CURRENT INDIAN EYE RESEARCH 49 Current Indian Eye Research Journal of Ophthalmic Research Group (Peer reviewed open access journal) Editor: Dr Sambuddha Ghosh Associate Editor: Dr. Somnath Mukhopadhyay Editorial Office: 16B Prince Golam Mohammad Road, Kolkata- 700026 Contact: Phone: 033 40071886 E-mail: [email protected]Contents Editorial 50 Sambuddha Ghosh Review Article Autologous Ex-Vivo Cultivated Limbal Transplantation for the Treatment of Unilateral Limbal Stem Cell Deficiency 51 Sayan Basu, Virender S Sangwan Osteo-Odonto Keratoprosthesis (OOKP): A Review of Surgical Techniques and Clinical Outcomes 58 Sayan Basu Original Article Synthesis Of Nanoparticles As A Probe For Diagnosis Of Dry Eye Disease 63 Mohammad Azharuddin, Anjan Kr Dasgupta, Himadri Datta A Study Of Correlation Of Plasma Homocysteine With Serum Lipid Profile In Retinal Vein Occlusion 68 Kapil Deb Lahiri, Arunava Kundu, Joya Ghosh, Mriganka Baruah, Champakali Biswas, Amitava Das, Nazneen Nazm Texture Quantification Of Choroidal Neovascularization Images Through Differential Box Counting Method 73 Sandeep V Paranjape, Sangmeshwar S Pendalwar, Ajoy K Ray, Jyotirmoy Chatterjee, Sambuddha Ghosh Case Report Unusual Manifestation Of Ocular Tuberculosis Presenting As Corneal Fistula 76 Somnath Mukhopadhyay, Debjani Mishra Research Methodology Sample Size Calculation For Research Studies In Ophthalmology 78 Arun Sharma History of Ophthalmology History Of Endeavour: Ophthalmology In India 82 Simantini Bhattacharya Author Guideline 84 Cover photo: Transmission electron microscopy of gold nano particles using tear proteins from dry eye patients For free circulation Volume 1, Issue 2, December 2014
Transcript
CURRENT INDIAN EYE RESEARCH 49
Current Indian Eye ResearchJournal of Ophthalmic Research Group
(Peer reviewed open access journal)
Editor:Dr Sambuddha Ghosh
Associate Editor:Dr. Somnath Mukhopadhyay
Editorial Office:16B Prince Golam Mohammad Road,Kolkata- 700026
Texture Quantification Of Choroidal NeovascularizationImages Through Differential Box Counting Method 73
Sandeep V Paranjape, Sangmeshwar S Pendalwar,Ajoy K Ray, Jyotirmoy Chatterjee, Sambuddha Ghosh
Case ReportUnusual Manifestation Of Ocular Tuberculosis Presenting AsCorneal Fistula 76
Somnath Mukhopadhyay, Debjani Mishra
Research MethodologySample Size Calculation For Research Studies In Ophthalmology 78
Arun Sharma
History of OphthalmologyHistory Of Endeavour: Ophthalmology In India 82
Simantini Bhattacharya
Author Guideline 84
Cover photo: Transmission electronmicroscopy of gold nano particles usingtear proteins from dry eye patients
For free circulation
Volume 1, Issue 2, December 2014
CURRENT INDIAN EYE RESEARCH50
Editorial
Lack of research publications with multidisciplinary approach is an area that needs attention from Indian Ophthalmologists.In the previous issue I announced that Current Indian Eye Research plans to publish articles based on researchesconducted in the Indian perspective with special thrust on inter disciplinary research. Emerging issues in ophthalmologywas promised special place in this journal. In this issue I am happy to publish all the original articles based onmultidisciplinary research.
The last decade has seen progress in nanomedicine with development of various nanoparticles for therapy and diagnosis1.Authors here report a nano-clustering based synthesis of nanoparticles as a probe for diagnosis of dry eye disease.
Texture information from an image is a useful method of image analysis. Texture quantification of choroidal neovascularmembrane on fluorescein angiography image may add useful information in the diagnosis of this disease. In this issuewe publish one multi institutional research report on this subject.
Dyslipidemia2 and hyperhomocysteinemia3 are considered independent risk factors for retinal vein occlusion, the secondmost common retinal vascular disorder. We publish one article on relation between these two risk factors in retinal veinocclusion.
Sample size is a very important component of research design. We publish an article on how to calculate sample size inophthalmic research. I hope this article with useful examples will be of help for serious ophthalmic researchers.
Autologous ex-vivo cultivated limbal epithelial transplantation for the treatment of limbal stem cell deficiency in ocularsurface disease following chemical or thermal burns is a relatively new technique of management. We publish a reviewon this subject in this issue. We also publish a review on osteo-odontokeratoprosthesis, a ray of hope for the hopeless.
I thank all the contributors and our readers for the overwhelming response, the words of encouragement and advice wereceived after the publication of our first issue.
Reference
1. Singh R, LillardJr JW. Nanoparticle-based targeted drug delivery. Experimental and molecular pathology 2009;86:215-23.
2. O'Mahoney PR, Wong DT, Roy JG. Retinal vein occlusion & traditional risk factors for atherosclerosis. Arch Ophthalmol2008; 126: 692-9.
3. Chau B, Kifley A, Wong TY, Mitchell P. Homocysteine and retinal vein occlusion: population based study. Am JOphthalmol 2005; 139: 181–2
Autologous Ex-Vivo Cultivated Limbal Transplantation for theTreatment of Unilateral Limbal Stem Cell DeficiencySayan Basu1, Virender S Sangwan1
1Cornea and Anterior Segment Services, Sudhakar and Sreekanth Ravi Stem Cell Biology Laboratory, Hyderabad Eye Research Foundation, L VPrasad Eye Institute, Kallam Anji Reddy Campus, Road No.2, Banjara Hills, Hyderabad-500034, IndiaCorresponding Author : Dr. Virender S Sangwan, E-mail: [email protected] on : 25/01/2015, Accepted on : 03/02/2015Conflict of Interest : None, Financial Disclosure : None
Ocular surface disease following chemical or thermalburns is a rare but severe form of corneal blindness.
Initially corneal surgeons believed that like other cornealdiseases, corneal transplantation could restore cornealtransparency and vision. In fact, the first successful cornealtransplantation, by the Austrian surgeon Dr Eduard Zirmin 1905, was in the left eye of a farmer with bilateral chroniclime burns.1,2 However, with experience corneal transplantsurgeons realized that almost all corneal grafts performedfor ocular burns failed within a year because of recurrenceof epithelial defects and vascularization.3 In the late 1970sand early 1980s Dr Richard Thoft showed in a small seriesof cases that autologous conjunctival transplantation asopposed to corneal transplantation was effective instabilizing the corneal surface and moderately improvingvision in eyes with ocular burns.4 He later proposed thatthe limbus and not the conjunctiva was the source ofcorneal epithelium hinting that adult corneal epithelial stemcells could be present at that location.5 Soon in 1986, Sunand associates actually demonstrated the presence ofstem-cell like cells in the basal layers of the limbus whichwere slow-cycling, did not express cytological markers foreither the conjunctiva or the cornea and were capable ofproliferation in-vitro.6 This discovery led to a paradigm shiftin the understanding of the patho-physiology of ocularburns suggesting that limbal stem cell deficiency (LSCD)was the reason behind corneal epithelial problems in ocularburns. 7
The obvious implication of this new knowledge waswhether limbal stem cell deficiency could be treated byperforming limbal transplantation? 7 Following successfulpre-clinical animal trials, 8 Kenyon and Tseng in 1989provided the proof-of-principle by describing successfulcorneal regeneration in patients with unilateral acute andchronic chemical burns following limbal autografttransplantation. 9 This technique involved removing asmuch as six clock hours of donor limbal tissue from healthy
donor eyes and transplanting it on the recipient eyes afterclearing the pathological pannus covering the cornea. 9
Although this technique was extremely effective, othergroups who tried to replicate the results reported rareincidents of iatrogenic LSCD in the donor eyes.10-12 In 1997Pellegrini and associates proposed a way around thisproblem by developing a technique of culturing the limbalcells ex-vivo in a laboratory to form a transplantable sheetof epithelium from less than one clock hour of donor limbaltissue.13 Following this, several large clinical trials haveestablished the safety and efficacy of autologous ex-vivocultivated limbal epithelial transplantation for the treatmentof unilateral LSCD. 14-17
Advantages of Ex-vivo Cultivated LimbalEpithelial Transplantation:
Although improving the safety of limbal transplantation wasprobably the driving force behind its development, thistechnique offers several other advantages as comparedto conventional limbal transplantation.
1. Minimal Donor Tissue: Since first described in 1997,cultivated limbal transplantation has been performedin hundreds of patients with LSCD and till date thereare no reports of donor site complications.14,15 Theauthors specifically looked at the donor eyes in 200cases of unilateral LSCD which underwent autologouscultivated limbal epithelial transplantation and notedthat the donor-site epithelized within two weekswithout complications. 17
2. Repeatability: One or two repeat limbal biopsies canbe safely obtained from the same donor eye if theprimary procedure fails, because more than 90% ofthe limbus is left untouched by a single biopsy.16,18
This is not possible in conventional limbaltransplantation as the donor eye is not left with anylimbal reserve.
3. Early Corneal Epithelization: Since a ready-madeepithelial sheet is transplanted in cultivated limbalepithelial transplantation, corneal epithelization is
almost immediate or is completed by the first week.16-19 In conventional limbal transplantation, the entirecornea is epithelized only by six weeks.19
4. Less Surface Inflammation: Post-operative ocularsurface inflammation subsides faster after cultivatedlimbal epithelial transplantation as compared toconventional limbal transplantation. 19
5. Less Scarring: Cultivated limbal transplantation isassociated with less scarring on the recipient cornealsurface and probably better visual recovery ascompared to the conventional technique. 19
6. Amplification in number of transplanted stemcells: Ex-vivo cultivation results in increase in thenumber of limbal stem cells obtained by biopsy andthis in turn can lead to better long-term survival of thegraft.14,15
Indications for Autologous LimbalTransplantation:
Any traumatic or inflammatory damage to the limbus cancause permanent functional damage to the limbal stemcells.20,21 This leads to corneal epithelial instability, recurrentor persistent epithelial defects, invasion of the cornealsurface by the surrounding opaque conjunctival tissue(conjunctivalization) and consequently severe visual loss.21 The commonest indication of autologous limbaltransplantation the world over is unilateral ocular surfaceburns, due to chemical or thermal injury.14,15 Earlier thisprocedure was performed both during the acute andchronic stages,9 but it is presently indicated only in thechronic stage, after the ocular surface inflammation hassubsided. The other rare indication is iatrogenic LSCD aftermultiple or extensive ocular surface surgery like excisionof ocular surface squamous neoplasia (OSSN). LSCD dueto Stevens Johnson syndrome (SJS), ocular cicatricialpemphigoid (OCP), severe allergic eye disease aniridiaassociated keratopathy have bilateral affliction and needeither allogeneic limbal transplantation or keratoprosthesissurgery.14,15 However, ex-vivo cultivated autologous limbalepithelial transplantation can be performed in patients whohave bilateral LSCD but with asymmetrical involvementhaving at least one clock-hour of healthy limbus in eithereye .22
Pre-operative Clinical Assessment andCounseling:
Selecting the proper cases is probably the most importantdeterminant of the outcome of limbal transplantation. Thefirst step is clinically assessing whether the affected eyehas visual potential by performing simple macular functiontests or electrophysiological testing. Additionally, youngchildren developing unilateral blindness before the age of8 years, fixing light poorly, and with monocular deviation
are likely to have dense amblyopia with poor visualpotential. Limbal transplantation may still be performed inamblyopic eyes to provide cosmetic relief, but the poorvisual prognosis must be explained to the patient orparents, as appropriate. As there is no objective way ofaccurately assessing ocular surface inflammation andsince these eyes are heavily scarred and vascularized,some surgeons prefer to wait for 3 to 6 months after theacute event before performing limbal transplantation. Lidabnormalities like notches, improper closure, entropion andtrichiasis also need to looked for and addressed. Eyeswith severe dry eye disease, with a Schirmer’s test 1 scoreof less than 10mm at 5 minutes are unsuitable for thisprocedure and punctual occlusion may be needed prior tosurgery. In summary the ocular surface environment mustbe conducive for the limbal transplantation to succeed.Any cause which may inflict inflammatory damage on thegrafted cells post-operatively need to be taken care of priorto planning limbal transplantation. The extent of cornealstromal scarring is also difficult to assess pre-operativelyand patients must be counseled that they may needadditional surgery in the form of an anterior lamellar orpenetrating keratoplasty (PK) for visual improvementdespite a successful limbal transplantation. In the authors’experience it is prudent to perform limbal and cornealtransplantation as a two-stage rather than a single-stageprocedure.23
Technique of Limbal Biopsy: A biopsy is taken from ahealthy part of the limbus; a 2x2 mm piece of conjunctivalepithelium with 1 mm into clear corneal stromal tissue atthe limbus is dissected; conjunctiva is excised just behindthe pigmented line (palisades of Vogt), and the limbal tissuethat contained epithelial cells and a part of the cornealstroma is obtained.24
Technique of Limbal Culture: Broadly there are twotechniques of limbal cultivation, a) the suspension culturewhere the a cell suspension of the biopsied limbal tissueis prepared and spread over a suitable substrate; and b)explant culture where the limbal tissue is sectioned intosmaller pieces and directly placed on the substrate withoutseparating the epithelial cells from the stroma.14,15
Additionally the constituents of the culture medium may ormay not contain animal derived products or xenobioticmaterials.25 Xenogenic constituents of a limbal culturesystem can be in the form of murine feeder-cells, bovineserum, or animal derived growth factors.25 To avoid theuse of animal-derived products four groups,26-28 includingour own,24 have independently developed completely xeno-free laboratory protocols of limbal culture.
In our technique, 24 the tissue is transported to thelaboratory in human corneal epithelium (HCE) medium.HCE is composed of modified Eagle’s medium/F12 medium(1:1) solution containing 10% (vol/vol) autologous serum
(AS), 2mM l-glutamine, 100 U/ml penicillin, 100 µg/mlstreptomycin, 2.5 µg/ml amphotericin B, 10 ng/ml humanrecombinant epidermal growth factor, and 5 µg/ml humanrecombinant insulin. Under strict aseptic conditions, thedonor limbal tissue is shredded into small pieces. Humanamniotic membrane (hAM), prepared and preserved by oureye bank is used as a carrier. A 3x4cm hAM sheet is de-epithelized using 0.25% recombinant trypsin and EDTAsolution for 15 minutes. The shredded bits of limbal tissueare explanted over the center of de-epithelized hAM withthe basement membrane side-up. A similar parallel cultureis also prepared as a backup. A submerged explant culture
system without a feeder-cell layer is used. We used theHCE medium to nurture the culture. The culture isincubated at 370C with 5% CO2 and 95% air. The growth ismonitored daily under an inverted phase contrastmicroscope and the medium is changed every other day.The culture is completed when a monolayer of the cellsgrowing from the explants became confluent, typically in10 to 14 days.
