23
Current Challenges in the ICU Prof Craig Williams Institute of Healthcare Associated Infection UWS
| Date post: | 18-Dec-2015 |
| Category: |
Documents |
| Upload: | easter-henderson |
| View: | 214 times |
| Download: | 0 times |
Current Challenges in the ICU
Prof Craig WilliamsInstitute of Healthcare Associated
Infection UWS
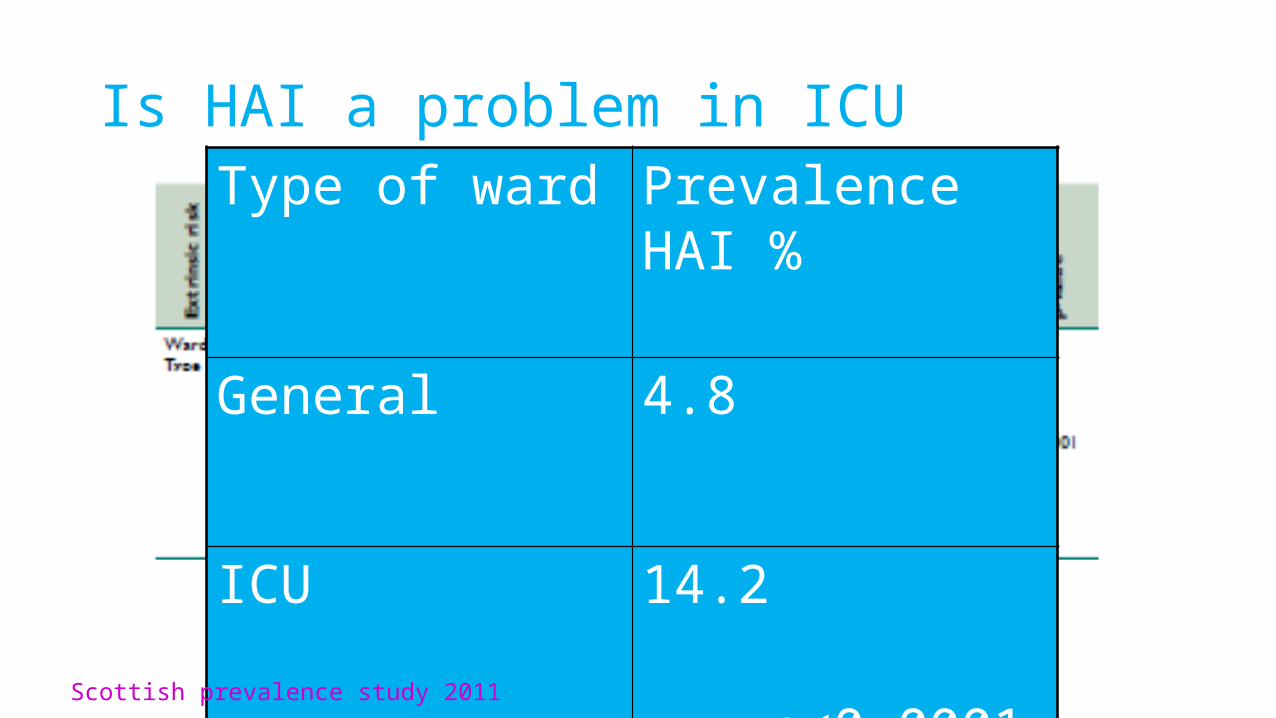
Is HAI a problem in ICUType of ward Prevalence HAI %
General 4.8
ICU 14.2 p<0.0001
Scottish prevalence study 2011
Does it matter?
• Analysis of an American hospital database:
• In-hospital mortality in ICU patients was 4 times higher in patients with
HAI (18.5% vs 4.5%).
• Length of stay in the ICU doubled in patients with HAI, from a mean of
8.1 days to 15.8 days.
