving services, is being met by the Trust.
3. FUNCTIONSThe Committee will:
• Listen to the view of service users and carers to help shape the Trust’sservices via reports received and understand how these views areused to improve services.
• Receive updates on any issues raised with the Trust through the LocalInvolvement Networks and Overview and Scrutiny Committees
4. MEETINGSIt is expected that the Committee will meet a minimum of 4 times a year inorder to fulfil the remit. The work of the Committee will be supported by theAssociate Director of Quality & Patient Experience who will progress aspectsof the work, as agreed by the Committee, between meetings.
5. MEMBERSHIP AND ATTENDANCEThe membership of the Committee shall consist of a minimum of 7 Governors.
The Committee Meeting shall be quorate provided that 4 members includingthe Chair of which, at least 2 Public Governors are present.
6. AGENDAThe agenda will include the following:
• Customer Care Report including Complaints & Compliments• Friends & Family Test

• Inpatient Survey Results• PLACE Visit Outcomes• Questions/Comments from Healthwatch and Overview & Scrutiny
Committee• Focused thematic reviews of network service lines in relation to
patient/service-user experience
The agenda and supporting papers will be sent out to committee members 5 working days prior to the committee, unless authorised by the Chair for exceptional circumstances
7. REPORTING MECHANISMSThe Committee will report to the Council of Governors via the Key Messagesdocument.
8. REVIEWThe Chair of the meeting is agreed by the Council of Governors and isreviewed on an annual basis. The Chair will be responsible for reporting therecommendations of the Committee to the Council of Governors and annuallyreporting to the Council of Governors on work undertaken by the Committeeduring the year.
9. RELATIONSHIPSThe Committee will support the work of the Council of Governors indischarging its statutory duties.
10. CONDUCT OF COMMITTEE MEETINGSThe Committee shall be supported by the Council of Governors SupportOfficer, who will agree the agenda with the Chair produce all necessarypapers, minute meetings, keep a record of matters arising and issues to becarried forward and generally provide support to the Chair and Members ofthe Committee.

AGENDA NUMBER: CG 023/14
COUNCIL OF GOVERNORS – 10 April 2014 REVISED PROCEDURE FOR NED APPRAISALS
FOIA STATUS: No Exemption
PAPER TITLE: Revision of the procedure for the appraisal of Non-Executive Directors
PURPOSE: The purpose of this report is to outline the changes made to the procedure
ACTION RECOMMENDED:
Decision
PAPER PREPARED BY: Jo Alker, Acting Assistant Company Secretary
1.0 BACKGROUND At the Council of Governors Joint Nomination/Remuneration Committee held on 19 February 2014, the Trust Chair presented the revised procedure for appraisals of Non-Executive Directors and the supporting documentation that had been updated in light of Governors new duties and the recent changes to the Monitor Code of Governance. The Committee approved the revised procedure and supporting documentation subject to further guidance being developed to align the procedure to the feedback forms in more detail and a review and refresh of definitions and language included in the procedure.
2.0 CHANGES MADE TO THE PROCEDURE At the Council of Governors Joint Nomination/Remuneration Committee held on 18 March 2014, the additional work was undertaken and the procedure was refreshed. The changes included:
2.1 More detail has been provided to the assessment rating definitions; 2.2 The Competency Framework (appendix one to the procedure) is now
aligned to the key competencies and the Trust’s strategic priorities. Where this was detailed in the procedure (points 4.a.i and 4.b.i) has also been updated;
2.3 The experience requirements detailed in the Competency Framework has been reworded to reflect the content of the Non-Executive Director person specification previously approved by the Committee;
2.4 The procedure now details the verbal feedback to be provided by the Trust Chair (and Senior Independent Director in relation to the Chair) on his overall rating of the Non-Executive Directors at the half year point.
The refreshed procedure can be seen at appendix one.

AGENDA NUMBER: CG 023/14
COUNCIL OF GOVERNORS – 10 April 2014 REVISED PROCEDURE FOR NED APPRAISALS
3.0 GUIDANCE FOR GOVERNORS A brief guidance document has been developed for Governors that aligns the feedback questions to the relevant key competencies detailed in the procedure. This guidance can be seen at appendix two.
The Lead Governor will also be offering a presentation that outlines Governors duties as a contributor to the process and how they effectively discharge this duty. The date identified to deliver that presentation is 1 April 2014.
3.0 COUNCIL OF GOVERNOR ACTION The full Council of Governors are asked to approve the refreshed procedure for the appraisal of Non-Executive Directors so that the Governance Handbook can be updated accordingly.

PROCEDURE FOR APPRAISAL OF NON-EXECUTIVE DIRECTORS
1. IntroductionThe NHS Foundation Trust Code of Governance states that the Board of Directors shouldundertake a formal, rigorous annual evaluation of its own performance and of its committeesand of its individual Directors.
The purpose of individual appraisal is to assess whether each member contributes effectivelyand demonstrates commitment.
In line with the requirements of the Foundation Trust Code of Governance the Chief Executivetakes lead responsibility on the appraisal of the Executive Directors.
The Council of Governors has the lead on agreeing a procedure for appraisal of the Chair andNon-Executives with the Chair. The outcomes of the evaluation of both will be reviewed byGovernors with a view to reaching agreement.
The Code also recommends the desirability of using a Senior Independent Director to lead Non-Executive Directors (and the Governors and Chief Executive as appropriate) in the appraisal ofthe Chair.
2. PolicyIt is the policy of Lancashire Care NHS Foundation Trust to ensure regular appraisal of its Boardand of the Board’s constituent members.
This document sets out the framework for that procedure.
The Trust’s Annual Report will state how the required appraisals of the Board, its committeesand individual members have been conducted.
3. Appraisal SchemeThe Trust’s Chair will be responsible for the annual appraisal of all Non-Executive Directors.The Senior Independent Director will undertake the appraisal of the Chair, taking soundingsfrom the Chief Executive, the Board and the Council of Governors. All appraisals will consist ofthree essential elements:
A self-assessment form completed by the individual; An assessment form completed by Board members and Governors; Agreed objectives and personal development plan for the coming year.
Where there are concerns during the year regarding the performance of an individual subject to this procedure, action will be taken to address those concerns at that time independently of this procedure. A procedure for the monitoring and progression of performance improvement which includes provisions relating to; the agreement of an action plan to address areas of poor performance; monitoring and ongoing review arrangements and the consequences of continued poor performance is available separately and should be read in conjunction with this procedure.

Verbal feedback will be provided to the Council of Governors Joint Nomination/Remuneration Committee by the Trust Chair (and the Senior Independent Director in relation to the Chair) on the overall rating of Non-Executive Directors at the half year point.
4. Appraisal Framework
a) Chair
(i) Self-AssessmentThe Chair will undertake a written self-assessment of his/her performance based on the following criteria.
Objectives will be framed each year around the Foundation Trust’s Business Plan in line with the following competencies:
Patient and community focus Strategic direction Holding to account Effective influencing and communication Team working Self-belief and drive Intellectual flexibility
(ii) Evidence The Chair will refer to a range of evidence (e.g., documents, minutes, press releases etc.) Reference should be made to the Competency Framework at Appendix 1.
(iii) Validation The designated Senior Independent Director will review the Chair’s self-assessment and the external evidence taking soundings as appropriate from other Board Directors and Council of Governors.
(iv) Overall Assessment Rating A rating will be discussed with a view to agreement between the Chair and the SID to describe the overall contribution of the individual as set out below:
Outstanding performance Making critically important contribution to the work of the Board and shows detailed evidence against the leadership competencies
Full satisfactory performance Demonstrating the range of skills and qualities required to fulfil the role and shows positive evidence against the leadership competencies
Generally satisfactory performance Satisfactory performance and some evidence against the leadership competencies but room for improvement

Cause for concern Significant number of areas requiring prompt improvement with a lack of evidence provided against the leadership competencies
(v) Scrutiny and Recommendation The self-assessment and review of the Chair’s performance will be scrutinised annually by the Council of Governors Joint Nomination/Remunerations Committee and a report recommended to the Council of Governors by the Senior Independent Director.
b) Non-Executive Directors
(i) Self-AssessmentIndividual Non-Executive Directors will complete a self-assessment of their performance and contribution to the Board of Directors which will be discussed with the Chair.
Performance will be assessed against personal objectives agreed with the Chair in line with the following competencies:
Patient and community focus Strategic direction Holding to account Effective influencing and communication Team working Self-belief and drive Intellectual flexibility
(ii) Evidence The Chair will refer to a range of evidence and reference should be made to the Competency Framework at Appendix 1.
(iii) Chair’s Assessment The Chair will review each individual’s self-assessment and will add to this a personal commentary of his/her own assessment of performance.
(iv) Overall Assessment Rating A rating will be discussed with a view to agreement between Non-Executive Director and the Chair to describe the overall contribution of the individual as set out below:
Outstanding performance Making critically important contribution to the work of the Board and shows detailed evidence against the leadership competencies
Full satisfactory performance Demonstrating the range of skills and qualities required to fulfil the role and shows positive evidence against the leadership competencies

Generally satisfactory performance Satisfactory performance and some evidence against the leadership competencies but room for improvement
Cause for concern Significant number of areas requiring prompt improvement with a lack of evidence provided against the leadership competencies
(v) Scrutiny and Recommendation The Chair will be invited to present a summary of each Non-Executive Director’s appraisal outcome to the Council of Governors Joint Nomination/Remuneration Committee for scrutiny. A report will then be presented to the full membership of the Council of Governors by the Chair of the Council of Governors Joint Nomination/Remunerations Committee.
Where a Non-Executive Director is being considered for re-appointment, the Chair will make a formal recommendation to the Council of Governors Joint Nomination/Remuneration Committee who will take this recommendation into account when making recommendations for re-appointment to the full Council of Governors.
5. ReviewThis framework will be reviewed every 12 months to ensure its effectiveness.

