28
Delivering pain neuroscience education, manual therapy, and exercises—a case example Andrew Somers, PT, DPT, OCS
Delivering pain neuroscience education, manual therapy, and
exercises—a case exampleAndrew Somers, PT, DPT, OCS

Background• Graduate from OUHSC in
2015
• Finished MTC through EIM in January 2017
• OCS as of 2017
• No advanced certifications in pain sciences
• Work for Physical Therapy Central in Elk City
2

Meet our mock patient• 22 y/o male with recurrent LBP, R foot
pain (unclear connection)
• S/I: 0-4-8/10, intermittent/unpredictable/sec-min to decrease
• N: unknown (for now)
• S: acute on chronic
• S: staying the same
• Agg: running, walking, Ham str, sitting long periods
• Ease: avoidance
• Daily routine: PT tech, student
3

Lower quarter screen• P1: ache in back, burning/
ache in foot
• Function screens, dermatomes, myotomes, reflexes, all other AROM: ✔
• AROM: ext inc P1 in back, no centralize
• Slump + in foot, SLR -
• Accessory: foot pain with lower L spine PAs
Flynn, Cleland & Whitman, Users’ Guide to Musculoskeletal Examination, 20084

Diagnosis
“Patient exhibits a clinical presentation consistent with R mechanical LBP with mechanically
modifiable, peripheral neurogenic/referred pain resulting in an inability to run without increased
pain and dysfunction.”
Series of articles by Smart et al., Manual Therapy, 2012, vol. 175

Treatment
Advice & Education
Adapted from @AdamMeakins, Physio Treatment Pyramid
General movements
Resistance Exercise
Manual Therapy
Modalities
6

Pain as output from brain
Butler & Moseley, Explain Pain, 20137

Why so threatening?
Butler & Moseley, Explain Pain, 20138

DethreateningMechanical LBP with neuropathic P
DirPrefManip/Mob
Resistance
Str/PostNeuroD
9

How does it work?
Supraspinal
Mechanical
Spinal
10

Cortical remapping?https://www.youtube.com/watch?v=3QVAY5stO3U
11Moseley & Flor, Neurorehabil and Neural Repair, 2012

What about surgery?
Forced rest?
Build new neurotags
Mechanical
BiomechanicsCorrects damage
(Supra)spinal
Interneuron Belief
Cortical maps
12

Adaptation
13

Common patient questions“How do we know when damage occurs?”
14

Common patient questions• Priming the expectation of pain
modulates heat sensitivity to repeated stimulus1
• Telling patients clockwise ultrasound is more effective for pain improves SLR ability2
• Showing patients excised disc material improves leg pain, back pain, limb weakness, paraesthesia, and reduces pain med usage3
“So it’s all in my head?”
3) Tait & Levy, J Neurol Neurosurg Psychiatry, 2009 2) Louw et al., South African Journal of Physiotherapy, 2016
1) Dogancil et al., European Journal of Pain, 2012
15

Keys to the process
• Empathy fosters therapeutic alliance
• Therapeutic alliance improves outcomes
• Empathy can be trained
1) Empathy
Lakke & Meerman, J Compassionate Health Care, 2016 Kelm et al., BMC Medical Education, 2014
16

Keys to the process
• Imaging
• “Fix me”
• Pain ≠ damage
• Pain ≠ disability
2) Deconstruct faulty beliefs
1. Must be dissatisfied with current perceptions of pain
2. New explanation must be intelligible
3. New explanation must be plausible/beneficial
4. Must be shared and confirmed by direct environment
5. Interaction with therapist is necessaryBlickenstaff & Pearson, Physiother Theory Pract, 2016
Nijs and Meejus, conference, 2015 17

Keys to the process• Active coping
strategies
• Limiting catastrophizing & fear-avoidant behaviors
• Deconstructing habits that lead to increased pain
3) Focus on behaviors
18
Paroli et al., Pain Medicine, 2017 Fersum et al., European Journal of Pain, 2012
George & Sandra, J Orthop Sports Phys Ther, 2011
http://specialneedsparenting.net/wp-content/uploads/2016/05/doubt-and-fear-ahead.jpg