• Central catheter use OR, 3.4 or mechanical ventilation [OR, 2.8],
trebled the risk of developing an HAI Joly 22nd European Congress of Clinical Microbiology and Infectious Diseases 2012
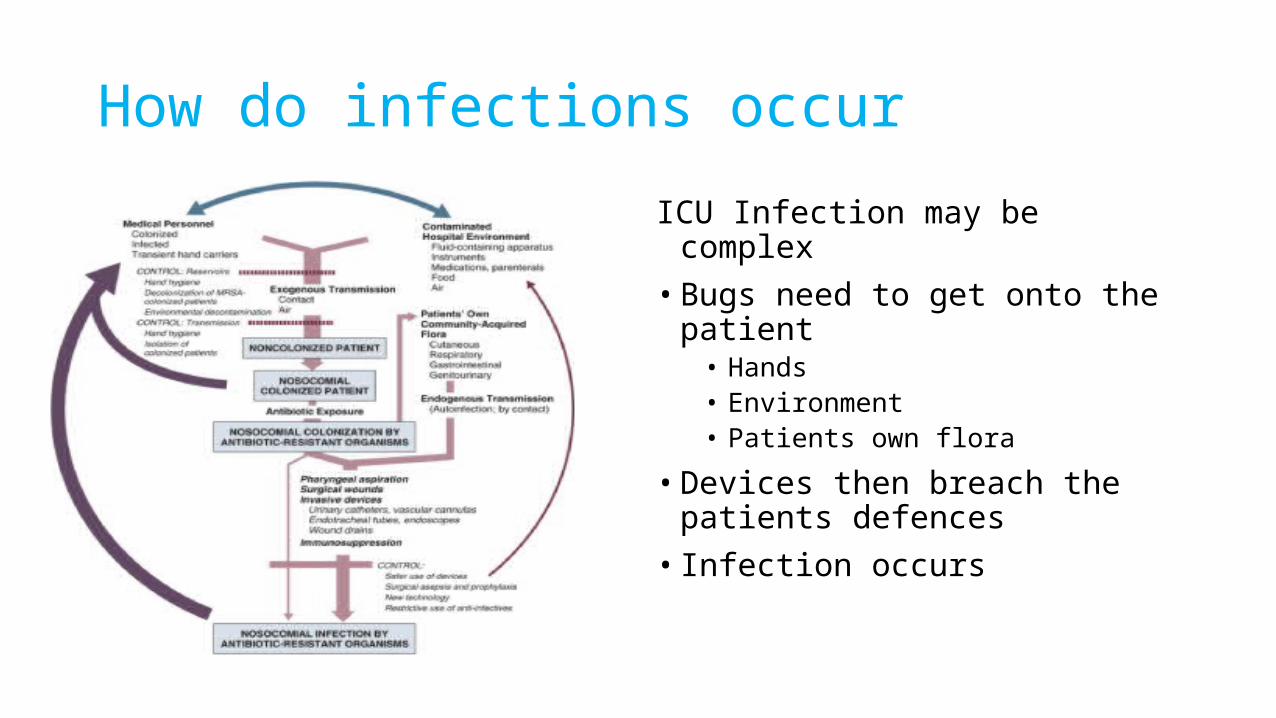
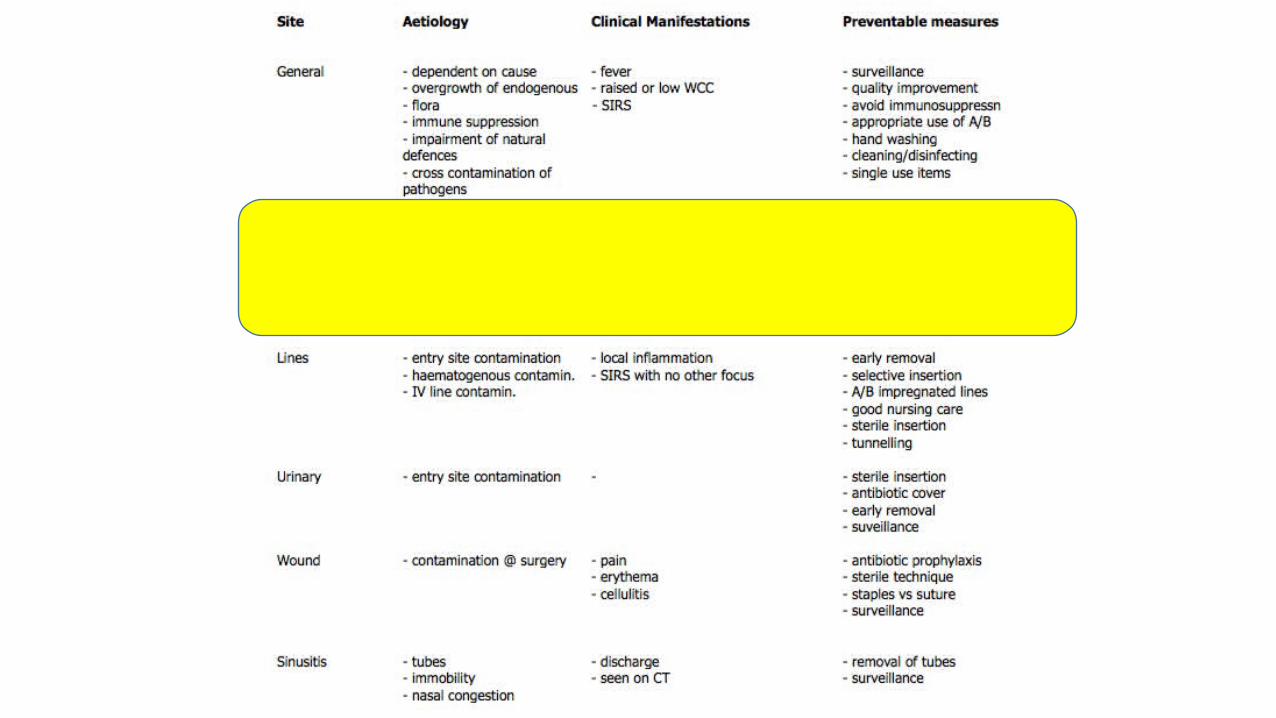
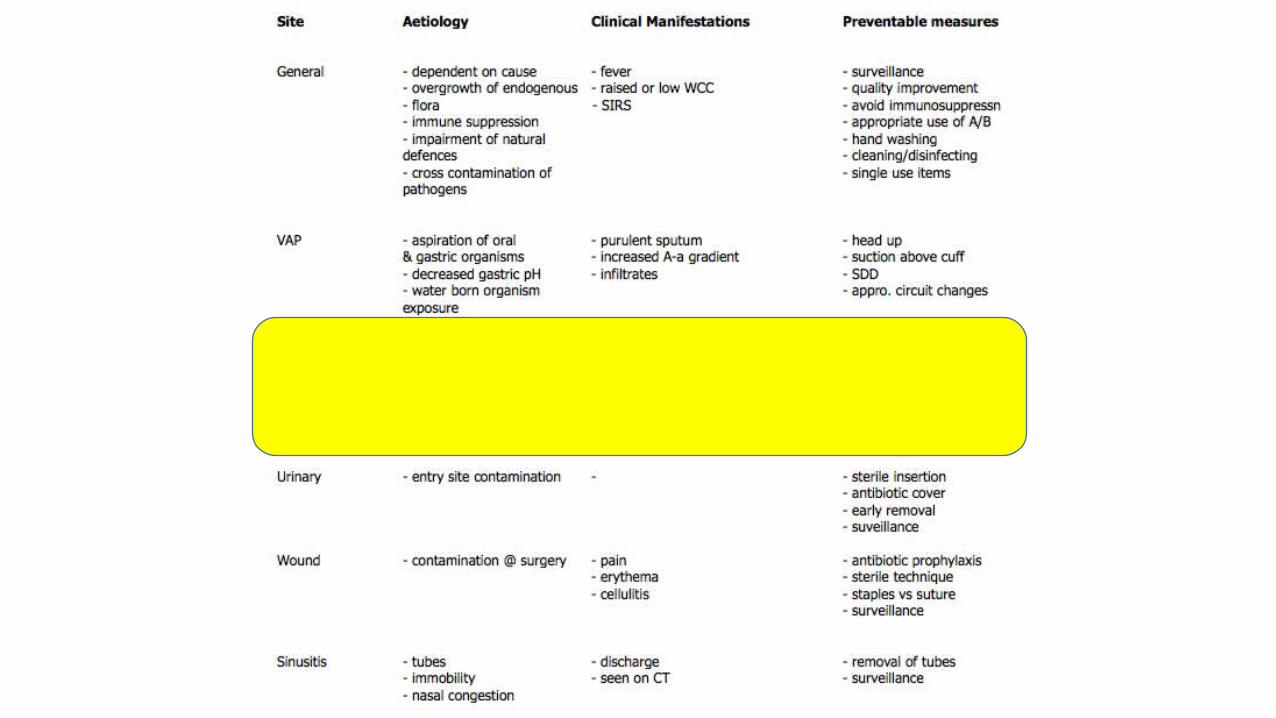