GUIDANCE FOR PREPARATION FOR MEETING WITH APPRAISER
1. OBJECTIVESUsing the headings below you should outline your plans for your personal contribution to theBoard of Directors. These objectives will provide the framework for the discussion with theChair (Senior Independent Director for Chair’s appraisal).
1.1 Strategic direction – LeadershipLead the Trust successfully through the first challenging financial year following the UKrecession bringing together Commissioners, PCTs and other stakeholders through personalnetworking to maintain support for the Service Transformation Programme
[Demonstrated by: Meeting the Trust’s Objectives for the year]
1.2 Holding to account – (Trust Value: Respect and Excellence)Valuing and balancing the interests of all who have a stake in the Trust and what it seeks toachieve
Drive for cost effective and continuous improvement in both the Trust’s results and the way inwhich they are achieved
[Demonstrated by: A proportionate, listening engagement with all who are part of the Trust]
[Demonstrated by: Supporting, challenging and encouraging the Executive Team to increaserecurrent elements in the Cost Improvement Programme]
1.3 Patient and community focus – (Trust Value: Excellence)Establish the rigorous governance required to deliver improved levels of quality and RiskManagement
[Demonstrated by: Focus of the Board and Council of Governors on improving andperformance review of quality, the Care Quality Commission standards and implementation ofthe improved Trust Risk Register]
1.4 Effective influencing and communication – (Trust Value: Accountability)Accepting responsibility for the strategic direction of the Trust, helping it to manage itsreputation
[Demonstrated by: The views of Governors, Members, Partners and other Stakeholders]
1.5 Team working – (Trust Value: Teamwork)Build good relationships with and between the Board, Council of Governors, the Staff andTrust’s stakeholders working collaboratively to achieve the Annual Plan
[Demonstrated by: The culture within the Board, Council of Governors and the organisation]
1.6 Self-belief and drive – (Trust Value: compassion)Develop a broad knowledge and understanding of the challenges facing the Trust’s serviceusers and carers

[Demonstrated by: Empathy with patients, family members and carers]
1.7 Intellectual flexibility – (Trust Value: Integrity) Being open and fair principled in dealing with all
[Demonstrated by: A principled as well as grounded approach to the issues and challenges facing the Trust]

KEY COMPETENCIES FOR THE CHAIR AND NON-EXECUTIVE DIRECTORS
Below are the key competencies for the Chair and Non-Executive Directors to be used as part of the appraisal process. Further detail is provided below and provides the link to the Trust’s strategic priorities.
Patient and community focus A high level of commitment to patients, carers and the community, especially to disadvantaged groups
Strategic direction The ability to think and plan ahead, balancing needs and constraints
Holding to account The ability to accept accountability and probe and challenge constructively
Effective influencing and communication Be able to influence and persuade others
Team working Be committed to working as a team member
Self-belief and drive The motivation to improve NHS performance and confidence to take on challenges
Intellectual flexibility The ability to think clearly and creatively

LCFT STRATEGIC PRIORITIES
KEY SKILLS LEADERSHIP COMPETENCIES EXPERIENCE
Patient and community focus
To provide high quality services
To provide high quality accessible service delivering commissioned outputs and outcomes
Empathy Results focus Digest and analyse
information
Quality Governance - clinical effectiveness and patient outcomes, patient safety, quality of the patient experience Take an active leadership role on quality and a proactive approach to its improvement Actively engage in the delivery of quality improvements by engaging with key
stakeholders and patients Demonstrate an understanding of the current and future risks to quality across LCFT
and the process for escalating and resolving quality performance issues/risks Proactively seeks to review and interrogate complaints and serious untoward incident
data Consider and were appropriate challenge the quality information and data being
presented to the Board to enable sufficient assurance is being provided Place user and carer involvement at the centre of what we do and learn from their
experience to redesign better services
Clinical or medical recent andrelevant experience at asenior level in an acute orcommunity/social careprovider
Experience in clinicalenvironments with a focus onpatient outcome experience
Exposure in clinical decisionmaking or service delivery inthe NHS
Sound knowledge ofgovernance
Ability to understand complexstrategic issues and resolvedifficult problems
Strategic direction
To become recognised for excellence
To provide excellent value for money in a financially sustainable way
Results focus Efficiency Critical information
seeking See the big picture
as well as the detail Communication Self-marketing Strategic
influencing/ politicalastuteness
Seizing the Future – being prepared to take action now to shape and implement a vision for the future development of services Making the most of current opportunities to bring about improvements that are of
benefit to staff, carers or patients Being able to interpret the likely direction of changes in the health service and beyond Using your insights into the board strategic direction of health and social care to help
shape and implement the approaches and culture in the organisation Underpinning the vision and action with a strong focus on local needs Anticipate the harsher financial climate, improving efficiency and the effective use of
resources
Experience of leading complexorganisations
Financialanalysis/management
Audit Private Sector – financial
experience Ability to understand complex
strategic issues and resolvedifficult problems
Sound, independentjudgement
Analytical skills High level understanding of
healthcare issues
Political Astuteness – showing commitment and ability to understand diverse interest groups and power bases within organisations and the wider community and the dynamic between them, so as to lead health services more effectively Understand the climate and culture in your own organisation and in the wider health
and social care environment

LCFT STRATEGIC PRIORITIES
KEY SKILLS LEADERSHIP COMPETENCIES EXPERIENCE
Knowing who the key influencers are, both internally and externally to the organisationand how to go about involving them
Being familiar with health strategy and policy at a national and local level and with theability to plan ahead that takes account of these strategies
Understanding the role of a leader in the health service is now broader than simplybeing responsible for one organisation and that no one organisation in the healthservice can “stand alone”
Remain alert to the changes in the regulatory environment and demonstrate evidence-based improvements in the quality of our services
Political awareness Application of large scale
change management
Holding to account
To provide high quality services
To provide high quality accessible service delivering commissioned outputs and outcomes
Results focus Efficiency Critical information
seeking
Holding to Account – strength of resolve to hold others to account for agreed targets and to be held accountable for delivering a high level of service Setting clear targets and standards for performance and behaviours, ensuring the
processes are in place to support individuals in achieving these standards Insisting upon improved performance if standards are slipping Holding people to account for what they have agreed to deliver e.g. recognising when
performance issues need to be addressed, challenge when performance is below theagreed standard
Being prepared to be held to account by others for what they have contracted you todo as the leader
Experience of leading complexorganisations
Financialanalysis/management
Audit Private Sector – financial
experience Understanding of the duties as
a non-executive director Experience of service
redesign Clinical or medical recent and
relevant experience at asenior level in an acute orcommunity/social careprovider
Experience in clinicalenvironments with a focus onpatient outcome experience
Exposure in clinical decisionmaking or service delivery inthe NHS
Experience of services asuser/carer
Broad Scanning – taking the time to gather information from a wide range of sources Making it a priority to know about how services are being delivered and what the
experience is of patients and users on the ground. Being persistent in getting the key facts of a situation. Having systematic ways of informing yourself about key developments
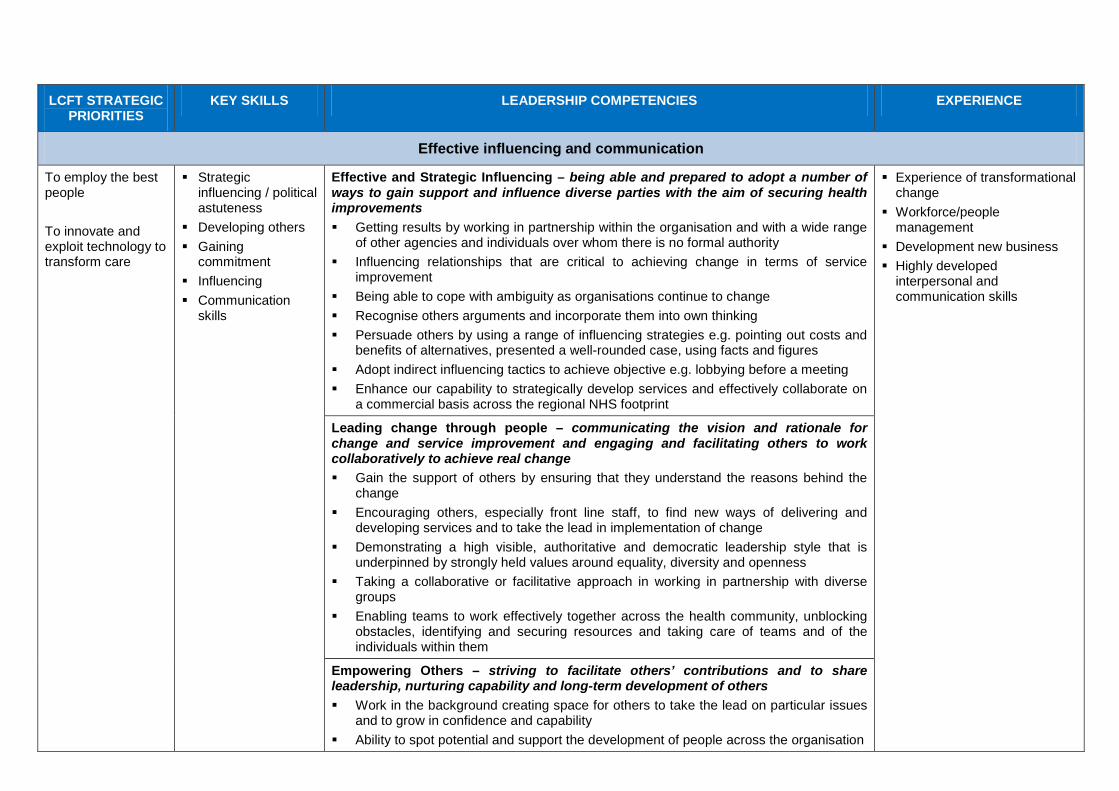
LCFT STRATEGIC PRIORITIES
KEY SKILLS LEADERSHIP COMPETENCIES EXPERIENCE
Effective influencing and communication
To employ the best people
To innovate and exploit technology to transform care
Strategicinfluencing / politicalastuteness
Developing others Gaining
commitment Influencing Communication
skills
Effective and Strategic Influencing – being able and prepared to adopt a number of ways to gain support and influence diverse parties with the aim of securing health improvements Getting results by working in partnership within the organisation and with a wide range
of other agencies and individuals over whom there is no formal authority Influencing relationships that are critical to achieving change in terms of service
improvement Being able to cope with ambiguity as organisations continue to change Recognise others arguments and incorporate them into own thinking Persuade others by using a range of influencing strategies e.g. pointing out costs and
benefits of alternatives, presented a well-rounded case, using facts and figures Adopt indirect influencing tactics to achieve objective e.g. lobbying before a meeting Enhance our capability to strategically develop services and effectively collaborate on
a commercial basis across the regional NHS footprint
Experience of transformationalchange
Workforce/peoplemanagement
Development new business Highly developed
interpersonal andcommunication skills
Leading change through people – communicating the vision and rationale for change and service improvement and engaging and facilitating others to work collaboratively to achieve real change Gain the support of others by ensuring that they understand the reasons behind the
change Encouraging others, especially front line staff, to find new ways of delivering and
developing services and to take the lead in implementation of change Demonstrating a high visible, authoritative and democratic leadership style that is
underpinned by strongly held values around equality, diversity and openness Taking a collaborative or facilitative approach in working in partnership with diverse
groups Enabling teams to work effectively together across the health community, unblocking
obstacles, identifying and securing resources and taking care of teams and of the individuals within them
Empowering Others – striving to facilitate others’ contributions and to share leadership, nurturing capability and long-term development of others Work in the background creating space for others to take the lead on particular issues
and to grow in confidence and capability Ability to spot potential and support the development of people across the organisation

