34
Current Clinical Trials in SJIA & MAS Daniel J. Lovell, MD, MPH Joseph E. Levinson Professor and Chair in Pediatric Rheumatology Chairman, Pediatric Rheumatology Collaborative Study Group 1
| Date post: | 28-Jan-2018 |
| Category: |
Science |
| Upload: | systemic-jia-foundation |
| View: | 206 times |
| Download: | 3 times |

Current Clinical Trials in SJIA & MAS
Daniel J. Lovell, MD, MPH
Joseph E. Levinson Professor and Chair in Pediatric Rheumatology
Chairman, Pediatric Rheumatology Collaborative Study Group
1

Recent Clinical Trials in SJIA
• Recent breakthroughs have been the testing of inflammatory mediators known to have a central role in the SJIA disease process
– Interleukin 1- Anakinra (Kineret) and Canakinumab (Ilaris)
– Interleukin 6- Tocilizumab (Actemra)
• Ilaris and Actemra have been approved by the FDA for the treatment of SJIA
2

Effects of Interleukin 1
3

Fever Joint Inflammation
Growth Impairment
Interleukin-6 in sJIA
Anemia
Thrombocytosis
J Exp Med 1998
J Clin Invest 1997Endocrinol 2001
A&R 1991
A&R 1991
Lancet 1995Blood 1996
J Clin Invest 1994
IL6/soluble IL6R and CRP
MASOsteoporosis
A&R 2006
JIA CLINICAL TRIAL METHODS AND DEFINITIONS
5

JIA core set and response criteria� JIA core set
1. Physician global assessment of overall disease activity2. Parent or patient global assessment of overall well-being 3. Functional ability (CHAQ)4. Number of joints with active arthritis5. Number of joints with limited range of motion6. Index of inflammation: ESR or CRP7. (FEVER for systemic JIA)
� ACR Criteria: 3/6 core set variables improved ≥ 30% (50%, 70%, 90%, 100%) with no more than 1/6 worsened by >30% (AND NO FEVER)
� FDA and EMA acceptedGiannini, Ruperto et Al. Arthritis Rheum 1997

JIA clinical inactive disease/remission� Inactive disease
– No joints with active arthritis– No fever, rash, serositis, splenomegaly, or generalized
lymphadenopathy attributable to JIA– No active uveitis (to be defined)– Normal ESR or CRP– No disease activity according to MD evaluation– Morning stiffness ≤ 15 minutes
� Clinical remission– On medication for 6 months and – off medication for 12 months
Wallace, Ruperto et al J Rheumatol 2004Wallace…for CARRA/PRINTO/PRCSG. Arthritis Care Res 2011

BLINDED WITHDRAWAL STUDIES
Screen
Blinded Follow-Up
Placebo Arm
Experimental Arm
En
d O
f Stu
dy
All subjects receive experimental therapy for several months
Responders Randomized
Flares go to Open3-6 moopen
Open label extension

S1
S2
S3
S4
S5
S6
S7S8
S9
0
3
6
9
12
Baseline 1 week 1 month follow-up
S1
S2
S3
S4
S5S6
S7
S8S9
baseline 1 week 1 month follow-up
n. o
f ac
tive
join
ts
CR
P (m
g/dL
)
A
NS
P = 0.005
P = 0.005P = 0.005
P = 0.005
P = 0.005 P = 0.005
B
S10
S10
0
2
4
6
8
10
12
14
16
18
2030
Gattorno et al, Arthritis Rheum 2008
Anti IL-1 (anakinra) and systemic JIA
Pascual et al: J Exp Med 2005

Anakinra in systemic JIA: study design
Quartier et al. Annals Rheum Dis 2012

Anakinra in systemic JIA (1 month results)
Response Anakinra (N=12)
Placebo (N=12)
P value
Mod ACR 30 10 (83%) 3 (25%) 0.004
Mod ACR 50 7 (58%) 0 0.005
Mod ACR 70 5 (42%) 0 0.038
Mod ACR 100 0 0 1
Quartier et al. Annals Rheum Dis 2012

