34
CPC on Cervical Pathology Dr. W.K. Ng Senior Medical Officer Department of Clinical Pathology Pamela Youde Nethersole Eastern Hospital
CPC on Cervical Pathology
Dr. W.K. Ng Senior Medical Officer
Department of Clinical Pathology Pamela Youde Nethersole Eastern
Hospital

Cervical Smear: High Grade SIL (CIN III)
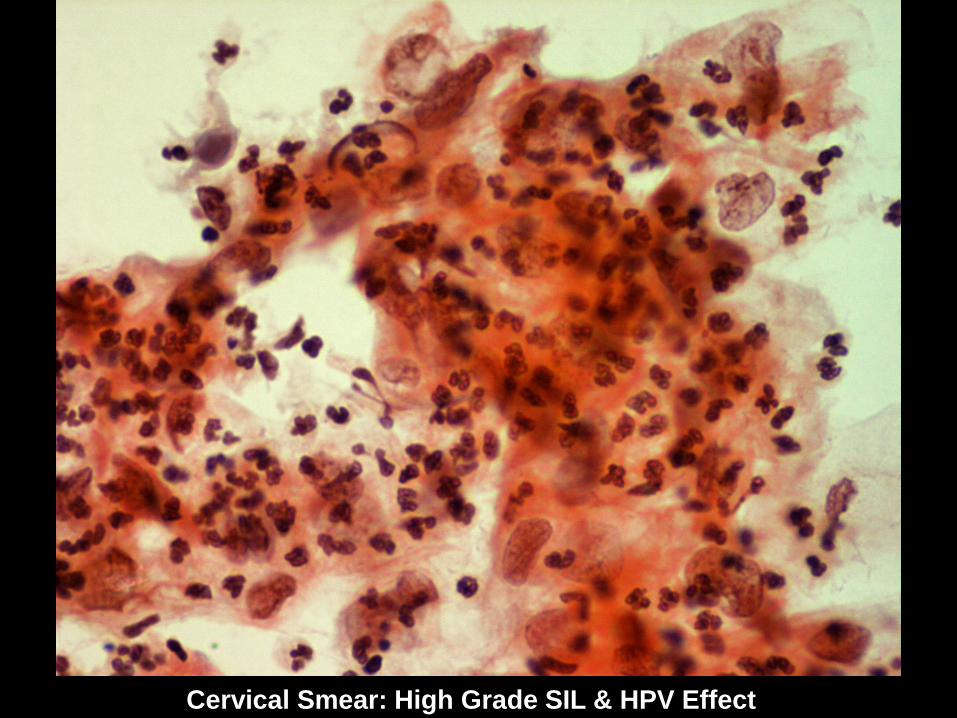
Cervical Smear: High Grade SIL & HPV Effect

Punch Biopsy: CIN III / Carcinoma-in-situ with ? Early Invasion

Punch Biopsy: CIN III / Carcinoma-in-situ

Cone Biopsy: CIN III / Carcinoma-in-situ

Cone Biopsy: CIN III Extending to Endocervical Gland

Cone Biopsy: Microinvasive Squamous Cell Carcinoma
Depth of Invasion = 3.6 mm
Histologic Diagnosis Microinvasive squamous cell
carcinoma At 11 & 12 o’clock (horizontal
spread < 7 mm) Depth of invasion = 3.6 mm

Microinvasive Squamous Cell Carcinoma
Synonym: Superficially invasive CA; CA with early stromal invasion. Corresponds to FIGO stage IA: CA
with maximum depth of invasion = 5 mm & maximum horizontal spread = 7 mm. Capillary-lymphatic space invasion may or may not be present.

Microinvasive Squamous Cell Carcinoma
21% of all cervical squamous cell CA. Overall risk of lymph node metastasis
about 1%: - Invasion up to 3 mm: < 1%. - Invasion of 3.1 – 5 mm: 4.3%. Refined definition: - 3 mm as cutoff point with no capillary-
lymphatic space invasion (Society of Gynecologic Oncology).
- Tumor volume (< 420 mm2).