LCFT STRATEGIC PRIORITIES
KEY SKILLS LEADERSHIP COMPETENCIES EXPERIENCE
Fostering the development of others across the health community so that healthimprovement and service development agendas can be developed and owned
Help others to learn from their mistakes in a non-critical setting
Team working
To become recognised for excellence
To provide excellent value for money in a financially sustainable way
Respectful Understanding
NED/Execboundaries
Ability to shareknowledge andexperience
Collaborative Working – being committed to working and engaging constructively with internal and external stakeholders Understanding and being sensitive to diverse viewpoints. Strive to create the conditions for successful partnership working. Consult with others when appropriate. Demonstrates a commitment to common goals. Makes a point of viewing things from other people’s perspectives.
Commit sufficient time to fulfilthe role
Commitment to the Trustsvalues
Management experience Contract negotiation Relationship management Financial management Acquisitions/mergers
Self-belief and drive
To provide high quality services
Results Focus Efficiency Critical Information
seeking Strategic
Influencing /Political Astuteness
Team Working Developing Others Gaining
commitment Flexibility Self-presentation Tenacity Personal integrity Self-control Self-awareness
Drive for Results – strong commitment to making service performance improvements and a determination to achieve positive service outcomes for users Determination to meet objectives set by others Able to focus on the priorities that are urgent and most important Focus on what really makes a difference, rather than being constrained by methods
that were used in the past Actively seek out opportunities to improve delivery of service through partnership and
new ways of working
Experience of leading complexorganisations
Financialanalysis/management
Audit Private Sector – financial
experience Experience of transformational
change Workforce/people
management Development new business Management experience Contract negotiation Relationship management Financial management Acquisitions/mergers
Drive for Improvement – deep motivation to improve in the health service and thereby to make a real difference to others’ health and quality of life Stays focused on the goal of the service improvement and resist being side tracked Focused on achievements of goals for the greater good of others and not own
reputation Work with key stakeholders inside and outside of the organisation to achieve positive
outcomes
Self-Belief – confidence that you will succeed and can overcome obstacles to achieve the best outcomes for service improvement

LCFT STRATEGIC PRIORITIES
KEY SKILLS LEADERSHIP COMPETENCIES EXPERIENCE
Communication Relish a challenge Being prepared to stand up for what you believe in
Intellectual flexibility
To innovate and exploit technology to transform care To employ the best people
Customer focus Gaining
commitment Initiative Self-marketing
Intellectual Flexibility – the facility to embrace and cut through ambiguity and complexity and to be open to creativity in leading and developing services Consider information from a wide range of sources when taking decisions Prepared to consider new information or alternative views that differ from own when
reaching conclusions See’s patterns and trends in information Able to see the bigger picture Delve into detail and looks for models and examples of how organisations work to
inform decision making Leverage our competitive strength to use our asset base to invest in quality
Performance management Stakeholder management Talent management Service development

GUIDANCE FOR GOVERNORS ON COMPLETING NON-EXECUTIVE DIRECTOR APPRAISAL FEEDBACK
Introduction This guidance provides a brief outline of the areas that Governors should consider when completing appraisal feedback for a Non-Executive Director. It should be read in conjunction with the procedure for appraisal of Chair and Non-Executive Directors.
Competency Framework There are seven key competencies that make up the Competency Framework which are:
1. Patient and community focus2. Strategic direction3. Holding to account4. Effective influencing and communication5. Team working6. Self-belief and drive7. Intellectual flexibility
The Competency Framework seeks to provide Governors with positive tasks that should be identifiable in Non-Executive Directors interactions and activity under each of the seven key competencies. The Competency Framework does this by aligning the seven key competencies to the Trust’s strategic priorities and identifying key skills and experience required to fulfil each of the positive tasks. The experience requirements are aligned to the Non-Executive Directors person specification.
This Competency Framework is appendix one to the procedure for appraisal for Chair and Non-Executive Directors which is attached to this guidance.
Feedback Questions This section identifies the key competencies to be considered under each question on the Governor Feedback form.
Question Key competency to be considered
1. During 2013/14 how has the NED contributed to the Trust achievingits outcomes by improving its performance? Strategically as a member of the Board Informal contributions Participation in other activities
2, 5, 6, 7
2. Can you give examples of how the Trust’s values of Teamwork;Accountability; Excellence; Integrity; Compassion and Respect have been demonstrated by the NED?
1, 3, 4, 5, 6
3. How has the NED helped ensure a focus upon quality in all that theTrust does? 1, 2, 3

Question Key competency to be considered
4. What special contribution can you highlight in support of the NEDsrole as critical friend aligned to Executives/Sub-Committees? 1, 5, 7
5. Are there any other specific areas where you feel the NED haspersonally made a special contribution?
6. How has the NED contributed to building constructive butchallenging relationships within the Trust and held the organisation to account for its performance?
3, 4
7. How has the NED contributed to building positive relationships withGovernors and other stakeholders? 5
Further Guidance A pack of evidence material will be produced for Governors providing feedback which will remind or prompt Governors of the work undertaken by the relevant Non-Executive Director throughout the year. This will include the Non-Executive Directors committee membership and copies of presentations delivered for Governors.
The Lead Governor will be delivering a presentation that will outline the role of a Governor in the appraisal process and how this duty should be effectively discharged.

AGENDA NUMBER: CG 024/14
COUNCIL OF GOVERNORS – 10 April 2014 Governor Training Programme
FOIA STATUS: No Exemption
PAPER TITLE: Governor Training Programme 2014/15
PURPOSE: To provide the Council with a Governor Training Programme linked to Health & Social Care Act duties.
ACTION RECOMMENDED:
Decision
PAPER PREPARED BY: Ashley Christian, Governor Project Support Officer
1.0 BACKGROUND Ensuring Foundation Trust (FT) Governors are equipped to fulfil the governor duties set out by the Health & Social Care Act 2012 is a key topic of discussion amongst Foundation Trusts in the North West.
Governors were updated last year about the potential for development of a regional training programme that if successful, would be rolled out for Governors of FTs across the North West.
The development stage of the training and development programme has now been completed and the attached schedule sets out a Governor Development and Training Programme for consideration by the Council of Governors.
2.0 GOVERNOR TRAINING & DEVELOPMENT PROGRAMME 2014/15 Developed in conjunction with the North West Company Secretaries Forum, the Governor Training & Development programme has been carefully considered to equip governors with the knowledge and skills to enable them to discharge their statutory duties including those additional duties set out in the Health and Social care Act 2012.
The training programme attached at Appendix A has two aspects; standardised governor training modules; and bespoke training sessions.
The intended roll out of this regional programme across the North West was deferred earlier this year due to ongoing conversations between the North West Company Secretary Forum and the NHS Leadership Academy which could potentially bring additional training resource and funding to enable the training programme to be fully embedded across the region.
Despite this delay, Lancashire Care has chosen to implement the Training & Development Programme at a local level to ensure governors have access to
AGENDA NUMBER: CG 024/14
COUNCIL OF GOVERNORS – 10 April 2014 Governor Training Programme
high quality, relevant training and as such adjustments have been made to the programme to ensure it is fully tailored to LCFT Governor requirements.
Lancashire Care will continue to support the development of the regional training programme and ensure Governors are kept up to date with future developments as appropriate.
3.0 COUNCIL OF GOVERNOR ACTION The Council of Governors are asked to approve the Governor Training and Development Programme 2014/15 for implementation.