How do infections occur
ICU Infection may be complex• Bugs need to get onto the patient
• Hands• Environment• Patients own flora
• Devices then breach the patients defences
• Infection occurs
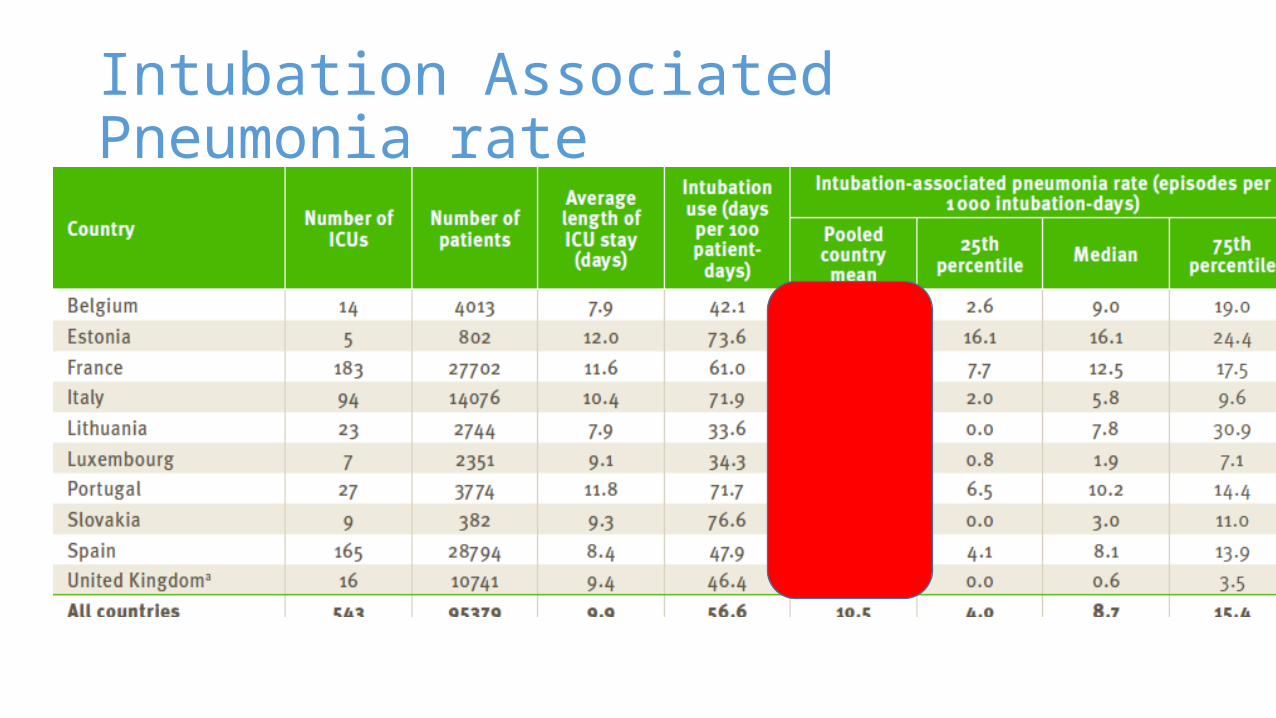
Intubation Associated Pneumonia rate
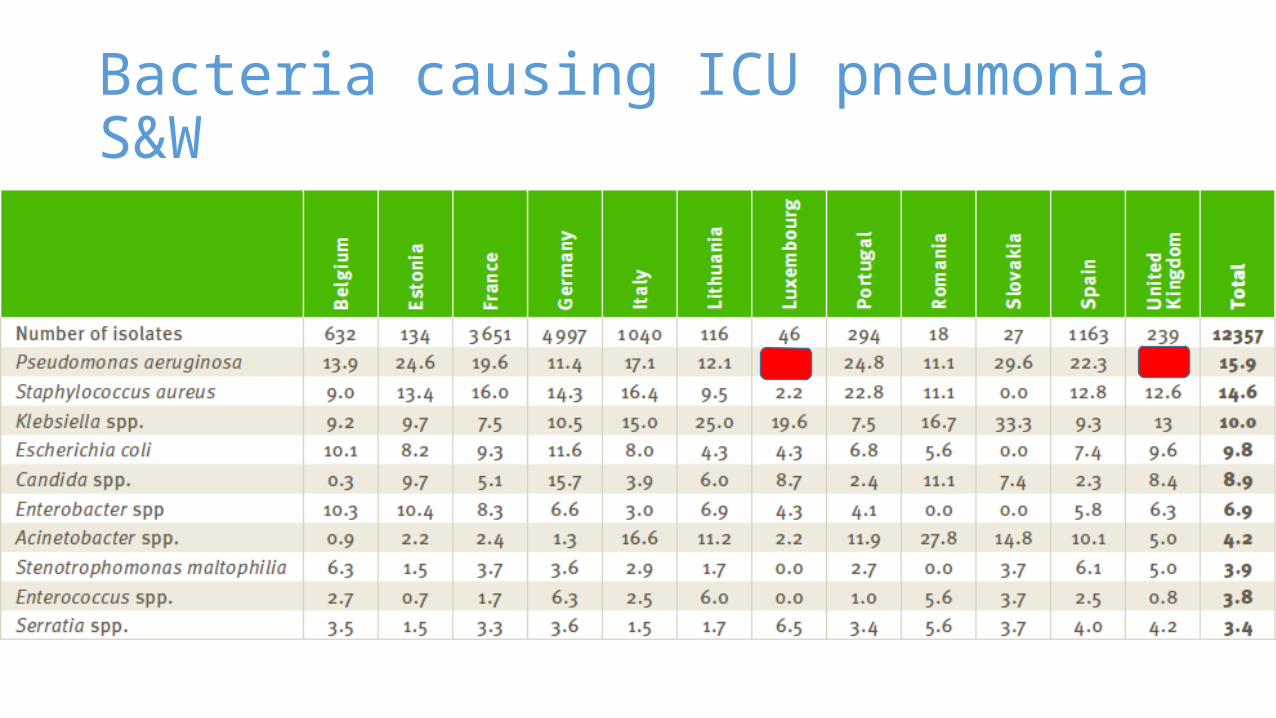
