Kathleen Alloway – Senior Policy Officer Activity Based Funding and Management Department of Health, Western Australia Counting Activity Correctly and Consistently Counts The application and evaluation of the Admission, Readmission , Discharge and Transfer (ARDT) Policy in implementation of ABF
Transcript
Kathleen Alloway – Senior Policy OfficerActivity Based Funding and Management Department of Health, Western Australia
Counting Activity Correctly and Consistently CountsThe application and evaluation of the Admission, Readmission , Discharge and Transfer (ARDT) Policy in implementation of ABF
Slide 2
Slide 3
Change Management
� The new environment of ABF/ABM impacts on all aspects of health service delivery
� Purpose of existing data collections� Every admission is an invoice
requesting payment for product/service delivered
� Clinical practice alignment � Policy required to ensure appropriate
and legitimate funding of activity� Rules required to guide health services
Slide 4
� Thinking differently� WHADILT� Processes and Practices
for activity recording do not work in ABF
� Did not matter before now it matters
The way it is
The way we were
Slide 5
� Consistent classification and tracking of activity provides access to reliable data so that we may understand and manage our business better
� National activity based funding program requires a standardised approach
� High quality robust data is an integral part of the practical application of ABF/ABM
� We need rules on how we count and classify activity
� Activity data is used for a range of applications
�WA health services have an obligation to count and label activity in an accurate and consistent fashion
Slide 6
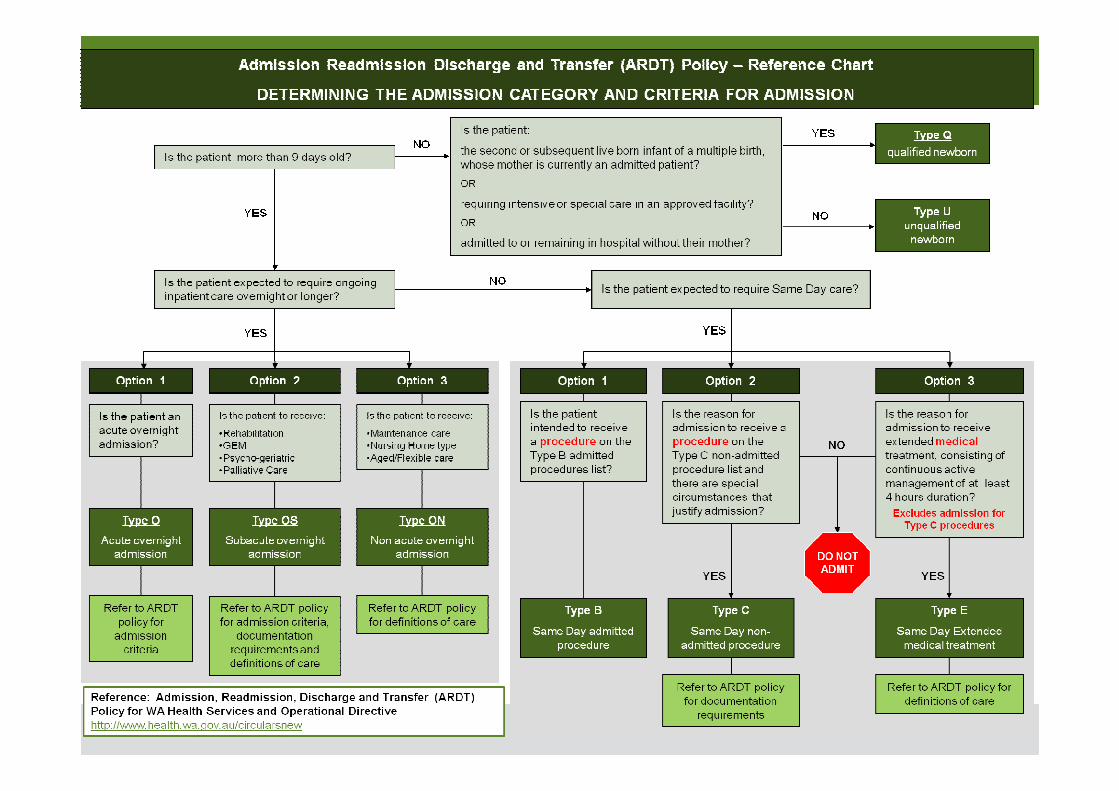
An admitted patient must meet the criteria for admission related to the admission category and care type. These include :� Expected levels of care� Documentation requirements � Same day specific criteria for emergency