Keys to the process
• Create a caring atmosphere—make it FUN
• Do not settle for avoidance
• Limit words that harm
4) Prime the environment
19Bedell et al., Arch Intern Med, 2004
https://pastortravisdsmith.files.wordpress.com/2014/02/words_can_hurt_or_heal_small.jpg

Words that harm
Bedell et al., Arch Intern Med, 200420
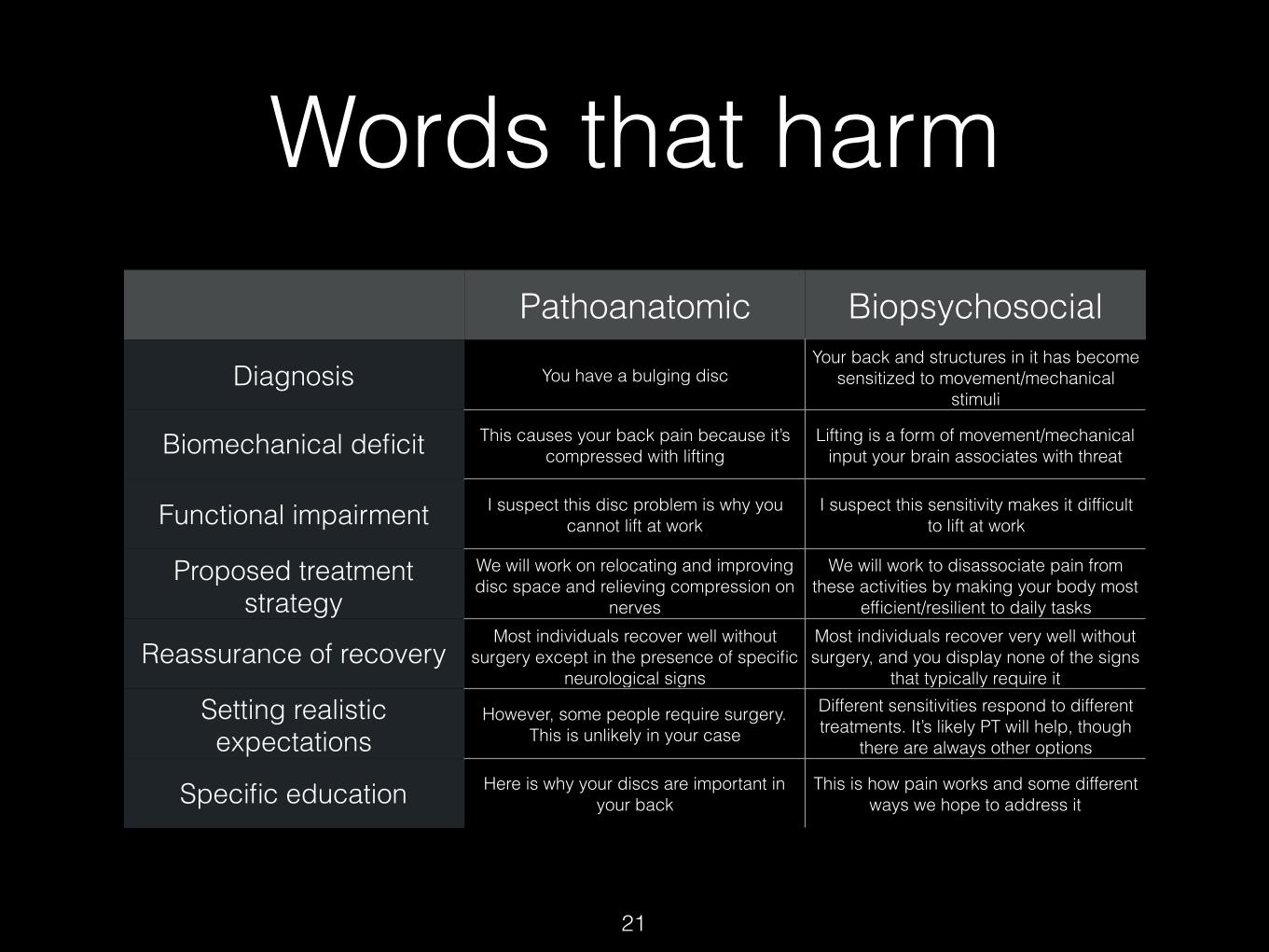
Words that harmPathoanatomic Biopsychosocial
Diagnosis You have a bulging discYour back and structures in it has become
sensitized to movement/mechanical stimuli
Biomechanical deficit This causes your back pain because it’s compressed with lifting
Lifting is a form of movement/mechanical input your brain associates with threat
Functional impairment I suspect this disc problem is why you cannot lift at work
I suspect this sensitivity makes it difficult to lift at work
Proposed treatment strategy
We will work on relocating and improving disc space and relieving compression on
nerves
We will work to disassociate pain from these activities by making your body most
efficient/resilient to daily tasks
Reassurance of recoveryMost individuals recover well without