�����������
�
�
NORTH WEST GOVERNOR TRAINING & DEVELOPMENT PROGRAMME
�� � �������� ��� ����������� ������ �� ���
���� ��� ����� ���� � ��
�
����� ��� ��������� � ���� �����! ! ���
• � ������� ��� ��� ����������
• � ������� ���������������������� �� �
• � ���� � ��� � ��� � �������� �� � ���� �������� �� �� ���� �������� ����!"� ������
�� ��� ��������������������# ������� ��������� ������$��
• ������������%�& �����'�( ������������������������� �
• ��������!�����) ��������(���� �*�+��������������� ���� ���%)�,-.,�
• /������ ����0 �� �� ��������1� �����������!2�
• 0 �������!�����+���������3��������� ��4�
• %���������&������� ������������
• 5�!�(��� ��
• &��������%�� � ���������� ���6��������
• &��������1�����7�� ������6� �������������
• %������%��������
• (�������������+����� � �
• 0 ��������%�����
• 5�!�0 �� �� ����� ����%������ �
• (�!����(�!���������
o /$��� � �1����������������� �
o &��������+( �'�����
�
�"��� �� ��#������$� ���� � ���� ����%��
+������������������+���������1������ � �"�&������� � �����������������+���������1����
� ������ ��������������������� ���8�
�
• &�������������� ����
• 9������������!�(���� �*�)�6��������&�������� ����������������� ��&������� ��
• %������&����������
• ��� ��%�� ����������
• 5�!�(��� ����&������� �
• &������� �%������ ��
• &������� �%������%�������
• (�������������+����� � ����� �
• /$��� � ����� �����/$��� � �1���������
• &��������%�� � ���������� ���6��������
�
�
�
�
�
�

�����������
�
�
������� ������� ���
�
&��� '����$� ����#��� ��'��� �#��#� �( ���� ����� ��)���$�#��! � ���*+�#����,-�
• �������� �������&�������� ��������������� �������������)������1���2�
• ��� ����� ����� �� &�������� � ����� � ���� ��� ��� � � ������ ���� �� ����������
�������� �������:���� ��������3� ��������������� ���������������������������
�����������4�
• ��� �$������ ��� � &������� � ���� ������� ��������!� � ���� ���� '����� ��
(������� ������ �� �� ��������� ����� ������� ������������)������1��������
������������������ ��� � �
�
.��� +�#�� ��������� �/���� � ��0����� ��"�#��,�( ��'�##� ���*+�#����,-��
• ��� ����� ����� ���� ����"� ���������� ��!� �������� "� �� &������� � ���� ���
/$��������(������� ��
• ��� �$������ ���� �������� �� :�������� ��� ��������"� ���� ��� � ��� ������ � ���
&������� �
• ���������!�� ���� :��������������������� ��� ���� ��������"����� ����� ����� �
������ ������&������� ������� ������� ������������ ��� ��� � ����!�
• /$������&���������������� ����!����������� ��� �� �� ���2�
• ������������ ������ ������������!"���� ����� ;������"�<�� �������������������
��� ���������!� �������� � ��������� �� �������� � ����� "� ��������� ����
���������7��� ����
• '�������� �= ������ � � ���������������� �������� �������
• ���������!���!����� ��� ��������;����� �������� ��������� ����� ������
�
1��� �� �$� ��� ����! � ��( ���� ����� �� � ���! � ��*+�#����,-��
• �������� �����>� �������������!� ���������� ������� ���������������� �?@�
• ����$��������!��������������� �������� ���������0 ���������<����� ������
������� ���������� �� �� ���2�
• ������������� ��������� � ����������������������� ���� 2�
• ���������!���������� ����� ���������� ����������� ����!����� ����������
������������
• ��� �$������ ��� � &������� � ���� :����� ����� ���� ���� � ���� ������ � � ��
����� �������� ;������"� ��������������������� �!�
�
2��� ��+��)�)� � ���( �3 �#��,/������� ��������� ������$� ���*) ##���,-��
�� ���������� ����� ���������������� �� ���������� ���
• ��� ����� ����� ���� �������!� ���!� ��� �� � ����� ��� �������� ��� �������
������� ���� ������� "� � � �� � ���� � �!� �� �� ��������� �������� ����!� ���
� �� �� "���$��!�� ����� �������� �� ���� ��� ��� �������� ����� ���!�
• ��� ����� ����� ���� ��!� ���� ��� � �� ��� ��� )������ "� ��!� ��������� � ��
�������������������� �����������!����� �����$���������� !�&������� �
• ��� ������ � ���� ����� � �� ���� ���� ���� ��� � ��� ���������� ��!� � �������
����� ��
• ��� �$������ ���� &�������� ����� ��� ������ ���� ���� A �����!� )������� ���� ����
�� �����������A �����!�
• 5�!� ���� �������� ����������������������*�� ����&������� ������������������

�����������
�
�
4���� 5�������� ���
�
6�� � ����� �� ��� ����( ��'����#������'���7�� �#�� �����*+�#����,-�
• ����$������������� ��������������)������ ������������� ��
• ������� ���$� ��������� �����������������)�����%�� � ������
• ����$���������������������/$�������)�������
• (� �� �����&�������������������������������/$�������)�������
�
8�� � � ��� ��( ��$���� ���� �#��������� ������*+�#����,-�
• )�� ������� ����!���� ����������� "������������!�� ������ �
• �������� ��������������������� ��� ����������������������
• ��� �$������ � �! � �� ��������� ���� � �������� ������� � ��� ���� ����� ��
���������= � �������� �� ����� ���
�

�

AGENDA NUMBER: CG 026/14
FOIA STATUS: Part Document Exempt Part exemption applies to page/s: Appendix 1
Not Applicable
PAPER TITLE: Chief Executive Assurance Report
PURPOSE: To purpose of this report is to provide an overall summary of Trust performance.
ACTION RECOMMENDED:
Noting
PAPER PREPARED BY: Heather Tierney-Moore, Chief Executive
PERFORMANCE
Performance Dashboard The Trust Performance Dashboard for February 2014 can be found in Appendix 1.
Quality and Performance The Board’s attention is drawn specifically to the following:
Workforce and Culture The monthly sickness figures have decreased slightly from 6.09% in January to 6.01% in February. The increase last month caused the year-to-date sickness figures to rise from 5.31% in January to 5.35% in February, it is likely the annual figure at the end of March will not achieve the 5% target.
Finance and Business The trend in financial performance is improving with the Trust performing only slightly below plan, with a year to date surplus of £3.65m with the projected outturn has recovered to be in excess of the plan of £4.0m at £4.2m surplus.
The CIP performance of £1.1m below plan is a little off track with a projected outturn of £9.75m against a raw plan of £11.0m, though we are achieving a position that is better than the Risk Adjusted Plan (£9.1m for the full year).
The financial position has allowed cash balances continue to hold up strongly (£31.5m v plan £19m) and the forecast outturn (£19.5m v plan £19.7m) will produce acceptable financial risk ratings for the year under both Financial Risk Rating (3 v plan 3) and Continuity of Services Risk Rating (4 v plan 4) bases.
The main driver of underperformance is within mental health inpatients. There are overall pressures of £3.7m year to date, projected to be £4.1m for the full year. These figures are allowed for in the overall position, implying mitigation of more than £4.3m for the full year, mainly from non-recurrent commissioner funds and unutilised reserves.

AGENDA NUMBER: CG 026/14
The position has been discussed with Monitor as part of the regular quarterly review and they recognise that the Trust is seeking to support the stability of the Lancashire health economy in managing demand issues.
Financial budgets for 2014/15 have been set. These are consistent with the figures in the Annual Plan submitted to Monitor. It is expected that delivery of this position will achieve a £4.1m surplus with a Continuity of Services risk rating of 4. The figures assume inflationary provision of £9.7m, internal pressures of £7.1m and cost improvement programmes amounting to £13.6m.
Red Rose Property Services Management Agreement The Trust is proposing to sign two contracts that set out future working arrangements with our joint venture partnership RRCS as explained at last month’s CoG meeting. These 2 contracts will replace the current interim management arrangements when enacted.
• Red Rose Property Services Management Agreement. This contract describes howProperty Services Management is to be transacted in the future with the service provision isplanned to commence on 1st May 2014.
• Capital Project and Feasibility Works Management Services Agreement. This contractdescribes how the Trust may choose to transact future capital project works with RRCS.Any significant capital project would come to the Trust for approval in the form of abusiness proposal and subsequently a business case.
Annual Plan The Operational Plan for 2014/16 was submitted to Monitor on 4th April 2014. The completion of the financial template that accompanies the Operational Plan reflected the financial position set out in the Acting Director of Finance’s report to the Board. The financial template also includes a declaration of compliance with key targets and indicators. A risk to compliance with the delayed transfers of care target has been declared as part of the submission in addition to acknowledging the moderate concerns raised by CQC following the routine visit to the ABI unit.
As part of the annual planning timetable, the corporate governance statement will be submitted at the end of June, alongside the five year strategic plan. The Phase 2 submission will focus on Strategic planning and sustainability and will be informed by the refresh of the Trust’s strategy.
The Board and Council of Governors received presentations from the Director of Workforce, Innovation and Transformation in March 2014 on the key planning assumptions together with the draft plan. The Board approved the Plan on 01 April 2014.
The Operational Plan will be published online; Governors will be signposted to the web link outside of the meeting to access and review the Plan.
Contracts and Performance The demand for out of area beds increased to 33 at the end of February. Pressure on beds within the Adult Mental Health network increased showing occupied bed days at 101.49%, from 99.27% in January. Average length of stay in February had a slight decrease this month to 31.98 days, from the previous month of 32.68 days, still exceeding the 30 day target.