Technique of Limbal Transplantation: Any symblepharonwhich prevented adequate separation of the lids is releasedto permit the insertion of a wire speculum (no additional
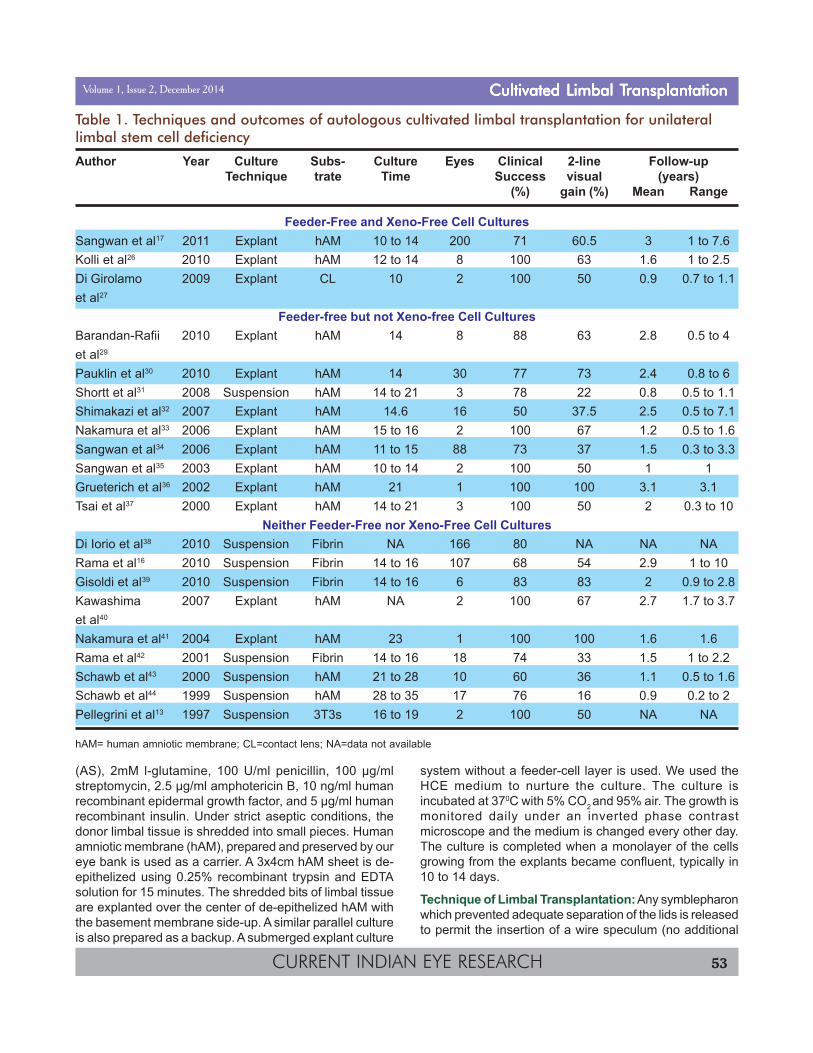
Table 1. Techniques and outcomes of autologous cultivated limbal transplantation for unilaterallimbal stem cell deficiency
Author Year Culture Subs- Culture Eyes Clinical 2-line Follow-upTechnique trate Time Success visual (years)
(%) gain (%) Mean Range
Feeder-Free and Xeno-Free Cell CulturesSangwan et al17 2011 Explant hAM 10 to 14 200 71 60.5 3 1 to 7.6Kolli et al26 2010 Explant hAM 12 to 14 8 100 63 1.6 1 to 2.5Di Girolamo 2009 Explant CL 10 2 100 50 0.9 0.7 to 1.1et al27
Feeder-free but not Xeno-free Cell CulturesBarandan-Rafii 2010 Explant hAM 14 8 88 63 2.8 0.5 to 4et al29
Pauklin et al30 2010 Explant hAM 14 30 77 73 2.4 0.8 to 6Shortt et al31 2008 Suspension hAM 14 to 21 3 78 22 0.8 0.5 to 1.1Shimakazi et al32 2007 Explant hAM 14.6 16 50 37.5 2.5 0.5 to 7.1Nakamura et al33 2006 Explant hAM 15 to 16 2 100 67 1.2 0.5 to 1.6Sangwan et al34 2006 Explant hAM 11 to 15 88 73 37 1.5 0.3 to 3.3Sangwan et al35 2003 Explant hAM 10 to 14 2 100 50 1 1Grueterich et al36 2002 Explant hAM 21 1 100 100 3.1 3.1Tsai et al37 2000 Explant hAM 14 to 21 3 100 50 2 0.3 to 10
Neither Feeder-Free nor Xeno-Free Cell CulturesDi Iorio et al38 2010 Suspension Fibrin NA 166 80 NA NA NARama et al16 2010 Suspension Fibrin 14 to 16 107 68 54 2.9 1 to 10Gisoldi et al39 2010 Suspension Fibrin 14 to 16 6 83 83 2 0.9 to 2.8Kawashima 2007 Explant hAM NA 2 100 67 2.7 1.7 to 3.7et al40
Nakamura et al41 2004 Explant hAM 23 1 100 100 1.6 1.6Rama et al42 2001 Suspension Fibrin 14 to 16 18 74 33 1.5 1 to 2.2Schawb et al43 2000 Suspension hAM 21 to 28 10 60 36 1.1 0.5 to 1.6Schawb et al44 1999 Suspension hAM 28 to 35 17 76 16 0.9 0.2 to 2Pellegrini et al13 1997 Suspension 3T3s 16 to 19 2 100 50 NA NA
hAM= human amniotic membrane; CL=contact lens; NA=data not available
surgery to treat the symblepharon is performed). A peritomyis performed and the corneal fibrovascular pannus isexcised. If an impending or frank corneal perforation isnoted at this stage a PK is performed prior to placing thelimbal graft.23 The hAM and monolayer of cultivated limbalepithelial cells is spread over the cornea, epithelial sideup.17,18 The graft is then secured to the peripheral corneaby interrupted, circumferential 10-0 nylon sutures and tothe surrounding conjunctival edge by interrupted 8-0polyglactin sutures. Alternately, using a suturelesstechnique, the graft is secured to underlying ocular surfacewith fibrin glue (TISSEEL™ Kit from Baxter AG, Austria)and the margins of the graft are tucked under thesurrounding conjunctival edge. Bandage contact lensesare not applied at the end of surgery.
Postoperative management: All patients receive 1%prednisolone acetate eye drops eight times a day taperedto once a day in 35-42 days and 0.3% ciprofloxacinhydrochloride eye drops four times a day for 1 week, inboth the biopsied and transplanted eye. The latter arecontinued till the epithelial defect completely resolves. Nosystemic antibiotics or steroids are needed. Patients areexamined on postoperative days 1, 7, 42 and at an intervalof 90-180 days thereafter, as customized by the clinicalappearance of the transplant. Each examination includesa complete history, visual acuity assessment with Snellen’scharts, intraocular pressure measurement and detailedocular examination with slit-lamp bio-microscopy.
Clinical Outcomes of Cultivated LimbalTransplantation: The techniques and outcomes of
autologous cultivated limbal transplantation described byvarious groups are summarized in Table 1.13,17,26-44 Successwas defined clinically in most studies; a few studiesadditionally used impression cytology or symptom scoring.With our technique the hAM usually disappeared (it eitherdisintegrates or is incorporated as a part of the cornealstroma) by 4 weeks and the recipient ocular surfacestabilized by 6 weeks. The donor site completely epithelizedwithout scarring within two weeks of limbal biopsy. Overall,the success rate of autologous cultivated limbaltransplantation varied from 50 to 100% and a two-lineimprovement in visual acuity after cultivated limbaltransplantation alone was seen in 22 to 100% cases(Table 1). More than 90% of failures occurred by the endof one year and more than half of these by six monthsafter transplantation.15,16
Although on cursory review it appears that there is noclinical advantage that one culture technique holds overthe other, comparing success rates among different culturetechniques may be misleading as the indications forsurgery, sample size, and follow-up duration are variableamong different studies. Shimakazi et al32 and Nakamuraet al33 compared the explant and suspension culturetechniques, finding no significant difference in theoutcomes. It is noteworthy in this context that with similarindications for surgery, clinical criteria for success, andfollow-up Sangwan et al (explant culture, 71%, 200 eyes),17
Rama et al (suspension culture, 68%, 107 eyes)16 and DiIorio et al (suspension culture, 80%, 166 eyes)38 reportedsimilar and impressive success rates of cultivated limbal
Table 2. Clinical Outcomes of Conjunctival Limbal Autografting or Conventional LimbalTransplantation for eyes with Unilateral Limbal Stem Cell Deficiency.
Author Year Eyes Clinical 2-line Complications Follow-upSuccess vision (Months)
(%) gain (%) Mean Range
Miri et al45 2011 25 NA NA Filamentary keratitis (4) 41 3 to 127Miri et al46 2010 12 100 81.3 None 46 12 to 120Santos et al47 2005 10 80 61 None 33Ozdemir et al48 2004 15 87 80 None 13.9 3 to 24Dua et al49 2000 6 100 83 Filmentary keratitis (1) 18.8 14 to 31Rao et al50 1999 16 94 82 None 19.3 3 to 45Basti et al10 1999 3 100 100 LSCD in donor eye (1) NA 9 to 15Frucht-Pery et al51 1998 9 100 100 None NA 15 to 60Tan et al11 1996 9 77 77 LSCD in donor eye (1) 27.1 2.5 to 46Morgan et al52 1996 6 83 83 Donor site micro-perforation (1) 3 to 24Kenyon et al9 1989 26 77 65 None 18 2 to 45
NA= data not available; LSCD: Limbal Stem Cell Deficiency
epithelial transplantation with mean follow-up ranging from1.5 to almost 3 years and maximum follow-up of up to 8years. It is noteworthy that of the various groups onlySangwan et al,17 Kolli et al, 26 Di Girolamo et al,27 andZakaria et al28 described completely xeno-free techniquesof culturing limbal epithelium while others used at leastone or more animal derived products for culture. None ofthe studies reported any donor-site complications.
Around 18 to 38% of all eyes treated with autologouscultivated limbal epithelial transplantation also needed aPK for visual improvement.14,15 The authors have foundthat adopting a staged approach of performing limbaltransplantation first, followed at least six weeks later byPK resulted in better clinical outcomes as compared to asingle-staged approach of combined limbal transplantationand PK. 23 Therefore PK and limbal transplantation shouldnot be combined unless PK is absolutely unavoidable asin the case of an impending or frank corneal perforationdiscovered after removal of the vascular pannus. Theauthors also found that a repeat limbal biopsy from thehealthy eye followed by ex-vivo cultivation andtransplantation of the cultured cells on the affected eyecan successfully restore the ocular surface and improvevision in at least two thirds of cases with failure of therapywith primary autologous cultivated limbal epithelialtransplantation.18 Therefore combining the efficacy ofprimary (71%) and repeat autologous cultivated limbalepithelial transplantation (67%) almost 90% of cases ofunilateral LSCD can be treated successfully without anyadverse impact on the healthy donor eye. 17,18
Conclusions:
In terms of clinical efficacy there is hardly any differencebetween conventional and cultivated autologous limbaltransplantation as treatment options for unilateral LSCD(Table 2).9-11,45-52 Proponents of ex-vivo cultivation cite thesafety of the donor eye as the main advantage of theirtechnique. However, ex-vivo cultivation requiresspecialized expertise and a licensed (by the Human TissueAuthority in the United Kingdom) laboratory. It can take upto 2 weeks to generate a sheet of desired dimensions,and it is expensive, costing approximately 10 300 PoundsSterling or 12 000 Euros at current exchange rates forcultivation alone.46 Furthermore, many groups practicingthis technique continue to use xeno-biotic materials forcell culture (Table 1). Not surprisingly, conventional limbaltransplantations are still widely performed worldwide andcultivated limbal transplantation is restricted to few selectcenters around the globe.14,15 There are however certainclinical scenarios where cultivated limbal epithelialtransplantation can be a superior alternative toconventional limbal transplantation. For example, inpatients with bilateral but asymmetrical LSCD, even oneclock hour of healthy limbal area in either eye can be
utilized to restore the ocular surface and improve vision inboth eyes.22
The only study that compared conventional andcultivated limbal transplantation reported slowerepithelization rate, prolonged ocular surface inflammationand significantly more scarring with the conventionaltechnique.53 However, for cultivated limbal epithelialtransplantation to emerge as the more popular techniqueof treating unilateral LSCD the economic and logisticbarriers of cell culture have to be overcome first. Moreoverthe actual mechanism by which limbal transplantationworks is still debated. It is unclear whether this therapyreplenishes the stem cell reserve16 or revives the survivingstem cells by improving the micro-environment.14 It is alsowidely accepted that the cause of failure of limbaltransplantation is multi-factorial and poorly understood.16,17
In the large clinical trials Rama et al and Sangwan et alinvestigated the cause for failure and found that eyes withmore severe injuries and post-operative complications weremore likely to fail.16,17 Rama et al also found that theproportion of holoclone forming cells (actual stem cells) inculture needed to be more than 3% of the total cellpopulation for the transplant to have higher chances ofsuccess.16
In summary, the last two decades have witnessedtremendous progress in the understanding of ocularsurface disease due to corneal burns and this has in turnled to therapeutic innovations, at the cutting edge of whichstands ex-vivo cultivated limbal epithelial transplantation.Stem-cell based therapy for LSCD has already benefittedhundreds of patients worldwide and continuous researchand medical development in this field holds promise foran even more exciting future.
References:
1. Zirm E. Eine erfolgreiche totale Keratoplastik. Alberchtvon Graefes. Acrh Ophthalmol 1906;64: 580-93.
2. Armitage WJ, Tullo AB, Larkin DFP. The firstsuccessful full-thickness corneal transplant: acommentary on Eduard Zirm’s landmark paper of1906. Br J Ophthalmol 2006;90:1222-23.
3. Brown SI, Bloomfield SE, Pearce DB. Follow-up reporton transplantation of the alkali burned cornea. Am JOphthalmol 1974;77:538-42.
4. Thoft RA. Conjunctival transplantation as analternative to keratoplasty. Ophthalmology1979;86:1084-92.
5. Thoft RA, Friend J. The X, Y, Z hypothesis of cornealepithelial maintenance. Invest Ophthalmol Vis Sci1983 ;24:1442-3.
6. Schermer A, Galvin S, Sun TT. Differentiation-relatedexpression of a major 64K corneal keratin in vivo and
in culture suggests limbal location of corneal epithelialstem cells. J Cell Biol 1986l;103:49-62.
7. Cotsarelis G, Cheng SZ, Dong G, Sun TT, Lavker RM.Existence of slow-cycling limbal epithelial basal cells thatcan be preferentially stimulated to proliferate: implicationson epithelial stem cells. Cell 1989;57:201-9.
8. Tsai RJ, Sun TT, Tseng SC. Comparison of limbal andconjunctival autograft transplantation in cornealsurface reconstruction in rabbits. Ophthalmology1990;97:446-55.
10. Basti S, Mathur U. Unusual intermediate-termoutcome in three cases of limbal autografttransplantation. Ophthalmology 1999;106:958–63.
11. Tan DT, Ficker LA, Buckley RJ. Limbal transplantation.Ophthalmology 1996;103:29–36.
12. Jenkins C, Tuft S, Liu C, Buckley R. Limbaltransplantation in the management of chronic contact-lens-associated epitheliopathy. Eye 1993;7:629–33.
13. Pellegrini G, Traverso CE, Franzi AT, Zingirian M,Cancedda R, De Luca M. Long-term restoration ofdamaged corneal surfaces with autologous cultivatedcorneal epithelium. Lancet 1997;349:990-3.
14. Shortt AJ, Secker GA, Notara MD, Limb GA, KhawPT, Tuft SJ, Daniels JT. Transplantation of ex vivocultured limbal epithelial stem cells: a review oftechniques and clinical results. Surv Ophthalmol2007;52:483-502.
15. Baylis O, Figueiredo F, Henein C, Lako M, AhmadS.13 years of cultured limbal epithelial cell therapy: Areview of the outcomes. J Cell Biochem 2011;112:993-1002.
16. Rama P, Matuska S, Paganoni G, Spinelli A, De LucaM, Pellegrini G. Limbal stem-cell therapy and long-term corneal regeneration. N Engl J Med2010;363:147-155.
17. Sangwan VS, Basu S, Vemuganti GK, Sejpal K,Subramaniam SB, Bandyopadhyay S et al. Clinicaloutcomes of xeno-free autologous cultivated limbalepithelial transplantation: a 10-year study. Br JOphthalmol 2011;95:1525-29.
18. Basu S, Ali MH, Sangwan VS. Clinical Outcomes ofRepeat Autologous Cultivated Limbal EpithelialTransplantation for Ocular Surface Burns. Am JOphthalmol 2012;153:643-50
19. Ang LP, Sotozono C, Koizumi N, Suzuki T, Inatomi T,Kinoshita S. A comparison between cultivated andconventional limbal stem cell transplantation forStevens-Johnson syndrome. Am J Ophthalmol2007;143:178-80.
20. Tseng SC. Concept and application of limbal stemcells. Eye 1989;3:141–57.
21. Dua HS, Saini JS, Azuara-Blanco A, Gupta P. Limbalstem cell deficiency: concept, aetiology, clinicalpresentation, diagnosis and management. Indian JOphthalmol 2000;48:83–92.
22. Sangwan VS, Vemuganti GK, Iftekhar G, Bansal AK,Rao GN. Use of autologous cultured limbal andconjunctival epithelium in a patient with severebilateral ocular surface disease induced by acid injury:a case report of unique application. Cornea 2003;22:478-81.
23. Basu S, Mohamed A, Chaurasia S, Sejpal K,Vemuganti GK, Sangwan VS. Clinical outcomes ofpenetrating keratoplasty after autologous cultivatedlimbal epithelial transplantation for ocular surfaceburns. Am J Ophthalmol 2011;152:917-924.e1.
24. Mariappan I, Maddileti S, Savy S, Tiwari S, Gaddipati S,Fatima A et al. In vitro culture and expansion of humanlimbal epithelial cells. Nat Protoc 2010;5:1470-79.
25. Schwab IR, Johnson NT, Harkin DG. Inherent risksassociated with manufacture of bioengineered ocularsurface tissue. Arch Ophthalmol 2006;124:1734–40.
26. Kolli S, Ahmad S, Lako M, Figueiredo F. Successfulclinical implementation of corneal epithelial stem celltherapy for treatment of unilateral limbal stem celldeficiency. Stem Cells 2010; 28:597–610.
27. Di Girolamo N, Bosch M, Zamora K, Coroneo MT,Wakefield D, Watson SL. A contact lens-basedtechnique for expansion and transplantation ofautologous epithelial progenitors for ocular surfacereconstruction. Transplantation 2009;87:1571–78.
28. Zakaria N, Koppen C, Van Tendeloo V, Berneman Z,Hopkinson A, Tassignon MJ. Standardized limbalepithelial stem cell graft generation andtransplantation. Tissue Eng Part C Methods2010;16:921-27.
29. Baradaran-Rafii A, Ebrahimi M, Kanavi MR, Taghi-Abadi E, Aghdami N, Eslani M et al. Midtermoutcomes of autologous cultivated limbal stem celltransplantation with or without penetratingkeratoplasty. Cornea 2010;29:502–9.
30. Pauklin M, Fuchsluger TA, Westekemper H, SteuhlKP, Meller D. Midterm results of cultivated autologousand allogeneic limbal epithelial transplantation inlimbal stem cell deficiency. Dev Ophthalmol2010.45:57–70.
