• Eccentric, not necessarily associated with joint
US findings
• Double contour sign
• Hyperechoic soft tissue area
• Bright dotted foci
• Snowstorm appearance of synovial fluid
• Hypervascularization (Doppler US)
• Tophi with or without posterior shadow
• Soft tissue edema
CT
• CT more sensitive to detect erosion and tophi
.
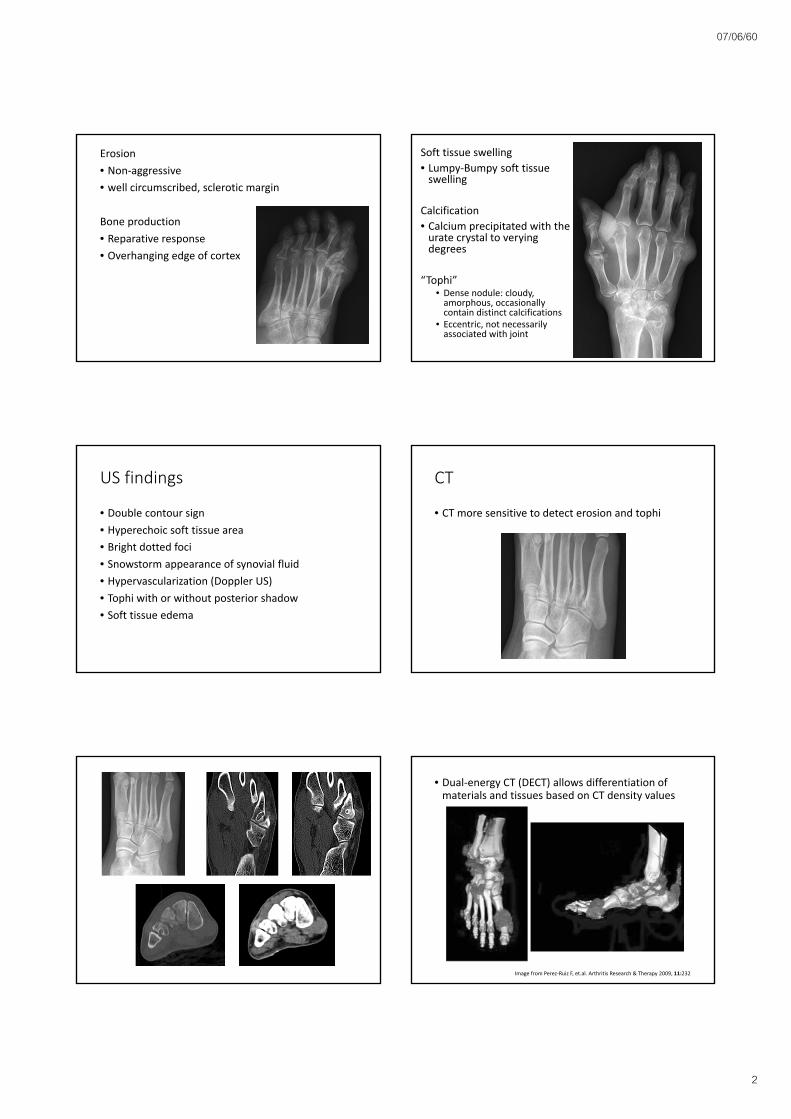
• Dual‐energy CT (DECT) allows differentiation of materials and tissues based on CT density values
Image from Perez‐Ruiz F, et.al. Arthritis Research & Therapy 2009, 11:232
07/06/60
3
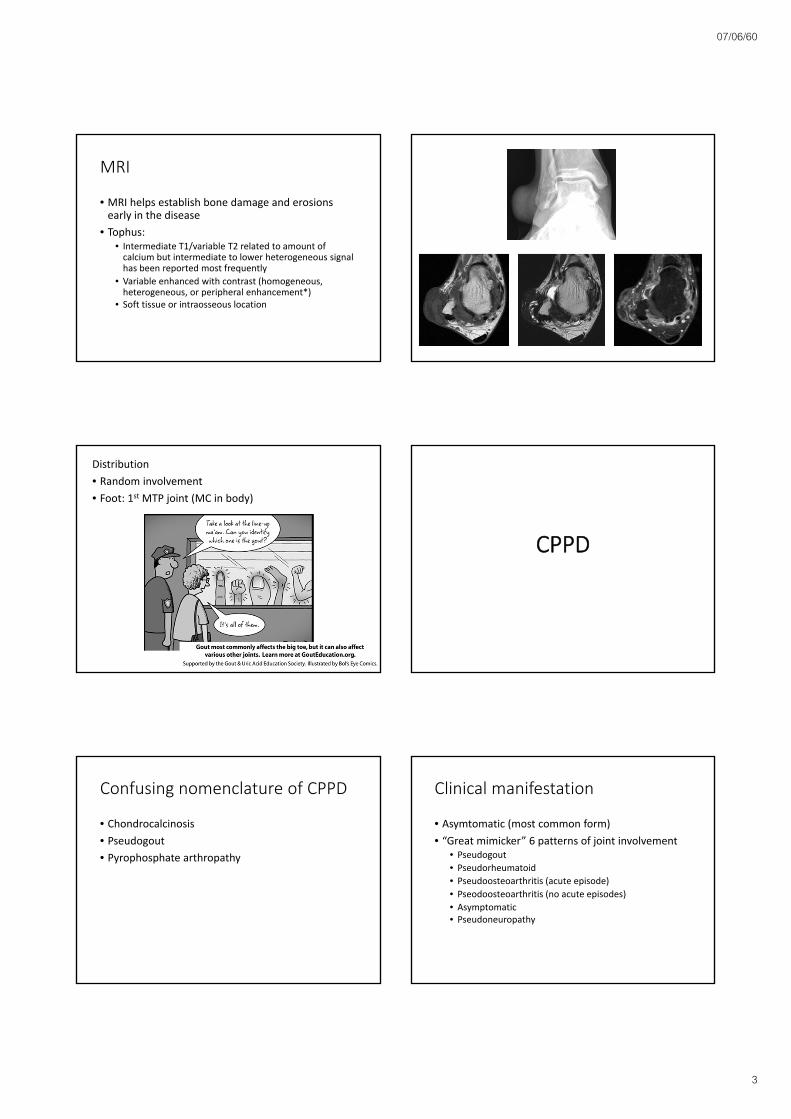
MRI
• MRI helps establish bone damage and erosions early in the disease
• Tophus: • Intermediate T1/variable T2 related to amount of calcium but intermediate to lower heterogeneous signal has been reported most frequently
• Variable enhanced with contrast (homogeneous, heterogeneous, or peripheral enhancement*)
• Soft tissue or intraosseous location
Distribution
• Random involvement
• Foot: 1st MTP joint (MC in body)
CPPD
Confusing nomenclature of CPPD
• Chondrocalcinosis
• Pseudogout
• Pyrophosphate arthropathy
Clinical manifestation
• Asymtomatic (most common form)
• “Great mimicker” 6 patterns of joint involvement• Pseudogout
• Pseudorheumatoid
• Pseudoosteoarthritis (acute episode)
• Pseodoosteoarthritis (no acute episodes)
• Asymptomatic • Pseudoneuropathy
07/06/60
4
Imaging characteristic
• Soft tissue calcification• Chondrocalcinosis
• Synovial and capsular calcification
• Tendon, ligament and bursal calcification
• Pyrophosphate arthropathy
Chondrocalcinosis
• Hyaline cartilage
• Fibrocartilage
Chondrocalcinosis
• Hyaline cartilage
• Fibrocartilage
CT
MRI
• MRI of chondrocalcinosis can be confusion (high or low SI on either T1 or fluid‐sensitive sequences
• Decreased sensitivity and specificity for diagnosis meniscal tear
Synovial and capsular calcification
07/06/60
5
Tendon, ligament and bursal calcification Pyrophosphate arthropathy