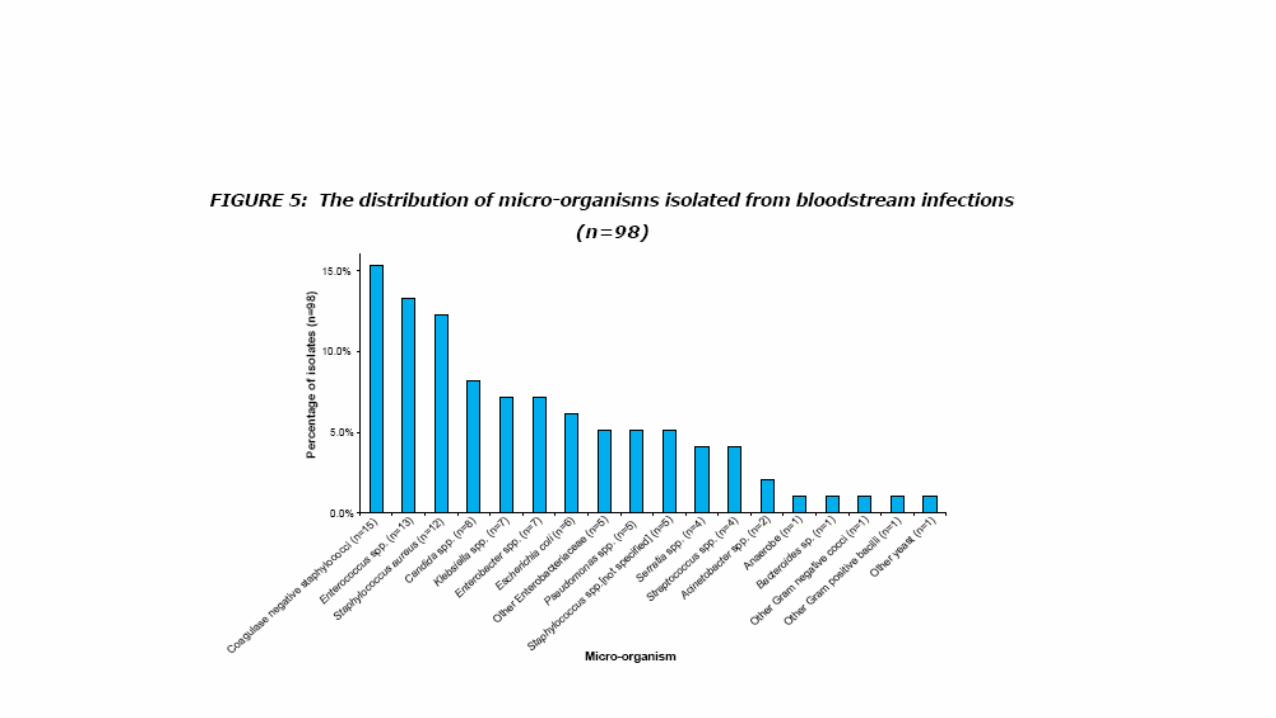
Bacteria causing ICU pneumonia S&W
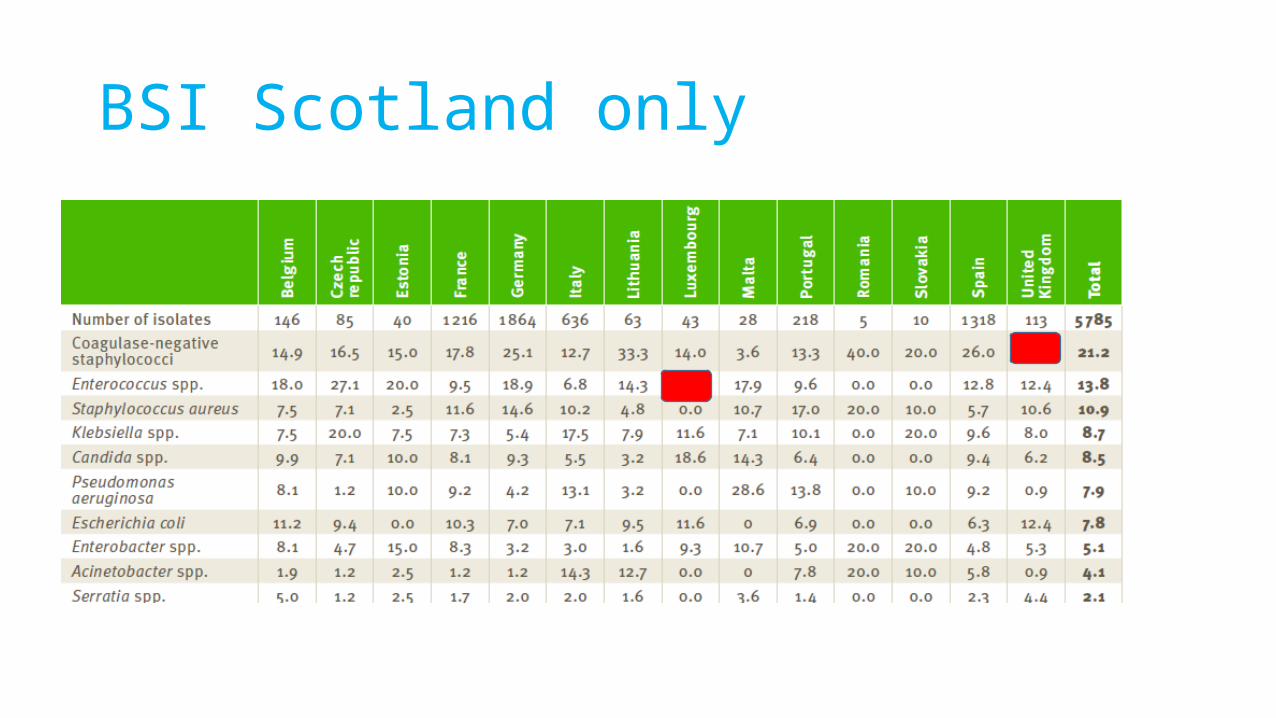
BSI Scotland only
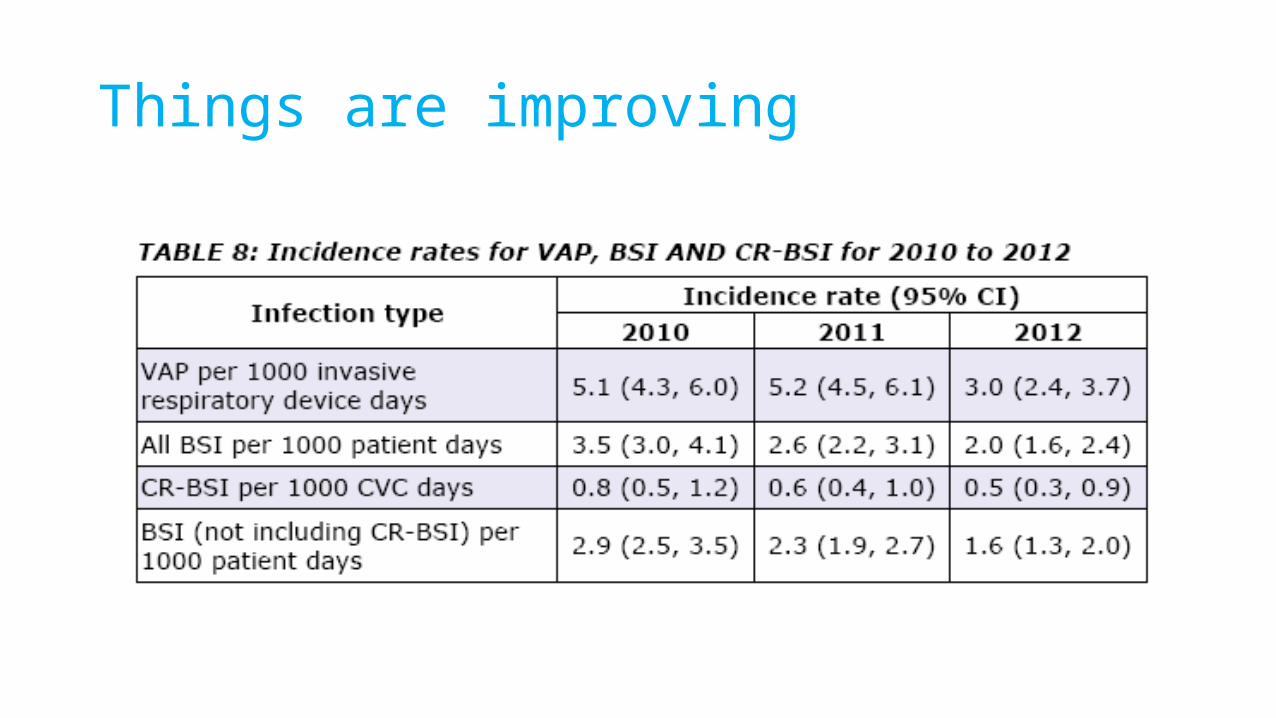
Things are improving
Current Challenges
•We know the bugs•We understand the route of infection•We’ve got the bundles•Why are we still getting HAI
Unit as a whole
Patient Factors
Hospital Environment
Unit as a whole: Effect of Surveillance• 2,771 patients, 19,848 intubation-days• A quasi-experimental study 2004-2010 in two ICUs• Surveillance was interrupted during the year 2007 in unit A and
continuous in unit B• The VAP rate increased in unit A from 7.8% to 17.1% 2 (P <0.001);• in unit B, it was 7.2% and 11.2% (P = 0.17). • All-cause mortality and length of stay increased in unit A (P = 0.028
and P = 0.038), In unit B, no change in mortality was observed (P = 0.22),
• VAP incidence, length of stay and all-cause mortality rose after HAI surveillance disruption in ICU.