31. Shortt AJ, Secker GA, Rajan MS, Meligonis G, DartJK, Tuft SJ et al. Ex vivo expansion and transplantationof limbal epithelial stem cells. Ophthalmology2008;115:1989–97.
32. Shimazaki J, Higa K, Morito F, Dogru M, Kawakita T,Satake Y et al. Factors influencing outcomes incultivated limbal epithelial transplantation for chroniccicatricial ocular surface disorders. Am J Ophthalmol2007;143:945–53.
33. Nakamura T, Inatomi T, Sotozono C, Ang LPK, KoizumiN, Yokoi N et al. Transplantation of autologous serum-derived cultivated corneal epithelial equivalents forthe treatment of severe ocular surface disease.Ophthalmology 2006; 113:1765–72.
34. Sangwan VS, Matalia HP, Vemuganti GK, Fatima A,Ifthekar G, Singh S et al. Clinical outcome ofautologous cultivated limbal epitheliumtransplantation. Indian J Ophthalmol 2006;54:29-34.
35. Sangwan VS, Vemuganti GK, Singh S,Balasubramanian D. Successful reconstruction ofdamaged ocular outer surface in humans usinglimbal and conjunctival stem cell culture methods.Biosci Rep 2003;23:169-74.
36. Grueterich M, Espana EM, Touhami A, Ti S-E, TsengSCG. Phenotypic study of a case with successfultransplantation of ex vivo expanded human limbalepithelium for unilateral total limbal stem celldeficiency. Ophthalmology 2002;109:1547–52.
37. Tsai RJ, Li LM, Chen JK. Reconstruction of damagedcorneas by transplantation of autologous limbalepithelial cells. N Engl J Med 2000;343:86-93.
38. Di Iorio E, Ferrari S, Fasolo A, Böhm E, Ponzin D,Barbaro V. Techniques for culture and assessment oflimbal stem cell grafts. Ocul Surf 2010;8:146-53.
39. Colabelli Gisoldi RAM, Pocobelli A, Villani CM, Amato D,Pellegrini G. Evaluation of molecular markers in cornealregeneration by means of autologous cultures of limbal cellsand keratoplasty. Cornea 2010; 29:715–22.
40. Kawashima M, Kawakita T, Satake Y, Higa K,Shimazaki J. Phenotypic study after cultivated limbalepithelial transplantation for limbal stem celldeficiency. Arch Ophthalmol 2007;125:1337–44.
41. Nakamura T, Inatomi T, Sotozono C, Koizumi N,Kinoshita S. Successful primary culture andautologous transplantation of corneal limbal epithelialcells from minimal biopsy for unilateral severe ocularsurface disease. Acta Ophthalmol Scand 2004;82:468–71.
42. Rama P, Bonini S, Lambiase A, Golisano O, PaternaP, De Luca M et al. Autologous fibrin-cultured limbalstem cells permanently restore the corneal surface ofpatients with total limbal stem cell deficiency.Transplantation 2001;72:1478–85.
43. Schwab IR. Cultured corneal epithelia for ocularsurface disease. Trans Am Ophthalmol Soc1999;97:891–986.
44. Schwab IR, Reyes M, Isseroff RR. Successfultransplantation of bioengineered tissue replacementsin patients with ocular surface disease. Cornea2000;19:421–26.
45. Miri A, Said DG, Dua HS. Donor Site Complications inAutolimbal and Living-Related AllolimbalTransplantation. Ophthalmology 2011;118:1265-71.
46. Miri A, Al-Deiri B, Dua HS. Long-term outcomes ofautolimbal and allolimbal transplants. Ophthalmology2010;117:1207-13.
47. Santos MS, Gomes JA, Hofling-Lima AL, Rizzo LV,Romano AC, Belfort R Jr. Survival analysis ofconjunctival limbal grafts and amniotic membranetransplantation in eyes with total limbal stem celldeficiency. Am J Ophthalmol 2005 ;140:223-30.
48. Ozdemir O, Tekeli O, Ornek K, Arslanpençe A,Yalçindað NF. Limbal autograft and allografttransplantations in patients with corneal burns. Eye2004 ;18:241-8.
49. Dua HS, Azuara-Blanco A. Autologous limbaltransplantation in patients with unilateral corneal stemcell deficiency. Br J Ophthalmol 2000;84:273– 8.
50. Rao SK, Rajagopal R, Sitalakshmi G, PadmanabhanP. Limbal allografting from related live donors forcorneal surface reconstruction. Ophthalmology1999;106:822– 8.
51. Frucht-Pery J, Siganos CS, Solomon A, Scheman L,Brautbar C, Zauberman H. Limbal cell autografttransplantation for severe ocular surface disorders.Graefes Arch Clin Exp Ophthalmol 1998 ;236:582-7.
52. Morgan S, Murray A. Limbal autotransplantation in theacute and chronic phases of severe chemical injuries.Eye 1996;10:349-54.
Osteo-Odonto Keratoprosthesis (OOKP): A Review of SurgicalTechniques and Clinical OutcomesSayan Basu1
Abstract
Osteo-odonto keratoprosthesis (OOKP) is a multi-staged procedure for the treatment of blindness due to bilateral severe end-stage corneal disease. Developed by Strampelli over fifty years ago and modified thereafter by Falcinelli, the OOKP is by far theonly keratoprosthesis that has been retained in eyes for over twenty to thirty years. This procedure can be performed in eyes withbone dry and keratinized ocular surfaces and basically consists of a optical cylinder help in place by a skirt of dento-alvelolar bone.This review describes the surgical technique of OOKP and the clinical outcomes reported by various series including the author’spersonal experience with this keratoprosthesis.
1Cornea and Anterior Segment Services, L V Prasad Eye Institute, Hyderabad, IndiaCorresponding Author : Sayan Basu, E-mail: [email protected] on : 25/01/2015, Accepted on : 03/02/2015Conflict of Interest : None, Financial Disclosure : None
Osteo-odonto-keratoprosthesis (OOKP) surgery is atechnique developed half a century ago by the Italian
ophthalmologist Strampelli and usesthe patient’s own toothroot and alveolar bone to support an optical cylinder.1 Thismulti-staged procedure is indicated in cases of severebilateral corneal blindness, when conventional cornealtransplantation or even the Boston type1 keratoprosthesisis doomed to failure. Although initially conceptualized byPellier de Quengsy, a French ophthalmologist, the firstkeratoprosthesis implantation in a human was performedbyNussbaum in 1855. This was a quartz crystal implantthat remained in the eye forsix months. Subsequently owingto the inevitable extrusion of the early implants and alsodue to the increasing popularity of penetrating keratoplasty,the initial enthusiasm surrounding keratoprosthesis dieddown. However, as experience with penetratingkeratoplasty grew, surgeons the world over realized thatthere were still some forms of corneal blindness that werenot amenable to treatment by replacing the diseasedcornea with a healthy donor cornea. Thus interest inkeratoprosthesis was renewed and numerous designs andtechniques were subsequently described.2
An ideal keratoprosthesis should be a suitable replacementof the cornea being optically clear, bio-integrable, resistantto infection and most importantly it should be long-lasting.3,4Keratoprosthesis can be classified based on thematerial of the optical cylinder (optic) and the support forthe optical cylinder (haptic).Most modelshave a non-biological haptic(Boston KPro, Pintucci, Leon-Barraquer,
Legeais and AlphaCor), while few use biologicalhaptics(Strampelli OOKP, Casey and Temprano).Among these theBoston type 1 keratoprosthesis is currently the mostpopular while the OOKP has the longest follow-up andbest retention rate.The OOKP can also be used in bonedry eyes with keratinized ocular surface and it is the onlypotentially vision restoring surgery that is possible in sucheyes. The original technique of OOKP described byStrampelli has been modified by Falcinelli to improve visualresults and retention of thedevice.5,6 Therefore thistechnique is now also referred to as the modified OOKPor MOOKP.
Indications:
Patients with bilateral corneal blindness resultingfromsevere end-stage Stevens-Johnson syndrome (SJS),ocularcicatricial pemphigoid (OCP), chemical burns,trachoma,dry eyes or multiple corneal graft failure may beconsideredfor OOKP surgery. However, this technique isbest reserved for bilateral corneal blindness with dry andkeratinized ocular surfaces. In wet eyes the Boston type 1keratoprosthesis is preferred over the OOKP.
Contraindications:
This procedure should not be recommended for patientswho are otherwise well adjusted to their visual handicap,children under the age of 17, or in cases of doubtful or novisual potential. Another important consideration is thepatient’s expectations from surgery. Since the final look of
the eye after all stages of OOKP is unnatural, the procedureshould not be considered in patients who aspire to haveboth vision and cosmesis (Figure 1). There have beenanectodal reports of patients who after regaining visionand looking at themselves in the mirror have asked for theOOKP to be removed or even committed suicide.
Pre operative assessment:
The most important preoperative examination involvesdetermining the visual potential. This can be done bychecking accurate light projection in all quadrants, B-scanultrasonography, and electrophysiological tests like flashERG and VEP. However certain macular pathologies likea macular hole or scar can still be missed. The intra-ocularpressure is determined digitally and past records arechecked to find out if the patient has been treated forglaucoma. A-scan is performed to measure the axial lengthwhich is used to calculate the power of the optical cylinder.After ruling out any contraindications to the procedure asdescribed above, the patient is explained about the risksand complications, the need for frequent and lengthy follow-up. The patient must be encouraged to take an informeddecision after consultation with family and friends.
Pre-operative oral assessment:The buccal mucosa is inspected to look for areas of
keratinisation or scarring. Patients who smoke or chewbeetel nut should be advised to discontinue such habitsbefore surgery. For patients with poor oral hygiene, aprophylactic antiseptic mouthwash may be advised priorto surgery. Similary the condition and health of the teethare also inspected. The ideal donor tooth is the caninebecause it is mono-radicular. It is not mandatory to performradiographs, but they can help in identifying the proximityof the floor of the maxillary antrum to the root of the toothwhich can help avoid inadvertent oro-antral fistula creationduring surgery.
Surgical technique:
Stage 1A: Before the implantation of the keratoprosthesisa complete iridectomy, lens extraction and anteriorvitrectomy is performed. During this procedure the surgeongets an opportunity to examine the posterior segment byperforming intra-operative indirect ophthalmoscopy. Aftersuturing the limbal wound, the cornea is covered byadvancing the Tenon’s capsule and residual conjunctiva(Figure 2, A to D).
Stage 1B: The ocular surface is de-epithelized and abuccal mucous membrane graft is placed on it. The graftis sutured to the four recti and underlying epiclera as wellas the surrounding Tenon’s capsule and conjunctiva (Figure2 E and F).
Figure 1: Slit-lamp biomicroscopy photograph of the left eye of a 44 year old woman before and after osteo-odonto keratoprosthesis (OOKP)surgery. (A) Pre-operative photograph shows a dry and keratinized ocular surface with loss of corneal transparency. This patient developedblindness after an episode of Stevens Johnson Syndrome when she was 17 years of age. (B) Two years after OOKP all stages of OOKPsurgery were completed, her vision in this eye is 20/20 unaided for distance and N6 for near with +3.0D Sphere. The photograph shows theanterior part of the PMMA optical cylinder protruding through the mucous membrane covered bony lamina. Note that the cosmetic appearanceis unnatural and there is significant pseduoproptosis induced by the OOKP.
OOKPOOKPOOKPOOKPOOKPVolume 1, Issue 2, December 2014
CURRENT INDIAN EYE RESEARCH60
Stage 1C: A monoradicular tooth (preferably canine) isharvestedto prepare an osteo-odonto-lamina. The root andsurroundingjaw bone is removed using a cuttingmechanised saw.The bone is thinned on one side toexpose the dentine and a hole is drilled through dentinethroughwhich the anterior part of a PMMA optical cylinderiscemented in place (Figure 2, G to L). The crown isremoved and the osteo-odonto-lamina is implantedinto asubmuscular pouch just below the lower eye lid of thefelloweye for a period of 8 to 10 weeks.
Stage 2: The osteo-odonto-lamina along with itsfibrovascular capsule is removed from the submuscular
pocket and cleaned, the soft tissue isexcised from theposterior surface and trimmed fromthe anterior. The buccalmucosa is incised and a flap hinged inferiorly is raised toexpose the cornea. A Flieringa ring large enough toaccommodate the lamina is secured to the episclera. Thecenter ofthe cornea is marked and a central opening justlarge enough to fit the posterior part of the optical cylinderis made with a trephine and scissors. After adequateanterior vitrectomy the lamina is fitted into place andsutured to the episclera. The buccal mucosal flap isrepositioned and an opening is made in the flap to exposethe anterior part of the optical cylinder (Figure 2, M to P).
Figure 2: This composite photograph shows the various stages of the osteo-odonto keratoprosthesis from the surgeons view. (A to D) InStage 1A, the limbus is exposed and a 180o full thickness incision is made. The iris is removed from its root and the lens is removed by cryo-extraction. Anterior vitrectomy is performed and the limbal wound is closed with 10-0 nylon interrupted sutures. (E and F) In Stage 1B, theepithelium covering the ocular surface is removed and a buccal mucosal graft in sutured on to the surface to cover the cornea. (G to L) InStage 1C, the canine tooth with the adjoining bone is removed with a saw. The bone is thinned to expose the dentine and a small hole is drilledthrough it. The PMMA optical cylinder in cemented in place and the assembled osteo-dental lamina is placed in a sub-muscular pocket in theopposite cheek. (M to P) In Stage 2, the lamina is retrieved after 2 months and cleaned. The buccal mucosa is incised and an inferior hingedflap is raised to expose the ocular surface. The cornea is trephined in the centre and the osteo-dental lamina is fixed in place by suturing it tothe epislera. The mucosal flap is replaced and an opening is made in it to expose the optical cylinder.
OOKPOOKPOOKPOOKPOOKPVolume 1, Issue 2, December 2014
CURRENT INDIAN EYE RESEARCH 61
Stage 1B and 1C are frequently combined together as thefirst step and Stage 1A and Stage 2 as the second step.This separates the extra-ocular and intra-ocular parts ofthe procedure and makes the procedure a two-stage affair.Others combine stage 1B and 1C as a single procedurereducing the number of procedures to three. We prefer afour- staged procedure as it gives time for the patient torecover from each operative insult and reduces thechances of inflammatory complications which can be quiteunpredictable in patients with SJS or OCP.
Post operative care and follow up:
Systemic antibiotics, corticosteroids and ocularhypotensive agents are administered till the patient canbe discharged. Topical antibiotic ointments are prescribedfor the operated eye. Patients are usually seen after oneweek of discharge from the hospital and again at onemonth, three months and six monthly thereafter. At thefollow-up visits the best spectacle corrected vision isassessed. Additionally, the digital assessment of the intra-ocular pressure, health of the buccal mucous membraneand stability of the optical cylinder is also assessed.Fundoscopy is carried out to check the opticdisc andmacula, B-scan to detect early peripheraldetachments andvisual field assessments are made6 monthly for diagnosisand monitoring glaucoma.
Clinical outcomes
Anatomical retention rates and visual outcomes in eyeswith blindness due to sequelae of inflammatory diseasehave been better with the OOKP7-18as compared to purelysyntheticprostheses.19"30The overall results with OOKP aregood comparedwith those reported in literature for otheravailablemethods in patients with end stage ocular surfacediseasedue to severe inflammatory syndromes like SJSand OCP. 17Tan et al reviewed the largest eight case seriesof OOKP published in the scientific literature with samplesizes ranging from 4-181 eyes.17 The most commonindications for surgery were severe cases of SJS andocular burns. Anatomical survival rate in all the studieswas 87.8% (range 67-100%) at 5 years, and three studiesshowed survival rates of 81% (range 65-98%) at 20 years.Visual acuity was more than 6/18 in 52% (range 46-72%)of the eyes with OOKP surgery. The most commonintraoperative complication was vitreous hemorrhage (0-52%) and the most common long-term blindingcomplication was glaucoma (7-47%). Endophthalmitisranged from 2-8%. The most common repeat surgicalprocedure was mucosal trimming due to mucosal
overgrowth at the optical cylinder and mucosal grafting forextrusion of the OOKP or mucosal ulceration.
In our series we performed OOKP in 31 eyes of 30 patientsblinded by SJS and one patient blinded by severe ocularburns. The anatomical success rate was 100% at a meanfollow-up of 14.2±7.2 months. The visual acuity improvedfrom hand motions or light perception to 20/40 or better in18 eyes, 20/50 to 20/200 in 9 eyes, 20/400 in two eyesand remained hand motions or light perception in 2 eyes.Retinal detachment occurred in 2 eyes, mucosal ulcerationin 9 eyes and mucosal overgrowth in one eye.
Conclusion:
Although the surgical procedure of OOKP is very tedious,the overall results are very satisfying. Most patients regaingood vision and maintain this for long periods of time. Thereis no doubt that the retention rate of the OOKP is stillunparalleled among all keratoprosthesis designs. However,setting up of an OOKP practice requires a dedicated teamof surgeons and a multi-disciplinary approach.Complications are common but mostly manageable,provided they are addressed early and appropriately. Themost important caveat in OOKP surgery is choosing theright patients, who do not have unrealistic expectations,are committed to come for long follow-ups and are readyto face the prospect of additional surgery for managementof complications. It is entirely heartening for an OOKPsurgeon to see patients completely blinded for decades toresume the near normal life of a sighted individual free ofdependence after OOKP.