admissions� Procedure exclusions set by the Commonwealth� Assessment and Care planning
�Activity Based Funding and Management as the principal resource allocation and funding mechanism means that correct labelling and
counting of activity is now especially important
�The ARDT policy provides a framework, containing detailed rules and criteria to enable this to occur
Slide 7
The ARDT policy has range of benefits:� Ensuring health services are correctly
funded� Accurate activity for use in clinical
costing � Inform and position the state to align with
national hospital funding reforms
� Provide a reliable care delivery profile to inform clinical services planning
Key information from a range of related documents provides a “one stop policy document” to support staff as they record and
classify this information
The ARDT policy had been developed through research into other jurisdictions and in collaboration with staff across WA Health
Slide 8
Policy research – DoH policy documents
� Admission Policy for WA Hospitals (Technical Bulletin 17/3, 2002).� Transferred Patients (Technical Bulletin 50/0, 2002).� Neonatal care information reporting (Technical Bulletin 14/5, 2004).� Renal Dialysis (Technical Bulletin 4/5, 2002).� Reporting different episodes of care (Technical Bulletin 26/5, 2004).� Hospital Morbidity Information (Technical Bulletin 10/6, 2005).� Rehabilitation program – definitions and reporting requirements (Operational
Directive 0025/06, 2006).� Hospital in the Home care (Technical Bulletin 78/0, 2006).� Subacute and non-acute care (Technical bulletin: 20/6, 2004). � Discharge Policy in WA Hospitals (Technical bulletin: 40/1, 2001).� Geriatric Evaluation and Management (GEM) – Definitions and Reporting
Requirements (Technical Bulletin 79/0, 2006)� Palliative Care Program (Technical Bulletin 42/3, 2002)
Slide 9
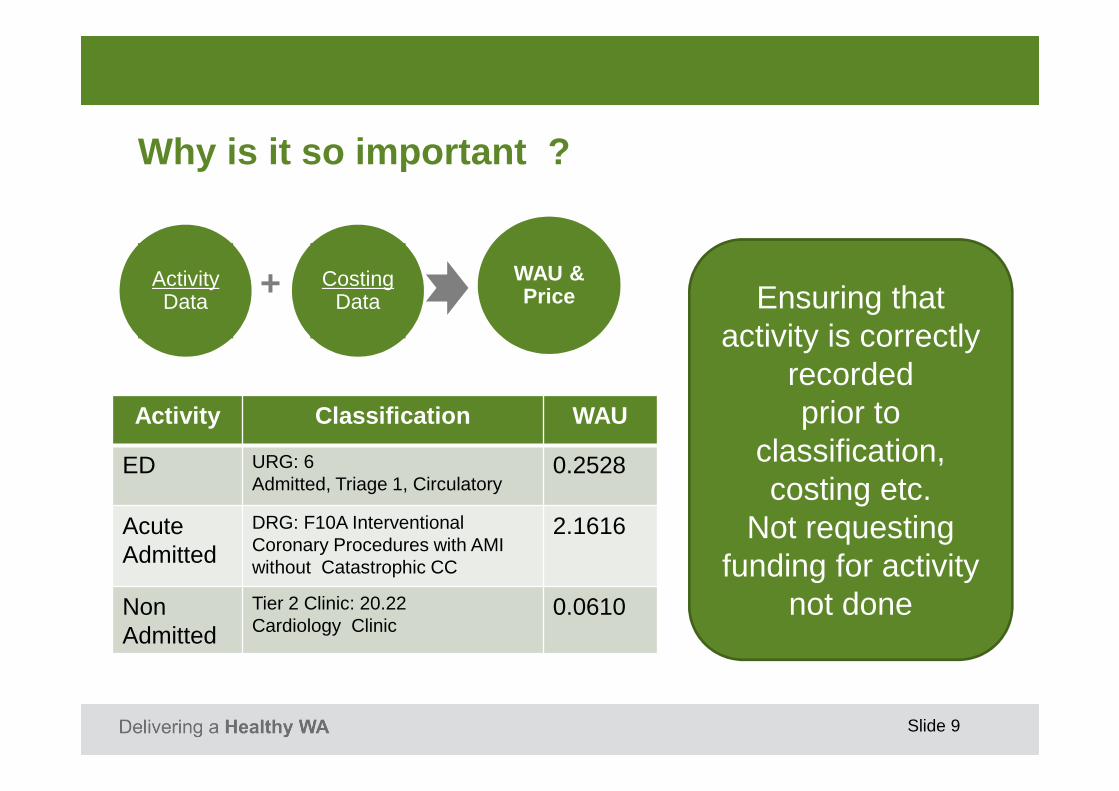
Why is it so important ?