• Unusual articular distribution
• Unusual intra‐articular distribution
• Prominent subchondral cyst formation
• Severe & progressive destructive bone changes• Variable osteophyte formation
Hand and wrist involvement
• Radiocarpal joint space narrowing SLAC wrist and stepladder appearance
• The triscaphe joint more commonly affected in CPPD crystal disease than in OA
• Narrowing MCP (especially 2nnd and 3rd) with sparing IP joint
• Drooping osteophytes (radial aspect)• Sclerosis, cysts or collapse metacarpal head
Knee joint
• Isolated patellofemoral compartment
Knee joint
• Isolated patellofemoral compartment
07/06/60
6
HADD
Clinical presentation
• Pain, erythema, swelling, and limitation of motion of the neighboring joint
• Most commonly between the ages of 40 and 70 years (rare in children)
HADD
• Characterized by periarticular calcifications, usually in tendons near their osseous attachments
• Usually monoarticular
• Tends to be self‐limiting with resolution of both clinical and imaging findings
Acute calcific periarthritis
• 60% at shoulder joint (M/C)
• Second most common is hip (gluteus medius near greater trochanter or acetabulum, gluteus maximusattachment along the posterolateral femoral shaft of the femur
• Can see erosive change adjacent to area of deposition
Radiographs Ultrasound
07/06/60
7
HADD and joint abnormality
• OA
• Milwaukee shoulder epitomizes
• HADD athropathy• Elderly
• Mostly women (90%)
• Predilection for large joints (shoulder, hip, knee, elbow)
• Large joint effusion ( hemorrhagic and non‐inflammatory, extensive bone destruction, accerelatedOA, intraarticular bodies









![Electrochemical Study of Under-Potential Deposition .../67531/metadc5372/m2/1/high_res_d/thesis.pdfdeposition of different metals on polycrystalline [5] and single crystal surfaces](https://static.documents.pub/doc/80x56/5e3dd30620d9db0d7548fbd8/electrochemical-study-of-under-potential-deposition-67531metadc5372m21highresdthesispdf.jpg)