References
1. Strampelli B. Keratoprosthesis with osteodontal tissue.Am J Ophthalmol 1963; 89:1029–39.
3. Liu C, Tighe B. The properties of the idealkeratoprosthesis. Anales Del Instituto Barraquer(Barc.) 1999; 28(S):155–6.
4. Liu C, Tighe B. Striving for the perfect kerato-prosthesis. Br J Ophthalmol 1998; 82:3–4.
5. Falcinelli GC, Barogi G, Caselli M, Colliardo P, TaloniM. Personalchanges and innovations in Strampelli’sosteo-odontokeratoprosthesis. Anales Del InstitutoBarraquer (Barc.) 1999;28(S):47–8.
6. Liu C, Pagliarini S. Independent survey of long termresults of theFalcinelli osteo-odonto-keratoprosthesis(OOKP). Anales Del Instituto Barraquer (Barc.)1999;28(S):91–3.
OOKPOOKPOOKPOOKPOOKPVolume 1, Issue 2, December 2014
CURRENT INDIAN EYE RESEARCH62
7. Falcinelli G, Barogi G, Taloni M. Osteo-odonto-keratoprosthesis:Present experience and futureprospects. Refract Corneal Surg 1993;9:193–4.
8. Caselli M, Colliardo P, Falcinelli G, Nebbioso M.Falcinelli’s osteoodonto-keratoprosthesis: Long termresults. An Inst Barraquer (Barc.) 1999; 28(S):113–4.
9. Colliardo P, Caselli M, Falcinelli GC, Grabner G,Micozzi I. Osteoodonto-keratoprosthesis in thetreatment of corneal blindness dueto “dry eye”. AnInst Barraquer (Barc.) 2001; 30:189–90.
10. Falcinelli G, Colliardo P, Corazza E, Taloni M.Falcinelli’s osteoodonto-keratoprosthesis: 25 years ofsurgical experience. An Inst Barraquer (Barc.) 2001;30:53–4.
11. Hille K, Landau H, Ruprecht KW. Osteo-odonto-keratoprosthesis.A summary of 6 years surgicalexperience. Ophthalmologe 2002;99:90–5.
12. Liu C, Sciscio A, Smith G, Pagliarini S, Herold J.Indications and technique of modern Osteo-odonto-keratoprosthesis (OOKP) surgery. Eye News 1998;5:17–22.
13. Liu C, Herold J, Sciscio A, Smith G, Hull C. Osteo-odontokeratoprosthesissurgery. Br J Ophthalmol1999; 83:127.
14. Falcinelli GC, Taloni M, Corazza E, Buratto E, FalcinelliG. Extensionof indications for osteo-odonto-keratoprosthesis. An Inst. Barraquer(Barc.) 1999;28(Suppl.):151–2.
15. Tandon R, Herold J, Thorp S, Hull C, Britain P,Goldberg L, Liu C. Results of the osteo-odonto-keratoprosthesis (OOKP) in severe inflammatory eyediseases. Experience from the United Kingdom.Proceedings of the 5th KPro-8th IOSS Joint Meeting,Miami, Florida,9–10 May 2003.
16. Marchi V, Ricci R, Pecorella I, Ciardi A, Di Tondo U.Osteo-Odonto-Keratoprosthesis. Description ofsurgical technique with results in 85 patients. Cornea1994; 3:125–30.
17. Iyer G, Pillai VS, Srinivasan B, Falcinelli G,Padmanabhan P, Guruswami S, Falcinelli G. Modifiedosteo-odonto keratoprosthesis—the Indianexperience—results of the first 50 cases. Cornea2010;29:771-6.
18. Tan A, Tan DT, Tan XW, Mehta JS. Osteo-odontoKeratoprosthesis: Systematic Review of SurgicalOutcomes and Complication Rates. Ocul Surf2012;10:15-25.
19. Dohlman CH, Doane MG. Keratoprosthesis in end-stage dry eye. Adv Exp Med Biol 1994; 350:561–4.
20. Dohlman CH, Terada H. Keratoprosthesis inpemphigoid and Stevens-Johnson syndrome. Adv ExpMed Biol 1998; 438:1021–5.
21. Legeais JM, Renard G, Pouliquen Y. A secondgeneration of biointegrable keratoprostheses. An InstBarraquer (Barc.) 1999; 28(S):57–8.
22. Legeais JM, Renard G. A second generation of artificialcornea withsoft optical system: first human investigation.An Inst Barraquer (Barc.) 2001; 30:101–2.
23. Lund OE. Grenzen und Moglichkeiten der optischenKeratoprothese.Ein klinischer und histopathologischerBericht. Klin Monatsbl Augenheilkd 1982; 180:3–12.
24. Pintucci S, Pintucci F, Cecconi M, Caiazza S. NewDacron tissue colonisable keratoprostheis: clinicalexperience. Br J Ophthalmol 1995;79:825–9.
25. Pintucci S, Pintucci F, Caiazza S, Cecconi M. TheDacron felt colonisable keratoprosthesis: after 15years. Eur J Ophthalmol 1996; 6:125–30.
26. Pintucci S, Pintucci F, Caiazza S, Karcioglu ZA. Shortand long term complications of the PMMA/Dacronbiointegrated keratoprosthesis:18 years ofexperience. Invest Ophthalmol Vis Sci 1998; 39:S77
27. Pintucci S, Pintucci F, Cecconi M, Caiazza S. ThePintucci Dacrontissue KP: long-term results,postoperative care and revisions in dryeyes and ineyes with tear secretion. An Inst Barraquer (Barc.)1999;28(S):109–12.
28. Crawford GJ, Hicks CR, Lou X, Vijayasekaran S, TanD, Mulholland B,Chirila TV, Constable IJ. The ChirilaKeratoprosthesis: phase I human clinical trial.Ophthalmology 2002; 109:883–9.
29. Nouri M, Terada H, Alfonso EC, et al. Endophthalmitisafter keratoprosthesis; incidence, bacterial causes,and risk factors. Arch Ophthalmol 2001; 19:484–9.
30. Nouri M, Terada H, Durand ML, Alfonso E, DohlmanCH. Risk factorsfor endophthalmitis in kerato-prosthesis patients. An Inst Barraquer (Barc.) 2001;30:123–4.
OOKPOOKPOOKPOOKPOOKPVolume 1, Issue 2, December 2014
CURRENT INDIAN EYE RESEARCH 63
Synthesis Of Nanoparticles As A Probe For Diagnosis Of Dry Eye DiseaseMohammad Azharuddin1, Anjan Kr Dasgupta1, Himadri Datta2
Abstract
Purpose: To study whether dry eye is protein conformational disease by synthesis of metallic nanoparticles as a probe. Methods:20 dry eye patients and 18 control individuals were recruited for this study. Schirmer’s test was performed for diagnosis of dry eyepatients. Collection and extraction of tear proteins was done with the help of Schirmer’s strip. Synthesis of nanoparticles was doneusing tear proteins as template. Results: Nanoparticles synthesized from dry eye tear proteins have been compared with thosefrom control subjects and are seen to have a significantly higher degree of clustering. The observation supports our recent observationthat the dry eye tear proteins are more prone to aggregation, and the nanoparticle clustering can be explained by the report thatunfolded proteins facilitate formation of clustered nanoparticles. Conclusion: The reducing property of tear proteins is exploitedfor synthesis of metallic nanoparticles. The degree of clustering of nanoparticles depends on the pathological origin of the tearproteins and consequently this dependence can be useful for prognosis of dry eye disease.
Keywords: Dry eyes, Tear proteins, Nanoparticles, Protein aggregation.
Nanoparticles have been used as drug delivery agentsand diagnostic probes1-3. Unconventional use of
nanoparticles has also been reported. For exampleplasmonic properties of nanoparticles have been used todetect glycation of proteins4, to trace conformational andfolding properties of proteins5, to enhance efficacy of drug6,as contrast agents (in MRI or microscopy for example)7. Inthe field of sensing and detection there have been severalreports, notable ones being detection of bacteria8, detectionof cancer cells1, 9, sensing various metabolites and alteringthermodynamic properties of energy rich fuels10. In the fieldof therapy and diagnostics various smart nanoparticles(e.g. designed core shell nanoforms) have been reportedwhich performs intelligent therapy, e.g. releasing a drug ina targeted fashion11, 12. There have been fewer reports onnanoparticle dictated photothermal therapy. Selected useof nanoparticles has also been reported in proteomicsgenomics and flow cytometry13, 14.
Dry eye is a multi-factorial disease which leads to burningand irritation on the ocular surface. The most commonsymptom of the disease is that the quantity of tearproduction decreases. Diagnosis of dry eye by Schirmer’stest is routinely followed by many ophthalmologistsworldwide. Although extensive researches have beenconducted on the disease, starting from SDS-PAGE15
protein analysis to proteomics16 and lipidomics17 still the
mechanism for the disease progression is obscure.Treatment of dry eyes with sodium hyaluronate18,autologous serum19, trehalose20 and artificial tear eyedrops21 have been experimented in animals. Thesetreatment methods are still not frequently used byophthalmologists because of the inconsistency in results.Our study would provide a new insight into the diseasediagnosis and treatment.
Despite the multidimensional progress in nanomedicinein the last decade in particular, the nano-clustering hasbeen ignored as a useful tool in diagnosis. In this paperwe have reported a simple cluster formation baseddiagnostic tool in dry eye disease. The report though in itspreliminary form has the unique perspective, that the wholeproperty has been holistically mapped such that there is adisease signature embedded in the nanoclustermorphology.
Our work also provides a nanotechnology route to traceprotein folding disease in general and dry eye disease inparticular as we have shown the extent of nano-clusteringmay be an implicit function of the disease status.
Methods
The study adhered to the tenets of the declaration ofHelsinki. Informed consent was obtained from both the
1Department of Biochemistry, University of Calcutta, 35 Ballygunge Circular Road, Kolkata-700019. 2Regional Institute of Ophthalmology,Calcutta Medical College, Kolkata-700073.Corresponding Author : Himadri Datta, E-mail: [email protected] on : 30/11/2014, Accepted on : 28/12/2014Conflict of Interest : None, Financial Disclosure : None
Original ArticleOriginal ArticleOriginal ArticleOriginal ArticleOriginal Article
CURRENT INDIAN EYE RESEARCH64
groups (Dry eyes and Control) prior to the start of theresearch.
Subjects
Twenty dry eye patients (20 female: 10 male; mean age29 ± 1.7 years) were recruited from the out patientsdepartment. Eighteen control individuals (11 female: 7male; mean age 28 ± 2.1 years) were enlisted from amongthe hospital staff. The inclusion and exclusion criteria weresame as mentioned in22.
Collection and extraction of tear fluid fromSchirmer’s strip
Tear fluids were collected using Schirmer’s strip. Followingthe collection process the wet portion of the strip wastransferred into 0.5ml eppendorf with a punctured bottom.The punctured eppendorf was then placed on top of 1.5mleppendorf with addition of 100µl extraction buffer (50mMNH4HCO3) on top of the strip and then centrifuged at 13,000rpm for 15 minutes at 4C23. Total time needed fromcollection to extraction process was 20 minutes. All theexperiments were conducted immediately after proteinextraction.
Total protein estimation by Bradford method
Biorad protein kit assay was used for total tear proteinestimation for dry eye patients and control. Absorption wasmeasured (Evolution 300 UV-VIS, Thermo Scientific) at595nm. Total tear protein concentration was normalizedto 0.1mg/ml for both groups for carrying all the experiments.
Synthesis and characterization of goldnanoparticles (GNPs) using tear proteins
To 1ml of tear proteins 1mM chloro auric acid (HAuCl4,
purchased from Arora Matthey, Kolkata, India) was addedand kept under stirring condition at room temperature untilthe solution color changes to red. Size and correlation co-efficient of the synthesized nanoparticles was measuredby Zeta Sizer Nanoseries- NANO-ZS. Transmissionelectron microscopy (TEM) was done on a copper grid(Siemens Elmiskon 101 TEM).
Results
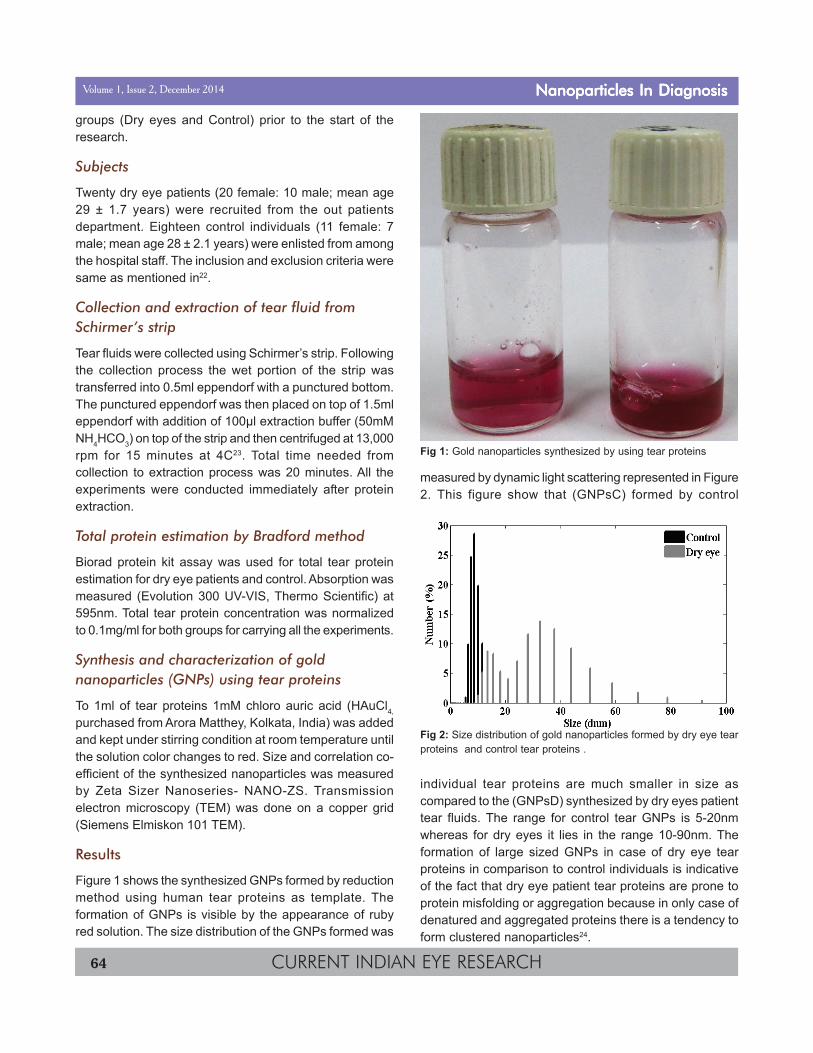
Figure 1 shows the synthesized GNPs formed by reductionmethod using human tear proteins as template. Theformation of GNPs is visible by the appearance of rubyred solution. The size distribution of the GNPs formed was
measured by dynamic light scattering represented in Figure2. This figure show that (GNPsC) formed by control
individual tear proteins are much smaller in size ascompared to the (GNPsD) synthesized by dry eyes patienttear fluids. The range for control tear GNPs is 5-20nmwhereas for dry eyes it lies in the range 10-90nm. Theformation of large sized GNPs in case of dry eye tearproteins in comparison to control individuals is indicativeof the fact that dry eye patient tear proteins are prone toprotein misfolding or aggregation because in only case ofdenatured and aggregated proteins there is a tendency toform clustered nanoparticles24.
Fig 2: Size distribution of gold nanoparticles formed by dry eye tearproteins and control tear proteins .
Fig 1: Gold nanoparticles synthesized by using tear proteins
Nanoparticles In DiagnosisNanoparticles In DiagnosisNanoparticles In DiagnosisNanoparticles In DiagnosisNanoparticles In DiagnosisVolume 1, Issue 2, December 2014
CURRENT INDIAN EYE RESEARCH 65
Our hypothesis that dry eye tear proteins leads to largersized or clustered nanoparticles formation is further verifiedby TEM images shown in Figure 3, 4A and B. Figure 3shows TEM image of GNPsC, it can be seen from theimage that control tear proteins leads to smaller sized GNPswithout any cluster formation indicative of the fact that thereis no protein aggregation or misfolding. Whereas in caseof GNPsD as represented in Figure 4A and B, there is astrong indication that dry eye patients tear proteins aremore prone to protein misfolding leading to clusterednanoparticles formation with a much higher size distributioncompared to GNPsC.
Discussion
Protein mediated synthesis of metallic nanoparticles havebeen carried our earlier25. It has been reported that thereis an impressive relation between the folding status andthe nanosurface topology26. The unfolded proteins in whichmore hydrophobic surface is exposed are likely to offer adifferent template for synthesis of nanoparticles ascompared to proteins in their native state in which there isa known hydrophobic collapse (hydrophobic groups in theirnative state been mostly concealed from the aqueousenvironment), as higher hydrophobic surface would leadto formation of nanoparticles with extended clusteringpropensity. The whole process may be considered as asnap shot of the folding status of the proteins.
While in this paper we show that the method may be areliable indicator of dry eye disease, what remains to beexplored is a general validity of this folding basedtemplating approach in exploring protein conformationaldisease in general.
Furthermore the different classification of dry eye diseaseas for example evaporative dry eye can also be comparedusing this method. The method can be particularly usefulfor determining the efficacy of a drug which would curedry eye disease. This drug discovery tool has particularimportance as presently there is no known drug fortreatment of dry eyes and the mechanism is yet to bediscovered. The fact that there is abundance of unfolded
Fig 4A: TEM image of GNPsD.