Long-term Efficacy and Safety of Canakinumab in Patients With Active Systemic Juvenile Idiopathic Arthritis
(SJIA): Results From a Phase III Extension Study
H. I. Brunner1, N. Ruperto2, P. Quartier3, T. Constantin2, E. Alexeeva2, I. Kone-Paut4, K. Marzan2, N. Wulffraat2, R. Schneider1, S. Padeh2, V. Chasnyk2, C. Wouters2, J. B. Kuemmerle-Deschner2, T. Kallinich2, B.
Lauwerys5, E. Haddad2, E. Nasonov2, M. Trachana2, O. Vougiouka2, K. Leon6, E. Vritzali7, K. Lheritier7, A. Martini2, D. Lovell1
1PRCSG, Cincinnati, United States; 2PRINTO-Istituto Gaslini, Genoa, Italy; 3Necker-Enfants Malades Hospital, Paris; 4Bicêtre hospital, Paris Sud, France; 5Cliniques Universitaires Saint-Luc and Université Catholique de Louvain, Brussels, Belgium; 6Novartis Pharmaceuticals Corporation,
East Hanover, United States; 7Novartis Pharma AG, Basel, Switzerland

13
Patients aged ≥2 to <20 yrs, with active SJIA features (≥2 of the following): 1. Spiking intermittent fever of >38°C for 1 day within
1 week of baseline
2. ≥2 joints with active arthritis
3. CRP levels of >30 mg/L [normal <10 mg/L]
4. Rash, serositis, lymphadenopathy and hepatosplenomegaly were included
MethodsEligibility Criteria

14
ResultsDemographics and Baseline Disease Characteristics
Variable OverallN=123
Age (years), mean (SD) 9.0 (4.5)
Female, n (%) 75 (61.0)
Predominant race: Caucasian, n (%) 111 (90.2)
Fever at entry, n (%) 70 (57.0)
Presence of systemic signs after first 6 months of disease, n (%) 95 (77.2)
Time from SJIA diagnosis to study entry (years), mean (SD) 2.66 (3.27)
Prior use of other biologics, n (%) 32 (26.0)
CRP at baseline (mg/L), median (Q1, Q3) 79 (22.0, 170.0)
PGA (VAS, mm), median (Q1, Q3) 54.7 (39.0, 70.0)
Number of active joints median (Q1, Q3) 5.0 (3.0, 14.0)
Number of joints with limitation of motion, median (Q1, Q3) 5.0 (2.0, 12.0)
CHAQ score, median (Q1, Q3) 1.37 (0.62, 2.0)
JADAS10-CRP, median (Q1, Q3) 22.3 (17.2, 28.0)
JADAS27-CRP, median (Q1, Q3) 21.5 (16.8, 28.4)
Mean prednisone-equivalent dose (mg/kg/day) (SD) 0.95 (2.3)

15
Canakinumab treatment provided a rapid response at Day 15. Over 50% of patients had aACR70 responses; 23.5% had aACR100 responses at Day 15
At last assessment, 67% of patients had aACR ≥70 responses and 51% were aACR100
ResultsEfficacy: aACR Responses in Naïve Patients

16
ResultsEfficacy: Clinical remission on medication
*At least 6 consecutive months of inactive disease; #at least 12 consecutive months of inactive disease
#
% o
f 12
3 p
atie
nts

17
SAEs were reported in 40 (32.5%) patients No deaths occurred
Results: Rates of Most Common Serious Adverse Events (SAEs)
SAEs by preferred term (>2 events) Canakinumab (N= 123; rate /100 pt days)
Total SAEs, n (incidence rate/100 Pt days)* 103 (0.15)
Juvenile idiopathic arthritis flare 16 (0.02)
Macrophage activation syndrome 8 (0.01)
Fever 5 (0.01)
Pneumonia 3 (<0.01)
Lymph node inflammation 3 (<0.01)
Lymph node enlargement 3 (<0.01)
Hepatitis toxic 2 (<0.01)

18
Rapid response and sustained therapeutic efficacy were demonstrated in canakinumab-naïve patients with active SJIA
• More than 50% of the patients achieved aACR 70 response by Day 15, and the response was sustained until last assessment
• At least 50% with inactive disease at the last assessment
• Almost 1/3 of the patients were in clinical remission for 1 year
No new safety findings were observed upon long-term use of canakinumab, and the safety profile was consistent with that observed in the pivotal program
Conclusions