surgery except in the presence of specific neurological signs
Most individuals recover very well without surgery, and you display none of the signs
that typically require it
Setting realistic expectations
However, some people require surgery. This is unlikely in your case
Different sensitivities respond to different treatments. It’s likely PT will help, though
there are always other options
Specific education Here is why your discs are important in your back
This is how pain works and some different ways we hope to address it
21
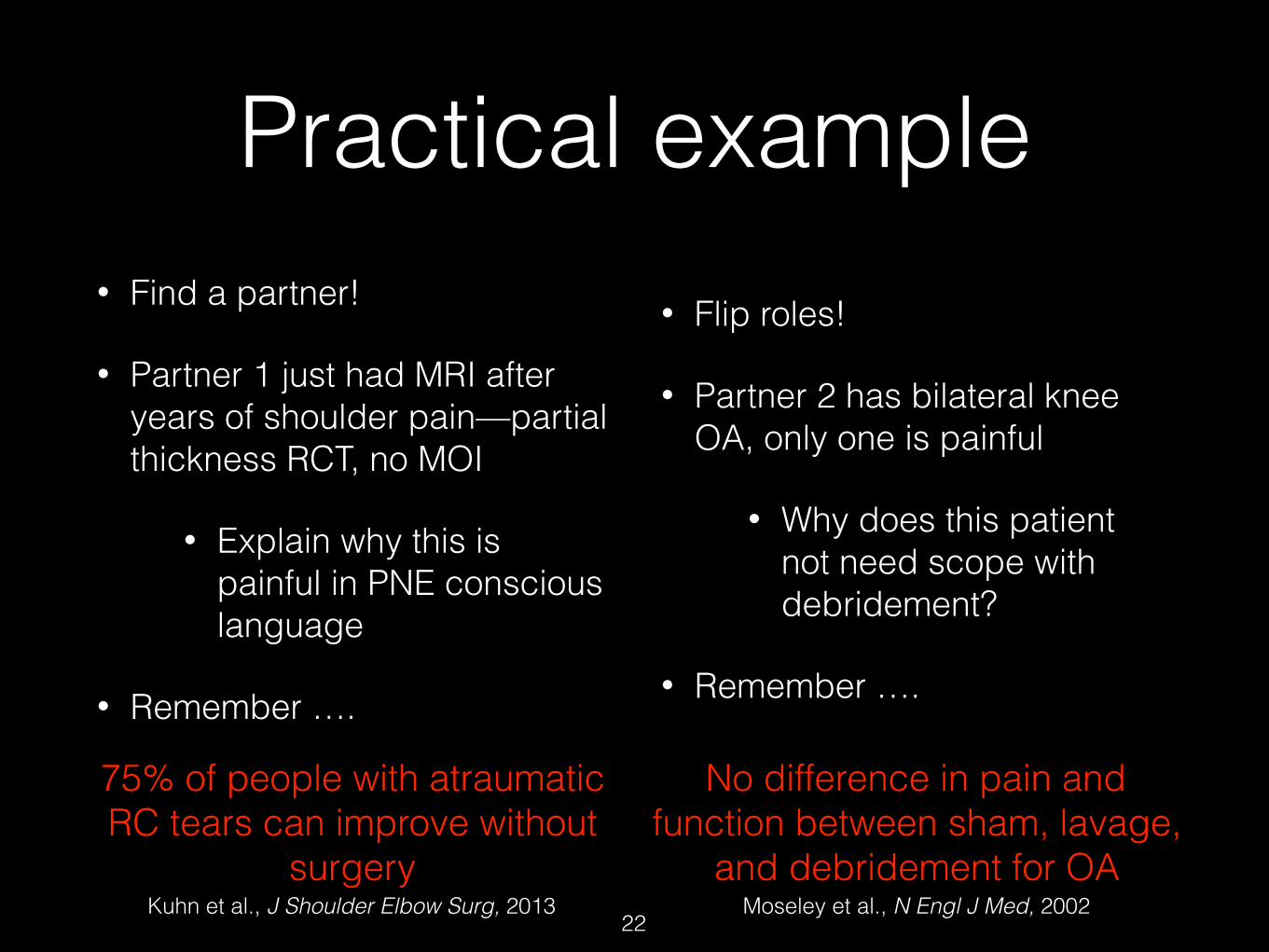
Practical example• Find a partner!
• Partner 1 just had MRI after years of shoulder pain—partial thickness RCT, no MOI
• Explain why this is painful in PNE conscious language
• Remember ….
• Flip roles!
• Partner 2 has bilateral knee OA, only one is painful
• Why does this patient not need scope with debridement?
• Remember ….
75% of people with atraumatic RC tears can improve without
surgery22
No difference in pain and function between sham, lavage,
and debridement for OAMoseley et al., N Engl J Med, 2002 Kuhn et al., J Shoulder Elbow Surg, 2013

