52
Post-travel case scenarios When to refer, when to panic and when to reassure MALARIA!! DENGUE!! Diarrhoea!!

Post-travel case scenarios When to refer, when to panic and when to reassure
MALARIA!!
DENGUE!!
Diarrhoea!!
ObjectivesObjectives
Develop a framework for triage of travelers Develop a framework for triage of travelers presenting with medical complaints. presenting with medical complaints. Recognize the most common post travel emergency Recognize the most common post travel emergency scenarios. scenarios. Recognize common post travel health scenarios Recognize common post travel health scenarios requiring reassurance, referral or both.requiring reassurance, referral or both.Name the symptoms of malaria, dengue fever, Name the symptoms of malaria, dengue fever, typhoid fever and persistent travellertyphoid fever and persistent traveller’’s diarrhoea.s diarrhoea.Have funHave fun
Practice questionPractice question
In the five minutes In the five minutes following this scene, the following this scene, the monkey:monkey:
A.A.
Bit meBit me
B.B.
Crawled down my shirtCrawled down my shirt
C.C.
Pick pocketed mePick pocketed me
D.D.
Threw a fruit at meThrew a fruit at me
E.E.
All of the aboveAll of the above
Case #1Case #1A 44 year old Ghananese woman presents with sudden A 44 year old Ghananese woman presents with sudden onset fever (38.9onset fever (38.9ººC, measured). C, measured). She returned to Winnipeg from Ghana 12 days prior after She returned to Winnipeg from Ghana 12 days prior after visiting her mother and brothers in Ghana, where she also visiting her mother and brothers in Ghana, where she also visited numerous other subvisited numerous other sub‐‐Saharan African countries Saharan African countries (Nigeria, Angola, Namibia and South Africa).(Nigeria, Angola, Namibia and South Africa).In Ghana, she stayed with her family near the town of In Ghana, she stayed with her family near the town of Tamale. Tamale. For her other destinations, she was part of an organized For her other destinations, she was part of an organized tour. tour. She did not seek preShe did not seek pre‐‐travel advice and is unsure of her travel advice and is unsure of her vaccination status. She reports multiple episodes of vaccination status. She reports multiple episodes of malaria during her childhood but never recalls it being malaria during her childhood but never recalls it being ““quite this badquite this bad””..
What is the best immediate course of What is the best immediate course of action?action?
A.A.
Start quinine and Start quinine and doxycycline on the phone.doxycycline on the phone.
B.B.
Reassure and refer to GP as Reassure and refer to GP as required.required.
C.C.
Refer to local travel clinic.Refer to local travel clinic.
D.D.
Refer to hospital emergency Refer to hospital emergency department.department.
E.E.
None of the aboveNone of the above
What are the top three diagnoses?What are the top three diagnoses?
A.A.
Malaria, Malaria, MalariaMalaria, Malaria, Malaria
B.B.
Malaria, Dengue, Malaria, Dengue, unknown cause or not unknown cause or not
travel related.travel related.
C.C.
Typhoid, Malaria, DengueTyphoid, Malaria, Dengue
D.D.
Malaria, unknown or not Malaria, unknown or not travel related, tick typhustravel related, tick typhus
Fever in SubFever in Sub‐‐Saharan AfricaSaharan Africa
Malaria accounts for ~2/3 of all systemic febrile illnesses in Malaria accounts for ~2/3 of all systemic febrile illnesses in returned travellers from subreturned travellers from sub‐‐Saharan Africa.Saharan Africa.••
By far the worst region for malariaBy far the worst region for malaria
••
Major risk factors are VFRs, no prophylaxis, exposure to Major risk factors are VFRs, no prophylaxis, exposure to
rural areas, during nightrural areas, during night‐‐time hours.time hours.Almost 3/10 cases of fever in travellers from SSA are Almost 3/10 cases of fever in travellers from SSA are undiagnosed or cosmopolitan infections.undiagnosed or cosmopolitan infections.1/20 cases of fever in travellers from this area are due to 1/20 cases of fever in travellers from this area are due to rickettsial infection, almost all rickettsial infection, almost all R. africaeR. africae••
Almost exclusive to Southern Africa region (South Africa, Almost exclusive to Southern Africa region (South Africa,
Botswana, Namibia, Swaziland, Lesotho and Zimbabwe).Botswana, Namibia, Swaziland, Lesotho and Zimbabwe).••
Physical exam should point this diagnosis. Physical exam should point this diagnosis.
N Engl J Med. 2006 Jan 12;354(2):119‐30