Efficacy and Safety of Tocilizumab (TCZ) in Patients with Systemic
Juvenile Idiopathic Arthritis (sJIA): TENDER 52-Week Data
F. De Benedetti, H. Brunner, N. Ruperto, I. Calvo, R. Cuttica, C. Malattia, R. Schneider, P. Woo, C. Wouters, R. Xavier, L. Zemel, S. Wright,
A. Kenwright, D. Lovell, A. Martini

TENDER: 12-Week Randomized, Double-blind, Placebo-Controlled, Parallel Group, 2-Arm Study (Part I) with Single Arm Open-label Extension (Parts II and III)—5 Years in Total
Open-Label Period (Parts II - III)
Tocilizumab 8 or 12 mg/kga every 2 weeks for
92 weeks (subsequent 3-year extension added)
Double-Blind Period (Part I)
Tocilizumab 8 or 12 mg/kga x 6
Placebo x 6
75 pts
37 pts
Scr
een
ing
& R
and
om
iza
tio
n
0
Escape with rescue therapy
2 4 6 8 10 12 WeekDay 3
Study Design

TENDER: Key Inclusion Criteria
• Diagnosis of sJIA according to ILAR criteria
• Age 2–17 years
• Persistent disease activity for ≥6 months, with an inadequate response to corticosteroids and NSAIDs due to toxicity or lack of efficacy
• ≥5 active joints OR ≥2 active joints with fever >38°C
• Maximum dose of oral corticosteroids: 0.5 mg/kg/day of prednisone equivalent
• Stable dose of oral corticosteroids, MTX, and/or NSAIDs
• No other DMARDs or biologic allowed

TENDER: Efficacy in Double-Blind Phase
24.3
85.3
0
20
40
60
80
100
Placebo(n=37)
TCZ (n=75)
61.5% (95% CI: 44.9–78.1)*,†
n=9 n=64
JIA ACR30 + Absence of Fever at Week 12
JIA ACR 50/70/90 responses at Week 12
10.8
90.7
8.1
85.3
5.4
70.7
0
20
40
60
80
100
JIAACR50
JIAACR70
JIAACR90
Placebo (n=37) TCZ (n=75)
†
†
†
Res
po
nd
ers
(%)
Res
po
nd
ers
(%)

TENDER: Demographic and Baseline Characteristics
N = 112Age (y), mean (SD) 9.7 (4.6)
Disease duration (y), mean (SD) 5.2 (4.1)
Number of previous DMARDs, mean (SD) 1.3 (1.2)
Number of previous biologics, mean (SD) 1.8 (1.4)
Physician VAS, mean (SD) 64.9 (22.3)
Parent/patient VAS, mean (SD) 58.7 (24.4)
Number of active joints, mean (SD) 19.8 (15.7)
Number of joints with LOM, mean (SD) 19.8 (15.6)
ESR (mm/hr) mean (SD) 57.6 (34.2)
CHAQ, mean (SD) 1.7 (0.9)
CRP (mg/l), mean (SD) 166.43 (349.25)
Fever (last 7 days), n (%) 48 (43)
Background oral corticosteroid dose, (mg/kg/day PDN eq), mean (SD) 0.30 (0.20)

TENDER: JIA ACR Responses + Absence of Fever Over 52 Weeks
N = 112*20
40
60
80
100
0 6 12 18 24 30 36 42 48 54Time (weeks)
Res
po
nse
(%
)
JIA ACR30 + absence of fever JIA ACR50 + absence of fever
JIA ACR70 + absence of fever JIA ACR90 + absence of fever
2 52
0

TENDER: Mean Active Joints and Joints with Limited Motion Over 52 Weeks
112 111 111 110 105 107 105 99n =
02468
101214161820
Mea
n ±
SE
Jo
int
Co
un
t
Active Joints (71 Joints)
Joints with Limited Motion (67 Joints)
0 6 12 18 24 30 36 42 48 54Time (weeks)
2 52