AGENDA NUMBER: CG 026/14
The occupied bed days for Older Adults decreased for February to 61.71%, from 66.35% in January and 75.51% in December. Work continues to support effective bed management and discharge planning. The average length of stay on discharge for the network increased significantly to 81.12 days from 57.12 days in January. This increase reflects the discharge of long stay patients, where the number of bed days for their total length of stay is included in the monthly discharge figures.
Advancing Quality for Dementia achieved a good monthly position of 80.25% for January against the target of 76.69%. However the annual figure for this indicator predicts a fail against target. The Dementia indicator is comprised of 7 measures (assessments), which must be completed with a particular timeframe. Each of the assessments required certain data items to be recorded for it to count towards a pass. On initial investigation, it would appear that although assessments are taking place, they are not always completed with the required timescales and therefore do not count towards the target. This will be addressed as part of the Performance Strategy and improvement plan.
Quality, Compliance and Innovation 7-Day follow-up continues to achieve the 95% target, at 96.8% for February, reflecting the on-going work to proactively follow-up patients. The reported failure against CPA 12 month reviews at Q3 has now been completely validated, and the Trust actually passed Q3 (and Q1 and Q2) against the revised definition for this indicator.
Delayed Transfers of Care continue to present issues, currently running at 10.9% in Q4 against the 7.5% threshold. Active work is ongoing to bring performance into line with expectations. This will involve improving the data quality used for reporting, active management of current delays, and better planning of discharges to prevent delays occurring. It is estimated that performance will be back to the 7.5% threshold in Q1 or Q2.
External Performance and Data Quality Review The Chief Executive commissioned a data quality review which was conducted by KPMG. The 3 key objectives were:
• Overall assessment of performance reporting function• Risk assessment of performance indicators• Sampling of performance indicators
Six elements of performance function were reviewed (strategy, people, governance, systems and processes, reporting and technology).
The report shows the overall conclusion on risk for a range of indicators as an assessment of the risk of misstatement through poor data quality, not of failure to achieve the target and detailed results can be found in the report.
The review recommended proposed sampling largely from the higher risk indicators to provide some assurance around data quality to Board. The proposed sampling would be biased particularly towards indicators for which no external assurance is currently available and the sampling approach could mirror that used for mandated Quality Accounts indicators. Recommendation also included conducting high level analysis of the year’s total results to analyse any trends and characteristics of the datasets that may suggest risk. This work is now underway by KPMG.

AGENDA NUMBER: CG 026/14
The draft findings have identified significant concerns with the current performance function of the Trust as expected. This is reflected in the rating of four of the elements as Inadequate, and two elements as requires Improvement. �
All the recommendations have been agreed and are in the process of being actioned. A Performance and Data Quality Strategy has been developed by the Interim Performance Director and will be implemented in partnership with Executive Directors to address each of the thematic areas identified. The final report including the outcome of the data sampling and progress in addressing any shortfalls will be presented to the Board in June and also shared with Council of Governors.

AGENDA NUMBER: CG 026/14
APPENDIX 1

�

AGENDA NUMBER: CG 027/14
COUNCIL OF GOVERNORS – 10 April 2014 Quarterly Workforce Report
FOIA STATUS: No Exemption Part exemption applies to page/s:
Not Applicable
PAPER TITLE: Quarterly Workforce Report
PURPOSE: To provide CoG members with an update on workforce activity for Quarter 3
ACTION RECOMMENDED:
Noting
PAPER PREPARED BY: Craig Barratt, Director of Workforce, Innovation and Transformation
1.0 EXECUTIVE SUMMARY The attached scorecard is provided to inform CoG members updated on the Workforce Directorate.
2.0 INTRODUCTION The Workforce report provides an update in four areas:
o Workforce Capacityo Leadership & Qualityo Engagement & Wellbeingo Employee Relations
Quarter 4 will have an enhanced section on Equality and Diversity.
Workforce capacity remains stable this quarter with a small increase in agency usage reflecting the winter period. Headcount is also stable as is sickness absence. Mandatory training compliance has dropped below the 85% threshold in 4 areas. The target for flu vaccination for frontline staff was exceeded and there has been an overall increase in staff engagement.
3.0 RECOMMENDATION The Council is asked to note the content of the Quarter 3 Workforce report.

LCFT Workforce Scorecard Report October to December 2013

This document has been created to allow the Trust Board and senior management to make informed decisions on workforce needs in the future.
The document is split into four sections, Workforce Capacity, Leadership & Quality, Engagement & Wellbeing and Employee Relations and will allow exploration of trends, highlighting risks and identifying opportunities for action.
Where not otherwise indicated the data is as at the end of the quarter.
Workforce at a Glance
(WAG)
Workforce Capacity
Leadership & Quality
Engagement & Wellbeing
Employee Relations
REPORT OF KEY WORKFORCE METRICS TO SUPPORT TRUST BUSINESS OBJECTIVES
LCFT Workforce Scorecard October to December 2013

WORKFORCE CAPACITY
LEADERSHIP & QUALITY
ENGAGEMENT & WELLBEING
EMPLOYEE RELATIONS
Bank & Agency | Capacity | Headcount /Turnover | Redundancies & Redeployments | Wellness Presence |
Sickness Absence | Equality Delivery System
Appreciative Leadership | Aspiring Leaders | Mandatory Training | Safety | Induction | e-PDR | Staff Survey - Leadership
Sickness Absence (Top 3 Reasons) | Flu Vaccinations | Overall Staff Engagement Questions/Score | PDR Engagement Scores
Formal Action | Number of Live Suspensions by Network | Risk Level of Current Employee Relations Cases Split by Type |
Number of Formal Absence Cases (with Workforce Support) by Network
CONTENTS
LCFT Workforce Scorecard October to December 2013

WORKFORCE CAPACITY
LCFT Workforce Scorecard October to December 2013

Bank and Agency
The charts below show % shifts filled by the Temporary Staffing team.
The charts below show numbers of shifts filled by qualified/unqualified temporary staff.
WORKFORCE CAPACITY
LCFT Workforce Scorecard October to December 2013
2013 Q4 2014 Q1 2014 Q2 2014 Q3
Agency Filled 18% 20% 18% 23%
Bank Filled 75% 76% 76% 69%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
The charts below show average fill percentage per quarter.
1355 4716
2013 10
Qualified Unqualified
1887 6134
2013 11
1692
6622
2013 12
21%
73%
6%
2013 10
Agency Filled Bank Filled Not Filled
23%
71%
6%
2013 11
22%
74%
4%
2013 12
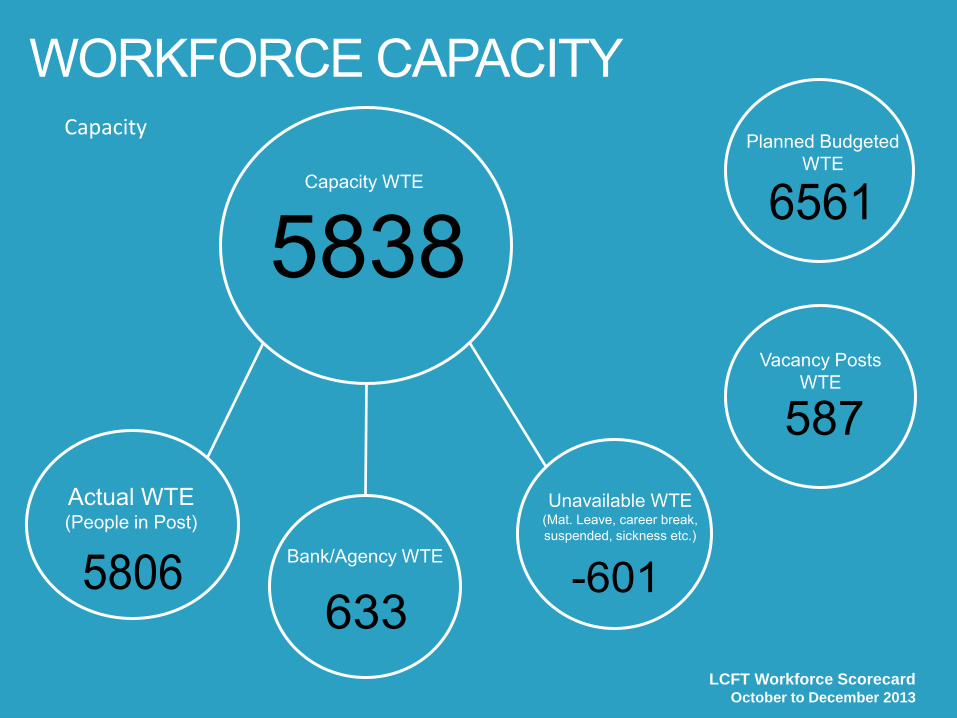
Capacity
WORKFORCE CAPACITY
LCFT Workforce Scorecard October to December 2013
Unavailable WTE (Mat. Leave, career break, suspended, sickness etc.)
-601
Actual WTE (People in Post)
5806
Planned Budgeted WTE
65615838Capacity WTE
Vacancy Posts WTE
587
Bank/Agency WTE
633

Headcount /Turnover Redundancies & Redeployments
WORKFORCE CAPACITY
LCFT Workforce Scorecard October to December 2013
2013 10 2013 11 2013 12
Redundancies 2 4 5
Redeployments 9 9 45
0
5
10
15
20
25
30
35
40
45
50
2013 10 2013 11 2013 12
Ave Mthly HC 6,631 6,619 6,676
Ave Mthly WTE 5,886 5,879 5,925
Turnover 10.29% 10.14% 10.07%
0.00%
2.00%
4.00%
6.00%
8.00%
10.00%
12.00%
0
1,000
2,000
3,000
4,000
5,000
6,000
7,000
8,000

Wellness Presence
WORKFORCE CAPACITY
LCFT Workforce Scorecard October to December 2013
2013 Q3
94.35%2012 Q3
94.11%

Sickness Absence
WORKFORCE CAPACITY
Episodes SICKNESS ABSENCE
SHORT TERM LONG TERM
FTE Days Lost
Episodes
FTE Days Lost
LCFT Workforce Scorecard October to December 2013
2,824
10,381
546
20,365

LCFT Workforce Scorecard October to September 2013
WORKFORCE CAPACITY Equality Delivery System (EDS) – Opportunity Knocks Event November 2014
Scrutiny of EDS Goals 3 and 4