Cosmopolitan and other causes of feverCosmopolitan and other causes of fever
Dengue and Typhoid are rare in SSA Dengue and Typhoid are rare in SSA –– account for account for less than 1% of SFIless than 1% of SFI’’s.s.Mononucleosis accounts for ~1% of fevers in SSA Mononucleosis accounts for ~1% of fevers in SSA travellers.travellers.Cosmopolitan or unknown causes account for Cosmopolitan or unknown causes account for ~40% of cases of in cases of FRT (overall).~40% of cases of in cases of FRT (overall).••
~15% respiratory~15% respiratory
••
~5% Urinary tract~5% Urinary tract••
~20% unknown~20% unknown
••
~5% other~5% other
N Engl J Med. 2006 354(2):119‐30 Clin Infect Dis. 2007 44(12):1560‐8
What initial lab investigations are What initial lab investigations are essential?essential?
A.A.
Malaria smearsMalaria smears
B.B.
Blood culturesBlood cultures
C.C.
Rickettsial and Rickettsial and Arboviral serologyArboviral serology
D.D.
EBV serologyEBV serology
E.E.
A and BA and B
F.F.
All of the aboveAll of the above

Investigations in hospitalInvestigations in hospital
Three malaria smears should be ordered, ~12 Three malaria smears should be ordered, ~12 hours apart, preferably when the patient is hours apart, preferably when the patient is febrile.febrile.••
Alternatives include malaria antigen detection and Alternatives include malaria antigen detection and
PCR. Neither are easily available.PCR. Neither are easily available.Blood cultures useful to diagnose typhoid and Blood cultures useful to diagnose typhoid and many cosmopolitan infections.many cosmopolitan infections.Rickettsia and arboviral serology may be useful, Rickettsia and arboviral serology may be useful, but can be defered unless clinical findings suggest but can be defered unless clinical findings suggest these.these.EBV unlikely.EBV unlikely.
Case #2Case #2
A 24 year old female returns from her July A 24 year old female returns from her July honeymoon vacation in Italy where she stayed honeymoon vacation in Italy where she stayed only in four and five star hotels and traveled by only in four and five star hotels and traveled by train. train. Their honeymoon started in Rome with travel Their honeymoon started in Rome with travel south to Naples and north along the Adriatic Sea south to Naples and north along the Adriatic Sea to Venice. to Venice. They returned to Winnipeg 10 days ago. She now They returned to Winnipeg 10 days ago. She now presents with subjective fever, malaise and joint presents with subjective fever, malaise and joint pain. She reports a mild headache and feels tired. pain. She reports a mild headache and feels tired. She has no neck stiffness, nausea or vomiting.She has no neck stiffness, nausea or vomiting.
What is the best course of action?What is the best course of action?
A.A.
Send to ER for assessment.Send to ER for assessment.
B.B.
Send to family doctor as required.Send to family doctor as required.
C.C.
Send to Travel and tropical medicine at next Send to Travel and tropical medicine at next available appointment and suggest she go to available appointment and suggest she go to the hospital if symptoms worsen.the hospital if symptoms worsen.
D.D.
Reassure and tell her it will go away.Reassure and tell her it will go away.
E.E.
Offer to bring her some chicken soup.Offer to bring her some chicken soup.
Huh? What about the fever?Huh? What about the fever?
Neither of the Neither of the ““bad boysbad boys”” malaria nor typhoid malaria nor typhoid occur in Italy.occur in Italy.
Many cosmopolitan, local and travel related Many cosmopolitan, local and travel related illnesses can cause fever, and many illnesses can cause fever, and many ““feversfevers””are not real.are not real.
Need for urgent care no different than a Need for urgent care no different than a ““westernerwesterner”” with same symptoms.with same symptoms.
Cannot guarantee benign cause!Cannot guarantee benign cause!
Approximately what percentage of people who Approximately what percentage of people who ““feel like they have a feverfeel like they have a fever””
actually do?actually do?
A.A.
<10%<10%
B.B.
10 10 ––
20%20%
C.C.
20 20 ––
30%30%
D.D.
30 30 ––
40%40%
E.E.
40 40 ––
50%50%
Lancet 350:781.
What is the most likely diagnosis?What is the most likely diagnosis?
A.A.
MalariaMalaria
B.B.
DengueDengue
C.C.
InfluenzaInfluenza
D.D.
Travel acquired mononucleosisTravel acquired mononucleosis
E.E.
None of the aboveNone of the above