Fig 4B: TEM image of GNPsD.
Fig 3: TEM image of GNPsC.
Nanoparticles In DiagnosisNanoparticles In DiagnosisNanoparticles In DiagnosisNanoparticles In DiagnosisNanoparticles In DiagnosisVolume 1, Issue 2, December 2014
CURRENT INDIAN EYE RESEARCH66
proteins leading to such extended nanocluster formationalso indicates that dry eye may be a class of proteinconformational disease.
Our study was conducted on patients with Schirmer’s score<5mm, from the Schirmer’s strip tear proteins was extractedand total tear protein estimated and normalized for furtherexperimental procedure. The idea that tear proteins couldform a template for nanoparticles synthesis came fromearlier work25. After the synthesis of GNPs by dry eyesand control individuals tear proteins, the size measurementand particle formation analysis was done by DLS and TEM.The DLS data shown in Figure 2 represents size distributionhistogram for GNPsC and GNPsD respectively. The figuresuggests that control tear proteins forms smaller GNPswith respect to dry eye tear proteins. This could be due tothe fact that diseased state tear proteins are in a misfoldedor aggregated structure which serves as a less preferredtemplate for monodisperse particle formation as opposedto healthy tear proteins where there is no proteinaggregation. The presence of extended structures in dryeye tear proteins increases the hydrophobicity which alsoresults in decrease reduction capacity for nanoparticlesformation.
To further validate our hypothesis TEM study wasperformed, from the TEM images it is apparent that GNPsCand GNPsD lead to monodisperse and clusterednanoparticles formation. Figure 3 demonstrate that controltear proteins forms smaller and monodisperse goldnanoparticles owing to the absence of any extended ormisfolded protein aggregates. This observation iscontradicted in case of dry eye patient tear protein (shownin Figure 4A & B), here the particle size as well asmonodispersity is different. Dry eye tear proteins lead tobigger size GNPs formation along with it there is formationof cluster, which may be due to extended proteinaggregates in dry eye tear proteome.
Conclusion
To conclude we can say that dry eyes falls into proteinconformational related disease. This study would help inthe near future for the correct and accurate treatment ofthe disease.
References
1. Brigger I, Dubernet C, Couvreur P. Nanoparticles incancer therapy and diagnosis. Advanced drug deliveryreviews 2002;54:631-51.
2. Liu Y, Miyoshi H, Nakamura M. Nanomedicine for drugdelivery and imaging: a promising avenue for cancertherapy and diagnosis using targeted functionalnanoparticles. International Journal of Cancer2007;120:2527-37.
3. Emerich DF, Thanos CG. The pinpoint promise ofnanoparticle-based drug delivery and moleculardiagnosis. Biomolecular engineering 2006;23:171-84.
4. Singha S, Bhattacharya J, Datta H, Dasgupta AK. Anti-glycation activity of gold nanoparticles. Nanomedicine:Nanotechnology, Biology and Medicine 2009;5:21-9.
5. Sen T, Haldar KK, Patra A. Au nanoparticle-basedsurface energy transfer probe for conformationalchanges of BSA protein. The Journal of PhysicalChemistry C 2008;112:17945-51.
6. Chen AM, Zhang M, Wei D, et al. Co delivery ofDoxorubicin and Bcl 2 siRNA by Mesoporous SilicaNanoparticles Enhances the Efficacy ofChemotherapy in Multidrug Resistant Cancer Cells.Small 2009;5:2673-77.
7. Frias JC, Williams KJ, Fisher EA, Fayad ZA.Recombinant HDL-like nanoparticles: a specificcontrast agent for MRI of atherosclerotic plaques.Journal of the American Chemical Society2004;126:16316-17.
8. Lee H, Yoon TJ, Weissleder R. UltrasensitiveDetection of Bacteria Using Core–Shell Nanoparticlesand an NMR Filter System. Angewandte ChemieInternational Edition 2009;48:5657-60.
9. Herr JK, Smith JE, Medley CD, Shangguan D, TanW. Aptamer-conjugated nanoparticles for selectivecollection and detection of cancer cells. AnalyticalChemistry 2006;78:2918-24.
10. Nielsen LJ, Olsen LF, Ozalp VC. Aptamers embeddedin polyacrylamide nanoparticles: a tool for in vivometabolite sensing. Acs Nano 2010;4:4361-70.
11. Cheng J, Teply BA, Sherifi I, et al. Formulation offunctionalized PLGA–PEG nanoparticles for in vivotargeted drug delivery. Biomaterials 2007;28:869-76.
12. Singh R, Lillard Jr JW. Nanoparticle-based targeteddrug delivery. Experimental and molecular pathology2009;86:215-23.
13. Gao X, Nie S. Quantum dot-encoded mesoporousbeads with high brightness and uniformity: rapidreadout using flow cytometry. Analytical chemistry2004;76:2406-10.
14. Coto-García AM, Sotelo-González E, Fernández-Argüelles MT, Pereiro R, Costa-Fernández JM, Sanz-Medel A. Nanoparticles as fluorescent labels foroptical imaging and sensing in genomics andproteomics. Analytical and bioanalytical chemistry2011;399:29-42.
Nanoparticles In DiagnosisNanoparticles In DiagnosisNanoparticles In DiagnosisNanoparticles In DiagnosisNanoparticles In DiagnosisVolume 1, Issue 2, December 2014
CURRENT INDIAN EYE RESEARCH 67
15. Grus F, Augustin A, Evangelou N, Toth-Sagi K.Analysis of tear-protein patterns as a diagnostic toolfor the detection of dry eyes. European journal ofophthalmology 1997;8:90-7.
16. Zhou L, Beuerman RW, Chan CM, et al. Identificationof tear fluid biomarkers in dry eye syndrome usingiTRAQ quantitative proteomics. Journal of proteomeresearch 2009;8:4889-905.
17. Chen J, Green-Church KB, Nichols KK. Shotgunlipidomic analysis of human meibomian glandsecretions with electrospray ionization tandem massspectrometry. Investigative ophthalmology & visualscience 2010;51:6220-31.
18. Shimmura S, Ono M, Shinozaki K, et al. Sodiumhyaluronate eyedrops in the treatment of dry eyes.British journal of ophthalmology 1995;79:1007-11.
19. Tsubota K, Goto E, Fujita H, et al. Treatment of dryeye by autologous serum application in Sjögren’ssyndrome. British journal of ophthalmology1999;83:390-5.
20. Matsuo T, Tsuchida Y, Morimoto N. Trehalose eyedrops in the treatment of dry eye syndrome.Ophthalmology 2002;109:2024-9.
21. Giibbels M. Corneal epithelial permeability of dry eyesbefore and after treatment with artificial tears.Ophthalmology 1992;99.
22. Azharuddin M, Bera SK, Datta H, Dasgupta AK.Thermal fluctuation based study of aqueous deficientdry eyes by non-invasive thermal imaging.Experimental eye research 2014;120:97-102.
23. Posa A, Bräuer L, Schicht M, Garreis F, Beileke S,Paulsen F. Schirmer strip vs. capillary tube method:non-invasive methods of obtaining proteins from tearfluid. Annals of Anatomy-Anatomischer Anzeiger2013;195:137-42.
24. Basu N, Bhattacharya R, Mukherjee P. Protein-mediated autoreduction of gold salts to goldnanoparticles. Biomedical Materials 2008;3:034105.
25. Ravindra P. Protein-mediated synthesis of goldnanoparticles. Materials Science and Engineering: B2009;163:93-8.
26. Mahmoudi M, Lynch I, Ejtehadi MR, Monopoli MP,Bombelli FB, Laurent S. Protein• nanoparticleinteractions: opportunities and challenges. ChemicalReviews 2011;111:5610-37.
Nanoparticles In DiagnosisNanoparticles In DiagnosisNanoparticles In DiagnosisNanoparticles In DiagnosisNanoparticles In DiagnosisVolume 1, Issue 2, December 2014
CURRENT INDIAN EYE RESEARCH68
A Study Of Correlation Of Plasma Homocysteine With Serum LipidProfile In Retinal Vein OcclusionKapil Deb Lahiri1, Arunava Kundu2, Joya Ghosh1, Mriganka Baruah1, Champakali Biswas2, Amitava Das2,Nazneen Nazm2
Abstract
Purpose: Both hyperhomocysteinemia and dyslipidaemia are considered as an independent risk factor in retinal vein occlusion.This study was done to find out the correlation of plasma homocysteine with serum lipids in patients with retinal vein occlusion.Material & Methods: A total of 84 retinal vein occlusion cases and 65 age and sex matched controls were assayed to explore therelationship of plasma homocysteine with serum lipid profiles in this observational, cross sectional, open, comparative, eight monthstudy. Results: Plasma homocysteine, total cholesterol, triglyceride, LDL cholesterol and VLDL cholesterol levels were elevatedsignificantly (P <0.001) and HDL cholesterol was decreased significantly (P <0.001) in the patients with RVO as opposed tothe control subjects. Significant negative correlation was found between homocysteine and HDL cholesterol in RVO patients (r= -0.273, P < 0.029). Conclusions: Patients with low HDL cholesterol should be screened for HHcys as association of lowHDL cholesterol and HHcys might have a synergistic effect on the retinal circulation. Future study is needed to see whethertreatment of HHcys will increase the HDL cholesterol level and that can be an important preventive measure against developmentas well as treatment of retinal vein occlusion.
Keywords: Homocysteine (Hcys), Hyperhomocysteinemia (HHcys), High density lipoprotein (HDL), Low density lipoprotein(LDL), Retinal vein occlusion (RVO).
Retinal vein occlusion (RVO) is the 2nd most commonretinal vascular disorder after diabetic retinopathy with
prevalence ranging from 0.7% to 1.6%1. It is of three typesdepending on the site of occlusion and the consequentvascular damage - central retinal vein occlusion (CRVO),branch retinal vein occlusion (BRVO) and hemi centralretinal vein occlusion (HCRVO)2. Among them, CRVO havepoorer prognosis than the BRVO. The basic pathology ofthe disease is localized atherosclerosis. Both local (Raisedintra ocular tension) and systemic risk factors (Diabetesmellitus, Hypertension, Hyperlipidaemia) have beenassociated with RVO3.
In 1969, McCully suggested that moderate levels ofhyperhomocysteinemia (HHcys) might be associated withatherosclerosis4, 5. Mild hyperhomocysteinemia (HHcys) isalso reported as a risk factor for atherosclerosis in thecoronary, cerebral, and retinal vasculature6-9. There werealso reports in support of the hypothesis that HHcys wereassociated with RVO cases10-12.
Hcys is an amino acid containing sulfur. It is derived fromdietary methionine which is initially converted into S-
adenosyl methionine that donates the methyl group to amethyl accepter and itself forms S-adenosyl Hcys whichis eventually converted back to Hcys. It is eitherreconverted to methionine requiring B12 and folate ormetabolized to cystathionine requiring B6
13. Enzymesdficiency like cystathionine â-synthase (CBS) andmethyltetrahydrofolate reductase or nutritional deficienciessuch as B12, B6 and folate are the major causes of HHcys14.
Dyslipidaemia3, 15 and hyperhomocysteinemia10 wereconsidered as an independent risk factor in retinal veinocclusion but no study was done to find out the correlationbetween them in RVO. In this context, this study wasperformed to find out the correlation of plasmahomocysteine with serum lipids in patients of RVO.
Materials and methods
This observational, cross sectional, open, comparative,eight month study was conducted in ESIPGIMSR & ESICMedical College, Joka with a total of consecutive 84 (47males and 37 females) unilateral RVO cases attendingthe outpatient department of Ophthalmology. Sixty five (35
1Department of Biochemistry, 2Department of Ophthalmology, ESIPGIMSR & ESIC Medical college, Joka, Kolkata.Corresponding Author : Kapil Deb Lahiri, E-mail: [email protected] on : 27/11/2014, Accepted on : 30/12/2014Conflict of Interest : None, Financial Disclosure : None
Original ArticleOriginal ArticleOriginal ArticleOriginal ArticleOriginal Article
CURRENT INDIAN EYE RESEARCH 69
males and 30 females) age and sex matched controls wereincluded in the study. Presence of any of the followingconditions like pregnancy, lactation, malignancy, sepsis,liver and renal failure, recent vascular accidents (< 6months), previous thromboembolic events, inflammatorydisorders, thyroid disorder, diabetes mellitus, vitamin intake(B6 , B12 and folate), alcohol, drugs (methotrexate, fibrates)and smoking were excluded from the study population bydetailed history, clinical and biochemical examination. Thestudy was approved by the institutional ethics committeeand informed consent was obtained from all the studypopulations, in accordance with the Declaration of Helsinki.
Fasting blood samples were collected from the patientsand the controls. The blood samples were collected byvein puncture in EDTA vial and plain vial using disposablesyringe. The blood collected in EDTA vial was immediatelycentrifuged at 1000g at 25°C for 3 minutes and plasmawas separated and analyzed for Hcys. Samples werestored tightly capped at 2-8 °C for up to 48 hours if testingwas delayed. Plasma Hcys was estimated by enzymaticmethod in autoanalyser (Toshiba TBA40FR Biochemistryanalyser) with a Reagent kit, supplied by Lilac Clinicalchemistry division16. (Linearity extends to 50 ìmol/L)
The blood collected in plain vial was kept in tilted positionfor 30 minutes at room temperature and then centrifugedto separate serum for the estimation of lipid profile. Serumtotal cholesterol was measured after enzymatic hydrolysis
and oxidation17. The High density lipoprotein (HDL)cholesterol level was determined after precipitating thechylomicrons, Very low density lipoprotein (VLDL) and lowdensity lipoprotein (LDL) fragments, using phosphotungsticacid and magnesium chloride18. Serum triglyceride levelwas determined after enzymatic hydrolysis with lipases19.The serum LDL and VLDL cholesterol levels weredetermined using the formula of Friedwald T (1972)20.Serum lipid profiles were estimated in autoanalyser(Toshiba TBA40FR Biochemistry analyser) with a Reagentkit, supplied by coral.
Statistical analysis was performed using the Student’s t-test and Pearson’s correlation coefficient by SPSS software(Versions 16.0).
Results
The mean age of RVO patients and control participantswere 44.1 ± 15.2 years and 50.2 ± 10.6 years respectively.Of the 84 RVO cases 59 patients were BRVO, 22 wereCRVO and 3 were HCRVO.
Hcys levels were increased significantly in the patients withRVO (mean total Hcys, 17.86 ± 5.13 ìmol/L) as opposedto the control subjects (mean total Hcys, 12.05 ± 2.11 ìmol/L; P < 0.001). (Figure- 1)
Total cholesterol (209.2 ± 53 mg/dl) levels were elevatedsignificantly as opposed to the control (159.2 ± 30 mg/dl)(P <0.001). Triglyceride (175.3 ± 45.6 mg/dl) levels were
Fig: 1 :Comparison of Plasma Total Homocysteine level between RVO cases and Control
Lipid & Homocysteine In RvoLipid & Homocysteine In RvoLipid & Homocysteine In RvoLipid & Homocysteine In RvoLipid & Homocysteine In RvoVolume 1, Issue 2, December 2014
CURRENT INDIAN EYE RESEARCH70
elevated significantly as opposed to the control (96.4 ±22.1 mg/dl) (P <0.001). LDL cholesterol (127.7 ± 33.7 mg/dl) levels were elevated significantly as opposed to thecontrol (93.3 ± 17.2 mg/dl) (P <0.001). VLDL cholesterol(34.6 ± 9 mg/dl) levels were elevated significantly asopposed to the control (19.3 ± 4.6 mg/dl) (P <0.001) aswell as HDL cholesterol (30.8 ± 8.3 mg/dl) levels weredecreased significantly as opposed to the control (45.5 ±6.6 mg/dl) (P <0.001).
There was also significant negative correlation foundbetween homocysteine and HDL cholesterol in RVOpatients (r = -0.273, P < 0.029). (Table-1)
Discussion
A retinal arteriol and its corresponding vein share acommon adventitial sheath. Thickening of the arteriolappears to compress the vein. This causes secondarychanges, including venous endothelial cell loss, thrombusformation, and potential occlusion. Similarly, the centralretinal vein and artery share a common adventitial sheathat the arteriovenous crossings posterior to the laminacribrosa so that atherosclerotic changes of the artery maycompress the vein and precipitate the CRVO. It thereforeappears that both arterial and venous disease contributeto RVO. Venous occlusion causes elevation of venous andcapillary pressure with stagnation of the blood flow. Thisresults in hypoxia of the retina drained by the obstructedvein, which in turn results in damage to the capillaryendothelial cells and extravasation of blood constituents.Tissue presure is increased, causing further stagnation ofthe circulation and hypoxia, so that a vicious cycle isestablished.3
HHcys was reported as an independent risk factor forCRVO11-12, 21. An Odds Ratio (OR) of 3.0 for fasting HHcysin patients with CRVO was reported by Lattanzio et al14
and an OR of 1.3 was reported by another study in a
Chinese population22. Janssen et al23 have observed anoverall OR of 8.9 (95% CI, 5.7–13.7) for Hcys. The meta-analysis by Cahill et al24 have shown that raised plasmaHcys levels and low serum folate levels were associatedwith retinal vascular occlusion. Dayal S et al25 haveobserved that deficiency of either methionine synthase orfolate produces oxidative stress leading to the endothelialdysfunction in the cerebral microcirculation of mice. Thedirect cytotoxic effect on retinal vascular endothelial cellsby Hcys and Hcys thiolactone has also been reported in acase report by Poloshek et al26.