Why have we included this data?THESE FIGURES RELATE TO A TRADITIONAL DATA SET. CAPACITY AND ACTUAL USAGE GIVE AN INDICATOR OF WHERE TEMPORARY STAFFING IS USED TO DELIVER FLEXIBILITY OF THE WORKFORCE.
FUTURE DEVELOPMENTS WILL INCLUDE A WIDER VARIETY OF DATA RELATING TO EQUALITY AND DIVERSITY.
What is this telling us?
•The gap between establishment and capacity and corresponding use of temporary staffing is relatively constant. Much of this is accounted for byroles under advertisement. Anecdotal evidence suggests, the small proportion of other roles remains vacant for a variety of reasons such as holding posts to meet CIPs, flexible resourcing to cover sickness absence, pending restructures etc. •There is no correlation between sickness absence rates and bank usage and the highest reported reason for bank usage remains acuity.•There has been a slight % increase in agency use in favour of bank use in Q3. This reflects the month on month increase in requests for bank staff(over 4000 more in Q3 than Q1) as well as an expected seasonal fluctuation. •When we have insufficient bank resource available, requestors are given the option of using unqualified bank staff or using an agency. Agency usemay be appropriate as a last resort to ensure high quality patient care and safety. The more quality staff we recruit to the bank, the fewer expensive, agency workers will be required. •Scrutiny of EDS Goals 3 and 4 show improvement in four of the nine areas with three rated ‘excellent’, five ‘achieving’ and only one ‘developing’.
What’s new?
•Resource has been dedicated to specialist bank recruitment campaigns which have now been run for all inpatient units with the exception of CAMS,which is to follow. We anticipate a consequential reduction in agency use when compared with bank use in Q4. •Vacancy approval process has been amended to allow managers to recruit above establishment when appropriate.•Engagement with Health Education England to collaborate on workforce planning initiative.
What else should we do about it? •Increase use of specialist recruitment campaigns to expand the bank and reduce reliance on agency workers.•Review use of volunteers and promote the valuable contribution they can make.•Undertake a review of workforce data in relation to EDS goals and with particular reference to provision of usable, meaningful information.•Refresh Equality and Diversity strategies with a focus on improving workforce representation in relation to protected characteristics , encouragingcommitment to the Personal, Fair, Diverse campaign and promoting inclusion through sharing stories.
WORKFORCE CAPACITY
LCFT Workforce Scorecard October to December 2013

LEADERSHIP & QUALITY
LCFT Workforce Scorecard October to December 2013

Appreciative Leadership
LEADERSHIP & QUALITY
Overall the workshops have been valuable
AGREE 100%
DISAGREE 0%
Workshops have had value
to me in my leadership
AGREE 99%
DISAGREE 1%
Relevance of the learning and
development in supporting the
delivery of operational
objectives and targets
AGREE 98%
DISAGREE 2%
Attending the programme is
reflected on my PDP
AGREE 87%
DISAGREE 13%
The process has helped affirm my strengths
AGREE 94%
DISAGREE 6%
The process has helped
identify areas for change
AGREE 91%
DISAGREE 9%
LCFT Workforce Scorecard October to December 2013
Evaluation data taken from Extension Programme

Aspiring Leaders
Data from Aspiring Leaders Cohort 2
LEADERSHIP & QUALITY
Number Completed
25
Number Promoted
10
Number of Attendees
32
LCFT Workforce Scorecard October to December 2013

Mandatory Training
LEADERSHIP & QUALITY
LCFT Workforce Scorecard October to December 2013
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Fire E & D SafeguardingChildren
Moving &Handling L1
BLS Infection Control ConflictResolution
Health & Safety I G SafeguardingAdults
Staf
f A
tte
nd
ed
Q2 Q3 Target

Safety
LEADERSHIP & QUALITY
TYPE OF INCIDENT TOTAL STAFF RELATED TOP CATEGORY
TOTAL STAFF RELATED TOP SUB-CATEGORY
TOTAL
Personal Accident – Staff 94 Slips/Trips/Falls – Staff 27 Slip 10
Ill Health Staff 15 Staff Unwell 15 Other 12
Physical Violence 819 Patient on Staff 629 Assaults 583
Non Physical Violence 550 Patient on Staff 373 Verbal 157
Vehicle 24 Collision 19 Contact with Another Vehicle 10
Patient Safety – Staff Related 1340 Health Records 731 Entry Filed in Wrong Patient
Record
275
Service Deficit 609 Staff Unable to Take Breaks 331
LCFT Workforce Scorecard October to December 2013
Patient Safety Incidents : 3089 (This is all patient safety incidents for the quarter which include patient related incidents i.e.. Medication, AWOL, treatment etc.)
Staff Related Incidents : 2037 (These are the incidents for the quarter which affect staff rather than patients including patient safety and health records)
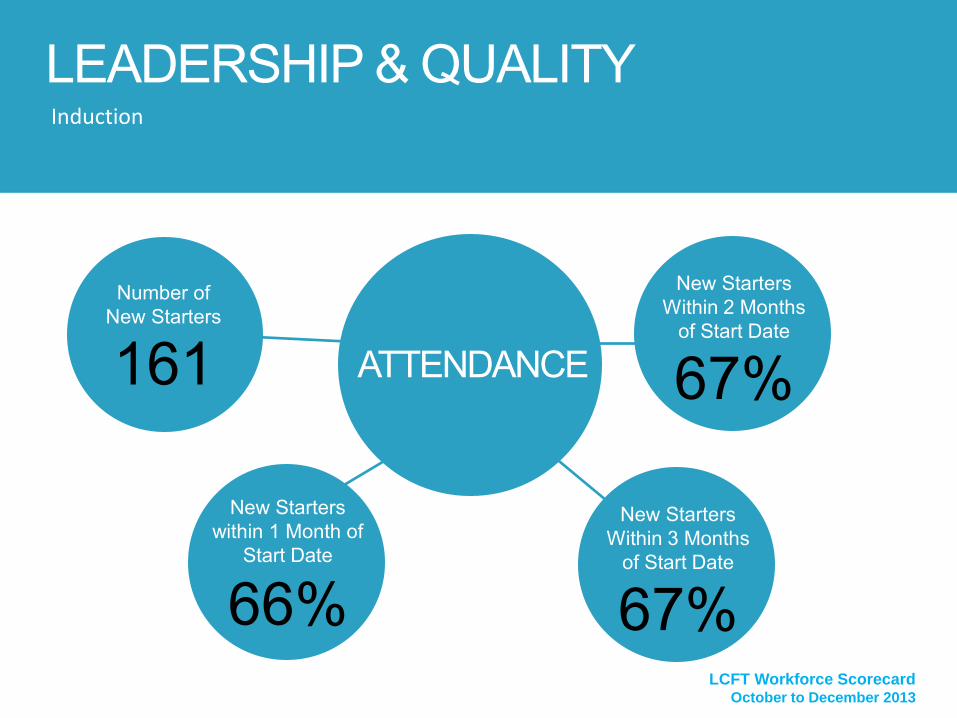
Induction
ATTENDANCE
Updated figures will be included in Q3 report.
LEADERSHIP & QUALITY
New Starters within 1 Month of
Start Date
66%
New Starters Within 2 Months
of Start Date
67%
New Starters Within 3 Months
of Start Date
67%
Number of New Starters
161
LCFT Workforce Scorecard October to December 2013

Co-Signed,
71%
Not Co-Signed, 29%
Access to e-PDR System and Objective Sign-off
LEADERSHIP & QUALITY
LCFT Workforce Scorecard October to December 2013
Not Accessed, 22% Accessed, 78%

Staff Survey - Leadership
LEADERSHIP & QUALITY
LCFT Workforce Scorecard October to December 2013
Q1 My immediate manager encourages those who work for her/him to work as a team
Q2 My immediate manager can be counted on to help me with a difficult task at work
Q3 My immediate manager gives me clear feedback on my work
Q4 My immediate manager asks for my opinion before making decisions that affect my work
Q5 My immediate manager is supportive in a personal crisis
Q6 I know who the senior managers are here
Q7 Communication between senior management and staff is effective
Q8 Senior managers here try to involve staff in important decisions
Q9 Senior managers act on staff feedback
Q10 Senior managers where I work are committed to patient care 0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Q1 Q2 Q3 Q4 Q5 Q6 Q7 Q8 Q9 Q10
Overall Agree % Overall Disagree %

Why have we included this data?THE LINKS BETWEEN LEADERSHIP, QUALITY AND SERVICE USER OUTCOMES ARE WIDELY RECOGNISED. THIS SECTION EXPLORES THESE AND WILL IN TIME UTILISE EAM, DATIX AND THE QUALITY SEEL TOOL TO IDENTIFY RISKS AND ANALYSE TRENDS. WE WILL DEVELOP THIS SECTION TO INCLUDE EVALUATION OF OTHER PROGRAMMES SUCH AS MEDICAL LEADERSHIP. IN ADDITION TO REPORTING COMPLIANCE, WE ARE CONSIDERING MECHANISMS TO ASK A EMPLOYEES POWERFUL QUESTIONS RELATING TO THE QUALITY AND EFFECTIVENESS OF EDUCATION, LEARNING AND DEVELOPMENT ACTIVITY.
What is this telling us?•40% of those completing the Aspiring Leaders programme were promoted during the course.•Nearly half of our Band 7 and above employees have completed the Appreciative Leadership course, finding the workshops valuable and the learningrelevant to achieving operational objectives and targets. •Only two thirds of new starters attend induction within the first three months of employment.•Compliance with mandatory training has improved on the majority of courses when compared with Q2, however there are four areas below the 85%target. These are Fire, Basic Life Support, Infection Control and Conflict Resolution. •The staff survey gives insight into our employees’ view of their leaders, with the majority feeling they are encouraged and supported. Particularconcerns are around effective communication between senior managers and staff, people not feeling involved in important decisions or that their feedback is acted upon. In these questions respondents were more negative than positive. •The greatest risk to our staff in terms of safety comes from physical and verbal abuse.•Online PDR completion rates have increased to 78% .
What’s new? •Additional mandatory training courses are being offered during February and March 2014 with particular focus on modules with below targetattendance. •Next cohort of Appreciative Leadership delegates are currently completing Workshop 2.•Additional induction programmes scheduled for 2014/15.
What else should we do about it? •Promote e-learning packages (Fire and Infection Control) and face to face training (BLS) and ensure employees are released to attend mandatorytraining with particular focus on courses below the 85%. •Review reasons for non-attendance at induction and assess criteria for attendance. Do we need more courses?•Staff Survey results to inform targeted action at Network level.•Support employees to access externally funded clinical and apprenticeship programmes.
LEADERSHIP & QUALITY
LCFT Workforce Scorecard October to December 2013