What What arboviralarboviral
diseases circulate in Italy?diseases circulate in Italy?
A.A.
ToscanaToscanaB.B.
ChikungunyaChikungunyaC.C.
West NileWest NileD.D.
RickettsiaRickettsia
conoriiconoriiE.E.
DengueDengueF.F.
A and BA and BG.G.
A, B and CA, B and CH.H.
All of the aboveAll of the above
Parassitologia. 2008 50:109‐11

Case #3Case #3A 26 year old female calls the THN A 26 year old female calls the THN because of an episode of diarrhoea because of an episode of diarrhoea which occurred while on her fantasy which occurred while on her fantasy spring break holiday in the Hedonism II spring break holiday in the Hedonism II Resort in Jamaica.Resort in Jamaica.She experienced severe diarrhoea, She experienced severe diarrhoea, abdominal cramping and vomiting for abdominal cramping and vomiting for two days starting three days into her two days starting three days into her holiday. holiday. She is upset that she couldnShe is upset that she couldn’’t party it up t party it up with her friends, but is now well and has with her friends, but is now well and has no symptoms at all. She wants to know no symptoms at all. She wants to know what she should do now.what she should do now.

What course of action is most appropriate?What course of action is most appropriate?
A.A.
Refer her to the travel health clinic at the next Refer her to the travel health clinic at the next available appointment.available appointment.
B.B.
Tell her to rush to emergency for assessmentTell her to rush to emergency for assessmentC.C.
Reassure her that travellerReassure her that traveller’’s diarrhoea is common s diarrhoea is common and usually resolves as hers has, and tell her to call and usually resolves as hers has, and tell her to call back or talk to her doctor if she has any further back or talk to her doctor if she has any further
concerns.concerns.D.D.
Have her make an appointment with her doctorHave her make an appointment with her doctorE.E.
Sigh, roll back your eyes and hang up after Sigh, roll back your eyes and hang up after suggesting an STI work up.suggesting an STI work up.

What proportion of travellerWhat proportion of traveller’’s diarrhoea episodes s diarrhoea episodes spontaneously resolve with no further need for spontaneously resolve with no further need for
assessment?assessment?
A.A.
>90%>90%
B.B.
~75%~75%
C.C.
~50%~50%
D.D.
~25%~25%
E.E.
<10%<10%
Delhi Belly EpidemiologyDelhi Belly Epidemiology
Most episodes of travellerMost episodes of traveller’’s diarrhoea s diarrhoea are self resolving.are self resolving.
Between 8% and 50% of travellers Between 8% and 50% of travellers develop diarrhoea; depending on the develop diarrhoea; depending on the country visited. country visited.
>90% of cases occur within two weeks of >90% of cases occur within two weeks of arrival.arrival.
Adv Ther. 2006 Jul‐Aug;23(4):519‐27
Outcomes of TDOutcomes of TD
About 50% of cases are resolved by 48h.About 50% of cases are resolved by 48h.
4 to 10% of individuals may develop 4 to 10% of individuals may develop persistent undiagnosed symptoms.persistent undiagnosed symptoms.
Post infectious IBS?Post infectious IBS?
••
TravellerTraveller’’s diarrhoea can unmask IBD, s diarrhoea can unmask IBD, celiac disease, autoceliac disease, auto‐‐immune diseases immune diseases (<1%).(<1%).
Clinical Infectious Diseases 2005;41:S536–S540
What modalities exist to prevent travellerWhat modalities exist to prevent traveller’’s s diarrhoea?diarrhoea?
A.A.
Only eating food from a Only eating food from a
renowned 5 star resort.renowned 5 star resort.
B.B.
Avoid eating Avoid eating
raw/undercooked food, raw/undercooked food,
including fruit without peels including fruit without peels
and raw vegetables.and raw vegetables.
C.C.
Drinking alcoholic Drinking alcoholic
beverages.beverages.
D.D.
An effective vaccine.An effective vaccine.
E.E.
All of the above.All of the above.
TD preventionTD prevention
Wide range of incidence, not related to quality of resort.Wide range of incidence, not related to quality of resort.••
High class resort can be associated with high rates.High class resort can be associated with high rates.
••
++ food handling, susceptible population, poor hand ++ food handling, susceptible population, poor hand
hygiene.hygiene.Behavioural methods Behavioural methods ““Boil it, Cook it, Peel it or Forget itBoil it, Cook it, Peel it or Forget it””have been shown effective.have been shown effective.Alcohol at levels that humans can tolerate does not kill Alcohol at levels that humans can tolerate does not kill bacteria, much less cysts and viruses.bacteria, much less cysts and viruses.••
Bottled alcohol (e.g. beer & wine) are Bottled alcohol (e.g. beer & wine) are ““cleanclean””..
The available vaccine (The available vaccine (DukoralDukoralTMTM) is marginally effective for ) is marginally effective for only one major cause of TD and conservatively may prevent 1 only one major cause of TD and conservatively may prevent 1 –– 7% of cases of TD overall.7% of cases of TD overall.
Lancet Infect Dis 2006; 6:361–73Adv Ther. 2006 4:519‐27Int. J Epidemiol. 1985 14 169‐172