Benet Critical Care 2012, 16:R161
Patient factors:Oral Hygiene and VAP • Does dental treatment enhance oral antisepsis, thus preventing (LRTIs)• Observer-blind randomized clinical trial 254 adult patients in ICU • The experimental group (n = 127) had access to dental care provided by a dental
surgeon, 4-5 times a week. Besides routine oral hygiene, care also included teeth brushing, tongue scraping, removal of calculus, atraumatic restorative treatment of caries, and tooth extraction.
• The control group (n = 127) had access to routine oral hygiene only, which included the use of chlorhexidine as a mouth rinse, which was performed by the ICU nurse staff.
• Ventilator-associated pneumonia rates per 1,000 ventilator-days were 16.5 (95% CI, 9.8-29.5) in the control group and 7.6 (95% CI, 3.3-15.0) in the experimental group (P < .05).
Bellissimo-Rodrigues, ICHE 2014 Nov;35(11):1342-8.
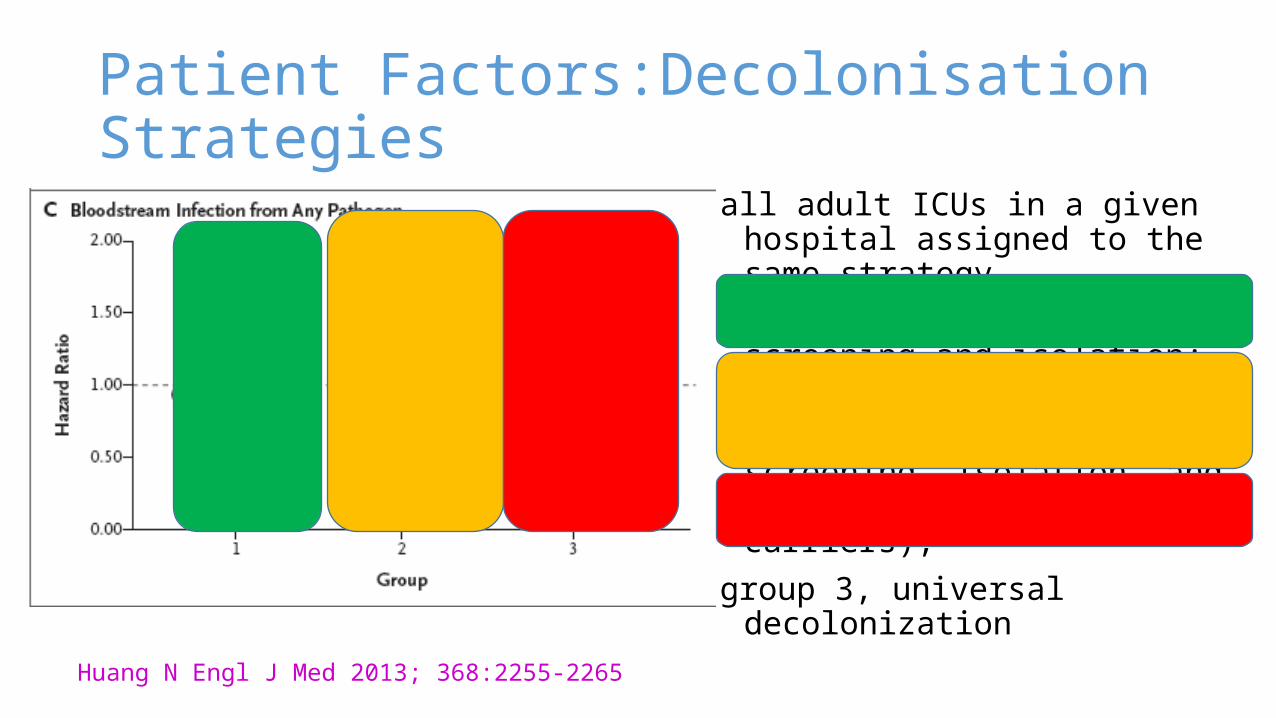
Patient Factors:Decolonisation Strategies
all adult ICUs in a given hospital assigned to the same strategy.
Group 1 implemented MRSA screening and isolation;
group 2, targeted decolonization (i.e., screening, isolation, and decolonization of MRSA carriers);
group 3, universal decolonization
Huang N Engl J Med 2013; 368:2255-2265
Hospital environment: Copper
ICU patients assigned to: traditional patient roomcopper room where bed rails, tables, IV poles, and nurse’s call buttons were made solely from copper-based metals.