TENDER: Mean Oral Corticosteroid Dose Over 52 Weeks
0.3
0.06
0.00
0.05
0.10
0.15
0.20
0.25
0.30
0.35
0 6 12 18 24 30 36 42 48 54Time (weeks)
112112 112 109 109 109 108 99n =
522
Mea
n ±
SE
do
se (
mg
/kg
/day
)
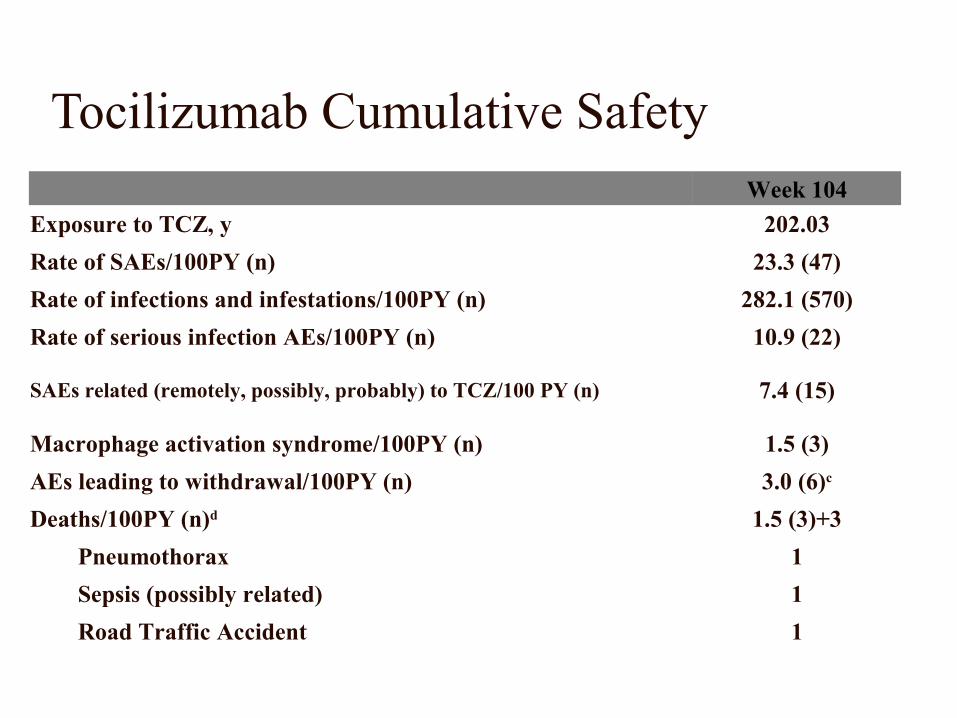
Tocilizumab Cumulative Safety Week 104
Exposure to TCZ, y 202.03
Rate of SAEs/100PY (n) 23.3 (47)
Rate of infections and infestations/100PY (n) 282.1 (570)
Rate of serious infection AEs/100PY (n) 10.9 (22)
SAEs related (remotely, possibly, probably) to TCZ/100 PY (n) 7.4 (15)
Macrophage activation syndrome/100PY (n) 1.5 (3)
AEs leading to withdrawal/100PY (n) 3.0 (6)c
Deaths/100PY (n)d 1.5 (3)+3
Pneumothorax 1
Sepsis (possibly related) 1
Road Traffic Accident 1
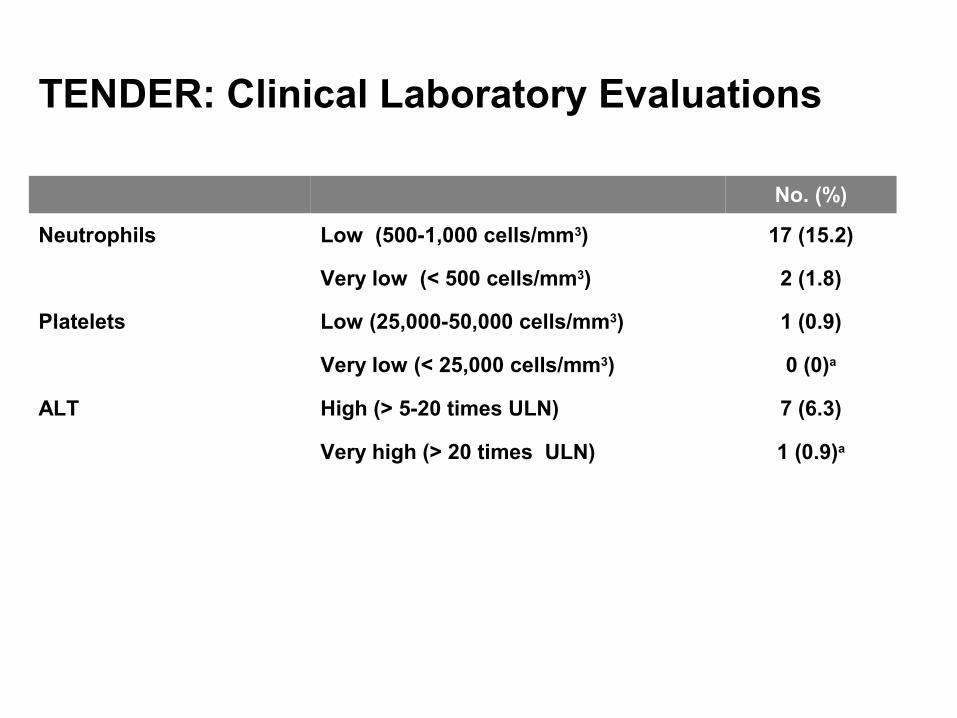
TENDER: Clinical Laboratory Evaluations
No. (%)
Neutrophils Low (500-1,000 cells/mm3) 17 (15.2)
Very low (< 500 cells/mm3) 2 (1.8)
Platelets Low (25,000-50,000 cells/mm3) 1 (0.9)
Very low (< 25,000 cells/mm3) 0 (0)a
ALT High (> 5-20 times ULN) 7 (6.3)
Very high (> 20 times ULN) 1 (0.9)a