Case #4Case #4
A 24 year old male originally from Bangladesh now A 24 year old male originally from Bangladesh now living in Winnipeg returns from Bangladesh after living in Winnipeg returns from Bangladesh after visiting friends and relatives.visiting friends and relatives.One week after returning, he feels unwell with One week after returning, he feels unwell with rigors, fever (measured at 38.5rigors, fever (measured at 38.5ººC) and significant C) and significant malaise. malaise. He reports He reports myalgiasmyalgias, weakness, fatigue and severe , weakness, fatigue and severe headache. He reports significant insomnia.headache. He reports significant insomnia.While in Bangladesh, he lived with his relatives and While in Bangladesh, he lived with his relatives and ate, drank and lived as they did. He had not sought ate, drank and lived as they did. He had not sought any preany pre‐‐travel advice.travel advice.

What is the most appropriate course of What is the most appropriate course of action?action?
A.A. Start ciprofloxacin on the phone.Start ciprofloxacin on the phone.B.B. Reassure and refer to GP as Reassure and refer to GP as
requiredrequiredC.C. Refer to local travel clinicRefer to local travel clinicD.D. Refer to hospital emergency Refer to hospital emergency
departmentdepartmentE.E. None of the aboveNone of the above
True fever is an emergency!True fever is an emergency!
Malaria smears, blood Malaria smears, blood cultures and evaluation cultures and evaluation is essential!is essential!
Blood counts, platelet Blood counts, platelet counts, renal and liver counts, renal and liver function can help make function can help make a diagnosis and guide a diagnosis and guide therapy.therapy.
Excluding Excluding ““unknown causeunknown cause””, what are the , what are the top three diagnoses?top three diagnoses?
A.A.
Malaria, Malaria, MalariaMalaria, Malaria, Malaria
B.B.
Dengue, Malaria, Scrub typhusDengue, Malaria, Scrub typhus
C.C.
Typhoid, Dengue, MalariaTyphoid, Dengue, Malaria
D.D.
Typhoid, Mononucleosis, MalariaTyphoid, Mononucleosis, Malaria
E.E.
Influenza, Influenza, ChikungunyaChikungunya, Dengue, Dengue
WhatWhat’’s in Bangladesh?s in Bangladesh?
Typhoid, Dengue and Malaria are almost neck Typhoid, Dengue and Malaria are almost neck and neck in this area.and neck in this area.••
Each accounts for ~14% of Each accounts for ~14% of SFIsSFIs
in returned travellers.in returned travellers.
All three present with an undifferentiated fever.All three present with an undifferentiated fever.
Being a VFR puts this man at greater risk of all Being a VFR puts this man at greater risk of all three.three.
All three are preventable with education, All three are preventable with education, vaccination and/or prophylaxis.vaccination and/or prophylaxis.
N Engl
J Med. 2006 354(2):119‐30

First rule out the deadlyFirst rule out the deadly
Blood cultures and malaria smears are Blood cultures and malaria smears are essential to rule out the truly deadly.essential to rule out the truly deadly.
In the absence of haemorrhage or clotting In the absence of haemorrhage or clotting dysfunctiondysfunction’’ dengue serology is optionaldengue serology is optional••
May help predict future risk of DHFMay help predict future risk of DHF
••
Consider if negative cultures and malaria smears.Consider if negative cultures and malaria smears.
Bangladesh is in the Bangladesh is in the tsutsugamushitsutsugamushi belt.belt.••
Disease is uncommon, clinical presentation should Disease is uncommon, clinical presentation should
point to diagnosis. point to diagnosis.
Assuming he is well enough for outpatient treatment, what Assuming he is well enough for outpatient treatment, what
antibiotic should be prescribed if a blood culture is reported aantibiotic should be prescribed if a blood culture is reported as s
““Salmonella Salmonella entericaenterica
subsp. subsp. entericaenterica
ser. ser. TyphiTyphi””??
A.A.
Ciprofloxacin 500mg BIDCiprofloxacin 500mg BID
B.B.
AzithromycinAzithromycin
500mg OD500mg OD
C.C.
TrimethoprimTrimethoprim‐‐ sulfamethoxazolesulfamethoxazole
160:800mg BID160:800mg BID
D.D.
LevofloxacinLevofloxacin
500mg OD500mg OD
E.E.
ChloramphenicolChloramphenicol
500mg 500mg QIDQID
Treatment of Typhoid FeverTreatment of Typhoid Fever
QuinolonesQuinolones, , azithromycinazithromycin, TMP/SMX, , TMP/SMX, cefiximecefiximeand and chloramphenicolchloramphenicol are all indicated for are all indicated for Typhoid...Typhoid...
But...resistance to But...resistance to fluoroquinolonesfluoroquinolones, and , and TMP/SMX is very high (70TMP/SMX is very high (70‐‐100%) in South 100%) in South Asia.Asia.
ChloramphenicolChloramphenicol is more toxic, less effective is more toxic, less effective and hard to get.and hard to get.
J Infect Chemother. 2006 Dec;12(6):402‐4Clinical Infectious Diseases 2000;31:1134–1138Antimicrob. Agents Chem., 1999;43:1441‐4.
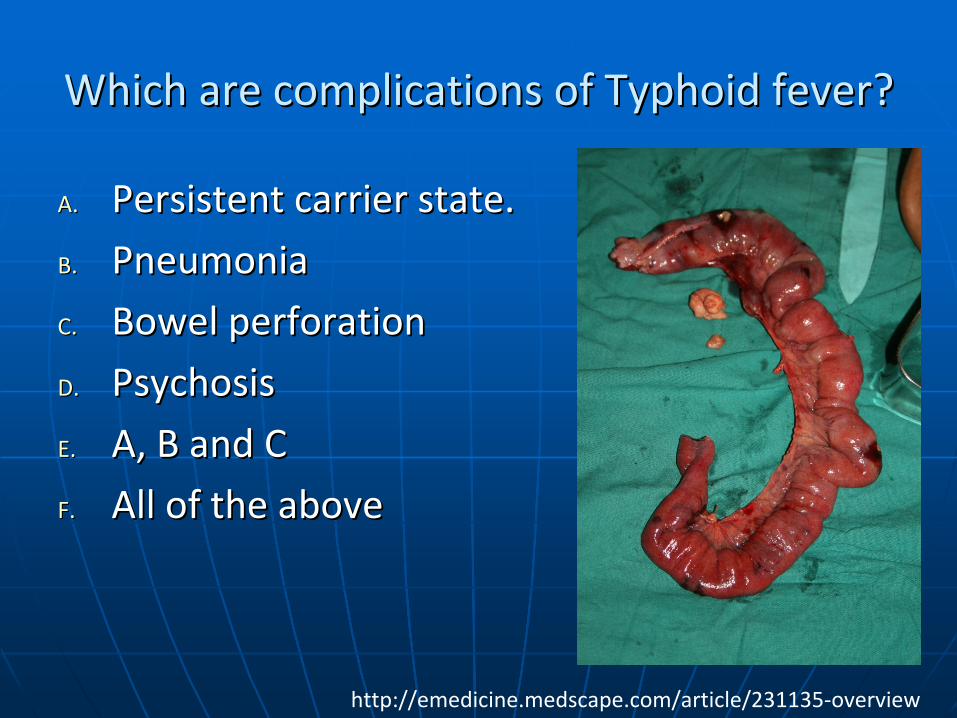
Which are complications of Typhoid fever?Which are complications of Typhoid fever?
A.A.
Persistent carrier state.Persistent carrier state.
B.B.
PneumoniaPneumonia
C.C.
Bowel perforationBowel perforation
D.D.
PsychosisPsychosis
E.E.
A, B and CA, B and C
F.F.
All of the aboveAll of the above
http://emedicine.medscape.com/article/231135‐overview

Case #5Case #5A 35 year old woman calls the THN to tell her that 4 days ago, A 35 year old woman calls the THN to tell her that 4 days ago, during the last part of her Kenya holiday she was touring the during the last part of her Kenya holiday she was touring the Nairobi Arboretum and was attacked and bitten on the back Nairobi Arboretum and was attacked and bitten on the back of the leg by of the leg by ““a seriously nuta seriously nut‐‐bag monkeybag monkey””. . She had received rabies preShe had received rabies pre‐‐exposure prophylaxis. She exposure prophylaxis. She consulted the back of her vaccine record and did the consulted the back of her vaccine record and did the following:following:
1.1.
Washed the wound with soap and water, encouraged Washed the wound with soap and water, encouraged
bleeding and washed the wound with bleeding and washed the wound with povidonepovidone
and alcohol.and alcohol.
2.2.
Went to the Nairobi hospital (a highWent to the Nairobi hospital (a high‐‐end private westernend private western‐‐type type
hospital) that day where she received amoxicillinhospital) that day where she received amoxicillin‐‐clavulanateclavulanate
and two doses of and two doses of ImovaxImovax
(HDCV) vaccine (day 0 and day 3). (HDCV) vaccine (day 0 and day 3).
3.3.
The attending physician examined the wound on the morning The attending physician examined the wound on the morning
of day 3 (on her way to the airport) and decided there was no of day 3 (on her way to the airport) and decided there was no
infection, and that sutures could be placed to achieve closure infection, and that sutures could be placed to achieve closure
with low risk of infection. The antibiotic was prescribed for 10with low risk of infection. The antibiotic was prescribed for 10
days (she is still taking it).days (she is still taking it).

The biteThe bite……

What is the most appropriate course of What is the most appropriate course of action?action?
A.A.
Congratulate her on the appropriate management Congratulate her on the appropriate management of a potential exposure to rabies and tell her she of a potential exposure to rabies and tell her she
needs no followneeds no follow‐‐up.up.B.B.
Tell her to come in to the clinic today Tell her to come in to the clinic today ““just to be just to be safesafe””..
C.C.
Arrange for her to get two shots of appropriate Arrange for her to get two shots of appropriate rabies vaccine at the local ER.rabies vaccine at the local ER.
D.D.
Arrange for her to get rabies immune globulin and Arrange for her to get rabies immune globulin and five appropriate rabies vaccines (day 0, 3, 7, 14 and five appropriate rabies vaccines (day 0, 3, 7, 14 and 28), just to be safe.28), just to be safe.
E.E.
Hang up.Hang up.

What pathogens can be theoretically What pathogens can be theoretically acquired from directly from monkeys?acquired from directly from monkeys?
A.A.
RabiesRabiesB.B.
CHVCHV‐‐1 (1 (CercopithecineCercopithecine
Herpes Herpes Virus)Virus)
C.C.
SV40 SV40 D.D.
PoliovirusPoliovirusE.E.
TapewormsTapewormsF.F.
Simian Immunodeficiency Simian Immunodeficiency VirusVirus
G.G.
Monkey PoxMonkey PoxH.H.
Most of theseMost of theseI.I.
All of theseAll of these
?

Why refer?Why refer?
The risk of potentially The risk of potentially deadly infections (such deadly infections (such as SIV and Herpes B as SIV and Herpes B (CHV(CHV‐‐1)) and the 1)) and the decision for treatment decision for treatment depends on the type of depends on the type of monkey and duration monkey and duration since exposure.since exposure.
Emerg
Infect Dis. 2002 May;8(5):451‐7Clin. Infect. Dis. 2002;35:1191–1203

Case #6Case #6
A 21 year old female returned from India two A 21 year old female returned from India two months ago. months ago. She experienced a severe bout of travellerShe experienced a severe bout of traveller’’s s diarrhoea while in Bangalore. diarrhoea while in Bangalore. She was treated by a local physician with She was treated by a local physician with fluids, fluids, chloramphenicolchloramphenicol and and tinidazoletinidazole, but the , but the diarrhoea only got marginally better.diarrhoea only got marginally better.Diarrhoea has persisted for the past two Diarrhoea has persisted for the past two months.months.She reports her stools are loose but not She reports her stools are loose but not watery and extremely foul smelling.watery and extremely foul smelling.

What is the best course of action?What is the best course of action?
A.A.
Send to hospital emergency departmentSend to hospital emergency department
B.B.
Send to family doctor for referral to Send to family doctor for referral to
infectious diseasesinfectious diseases
C.C.
Send to travel health clinic for the next Send to travel health clinic for the next
available appointment.available appointment.
D.D.
Reassure and tell them they have IBSReassure and tell them they have IBS
E.E.
Start Start metronidazolemetronidazole

Diarrhoea only feels like and emergency!Diarrhoea only feels like and emergency!
Most cases of chronic diarrhoea can be Most cases of chronic diarrhoea can be managed as outpatients.managed as outpatients.
Fever, dehydration, confusion, loss of Fever, dehydration, confusion, loss of consciousness are danger signs.consciousness are danger signs.
Weight loss is a major concern, but not Weight loss is a major concern, but not emergent.emergent.
What are the top three diagnoses?What are the top three diagnoses?
A.A.
AmebiasisAmebiasis, tropical , tropical spruesprue, ,
cryptosporidiosiscryptosporidiosis
B.B.
Norwalk, Salmonella, Norwalk, Salmonella, ShigellaShigella
C.C.
GiardiasisGiardiasis, , amoebiasisamoebiasis, Norwalk virus, Norwalk virus
D.D.
ETEC, Norwalk, CampylobacterETEC, Norwalk, Campylobacter
E.E.
Unknown, Unknown, GiardiaGiardia, , AmoebiasisAmoebiasis
What investigations are appropriate?What investigations are appropriate?
A.A.
Stool for ova and parasitesStool for ova and parasites
B.B.
Stool for Stool for Clostridium Clostridium difficiledifficile
toxintoxin
C.C.
Stool electron microscopy for virusStool electron microscopy for virus
D.D.
A and BA and B
E.E.
A, B and CA, B and C

Take home pointsTake home points
Enteric viruses donEnteric viruses don’’t cause chronic diarrhoea.t cause chronic diarrhoea.Bacteria, besides Bacteria, besides C. C. difficiledifficile, rarely cause chronic , rarely cause chronic diarrhoea.diarrhoea.““UndiagnosedUndiagnosed”” (functional diarrhoea and post (functional diarrhoea and post infectious IBS) is the most common causes of infectious IBS) is the most common causes of chronic diarrhoea in returned travellers.chronic diarrhoea in returned travellers.GiardiasisGiardiasis is the most commonly is the most commonly identifiedidentified cause cause of chronic diarrhoea in returned travellers from of chronic diarrhoea in returned travellers from India.India.
Dupont, CID 2008
She is diagnosed with She is diagnosed with giardiasisgiardiasis
and fails two and fails two subsequent regimens of subsequent regimens of metronidazolemetronidazole. What is . What is
the next course of action?the next course of action?
A.A.
Try a third course of Try a third course of metronidazolemetronidazole
at 750mg at 750mg popo
TIDTID
B.B.
Send her back to the travel and tropical Send her back to the travel and tropical medicine clinic.medicine clinic.
C.C.
Refer for a Refer for a cholecystectomycholecystectomy
D.D.
Treat her family empiricallyTreat her family empirically
E.E.
A bowel washout with bleachA bowel washout with bleach
SecondSecond‐‐line drugs are available for line drugs are available for resistant or persistent resistant or persistent giardiasisgiardiasis!!
TinidazoleTinidazole, , SecnidazoleSecnidazole, , OrnidazoleOrnidazole
AlbendazoleAlbendazole
NitazoxanideNitazoxanide
QuinacrineQuinacrine
FurazolidoneFurazolidone
ParomomycinParomomycin
Case #7Case #7A 24 year old female adventure traveller returned A 24 year old female adventure traveller returned from a five week adventure rafting trip in Costa Rica from a five week adventure rafting trip in Costa Rica where she was camping with no access to where she was camping with no access to civilization. civilization. She drank treated river water and all food was She drank treated river water and all food was thoroughly cooked. thoroughly cooked. Developed travellerDeveloped traveller’’s diarrhoea now asymptomatic.s diarrhoea now asymptomatic.She presents with a nonShe presents with a non‐‐healing ulcerated lesion on healing ulcerated lesion on her right arm that is her right arm that is pruriticpruritic but nonbut non‐‐tender with no tender with no redness and intermittently expressing a clear redness and intermittently expressing a clear discharge. discharge. She has seen her doctor who prescribed an antibiotic She has seen her doctor who prescribed an antibiotic and steroid cream which worsened the condition.and steroid cream which worsened the condition.

The lesionThe lesion
What is the most appropriate course of What is the most appropriate course of action?action?
A.A.
Start a course of TMP/SMX for presumed Start a course of TMP/SMX for presumed MRSA infection.MRSA infection.
B.B.
Refer back to her family doctorRefer back to her family doctor
C.C.
Send her to the Travel Health SpecialistSend her to the Travel Health Specialist
D.D.
Send to the hospital emergency departmentSend to the hospital emergency department
E.E.
Reassure her and tell her it will go awayReassure her and tell her it will go away
Take a breatherTake a breather
Most skin disorders are not medical Most skin disorders are not medical emergencies.emergencies.••
Presence of fever, significant oedema, rapid Presence of fever, significant oedema, rapid
change or excessive pain are danger signs!change or excessive pain are danger signs!
ChronicityChronicity suggests a delay of a few days isnsuggests a delay of a few days isn’’t t dangerous.dangerous.Cause should always be sought.Cause should always be sought.••
Presentation, travel destination and appearance Presentation, travel destination and appearance
often point to a diagnosis.often point to a diagnosis.
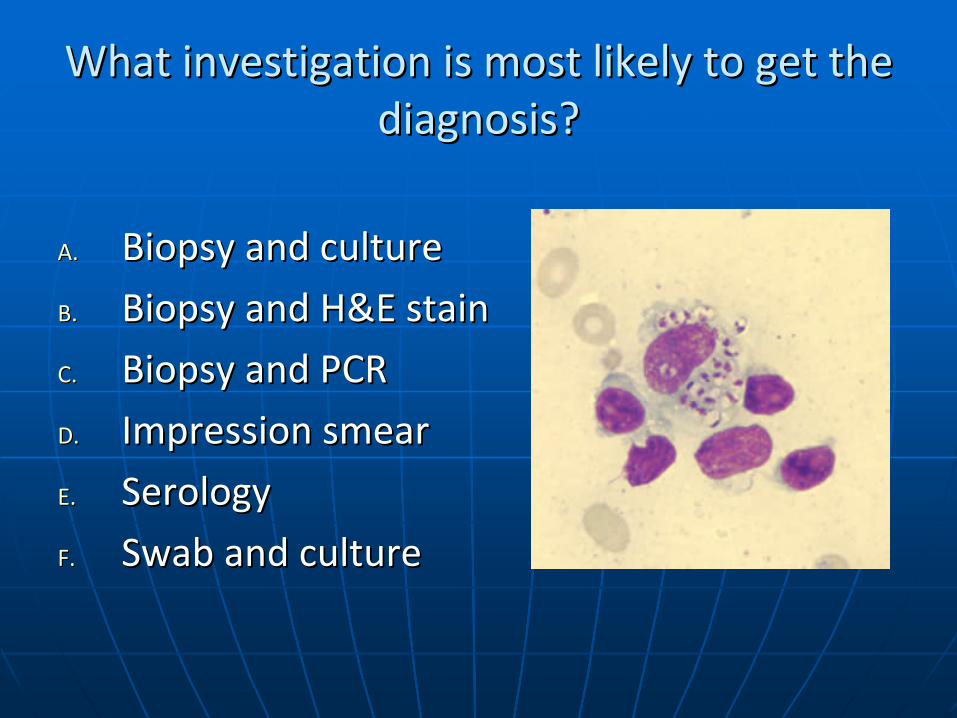
What investigation is most likely to get the What investigation is most likely to get the diagnosis?diagnosis?
A.A.
Biopsy and cultureBiopsy and culture
B.B.
Biopsy and H&E stainBiopsy and H&E stain
C.C.
Biopsy and PCRBiopsy and PCR
D.D.
Impression smearImpression smear
E.E.
SerologySerology
F.F.
Swab and cultureSwab and culture

Given the result of the tests and history, what is Given the result of the tests and history, what is the most likely pathogen?the most likely pathogen?
A.A.
L. L. chagasichagasi
B.B.
L. L. costaricensiscostaricensis
C.C.
L. L. panamensispanamensis
D.D.
L. L. mexicanamexicana
E.E.
L. L. braziliensisbraziliensis
Am. J. Trop. Med. Hyg., 41:687‐
725
The End!The End!

