The results of the present study indicated that hcys levelswere increased significantly in the patients with RVO (meantHcys, 17.86 ± 5.13 ìmol/L) as opposed to the controlsubjects (mean tHcys, 12.05 ± 2.11 ìmol/L ; P < 0.001).(Figure-1)
There are various mechanisms reported regardingendothelial dysfunction by Hcys. These include diminishedbioavailability of nitric oxide27, abnormal expression ofvarious thrombotic factors28. Hcys can form stable disulfidebonds with protein cysteine residues and, in the process,alters or impairs the function of many proteins like albumin,fibronectin, transthyretin, annexin II, and factor V29. Hcysmay be metabolised into hcys-thiolactone which is a highlyreactive compound that contributes to Hcys toxicity inhumans30 (Hcys-thiolactone hypothesis) leading toendothelial dysfunction. HHcys can lead to upregulationof the inflammatory response in the vascular smoothmuscle cells that characterizes early atherogenesis31.
This study also observed that total cholesterol, triglyceride,LDL cholesterol and VLDL cholesterol levels were elevatedsignificantly (P <0.001) as well as HDL cholesterol wasdecreased significantly (P <0.001) in the patients with RVOas opposed to the control subjects. There are variousmechanisms reported regarding endothelial dysfunction
Total Triglycerides LDL HDL VLDLcholesterol cholesterol cholesterol cholesterol
* Correlation is significant at the 0.05 level (2-tailed).
Table-1: Correlations of Homocysteine with Total cholesterol, Triglycerides, LDL cholesterol, HDLcholesterol and VLDL cholesterol in RVO patients (N=84).
Lipid & Homocysteine In RvoLipid & Homocysteine In RvoLipid & Homocysteine In RvoLipid & Homocysteine In RvoLipid & Homocysteine In RvoVolume 1, Issue 2, December 2014
CURRENT INDIAN EYE RESEARCH 71
by LDL Cholesterol. It is initially converted into oxidizedLDL cholesterol by free radicals. The oxidized LDL is takenup by scavenger receptor on monocyte macrophagesleading to foam cell. It decreases the expression ofendothelial nitric oxide synthase and in turn inhibiting nitricoxide mediated vasorelaxation33. It also stimulatesInterleukin-1, tumor necrosis factor-alpha and interferon-gamma which cause leukocyte recruitment and adhesionto the endothelial cell34.
Although Jadav et al35 did not find any correlation betweenHcy with lipid profile in ischemic heart disease patientsbut our study observed a significantly negative correlationwith HDL Cholesterol in RVO patients (Table-1). This canbe explained by possible action of Hcys in reducing theexpression of peroxisome proliferator-activated receptor(PPARá) and decreased the ApolipoproteinA-I promoteractivity and its protein levels36. In addition to its influenceon ApolipoproteinA-I, hyperhomocysteinemia inhibitesreverse cholesterol transport by reducing circulating HDLvia inhibiting ApolipoproteinA-I protein synthesis andenhancing HDL cholesterol clearance in mice37.
It was well established that both HHcys and Dyslipidimeacan induce atherosclerotic changes. Our study showedthat low HDL cholesterol was aggravated by HHcys in RVOcases as evidenced by strong negetive correlation betweenthem. So the Patients with low HDL cholesterol should bescreened for HHcys as association of low HDL cholesteroland HHcys might have a synergistic effect on the retinalcirculation. Future study is needed to see whethertreatment of HHcys will increase the HDL cholesterol leveland that can be an important preventive measure againstdevelopment as well as treatment of retinal vein occlusion.
References:1. Klein R, Klein BE, Moss SE, Meuer SM: The
Epidemiology of retinal vein occlusion: The BeaverDam Study. Trans Am Ophthalmol Soc 2000; 98: 133-41.
2. Mitchell P, Smith W, Chang A. Prevalence andassociations of retinal vein occlusion in Australia. TheBlue Mountais Eye Study. Arch. Ophthalmol 1996; 114:1243–7.
4. McCully KS: Homocysteine, vitamins, and preventionof vascular disease. Mil Med 2004; 169(4): 325-9.
5. McCully KS: Vascular pathology of homocysteinemia:implications for the pathogenesis of arteriosclerosis.Am J Pathol 1969; 56:111-28.
6. Genser D, Prachar H, Hauer R, Halbmayer M, MlczochJ, Elmadfa I. Homocysteine, folate and vitamin B12in patients with coronary heart disease. Ann NutrMetab 2006; 50: 413–9.
7. Pianka P, Almog Y, Man O, Goldstein M, Sela BA,Loewenstein A. Hyperhomocysteinemia in patientswith nonarteric anterior ischemic optic neuropathy:central retinal artery occlusion and central retinal veinocclusion. Ophthalmology 2000;107:1588–92.
8. Wenzler EM, Rademakers AJ, Boers GH, CruysbergJR, Webers CA, Deutman AF. Hyperhomocysteine inretinal artery and retinal vein occlusion. Am JOphthalmol 1993;115:162–7.
9. Brown BA, Marx JL, Ward TP, Hollifield RD, Dick JS, BrozettiJJ, et al. Homocysteine: a risk factor for retinal venousocclusive disease. Ophthalmology 2002;109:287–90.
10. Lahiri KD, Dutta J, Datta H, Das H.Hyperhomocysteinemia, as an independent risk factorfor retinal venous occlusion in an Indian population.Ind J Clin Biochem 2013;28:61-4.
11. Chua B, Kifley A, Wong TY, Mitchell P. Homocysteineand retinal emboli the Blue Mountains eye study. AmJ Ophthalmol 2006;142:322–4.
12. Chau B, Kifley A, Wong TY, Mitchell P. Homocysteineand retinal vein occlusion: population based study.Am J Ophthalmol 2005;139:181–2.
14. Lattanzio R, Sampirtro F, Ramonia A, Fattorini A,Brancato R. Moderate hyperhomocysteinemia andearly-onset central retinal vein occlusion. Retina 2006;26:65–70.
15. O Mahoney PR, Wong DT, Roy JG. Retinal VeinOcclusion & Traditional risk factors for Atherosclerosis.Arch Ophthalmol 2008;126:692-9.
16. Ueland PM, Refsum H, Stabler SP, Malinow MR,Andersson A, Allen RH et al. Total Homocysteine inPlasma or Serum: Methods and Clinical Applications.Clin Chem 1993;39:1764-79.
17. Allian CC, Poon LS, Chan SG, Richard W and PaulFF. Enzymatic determination of total serumcholesterol. Clin chem 1974;20:470-75.
18. Steele BW, Kochler DF, Azar MM, Blas Z and KpwaskiPT. High density lipoprotein cholesterol fractions,prepared by precipitation technique. Clin chem 1976;22:98-101.
19. Buccola G and David M. Quantitive determination ofserum triglycerides by use of enzymes. Clin Chem1973;19:476-81.
Lipid & Homocysteine In RvoLipid & Homocysteine In RvoLipid & Homocysteine In RvoLipid & Homocysteine In RvoLipid & Homocysteine In RvoVolume 1, Issue 2, December 2014
CURRENT INDIAN EYE RESEARCH72
20. Fredickson DS and Frieldwald T. estimation of theconcentration of low density cholesterol in plasma,without use of preparative centrifuge. Clin Chem 1972;18:499-504.
21. Di Crecchio L, Parodi MB, Sanguinetti G, Iacono P,Ravalico G. Hyper homocysteinemia and themethylenetetrahydrofolate reductase 677C-T mutationin patients under 50 years of age affected by centralretinal vein occlusion. Ophthalmology 2004;111:940–5.
22. Gao W, Wang YS, Zhang P, Wang HY.Hyperhomocysteinemia and low plasma folate as riskfactors for central retinal vein occlusion: a case-controlstudy in a Chinese population. Graefes Arch Clin ExpOphthalmol 2006;244:1246–9.
23. Janssen MC, den Heijer M, Cruysberg JR,Wollersheim H, Bredie SJ. Retinal vein occlusion: aform of venous thrombosis or a complication ofatherosclerosis?—a meta-analysis of thrombophilicfactors. Thromb Haemost 2005;93:1021–6.
24. Cahil MT, Stinnett SS, Fekrat S. Meta-analysis ofplasma homocysteine, serum folate, serum vitaminB12, and thermolabile MTHFR genotype as risk factorsfor retinal vascular occlusive disease. Am JOphthalmol 2003;136:1136–50.
25. Dayal S, Devlin AM, McCaw RB, Liu ML, Arning E,Bottiglieri T et al. Cerebral vascular dysfunction inmethionine synthase-deficient mice. Circulation 2005;112:737–44.
26. Poloshek Fowler B, Unsold R, Lorenz B. Disturbedvisual system function in methionine synthasedeficiency. Graefes Arch Clin Exp Ophthalmol 2005;243:497–500.
27. Weiss N. Mechanisms of increased vascular oxidantstress in hyperhomocysteinemia and its impact onendothelial function. Curr Drug Metab 2005;6:27–54.
28. Postea O, Krotz F, Henger A, Keller C, Weiss N.Stereospecific and redox-sensitive increase inmonocyte adhesion to endothelial cells by
29. Jacobsen DW, Catanescu O, Barbato JC. Moleculartargeting by homocysteine: a mechanism for vascularpathogenesis. Clin Chem Lab Med 2005; 43:1076-83.
30. Selhub J. The many facets of hyperhomocysteinemia:studies from the Framingham cohorts. J Nutr 2006;136:1726S–30S.
31. Kerkeni M, Tnani M, Chuniaud L, Miled A, MaaroufiK, Trivin F. Comparative study on in vitro effects ofhomocysteine thiolactone and homocysteine onHUVEC Cells: evidence for a stronger proapoptoticand proinflammative homocysteine thiolactone. MolCell Biochem 2006;291:119–26.
32. Witztum JL and Steinberg D. Role of oxidized lowdensity lipoprotein in athero-genesis. J Clin Investig1991;88:1785-92.
33. Liao JK, Shin WS, Lee WY and Clark SL. Oxidizedlow density lipoprotein decreases the expression ofendothelial nitric oxide synthase. J Biol Chem 1995;270;319-24.
34. Witztum JL. Immunological response to oxidized LDL.Atherosclerosis 1997;131:S9-S11.
35. Jadav AS, Bhagwat VR, Rathod IM. Relationshipstudy of plasma homocysteine with lipid profileparameters in ischemic heart disease. Ind J ClinBiochem 2006;21:106-10.
36. Mikael LG, Genest J Jr, Rozen R. Elevatedhomocysteine reduces apolipoprotein A-I expressionin hyperhomocysteinemic mice and in males withcoronary artery disease. Circulation research 2006;98:564-71.
37. Liao D, Tan H, Hui R, Li Z, Jiang X, Gaubatz J, YangF, et al. Hyperhomocysteinemia decreases circulatinghighdensity lipoprotein by inhibiting apolipoprotein A-I Protein synthesis and enhancing HDL cholesterolclearance. Circulation research 2006; 99: 598-606.
Lipid & Homocysteine In RvoLipid & Homocysteine In RvoLipid & Homocysteine In RvoLipid & Homocysteine In RvoLipid & Homocysteine In RvoVolume 1, Issue 2, December 2014
CURRENT INDIAN EYE RESEARCH 73
Texture Quantification Of Choroidal NeovascularizationImages Through Differential Box Counting MethodSandeep V Paranjape1, Sangmeshwar S Pendalwar2, Ajoy K Ray3, Jyotirmoy Chatterjee1, Sambuddha Ghosh5
1School of Medical Science and Technology, IIT Kharagpur, India, 2SSGM College of Engineering Shegaon, India, 3Bengal Engineering andScience University, Shibpur, India, 4Regional Institute of Ophthalmology, MCH, Kolkata, India.Corresponding Author : Sandeep V Paranjape, E-mail: paranjapesand@ gmail.comReceived on : 24/11/2014, Accepted on : 30/12/2014Conflict of Interest : None, Financial Disclosure : None
Abstract
Purpose: To quantify the Choroidal Neovascularization (CNV) image textures using Differential Box-Counting method. Method:DFA images of 10 individuals including pathological subjects were used for textural quantification. Pre-processing was carried outfor the generation of vessel free fundus images for better discrimination with more detailed texture information. Subsequently, toquantify textural information fractal based method is used. Result: The fractal features; fractal dimension, standard deviation andLacunarity measures found to be promising in pathological images over normal fundus images. Conclusion: The empiricalevaluation of pre-processed fundus images with DBC features has shown the minute difference between normal and CNV affectedimages.
Digital fundus angiography (DFA) images have beenwidely used by the ophthalmologists for treatment
planning and diagnosing retinal vascular and non-vascularpathology. Visual inspection of the retinal non-vasculaturemay reveal severity of diseases related with Age relatedMacular Degeneration (AMD); specifically choroidalneovascularization (CNV), which is a major cause of adultblindness due to proliferation of blood vessels and requiresextensive analysis from specialist. Endeavoring to reducethe effect of CNV includes obtaining and analyzing DFAimages of the optic fundus at regular intervals. Earlydetection of changes to the blood vessel patterns canprevent major vision loss.
An automatic assessment of optic fundus abnormalitiesinitially requires the segmentation and removal of thevessels from the background. Next, obtained vessel-freeimages are used for texture quantification.
Texture information is one of the most important imagefeatures that can be used in many fields including medicalimage analysis extensively1.
A fundamental characteristic of texture is that it cannot beanalyzed without a frame of reference of tonal primitivebeing stated or implied2.
The texture features are obtained from several methods:statistical, geometrical, model-based, transform-basedmethods and Local Binary Operator (LBP3).
Fractal analysis has been useful in image processing forcharacterizing shape and gray-scale complexity. Thestatistical self-similarity and scale-invariance are twofundamental principles of fractal geometry. Fractalgeometry and fractal models are applied to most of naturalobjects which are not ideal but semi-fractal. Fractaldimension gives detail characteristics on the statistical self-similarity and the spatial distribution irregularity ofbiomedical images4.
Sarkar and Chaudhuri5 proposed a differential box-counting(DBC) method advantageous with its wide independentscale range and low computational complexity. The DBCmethod was testified to be an effective method and usedfor texture image classification successfully.
Materials and Methods:
We have tested our method on publically availabledatabase (DRIVE) consisting of digital fundus angiogramimages. It consists of 40 images legitimate data. Theimages are acquired in digital form using 3 CCD cameras
Original ArticleOriginal ArticleOriginal ArticleOriginal ArticleOriginal Article
CURRENT INDIAN EYE RESEARCH74
with 45o FOV. The image resolution is 768 X 584 pixels, 8bits per pixel. The training set of 20 images including threepathological images and remaining non-CNV images9including images of diabetic retinopathy) were consideredfor texture quantification. The labeled images wereobtained through manual segmentation and also testedour method on 10 individual subject’s DFA images providedby the ophthalmologist.
The green channel shows better contrast over the otherchannels of RGB image. Hence green channel wasextracted from RGB image. Next, the gray scale imageobtained through green channel image was taken as inputfor vessel removal. The resulting image was then used fortexture quantification through DBC method.
Differential Box-counting method requires a meshing ofthe fractal object and formulation of a probability in eachgenerated box. Finally the log of the number of boxescounted is plotted alongside the log of the scaling factorfor each stage of partitioning, yielding a set of points on aline. The measures at different scales are obtained throughcounting the minimum number of boxes of different size,which entirely cover the whole surface instead of directlymeasuring an image surface. The DBC5 can also be usedin FD evaluation of multi-fractal spectrum computingmethods. By covering a fractal object with boxes of lengthr, the FD is estimated as:
)log())(log(lim
0 rrNFD
r→=
Where N(r) is total number of boxes needed to completelycover fractal object and r is the scaling factor. The slope ofthe best-fitting straight line is obtained from least-square
regression by plotting ))(log( rN versus )log(r .
Assuming the image of size M X M pixels scaled down toa size s x s where M/2 e” s >1 and s is an integer. Thereforewe have r=s/M. Consider the image as a 3-D space with(x, y) denoting 2-D position and the third coordinate (z)denoting gray level. The (x, y) space is partitioned intogrids of size s x s. Each grid is consisting of the column ofboxes of size s x s x s’. If the total number of gray levels isG then,
G/s' = M/s
Let the minimum and maximum gray level of the image inthe (I, j) th grid fall in box number k and l, respectively. The
equation below is the contribution of rN in (I, j)th grid.
1),( +−= kljinr
Taking contributions from all grids, ),(,
jinNji
rr ∑=
Because of the differential nature of computing rn , it is
called DBC approach. It gives a better approximation tothe boxes intersecting the image intensity surface, whichis quantized in space and gray value, in particular whenthere is sharp gray level variation in neighboring pixels inthe image.
Lacunarity is one of the most reliable fractal featuresdefined as the measure of lumpiness in an image;heterogeneity. It aids in discrimination of the visualperception sham in case of two almost identical fundusimages regarding fractal dimension.
Results:
The fractal features; fractal dimension, standard deviationand Lacunarity measures found to be promising inpathological images over non-CNV fundus images.