ENGAGEMENT & WELLBEING
LCFT Workforce Scorecard October to December 2013

Sickness Absence Occurrences (Top 3 Reasons)
ENGAGEMENT & WELLBEING
LCFT Workforce Scorecard October to December 2013
2013 10 2013 11 2013 12 Grand Total
S13 Cold, Cough, Flu - Influenza 21.71% 22.40% 19.78% 21.33%
S25 Gastrointestinal problems 16.81% 20.38% 21.48% 19.48%
S99 Unknown causes / Not specified 13.87% 10.40% 11.44% 11.93%
0.00%
5.00%
10.00%
15.00%
20.00%
25.00%
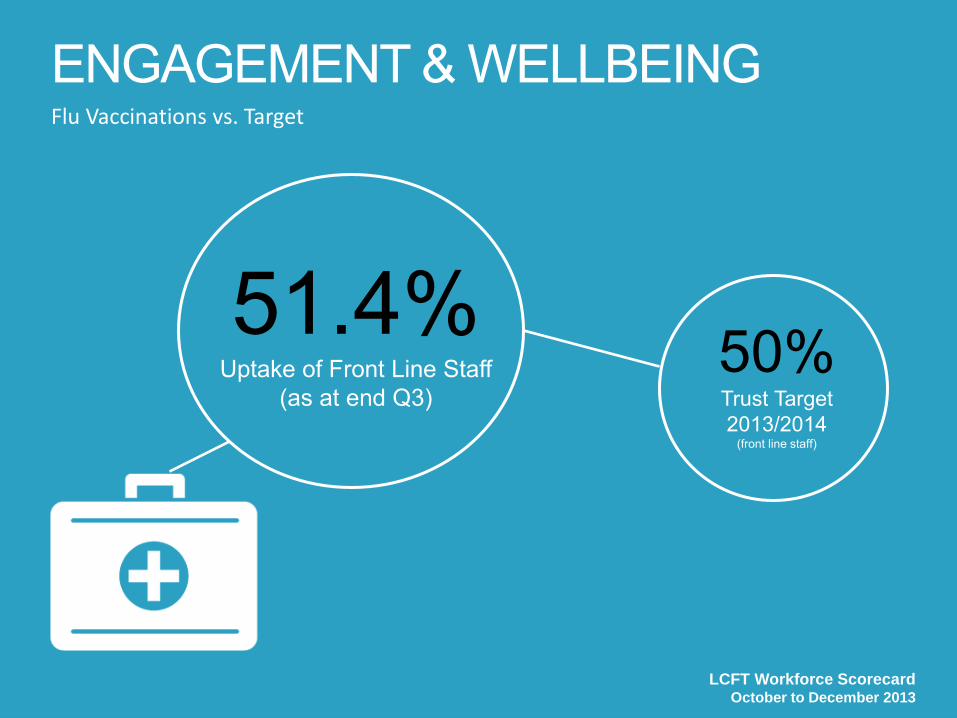
ENGAGEMENT & WELLBEING Flu Vaccinations vs. Target
51.4% Uptake of Front Line Staff
(as at end Q3) 50% Trust Target 2013/2014
(front line staff)
LCFT Workforce Scorecard October to December 2013

Overall Staff Survey Engagement Questions/Score
ENGAGEMENT & WELLBEING
LCFT Workforce Scorecard October to December 2013
71%
29%
Staff Ability To Contribute Towards Improvements At Work
Agree Disagree
3.70
3.71
3.79
1.00 2.00 3.00 4.00 5.00
Trust Score 2012
Trust Score 2011
Poorly Engaged Staff
Highly Engaged Staff
3.65
3.54
1 2 3 4 5
Staff Motivation At Work
Staff Recommendation Of TheTrust As A Place To Work OrReceive Treatment
Poorly Engaged Staff Highly Engaged Staff

PDR Engagement Scores
ENGAGEMENT & WELLBEING
LCFT Workforce Scorecard October to December 2013
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
I know what is expected of me atwork
I have the materials andequipment I need to do my job
right
At work, I have the opportunityto do what I do best every day
My line manager, or someone atwork, seems to care about me as
a person
There is someone at work whoencourages my development
At work, my opinions seem tocount
The mission or purpose of myorganisation makes me feel my
job is important
In the last six months, someoneat work has talked to me about
my progress
This last year, I have hadopportunities at work to learn
and grow
Strongly Agree
Disagree
Not Specified

Why have we included this data? EVIDENCE INDICATES THAT ENGAGEMENT AND WELLBEING SIT ALONGSIDE LEADERSHIP AS A KEY CONTRIBUTOR TO HIGH ORGANISATIONAL PERFORMANCE. THIS SECTION INCLUDES SICKNESS DATA BUT ALSO SHOWS MORE DETAILED INFORMATION AROUND REASONS FOR ABSENCE, SUCH AS STRESS. ALONGSIDE THIS, WE PROVIDE NEW INFORMATION WHICH ENABLES VISIBILITY OF A WIDER PICTURE OF EMPLOYEE WELLBEING. What is this telling us? •Monthly figures show an encouraging, slight reduction in sickness cases relating to Anxiety/Stress/Depression/Other psychiatric illness and
sickness cases reported for this reason have dropped from the top 3 reasons this quarter. However, this is mainly attributable to the
seasonal spike in sickness relating to Cold, Cough, Flu-Influenza and we would expect this position to revert in Q4.
•Both the e-PDR engagement scores and the overall engagement scores from the staff survey demonstrate that LCFT employees are
engaged.
•The annual flu vaccination target has been met for front line staff.
What should we do about it? •Share best practice across Networks.
•Workforce has developed and scheduled workshops for performance management training and will actively encourage participation.
•Monitor success of Wellbeing Strategy in relation to initiatives aimed at reducing Anxiety/Stress/Depression/Other psychiatric illness and
allocate resources accordingly.
•Continue to promote flu vaccinations to meet aspirations of 75%.
•Promote occupational health services such as physio service to raise wider awareness among staff.
ENGAGEMENT & WELLBEING
LCFT Workforce Scorecard October to December 2013
EMPLOYEE RELATIONS
LCFT Workforce Scorecard October to December 2013

Formal Action
EMPLOYEE RELATIONS
LCFT Workforce Scorecard October to December 2013

Number of Live Suspensions by Network
EMPLOYEE RELATIONS
LCFT Workforce Scorecard October to December 2013
3
2
1
351 Adult Mental Health (CCA) L4
351 Children and Families (ECD) L4
351 Specialist Services Network (BCS) L4

Risk Level of Current Employee Relations Cases Split by Type
Number of Formal Absence Cases (with Workforce Support) by Network
EMPLOYEE RELATIONS
LCFT Workforce Scorecard October to December 2013
54%
24%
22%
High
Medium
Low
33.65%
27.88%
19.23%
10.58%
4.81% 1.92% 0.96% 0.96%
Adult Community
Adult Mental Health
Children And Families
Specialist Services
Corporate
Psychological Services
Bank staff
Estates & Facilities

Why have we included this data?THIS SECTION INCLUDES INFORMATION RELATING TO NUMBERS AND TYPES OF EMPLOYEE RELATIONS CASES TO GIVE AN INDICATION OF THE EMPLOYEE RELATIONS CLIMATE WITHIN THE TRUST. THERE ARE PLANS TO INCLUDE STAFF RELATED COMPLAINTS AND SUI’S IN THIS DOMAIN MOVING FORWARD.
What is this telling us?•54% of current employee relations cases are rated as high risk in line with the case risk model and therefore the resource impact on both
the Networks and the Workforce Directorate is high.
•There are currently 7 suspensions, 3 within Adult Mental Health, 3 in Children & Families and 1 in Secure Service.
•The Trust currently has 3 employment tribunal cases which is low when compared with the number of high risk cases typically ongoing
with the Trust.
•There is currently a very low level of employees subject to formal performance procedures. Typically we would expect this to be around
5-10%.
What should we do about it?•Continue to closely manage high risk cases with a view to concluding cases where an employee is suspended as soon as possible.
•Coach managers and discuss potential performance issues before cases are activated to try to mitigate risk.
•Develop Network level plans to reduce the number of employee relations cases.
•Roll out a programme of management development courses (commencing Feb 2014) to build line management capability in managing
performance, sickness absence and misconduct.
EMPLOYEE RELATIONS
LCFT Workforce Scorecard October to December 2013

AGENDA NUMBER: CG 028/14
COUNCIL OF GOVERNORS – 10 April 2014 Sub Committee Key Messages
FOIA STATUS: No Exemption
PAPER TITLE: Sub Committee Key Messages
PURPOSE: To provide the Council with the Key Messages arising out of the CoG sub-committees since the last formal CoG meeting
ACTION RECOMMENDED:
Noting
PAPER PREPARED BY: Ashley Christian, Governor Project Support Officer
1.0 BACKGROUND The use of a Key Messages update supports the focus of sub-committee business around the assurance required for them to discharge their responsibilities on behalf of the Council of Governors.
The implementation of Key Messages reporting takes the relevant issues, areas of concern/excellence and recommendations from each Committee for the Council of Governors to consider and either note or approve.
The Key Messages contain all relevant items arising from Committee minutes and have replaced sub-Committee minutes on the formal Council of Governor agenda.
2.0 COUNCIL OF GOVERNOR ACTION
The Council of Governors are asked to note the contents of the key message reports of the following sub-committees:
• Membership & Governance Committee 12 February 2014• Patient & Experience Oversight Group 20 January 2014• Standards & Assurance Committee 03 March 2014

Council of Governors
Membership & Governance Committee – 12 February 2014
Key Messages
Key Themes and Messages:
1. Membership conference proposal:The proposal of ' Public Health ' being the topic for the next members meeting wasapproved.
2. Public and Staff Governors to meet more often outside of meetings to have a chanceto get to know each other. Governors discussed that they would like the opportunityto meet with all the Governors more often outside meetings, so that they have achance to get to know each other better.
Areas of Concern or Excellence:
3. Governor engagement workshops:Concerns raised by a Staff Governor about the lack of involvement of Staff Governor.A Staff Governor confirmed that whilst she was happy to support the workshops, shewas concerned about the lack of involvement of Staff Governors and requested thatthe Company Secretary, in conjunction with the engagement team, bring a proposalto the next meeting. The Head of Company Secretary Service explained to thecommittee that the idea was to do a pilot workshop first and then extend it out toboth Public and Staff Governors. She noted that the Company Secretary wouldpresent this at the next meeting as an agenda item. The Chair has also been invitedto attend the next meeting in April to further discuss on the staff involvement andthat we are pending a way forward.
Recommendations:
Level of Assurance:
Based on the work carried out by the Membership & Governance Committee, the Council of Governors can be reasonably assured of the Trust’s compliance with standards.