What about our patient?
1) advice and education
R mechanical LBP with mechanically modifiable, peripheral neurogenic/referred pain
2) progressive loading
3) manipulation > mobilization
4) neurodynamic techniques Adapted from @AdamMeakins
23

10-20x, 2-3x/d
Slump stretching
Cleland, Manual Therapy, 2006
Heavy back squats
5x5, 1-2x/wSteele et al., Spine J, 2015
Smith et al., BMC MSK Disord, 2014; Louw et al., New Zealand J of Physio, 201524

Outcomes
• Able to complete all activities (running, etc) without increased pain/dysfunction
• Slump stretching reduced foot and back pain enough to complete progressive heavy lifting
• No back pain after 3 weeks of HEP only
25

Key resources• Pain Fundamentals (Greg Lehman): https://
static1.squarespace.com/static/57260f1fd51cd4d1168668ab/t/5734a441b6aa60fc5fe5ef7a/1463067714566/PainScienceLehmanWorkbook.pdf
• Treatment Fundamentals (Greg Lehman): https://static1.squarespace.com/static/57260f1fd51cd4d1168668ab/t/5734a47dcf80a15b6c04d4e9/1463067774474/PainScienceLehmanTreatment.pdf
• Pain Recovery Strategies (Greg Lehman): https://static1.squarespace.com/static/57260f1fd51cd4d1168668ab/t/590dca541e5b6c8e16e411cf/1494076002702/recovery+strategies+pain+guidebook+2017.pdf
26

Key resources• Explain Pain (Supercharged): Butler & Moseley
• The Graded Motor Imagery Handbook: NOIgroup
• Pain Reframed podcast (Jeff Moore, Tim Flynn): https://www.ispinstitute.com/pain-reframed-podcast/
• Pain Science and Sensibility podcast (Cory Blickenstaff, Sandy Hilton): http://ptpodcast.com/podcasts/pain-science-and-sensibility/
27

Key resources
• Watch the masters in action!
• Moseley: https://www.youtube.com/watch?v=gwd-wLdIHjs
• Butler: https://www.youtube.com/watch?v=4ABAS3tkkuE
• Basically any podcast with Greg Lehman
28

