Salgado ICHE 2013,34;5:479-86
Hospital environment: Copper
The proportion of patients who developed HAI and/or colonization with MRSA or VRE: copper surfaces (7.1%) traditional rooms (12.3%). The proportion of patients developing HAI with MRSA or VRE
copper rooms (3.4%) traditional rooms (8.1%).
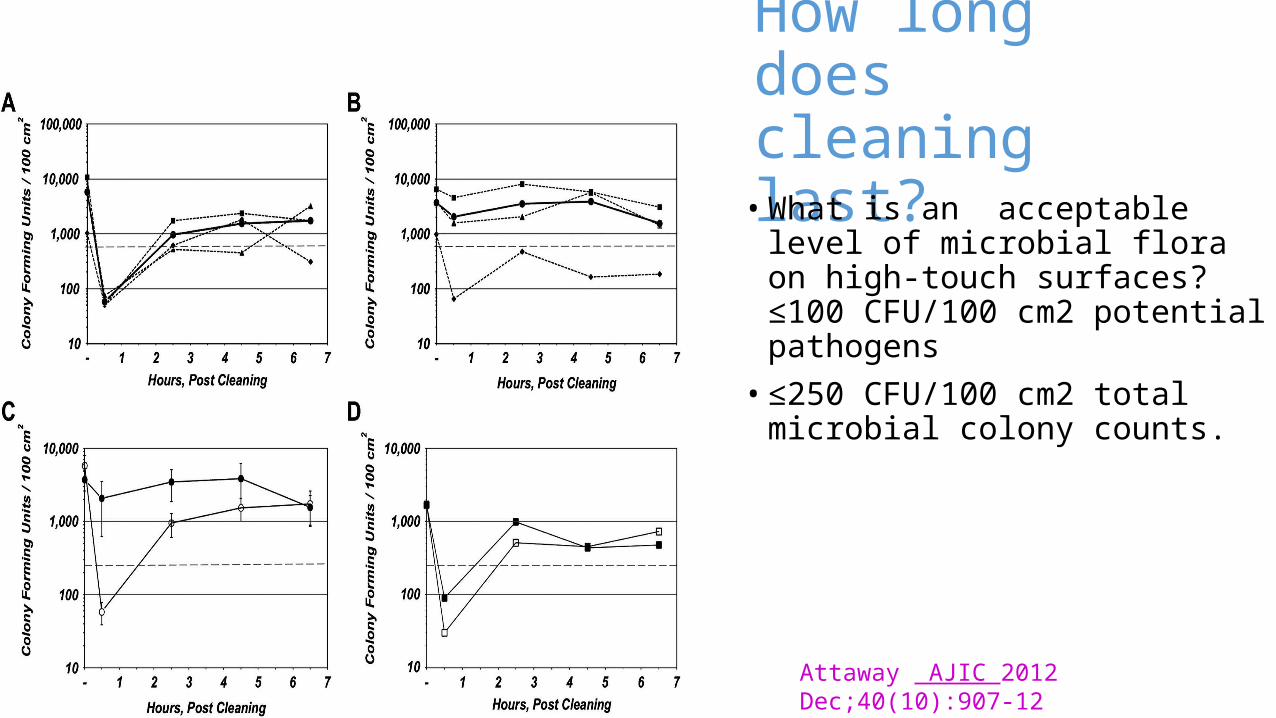
How long does cleaning last?
• What is an acceptable level of microbial flora on high-touch surfaces? ≤100 CFU/100 cm2 potential pathogens
• ≤250 CFU/100 cm2 total microbial colony counts.
Attaway AJIC 2012 Dec;40(10):907-12
Environment, single v multibed roomsRates of acquisition of infectious organisms in an ICU before and after a change from multibed to single rooms.
• The methicillin-resistant S aureus acquisition rate fell by 47% (95% CI,1%-71%)• C difficile acquisition rate fell by 43% (95% CI, 7%-65%), and the • yeast acquisition rate fell by 51% (95% CI, 34%-64%). • No effect was observed on the acquisition rate of coagulase-negative Staphylococcus species,
the most common endogenous organism, for which no change would be expected.
Conversion to single rooms can substantially reduce the rate at which patients acquire infectious organisms while in the ICU.
Teltsch Arch Intern Med. 2011,10;171(1):32-8.
Summary
• HAI in ICU is multifactorial• Many improvements have been made and the number of infections is
decreasing
• Additional further improvements may be made by focusing on• methods of reducing bacterial load/colonisation • The hospital environment• audit

Thanks
PJ Pseudomonas in the Paediatric Intensive care 1.pptx

