Council of Governors
Patient Experience Oversight Group – 20 January 2014
Key Messages
Key Themes and Messages:
The implementation of a newly formatted PEOG began on 20th January and the meeting, with the new reports and thematic review was very positive. Governors agreed the benefits to re-focussing the Committee on patient experience would become the driver to embedding the new format.
Areas of Concern or Excellence:
Governors wished to note the successful work underway around the implementation of the Friends and Family Test and in particular, note the work undertaken to ensure the Trust is delivering a value-adding Friends and Family Questionnaire to encourage relatives and carers to comment on care and support improvements to services.
Recommendations:
The Committee also approved the alterations to the PEOG Terms of Reference, and note that the updated version will be incorporated into the Governance Handbook. The most recent version of the Governance Handbook can be found online in CoG Zone.
Level of Assurance:
Based on the work carried out by the PEOG Committee, the Council of Governors can be reasonably assured that the Trust is meeting its duties to engage with the public and learn from patient experience.

Council of Governors
Standards and Assurance Committee – 03 March 2014
Key Messages
Key Themes and Messages:
1. The committee approved the Cycle of Business 2014/15 and the April and Octoberdates were changed to May and November.
2. The Mental Health Act Lead, Leander Nield was invited to the March SAC meeting toprovide an overview on the Mental Health Act as requested by Committee members.The committee found this very useful and they have a better understanding on MHA.
3. The Committee were informed that Steve Sansbury, Appointed Governor fromLancashire Constabulary is the Chair of the joint meeting with LancashireConstabulary.
Areas of Concern or Excellence:
Recommendations:
Level of Assurance:
Based on the work carried out by the Standards and Assurance Committee, the Council of Governors can be reasonably assured of the Trust’s compliance with standards.

AGENDA NUMBER: CG 029/14
COUNCIL OF GOVERNORS – 10 April 2014 Sub Committee Cycles of Business
FOIA STATUS: No Exemption
PAPER TITLE: Sub Committee Cycles of Business 2014/15
PURPOSE: To provide the Council with the CoG sub-committee Cycles of Business
ACTION RECOMMENDED:
Noting
PAPER PREPARED BY: Ashley Christian, Governor Project Support Officer
1.0 BACKGROUND A Cycle of Business sets out the intended annual business for a committee and is drawn from the Terms of Reference. The benefits of preparing a Cycle of Business ensure the committee has full oversight of the plan to discharge its functions and adopts a planned approach to seeking assurance on behalf of the Council of Governors.
2.0 SUB COMMITTEE CYCLES OF BUSINESS 2014/15 The Council are provided with the Cycle of Business for each of its sub-committees to provide assurances that the sub-committees are able to discharge its intended functions during 2014/15. The Cycles can be seen at Appendix A – D.
3.0 COUNCIL OF GOVERNOR ACTION The Council of Governors are asked to note the sub-committees Cycles of Business for 2014/15 for assurance.

MEMBERSHIP & GOVERNANCE ANNUAL CYCLE OF BUSINESS 2014 / 2015
MEETING DATE ITEMS FOR AGENDA COMMENTS
07 April 2014
Formal Business of the Group:
• Membership Strategy Updates
• Consider Format of Annual Members Meeting 2014
• Membership Survey Panels
Business to be discussed as Required:
• Review of Membership Applications
• Monitoring Governor compliance with Code of Conduct
• Review of Trust Constitution
22 July 2014
Formal Business of the Group:
• Membership Strategy Update
• Consider the Format of the Autumn member conference
• Annual Review of CoG Effectiveness
• Foundation News – Summer/Autumn edition
• Governor Elections Plan
Business to be discussed as Required:
• Review of Membership Applications
• Monitoring Governor compliance with Code of Conduct
• Review of Trust Constitution

MEETING DATE ITEMS FOR AGENDA COMMENTS
06 October 2014
Formal Business of the Group:
• Membership Strategy Updates
• Membership Panel Survey
• Governor Elections Update
Business to be discussed as Required:
• Review of Membership Applications
• Monitoring Governor compliance with Code of Conduct
• Review of Trust Constitution
12 January 2015
Formal Business of the Group:
• Membership Strategy Updates
• Consider the Format of the Spring member conference
• Update against CoG Effectiveness Review
• Governor Training & Development Programme 2015/16
• Cycle of Business 2015/16
• Foundation News Winter/Spring Edition
• Membership Panel Survey

NOMINATION/REMUNERATION COMMITTEE ANNUAL CYCLE OF BUSINESS 2014 / 2015
MEETING DATE ITEMS FOR AGENDA PAPER DEADLINES
19 February 2014
Formal Business of the Group:
• Rem/Nom Cycle of Business 2014/15
• Succession planning for NEDs
• NED recruitment process (inc recommendation for CH)
• NED Appraisals proposal7th February 2014
23 April 2014
Formal Business of the Group:
• NED Appraisals Update
• NED Recruitment Update
• Terms of Reference Review15th April 2014

MEETING DATE ITEMS FOR AGENDA PAPER DEADLINE
9 June 2014
Formal Business of the Group:
• NED Appraisal Results
• NED Remuneration
• Extension to Terms of Office (DB & TW)
• NED Recruitment Results
30th May 2014
TBC December 2014
Formal Business of the Group:
• Verbal update from the Chair of Trust Board around NED performance
• Verbal update from the SID around performance of the Chair
• Reflection of Key Decisions made by Committee (NH)
TBC February 2015
Formal Business of the Group:
• Recommendation for NED extension/recruitment (PB)

PATIENT EXPERIENCE & OVERSIGHT GROUP ANNUAL CYCLE OF BUSINESS 2014 / 2015
MEETING DATE ITEMS FOR AGENDA COMMENTS
20 January 2014
Thematic Review
• Harmfree Care
Formal Business of the Group:
• Complaints and Compliments Report
• Cycle of Business 2014/15
• Terms of Reference review
• Friends & Family Test• Inpatient Surveys• PLACE visits
Reports Issued for Information/Assurance
• Questions/comments from Healthwatch (LINKs) and Overview and
Scrutiny Committee
17 April 2014
Thematic Review
• Offender Health service line – HMP Kirkham
Formal Business of the Group:
• Complaints and Compliments Report• Friends & Family Test• Inpatient Surveys• PLACE visits
Reports Issued for Information/Assurance
• Questions/comments from Healthwatch (LINKs) and Overview and
Scrutiny Committee

MEETING DATE ITEMS FOR AGENDA COMMENTS
17 July 2014
Thematic Review
• 0 – 19 service line (0-19 Health Visitors)
Formal Business of the Group:
• Complaints and Compliments Report
• Friends & Family Test• Inpatient Surveys• PLACE visits
Reports Issued for Information/Assurance
• Questions/comments from Healthwatch (LINKs) and Overview and
Scrutiny Committee
21 October 2014
Thematic Review
• Rehabilitation, MSK and Rheumatology service line
Formal Business of the Group:
• Complaints and Compliments Report
• Annual Report of Complaints
• Friends & Family Test• Inpatient Surveys• PLACE visits
Reports Issued for Information/Assurance
• Questions/comments from Healthwatch (LINKs) and Overview and
Scrutiny Committee
MEETING DATE ITEMS FOR AGENDA COMMENTS
21 January 2015
Thematic Review
• Adult Mental Health Inpatients – Parkwood & Ridge Lea
Formal Business of the Group:
• Complaints and Compliments Report
• Friends & Family Test• Inpatient Surveys• PLACE visits
Reports Issued for Information/Assurance
• Questions/comments from Healthwatch (LINKs) and Overview and
Scrutiny Committee

STANDARDS & ASSURANCE ANNUAL CYCLE OF BUSINESS 2014 / 2015
MEETING DATE ITEMS FOR AGENDA COMMENTS
6th May 2014
Formal Business of the Group:
• Minutes of previous meeting
• Action Tracker Updates
• Changes to the CQC inspections (thematic review)
• Terms of Reference review
• Quality Account
• Quality Strategy Quarterly Update
• Good Practice Visit Updates
• Key Messages for CoG
29th July 2014
Formal Business of the Group:
• Minutes of previous meeting
• Action Tracker Updates
• NICE & Quality Standards (thematic review)
• Quality Strategy Quarterly Update
• Good Practice Visit Updates
• Key Messages for CoG

MEETING DATE ITEMS FOR AGENDA COMMENTS
4th November 2014
Formal Business of the Group:
• Minutes of previous meeting
• Action Tracker Updates
• Care Pathways (thematic review)
• Quality Strategy Quarterly Update
• Good Practice Visit Updates
• Key Messages for CoG
27th January 2015
Formal Business of the Group:
• Minutes of previous meeting
• Action Tracker Updates
• Cycle of Business 2015/16
• SAC Calendar of Meetings 2015/16
• CQC & internal quality visits (thematic review)
• Quality Strategy Quarterly Update
• Good Practice Visit Updates
• Key Messages for CoG

