Updated FIGO Staging of CA Cervix 0 CA-in-situ I CA strictly confined to cervix (extension to
uterus corpus should be disregarded & lymphovascular permeation does not alter the stage).
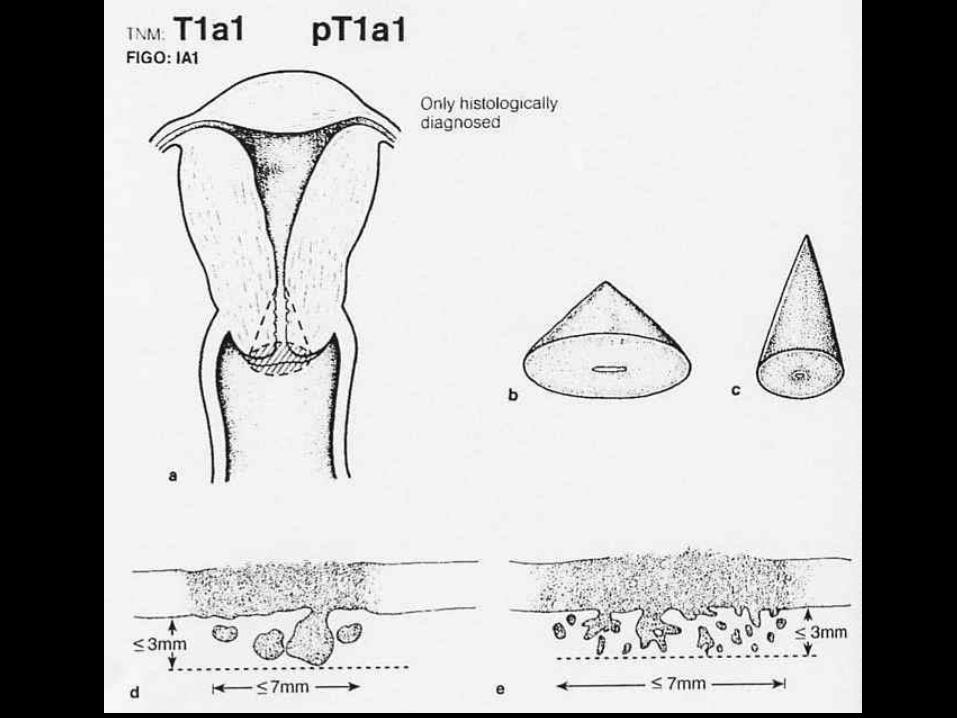
IA Preclinical invasive CA (microinvasive CA), i.e. diagnosed only by microscopy.
- IA1 Stromal invasion 3 mm or less in depth & 7 mm or less in horizontal spread.
- IA2 Stromal invasion > 3 mm & not more than 5 mm in depth, with horizontal spread of 7 mm or less.
IB Clinically visible lesion confined to cervix or microscopic lesion greater than IA2.
Updated FIGO Staging of CA Cervix II Invasive CA that extends beyond uterus, but
not reaching pelvic side wall or lower one-third of vagina.
IIA Without parametrial invasion IIB With parametrial invasion III Invasive CA that extends to either lateral
pelvic wall & / or lower third of vagina & / or hydronephrosis or nonfunctioning kidney due to tumor.
IVA Invasive CA that invades mucosa of urinary bladder & / or rectum or extends beyond true pelvis.
IVB Distant metastasis.







Technical & Practical Problems in Cervical
Biopsies

Types of Cervical Biopsies Colposcopically-directed punch
biopsy Endocervical curettage Cone biopsy LLETZ (large loop excision of the
transformation zone) / LEEP (loop electrosurgical excision procedure)
Technical & Practical Problems in Cervical Biopsies: Punch Biopsy Sampling problems: - Entire transformation zone may not be
visualized & will then not be accessible to biopsy.
- Loss of fragile surface mucosa may lead to false-negative result.
Interpretation problems: - Tangential sectioning may lead to
overestimation of severity of changes or produce artifacts mimicking invasion.
Tips A negative punch biopsy result, where
there is definite abnormality on cytology smears or colposcopy, should be followed by further examination & possibly cone biopsy & should not be considered a conclusive investigation.

Technical & Practical Problems in Cervical Biopsies: Endocervical
Curettage Sampling problems: - Material not obtained under direct
visualization & may not be representative. Interpretation problems: - Fragmentation & poor orientation
makes grading difficult.
Tips A negative endocervical curettage
result sometimes has uncertain diagnostic reliability. If a significant endocervical glandular lesion is suspected on cytology, cone biopsy provides a more reliable investigation.

Technical & Practical Problems in Cervical Biopsies: Cone Biopsy Interpretation problems: - In laser cones, heat artifact at biopsy
edge makes detailed assessment not possible.

Cone Biopsy (Using Laser): Marked Heat Artifact

Cone Biopsy (Using Cold Knife): For Comparison

Technical & Practical Problems in Cervical Biopsies: LLETZ / LEEP Interpretation problems: - Heat artifact can cause nuclear
hyperchromasia, apparent nuclear elongation & crowding in glandular mucosa, resulting in misinterpretation as CIN or AIS.
- Status of resection margins sometimes difficult to assess due to heat artifact & coagulative necrosis.

LEEP Biopsy: Marked Cauterization Artifact

LEEP Biopsy: Marked Cauterization Artifact
Tips Negative cone / LEEP biopsy can be due to: - False-positive cytology - Regression of lesion - Complete ablation by previous punch
biopsy - Insufficient sectioning - Tissue damage (due to heat artifact or loss
of surface mucosa) - Failure to excise the lesion (abnormal
cytology due to vaginal lesion)


