The results were obtained by taking non-CNV andpathology (CNV affected) images. Prior to crop sections,images were pre-processed, to improve the texture featurediscrimination, for textural feature quantification throughDBC method to extract prominent fractal feature. Both, non-CNV and pathology image cross-sections of macular regionwere taken (Figure 1 (a),(b)) for further analysis and thevalues of fractal features were obtained. The mostpromising outcomes are drawn [Table 1].
Table 1: Comparison of fundus images forFractal features quantification
Image/Features FDAvg FDSD FDLacunarity
Image1_N 1.8047 0.3828 0.0450
Image2_P 1.6701 0.4306 0.0665
Image1_N 1.8080 0.4056 0.0503
Image2_P 1.6970 0.4010 0.0558
FDAvg = Average fractal dimension, FDSD = Standarddeviation in FD, FDLacunarity = Lacunarity in FD, Image_N =Normal image, Image_P = Pathology image
TTTTTexture of CNVMexture of CNVMexture of CNVMexture of CNVMexture of CNVMVolume 1, Issue 2, December 2014
CURRENT INDIAN EYE RESEARCH 75
Discussion
Values of non-CNV images revealed almost samedimensions, standard deviation and lacunarity. WhereasCNV affected images demonstrated drastic change in allthe fractal feature values. Lacunarity estimated in Table 1shows a clear discrimination between non-CNV andpathology DFA image textures. The empirical evaluationof pre-processed fundus images with DBC features thuscan reveal the difference between non-CNV and CNVimages.
Acknowledgement:
The authors would like to thank Regional Institute ofOphthalmology, MCH, Kolkatta and Dr. PrashantBavankule, Nagpur for the support in obtaining the images.
References
1. Tuceryan M, Jain AK. Texture analysis, Ch. 2.1, inHandbook of Pattern Recognition and ComputerVision. Chen CH, Pau LF, Wang PSP, eds., WorldScientific, Singapore, 1993. pp. 235-76.
2. Haralick RM. Statistical and Structural Approaches toTexture. Proceedings of the IEEE 1979; 67:786-804.
3. Sarkar N, Chaudhuri B. An Efficient Differential Box-counting Approach to Compute Fractal Dimension ofImage. IEEE Trans.Systems, Man and Cybernetics1994; 24: 115-20.
4. Ojala T, Pietikainen M, Harwood D. A comparative studyof texture measures with classification based on featuredistribution. Pattern Recogn 1996; 29: 51–9.
5. R. Lopes, N. Betrouni. Fractal and multifractal analysis:a review. Med Image Anal 2009; 13: 634–49.
Ocular involvement of tubercular bacilli is diverse and extensive. Predominant anterior segment involvement includes interstitialkeratitis, phlyctenular nodules and scleritis. We describe a rare manifestation of ocular tuberculosis presenting as corneal fistula.
1Department of Ophthalmology, Nil Ratan Sircar Medical College and Hospital, 138 AJC Bose Road, Kolkata-14.Corresponding Author : Somnath Mukhopadhyay, E-mail: [email protected] on : 15/04/2014, Accepted on : 30/11/2014Conflict of Interest : None, Financial Disclosure : None
Tuberculosis is fast emerging as the most commoncause of mortality and morbidity globally. It is estimated
that about one-third of world’s population is currentlyinfected with Mycobacterium tuberculosis.1 During the lasttwo decades with the emergence of HIV infection especiallyin African and in Asian countries, the incidence of extra-pulmonary and multi-drug resistant tuberculosis is on therise.2 Among other organs of the body having high oxygentension, eye is vulnerable to tuberculous infection.Ophthalmological involvement of tuberculosis is diverseand inclusive of both anterior segment (lid granuloma,scleritis, phlyctenular keratoconjunctivitis and interstitialkeratitis) and posterior segment (choroidal tubercles, sub-retinal abscess, retinal vasculitis, neuroretinitis and opticneuritis) involvement.3 We present an interesting case oftubercular corneal fistula.
Case Report
A 22 year male patient presented to Institutional corneaclinic about a month ago with a history of corneal ulcer inright eye persisting for more than six weeks. He was initiallytreated elsewhere with a combination of topical natamycinand moxifloxacin for about a month without improvement.No history of trauma or ocular foreign-body was obtained.His presenting vision in the involved eye was 6/60 withaccurate projection in all directions. Slit-lamp evaluationrevealed presence of a corneal fistula near 7 o’clock areawith positive Seidel’s test. A 1mm zone of cellular infiltrationwas seen around the fistula. Iris was incarcerated aroundthe fistulous tract (causing a pupillary drag) with a central
hole through which aqueous seepage was documented.Anterior chamber was maintained except the area of iris-adherence. Iris pigment dispersion was noted on theanterior lens capsule. No abnormal anterior chamberreaction and endothelial deposit was noted in righteye.Fundus evaluation by indirect ophthalmoscope wasnormal in both the eyes. Vision and anterior segmentevaluation of the fellow eye was normal.
A decision was made to perform a full thickness patch graftin the right eye. Medical records of the patient revealedthat he was getting anti-tubercular treatment (ATT) forpulmonary tuberculosis (PTB) in the Department of ChestMedicine of our hospital. Systemic examination revealeda high ESR but normal HIV, HBV and HCV serology. Full
Case ReportCase ReportCase ReportCase ReportCase Report
CURRENT INDIAN EYE RESEARCH 77
thickness patch graft was performed (SM) under peribulbaranaesthesia with sedation taking a donor disc that was0.25mm larger than the zone of infiltration in the recipientcorneal bed. The removed recipient button was sent formicrobiological examination. He was put on topicalmoxifloxacin (0.5%) four times a day for two weeks andtopical prednisolone acetate (1%) with a slow taper. Therecipient button showed presence of MycobacteriumTuberculosis bacilli in Z-N stain. Till the last follow-up sixmonths after operation, he had a clear graft with norecurrence.
Discussion
Haematological dissemination of tuberculous bacilli isresponsible for choroidal involvement.Granuloma formation(tuberculoma) causes lid involvement, choroidal masslesion and sub-retinal abscess formation. Somemanifestations (phlyctenulitis and interstitial keratitis) aresupposed to be due to immunogenic response tomycobacterium.4 Due to its avascularity, cornea is immune-privileged. We may assume that absence of other known
causes of corneal fistula formation (trauma, chemical insult,stem cell deficiency disorders, collagen vascular diseaseand hepatitis infection) in a patient on ATT for PTB alongwith microbiological report of recipient disc point towardstuberculous aetiology of corneal fistula formation.
References:1. Centers for Disease Control and Prevention.
Epidemiologic notes and reports, expandedtuberculosis surveillance and tuberculosis morbidity-United States (1993). MMWR Morb Mortal Wkly Rep1994; 43:361-6.
2. Centers for Disease Control and Prevention.Coincidence of HIV/AIDS and Tuberculosis-Chicago1982-1993. MMWR Morb Mortal Wkly Rep 1995. ;44:227-31.
Current Indian Eye Research (CIER) is the journal of Ophthalmic Research Group, which gives editorialfreedom to the editor of CIER. CIER follows guidelines of editorial independence proposed by World
Association of Medical Editors and code of good publication practice of the Committee of Publication Ethics.
CIER is intended for professionals associated with medical research and practice, without warranty, express or
implied. Statements in the journal are responsibilities of the authors and advertisers and not the author’sinstitution, publisher, editors or the Ophthalmic Research Group. Publication of advertisement does not imply
Sample Size Calculation For Research Studies In OphthalmologyArun Sharma1
Sample size is a crucial component of research design.More often researchers want sample size to be justified
on non statistical grounds. For example, a researcher maysay that I could get only these many cases in the specifiedtime period so as a statistician do something to make thestudy valid in spite of whatever sample size I have used.Similarly, financial constraint is sometimes cited an excusefor not having attained a given sample size. Others viewsample size as a biggest hurdle in their conduct of amethodologically correct research. So let us simplify theissue of sample size once forever.
Why do we need to calculate a sample size?An ideal research is one where no sample is required,meaning thereby that all eligible persons are included inthe study. More often than not, it is next to impossible dueto time, money and other resource constraints. Therefore,the focus is on conducting the research on a smallernumber of subjects in such a way that the findings areapplicable on the entire population in question and not theselected sample. It may be best explained by an analogyof buying rice from a traditional Indian grocery store. Theshopkeeper pulls out few grains of rice from a sackcontaining 40 kg of rice. By examining the few grains placedon the hand, one has to judge whether the rice in the sackis of good quality or not. Similarly, in research by conductingthe experiment on a few subjects we want to judge whetherthe findings will be applicable to all subjects of the sametype. In order to be as correct as possible in this endeavor,two criteria are to be met. One, the way sampling is doneor sample is selected and second the appropriate numberof subjects selected. In this article, we will focus on the
sample size that is the number of subjects to be selected.
In ophthalmology, we have to be careful about few thingsin sample size estimation. First that each person has twoeyes and that one person at a time may present one orboth of his/her eyes for the purpose of research. So here,each eye is a sample and the sample size calculated isthe number of eyes and not number of individuals.However, if right eye of person is different from the left eyeand this has a bearing on the research, then we have totreat right eye as a separate entity from left eye and thiswill have a bearing on the process of sampling. Similarly,if a pathology in one eye of a person has the potential ofspreading to the other eye of the same person, and weare looking at determinants of the illness, then we have touse individual persons as our sample and not individualeye as a sampling unit.
Every research study will have one outcome variable. Thisoutcome variable may be qualitative, for example outcomeof a treatment may be cure or death, occurrence of diseaseas a result of exposure to a risk factor or non occurrenceof the same. Variables which have two or more categoricaloutcomes are called qualitative variables. In case of suchvariables, outcome is expressed as proportion. Forexample, what proportion of patients suffering from cataractwill be cured after surgery.On the other hand, the outcome variable may be ameasurable quantity, like intra ocular pressure, focal length,body weight, hemoglobin level, such variables are calledquantitative variables. Here the outcome is expressed asmean and Standard Deviation or Standard Error, providedthe variable has a normal distribution.
ABSTRACT
An ideal research is one where no sample is required, meaning thereby that all eligible persons are included in the study. It is nextto impossible due to time, money and other resource constraints. In ophthalmology, we have to be careful about few things insample size estimation. First that each person has two eyes and that one person at a time may present one or both of his/her eyesfor the purpose of research. So here, each eye is a sample and the sample size calculated is the number of eyes and not number ofindividuals. However, if right eye of person is different from the left eye and this has a bearing on the research, then we have to treatright eye as a separate entity from left eye and this will have a bearing on the process of sampling. Sample size depends on type ofresearch design, whether it is descriptive, analytical or experimental. Different formulae are used for calculating the sample size fora study depending on the type of variables and study designs. Several software are available for calculating sample size.
1University College of Medical Sciences, University of Delhi, Delhi 110 095.Corresponding Author : Arun Sharma, E-mail: [email protected] on : 07/01/2015, Accepted on : 15/01/2015Conflict of Interest : None, Financial Disclosure : None
Research MethodologyResearch MethodologyResearch MethodologyResearch MethodologyResearch Methodology
CURRENT INDIAN EYE RESEARCH 79
Finally to talk about sample size, it depends on type ofresearch. Whether it is descriptive, analytical orexperimental.
A descriptive research study is one in which we want toestimate the magnitude of a problem/disease or healthcondition or the distribution of the disease/health conditionwith respect to time place and person. For example, toknow the prevalence of cataract in a given populationrequires a descriptive study design. Similarly, to estimatethe incidence of retinopathy among diabetics, a descriptivestudy design is required. Thus to calculate incidence orprevalence or age and gender distribution of an ophthalmiccondition we need to conduct a descriptive study. Fordescriptive studies, sample size is calculated using afollowing standard formula: (z(1-α/2))2pq/I2
Where,
p denotes the prevalence of the condition expressedas absolute percentage
q = 1-p
z = the z-score for the confidence interval of theprevalence to be estimated. Conventionally, 95%confidence interval is used and the correspondingvalue of z is 1.96 and for 99% confidence interval ( toget more precise value), it is 2.58
l denotes the permissible error within which theprevalence estimate will be considered as valid.
Many a times question is asked, if the prevalence is alreadyknown (p), why should I study it again? Or another questionasked is, what if the prevalence is not known. If theprevalence for the given population is already known,obviously there is no need to carry out the study. But ifprevalence in the given population is not known, we mayuse the prevalence value estimated by other researchersin other population groups which is similar to the populationthat the researcher wants to study. If no such prevalencevalue is available, there are two options. Either a scientificguess can be used or a pilot study may be conducted on asmall fraction of the population to derive a quick estimateof the prevalence.
Example: Suppose the estimated prevalence ofcataract is 30% as reported in a study conducted on asimilar population. In order to find a true estimate ofcataract prevalence within 5% of the known estimate(that is, the detected prevalence will be between 25%and 35%), the required sample size will be given asbelow:
Now, the question is 323 eyes or 323 persons. It dependson the premise of the study. If the research question is,“What proportion of eyes have cataract?”, we need toincluded 323 eyes. If the question is “What proportion ofpeople have cataract, at least in one eye?”, we need tostudy 323 people. In the second case, even if the personhas cataract in both eyes, it will be treated as one unit forsample size estimation. Answer to the first question isuseful, if we want to estimate the number of eyes to beoperated in a given area. The answer to second questionis useful if we want to know the magnitude of cataractrelated blindness in the community.
Usually population based surveys use such estimation ofsample size. This sample size estimation is valid whensimple random sampling is used. If cluster samplingtechnique is used then sample size estimate has to bemultiplied by a design effect. If stratified sampling techniqueis used then sample size should be estimated for eachstrata. For example, if there is a reason to believe thatcataract prevalence rates are different among male andfemale population, then sample size should be separatelycalculated for male and female populations.
Note: Prevalence is a qualitative variable expressed aspercentage. If the variable is quantitative and follows anormal distribution, the ‘pq’ of the above formula arereplaced by Standard Deviation (SD) of the quantitativevariable. For example, if intra ocular pressure is to beestimated in a population, then SD of mean intra ocularpressure is to be used, which again may be taken from apreviously conducted study or from a pilot study or can bea scientifically guessed estimate.
Analytical study: Case control study and cohort study arethe analytical studies. Case control studies are used tomeasure associations, commonly between risk factors anddiseases. The association is measured by Odds Ratio incase control studies and Relative Risk in cohort studies.In statistical parlance, these measures are also known aseffect size. Some statistical software calculate the samplesize based on Odds Ratio or Relative Risk, others ask foreffect size. In case control study, number of controls shouldbe at least equal to that of cases. Controls may be up to 4times the number of cases, any larger number of controlsbeyond this do not add value to the study.
In order to calculate the sample size for case controlstudies, the following formula is used
Where,r=ratio of control to cases,p*=average of proportion cases and controls exposedto the risk factor (p1+p2)/2, Zβ = Z score for the power of the study. For 80% power(type II error=20%), Z score is 0.84 and for 90% power(type II error= 10%), Z score is 1.28.Zα/2=Z score for the type I error (conventionally Type Ierror is fixed at 95% and α/2 is used for two tailedsignificanceNote: Z score tables are available in most of theStatistics text booksp1=proportion of cases exposed to the risk factor forwhich the study is being carried outp2=proportion of controls exposed to the risk factor forwhich the study is being carried outp1-p2 is a measure of effect size
In case of a normally distributed quantitative variable,instead of p and q, square of pooled Standard Deviation isused and p1-p2 in the denominator is replaced bydifference of mean between cases and controls.
Formula for calculating matched case control study isdifferent.
Example: Suppose a study is to be conducted to findout the association between obesity and glaucoma.Previous studies have shown that among obese peoplerisk of glaucoma is 3 times higher than that of nonobese people (OR=3.0) and prevalence of obesity inthe control group (normal population) is 10% and incases is 25%. (If OR is known and p2 is known, p1can be estimated from a formula). In order to estimatethe true Odds Ratio, by fixing Type I error at 5% andType II error at 20% (power = 80%), and taking 1 controlfor each case, the required sample size using aboveformula will be 62.72. Practically we need to take 32cases and 32 controls. The calculated sample size isalways the minimum sample size required.
Cohort studies are the other type of analytical studies,where point of selection of subjects in the study is prior toexposure to the factor(s) and occurrence of the event.
For example, if it is to be tested whether exposure tovolatile organic compounds (voc) increase the risk ofcorneal opacity; a cohort study can be conducted byrecruiting subjects before exposure to voc has startedand the exposed and unexposed subjects are followedup till a predetermined end point (development ofcorneal opacity) is reached or study is completed(censored). For such cohort studies, sample size iscalculated using following formula:
2
20101
10
11111
)(
)]()()([ )(
pp
ppZppZn m
ppm
−
−++∗−∗+=
−βα
Where, 101
++=∗mmppp
Please remember, n is the total number of subjects tobe recruited in the studyZα= Type I error (usually set at 5%), corresponding zscore is 1.96Zβ=Type II error (usually set at 20%), corresponding zscore is 0.84p0= probability of corneal opacity among the subjectsnot exposed to vocp1=probability of corneal opacity among the subjectsexposed to vocm=ratio of unexposed to exposed subjects
Sample size formula for paired cohort study is different
In this example, suppose we want to determine therelative risk of corneal opacity among subjects exposedto voc as against those not exposed. Let m=1, p0=0.2,p1=0.7, Zα=1.96, Zβ=0.84, p*=0.45
Then the required sample size will be: 45.03, hence45 subjects are to be recruited in this cohort study.