Tocilizumab Conclusions
• Year 1 results from this first global phase 3 study demonstrated that tocilizumab was highly effective for the treatment of sJIA
– The response to tocilizumab increased over time
– Over 50% of the patients were able to discontinue oral corticosteroids by week 52
– 55% in inactive disease status by week 52
• In this population of sJIA patients, tocilizumab exhibited an acceptable safety profile

MAS and IL-1 and IL-6 treatment
• Cases of MAS have occurred in both clinical trials even in patients with very well controlled disease
• Treatment with either IL-1 or IL-6 does not seem to increase the risk for MAS- the rate is the same or less than in overall SJIA
• Causes of MAS are the same as the general population
– Infection
– Flare of SJIA
– No obvious explanation
• Manifestations of MAS and response to treatment generally the same as MAS in those not on biologic therapy – With MAS and canakinumab lower ferritin compared to those not on
canakinumab
– With MAS and tocilizumab less often fever and more severe lab abnormalities compared to those not on tocilizumab
30

Earlier treatment with anti IL-1?
…It is possible, but far from proven, that anakinra or other biologic agents may take advantage of a «window of opportunity» in which disease pathophysiology can be altered to avoid chronic arthritis. Testing this hypothesis represents and important scientic priority in pediatric rheumatology
PA Nigrovic

What’s next
� Test effect of earlier treatment with biologics� Determine if biologics have effect on joint
erosions/narrowing� Determine clinical or lab tests that can predict
response/steroid discontinuation/clinical remission� Determine long term safety and efficacy data� Entirely new mechanism of action- JAK kinase
inhibition- tofacitinib in SJIA trial starting now in many PR centers

Roles for JAK in Arthritis

Overall Conclusions
• Both IL-1 and IL-6 blocking biologics represent huge breakthroughs in the treatment of SJIA especially in those with systemic features
• Other companies are developing other IL-1 and IL-6 blocking biologics that will likely have similar results
• Frequency and causes of MAS are similar with or without these treatments but manifestations are slightly different
• Effect of early onset treatment with either IL-1 or IL-6 is being evaluated
• Other types of treatments such as tofacitinib (a pill) will be tested in SJIA very soon
34

