ActivityData
+ CostingData
WAU & Price
Activity Classification WAU
ED URG: 6Admitted, Triage 1, Circulatory
0.2528
Acute Admitted
DRG: F10A Interventional Coronary Procedures with AMI without Catastrophic CC
2.1616
Non Admitted
Tier 2 Clinic: 20.22Cardiology Clinic
0.0610
Ensuring that activity is correctly
recordedprior to
classification, costing etc.
Not requesting funding for activity
not done
Slide 10
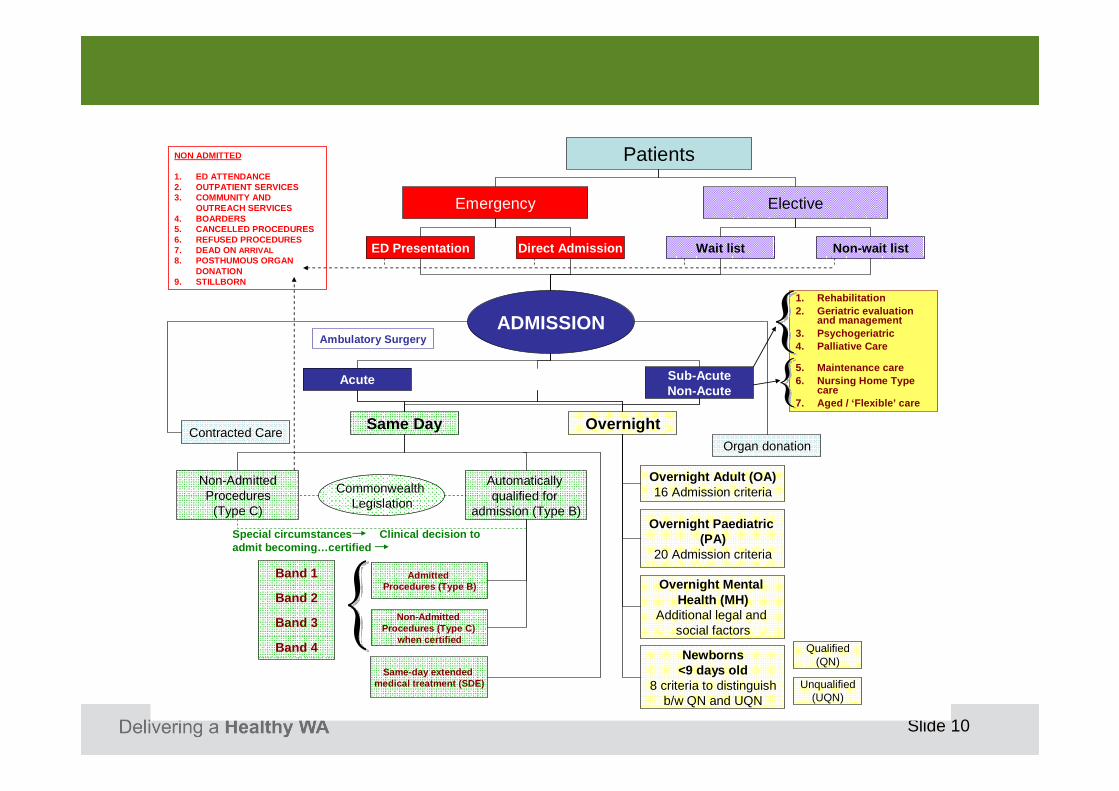
NON ADMITTED
1. ED ATTENDANCE2. OUTPATIENT SERVICES3. COMMUNITY AND
OUTREACH SERVICES4. BOARDERS5. CANCELLED PROCEDURES6. REFUSED PROCEDURES7. DEAD ON ARRIVAL8. POSTHUMOUS ORGAN
DONATION9. STILLBORN
Patients
ElectiveEmergency
Acute
ED Presentation Direct Admission Non-wait listWait list
ADMISSION
Sub-AcuteNon-Acute
Same Day Overnight
Non-AdmittedProcedures
(Type C)
Automatically qualified for
admission (Type B)
Commonwealth Legislation
Admitted Procedures (Type B)
Non-Admitted Procedures (Type C)
when certified
Same-day extended medical treatment (SDE)
Band 1
Band 2
Band 3
Band 4
Special circumstances Clinical decision to admit becoming…certified
Contracted CareOrgan donation
Overnight Adult (OA)16 Admission criteria
Overnight Paediatric (PA)
20 Admission criteria
Overnight Mental Health (MH)
Additional legal and social factors
Newborns<9 days old
8 criteria to distinguishb/w QN and UQN
Unqualified(UQN)
Qualified(QN)
1. Rehabilitation2. Geriatric evaluation
and management3. Psychogeriatric4. Palliative Care
5. Maintenance care6. Nursing Home Type
care7. Aged / ‘Flexible’ care
Ambulatory Surgery
Slide 11
Slide 12
Admitted Care
� An admitted patient is defined as a person who meets the criteria for admission and additional criteria specific to the applicable admission category and care type, and undergoes a hospital’s admission process (documented) to receive treatment and/or care for a period of time
Slide 13
All OK?
� Admitted data collections well established so should be all OK. (shouldn’t it)
BUT
� ED care segregated from admitted care and needs to be counted and classified by URG
� Has the ARDT policy been implemented ?
Slide 14
Policy compliance evaluation
� Corporate Governance Audit 2012:� 70% of ED admissions, no valid clinical reason for admission � Up to 65% less than 4 hours in duration
� Focus audit for < 4hr admissions from ED � 59% no valid clinical reason for admission � 50% did not leave ED (virtual ward)� Deceased in ED = 1 minute admission� Admission after Absconding � Waiting for bus service to commence
Slide 15
Audit issues
� In summary, health services are non-compliant with the ARDT policy
� National alignment risk � Activity data used for other
purposes incorrect It is a sad story Piglet and it does not improve with the telling
� Activity is not being counted and costed in the correct classification system
� Incorrect activity data for use in costing, funding, planning and other applications
Slide 16
Admission criteria for ED admissions
� When an ED patient is admitted for short stay/same day, admission to they must meet admission criteria:� Receive a minimum of four hours of continuous active
management; or� Are admitted to receive a procedure on the Type B
admitted procedures list
� Exceptional cases which do not meet the admission criteria, but which the treating medical officer decides require admission
Slide 17
ED Admission Exclusions
� A patient should not be admitted because they are or will be in the ED for longer than 4 hours.
� A patient should not be admitted if the reason for the admission is they are waiting for:
� review by an admitting team� diagnostic tests or results� transport home or to another health care facility� equipment or medications
Slide 18
Emergency Department– Guide to Short Stay Admission Criteria
The decision to admit can ONLY be made by an author ised medical officer or nursing practitioner. The decision to admit must be documented in the medical record.
Does the patient require a procedure?
Does the patient require 4 or more hours of continuous active management?
DO NOTADMIT
NO
Admission (Type E)
PLEASE NOTE that a patient is not eligible for admission just because/if:o They are/will be in the Emergency Department for longer than 4 hourso They are transferred to a short stay unit but do not meet admission criteria o They are only waiting for:
• review by an admitting team• diagnostic tests or results• transport home or transfer to another health care facility• equipment or medications
o They receive their entire care within the Emergency Department
Admission (Type B) Admission (Type C)
Examples:• Sedation/Anaesthesia • Infusion/transfusion of blood/blood
NB. IV therapy is the administrationby intravenous infusion of apharmacological/therapeutic agent.Ancillary, preparatory and linemaintenance procedures are NOTincluded as ‘therapy’.
Examples:• where general/regional anaesthesia
is required • Where intravenous or inhalational
sedation is required • Where the patient’s co-morbidities
place the patient under high dependency
NB. Reason for admission &special circumstances must bedocumented in the medical record
Reason for admissionPatient is to receive an admittedType B procedure.
Reason for admissionPatient is to receive a non-admittedType C procedure AND has acondition or special circumstance thatjustifies admission.
Reference: Admission, Readmission, Discharge and T ransfer (ARDT) Policy for WA Health Services and Operationa l Directive http://www.health.wa.gov.au/circularsnew
YES YES
NB. Admission time commences when the patient physicallyleaves the clinical area of ED for transfer to a ward, includingED short stay unit, or operating theatre/procedure room
Identify which of the following the patient will req uire and complete the associated documentation:
MANAGEMENT DOCUMENTATION REQUIRED
� Serial tests/investigations
� Tests Required & intervals� Results and actions
documented
� Regular periodic observations
Excludes: BP / pulse / temp monitoring only
� Required observations, intervals and duration
� 4 hours of observation must be documented
� Continuous monitoring
� Type of monitoring
� Active treatment (and review)
� Nature of treatment� Time of planned review
Slide 19
NEAT impact ?
� Desire to meet the NEAT = Routinely admitting patients 99% to the virtual ward?
� Admissions where entire stay from Triage to Discharge < 4 hours
� The clock does not stop until the patient is discharged from ED admitted to a ward
� Needed to admit to virtual ward to print documentation. � Impact to NEAT performance after adjustment for ED
admissions < 4hours is minimal, ranging from 0 -7 %, with an average 2% decrease across all metropolitan hospitals.
Slide 20
Key policy issues ED
Patients who receive their entire episode of care within an Emergency Department are not eligible for admission, even if they meet the criteria for admission.
Admissions to a virtual ward within an Emergency Department are invalid
Slide 21
Key policy issues ED
� Admission Time is the time the patient physically leaves the clinical area of the Emergency Department for immediate transfer to a ward or operating theatre/procedure room at the same hospital.
Non-admitted services provided to a patient who is subsequently classified as an admitted patient shall
not be regarded as part of the admitted episode.
Treatment in ED not coded
Slide 22
Policy variation
� The calculation four hours duration of continuous of four active management may include the care provided after the decision to admit.
� Admissions to the virtual ward for purpose of admission processing.
� No discharges from the virtual ward
Slide 23
Policy and Operational Directive not working?
Engagement & Consultation
GOYA management principal
Slide 24
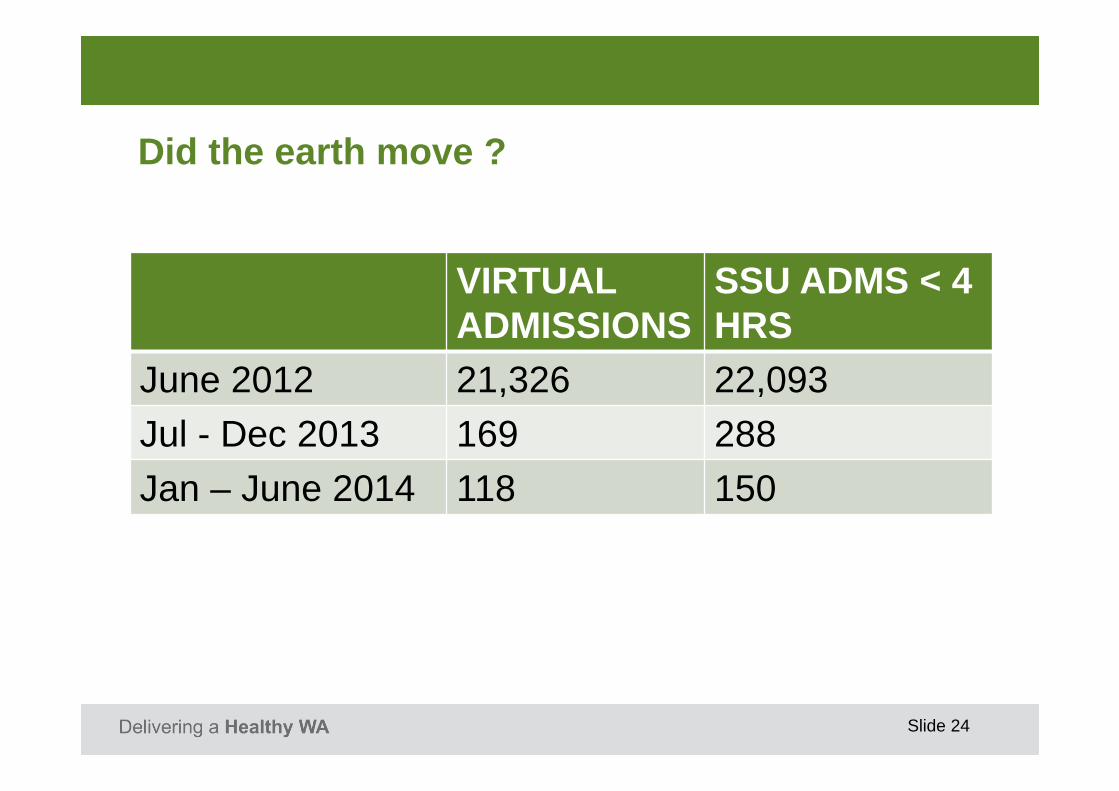
Did the earth move ?
VIRTUALADMISSIONS
SSU ADMS < 4 HRS
June 2012 21,326 22,093
Jul - Dec 2013 169 288
Jan – June 2014 118 150
Slide 25
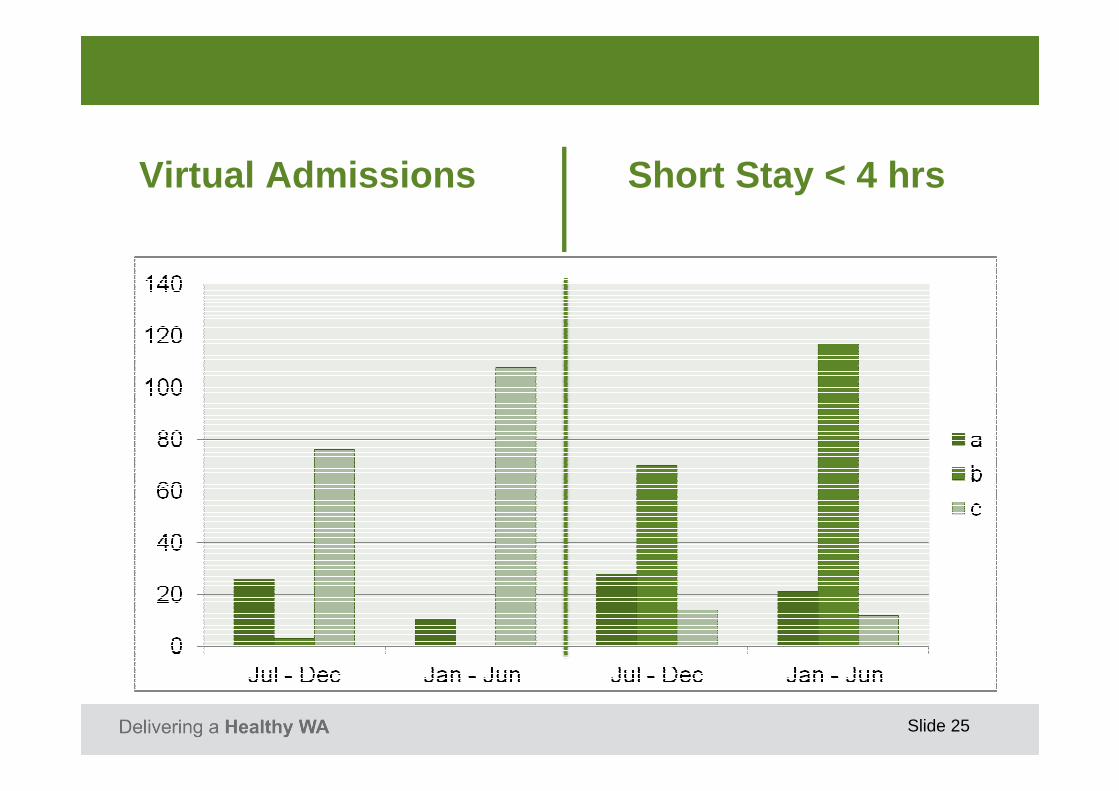
Virtual Admissions Short Stay < 4 hrs
Slide 26
Where did the admissions go?
Slide 27
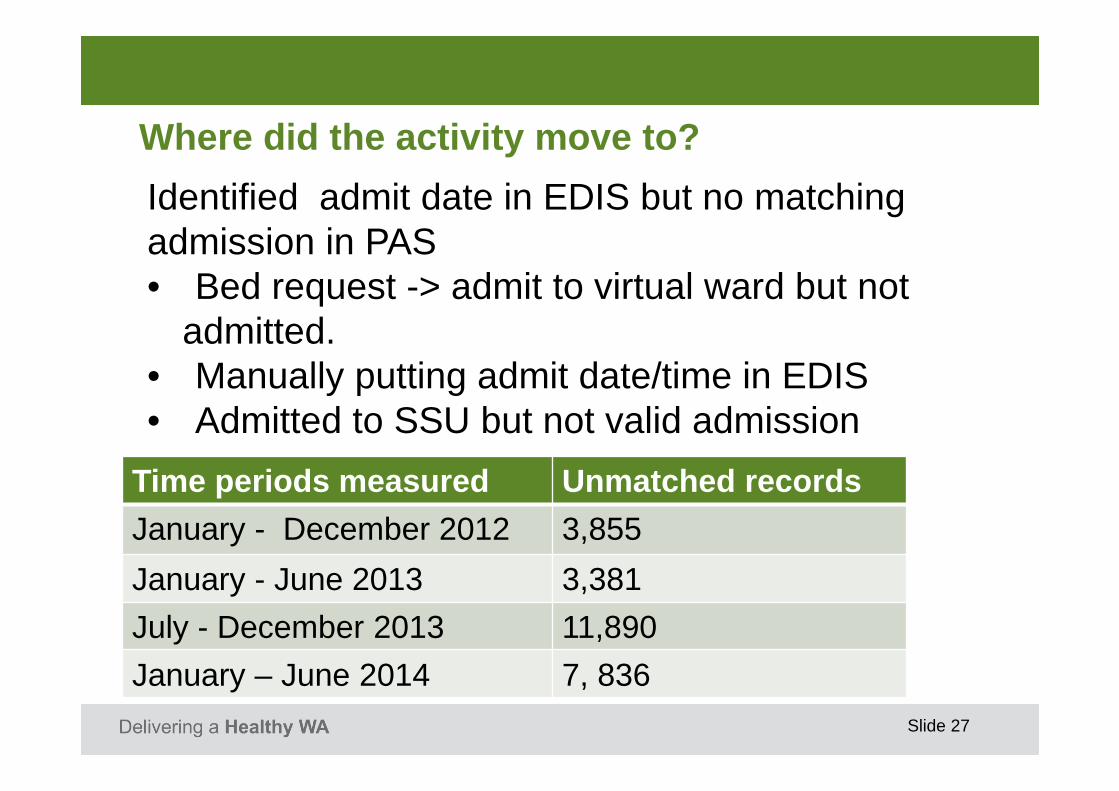
Where did the activity move to?
Time periods measured Unmatched records
January - December 2012 3,855
January - June 2013 3,381
July - December 2013 11,890
January – June 2014 7, 836
Identified admit date in EDIS but no matching admission in PAS• Bed request -> admit to virtual ward but not
admitted. • Manually putting admit date/time in EDIS• Admitted to SSU but not valid admission
� Daily monitoring� Reports on compliance issues� Consultation meetings� LEAN projects� Process mapping� Clerical role redesign� Clerical process changes� Clinical practice – admission checklist
Slide 30
Metropolitan Tertiary Hospitals
Slide 31
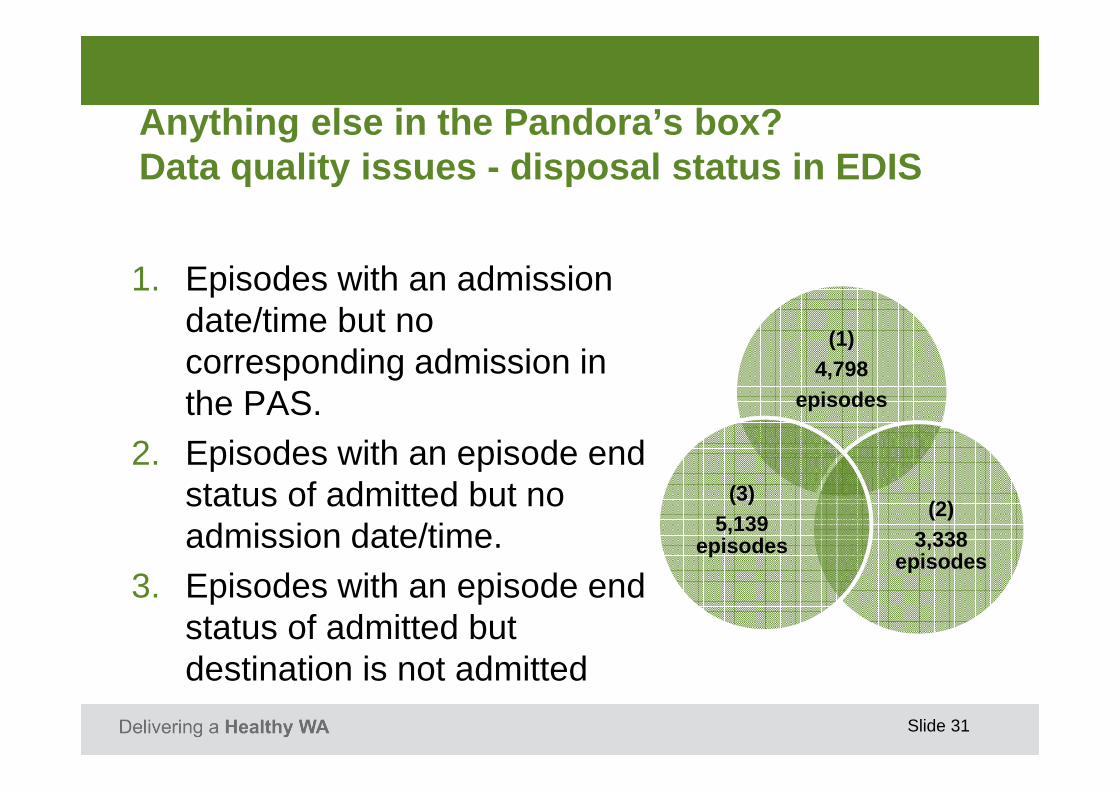
Anything else in the Pandora’s box? Data quality issues - disposal status in EDIS
1. Episodes with an admission date/time but no corresponding admission in the PAS.
2. Episodes with an episode end status of admitted but no admission date/time.
3. Episodes with an episode end status of admitted but destination is not admitted
(1) 4,798
episodes
(2)3,338
episodes
(3)5,139
episodes
Slide 32
Current Status
� ED no virtual admissions � ED disposal status WIP� Data quality edit checking
Other � HITH not HITH� Subacute Care
Slide 33
Lessons learnt
� Impact on other users of activity data� Change business practices � Conflict with other policy/reforms� Culture ready for change� Humans will avoid/work around it � A ward is not always a real ward � Policy ain’t policy without good policy

























![KS1 Assessment Update - EXS · using present and past tense mostly correctly and consistently o In Mowzer, the character description [B], the correct use of the simple present tense](https://static.documents.pub/doc/80x56/5f7c09fa96da5654467b49c2/ks1-assessment-update-exs-using-present-and-past-tense-mostly-correctly-and-consistently.jpg)