If the outcome variable is quantitative, p0 and p1 arereplaced by mean values in the denominator and theexpression p*(1-p*) are replaced by pooled SD, p0(1-p0)and p1(1-p1) are replaced by SD for unexposed group andSD for exposed group respectively.
Experimental studies: Experimental studies are similarto cohort studies except that in clinical trials exposure isunder control of the researcher. In cohort studies, theresearcher passively observes the exposure. In clinicaltrials, researcher creates exposure by giving interventions.All drug, vaccine trials, and non-pharmacologicalinterventions like health education etc. can be evaluatedusing a clinical trial design. The formula for calculatingsample size for such studies is:
2
2
)21()]21(2)11(1[]2/[
ppppppZZn
−−+−+= βα
You may note that the equation is very similar to that of acohort study sample size formula. This formula is usedwhen outcome variable is a qualitative variable and its valueis expressed as proportion (p). In this case p1 denotesoutcome in control group and p2 denotes outcome inexperimental/intervention group. Zα/2 is used when thesignificance is two tailed.
Example: Suppose the researcher wants to find out ifVitamin A intake (intervention) prevents night blindnessin school going children as compared to intake ofvitamin A rich food (control). The role of vitamin A intakewill be considered significant if occurrence of nightblindness in the intervention group is at least 50% lessthan that of the control group. If the incidence of nightblindness in the control group is 30%, it should be nomore than 15% in intervention group. After fixing alphaerror at 5% and power of study at 80%, , p1 30% andp2 15%, the number required to be recruited in eachgroup is N=117.6 thus by rounding off to the nearestinteger, 118 subjects are to be recruited in each group.
If the outcome variable is quantitative, the formula will be
2
22
)()(][
δσβα ZZn +=
Where σ is the pooled SD of the outcome variableand δ is the difference of the two means.
In the previous example, if impact of intervention ismeasured in terms of serum vitamin A level as outcome,the later formula should be used for sample size calculation.
A few checks that should be performed while calculatingthe sample size:
1. Outcome variable should be clearly defined.2. It should be measurable3. Check whether outcome variable is qualitative
(expressed as proportion) or quantitative (expressedas mean and Standard Deviation)
4. For quantitative variable, it is important to ensure thatthe variable follows normal distribution. For nonnormally distributed data, the above formulae do notapply
5. For descriptive studies and surveys, only Zα isrelevant, that is only type I error is taken intoconsideration.
6. For analytical and experimental studies, both Zα andZβ are required.
7. These formulae are based on the presumption thatsimple random sampling procedure will be adapted.
8. In case simple random sample is not achievable,alternative probability sampling techniques can be putto use, for example stratified random sampling andcluster sampling. In such cases the sample size
calculated by any of the above formula will require tobe corrected using a correction factor called designeffect.
9. In studies involving human beings, there is always achance of subjects withdrawing from the study, aphenomenon called attrition. This attrition should befactored into at the time of deciding the sample size.Suppose the required sample size for a cohort studyis 200 using simple random sampling method. But itis not feasible and cluster sampling technique is tobe used, and experts suggest that it requires a designeffect of 2.0, then the sample size will become, 200 x2=400. Now if you fear that 20% subjects may dropout or may be lost to follow up in course of the study,the effective sample size will become 400+20%=480.Hence 480 subjects should be recruited in this study.
10. There are other study designs and analysis methodsalso. As for example, survival analysis, Coxproportional hazard analysis, longitudinal dataanalysis etc. In such scenario different formulae areprescribed for calculating the sample size and it isbetter to be advised by a statistician with expertise insuch analysis.
Life for researchers have been made easier by thecomputing powers of the machines, which can handle largedata sets and carry out complex mathematical operationsin no time. Even sample size calculation has been madeeasy by computers. There are several software andfreeware available which compute the sample size for theresearcher. Most of these are menu operated and thereforeeasy to handle; but the researcher must know theparameters that are to be fed into the software to get theappropriate sample size calculation.
There are many online programs also which allow youto calculate the sample size and power of the study.Some of the freeware are given below:
1. Statcalc module of Epi- info, a softwaredistributed frr of cost by CDC, Atlanta. The mostrecent Version is Epi InfoTM 7.1.4. Can beaccessed at http://wwwn. cdc.gov/epiinfo/7/
2. PS: Power and Sample Size Calculation version3.1.2, 2014. Can be accessed at http://biostat.mc.vanderbilt.edu/wiki/Main/PowerSampleSize
3. G* Power: Statistical power analysis forWindows and Mac. Can be accessed at http://www.gpower.hhu.de/en.html
History of OphthalmologyHistory of OphthalmologyHistory of OphthalmologyHistory of OphthalmologyHistory of Ophthalmology
History Of Endeavour: Ophthalmology In IndiaSimantini Bhattacharya1
Abstract
This article presents the history of endeavour in ophthalmology in India, taking up some interesting and offbeat references. Anophthalmologist treating patients does not sound unusual but if a king, a prince or even a religious preacher is found indulged intreating ocular diseases, taking care of intricate ocular surgeries, its implication upon the mass becomes manifold. Grafting few ofsuch references the paper wants to ensure the need of a wide ranged awareness to contribute to the persistent glory of India in thisfield. Eye-care still needs to be propagated among the masses to substantiate the endeavour put forward by ophthalmologists,technologists and concerned persons.Keywords: medicine, endeavour, awareness, ophthalmology
Medical knowledge, especially Ophthalmology, in thispart of the globe has a fascinating antiquity. As an
‘object’ of medical concern, human eye, gained importanceat an early stage of civility. The Indian endeavour in the fieldof ophthalmology interestingly evolved from ancient Indianphilosophy. Unlike any other part of body, ‘Eye’ wasconsidered important. So as a field of study, Ophthalmology,where object of vision and object of knowledge coincideswith the mode of vision and mode of knowledge, developedunder special care. For centuries the mainstream knowledge-system of this sub-continent was being nourished under theconcept of ‘Darashana’. The term literally denotes the act ofseeing but its connotation goes far deeper and far wider. Itis not the mere corporeal seeing rather it is the perception ofthe truth critical behind the existence. So the act of ‘looking’at things not only through eyes but also through other sensoryorgans was taken quite seriously. And likewise, visual inabilitywas very often been metaphorized as the symbol ofignorance. Interestingly, the modern medicine is in tune withthe ancient metaphysical concept of ‘Darashana’; the all-pervasive seeing. The ‘clinical eye’1 encompasses a widerange of experience; it not only sees a disease but also itunderstands it, feels it, and even listens to it. With advancedtechnology it monitors the changes caused by it.
History of Indian ophthalmology is replete with vibrantactivities. Voluminous works on Susruta and his ‘Samhita’unanimously attribute him as the ‘Father of IndianOphthalmology’. Exercising ECCE in ca. 500 B.C.E2 is tilldate thought a rarity. But such cases are not beyondexpectation as at the day’s end we expect such ‘magic-healings’ if not expertise from physicians. Anophthalmologist treating patients does not sound unusualbut if a king, a prince or even a religious preacher is found
1Research Associate, IIEST, Shibpur, West Bengal, India.Corresponding Author : Simantini Bhattacharya, E-mail: [email protected] on : 18/10/2014, Accepted on : 30/12/2014Conflict of Interest : None, Financial Disclosure : None
indulged in treating ocular diseases, taking care of intricateocular surgeries, then the implication of it up on the massesbecomes manifold. Susruta, Charaka, Jivaka, Cakradattaet al were physicians by profession. They even reareddisciples. But Gautama Buddha was not a physician byprofession. Yet some literary texts call him ‘masterphysician’ who is expert in operating cataract3. Comparingthe Buddha with an ophthalmic surgeon is steeped withallegory. But if it were an actuality then its impact on themasses had been enormous. Equally interesting are theserecords which tell the story of princely figures who in spiteof not being physicians contributed significantly to theircontemporary ophthalmic endeavours; both treatment andawareness.
An 11th Century Tale: A reference of ca. 11th century healinghouse or ‘Atursalai’ of Tamil Nadu can be sited. Thishospital with 15 beds was constructed by the Chola rulerswithin the temple complex of Venkatesa Perumal. Apartfrom an outstanding team work of supervision underAsvatthama Bhattaraka, it used to keep a stock of medicinerequired for any given year3. This stock included ‘Sunetri’of which it earned specialization. ‘Sunetri’ was anophthalmic medicine especially effective for glaucoma.Other ocular problems also found a remedy in this. Sunetriattained specificity along with generality, the combinationwhich is intrinsic feature of modern medicine1. Medicinesfor cataract were also prepared with great distinction3. Thefact of keeping a good stock of an ophthalmic solutionalong with other medicines testifies their serious concern.This can be an inspiration for modern healing housesregarding the medicine-stock.
The Sultanate: Historical documents4 on medicinebelonging to sultanate period tell us of another royal figure,
CURRENT INDIAN EYE RESEARCH 83
Firuz Shah Tughlaq (1309-1388 C.E) as a physician. Hisspeciality was in bone-setting and ophthalmic treatment.He is credited in preparing an effective collyrium, knownas ‘Kuhl-e-Firuz Shahi’ from selected drugs and snakeskin4. It is pertinent to mention that collyrium had beenregarded as a mean to good vision from the time of Susruta.It was employed “to stimulate the growth of eye-lashes,brighten the lusture (lustre) of the eye-balls and clean thepupil.”5 Specific materials and metals were allotted tospecific kinds of collyrium; like - gold pot for sweet collyrium,silver and lapis lazuli for acidic, horn for salty, copper andiron for the astringent, bell-metal for bitter and the lot.5 FiruzShah further carried on the legacy. Under his dictation amedical treatise, Tibb-e-Firuz Shahi’, was composed but‘is not so far traceable’4. Another ruler, Muhammad QuliQutub Shah V of Golkonda Qutub Shahi had interests inocular studies. He ordered famous oculist of his timeShamsuddin Ali Husain al-Jurjani to translate the famous‘Tazkirat-ul-kahhalin’ or ‘Notebook of oculists’ of Ali bin ‘Isa4.The purpose behind these translations and compositionof medical treatises was to diffuse the knowledge amongthe masses. And the initiator wisely chose anophthalmologist to do the same for the sake of perfection.Such initiations were employed many a times due to itseffectiveness. It is pertinent here to refer that the firstBengali ophthalmologist6, Rai Bahadur Lal MadhabMookerjee also did a translation work in 1902. He translated‘A Manual of the Diseases of the Eye’ of C. Macnamara,into Bengali to help the native students in learning6.
Mughal story: Emperor Shah Jahan patronized Persianmen of medicine among who was the famous oculist HaikmAin-ul-Mulk Shiraji. He was appointed as the personalphysician to prince Dara. It is thought that the medical worknamed ‘Tibbe-e-Dara-Shikohi’ was his work though itacknowledged the prince for the purpose. According to itcataract was treated with medicine4.
Case-studies of Tanjore: The endeavour put forward bythe king Serfoji II (ruled 1798-1832 C.E) of ThanjavurMaratha dynasty is of signal importance in this field. Hehimself was an expert ophthalmic surgeon. The hospitalhe founded had British ophthalmologists. The endeavourhe put forward has at least two points of interests. First tomention is the ophthalmic records of patients which heordered to keep for further and future references.Researchers have found case studies of at least 44 patientswhose age limit varied from 5 to 60. Along with these 18paintings of patients were found7. These paintings can beaccounted as (probably) the first conscious effort, inophthalmology in India, to maintain a record that can helpin practical-study; the research and teaching. The frequentuse of complex medical terms7 like lens capsule, posteriorchamber, cornea etc and imaging diseases7 like springcatarrh, lenticular cataract, proptosis, leucomas etc hint at
the depth of study. Treatment was done applying bothoriental and occidental medicine. And second; in this eye-hospital patients were given cash reward after theirrecovery7. This is probably done to advertise their activitiesand for mass-awareness.
These references unmistakably present the fact that theseauthority shouldered with the renowned physicians inuplifting the status of respective medical works. Theirinitiation might have enriched ophthalmology but theirengagement surely aggravated the mass-awareness. Butthe problem of blindness and impaired vision is still loominglarge. Today’s India is approaching, in a very systematicway, to meet the target of “Vision 2020: the Right to Sight”through various schemes and programmes by NPCB andleading institutions of Ophthalmology. Following the past,the leaders of India, the emblematic personalities of Indiamust come forward to help NPCB and institutions ofOphthalmology. If such personalities are engaged asambassadors, as propagators in various awarenessprogrammes, in eye-donation propagations the result wouldyield better fruit. Manipulating the hero-worshiping, theawareness projects can bring qualitative change to thisfield. Such engagement worked effectively in the past andpromises are there to be worthy in present. History recordsthe endeavours but Present counts them.
Acknowledgement:
Professor Ajoy Kumar Ray, Director, IIEST, Shibpur for theguidance.
References:1. Das A. The Emergence of the Body: An essay in the
history of medical knowledge. (ed) Biswas A K. History,Science and Society in the Indian Context. The AsiaticSociety. Calcutta 2001. pp-293-302.
2. Kansupada KB, Sassani JW. Sushruta: the father ofIndian surgery and ophthalmology. Doc Ophthalmol1997; 93: 159-67.
3. Chakravarti R, Ray K. Healing and Healers Inscribed:Epigraphic Bearing on Healing-Houses in Early India.Institute of Development Studies Kolkata. OccasionalPaper 30. July 2011.
4. Verma R L. The Growth of Greco-Arabian Medicinein Medieval India. Indian J Hist Sci 1970; 5: 347-63.
5. Mukhopadhyaya G. Ancient Hindu Surgery, Vol-I.Cosmo Publishers. New Delhi 1994. pp- 324-325.
6. Bhattacharya A. Bangalir Bijnan-Bhabana o Sadhana.Dey’s Publishing. Kolkata 2006. pp-410.
7. Biswas J, Badrinath V, Badrinath SS. Ophthalmiccontributions of Raja Serfoji II (1798-1832). Indian JOphthalmol 2012; 60: 297-300.
History of OphthalmologyHistory of OphthalmologyHistory of OphthalmologyHistory of OphthalmologyHistory of OphthalmologyVolume 1, Issue 2, December 2014
CURRENT INDIAN EYE RESEARCH84
AUTHOR GUIDELINES
Manuscripts must be prepared in accordance with "Uniformrequirements for Manuscripts submitted to BiomedicalJournals" developed by the International Committee ofMedical Journal Editors (October 2004).The manuscripts will be reviewed for possible publicationwith the understanding that they are being submitted toone journal at a time and have not been published,simultaneously submitted, or already accepted forpublication elsewhere.Manuscripts will be sent for peer review.Articles accepted would be copy edited for grammar,punctuation, print style, and format.
Types of manuscripts and limits
• Review article: The limit of text is up to 3500 wordsexcluding about 70 references and abstract.
• Original article: The limit of the text is up to 3000 wordsexcluding about 50 references and structured abstractup to 250 words. This section will publish clinical,experimental and community reports.
• Research methodology: This includes educativearticles related to the conduct of research with wordcount up to 2000 and references up to 30.
• Case report: The limit is up to 1000 words excludingreferences and abstract with a maximum of 10references.
• Letter to the Editor: up to 500 words and 5 references.
• History of Ophthalmology: Up to 1000 words and 10references
Authorship credit should be based only on substantialcontributions1. Conception and design or acquisition of data or
analysis and interpretation of data;2. Drafting the article or revising it critically for important
intellectual content;3. Final approval of the version to be published.When you submit an article, the following items must beincluded.1. The covering letter2. Article file: Use doc files. Do not zip the files. Do not
incorporate images in the file. The first page will beTitle Page. All information which can reveal youridentity should be hereProvide the highest degree andinstitution of each author, Phone number and emailaddress of corresponding author. Also include
source(s) of support, acknowledgement, if themanuscript was presented earlier.
3. Images: Preferably black and white images. Colorimages will be considered if absolutely necessary.Image format jpeg/tiff is acceptable. Do not zip thefiles.
4. Legends: Legends for the figures/images should beincluded at the end of the article file.
The language should be American English.The text should be divided into sections with the headings:Abstract, Key-words, Introduction, Material and Methods,Results, Discussion, References, Tables and Figurelegends. Use double spacing throughout. Number pagesconsecutively, beginning with the title page.
The contributors’ form (available at http://ophthalmicresearch.in/journals.html) has to be submitted withthe signature of the corresponding author at the timeof submission via e-mail as a scanned image.
Clearance from ethics committee should be mentioned inmethod section. When informed consent has beenobtained, it should be indicated in the article.
References
References should be numbered consecutively in the orderin which they are first mentioned in the text (not inalphabetic order). Identify references in text, tables, andlegends by Arabic numerals in superscript before thepunctuation marks. The titles of journals should beabbreviated according to the style used in Index Medicus.Use complete name of the journal for non-indexed journals.Reference style:Journal article: Vinekar A, Dogra MR, Sangtam T, NarangA, Gupta A. Retinopathy of prematurity in Asian Indianbabies weighing greater than 1250 grams at birth: Ten yeardata from a tertiary care center in a developing country.Indian J Ophthalmol 2007;55:331-6.Incase of more than six authors, list the first threecontributors followed by et al.Chapter in a book: Phillips SJ, Whisnant JP. Hypertensionand stroke. In: Laragh JH, Brenner BM, editors.Hypertension: pathophysiology, diagnosis, andmanagement. 2nd ed. New York: Raven Press; 1995. pp.465-473.
Processing fee : NilArticle to be sent by email only to: